
Low back pain - bsphn.org.au · ~ 540 million people with activity limiting LBP at any one time!...
50
LOW BACK PAIN PRIMARY CARE USING THE PATTERN/SYNDROMIC APPROACH DR CORRIE BURGER CONSULTANT ORTHOPAEDIC SURGEON MBCHB(PRET), FCS(SA)ORTH, FRCSC, FRACS LOGAN HOSPITAL
Transcript of Low back pain - bsphn.org.au · ~ 540 million people with activity limiting LBP at any one time!...

LOW BACK PAINPRIMARY CARE USING THE PATTERN/SYNDROMIC APPROACH
DR CORRIE BURGER
CONSULTANT ORTHOPAEDIC SURGEON
MBCHB(PRET), FCS(SA)ORTH, FRCSC, FRACS
LOGAN HOSPITAL

DISCLOSURES:
• No affiliation or support from the Canadian Back Institute Health Group.
• This talk is based on my interpretation of the quotes and online
lectures/articles of Prof. Hamilton Hall, Canadian Spinal Surgeon.
• No affiliation with Udemy online education site.
• I’m not a Spinal Surgeon.

THE LEADING CAUSE OF DISABILITY WORLDWIDEGlobal point prevalence = 7,3%
~ 540 million people with activity limiting LBP at any one time!
“Just 25% of patients with LBP, generate 75% of the financial-and-social
costs for medical care and lost productivity”
Annual Cost USA ~ $ 100 Billion

IN AUSTRALIA, LOW BACKPAIN (LBP) IS THE MOST COMMON MUSCULOSKELETAL CONDITION FORWHICH PATIENTS CONSULT GENERAL PRACTITIONERS
• One in seven Australians(13.6%) have function limiting LBP on any day.
• Largest contributor to the burden of disease in Australia(Global Burden of Disease Study).
• Back problems: 3.7 million GP encounters annualy for LBP and are
likely to escalate. Expenditure on back pain alone is estimated to cost
~$1.2 billion / Year

IN AUSTRALIA, LOW BACKPAIN (LBP) IS THE MOST COMMON MUSCULOSKELETAL CONDITION FORWHICH PATIENTS CONSULT GENERAL PRACTITIONERS
• LBP is not a National Health Priority, despite having
higher burden of disease than Asthma, Diabetes,
Alzheimer, Ischaemic Heart Disease, Major
Depressive Disorders and Hearing Loss.
• From 2003 – 2013 the hospitalisation rate for back
problems increased from 762/100000 to
882/100000.

“ ElEmEntary my dear Watson, but how do we stem the tide ?
THE ‘BACK DOCTOR’
Prof. Hamilton Hall
How common is Low Back Pain?
Why is so common and on the
increase?

“DEATH, TAXES – AND - SORE BACKS, ARE THE PAINFULFACTS OF LIFE” - PROF. HAMILTON HALL
• “It’s more than common. It’s normal”. About eight out of every ten
humans are going to experience back pain at some time in their
lives.
• “Basically, people have a spine that’s built for cows and horses—for
four-legged creatures”. When we began walking on our hind legs,
we put the spine at a mechanical disadvantage. It needs support
front and back”. “Two hundred years ago people lived active lives
and had stomach muscles worthy of their back muscles”.
But why now, Prof ??
WHY ALL THE FUSS?
“90% of patients with back
ache get better within 90 days”

WHY ALL THE FUSS?
“90% of patients with back
ache get better within 90 days”

“Natural history = majority of backache heals spontaneously in 6 weeks”
• 1966 BMJ study by Dillane et al. suggested > 90% spontaneous
improvement within 6 weeks.
- Study never collected natural history data.
- Collected only care seeking data from GP scheduling logs.
- When patients did not return for follow up the researchers assumed
patient recovery.
Acute Back Syndrome – Study from General Practice
Dillane, Fry, Kalton BMJ 1966;2 :83 -84

TRUTH• ~ 20 – 44% of LBP sufferers will experience further episodes of pain
within one year, and > 75% will experience a recurrence in their
lifetime.
• Current EBM = Recurrences common.
= Recurrences worsen over time.
= Pain location often changes during episodes

“ < 2% of the average undergraduate – and -
post graduate curriculums at medical schools
are dedicated to LBP”
Major Guideline discordant rates: “ We rarely follow guidelines”
• MRI 60 – 90% False Positive order rate: 7% - 11,3% (2010 – 2015)
• Narcotic prescription rate for LBP: 19,3% - 29,1%.
• Specialist referral rate: 6.8% - 14,0%
(<10% referrals considered appropriate for Spinal Service assessment/Rx)

• No correlation between degenerative changes on X-ray and LBP.
• CT has > 30% False Positive rate.
• MRI 60 – 90% False Positive rate.
“Early MRI without indication has a strong negative iatrogenic
effect on acute LBP – No diagnostic benefit and worse
outcome.”
Webster et al. Spine 2013

• > 90% = Mechanical back pain of
benign origin.
• < 5% = “sinister” causes / Red flags :
# Tumour
# Infection
# Major trauma
# Other medical conditions: - Spondyloarthritis
- Retroperitoneal pathology

CURRENT “UPSIDE – DOWN” APPROACH
Exhaustively exclude the 5% “red canaries”
Blood tests MRI
Xrays CT scan
Non Specific Low Back pain (>90%)NSLBP
Non Specific ‘one size fits all’ Rx
“NSLBP” = MECHANICAL LOW BACK PAIN(DEFINITION)
• The most common (> 90% ) form of low back pain.
• IT IS PAIN RELATED TO MOVEMENT,
• IT IS PAIN RELATED TO POSITION,
• IT IS PAIN RELATED TO A PHYSICAL STRUCTURE IN THE BACK, IN WHICH THE
PHYSICAL STRUCTURE CANNOT BE PIN POINTED > 90% OF THE TIME.

“NSLBP” = MECHANICAL LOW BACK PAIN(DEFINITION)
• The most common (> 90% ) form of low back pain.
• IT IS PAIN RELATED TO MOVEMENT,
• IT IS PAIN RELATED TO POSITION,
• IT IS PAIN RELATED TO A PHYSICAL STRUCTURE IN THE BACK, WHICH
CANNOT BE PIN POINTED > 90% OF THE TIME.
BUT I HAVE TO
KNOW!!

Fortunately, you have
Non Specific Backpain,
which we will treat
non specifically!

Fortunately, you have
Non Specific Back pain,
which we will treat
non specifically!
Oh damn, they don’t
know what’s wrong,
IT’S SERIOUS, I’m
DOOMED !

ERRONEOUS TERMINOLOGY
• “Lumbago”
• “Sciatica”
• “Slipped disc”

IASP DEFINITIONS IN LBP
•Nociceptive back pain. BACK DOMINATED PAIN
•Somatic referred pain.
•Radicular pain.
•Radiculopathy.
On the definitions and physiology of back pain,
referred pain and radicular pain.
PAIN : 147(2009)17 -19 Nikolai Bogduk
LEG DOMINATED PAIN

WHY NOT START WITH:‘COMMON THINGS OCCUR COMMONLY’
Assess and manage MECHANICAL Low Back Pain > 90%
ASK LOOK
(HISTORY PARAMOUNT) FEEL
MOVE
FILTERING Process for the RARE conditions < 5%
LOW COST/
HIGH YIELD
Bloods, XR, CT, MRI ….
HIGH COST/
LOW YIELD

WHO’S THE BEST GATEKEEPER ?
• Task Forces, National and International Expert Committees agree:
“THE PRIMARY HEALTH CARE PROVIDER/ GENERAL PRACTITIONER
IS BEST SUITED IN MANAGING THE MAJORITY OF PATIENTS
WHO PRESENT WITH LOWER BACK PAIN, EITHER ACUTE-OR-
RECURRENT/CHRONIC IN NATURE.”

“ANOTHER WAY EXISTS”:
•In 1987 the Quebec Task Force noted:
‘‘Distinct patterns of reliable clinical findings
are the only logical basis for back pain
categorization and subsequent treatment”

THE PATTERN/SYNDROMIC APPROACH
• Employing syndrome recognition allows the
majority of patients with back pain to be
sorted into FOUR clearly defined groups, each
with recognizable physical characteristics and
pattern specific treatment.

“The goal is control, not cure,
and control is not only
possible,
it is readily achievable.”

SYNDROME RECOGNITION
•A Syndrome can be defined as a constellation
of signs and symptoms appearing together in
a consistent manner and responding to
treatment in a predictable fashion.

PATTERN/SYNDROME RECOGNITION
• The Key is correctly identifying the presenting syndrome or pattern of pain.
• This identification depends on:
# Precise history
and:
# A concordant physical examination.
# The third essential element of the process is progression to the anticipated
treatment response.
FILTERING / “FAIL SAFE”
•The inability to distinguish a clear pattern on first contact
or a syndrome’s failure to improve with the specified
therapy, demands reassessment, including a review of the
signs and symptoms, additional physical tests, and,
perhaps, ancillary investigations.

CLINICAL ORTHOPAEDIC RELEVANT EXAM




PATTERN APPROACH: PATIENT HISTORYDetermining the Patient’s Pain Syndrome:
1. Where is your pain the worst?
2. Is your pain constant or intermittent?
3. Does bending forward increase your typical pain?
Determining the Patient’s Bowel and Bladder Status: MANDATORY QUESTIONS
4. Since the start of your pain, has there been any change in your
bowel or bladder function?
Determining the Patient’s Disability Level and Confirming Site of Dominant Pain:
5. What can’t you do now that you could do before your pain started and why?
Assessing the Mechanical Aspects and History of the Patient’s Pain:
6. What are the relieving movements or positions?
7. Have you had this type of pain before?
8. Have you had treatment?

ONE ADDITIONAL NON MECHANICAL QUESTION
9. If you are < 45yrs old, do you have morning back stiffness that lasts more
than 30minutes ?
Consider spondyloarthropathy ( Ankylosing spondylitis, Reactive-, Psoriatic-,
enteropathic- spondyloarthropathy)

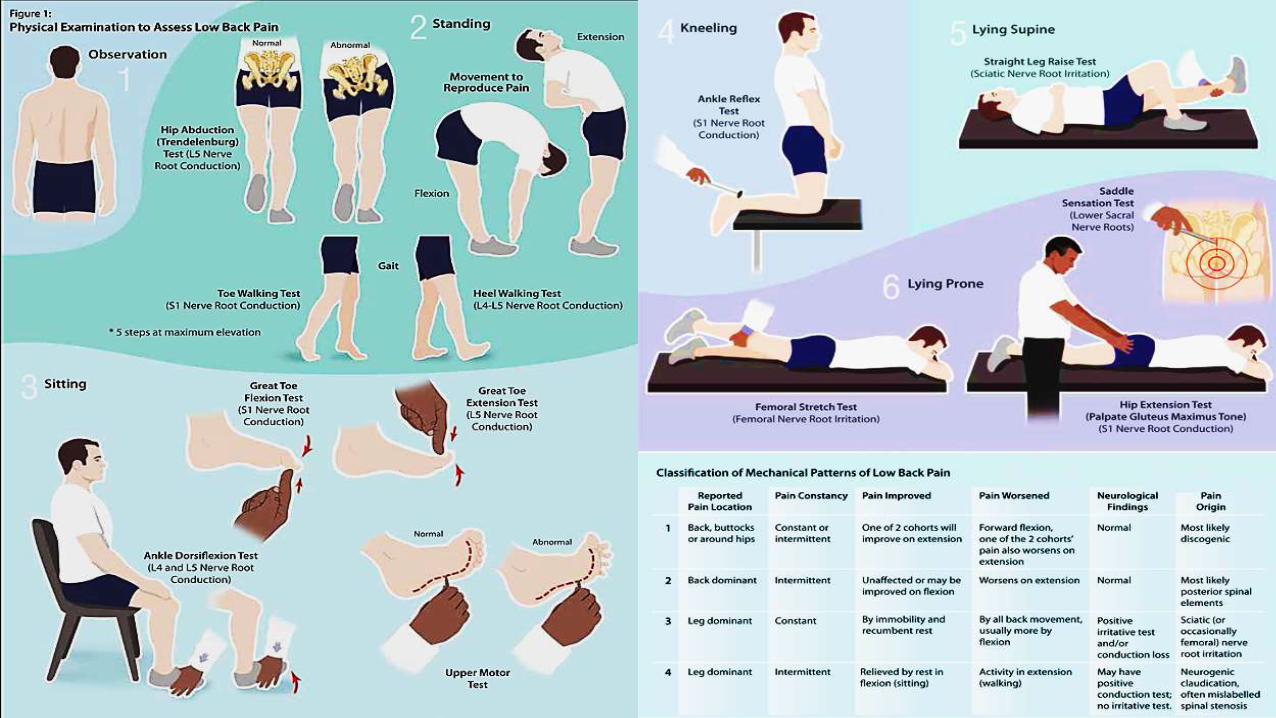

THE FOUR PATTERNS OF PAIN ARE:
• Pattern 1: Constant/intermittent Back dominant Aggravated by Flexion
• Pattern 2: Intermittent Back Dominant Pain
• Pattern 3: Constant Leg Dominant Pain Aggravated by Flexion
• Pattern 4: Intermittent Leg Dominant Pain
“The goal is control,
not cure,
and control is not only
possible,
it is readily achievable.”

WHAT CAN BE DONE FOR CHRONIC/RECURRENT BACK PAIN ?
Four A’s of Self Management:
• Attitude.
• Accountability.
• Abdominal exercise.
• Activities of Daily living.

“HOW DO PATIENTS GET BETTER ?”
• Attitude
Relax and realize that backache is not life-threatening and not a disease.
• Accountability
Accountability means taking responsibility for your own care if you’re going to get better.
• AODL’S
Sitting in controlled slump and standing in ‘pelvic thrust’ and use a foot stool (‘Bartenders brass rail’)
• Abdominal exercises
Pelvic tilt fundamental
PATTERN RECOGNITION PROF. HAMILTON HALL:
• “Pain pattern recognition is a rapid, reliable, and efficient triage
technique that increases diagnostic accuracy, enables patient-specific
management, and decreases needless investigations.”
• “Filtering out patients accurately identified with mechanical LBP and
successfully managing them with noninvasive physical treatment (more
than 90% of the total) greatly increases the probability of discovering
potentially menacing nonmechanical diagnoses among the remainder.”



PHYSIOTHERAPY REFERRAL FOR MECHANICAL LBP
• Absence of red flags.
• Pain is managed well, so that patient can tolerate treatment.
• Pain has mechanical directional preference – varies with movement, position
or activity.
• Patient is ready to be an active partner in goal setting and self management.

SURGICAL REFERRAL FOR MECHANICAL LBP
• Failure to respond to evidence based compliant conservative care of at least 12
weeks.
• Unbearable constant leg dominant pain.
• Worsening nerve irritation tests (SLR or femoral nerve stretch).
• Expanding motor, sensory or reflex deficits.
• Recurrent disabling radicular pain.
• Disabling neurogenic claudication.

BENEFITS OF THE CLASSIFICATION SYSTEM
• Significantly more patients discharged after education, self-care advice, and conservative
care(72%)
• More appropriate referrals to Spinal Surgeon(from < 10% to 38%)
• Inappropriate MRI use significantly reduced(92∙0%)
• Shorter waiting times for MRI and surgical assessment(25%)
• Fourney DR, Dettori JR, Hall H, Hartl R, McGirt MJ, Daubs MD. A systematic review of clinical pathways for lower back pain and
introduction of the Saskatchewan Spine Pathway. Spine 2011;36 : S164−71.
• Kindrachuk DR, Fourney DR. Spine surgery referrals redirected through a multidisciplinary care pathway: effects of non-surgeon
triage including MRI utilization. J Neurosurg Spine 2014;20: 87−92.
• Wilgenbusch CS, Wu AS, Fourney DR. Triage of spine surgery referrals through a multidisciplinary care pathway: a value-based
comparison with conventional referral processes. Spine 2014;39 : S129−35.

WEBSITE TRAINING:
https://www.udemy.com/home/mycourses/learning/


















