Localized bone augmentation and implant site development
55
LOCALIZED BONE AUGMENTATION AND IMPLANT SITE DEVELOPMENT Chapter 72
-
Upload
palm-immsombatti -
Category
Health & Medicine
-
view
113 -
download
1
Transcript of Localized bone augmentation and implant site development

LOCALIZED BONE AUGMENTATION AND IMPLANT
SITE DEVELOPMENTChapter 72
Localized bone augmentation and implant site development• Guided bone regeneration• Barrier membranes• Bone graft materials• Autogenous bone
• Localized ridge augmentation• Flap management• Horizontal bone augmentation• Simultaneous implant placement• Complications
Localized bone augmentation and implant site development• Alveolar ridge preservation/management of
extractions• Delayed implant placement• Staged implant placement• Delayed versus staged technique• Immediate implant placement

• Standard implant surgery • Adequate bone volume and quality• Adequate remodeling and maturation of bone
• Surgical bone augmentation• To correct or to prevent alveolar ridge deficiency
Localized bone augmentation and implant site development

• Guided tissue regeneration(GTR) : Specific cells contribute to the formation of specific tissue • Exclusion of the faster-growing epithelium and
CNT from a periodontal wound.• Osteoblasts, cementoblasts and periodontal
ligament cells -> regenerate a new periodontal attachment
Guided tissue regeneration(GTR)

Guided bone regeneration (GBR)• In membrane-protected defects, bone
regeneration was initiated by formation of woven bone along new blood vasculature at the periphery of the defect
• Bone was being isolated from the surrounding soft tissue : GBR
Schenk et al. Int J Oral Maxillofac Implants 1994
Guided bone regeneration (GBR)
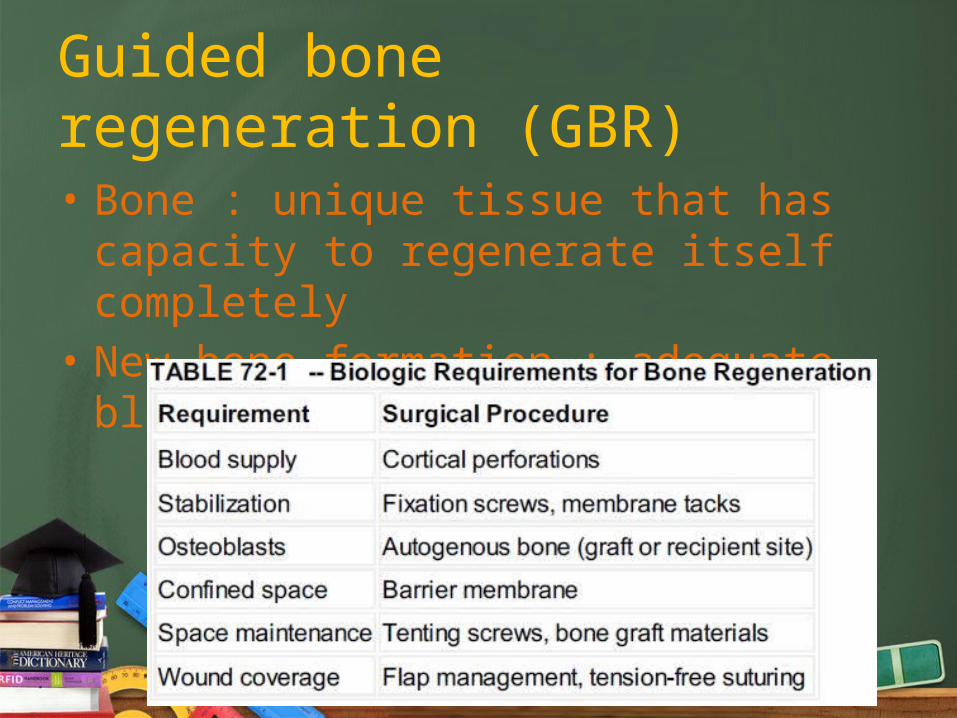
• Bone : unique tissue that has capacity to regenerate itself completely
• New bone formation : adequate blood supply

• Biocompatible materials• Protect blood clot• Prevent soft tissue cells from migrating into
bone defect• Resorbable / Nonresorbable materials
GBR: Barrier membranes
• Ideal properties 1. Biocompatibility2. Space maintainance3. Cell occlusiveness4. Good handling properties5. Resorbability or ease of removal(Nonresorbable)
GBR: Barrier membranes

• Nonresorbable barrier membranes• Latex, Teflon (ePTFE, Gore-tex)• Variety of shapes and sizes• Combined with bone graft material for space
maintainer
GBR: Barrier membranes
Case by Prof. Massimo Simion & Dr. Isabella Rocchietta, Italy/UK

• Nonresorbable barrier membranes• Require second surgery to remove (6-12 months)• Stiffer membranes (Titanium-reinforced) :
promote significant amount of new bone
GBR: Barrier membranes
• Nonresorbable barrier membranes• Advantages• Maintain separation of tissue over an extended
time• Disadvantages• If it becomes exposed, it will not heal• Membrane exposure -> infection
GBR: Barrier membranes
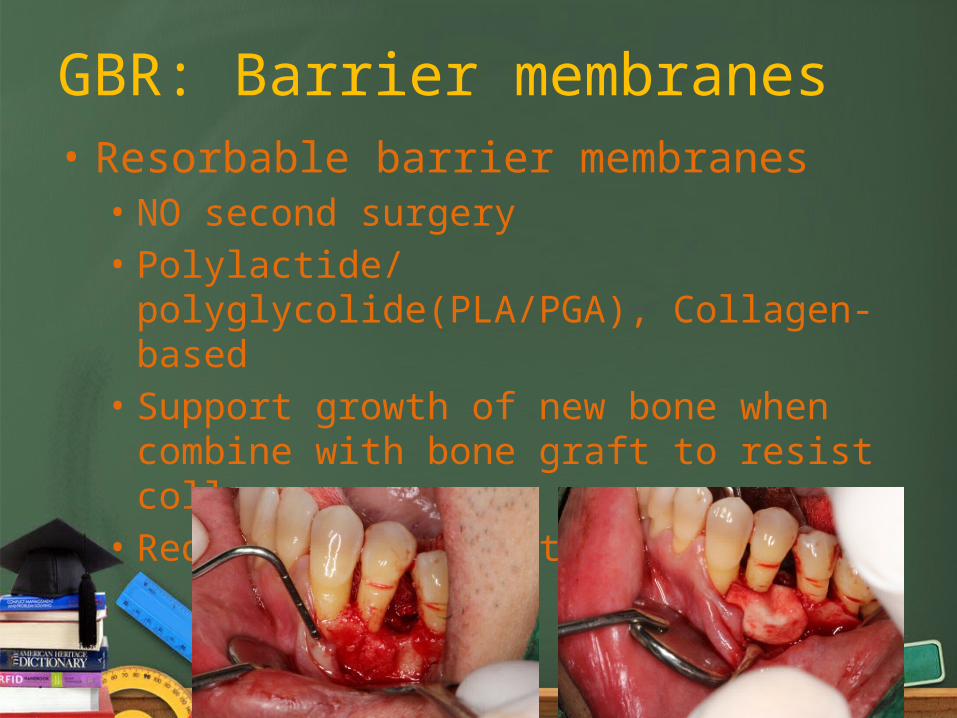
• Resorbable barrier membranes• NO second surgery• Polylactide/ polyglycolide(PLA/PGA), Collagen-
based• Support growth of new bone when combine with
bone graft to resist collapse• Reduce bone resorption
GBR: Barrier membranes
• Resorbable barrier membranes• Advantages• No second surgery• Less likely to become expose• Less problematic if they do become exposed
• Disadvantages• May degrade before bone formation complete• The degradation process may produce inflammation• Lack of stiffness -> tenting screws, plates
GBR: Barrier membranes

GBR: Bone graft materials
• To facilitate bone formation within a given space by occupying and allowing subsequent bone growth
• Biologic mechanism • Osteoconduction• Osteoinduction• Osteogenesis
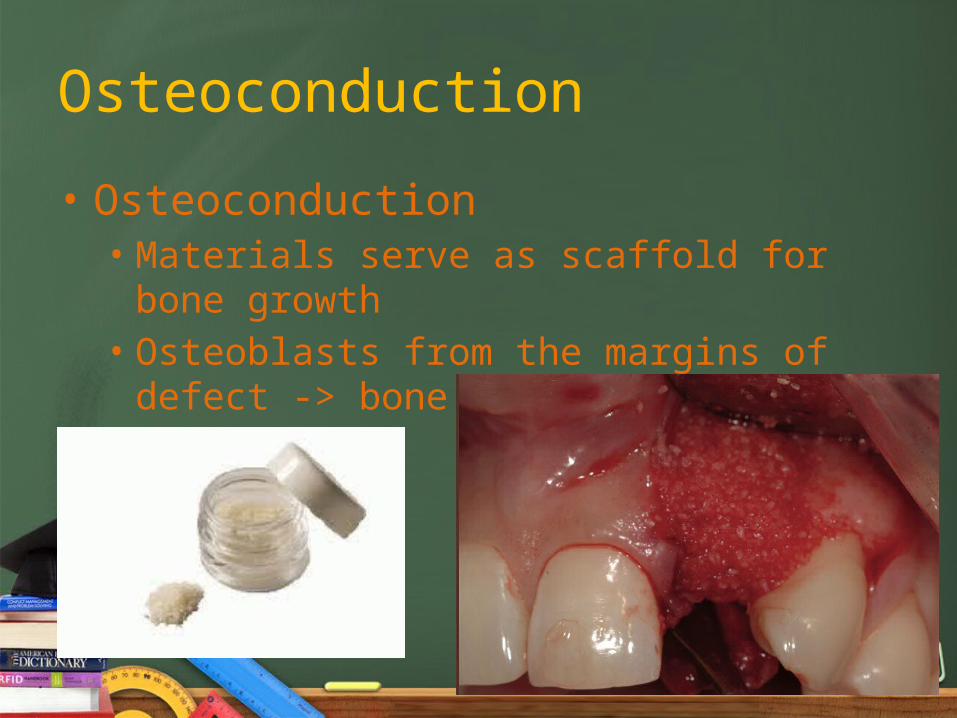
• Osteoconduction• Materials serve as scaffold for bone growth• Osteoblasts from the margins of defect -> bone
formation
Osteoconduction

Osteoinduction
• Osteoinduction• Stimulate osteoprogenitor cells from the defect to
differentiate into osteoblasts -> forming new bone• The induction of bone-forming process by
activating bone-forming cells through mediators• Bone morphogenic proteins (BMP)
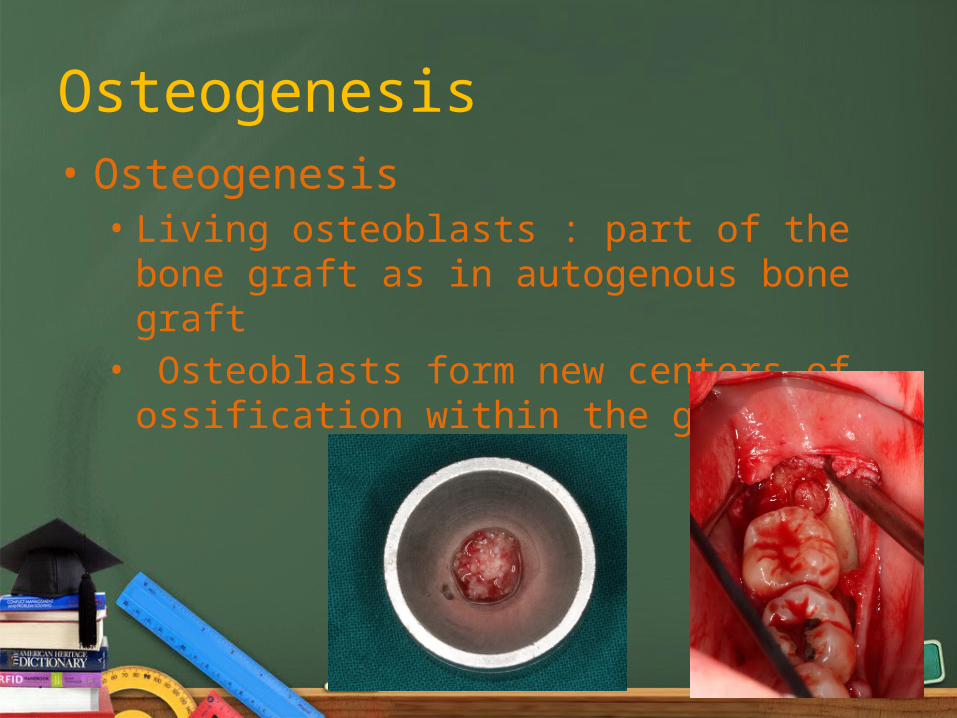
Osteogenesis• Osteogenesis• Living osteoblasts : part of the bone graft as in
autogenous bone graft• Osteoblasts form new centers of ossification
within the graft
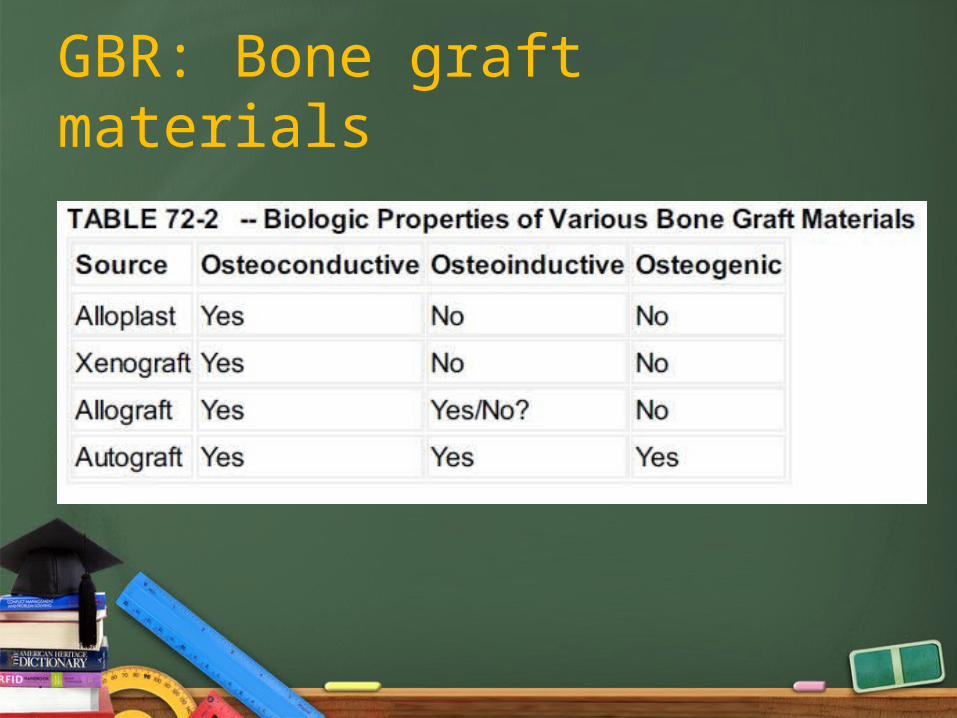
GBR: Bone graft materials
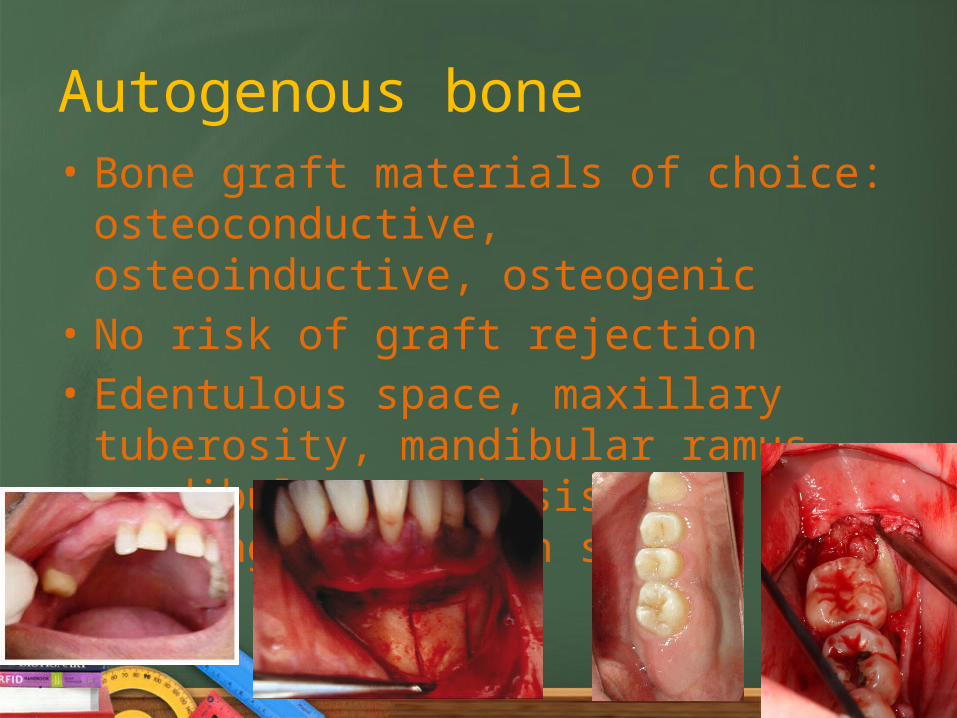
Autogenous bone• Bone graft materials of choice:
osteoconductive, osteoinductive, osteogenic• No risk of graft rejection• Edentulous space, maxillary tuberosity,
mandibular ramus, mandibular symphysis and healing extraction socket (6-12 weeks)

Autogenous bone
• Disadvantages : increase risk of morbidity• Mandibular symphysis : postoperative bleeding,
bruising, wound dehiscence, damage lower incisors and injury to nerves
• Retrospective analysis of 48 chin graft : 5-mm margin of safety between graft harvest and vital structures
Hunt et al. Int J Periodontics Restorative Dent 1999

• Basic principles to minimize the risk of postoperative morbidity• Radiographic evaluation • Locate mental nerve and foramen• Do not elevate or reflect muscle
attachment beyond the inferior border mandible
• 5 mm safety zone : tooth apices, inferior border of mandible, mental foramen
Autogenous bone

• Basic principles to minimize the risk of postoperative morbidity• Do no harvest deeper than 6mm • Suture the wound in layers• Prevent overheating : 47 °C can cause bone
necrosis -> proper irrigation / Piezoelectric bone surgery
Autogenous bone
Localized bone augmentation and implant site development• Guided bone regeneration• Barrier membranes• Bone graft materials• Autogenous bone
• Localized ridge augmentation• Flap management• Horizontal bone augmentation• Simultaneous implant placement• Complications
Localized ridge augmentation
• Size and morphology of defects : horizontal/ vertical
• Combine with barrier membrane• To achieve good results
• Blood supply• Stable and protect space for bone growth• Tension-free flap wound closure
Flap management
• Incisions, reflection, and manipulation should be designed to• Preserve vascularity of the flap• Minimize tissue injury
• Remote incision : wound opening is positioned away from the graft.
Flap management
• Periosteal releasing incision/ Coronal advancement of the flap + Crestal incision
• To achieve tension-free flap closure
• Suture removal 10-14 days• No prosthesis inserted for 2-3 weeks
• General concepts for flap management• Make incision remote to the placement of barrier
membrane• Elevate full thickness flap 5mm beyond the edge of bone
defect• Vertical releasing should be minimize• Tension-free suture : Periosteal releasing incision
Flap management
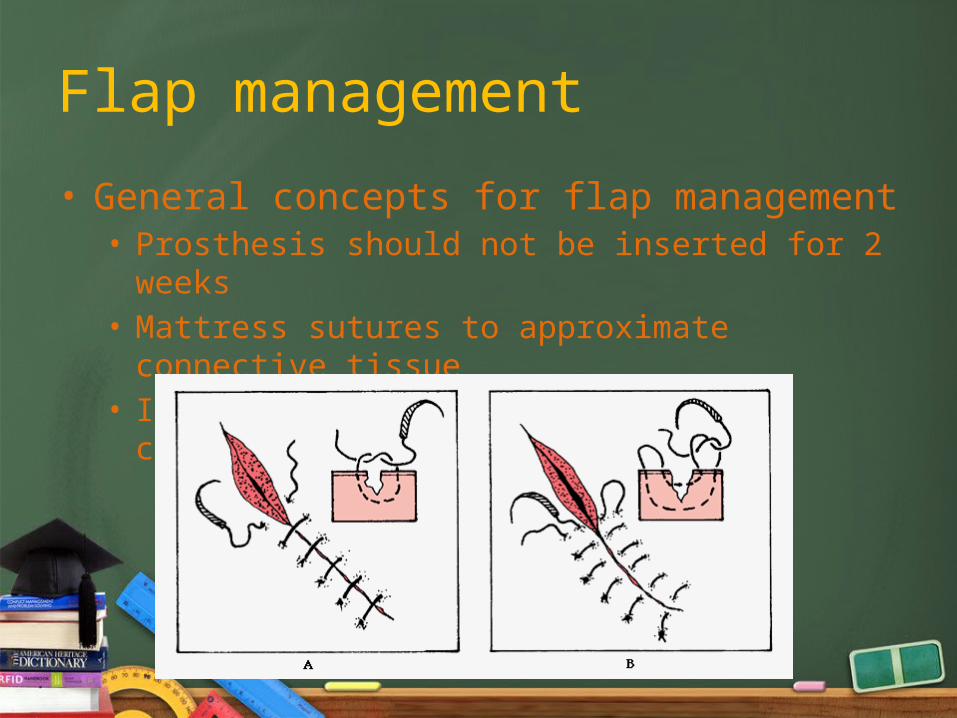
• General concepts for flap management• Prosthesis should not be inserted for 2 weeks• Mattress sutures to approximate connective tissue• Interupted sutures to adapt wound closure
Flap management

Horizontal bone augmentation
• Dehiscence / fenestration of implant surface• Maxillary tuberosity graft -> increased ridge
width but 50% resorption
• Block graft from retromolar/ symphysis show no clinical sign of resorption
Ten Bruggenkate et al. Int J Maxillofac Surg 1992
Buser et al. J Oral Maxillofac Surg 1996
Horizontal bone augmentation
• FDBA + Membrane -> increased amount of new bone and no remaining allograft materials in 9 months
• Particulate bone graft• Monobloc bone graft
Doblin et al. Int J Periodontics Restorative Dent 1996Nevin, Mellonig. Int J Periodontics Restorative Dent 1994
• Particulate bone graft• Smaller pieces rapid ingrowth of blood vessels• large osteoconduction surface• more expose osteoinductive growth factors• Lack of rigid• Easily displaced
Horizontal bone augmentation
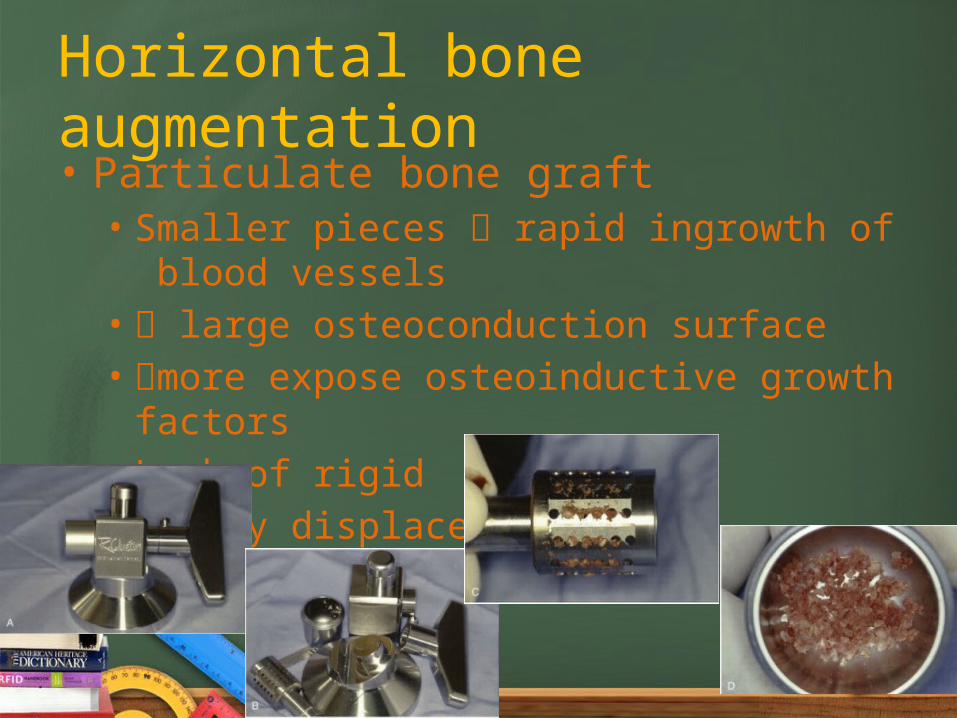
• Particulate bone graft• Smaller pieces rapid ingrowth of blood vessels• large osteoconduction surface• more expose osteoinductive growth factors• Lack of rigid• Easily displaced
Horizontal bone augmentation
• Particulate bone graft : indication• Defect with multiple osseous wall that will contain
the graft• Dehiscence or fenestration defect
• Bone graft and barrier membrane combination when bone defect does not containable
Horizontal bone augmentation


Monocortical block graft
• Harvest from the remote site : symphysis, ramus, iliac crest, tibia
• With/without barrier membrane • Screws or plate remove after an adequate of
time (6 months)• Disadvantages: biologic limitation of
revascularizing large block

Monocortical block graft
6 months

Monocortical block graft
Simultaneous implant placement
• In selected case, bone augmentation can be placed simultaneously with implant placement
• good primary stability in native bone

Simultaneous implant placement
Fenestration defects Dehiscence defects
• Barrier membrane VS periosteal flap coverage of expose implant surface
• Membrane was far superior with regard to bone file
• 66% of treated with membrane resulted in 95-100% elimination of dehiscence
Simultaneous implant placement
Dahlin et al. Clin Oral Implants Res 1991
Palmer et al. Clin Oral Implants Res 1994

• 55 Branemark implant(machine-surface, external hex) treated by ePTFE membrane alone -> 82% bone fill
-> Cumulative survival rate 84.7%(Max), 95%(Mand)
Simultaneous implant placement
Dahlin et al. Int J Oral Maxillofac Implants 1995
• The use of graft materials in conjunction with membrane treatment, especially FDBA+GBR
• Success rate of 96.8% (bone fill >90% of dehiscence)
Simultaneous implant placement
Rominger et al. J Oral Maxillofac Surg 1994
Complications• Bleeding• Postoperative infection• Bone fracture• Nerve dysfunction• Perforation of the
mucosa
• Sinusitis• Pain• Decubital ulcers• Wound dehiscence• Loss of portion of bone
graft
• The amount of new bone formation ->• The length of membrane healing• Size of the defect
• Bone regeneration depend on anatomy of bone defect at the time of implant placement
Complications
Localized bone augmentation and implant site development• Alveolar ridge preservation/management of
extractions• Delayed implant placement• Staged implant placement• Delayed versus staged technique• Immediate implant placement

Alveolar ridge preservation
• Tooth extraction -> alveolar ridge resorption
• Preservation of bone volume -> Goal• First 6- 24 months : most bone loss• Barrier membrane enhance predictability of
bone fill compared with mucoperiosteal flap alone

• Timing of implant placement depend on• Quantity, quality and support of existing bone• Agreement of clinician and patient • Immediate : implant place at the time of extraction • Delayed : implant place approximately 2 months after
extraction • Staged : implant placement allow for substantial bone
healing (4-6 months)
Alveolar ridge preservation
• Tooth extraction : atraumatic surgical technique, avoid bucco-lingual forces
• Remove soft tissue from extraction socket• Evaluate bone level and socket anatomy
• Whether to bone-graft the site, when to place the implant
Alveolar ridge preservation
Delayed implant placement
• Allow time for soft tissue healing to close the wound
• Facilitate more osteogenesis because bone formation is active within the first few months
• Resolution of infection
Staged implant placement
• Allow adequate time for osseous healing : complete hard and soft tissue healing
• Implant place into healed bone sites • Adequate coverage by hard and soft tissues• Disadvantage : require the time for bone
healing

Delayed VS staged technique
• When to place the implant : quantity and location of bone surrounding the tooth
bone sounding
• If little or no bone exists -> require bone augmentation

Immediate implant placementc
• Reduce healing time• Bone-to-implant healing begins immediately
with extraction site healing• Disadvantages : need for subsequent
mucogingival surgery to correct soft tissue

• Implant may be placed in extraction socket along with bone augmentation without flap advancement : One-stage surgery
• One-stage approach with immediate implant placement and provisionalization
Best way to manage hard and soft tissue
Immediate implant placementc

Conclusions
• Localized bone augmentation allow clinicians to reconstruct horizontal alveolar ridge defeciencies
• Implant can be placed simultaneously with the augmentation
• Bone augmentation can be used to preserve alveolar dimension following tooth extraction