Loss Hurts - Stroke Associationwcm/...can stick together and form clots. PLAVIX helps keep blood...
36
Loss Hurts The importance of allowing the grieving process JANUARY | FEBRUARY 2008 STROKE CONNECTION Growing Peace of Mind Tips from a gardening survivor Reclaiming My Dignity The frustration of dealing with insensitive people Sleep Apnea A wake-up call about a little-known stroke risk Going Downhill and Loving It Even a stroke on the slopes couldn’t stop this skier Life at the Curb Everybody Must Get Stones StrokeAssociation.org Stroke Connection is underwritten in part by Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership, makers of Plavix. ®
Transcript of Loss Hurts - Stroke Associationwcm/...can stick together and form clots. PLAVIX helps keep blood...

Loss HurtsThe importance of allowing
the grieving process
JAN UARY | FEBR UARY 2008
S T R O K E CO N N E C T I O N
Growing Peace of MindTips from a gardening survivor
Reclaiming My Dignity The frustration of dealing with
insensitive people
Sleep ApneaA wake-up call about a little-known stroke risk
Going Downhill and Loving It
Even a stroke on the slopes couldn’t stop this skier
Life at the CurbEverybody Must Get Stones
S t r o k e A s s o c i a t i o n . o r g
Stroke Connection is underwritten in part by Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership, makers of Plavix.
®

STAFF AND CONSULTANTS:
Dennis Milne Vice President
American Stroke Association
Wendy Segrest Director
American Stroke Association Operations
Debi McGill Editor-in-Chief
Jon Caswell Lead Editor
Pierce Goetz Art Director
Jennifer Sellers Writer
Kathy White Advertising Sales
Stroke Connection Magazine is underwritten in part by Bristol-Myers Squibb/Sanofi
Pharmaceuticals Partnership, makers of Plavix.
Cover S to ry
16 ‘The Way We Were’ Strokecausesallsortsoflossesfor
survivorsandtheirfamilies—fromphysicaldisabilitiestospeechimpairmentstocognitiveandemotionalchanges.Weinvestigatetheimportanceofgrievingthoselosses.
F e a t u r e s
14 Growing Peace of Mind SurvivorDavidLaytonofSummerfield,
NorthCarolinahasfoundthatgrowingasummergardenimprovesmanythings—hisrecovery,hismoodandhisdiet!
22 Reclaiming My Dignity Theworldoutsideofhomeisnotalways
afriendlyplaceforsurvivorswithaphasia.ForDonWeinsteinregularvisitstoaneighborhooddeliprovidedopportunitiestofeelelatedanddefeated.
24 Going Downhill and Loving It ToniJohnsonhadastrokewhileskiing
atage75,thenshebrokeherlegwhilerelearningthesport.At80,she’sbackontheslopes.
26 Get a Good Night’s Sleep AND Reduce Your Risk
Turnsoutsnoringmaybemorethanannoyingtoyourspouse—itmaydoubletheriskofstroke.Thegoodnewsisthere’ssomethingyoucandoaboutit.
Depar tments
4 LetterstotheEditor
6 StrokeNotes
10 ReadersRoom
29 LifeattheCurb
30 EverydaySurvival
a division of
Produced and distributed in cooperation with Vitality Communications
S t r o k e A s s o c i a t i o n . o r g
JA N UARY | FEBR UARY 2008
S T R O K E CO N N E C T I O N
Copyright 2008 American Heart Association ISSN 1047-014X
Stroke Connection is published six times a year by the American Stroke Association, a division of the American Heart Association. Material may be reproduced only with appropriate acknowledgment of the source and written per mission from the American Heart Association. Please address inquiries to the Editor-in-Chief.
The information contained in this publication is provided by the American Stroke Association as a resource. The services or products listed are not owned or provided by the American Stroke Association. Additionally, the products or services have not been evaluated and their listing or advertising should not be construed as a recommendation or endorsement of these products or services.
Contents
1 - 8 8 8 - 4 S T R O K E ( 1 - 8 8 8 - 4 7 8 - 7 6 5 3 )
1614
24
26
®
Help raise your protection against anotherstroke with PLAVIX. If you’ve had a heart attack or stroke, the last thing you want is another onesneaking up on you. PLAVIX may help. PLAVIX is aprescription medication for people who have had arecent heart attack or recent stroke, or who havepoor circulation in the legs (peripheral artery disease)causing pain.
IMPORTANT INFORMATION: If you have a stomachulcer or other condition that causes bleeding, youshould not use PLAVIX. When taking PLAVIX aloneor with some other medicines including aspirin, therisk of bleeding may increase so tell your doctorbefore planning surgery. And, always talk to yourdoctor before taking aspirin or other medicines withPLAVIX, especially if you’ve had a stroke. If youdevelop fever, unexplained weakness or confusion,tell your doctor promptly as these may be signs ofa rare but potentially life-threatening condition calledTTP, which has been reported rarely, sometimes inless than 2 weeks after starting therapy. Other rarebut serious side effects may occur.
PLAVIX offersprotection.PLAVIX isproven to helpkeep bloodplatelets from
sticking together and forming clots, which helpskeep your blood flowing. This can help protect youfrom another heart attack or stroke.
Talk to your doctor about PLAVIX. For more information, visit www.plavix.com
or call 1-888-852-9381.
Please see important product information forPLAVIX on the following page.
9Add more protection against heart attack or stroke
If you’ve had a stroke, your chance of having another
is 9 times greater.
If you need help paying for prescriptionmedicines, you may be eligible for assistance.Call 1-888-4PPA-NOW (1-888-477-2669).Or go to www.pparx.org.
US.CLO.07.11.127/November 2007 Printed in USA 264US07AB34104-11-07sanofi-aventis U.S. LLC© 2007 Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership
Blood platelets can stick together
and form clots.
PLAVIX helps keep blood platelets from
sticking together.
A1022 BMS_FP.indd 1 12/6/07 8:10:34 AM
Help raise your protection against anotherstroke with PLAVIX. If you’ve had a heart attack or stroke, the last thing you want is another onesneaking up on you. PLAVIX may help. PLAVIX is aprescription medication for people who have had arecent heart attack or recent stroke, or who havepoor circulation in the legs (peripheral artery disease)causing pain.
IMPORTANT INFORMATION: If you have a stomachulcer or other condition that causes bleeding, youshould not use PLAVIX. When taking PLAVIX aloneor with some other medicines including aspirin, therisk of bleeding may increase so tell your doctorbefore planning surgery. And, always talk to yourdoctor before taking aspirin or other medicines withPLAVIX, especially if you’ve had a stroke. If youdevelop fever, unexplained weakness or confusion,tell your doctor promptly as these may be signs ofa rare but potentially life-threatening condition calledTTP, which has been reported rarely, sometimes inless than 2 weeks after starting therapy. Other rarebut serious side effects may occur.
PLAVIX offersprotection.PLAVIX isproven to helpkeep bloodplatelets from
sticking together and forming clots, which helpskeep your blood flowing. This can help protect youfrom another heart attack or stroke.
Talk to your doctor about PLAVIX. For more information, visit www.plavix.com
or call 1-888-852-9381.
Please see important product information forPLAVIX on the following page.
9Add more protection against heart attack or stroke
If you’ve had a stroke, your chance of having another
is 9 times greater.
If you need help paying for prescriptionmedicines, you may be eligible for assistance.Call 1-888-4PPA-NOW (1-888-477-2669).Or go to www.pparx.org.
US.CLO.07.11.127/November 2007 Printed in USA 264US07AB34104-11-07sanofi-aventis U.S. LLC© 2007 Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership
Blood platelets can stick together
and form clots.
PLAVIX helps keep blood platelets from
sticking together.
A1022 BMS_FP.indd 1 12/6/07 8:10:34 AM

ItemNo: 264US07AB34104 TrimSize: 8.25" x 10.75” Publication:Stroke Connections Ad
WHO IS PLAVIX FOR?
WHO SHOULD NOT TAKE PLAVIX?
WHAT SHOULD I TELL MY DOCTOR BEFORE TAKING PLAVIX?
WHAT IMPORTANT INFORMATION SHOULD I KNOW ABOUTPLAVIX?
WHAT SHOULD I KNOW ABOUT TAKING OTHER MEDICINES WITHPLAVIX?
WHAT ARE THE COMMON SIDE EFFECTS OF PLAVIX?
HOW SHOULD I TAKE PLAVIX?
OVERDOSAGE
FOR MORE INFORMATION
264US07AB34104_9Ad 12/4/07 12:48 PM Page 2

NESS®, NESS L300™, NESS H200™ Intelli-Gait™ and Intelli-Sense Gait Sensor™ are trademarks of N.E.S.S. Neuromuscular Electrical Stimulation Systems, Ltd., Ra’anana, Israel | Manufacturer: N.E.S.S. Neuromuscular Electrical Stimulation Systems, Ltd. | North American Distributor: Bioness Inc. | Bioness®, the Bioness Logo® and LiveOn™ are trademarks of Bioness Inc., Valencia, CA |
Designed to improve hand function, the NESS H200 may reducemuscle spasms, decrease pain and increase muscle strength inthose living with certain upper extremity conditions.1, 2
Designed to eliminate the need to wear a rigid ankle brace, theNESS L300 may increase speed and stability in those living withcertain foot drop conditions.3
®
YOU MAY NOT BE AT THE END OF YOUR RECOVERY
923-10009 10-009-BA08
FOR MORE INFORMATION CALL US AT 800.211.9136 | BIONESS.COM
NESS H200™ HAND REHABILITATION SYSTEM
NESS L300™ FOOT DROP SYSTEM
Rx Only
1 - G. Alon, K. McBride and H. Ring. Improving selected hand functions using a noninvasive neuroprosthesis in persons with chronic upper extremity paresis following a stroke. Journal of Cerebrovascular Disease. 2002; 11:99-106.2 - G. Alon, KS Sunnerhagen, AC Geurts and A Ohry. A home-based, self-administered stimulation program to improve selected hand functions of chronic stroke. NeuroRehabilitation. 2003;18(3):215-225.23 - H. Weingarden and J. Hausdorff. FES Neuroprosthesis versus an Ankle Foot Orthosis: the effect on gait stability and symmetry. Presented on June 5, 2007 at the 15th World Confederation for Physical Therapy, Vancouver, Canada.
A1014_Bioness.indd 1 12/3/07 9:13:58 AM

4 S T RO K E CONNECT ION January | February 2008
YOUR LETTERS | Connecting You to Us
We’d like to hear from you!
E-MAIL US AT: [email protected]. Or send letters to: Editor-in-Chief, Stroke Connection, 7272 Greenville Avenue, Dallas TX 75231. Letters may be edited for length and scientific integrity. The opinions presented are those of the individual and do not reflect those of the American Stroke Association.
Thanks for an Inspiring Letter In response to Keith Millard’s letter in the July/August issue, I want to say THANK YOU. I, too, work a 40-hour week while caring for my stroke survivor husband. While I’m just glad he’s here and wouldn’t trade my life for anyone’s, sometimes it is a difficult balancing act. Keith
mentioned one of the hardest things as not being able to vent his anger and frustration adequately. There are support groups, but who has time for them? I’m fortunate to have friends who are also caregivers, and I admit that three years ago, I didn’t understand some of their pain like I do now.
I appreciate his mentioning that men have more strength for transfers. Every morning I search my closet for the Wonder Woman outfit, but so far, it has not appeared.
There was one thing he was very wrong about, and that’s saying that he and his wife are not a “success story.” Although his lovely wife may have experienced minimal recovery from her stroke, success is in the living. Both of them are not only living their lives to the fullest potential, they serve as an inspiration to everyone who knows them.
Thank you again for an uplifting letter!
Colleen Lewis, CaregiverWindsor, New York
Playing Again When my wife found me on the kitchen floor unable to form words properly or stand, she knew immediately that I had had a stroke. Our local hospital raced me through tests and quickly determined that I was a good candidate for TPA. Shortly after I received the drug, my walking returned and my speech slowly improved. I am a middle school band director and was worried about my ability to continue as a teacher in such an active job. Several of my band parents were
my doctors throughout my ordeal and continue to keep an eye on me. The most risky behavior I engage in is teaching middle school!
I’ve read with interest about constraint-induced therapies. I am a trumpet player and have used this approach by lightly resting my hand on the “good side” of my mouth to force the affected side to work harder. I’ve extended this forced response by making myself wink, by using my weak hand for everyday physical activities, and most importantly by resuming my trumpet playing, which works all my facial muscles.
Having a great support group makes this so much easier. My family, school staff, church family and my band parents, who are doctors and therapists, all have made this a surmountable situation. Keep up the timely articles.
David Teague, Survivor Waynesville, North Carolina
Turning Feelings Into Songs Today marks the third anniversary of my husband Eric’s ischemic stroke. It was devastating to him and to all of us. However, he has made great strides on his road to recovery.
A former singer and musician, Eric used the power of music to make that hard climb to where he is now. After his stroke, he was unable to speak, but on April 3, 2007, he sang at the opening of the Edward R. Gordon Stroke Center in Los Angeles.
Eric experiences involuntary emotional expression disorder (IEED), but we have worked together to turn this condition around and to use it as a “friend.” I’ve coached my husband to accept this feeling and use the energy to project his feelings into songs. He’s also published a poem in a local caregiver newsletter.
We appreciate the help and support of the Southern California Stroke Association, which propelled Eric forward to seek creative avenues of expression. This is just the beginning!
Emilia Scanlan, CaregiverLos Angeles, California
5January | February 2008 S T RO K E CONNE CT I ON
A revised and updated edition of
Do you have trouble putting on your shoes due to:
Stroke
MSShu-Aide can assist you with putting on your shoes. It was invented by stroke survivor, Mike Huske, who wanted more independence in his daily life.
SHUAIDE . . .For Independent Living
“I would recommend this device for anyone wanting to be independent putting on their shoes, with or without ankle foot orthosis (AFO).” - Corrine C. Voss, Physical Therapist
Shu-Aide comes fully assembled with instructions.
TO ORDER your Shu-Aide, send an e-mail to [email protected] or call (920) 323-9707 between the hours of 8 am – 5 pm Central.
Please send to:American Heart Association Planned Giving Department7272 Greenville Avenue • Dallas, TX 75231-4596
Putting Your House In OrderMeans More Than Cleaning It.
My sister would always leave her house spic-and-span whenever she went away on a trip — “just in case” something happened. When she died, the house was spotless, but her estate was a mess. We couldn’t even find her will, to find out what her wishes were.
Many people don’t realize how critical it is, for both themselves and their loved ones, to have a well-thought-out estate plan. To help you get started, request a copy of our free book Estate Planning Success® for Women*. A
representative from the American Heart Association will personally deliver it to you. We know you will find this information invaluable as you plan your estate.
*While supplies last
You can also call toll-free 1-888-227-5242, visit us at americanheart.org/plannedgiving or e-mail [email protected].
o Please deliver to me the free book Estate Planning Success® for Women. (FDA)
o Please put me in touch with an American Heart Association Representative. (FDD)
o I am considering a gift to the American Heart Association through my estate plan. (FDC)
o I have already included the American Heart Association in my will/estate plan. (FDB)
Name
Address
City/State/ZIP
Phone Birthdate
©2007, American Heart Association. 10/07LS1549
IAD SC 01/0808GPGBA

6 S T RO K E CONNECT ION January | February 2008
STROKE NOTES | Connecting You to the World
troke survivors who stop taking cholesterol-lowering drugs within a year of a stroke had a two-fold increased risk of death, researchers reported in Stroke: Journal of the American Heart Association.
Statins can benefit patients who have suffered an ischemic stroke, by lowering blood levels of low-density
lipoprotein cholesterol (LDL), known as “bad” cholesterol. However, these drugs have major side effects, and survivors often stop taking them.
The observational study ran for four-and-a-half years at San Filippo Neri Hospital in Rome, Italy, in collaboration with the Institute for Clinical Research Santa Lucia Foundation of Rome. Researchers identified 631 stroke survivors (322 men and 309 women, average age 70 years). None had any other major illness, including heart disease. All patients were discharged from the hospital with orders to take a drug regimen including statin therapy.
By the end of the study, 38.9 percent of the patients — 246 patients — had stopped taking statins. The average time to discontinuation was 48.6 days.
Seventy-one patients (28.8 percent) cited mild side effects, the most common of which was indigestion, as the reason for discontinuing the drug. In the other 175 cases (71.2 percent), neither the patient nor the primary care physician could give specific medical reasons for discontinuation. Similar figures have been reported in studies in the United States.
Because medication costs are covered by the Italian National Health Service, except for a small co-pay, cost was not the reason the patients discontinued their prescribed therapy.
During the study, 116 patients died. Eighty percent of these deaths were attributed to cardiovascular causes.
Statistical analysis determined that discontinuing statin therapy was independently and significantly associated with increased risk of death from any cause. Patients who had stopped taking statins within a year of stroke were more than twice as likely to die than others in the study group.
Stay on Your StatinsPatients who stop using statins after
stroke increase risk of death

7January | February 2008 S T RO K E CONNE CT I ON
Two campaigns to reduce stroke and CVD in women
Although many women don’t realize it, they are at major risk of heart disease and stroke. Did you know that more women die of strokes than men? It’s true, 61 percent of all stroke deaths occur in women, and
cardiovascular disease is the leading cause of death in women over age 25.
That’s the bad news. The good news is you can do something about it. The Centers for Disease Control and Prevention (CDC) has launched the WISEWOMAN program to help change those numbers. The program, administered through the CDC’s Division for Heart Disease and Stroke Prevention, works with low-income, under- or uninsured 40-to-60-year-old women, providing risk factor screening, lifestyle intervention and referral services. Women can also take advantage of lifestyle programs focused on nutrition, physical activity and smoking cessation, healthy cooking classes and fitness
competitions. There are 15 WISEWOMAN programs. For more information, including locations, visit www.cdc.gov/wisewoman/ or call 1–800–CDC–INFO (1–800–232–4636) and choose Option #1.
The American Heart Association’s Go Red For Women is a campaign to improve public awareness of women’s cardiovascular health. Participation is simple — wear red on Feb. 1, 2008, and register to receive a free monthly newsletter with health tips, a free red dress pin and shopping discounts from Macy’s. Over 12 million women have already registered. To learn more, visit www.goredforwomen.org.
People who have stroke-like symptoms but no stroke diagnosis incur physical and mental damage that significantly lowers their quality of life, according to a report in Stroke: Journal of the American Heart Association.
In a study reviewing data from more than 21,000 people, those reporting stroke-like symptoms had functional impairment similar to that of people who had a history of transient ischemic attack (TIA). Because almost 20 percent of people older than age 45 may have vague or “whispering stroke” symptoms, the condition poses a major public health problem.
“Silent” strokes are diagnosed with brain imaging that detects damage in people who did not have any apparent
stroke symptoms. However, some silent strokes may be better described as “whispering” because there are symptoms, but they are so minor that they don’t alarm the patient or raise concern to physicians.
In this study, 3,404 participants said they had experienced stroke-like symptoms but had no stroke or TIA diagnosis; 818 had a history of TIA; and 1,491 had a history of stroke.
Compared to people with no symptoms or history of stroke or TIA, people with stroke-like symptoms had a 5.5-point decrease on a scale of physical functioning. Participants who reported a history of weakness or numbness had larger current deficits in physical functioning.
A sudden loss of ability to understand or to talk or write had the greatest impact on function. Those symptoms were associated with a four-to-five point reduction in scores on the measures of physical and mental functioning.
Women and Their Health
Small Symptoms May Produce Big Consequences
“Whispering stroke” symptoms may damage health, lower quality of life

8 S T RO K E CONNECT ION January | February 2008
new act approved by a national law group addresses the problem of resolving multi-state jurisdictional disputes over adult guardianships, a growing concern with the country’s aging
population. The Uniform Adult Guardianship and Protective Proceedings Jurisdiction Act was approved in August by the Uniform Law Commission (ULC) at its 116TH Annual Meeting in Pasadena, Calif.
“Because there are more than 50 guardianship systems in the United States, problems of determining jurisdiction are frequent,” said David G. Nixon, chair of the committee that drafted the new act. “Questions of which state has jurisdiction to appoint a guardian for an incapacitated adult can arise between different states. The new Uniform Adult Guardianship and Protective Proceedings Act will provide the states with a much-needed solution for resolving these multi-state jurisdictional disputes.”
The new act addresses the issue of jurisdiction over adult guardianships, conservatorships and other protective proceedings.
The objective of the new uniform act is simple: to ensure that only one state has jurisdiction at any one time. The act has guidelines to specify which court has jurisdiction to appoint a guardian or conservator for an incapacitated adult. It does this by prioritizing the states that might claim jurisdiction. The state with primary jurisdiction is the “home state,” the state in which the adult has lived for at least six consecutive months immediately before the beginning of the adult guardianship or protective proceeding.
This act accomplishes the same certainty for adult guardianship determinations that exists in child custody law since the 1997 Uniform Child Custody Jurisdiction and Enforcement Act, which is now law in 48 states.
Further information on the Uniform Adult Guardianship and Protective Proceedings Act can be found at the ULC’s Web site, www.nccusl.org.
Source: Uniform Law Commission
he American Stroke Association (ASA) is conducting a multiyear initiative to improve stroke care across the nation by coordinating State Stroke Systems Planning in each of the
50 states. This effort includes working with partners and stakeholders involved in stroke care to assess each state’s current level of stroke care, evaluate available resources, identify opportunities for improvement and implement needed improvements.
Here are a few examples of the association’s recent successful stroke systems of care policy efforts:
• Georgia established the Joint Stroke Systems of Care Study Committee, designed to examine the stroke systems of care approach, including increasing the number of hospitals that are designated primary stroke centers.
• In Illinois, the ASA worked with volunteers and interested groups to introduce the Primary Stroke Center
Designation Act, legislation that would allow the director of the Illinois Department of Public Health to designate qualified facilities as Primary Stroke Centers.
• Massachusetts appropriated $500,000 for stroke care to ensure access to quality stroke prevention, treatment and rehabilitation services.
• The Montana State Legislature allocated $1.25 million in funding for the Cardiovascular Section of the Department of Public Health and Human Services for stroke awareness and education, as well as for funding a telemedicine project between a rural hospital and two of Montana’s certified stroke centers.
• In North Carolina, the General Assembly approved $900,000 in funding to begin efforts to establish a stroke system of care.
• Texas secured $1.5 million in funding for its previously enacted Stroke Act.
Taking Care of Parents across State LinesNew act addresses the problem of adult guardianship jurisdiction
Improving Stroke Systems in the StatesStates are gearing up for improvements in stroke care and education
STROKE NOTES | Connecting You to the World A Dynamic Solution for a Dynamic Problem™
What may happen when you put a dynamic hand in a static splint?
To learn more about this revolutionary new splint, visit our website at www.saebo.com or call 888-284-5433
Leaders in Stroke Rehabilitation
Position Your Hand for the Best Chance of Recovery
SaeboStretch®
Patent Pending
A785 Saebo.indd 1 12/3/07 10:32:55 AM

A Dynamic Solution for a Dynamic Problem™
What may happen when you put a dynamic hand in a static splint?
To learn more about this revolutionary new splint, visit our website at www.saebo.com or call 888-284-5433
Leaders in Stroke Rehabilitation
Position Your Hand for the Best Chance of Recovery
SaeboStretch®
Patent Pending
A785 Saebo.indd 1 12/3/07 10:32:55 AM

10 S T RO K E CONNECT ION January | February 2008
READE RS ROOM | Connecting You to Others
id I or didn’t I? That is the question on my mind since March 17, 2003. That’s the day I had a stroke. At least that is what the CT scan showed and what my doctor told me happened. Certainly I knew something bad had happened but I wasn’t sure what or why.
At the emergency room where my wife worked at the time, the doctor suspected I’d had a stroke and a CT scan confirmed it. But I was referred to another hospital that specialized in neurological events. My first CT scan was not available for some reason and they did another one. The neurologist there was not sure what had happened but seemed positive it was not a stroke.
Whatever happened, I could not talk for about three weeks and had right-side weakness. I could not read or write, tell time or handle more than one person at a time talking to me. I cried a lot and slept more. It was a pretty awful time for us, but gradually I have recovered a great deal and I am doing well.
I found two things healing for me. The first was humor. Shortly after the stroke, I received a book in the mail from the Heart and Stroke Association of Canada explaining things that a survivor can expect to experience after a stroke. I found it quite useful and soon it became my “what I can get away with” manual. If the book said that survivors may say inappropriate things at times, I would say something
inappropriate and point at the book when someone took offense. If it said my taste might be off and I refused to eat my vegetables, I would point at the book. This worked well until my wife read the book and realized what I was up to, but this got me through the first few weeks of my new reality.
The second healing thing was writing. I loved to write before the stroke and still do. It is probably the only time I truly feel whole. I cannot do it for as long as I used to, but it is such a wonderful thing for me that I try to write as often as I can.
I believe that humor and creativity are healing to us all. Choose a creative outlet you find rewarding and can still do. But whatever you do, do something. Even if you just get a little bit of peace and fun, it is way better than no fun at all!
This is not the life I thought I would have but thanks to good doctors, a lot of prayers and support, it is a rewarding life. It is odd that I have a split decision about what I had on St. Patrick’s Day almost five years ago. Whatever it was, it certainly has been a challenge for both me and my family. Now the future is uncertain, but whatever it brings, I know that I am stronger than I was before and will be able to handle it.
Andy Becker, SurvivorRegina, Saskatchewan, Canada
What Happened to Andy?I believe that humor and creativity are healing to us all.
above: Stella and Andy Becker; right: Andy and granddaughter Clara

11January | February 2008 S T RO K E CONNE CT I ON
My Journey am the oldest of five girls and the mother of one son, DeShown. He was 13 and I was 40 when I had my stroke on Christmas Eve 2005. I had just finished reading a Christmas card from my neighbor when my vision became blurred. When I tried to stand up, I fell. It was 11 a.m. and I was home alone. I tried to call my sister Danielle, but when she called back, she
couldn’t hear me. I didn’t realize that I could not talk. I didn’t get any help till 2 p.m.
I looked in the mirror and what I saw scared me — my entire right side was slumped. When I finally got 9-1-1, the operator said it sounded like I was having a stroke. My sister was the first family member to arrive, and she called my mom and said, “You better come quickly because she doesn’t look too good.” I slept for two days, though I did wake up occasionally and noticed there were a lot of family and friends around me. My sister, Andre, and my cousin stayed with me all night, giving me a bath and changing my diaper.
I found out that prayer works. There were lots of people praying for me; most important was my son. I cried horribly when he left to go live with his father in Richmond for a time.
My parents took turns staying with me while I was recuperating. On Jan. 4, 2006, I was transferred to a rehab unit, and a month and nine days later I surprised myself by walking out of there on my own. I also had apraxia and could only say “yes.” The moment I learned how to say “no,” I went around saying it all day long!
When I got out of rehab in February, I moved in with Danielle. In March I moved into my own apartment, and my sister Andre and my niece helped me get in and out of the shower. My sister Renitta came by every night and brushed my teeth because I could not use my right hand, and I’m right-handed. My sister Jacquetta brought a loaf of banana bread.
Here’s what I’ve learned: If you’re on high blood pressure medicine, take it! A stroke does not care how old or young you are. Through this journey, I never lost my faith in God. He has brought me a long way, and I know He won’t leave me now.
Michelle Boozer, SurvivorMidlothian, Virginia
I Had a Stroke (or Two) I had a stroke, blood flow stopped to my brain.
Six years later, it happened again,
But at least I’m alive, I can walk, I can drive,
And thank God, no paralysis or pain.
But I’m not all that lucky, you see,
The love of my life, she left me.
After 35 years — there were laughs, there were tears,
She took off, now how can this be?
All she could say to me was “You changed.
Your manners and moods are rearranged.
I do not see how I can live with you now.”
So she left me and now we’re estranged.
So here’s my advice — and no joke.
Eat healthy and don’t have a stroke.
Or at least do be very careful whom you marry,
Or she might take off, leaving you broke.
Remember, when making your plans,
Some things are just “out of your hands,”
Of which you have no control, and you fall in a hole,
Where you inflict too many demands.
Now please, do not shed a tear for me,
I’m a survivor, I’ll get by, you’ll see.
I’ve drawn the conclusion, life’s just an illusion.
Everything winds up as it’s going to be.
I don’t know what else I can say.
I’m to the point where words get in the way.
So I’ll leave it at that, in poker called “staying pat,”
But will write more another day.
Conrad Craber, SurvivorFairview, Oregon
Michelle Boozer with son DeShown
12 S T RO K E CONNECT ION January | February 2008
READE RS ROOM | Connecting You to Others
hirteen years ago, when I was 51 years old, I had a stroke that caused major physical and cognitive deficits. After several days in ICU, my initial prognosis was bleak. The neurologist told me I would be very limited in my daily tasks and hopes of full recovery were minimal. I was dazed and confused and did not fully comprehend that life as I
knew it was over. I was no longer the “old Joe.”Early on my road to recovery I discovered the true meaning of
hard work. In addition to my physical challenges, I experienced depression, anxiety, severe mood swings and an inability to focus. As for my physical deficits, I spent over a year in rehab. The simple tasks of learning to tell time, do mathematical equations, walk up steps, walk without a cane, drive a car, play golf and tie my shoes became important goals for me. It took many months of grueling work and much determination, but I finally reached my goals. I learned about patience.
My stroke affected the whole family — my wife Peggy and our three children, Tricia, Carol and Brian. Peggy was no longer with the “old Joe” but with a man who was mentally unstable for a time. I don’t think I’d have survived without their dedication and love. My priorities have forever changed — love, family, my Christian faith and friends are now at the top of the list.
I continue to struggle with several cognitive and physical
challenges. It is difficult for me to follow conversations, comprehend numbers and dates and to stay focused. I also have left-side paralysis. Facing the “real world” took courage as the “new Joe,” but despite the challenges, I live a happy and fulfilled life. I’ve found that there are two alternatives when dealing with a disability: Either it controls you, or you control it. It’s a lifelong process of achievements and setbacks, and I have learned to take the good with the difficult.
Although surviving a stroke has been life changing, many of those changes have been positive. The “old Joe” would never have taken time to reflect on the positive effects of this event. I volunteer at a nursing home, reaching out to others facing similar circumstances. I also share my experiences with graduating therapists. My spirituality has become stronger and deeper, and I have become a Eucharistic minister for my local parish.
Perhaps the most important lesson I have learned is that life is precious and nothing should ever be taken for granted, especially our health. I believe that God has a plan for each of us, and my stroke was God’s way of telling me to slow down. I have been blessed with an outstanding wife and children and a second chance at life. For that I am truly grateful, and that is why I call myself the “lucky one.”
Joe Ganey, SurvivorOak Hill, Virginia
I’m the Lucky One
I believe that God has a plan for each of us, and my stroke was God’s way of telling me to slow down.
The “new” Joe Ganey knows he’s a lucky man.

A1069 Innovative Neurotronics.indd 1 12/3/07 10:35:01 AM
14 S T RO K E CONNECT ION January | February 2008
et’s establish my gardening credentials (or lack thereof) before you start sending letters and
e-mails to Stroke Connection asking why they allowed me to write an article about gardening. Although my paternal grandfather spent most of his 83 years farming and raising his own food (much of which my grandmother either canned or froze), my gardening experience has been limited to our backyard. But I’ve received a tremendous amount of pleasure and satisfaction from those backyard gardens, especially since my stroke in 1999. After two cerebral hemorrhages, we questioned my ability to return to any of the daily activities that were routine before the strokes. Eighteen months of outpatient therapy and continued exercising at a local fitness center have helped
me regain the strength and stamina needed for gardening. Although I still use my cane to help me walk, most gardening tasks, such
as planting, watering and weeding can be accomplished from my chair.
Two years back my bride Charlotte and I noticed a raised planter constructed from landscape timbers outside the entrance to one of our favorite restaurants. The
owner was using the planter to grow herbs that she used in the delicious
Greek food found inside. We decided that
with a little effort and a trip to our neighborhood building supply store, we could build a similar raised planter for my vegetable garden. After a few hours of playing carpenters, we constructed two 4' x 8' raised planters.
My strokes took away all functional use of my left arm and hand. However, I still have a good, strong right arm and hand, so working together, with my bride assisting as my left side,
we were able to complete our mission. I used 16d galvanized nails in the construction and was very careful to hit only the nails when swinging my hammer. As my left hand, Charlotte courageously accepted the questionable duty of holding the nails while I hammered. I knew one misguided hammer striking her nails or any other part of her hand, and the project was over. After raising our two new planters to roughly 24 inches high, we filled each with store-bought potting soil.
Next, came one of the more enjoyable tasks of gardening: the trip to the garden center to select the plants. A word of caution: Unless you are into canning and freezing, or plan on feeding a multitude, don’t buy too many plants. With proper care and timely watering, each tomato plant can produce dozens of tomatoes. The same is true for squash and cucumber plants. Initially, I thought my green tomatoes would never turn red, but after they started ripening, keeping them picked before they turned bad on the vines was a real challenge. I initially bought and planted 10 tomato plants, two squash, two bell pepper and two cucumber plants. These plants more than filled
Growing Peace of Mind
by David P. Layton, Survivor; Summerfield, North Carolina
15January | February 2008 S T RO K E CONNE CT I ON
the space in my raised planters, so I expanded our garden to two 2' x 10' tilled areas next to my shop. A friend tilled this area for me. (I strongly recommend not using a tiller if you have use of only one side. Falling into a moving tiller would not be pretty and could be a big setback to your recovery.) We had just moved into this house, and I wanted to see how well the natural red clay soil worked with my plants, so I didn’t add anything to it. Much to my surprise and pleasure, the local soil nourished my plants as well as the store-bought stuff. Because of my additional beds, I planted six more tomato plants along with more squash and cucumber plants about two weeks after the initial planting.
The beauty of gardening in a raised planter is that weeding and watering the garden are much easier while sitting in a chair. This was the perfect use for that expensive white plastic shower chair that was so necessary when I first returned home from the hospital. Not only did we enjoy eating the fresh vegetables from our garden this summer, but this survivor derived a tremendous feeling of accomplishment and satisfaction from planting, tending and harvesting our fresh home-grown vegetables.
This is what I learned from this year’s crop:
1. Tie up the tomato plants before the tomatoes get large. You can buy tomato stakes at the garden store.
2. Pick the vegetables daily as soon as they start to mature. The tomatoes will quickly over-ripen in the hot days of August. Some of my cucumbers and squash grew much larger than I would have liked because I left them on the vine too long.
3. Plant your garden in a convenient spot for watering. Water is key for a successful crop.
4. Planting a few marigold plants in my garden helped keep the bugs away.
5. Don’t plant the pepper plants next to the squash. The squash plant’s large leaves shaded the pepper plants to the detriment of their growth. Once the squash season was over, I removed the large squash leaves, and my pepper plants loved the sunshine and produced abundantly.
6. There is a green stain that comes from the tomato leaves, so wash your hand(s) well after picking tomatoes and before drying your hand on Grandma’s white hand towels.
My friends and neighbors also shared our harvest. Along with store-bought lettuce, bread and mayonnaise, my tomatoes and cucumbers have become lunch sandwiches for a number of friends in small offices where I do business. The folks at the fitness center where I exercise were also very pleased to get home-grown tomatoes. Growing and sharing the crop were just a couple of the pleasures that have made my life a little more enjoyable and more like it was before the strokes. I’ll gladly accept every one of those activities I can get!
In addition to growing fresh vegetables, Grandma and I have two beautiful young grandchildren who also enjoyed our garden. Jonathan, who is seven, was a big help assisting Grandpa in tending and picking the fresh vegetables. Five-year-old Christina learned the pleasure of picking fresh tomatoes and proudly giving her harvest to Grandma. Raising a garden is not nearly as much fun as raising those grandchildren, but it definitely adds to our enjoyment of life and peace of mind. The pleasure and peace of mind from gardening far outweigh the effort and expense, so plan your garden for this spring and add a new dimension of delight to your summer.
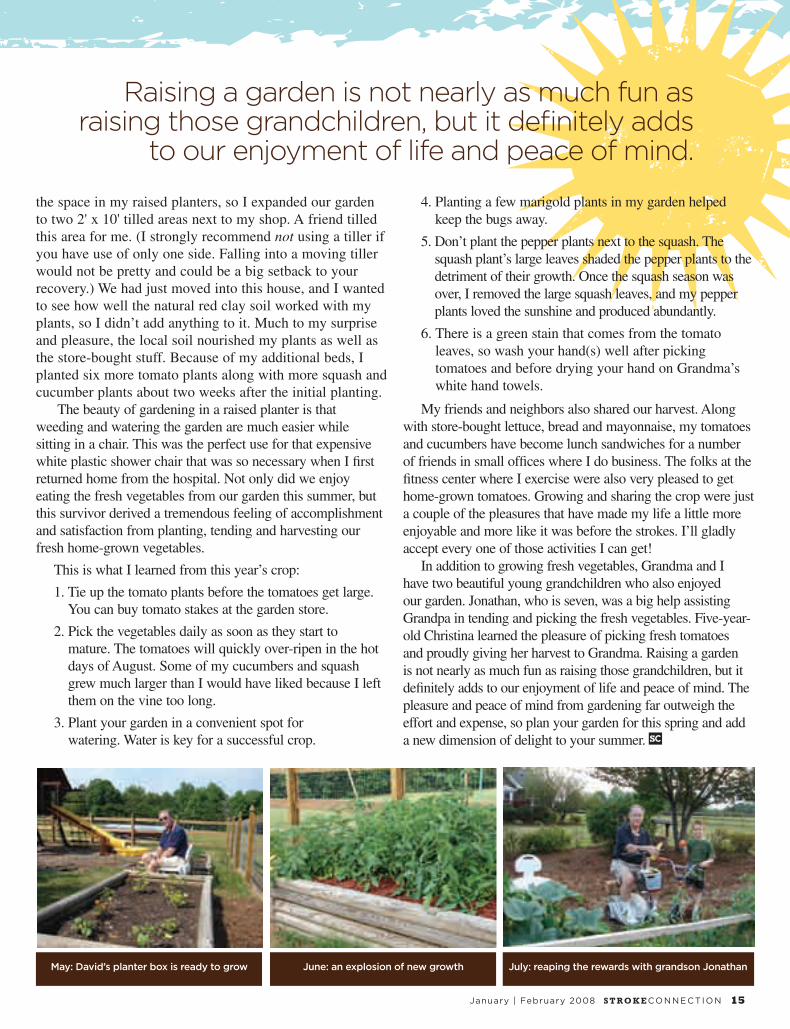
Raising a garden is not nearly as much fun as raising those grandchildren, but it definitely adds
to our enjoyment of life and peace of mind.
May: David’s planter box is ready to grow June: an explosion of new growth July: reaping the rewards with grandson Jonathan
16 S T RO K E CONNECT ION January | February 2008
COVER STORY
arol Monti lost her husband. Bill Winter lost his wife. Sisters Beth Henkel and Michelle Goldstein said good-bye to their mother. Even though their family members survived a stroke, these caregivers lost the loved ones they knew.
“You can lose a bond with a loved one in two ways: by the death of the person or by a severe change in the nature of your bond,” said J. Shep Jeffreys, a clinical psychologist and author of Helping Grieving People: When tears
are not enough. “When that happens, you experience the death of the person you knew. It’s as powerful as if the person had physically died.”
Jeffreys points to a basic formula for grief: “When you have any kind of change, you often have loss, and when you have loss, you have grief. It’s the human grief reaction based on the need to survive. The way things were has been severely altered.”
Jeffreys is an assistant professor in the department of psychiatry at Johns Hopkins University. He’s also an affiliate assistant professor in pastoral counseling at Loyola College and a fellow in thanatology (the study of death). He said that survivors of loved ones often mourn the past and are sad about the future.
‘I lost my helpmate’A wife might miss the husband who helped plant pansies. A son might be wistful
about the investment advice his father will never give. “It could be that the stroke survivor doesn’t call or smile or talk about the old days,” Jeffreys said. “When a father doesn’t recognize his son for the first time, then the father that son knew died.”
Gene Monti had a major stroke in January 2001 at 78. Before the stroke, he taught night school, played golf three to four times a week and fixed things around the house. “He laughed a lot and told jokes,” said Carol, his wife of 50 years. “He would find funny things about the everyday.” (continued)
Survivors, caregivers share what they’ve lost
‘The Way We Were’
by Dina Rogers

17January | February 2008 S T RO K E CONNE CT I ON
Carol misses the man who chopped the onions for dinner
and found funny things in the everyday. Bill remembers
the beautiful girl who sparked his attention at a beach party
more than 50 years ago. Beth and Michelle mourn the loss
of the “carpool mom” who was always there for her family.

18 S T RO K E CONNECT ION January | February 2008
Now, said Carol, his sense of humor is gone.“I’m in trouble,” is the way Gene describes his right-side
weakness. He can walk, although he drags his right leg. “Except for being disabled, I carry on the way I have. I’ve always accepted things the way they were. It’s a struggle, but I make it.”
Carol struggles as well. The couple still goes on vacation — they recently returned from an Alaskan cruise — but traveling is hard. And she mourns the man who has changed since they married.
“Number one, I’ve lost my helpmate,” she said. “He would help me vacuum or cut up the onions and do all the things around the house that now I must do; I mourn that. When you’re used to having a vital, strong man around, and then he becomes so badly disabled, you mourn the loss of having the kind of husband you had before.”
She added: “I try not to feel sorry for myself, but there is a loss of freedom when I need to make sure I’m back at a certain time, or enlist the help of others to go on vacation. Time away by myself is great. It’s very freeing for awhile, but there are always thoughts of how he’s doing at home.”
‘Life is slow-paced’“We met at a beach party,” recalled Bill Winter of his
first encounter with Laura, his future wife. “I was just out of the service and was looking to go out and have a good time. We became friendly and started dating. She was five years younger than I was, the youngest person I’d ever been out with. She’s a very attractive woman. Something just drew me to her. We were married in 1957.”
The couple spent more than three decades raising their four sons and traveling extensively. In 1990, Bill was told to pick out a funeral plot after Laura had a massive hemorrhage at 53. Before the stroke, she played tennis and bridge and was active in her husband’s business. Now she’s paralyzed on her left side and uses a wheelchair.
“I can’t drive. I’d be a menace on the road,” Laura said. “My friends pick me up so I can play bridge every Monday. That’s life. You have two choices: One is to sit in the corner and say ‘poor me’ and the other is to get out in life.”
But getting out isn’t so easy. Laura loves to travel. But while she craves adventures and chances to get away, Bill envisions cobblestone sidewalks and narrow steps.
“She wants to go all the time, but it’s not the same as it used to be. If she wants to go to the ocean, that’s no vacation for me,” Bill said. “She wants to visit England for our 50TH anniversary. But England isn’t wheelchair friendly. You have to remember I’m 75. If I were younger, maybe I’d be more adventurous.”
Life is often difficult. And slow-paced.“As a caregiver, it’s not easy and it can be extremely
frustrating,” Bill said. “But you can’t be negative. You have to look at the situation with a positive point of view and go forward.” (continued)
“When you’re used to having a vital, strong man around, and then he becomes so badly disabled, you mourn the loss of having the kind of husband you had before.”
In 1990, Bill was told to pick out a funeral plot after Laura’s stroke.
Before the stroke, she played tennis and bridge and was active
in her husband’s business. Now she’s paralyzed on her left side
and uses a wheelchair.
‘The Way We Were’
Gene and Carol Monti on an Alaskan cruise
Laura and Bill Winter
19January | February 2008 S T RO K E CONNE CT I ON
Give yourself permission to express your feelings. It could be a heartfelt talk with a trusted friend. Some like to write; others draw. “Some stroke survivors grieve simply by crying or withdrawing,” Jeffreys said. “Caregivers or family members are also dealing with grief issues because their loved one is not the same, and that’s the loss.”
Learn to listen … and listen some more. The grieving person’s agenda should drive the conversation. Talking and processing feelings out loud can help the person understand that the stroke really happened. “It’s not our job to tell them how to grieve, but to give them the space and permission to do so,” Jeffreys said. “It’s important that stroke survivors and their loved ones are listened to in a nonjudgmental way.”
Forge a spiritual connection. “I always ask caregivers: To what extent does your belief system play a role? For many, their faith can be an incredible resource and prayers can lessen the intensity of their grief,” Jeffreys said. “More and more churches recognize this need and have a bereavement or illness mission.”
Understand that there’s no right way to grieve. “Some grieve and cry on the inside; some cry on the outside,” Jeffreys said. “Tears are the universal way we expect to see people grieving, but not everyone cries. Family members need to respect that. Some might say ‘my brother isn’t sad. He hasn’t cried since my mom had her stroke.’ But many people grieve in private.”
Deal with your emotions, which might include pain, guilt or shame. There’s also fear: ‘If my dad had a stroke, could I have one too?’ And anger: ‘My grandfather was a nutritionist who never smoked or drank. Why us?’
Guilt can leave lasting scars and some caregivers dwell on what happened before the stroke. They berate themselves for not
convincing a loved one to stop smoking or for refusing to give an inch in a recent fight. “We will mine the depths of our soul to find reasons to implicate ourselves, and then we feel ashamed because we can’t bring someone to the house because we’re ashamed of how our dad acts after his stroke.” Allow yourself to experience these feelings but cut yourself some slack: There’s no benefit to beating yourself up.
Do something active. Visit the gym. Go for a jog. Swim a few laps. Just taking a walk can give the caregiver and the stroke survivor a different perspective. “Getting outside keeps them from having a limited sense of the world,” Jeffreys said. Rake leaves. Chop wood. Pick a few flowers. Can’t get outside? Stay inside and watch a funny DVD.
Let go with a ritual. Proactively cope with your losses — but only when you’re ready. “Rituals are useful because they give you something to do,” Jeffreys said. “It could be a ceremony or a repeated act that acknowledges the reality of what happened, and the hope for what could be.” Some suggestions: meditation, lighting a candle or planting a tree. Take a ritual bath, get a massage or play some music. Like hymns or Big Band tunes? Open your ears to whatever fills your heart.
Evaluate your roles and look to the future. For caregivers or loved ones of stroke survivors: Once you have a handle on day-to-day issues, think about what’s yet to come. How do I redefine who I am, who my loved one is and how we relate to each other? For stroke survivors: What can I do myself in this post-stroke world?
Both need to learn how to help each other — and themselves. “Sometimes people are frozen into dysfunction, but we need to make plans for the future,” Jeffreys said. “Above all, take some action. Don’t do nothing.”
Shep Jeffreys, clinical psychologist and author of
Helping Grieving People
Practical advice for coping Stroke survivors and their loved ones can benefit from Jeffreys’ advice for coping with grief. First, don’t fight it. “Is there a cure for sneezing? Grieving is as normal as that,” Jeffreys said. “It’s not an illness, and you can’t cure it.”

20 S T RO K E CONNECT ION January | February 2008
‘I miss my real mom’When Beth Henkel tried to give her mother, Peggy
Kranitz, medication and water for a brutal headache, the glass slipped out of her mom’s hand. Life hasn’t been the same since. Peggy’s mom had had a stroke.
“She suffered brain damage and complete short-term memory loss,” Beth said, of the 2001 event. “We live with the fact that she will never be the same, but it has been a very hard adjustment for all of us,” Beth said. “She can remember everything that happened 20 years ago, but ask her what she had for lunch and she’s perplexed.”
Beth, her husband David, and their son live with Peggy and their father, Jay. Sister Michelle and brother Howie live nearby.
“My mom was an athlete,” Beth remembered. “Growing up, she was the only girl on all-boys’ teams. She played everything from baseball to field hockey. When we were kids, she was always running bases and throwing the ball.”
A stay-at-home mom when her children were young, Peggy put her RN degree to use when her family needed the income. “My mom picked herself up by her bootstraps and went to work,” Beth said. “She loved being a nurse.”
Beth said her mom was active. Involved.
“It’s hard to put it into words. She ran the household and did ‘mom’ things. Now I can’t say ‘do me a favor and heat up a waffle.’”
Beth mourns the loss of a grandmother the young children in her family will never know. “That’s where I really miss my real mom, not the one I’m left with. Before her stroke, I couldn’t wait for the time when my mom would babysit my children or I could go to her for advice. But we can’t have Grandma watch the kids because she’s forgetful. She gets angry that none of us trust her, but she can’t do two things at once.”
Beth said her mom is angry and bitter about the stroke. “It has to be tough to be treated like a child. She has a limited ability to watch her tongue. Whatever comes to her
brain shoots right out of her mouth. If she’s thinking ‘Beth isn’t a good mom today,’ she’ll just say it. It’s hard not to get upset with that.’”
Beth’s sister, Michelle Goldstein, also feels anger at the loss of a mother she remembers for her “crazy spunkiness.”
“Every October 19th is a very sad day for me,” said Michelle, a third-grade teacher. “It’s the day I lost my mom. I’m so glad for what I have and that she’s alive, but it’s a huge, huge loss that can never be made up.”
Although joking and a sense of humor help keep her family together, Michelle said, the anger that her mom isn’t the same still surfaces.
“I hate it and I resent it and I’m angry,” said Michelle, who explored her feelings in therapy for awhile without great results. “I didn’t want to hear how lucky I was; I wanted my old mom back.”
‘The Way We Were’
Jeffreys said it’s common for caregivers and family members to feel anger or rage, even
toward the person who had the stroke. “They grieve over what’s never going to happen ...
It’s the loss of what might have been.”
Peggy Kranitz (top, left) and sisters Beth Henkel and Michelle Goldstein at
Beth’s 2006 wedding

21January | February 2008 S T RO K E CONNE CT I ON
‘Like pebbles dropping in a pond’Jeffreys said it’s common — and OK — for caregivers
and family members to feel anger or rage, even toward the person who had the stroke. “They grieve over what’s never going to happen. It’s such a painful loss. It’s the loss of what might have been.”
And for the stroke survivor, “it can become a horror to have someone see you or put food in your mouth like an infant when you’ve been a CEO or a working woman or the head of committees or raised five children.”
Some couples might have enjoyed long walks, going out to dinner or visiting relatives. These activities might no longer be possible. Loss of sexual activity is another issue that some couples face. “These losses are like pebbles dropping in a pond. The ripples go out and out and out. They affect the person with a stroke as well as the caregiver.”
While some caregivers and family members recognize that they’re grieving, others may dismiss or minimize the idea.
“Older generations often disenfranchise themselves from grief,” Jeffreys said. “The activity of caregiving can often displace or overtake the grief reaction, and they don’t see themselves as grieving people.”
One of Jeffreys’ patients did a tremendous amount of work for her husband after he had a stroke. “She provided all kinds of care, from feeding to toileting. It wasn’t until after he died that she allowed herself to feel the rage that she’d been pushing away all that time.”
In the mix of grief, people often hear that denial is bad. But a healthy dose can be helpful, Jeffreys said. “I love denial. I think it’s good. Denial allows us to take in reality in bits and pieces. We need it. It’s like a shock absorber.”
Stroke survivors also grieve lost relationships. Laura Winter looks forward to her weekly bridge games. And Gene Monti rarely misses a weekly breakfast that lets him enjoy a bagel and lox with his ROMEO (Retired Old Men Eating Out) group. But other stroke survivors have limited friendships. “We define ourselves by our social interactions,” Jeffreys said. “When you are suddenly cut off from the richness of social interaction, this is a loss.”
Michelle Goldstein tries to put her family’s losses in perspective. “Sometimes I’ll dream about the old days, and
these are great dreams. But you can’t change reality, so you have to start accepting it. All right, my mom’s different. In the beginning she didn’t know who we were. Now she’s making great strides. And whether I like it or not, I have to learn to love her for who she is now.”
Speech and Language Recovery
Unlimited, independent therapy using programs created by speech therapists. Used in homes and clinics since 1995. Money-back guarantee. Easy to use. No training needed.
Affordable therapy for• Aphasia• Apraxia• Speech• Word retrieval• Reading• Memory
“Bungalow Software is great. My husband spends several hours a day working on it. His progress was quite evident in the therapist’s follow-up evaluation.” Helen Talley Caregiver
Get your free information kit
1-800-891-9937www.StrokeSoftware.com
It’s never too late—or too early. Start Today!

22 S T RO K E CONNECT ION January | February 2008
n February 2002 I had an embolic stroke that resulted in severe aphasia. For the next 15 months I received speech therapy. It took me about three years to chronicle and sequence details of those 15 months. It was not only therapeutic, it was obligatory for me to go on with my life.
I was a frail, anguished stroke victim fighting hard to keep my dignity. There were some people who didn’t see me even when they saw me. I was invisible, unnoticed and nonexistent. Yet, each day, in minuscule ways, I tried to make my presence known to others and myself.
Tastes of dignity and humiliationDuring my first week or two at home, my wife Dale made sure that everything I
needed was in the house, especially lunch. I liked deli-sliced Boar’s Head™ low-salt turkey, Chicken of the Sea™ solid white albacore tuna in water, oranges and 12-grain bread. After the first couple of weeks, I needed to go to the supermarket to buy these items. I didn’t feel that Dale was responsible for getting my lunch food; I could do that for myself. So I walked to the supermarket. It was good to feel the cold on my face. As I strolled, I tried to think of the word “turkey.” It came to me once, but in a second I forgot it.
Entering the supermarket, I froze. Would there be a line at the deli counter? Would I be able to say any words at all? And most importantly, could I ask for turkey? The deli counter woman was servicing another customer, which allowed me to look around the deli area. There was an advertisement for Boar’s Head turkey, but I couldn’t say it at that second. Then a couple of seconds later, I was able to say turkey and I kept saying it over and over.
But when the deli counter woman asked me what I wanted, I couldn’t remember “turkey.” There were a few excruciating seconds before I pointed to the advertisement. The woman asked me if I wanted Boar’s Head or some other brand. I said, “Yes.” “Boar’s Head?” “Yes.” She then called out a litany of Boar’s Head turkey products. I said, “Yes.” “How much? A half pound, a pound?” “Yes.” “A pound?” “Yes.” She cut the turkey, weighed, packaged and priced it, gave it to me and wished me a good day.
As I walked out of the supermarket, I heaved a sigh. That sigh was more important than any sigh I felt after a teacher evaluation, administrative evaluation or college evaluation. That sigh indicated that I could feed myself. The deli counter woman was wonderful. She was considerate and helpful. She made me feel comfortable and treated me with dignity when my self respect was frail.
Reclaiming My Dignityby Donald F. Weinstein West Hempstead, New York
Life is full of bizarre
contradictions, fascinations and
repugnance. It has dynamism,
nuances and dualities whether
or not you’ve had a stroke.
There are Good Samaritans and
uncouth oafs.
23January | February 2008 S T RO K E CONNE CT I ON
Every couple of days I walked to the supermarket to buy a pound of low-sodium Boar’s Head turkey for lunch. Periodically, the deli counter woman was replaced by the deli counter man. Where deli counter woman was sensitive and accommodating, deli counter man was abrupt and discourteous. His tone and inflection made me feel that I was an affront to him, that I was grotesque.
The dialogue with deli counter man went something like this:
“Who’s next?” (I was the first person on line.)“Yea? (No smile.) What do you want? Come on, what
do you want?” (I wasn’t sure that I could say “me” or “yes,” much less what I wanted.)
“Turkey.” (This took all my energy.) “What kind of turkey do you want? Come on, I don’t know
what you want. Tell me what you want?” (I didn’t hear all his words because I had to focus on one question at a time.)
I pointed to the flyer next to counter. (Thank God for advertising!)
“Boar’s Head, right?”“Yes.” (I wasn’t sure that he said Boar’s Head.) “What kind of Boar’s Head? What do you want? Come on,
I’m waiting.” (I felt livid because he rushed me for no reason; he was just malicious. I wished my professorial self could cut him with my sharp tongue.)
I looked pensively at the ad for a couple of seconds. I couldn’t read it, but it calmed me to look at it.
“You want (whatever he said).” “Yea.” (You contemptible, nauseating bastard, I thought.) “OK, what do you want?” I look pensive again. “Did you say a pound?” “Yea.”This exchange took a minute or so, but it was excruciatingly
painful and humiliating. As more people lined up for service, he became surlier, and it seemed to me as if he were trying to play to the other customers at my expense. He rolled his eyes and looked at the other people in line.
My wife and the waitress
A couple of weeks after my hospitalization, Dale and I went out for breakfast to a neighborhood diner where we had eaten regularly for 10 years. Our regular waitress, who was about 50 and chatty, came over to find out why we hadn’t been in. Dale told her. She gasped and then asked for our orders. Dale ordered for both of us. I hadn’t asked her to do that. I know she thought ordering for me would save me from any embarrassment. She was probably right, but I had wanted to try.
A few weeks later we returned to the restaurant for breakfast. I looked around and saw a table with four couples. One of the men wasn’t talking and his wife was ordering his breakfast. He was not part of the conversations, and I thought he had probably had a stroke.
Right then the waitress came over. Dale gave her order, and then the waitress looked at me. In speech therapy, I had learned to read and sound out the word “egg.” Sometimes I got it right. Driving to the restaurant from our house, I had focused on the word “egg” so I could order by myself. I started to give my order, but stuttered “egg.” Immediately the waitress looked at Dale for my order. Although the waitress had known me for years, she didn’t allow me the few seconds I needed to say “egg.” Would it have been so terrible for Dale to have explained that I just needed a few seconds to pull the words together? Perhaps I couldn’t have said it, it was early in my recovery, but would it have caused a big problem for me to try? Notwithstanding the fact Dale loved me, she could not understand how painful it was for me to be dismissed by the waitress just because I couldn’t say “egg.” But Dale didn’t want to shake people up, so instead she ordered both breakfasts. Then we held hands and “talked” about our granddaughters.
Life is full of bizarre contradictions, fascinations and repugnance. It has dynamism, nuances and dualities whether or not you’ve had a stroke. There are Good Samaritans and uncouth oafs. As a result of my stroke, Dale and I have had several Catch-22 nightmares. That is real life. Each day, in some way, I have had to cross a moat in my brain to get my dignity back.
Above: Don and Dale at the beach with son Jeff, his wife Anne and their
daughters Jessica and AlisonBelow: Don and Dale with the next
generation of Weinsteins
Don often walks to the supermarket Don and Dale Weinstein

24 S T RO K E CONNECT ION January | February 2008
arch 12, 2002, dawned beautifully in northern Michigan. The air was crisp and the sun bright as my husband Bob and I hurried to finish breakfast. We put on our ski clothes and made the hour drive to Nub’s Nob, our favorite ski area. In less than two weeks, we would be meeting friends and family there to celebrate our 50th wedding anniversary.
At 75 I felt like a wonder woman who ran, biked, skied and swam. Bob joined me in these activities, and we also volunteered for causes in our Elk Rapids community. We loved retirement. Our daughter Amy and her husband John lived nearby with our grandchildren Emma and Charlie. Life was good! I was a bit overweight and had had high blood pressure for years, but I really felt I could do anything.
When we arrived at the ski area, the lovely, cold day promised hours of good skiing. Happiness and excitement filled me as I got on the chairlift. A longtime skier, I took the steep and intermediate slopes with confidence, but after several runs, I felt something was not quite right, like I couldn’t keep my balance. Bob and I skied down to the lodge to have a picnic lunch on the deck with some friends. During lunch, my left hand was “asleep” and would not wake up although I kept rubbing it hard. I tried to convince myself that I had a pinched nerve.
To prove to myself that I was OK, I decided to go back up and try a few more runs. When I got off the chairlift at the top, I almost fell. As I started down one of my favorite runs, I was losing my balance and felt completely out of control. I worried that I wouldn’t get to the bottom and out of my skis without falling. I don’t remember how, but I made it to the lodge in one piece. After removing my skis, I tried to lean them against the ski rack but kept dropping them. As I walked to the deck to wait for Bob, my left foot dragged in the snow.
I knew the symptoms of stroke, but denial and fear clouded my thinking. As we drove home I frantically tried to find other reasons for my symptoms, but other alarming ones appeared. I could not hold up my left arm. I would raise it using my right arm, but it would just fall into my lap. I tried this several times, hoping to prove to myself that there was nothing wrong. I finally asked Bob to take me to the emergency room 35 miles from home. It had been 10 hours since the symptoms had started, and things were becoming fuzzy and difficult to remember. A scan showed that I was having a stroke.
Going Downhill and Loving ItGoing Downhill and Loving ItGoing Downhill and Loving It
by Toni Johnson, Survivor Elk Rapids, Michigan

25January | February 2008 S T RO K E CONNE CT I ON
The next day, I couldn’t walk. But I could answer the therapist’s questions about the president and the year and month, and thankfully I had no problem speaking. Several days later I was transferred to the rehab section where I spent several weeks working with physical and occupational therapists for hours a day. One night while lying in bed, I was thrilled to wiggle the toes on my left foot.
Bob came and stayed every day. Amy and John also came almost every day and sometimes brought the kids. On our anniversary, a friend of Amy’s brought prime rib dinners for Bob and me. I graduated from a wheelchair to a walker and was allowed to return home with the stipulation that I would return three days a week for more therapy. My morale got a huge boost when I was given the OK to drive my “beetle” convertible again. I’ve been driving those bugs for over 40 years.
During warm months, Bob and I used to ride our mountain bikes almost daily; however, the stroke affected my balance, so I could no longer do this. I joined the Northern Michigan Adaptive Sports and Recreation (NMASAR) group and took a bicycling clinic. There I tried many types of adaptive bikes, including a 21-speed, recumbent three wheeler. I really liked it so we bought one.
I really wanted to ski again, and it turned out that NMASAR offered skiing lessons at nearby Crystal Mountain for people with all sorts of disabilities. My first time back, I trembled with fear and excitement as I was helped onto the chairlift. At the top, several
volunteers were assigned to ski with me. They fitted me with a harness with reins attached. One volunteer skied behind me and held the reins, which kept me from going too fast and kept me in control. Soon I was skiing again!
After several more lessons, Bob and I returned to Nub’s Nob. Could I do it on my own? We walked part way up the beginner slope and I slid down this easy grade to the bottom. A few weeks later I decided to try the chairlift on my own. The operators slowed it down so we could get on and then again at the top for us to get off. After three years, they still do this for me. Later that first year back, I did fall in soft, heavy snow and broke my leg! When the cast came off, my doctor sent me for aqua therapy, and I found that exercising in a large heated pool was fabulous. I’ve always been a swimmer, but after the stroke I sank so I wear a swim belt. I especially like swimming in the deep end where I vigorously jog or tread
water, getting much-needed aerobic exercise. I enjoy it so much that three years later I still do it.
I continue to ski every winter. It’s different now, but I still love it. As I ski down the slopes, there are often tears in my eyes. Are they from the wind? I don’t think so; I think they’re tears of gratitude.
Photos (clockwise from far left):
Toni (in white helmet) with NMASAR
volunteers; Bob and Toni with
daughter Amy, circa 1969; Toni and
Bob with Amy and husband John and
grandchildren Charlie and Emma; Toni
and Bob with Amy and the kids
Participating in Adaptive SportsThe past 20 years has seen tremendous growth in adaptive sports. Whether it’s golf, rock climbing, water skiing or horseback riding, there are organizations dedicated to bringing sports participation to people with disabilities. There’s even wheelchair hockey! Disabled Sports USA offers sports rehabilitation programs in most states to anyone with a permanent disability. For more information, visit www.dsusa.org.
I continue to ski every winter. It’s different
now, but I still love it. As I ski down the
slopes, there are often tears in my eyes.
26 S T RO K E CONNECT ION January | February 2008
he snoring we’re talking about is classified as “sleep apnea.” Sleep apnea is a potentially life-threatening sleep disorder in which tissues in the throat collapse and block the airway. Sensing the lack of oxygen, the brain forces the sleeper awake just enough to cough or gulp air,
which opens the trachea again. Typically, the sleeper is unaware that this is happening. Mild sleep apnea is defined as five to 15 such interruptions per hour; moderate is 16 to 30; and severe, more than 30.
Research by Dr. Henry Klar Yaggi at the Veterans Administration Connecticut Sleep Laboratory in West Haven, Conn., points to a direct link between sleep apnea and stroke risk. “When we started investigating the relationship, we knew that there was a 50 to 80 percent prevalence of sleep apnea in stroke survivors. That’s
compared to a prevalence of about 20 percent in the general population,” said Dr. Yaggi, the laboratory’s director. “It was a classic chicken and egg situation: Does sleep apnea cause stroke or is it a result of stroke?
“What we found is that those who have obstructive sleep apnea have a two-fold increased risk of stroke, transient ischemic attack (TIA) or death from all causes,” said Dr. Yaggi, who is also an assistant professor of medicine at Yale University School of Medicine.
Three types
There are three types of sleep apnea — obstructive sleep apnea (OSA), central sleep apnea (CSA) and a combination of the two. OSA accounts for more than 90 percent of all cases and is the result of tissue in the neck and upper body blocking the airway. It is closely associated with obesity and more common in men than women. “This is because men tend to put on weight in the upper body and neck and that predisposes the airway to collapse,” said Dr. Yaggi. “Women
Get a Good Night’s Sleep AND Reduce Your Risk
by Jon Caswell
Until recently, the only known consequence of snoring was frayed nerves — for the spouse who couldn’t sleep. But new evidence shows that snoring can lead to something far more serious — cardiovascular complications,
including stroke — and it’s the snorer, not the spouse, who’s affected.

tend to put on weight in the lower body. Population studies indicate that men have a two-to-three-fold increase in risk compared to women.” Increasing age is also a risk factor, as is a recessed chin, which causes crowding of the structures in the upper airway.
In CSA the brain doesn’t send regular signals to the diaphragm to contract and expand. CSA is much less common, but has been associated with brain stem stroke because the brain stem is where the impulse to breathe comes from. In CSA there is limited snoring.
Little sleep, big consequences
In OSA the upper airway closes off because the muscles that hold it open lose tone — the more weight, the more loss of tone and the more severe the sleep apnea. Each time the airway closes, there is a pause in breathing. “Pauses in breathing are associated with lower blood oxygen levels,” said Dr. Yaggi. “In addition, there is a rise in blood pressure and an increase in heart rate. All of those factors combine to increase stroke risk.”
Because OSA is associated with obesity, people with OSA are also at risk of other cardiovascular problems, including hypertension, atrial fibrillation, metabolic syndrome and diabetes. “In the sleep field, there is a lot of interest in looking at sleep loss and metabolic syndrome, which is also called Syndrome X,” said Dr. Yaggi. “In fact, sleep apnea is sometimes referred to as Syndrome Z because it seems to go along with Syndrome X.” (Metabolic syndrome is a group of metabolic risk factors that include abdominal obesity, low levels of HDL cholesterol, blood pressure of 130/85 mm Hg or higher and fasting glucose of 110 mg/dL or higher.)
Although the people with OSA are generally unaware that they are waking up every few minutes, they do not get adequate sleep and experience daytime drowsiness and cognitive impairment because of difficulty concentrating. Inadequate sleep also increases the risk of vehicular accidents.
“Bed partners are often the first to notice the interrupted breathing because of the loud — what we call ‘industrial strength’ — snoring,” said Dr. Yaggi. “If a spouse sees that, they should report it to the doctor. For diagnosis and treatment, the person needs to go for an overnight sleep study, where the severity of the problem can be determined. We often do a split-night study. The first half of the night we diagnose the severity, and in the second half we use a continuous positive airway pressure (CPAP) mask to eliminate the interruptions.” (continued)
The Anatomy of Apnea
Normal Breathing: air flows freely through airway
Snoring: air squeezes through partially occluded airway
Apnea: airway is blocked, shutting off airflow
Copyright Krames
Copyright Krames
Copyright Krames
27January | February 2008 S T RO K E CONNE CT I ON
28 S T RO K E CONNECT ION January | February 2008
Treatment
The CPAP mask, which is generally covered by insurance, is used for patients with moderate to severe OSA. (CPAP is sometimes used to treat CSA, but it is not as effective as it is for OSA.) An air compressor in the device creates enough pressure to produce a steady flow of air that keeps the airway open. Mild OSA may be treated with uvulo-palato-pharyngoplasty (UPPP) surgery, in which some of the soft tissue in the upper airway is removed, improving the air flow. “UPPP surgery is effective about half the time in patients with mild OSA and who aren’t overweight,” said Dr. Yaggi. “There is a third type of treatment that involves the use of an oral appliance called a mandibular advancement device that is a mouthpiece that moves the tongue and lower jaw forward and opens the airway. In addition, a 10 to 20 percent reduction in weight can halve the severity of OSA.”
In the past it was easy to disregard snoring as an irritating trait that a spouse simply had to live with. Now it is clear that for stroke survivors it may well be a symptom of a life-threatening condition. So the next time your spouse mentions that you’ve been snoring, do both of you a favor: Visit your doctor.
Stealing from the PoorRemember Robin Hood and his Merry Men? They had a noble purpose, “Steal from the rich and give to the poor.” It seems that when the brains of people are injured, including stroke, they do not react so nobly. A neurological reaction occurs that works in direct opposition to the Robin Hood principle, causing healthy body tissue to “steal” from damaged tissue. Scientists call it “reverse Robin Hood syndrome.”
“This term refers to the stealing of blood by unaffected brain tissues from brain tissues affected with stroke,” said Dr. Andrei Alexandrov, professor of neurology at the University of Alabama Birmingham (UAB) and director of the UAB Comprehensive Stroke Research Center.
Although this shifting of blood flow may result in worsening of arm and leg weakness or speech problems, most of the time the shift can only be detected by ultrasound or other brain imaging. “The reason the rich steal from the poor,” said Dr. Alexandrov, “is that the normal blood vessels react to stimuli much more effectively and faster than vessels affected by stroke. Relaxation of normal vessels creates an incentive for blood flow to follow the path of least resistance and avoid less relaxed vessels in the affected brain.”
Sleep apnea can worsen this syndrome because of its effect on blood chemistry. “Sleep apnea and changes in blood supply go hand in hand as interruption of breathing builds up carbon dioxide in the blood- stream,” said Dr. Alexandrov. “Increases in carbon dioxide cause vessels to relax and steal blood from vessels affected by stroke that cannot relax any further.
“We think that this syndrome may explain why correcting sleep apnea with positive airway pressure masks can help reduce the risk of stroke recurrence. We are conducting a prospective study to show this. In a few patients that had the syndrome and received correction, the worsening of the symptoms stopped. It is encouraging, but we have too few subjects in the study so far to draw a definitive conclusion.”
THE WARNING SIGNS OF STROKE:
THE WARNING SIGNS OF HEART ATTACK:
• Sudden numbness or weakness of the face, arm or leg, especially on one side of the body
• Sudden confusion, trouble speaking or understanding
• Sudden trouble seeing in one or both eyes
• Sudden trouble walking, dizziness, loss of balance or coordination
• Sudden, severe headache with no known cause
• Chest discomfort. Most heart attacks involve discomfort in the center of the chest that lasts more than a few minutes, or that goes away and comes back. It can feel like uncomfortable pressure, squeezing, fullness or pain.
• Discomfort in other areas of the upper body. Symptoms can include pain or discomfort in one or both arms, the back, neck, jaw or stomach.
• Shortness of breath. May occur with or without chest discomfort.
• Other signs: These may include breaking out in a cold sweat, nausea or lightheadedness.
Know Know
If you experience some or all of these heart attack or stroke warning
signs, don’t wait. Call 9-1-1 right away.

29January | February 2008 S T RO K E CONNE CT I ON
Learn More About John...
Read John’s personal stroke story, “Life is at the Curb,” from the September/October 2003 issue of Stroke Connection at StrokeAssociation.org/strokeconnection, or book his one-man show about stroke recovery, “Brain Freeze,” by contacting him at [email protected].
was staring out the window of our Manhattan apartment summoning the muses to inspire me with a topic for the next “Life At The Curb” article, when a magnificent fiery ball the size of Jupiter descended behind Gotham’s skyline. As it disappeared into the Hudson I whispered, “How sweet it is!” I’m sure Byron, Shelley and Keats would have banged out an epic poem or two, but for me that old Jackie Gleason quote captured the moment perfectly. I was glad to be alive taking it all in. The stroke was a close call, but like Tony Soprano after giving the Feds the slip, I survived.
Right in the middle of this euphoria I felt like I was giving birth to a pitchfork. I hobbled to the phone and called my internist. His diagnosis? Kidney stones. Stones? Try boulders. What I was feeling was no pebble. I thought, “This is not happening.” Stroke should be an “Illness — Get Out of Jail” card and I already did my time. Still, this stone wasn’t buying any of it. I needed immediate relief.
I staggered into the elevator thinking St. Vincent’s Hospital, where I had been an inpatient, is only two blocks away. I’ll walk. But by the time I hit the ground floor I was hunched over like Marty Feldman in “Young Frankenstein.” People in the lobby scattered like the villagers. I hobbled to the curb and hailed a cab. Well, I wouldn’t exactly call it “hail. ” It was more like “fall in front of.” I assumed the fetal position on the backseat,
and thought how urban ERs are like MASH units. But hey, I’m an alumnus. I graduated Rehab with honors. It’ll be like the Class of ’97 Reunion. They’ll welcome me with open arms — take me right away. Wrong! I waited and waited while the pain got worse and worse. You know you’re in bad shape when the guy with the knife wound points to you and yells to the nurse, “This guy needs help!” Meanwhile the character next to me said he had some stuff that could help me, but I didn’t think “Jimmy The Weasel” was an approved healthcare provider. The ER waiting room was a show and tell of various afflictions and diseases. Fortunately, in the middle of Carmine’s detailed colon bowel monologue they announced, “Don Kelly’s next.” “That’s Kawie,” I screamed. “John K-A-W-I-E.”
I figured once I was on a gurney relief wouldn’t be far behind. Of course it was, because first there’s the all-important intensive interrogation … social security number, mom’s maiden name, shoe size, favorite color, … you know, all those vital statistics. Why do they ask your date of birth, and then ask how old you are? Come on, my head’s spinning like Linda Blair in “The Exorcist.” Can’t they at least do the math?
Eventually I was rolled behind curtain #1. Was this the ER or “Lets Make A Deal”? Dr. Monty Hall flips back the curtain, holds up what looks like a garden hose, and starts talking about a catheter. “Don’t worry Don,” he said.
“It’s Joh…” I must have passed out because that’s when the muses spoke: “This is the new article.” How sweet it is.
LIFE at the CURB
Everybody Must Get Stones
A Unique Perspective on Survival by Stroke Survivor and Comedian John Kawie
You know you’re in bad shape when the guy with the knife wound points to you and
yells to the nurse, “This guy needs help!”

30 S T RO K E CONNECT ION January | February 2008
EVERYDAY SURVIVAL | Connecting You to Helpful Ideas
n the May/June issue I read a letter from Peter Hartley outlining problems using his typewriter because of limitations using his right arm and fingers. I have similar limitations typing only on my left side, and I thought my experience overcoming that challenge might be useful to him and others.
I am a retired sociology professor, and in February 2001, at age 73, I was visiting Melbourne, Australia, when I experienced a stroke. After two weeks in
the hospital, my left leg, arm and hand remained paralyzed, but fortunately I regained normal speech. Still in Australia, I was enrolled in a rehabilitation program designed mainly to enable me to walk again with the help of a cane. After two months, I was able to fly home to Rhode Island accompanied by my wife Alice.
After two weeks at home, I enrolled in a local rehabilitation program to further improve my walking ability and, possibly, regain some mobility in my left arm and hand. I divided my time among physical, occupational and speech therapists.
This intensive program was exactly what I needed, and I strongly committed myself to it to gain maximum improvement. Among the activities that the speech therapist sponsored was preparation and publication of a newsletter for the program’s clients, staff and supporters.
As I had devoted a considerable part of my academic career to research and publication, this attracted me, and I was happy to participate. I was asked to prepare an essay on my experience as a stroke patient in Australia.
Because of the restricted use of my left hand, I began preparing the essay by writing it out with my right hand. Noting this, my therapist suggested it might be easier to type on the computer, which I proceeded to do. I was never an expert typist, and typing with one hand proved to be especially frustrating and slow. When I told this to my speech therapist, she suggested I try using voice recognition software, which would allow me to dictate to the computer using a special program. I took a preliminary test, and the results showed that I was a promising candidate for this program.
The following week, my therapist sat down with me at a computer kept in a “soundproof” room and proceeded to initiate me to Dragon Naturally Speaking™, a speech recognition program that “listens” to speech and converts it to writing on a computer. To program the computer to the sound of my voice, I read “Dave Barry in Cyberspace.” The hardest part was not laughing because I found the story so humorous, but with concerted effort, I managed to record the essay. Then I began to dictate the essay on my experience in Australia. It was amazing to see my spoken words — including the appropriate punctuation and spelling — appear on the screen. I realized that this program could help me overcome the handicap imposed by my stroke.
TurningSpeechinto Printby Sidney Goldstein, Ph.D. Warwick, Rhode Island

31January | February 2008 S T RO K E CONNE CT I ON
It was a true miracle, and I could not wait to get home to share the experience with my wife.
For the next few days, I used every visit to the rehabilitation center to dictate the rest of my essay. My therapist followed my progress with great interest and took the time to provide me with helpful guidelines for more effective use of the Dragon software. Soon I delivered the finished nine-page essay for the newsletter. What a thrill that was and, even more, to see it published in the next issue.
Soon after, my therapist arranged for me to be tested for the accuracy of my dictation. The test showed that the computer recognized 90 percent or more of the material I was dictating. The errors in word recognition were sometimes quite humorous (e.g., “freezer” for “visa”) and could easily be corrected by editing and avoided in later dictation.
Completing the first essay and scoring so high on the test motivated me to initiate a project that I had long dreamed of pursuing. As a sociology professor I had specialized in population studies at Brown University. During 40 years, my research had given
me, and often my wife and three children, the opportunity to travel in Europe, Asia and Africa. On virtually every one of those trips, we had traveled within the country we were visiting to learn more about its society and culture. On many of those trips we encountered unusual experiences — some quite dangerous.
On my return home from each trip, I told my friends and relatives about those experiences, but I had always wanted to write them down so I could share them with my children and grandchildren in years to come. Unfortunately, because of the numerous writing commitments associated with my university research, I never had enough time to
record these adventures. Having successfully completed my first essay by dictating it to the computer, I realized that I could use the speech recognition program to record the essays in a very efficient manner.
And so I decided to write about a trip to Nigeria. I wanted to test both how well I could use my memory and what reaction I would get from those who read it. With my therapist’s permission, I went to work on the Nigeria essay. Because of my enthusiasm, I completed it in only a few sessions at the computer. It appeared in the next issue of the newsletter. Encouraged, I proceeded to use the time allocated for my speech therapy to prepare additional essays, each of which was published in the newsletter.
By December 2001, less than a year after my stroke, my therapy program had gone so well that I was able to leave the rehab program and began exercising on my own at the local gym. Although I was pleased with my progress, I was also worried about continuing my travel-writing project. Through my therapist, I learned that I could easily and inexpensively install a speech recognition program on my home computer; my wife arranged to have this done. I enjoyed dictating “Dave Barry in Cyberspace” to the newly installed program at home, and soon I was dictating the next essay in my series.
This meant a great deal to me: not only could I continue the series, but I also had a new, constructive way in which to use the free time I now had at home because I was retired and also unable to engage much in the outdoor activities that I had previously enjoyed. I recently completed the 20 th essay in my travel series. I have also used the program to dictate letters and prepare talks and research reports.
Having personally had such a wonderful experience with Dragon Naturally Speaking™, I have been surprised to read about the frustrations that other survivors have encountered because of their inability to type. I strongly recommend that anyone confronted with a partial or total paralysis of the arm or hand seriously consider using a voice recognition program. I am grateful that modern technology has made this possible. It’s made a world of difference in my efforts to resume my normal writing activities and restore my self-esteem.
“It was amazing to see my spoken words — including the appropriate punctuation and spelling — appear on the screen. I realized
that this program could help me overcome the handicap imposed by my stroke.”
Sidney and Alice Goldstein >
Sidney celebrates another birthday
32 S T RO K E CONNECT ION January | February 2008
EVERYDAY SURVIVAL | Connecting You to Helpful Ideas
Voice-recognition software is not the answer for every stroke survivor. It may be a particular
problem for those who have aphasia or dysarthria (slurred speech). While challenging, learning to type with one hand may be a better solution. There are several options available.
The Half QWERTY keyboard allows the typist to type all letters on only half the keyboard. If you have use of your left hand, then you type on the left half of the keyboard and access the right-hand keys by holding down the space bar. For right-handed users, it’s the opposite.
The BAT keyboard is a one-handed, compact input device that replicates all the functions of a full-size keyboard with only seven keys. Letters, numbers, commands and macros are simple key combinations called “chords.”
MALTRON single-handed keyboards use an entirely different keyboard arrangement and keyboard design. The concave keyboard was engineered so that keys can be accessed quickly and comfortably.
One-hand DVORAK is a regularly shaped keyboard on which the letters have been rearranged from the standard QWERTY arrangement. The developers claim that this arrangement allows for faster typing. Most computers have a switch that allows use of a DVORAK keyboard.
Big-key keyboards have larger keys (1” square) than regular keyboards and may be easier for survivors with either fine-motor skill challenges or visual impairments to navigate. They are available in either QWERTY or ABC formats. These keyboards have a “no run-on keys” feature, which means only a single character will be generated regardless of how long the key is held down.
One-handed QWERTY touch typing is a training program that puts home base at FGHJ. Finger 1 (index finger on the right hand or pinkie on the left hand) handles all keys to the left of R, F, V and the numeral 4; finger 4 handles all keys to the right of U, J, M and the numeral 7. Finger 2 handles T, G, B and 5; finger 3 handles Y, H, N and 6. Developed by a one-handed typist, this program aims to train people to type without looking at the keys.
For more information on these products and one-hand typing in general, visit www.aboutonehandtyping.com.
One-Handed Typing
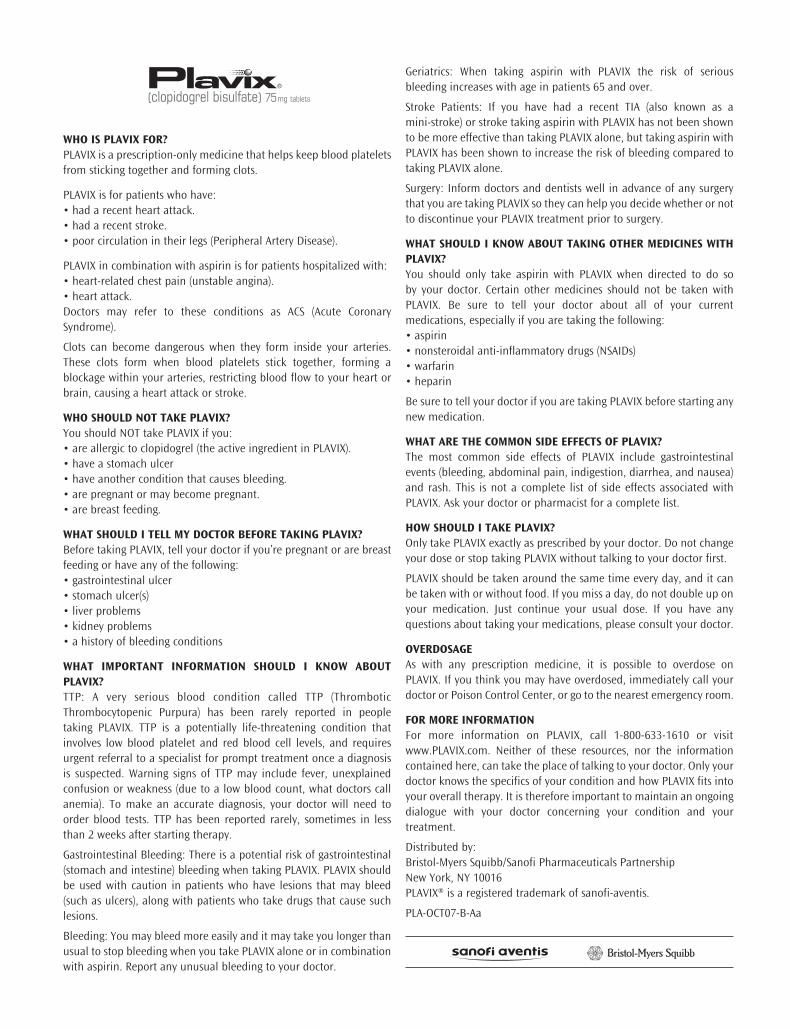
WHO IS PLAVIX FOR?PLAVIX is a prescription-only medicine that helps keep blood plateletsfrom sticking together and forming clots.
PLAVIX is for patients who have:• had a recent heart attack.• had a recent stroke.• poor circulation in their legs (Peripheral Artery Disease).
PLAVIX in combination with aspirin is for patients hospitalized with:• heart-related chest pain (unstable angina).• heart attack.Doctors may refer to these conditions as ACS (Acute CoronarySyndrome).
Clots can become dangerous when they form inside your arteries.These clots form when blood platelets stick together, forming ablockage within your arteries, restricting blood flow to your heart orbrain, causing a heart attack or stroke.
WHO SHOULD NOT TAKE PLAVIX?You should NOT take PLAVIX if you:• are allergic to clopidogrel (the active ingredient in PLAVIX).• have a stomach ulcer• have another condition that causes bleeding.• are pregnant or may become pregnant.• are breast feeding.
WHAT SHOULD I TELL MY DOCTOR BEFORE TAKING PLAVIX?Before taking PLAVIX, tell your doctor if you’re pregnant or are breastfeeding or have any of the following:• gastrointestinal ulcer• stomach ulcer(s)• liver problems• kidney problems• a history of bleeding conditions
WHAT IMPORTANT INFORMATION SHOULD I KNOW ABOUTPLAVIX?TTP: A very serious blood condition called TTP (ThromboticThrombocytopenic Purpura) has been rarely reported in peopletaking PLAVIX. TTP is a potentially life-threatening condition thatinvolves low blood platelet and red blood cell levels, and requiresurgent referral to a specialist for prompt treatment once a diagnosisis suspected. Warning signs of TTP may include fever, unexplainedconfusion or weakness (due to a low blood count, what doctors callanemia). To make an accurate diagnosis, your doctor will need toorder blood tests. TTP has been reported rarely, sometimes in lessthan 2 weeks after starting therapy.
Gastrointestinal Bleeding: There is a potential risk of gastrointestinal(stomach and intestine) bleeding when taking PLAVIX. PLAVIX shouldbe used with caution in patients who have lesions that may bleed(such as ulcers), along with patients who take drugs that cause suchlesions.
Bleeding: You may bleed more easily and it may take you longer thanusual to stop bleeding when you take PLAVIX alone or in combinationwith aspirin. Report any unusual bleeding to your doctor.
Geriatrics: When taking aspirin with PLAVIX the risk of seriousbleeding increases with age in patients 65 and over.
Stroke Patients: If you have had a recent TIA (also known as a mini-stroke) or stroke taking aspirin with PLAVIX has not been shownto be more effective than taking PLAVIX alone, but taking aspirin withPLAVIX has been shown to increase the risk of bleeding compared totaking PLAVIX alone.
Surgery: Inform doctors and dentists well in advance of any surgerythat you are taking PLAVIX so they can help you decide whether or notto discontinue your PLAVIX treatment prior to surgery.
WHAT SHOULD I KNOW ABOUT TAKING OTHER MEDICINES WITHPLAVIX?You should only take aspirin with PLAVIX when directed to do so by your doctor. Certain other medicines should not be taken withPLAVIX. Be sure to tell your doctor about all of your currentmedications, especially if you are taking the following:• aspirin• nonsteroidal anti-inflammatory drugs (NSAIDs)• warfarin• heparin
Be sure to tell your doctor if you are taking PLAVIX before starting anynew medication.
WHAT ARE THE COMMON SIDE EFFECTS OF PLAVIX?The most common side effects of PLAVIX include gastrointestinalevents (bleeding, abdominal pain, indigestion, diarrhea, and nausea)and rash. This is not a complete list of side effects associated withPLAVIX. Ask your doctor or pharmacist for a complete list.
HOW SHOULD I TAKE PLAVIX?Only take PLAVIX exactly as prescribed by your doctor. Do not changeyour dose or stop taking PLAVIX without talking to your doctor first.
PLAVIX should be taken around the same time every day, and it canbe taken with or without food. If you miss a day, do not double up onyour medication. Just continue your usual dose. If you have anyquestions about taking your medications, please consult your doctor.
OVERDOSAGEAs with any prescription medicine, it is possible to overdose onPLAVIX. If you think you may have overdosed, immediately call yourdoctor or Poison Control Center, or go to the nearest emergency room.
FOR MORE INFORMATIONFor more information on PLAVIX, call 1-800-633-1610 or visitwww.PLAVIX.com. Neither of these resources, nor the informationcontained here, can take the place of talking to your doctor. Only yourdoctor knows the specifics of your condition and how PLAVIX fits intoyour overall therapy. It is therefore important to maintain an ongoingdialogue with your doctor concerning your condition and yourtreatment.
Distributed by:Bristol-Myers Squibb/Sanofi Pharmaceuticals PartnershipNew York, NY 10016PLAVIX® is a registered trademark of sanofi-aventis.
PLA-OCT07-B-Aa
A1022 BMS_BC.indd 1 12/6/07 8:10:09 AM
Help raise your protection against another strokewith PLAVIX. If you’ve had a heart attack or stroke, the last thing you want is another onesneaking up on you. PLAVIX may help. PLAVIX is aprescription medication for people who have had arecent heart attack or recent stroke, or who havepoor circulation in the legs (peripheral artery disease)causing pain.
IMPORTANT INFORMATION: If you have a stomachulcer or other condition that causes bleeding, youshould not use PLAVIX. When taking PLAVIX aloneor with some other medicines including aspirin, therisk of bleeding may increase so tell your doctorbefore planning surgery. And, always talk to yourdoctor before taking aspirin or other medicines withPLAVIX, especially if you’ve had a stroke. If youdevelop fever, unexplained weakness or confusion,tell your doctor promptly as these may be signs ofa rare but potentially life-threatening condition calledTTP, which has been reported rarely, sometimes inless than 2 weeks after starting therapy. Other rarebut serious side effects may occur.
PLAVIX offersprotection.PLAVIX isproven to helpkeep bloodplatelets from
sticking together and forming clots, which helpskeep your blood flowing. This can help protect youfrom another heart attack or stroke.
Talk to your doctor about PLAVIX. For more information, visit www.plavix.com
or call 1-888-852-9381.
Add more protection against heart attack or stroke
If you need help paying for prescriptionmedicines, you may be eligible for assistance.Call 1-888-4PPA-NOW (1-888-477-2669).Or go to www.pparx.org.
US.CLO.07.11.085/November 2007 Printed in USA 264US07AB34103-11-07sanofi-aventis U.S. LLC© 2007 Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership
Blood platelets can stick together
and form clots.
PLAVIX helps keep blood platelets from
sticking together.
9If you’ve had a stroke, your chance of having another
is 9 times greater.
Please see important product information forPLAVIX on the previous page.
A1022 BMS_BC.indd 2 12/6/07 8:10:09 AM
National Center
7272 Greenville Avenue
Dallas, Texas 75231-4596
StrokeAssociation.org