Looking toward the future: Consumer preferences for blood-based screening for colorectal cancer...
15
Looking toward the future: Consumer preferences for blood-based screening for colorectal cancer PRESENTER: Dr Ian Zajac AUTHORS: Ian Zajac, Amy Duncan, Ingrid Flight, Carlene Wilson, Deborah Turnbull INSTITUTIONS: CSIRO, Adelaide, South Australia, Australia; The University of Adelaide, Adelaide, South Australia, Australia; Flinders University, Adelaide, South Australia, Australia November, 2013: 15 th World Congress of Psycho-Oncology, Rotterdam, Netherlands Abstract # K-4
-
Upload
dwain-fields -
Category
Documents
-
view
215 -
download
1
Transcript of Looking toward the future: Consumer preferences for blood-based screening for colorectal cancer...

Looking toward the future: Consumer preferences for blood-based screening for colorectal cancer
PRESENTER: Dr Ian Zajac
AUTHORS: Ian Zajac, Amy Duncan, Ingrid Flight, Carlene Wilson, Deborah Turnbull INSTITUTIONS: CSIRO, Adelaide, South Australia, Australia; The University of Adelaide, Adelaide, South Australia, Australia; Flinders University, Adelaide, South Australia, Australia
November, 2013: 15th World Congress of Psycho-Oncology, Rotterdam, NetherlandsAbstract # K-4

Blood Screening | Ian Zajac
• Bowel Cancer is a significant problem in many developed countries, including Australia.
The Problem
2 |

Blood Screening | Ian Zajac
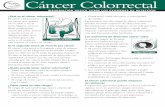
• Bowel Cancer takes many years to develop and progresses slowly.
The Problem
3 |
I
IIA
IIB
IIC
IIIA
IIIB
IIIC
IV
0% 10% 20% 30% 40% 50% 60% 70% 80%
5-Year Survival

Blood Screening | Ian Zajac
• The clear shift in CRC risk as age increases, the relatively slow progression of the disease, and potential for low mortality rates in early stages of CRC presents a ‘screening window’
– Screening involves testing for presence of the disease in apparently healthy people, where they have no recognised increase in risk for that disease
– Key goal: To reduce the community burden of “disease”, measured as a reduction in mortality
– A reduction in incidence can be achieved if we detect preinvasive lesions (adenomas)
– Screening reduces mortality in the vicinity of 15 – 40%
Current approach to CRC prevention
4 |

Blood Screening | Ian Zajac
• The Australian Government introduced ‘organised’ screening in 2006 as part of the National Bowel Cancer Screening Program. Individuals turning 50, 55, 60 and 65 are invited to complete a Faecal Occult Blood Test
• Faecal Occult Blood tests involve sampling from consecutive bowel movements and returning the completed kit within 7 days of sampling
• PROBLEM: Participation rates below 40% and regarded as suboptimal (breast & cervical screening @55-60%)
Organised Screening in Australia
5 |
Detection = sensitivity X participation

Blood Screening | Ian Zajac
• Factors associate with participation include:
• Generic Factors:– knowledge about CRC – perception of risk for developing CRC– Perceived benefits– Health Professional Endorsement*
• Test Specific Factors:– Self Efficacy– Faecal Aversion– Health Professional Endorsement*
Understanding low participation rates
6 |

Blood Screening | Ian Zajac
• Blood-based screening for CRC has been the focus of bench-top science for at least a decade
• Impetus: To develop more ‘sensitive’ tests for CRC detection, and also to overcome pervasive, test-specific factors including Faecal Aversion and Self-Efficacy
• ALSO: Researchers suggest that blood-based tests will ‘improve’ participation.
Improving screening technologies
7 |

Blood Screening | Ian Zajac
• The suggestion that blood-based tests will markedly improve participation is a largely untested hypothesis.
Problem
8 |

Blood Screening | Ian Zajac
• The introduction of blood-based screening may not actually ‘solve’ FOBt participation problems:
• WHY?• Generic Factors:
– knowledge about CRC – perception of risk for developing CRC– Perceived benefits– Health Professional Endorsement
• Test Specific Factors:– Needle Aversion?– Low GP attendance?– Time barriers?
Problem
9 |

Blood Screening | Ian Zajac
• This study sought to untangle our understanding of preference for blood-based screening technology
• In contrast to previous ‘limited’ findings, this study sought to explore proposed participation in ‘real-life’ screening scenarios, rather than measure preference for blood in a ‘dichotomous’ setting (i.e., blood versus stool)
• N=577 community volunteers recruited via CSIRO media completed an online questionnaire and were entered into a prize draw to win an Apple iPad Mini
Study Purpose:
10 |

Blood Screening | Ian Zajac
Scenarios
11 |
Stool-Test Blood-Test
You receive a home stool test kit in the mail. You collect small samples of your stool (bowel motion) at home on separate occasions. Then you mail the samples back for analysis. The test result is posted to your home address and to your doctor.
You receive a blood test kit in the mail. You collect small samples of your blood using a finger prick device at home. Then you mail the samples back for analysis. The test result is posted to your home address and to your doctor.
You receive a home stool test kit in the mail. You collect small samples of your stool (bowel motion) at home on separate occasions. Then you take the samples to a collection centre to be analysed. The test result is posted to your home address and to your doctor.
You receive a script for a blood test in the mail. Then you attend a collection centre to have your blood taken and analysed. The test result is posted to your home address and to your doctor.
You visit your doctor to get the home stool test kit. Then you collect small samples of your stool (bowel motion) at home on separate occasions. After this, you deliver the samples to the collection centre to be analysed. The test result is mailed to your home address and to your nominated doctor.
You visit your doctor to get a script for a blood test. Then you attend a collection centre to have your blood taken and analysed. The test result is posted to your home addressand to your doctor.
You visit your doctor to get the home stool test kit. Then you collect small samples of your stool (bowel motion) at home on separate occasions. After this, you deliver the samples to the collection centre to be analysed. The test result is mailed to your doctor only and you need to visit your doctor to get your result.
You visit your doctor to get a script for a blood test. Then you attend a collection centre to have your blood taken and analysed. The test result is mailed to your doctor only and you need to visit your doctor to get your result.
Incr
easi
ng C
ompl
exity

Blood Screening | Ian Zajac
Results
12 |
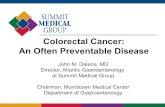
At Home Path Visit GP + Path GP + Path + GP1
1.5
2
2.5
3
3.5
4
4.5
StoolBlood
Sample type was significantly associated with likelihood of participating in screening. Blood tests were preferred over stool test regardless of the level of engagement, though participants were significantly more likely to participate in screening tests that involved either none (Home only) or only one point of contact (path lab). The model also indicated that increased level of engagement led to greater decreases in likelihood of participating for both blood and stool independently.
Parti
cipa
tion
Like
lihoo
d Ra
tings

Blood Screening | Ian Zajac13 |
ResultsComparing the current FOBt approach to Blood scenarios:
For which Blood screening scenarios is the likelihood of participation lower than that reported for FOBt?
Stool Test(mean,SD)
Blood Test(mean, SD)
t (df=576)
p
None (at home) 4.05 (1.14) 3.97 (1.23) 1.477 .140
1 (path lab) - 3.70 (1.14) 6.255 >.001
2 (path lab plus GP) - 3.12 (1.25) 14.501 >.001
3 (path lab plus GP x2)
- 2.77 (1.35) 17.935 >.001
DV = Participation Likelihood

Blood Screening | Ian Zajac14 |
Conclusions
• The potential introduction of blood-based screening methods will not automatically ‘solve’ screening participation issues
• Screening scenarios required for blood methods are inherently more time consuming, and are therefore accompanied by lower participation ‘likelihood’ ratings
• All ‘realistic’ blood scenarios had significantly lower ‘intended’ participation ratings than the current NBCSP/FOBt approach
• The entire ‘context’ of screening behaviour needs to be considered when developing and implementing new screening technologies. Human behaviour is complex and is not adequately represented in ‘dichotomous’ choice settings

Blood Screening | Ian Zajac
Thanks for listening!
15 |