
Long run effects of temporary incentives on medical care productivity in Argentina
21
JUNE 11, 2015 PABLO CELHAY PAUL GERTLER PAULA GIOVAGNOLI CHRISTEL VERMEERSCH Long Run Effects of Temporary Incentives on Medical Care Productivity
-
Upload
rbfhealth -
Category
Healthcare
-
view
52 -
download
0
Transcript of Long run effects of temporary incentives on medical care productivity in Argentina
J U N E 1 1 , 2 0 1 5
P A B L O C E L H A YP A U L G E R T L E R
P A U L A G I O V A G N O L IC H R I S T E L V E R M E E R S C H
Long Run Effects of Temporary Incentives on Medical Care Productivity
T E M P O R A R Y I N C E N T I V E S H A D A L O N G -R U N I M P A C T O N M E D I C A L C A R E
P R O D U C T I V I T Y
T E M P O R A R Y I N C E N T I V E S H E L P E D O V E R C O M E T H E I N I T I A L C O S T O F
I M P R O V I N G M E D I C A L C A R E R O U T I N E S
Main findings
Routines in medical care
Medical care is a complex technology
Coordination of team activities is key
Routines = “Established rules”, “standard operating procedures” that become habits

Institutions have a hard time changing their routines... It takes effort.. It takes time.. It might be costly

Medical care routines can be suboptimal
E.g.: Adherence to clinical practice guidelines (best-practice) is low.
18%
24%
45%
46%
50%
60%
67%
75%
81%
84%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
India - Diahrrea
Tanzania - Malaria
Rwanda - Prenatal Care
Indonesia - Tuberculosis
USA - Preventive Care
USA - Chronic Conditions
Netherlands - Family
Mexico - Prenatal Care
UK - Diabetes
UK - Asthma
Adherence to CPG
Source: Authors’ elaboration based on Schuster et al. (1998); Grol (2001); Campbell et al. (2007); Das and Gertler (2007); and Gertler and Vermeersch (2012).
Role of incentives – causal chain
Initial/Upfront cost inhibits change of routines
Financial incentives may help overcome this initial cost
Once the institution adopts new routines, it will continue them as long as recurrent costs are covered.

The Misiones experiment
Misiones Province

The Misiones experiment
Aim: Increase the probability that 1st prenatal visits take place in first trimester In primary care setting
Intervention: Temporary (8 months) increase in fees
40
120
40 40
0
20
40
60
80
100
120
140
Pre & post periods Intervention period
Fee-for-service payment for 1st prenatal visit before week 13
Treatment Control
+200%
Arg. Pesos

The Misiones experiment
Identification strategy:
Randomized assignment of 37 primary care clinics to treatment and control
Assignment not fully respected (but close enough) use IV estimator
Treated Not treated
Assigned to treatment
14 4
Assigned to control
1 18

Timeline
Jan
2009
May
2010
Dec
2010
Mar
2012
Dec
2012
Pre-intervention Intervention Post intervention I
Post intervention II
Data
Clinic records
services delivered
Registry of Plan Nacer beneficiaries
beneficiary status of the mother
Hospital medical records
birth outcomes
link using the mother’s national identity number

Results

Weeks pregnant at first prenatal visit
PRE POST
-1.47

Proportion of mothers with prenatal visit before week 13
PRE POST
+0.11
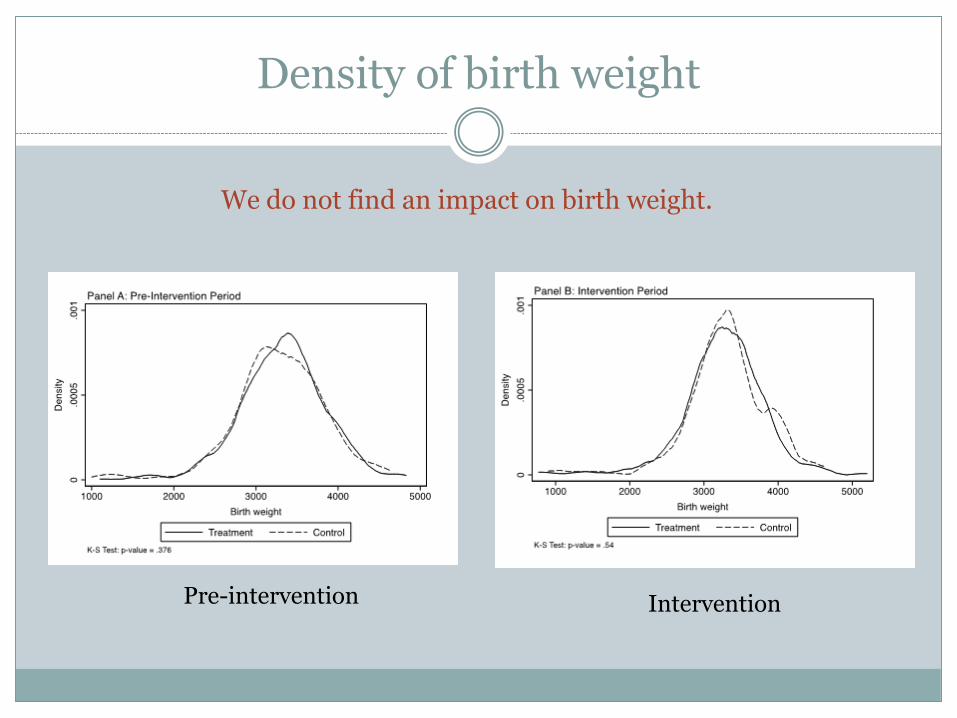
Density of birth weight
Pre-intervention Intervention
We do not find an impact on birth weight.
C H A N G E S I N R O U T I N E S
E V I D E N C E F R O M I N - D E P T H I N T E R V I E W S
Mechanisms
What did treatment clinics do?
Change in assignment of incentives to personnel
Conditioned on number of women brought in
Change in routines to improve efficiency of outreach by community health workers
Offer pregnancy tests to mothers when picking up milk for their children
Visit adolescents when parents aren’t home
Visit women who abandoned birth control pills
Organize the Ob/Gyn schedule to ensure predictability of service
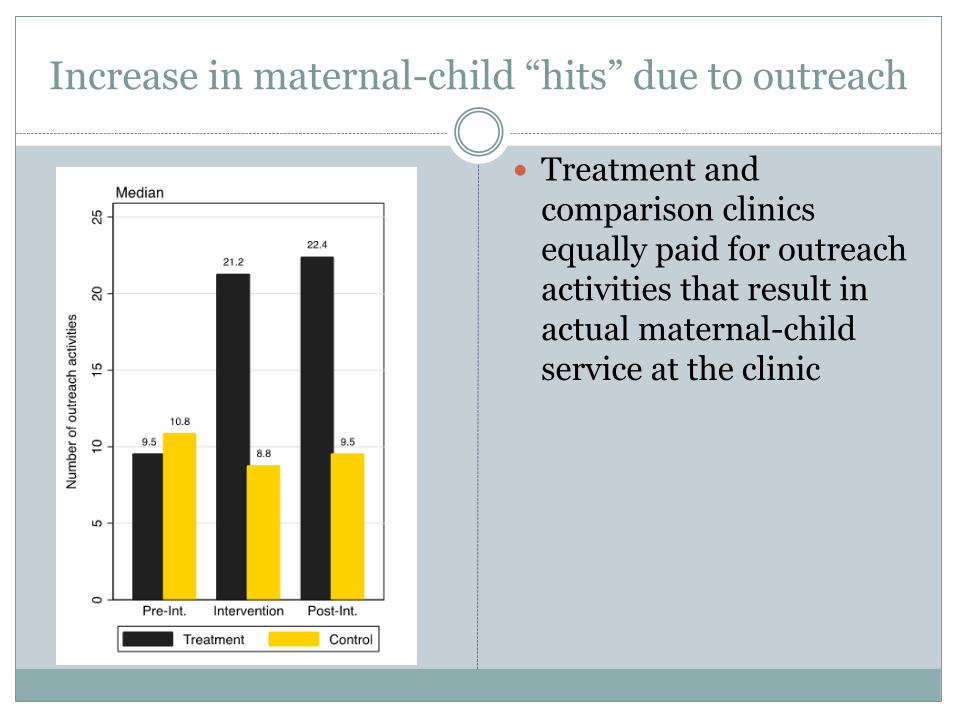
Increase in maternal-child “hits” due to outreach
Treatment and comparison clinics equally paid for outreach activities that result in actual maternal-child service at the clinic

Why no impact on birth outcomes?
Hypothesis: Impact of early prenatal care is uneven in the population
Need to be able to reach very high risk women
Impacts are washed out in a population average
I n c e n t i v e s i n c r e a s e d i n i t i a t i o n o f p r e n a t a l c a r e b e f o r e w e e k 1 3 b y 3 5 % .
E f f e c t p e r s i s t e d f o r a t l e a s t o n e y e a r a f t e r t h e i n c e n t i v e s e n d e d .
T e m p o r a r y i n c e n t i v e s h e l p p r o v i d e r s t o o v e r c o m e i n e r t i a a n d c h a n g e c l i n i c a l p r a c t i c e r o u t i n e s .
N e e d t o t a i l o r i n c e n t i v e s t o t a r g e t h i g h - r i s k p o p u l a t i o n s .
Conclusions

Martin Sabignoso, National Coordinator of Plan Nacer and Humberto Silva, National Head of Strategic Planning ofPlan Nacer led the development and implementation of the experiment.
Luis Lopez Torres and Bettina Petrella from the Misiones Office of Plan Nacer oversaw the implementation of thepilot facilitated access to provincial data, supported the authors in interpreting datasets and the provincial legalframework and in carrying out the in-depth interviews.
Fernando Bazán Torres, Ramiro Florez Cruz, Santiago Garriga, Alfredo Palacios, Rafael Ramirez, Silvestre RiosCenteno, and Adam Ross provided excellent assistance and project management support.
Alvaro Ocariz, Javier Minsky and the staff of the Information Technology unit at UEC provided valuable support inidentifying sources of data.
Sebastian Martinez, Luis Perez Campoy, Vanina Camporeale and Daniela Romero contributed to the initial designof the pilot.
The Health Results Innovation Trust Fund (HRITF) and the Strategic Impact Evaluation Fund (SIEF) of the WorldBank generously funded the evaluation.
The opinions in the paper are of the authors alone and do not necessarily represent the opinions of the funder ortheir affiliated institutions.
Acknowledgements


















