Long Gap Esophageal Atresia
23
Long Gap Esophageal Atresia: Magnetic Compression Anastomotic Repair Charles Wulff Tufts Medical Student
-
Upload
freemind323 -
Category
Documents
-
view
290 -
download
20
description
Presentation on EA and Magnetic Repair
Transcript of Long Gap Esophageal Atresia
-
Long Gap Esophageal Atresia: Magnetic Compression Anastomotic RepairCharles WulffTufts Medical Student
-
ObjectivesOverview of Esophageal AtresiaCurrent TreatmentsWhat is Long Gap Atresia and how its repair differsMCA Repair- Background and Procedure
-
Esophageal AtresiaEpidemiology1 in 2500 Live BirthsEtiology:No specific etiologySome associations with mutations of the N-myc, Sox-2 and CHD7 genesEmbryologyEsophagus and Trachea share same embryonic origin~4 weeks GA, improper development at of trachebronchial diverticulum and elongation of the esophagus results in atresia and fistula formationMultiple associated abnormalities (VACTERL Association)
-
Date of download: 2/19/2015Copyright 2015 McGraw-Hill Education. All rights reserved.
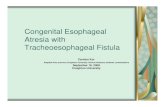
From: Specific ConsiderationsSchwartz's Principles of Surgery, 10e, 2014
Typce C is the most common-85%Type A second most common, 8-10%Type E- 8%Type D- 2%Type B- 1% *
-
Associated Conditions
VACTERL (VATERL, VATER) associationV = vertebral anomalies (hemi- and bifid vertebrae)A = anorectal malformation (imperforate anus)C = congenital cardiac defects (VSD, ASD, tetralogy of Fallot) TE = trachea-esophageal anomalies (esophageal atresia)R = renal-urinary defects (absent kidney, hypospadias)L = limb defects (radial dysplasia) Maternal PolyhydramniosCongenital Esophageal Stenosis
-
PresentationVery difficult to diagnose prenatallyUS: polyhdramnios, dilated proximal pouch and absence of gastric bubbleMRI: Non-visualization intra-thoracic esophagusPostnatal presentation, if Type A, B, C,or D:After initiating feeding: cough, apnea, cyanosis, tachypneaCan also occur due to inability to swallow secretionsAbdominal distension if distal pouch has fistula to tracheaX-ray shows impassible orogastric catheter with air in stomachType E- Presents with recurrent PNA and chemical pneumonitis of lungs
-
Imaging: Classic CXR
-
SequelaeAspiration/Choking/ApneaPneumoniaChemical Pneumonitis Failure to thriveCompression of diaphragm (from stomach inflation)Death in 1 week if unrecognized/untreatedUntil 1939, no effective surgical treatment.
-
PrognosisMost important predictors: Birth weightSeverity of pulmonary dysfunction Presence of major congenital cardiac disease
Montreal Childrens Hospital StagingGroupCharacteristicsSurvival RateI-Weight > 1,500 g-No major cardiac anomalies 97%II-Weight < 1,500 gOR-Major cardiac anomalies 59%III -Weight < 1,500 gAND-Major cardiac anomalies 22%
-
ManagementBefore treatment, stabilize: Ventilate, drainage for upper pouch, and possible gastrostomy tube to alleviate abdominal distension (which can compress lungs)Contraindications for immediate surgeryLong Gap AtresiaLow BWCongenital Heart DiseaseUnstable airway status
-
Treatment MethodsOnce patient is stable:Primary repair- Either thoracotomy or thorocoscopyThoracotomy: Right side incision, followed by mobilization of the pleura Ligation of azygous vein Transection of any tracheoesophageal fistula, with repair of the trachea with a single layer of interrupted suturesEnd to end anastomosis between proximal and distal esophagus with a single layer of interrupted sutures Thorocoscopy-Same approach, but less invasive
-
Post Operative ComplicationsLeak : 10-15%Stricture: 10-20%, serial balloon dilation or Tuck dilatorsGERD:CommonEsophageal Dysmotility: CommonThoracic Wall deformities (Winged Scapula, Scoliosis):~20%Recurrence of the atresia: Rare, but anastomosis can fail
-
Long Gap AtresiaLong gap atresia is defined as >2.5 Vertebral bodies or >3cmInitially, primary surgery is not usually possible.Repair has to be delayed for 1-3 months, though it can be up to a year before final repairDrainage placed in proximal pouch to drain swallowed secretionsGastrostomy tube placed in distal pouch for feedingSome long gaps self resolve and can be repaired with the primary surgical approach, most need lengthening
-
Long Gap Atresia TreatmentOften done as 2 step procedure: Extension AnastomosisCurrent extension techniques include:Foker Process: Replacement: Gastric pull up or gastric, jejunum, or colon transplant to bridge gapBakes Dilators: Repeated non-invasive lengthening maneuvers
-
Long Gap complicationsComplicationsSame as with the standard repairs, however, leaks are far more common, as well as a higher risk of stricturesMany have long term GI issues years after treatment More likely to fail completely, due to tension on the anastomotic sutures
-
Magnetic Compression Anastomotic Repair (MCA Repair)BackgroundFirst suggested in the 1975, using electromagnetic repair at MGHUsed external electromagnet to drive 2 metal bulletsStretching the esophageal pouches stimulated tissue growthWould then repair using standard surgical repair
-
MCA RepairCurrent methods:Case study in 2001-2004Still relies on stretching to stimulate tissue growthUses rare earth magnets (Samrium-cobalt and Neodymium-iron-boron) that are catheter based & latex-freeWhen magnets meet, they compress the tissueCenter of compression site becomes ischemic, causing tissue to slough off, making the esophagus patent The outer rim heals, uniting the pouches and creating an end to end anastmosis
-
MCA Repair Technique1st stage: Bakes dilators used to manually lengthen and widen pouches, with full thickness sutures placed for alignment1 placed at the center, 1 on the lateral pouch end bilaterally2nd Magnets placed using guide wires into each pouch, and checked for magnetic tension3-5 days for lengthening3-5 days for anastomotic compressionConfirm with contrast patency and integrity of anastomosis, then removePlacement and removal takes ~20 minutesNew anastomosis often then protected by feeding tube to allow feedings and prevent closure
-
Lovvorn, Harold N., Christopher M. Baron, Melissa E. Danko, Nathan M. Novotny, Brian T. Bucher, Krystal K. Johnston, and Mario F. Zaritzky. "Staged Repair of Esophageal Atresia: Pouch Approximation Andcatheter-based Magnetic Anastomosis."Journal of Pediatric Surgery Case Reports(2014): n. pag. Web.
-
OutcomesSutureless anastomosisAllows for anastomosis using only esophageal tissue, versus transplant of gastric or other GI tract tissueMinimizes the invasiveness compared to classic tension based approaches, which require multiple thoracotomy/thorocoscopy
-
Limitations and ComplicationsLimitationsMagnetic fields lose effectiveness over distance.Most are effective at maximum distance of 3-5cm Complications Still encounter the same problems of most long gap repairsNo reports of failuresMagnets can also theoretically become lost- Same issues of magnetic ingestions (Fistulas, perforations) and inability to use magnetic imagingNo such issues reported so far
-
Current EvidenceMost papers are limited to case studiesOf those studies, most have shown success, though small sample poolTrials limited by small number of long-gaps, plus novelty of treatmentLarger pool of MCA used for significant stricture or failure of anastomosis Primary repair still remains best treatment when it is possible
-
SummaryEsophageal Atresia is a life threatening congenital condition if not identified or repairedCurrent surgical repair allows for approximation and anastomosis of esophageal atresiaLong gap has additional complications for repair, requiring delay of treatment and often a 2 step repairMCA allows a less invasive, sutureless anastomosis of the esophagus; however, limited use has limited evaluation
-
SourcesHackam, David J., et al."Pediatric Surgery."Schwartz's Principles of Surgery, 10e.Eds. F. Charles Brunicardi, et al.New York, NY: McGraw-Hill, 2014. n. pag.AccessMedicine.Web.22 Feb.2015..Gonzales, Kelly D., and Hanmin Lee."Chapter 35. Congenital Disorders of the Trachea & Esophagus."CURRENT Diagnosis & Treatment in OtolaryngologyHead & Neck Surgery, 3e.Ed. Anil K. Lalwani.New York, NY: McGraw-Hill, 2012. n. pag.AccessMedicine.Web.22 Feb. 2015.Stringer, Mark D., Kathleen M. Mckenna, Ruth B. Goldstein, Roy A. Filly, N.scott Adzick, and Michael R. Harrison. "Prenatal Diagnosis of Esophageal Atresia."Journal of Pediatric Surgery30.9 (1995): 1258-263. Web.Zaritzky, Mario, Ricardo Ben, Gaston I. Zylberg, and Brian Yampolsky. "Magnetic Compression Anastomosis as a Nonsurgical Treatment for Esophageal Atresia."Pediatric Radiology39.9 (2009): 945-49. Web.Lovvorn, Harold N., Christopher M. Baron, Melissa E. Danko, Nathan M. Novotny, Brian T. Bucher, Krystal K. Johnston, and Mario F. Zaritzky. "Staged Repair of Esophageal Atresia: Pouch Approximation Andcatheter-based Magnetic Anastomosis."Journal of Pediatric Surgery Case Reports(2014): n. pag. Web.Takamizawa, Shigeru, Eigoro Yamanouchi, Toshihiro Muraji, Eiji Nishijima, Shiiki Satoh, and Jiro Tsugawa. "MCRA of an Anastomotic Stenosis after Esophagoesophagostomy for Long Gap Esophageal Atresia: A Case Report."Journal of Pediatric Surgery42.5 (2007): 769-72. Web.Hendren, W. Hardy, and J. Richard Hale. "Electromagnetic Bougienage to Lengthen Esophageal Segments in Congenital Esophageal Atresia."New England Journal of Medicine293.9 (1975): 428-32. Web.Esophageal Atresia - Radiographic Features. Digital image.Pediatric Radiology. The University of Virginia, 2013. Web. .
-
Questions?
Typce C is the most common-85%Type A second most common, 8-10%Type E- 8%Type D- 2%Type B- 1% *