
Local Security Management Policy & Procedures · Local Security Management Policy & Procedures ......
62
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 1 Local Security Management Policy & Procedures (Includes guidance on dealing with Abuse, Bomb Threats, Siege Situations, Suspect Packages, Violence and Aggression.) First issued by / date Issue version Purpose of Issue/Description of Change Planned Review Date Wirral CT October 2011 1 To ensure the protection of life and property. For further information about any aspect of this policy please contact the Local Security Management Specialist. Contact details can be found on page 12 November 2012 Named Responsible Officer: Approved by: Date: Local Security Management Specialist Quality & Governance Committee Policy File: Impact Assessment screening completed September 2011 Full Impact Assessment Not Required N o HS18 Key Performance Indicators: 1. This policy and procedures will be readily accessible to all members of Wirral Community NHS Trust. It will be included on the Trust intranet and hard copies available at any base where staff do not have access to the intranet. 2. Evidence that the security policy and procedures has been adopted by all employees will be examined and recorded in the schedule of annual security reviews of premises and the annual security report. This will be monitored through the quality and timeliness of incident reporting across the trust and evidence that breaches of security do not go undetected.
-
Upload
phungkhanh -
Category
Documents
-
view
218 -
download
1
Transcript of Local Security Management Policy & Procedures · Local Security Management Policy & Procedures ......
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 1
Local Security Management Policy & Procedures
(Includes guidance on dealing with Abuse, Bomb Threats,
Siege Situations, Suspect Packages, Violence and Aggression.)
First issued
by / date
Issue version
Purpose of Issue/Description of Change
Planned Review
Date
Wirral
CT October
2011
1
To ensure the protection of life and property. For further information about any aspect of this policy please contact the Local Security Management Specialist. Contact details can be found on page 12
November
2012
Named Responsible Officer:
Approved by:
Date:
Local Security Management Specialist
Quality & Governance
Committee
Policy File: Impact Assessment screening completed
September 2011 Full Impact Assessment
Not Required
No
HS18
Key Performance Indicators:
1. This policy and procedures will be readily accessible to all members of Wirral Community NHS Trust. It will be included on the Trust intranet and hard copies available at any base where staff do not have access to the intranet.
2. Evidence that the security policy and procedures has been adopted by all employees
will be examined and recorded in the schedule of annual security reviews of premises and the annual security report. This will be monitored through the quality and timeliness of incident reporting across the trust and evidence that breaches of security do not go undetected.

Local Security Management
Policy and Procedures
TABLE OF CONTENTS
PART 1
LOCAL SECURITY MANAGEMENT POLICY Page
1. INTRODUCTION 9 1.1. Commitment to a safe and secure environment 9 1.2. Complies with Human Rights Act 1998 9 1.3. Secretary of State Directions 2003 and 2004 9 1.4. Future changes may supersede policy 9 1.5. Promoting and developing a secure environment 9 1.6. All Trust employees have a responsibility for security 9 1.7. Document sets out framework for managing security 9 2. STRATEGIC OBJECTIVES 9
2.1. Personal safety of staff, patients and visitors 9 2.2. Protection of NHS property and Assets 9 2.3 Safe environment for delivery of healthcare 9 2.4. Working in partnership with local agencies 9 2.5. Appropriate action when security is breached 10 2.6 Commensurate with Major Incident Policy 10 2.7. Security breaches to be reported 10 2.8. Security of drugs, prescriptions and hazardous materials 10 2.9. Describe Remit of NHS Protect 10 2.10. Security of information 10 3. THE ROLE OF NHS PROTECT 10 3.1. Secretary of State Directions 2003 10 3.2. Aim of Secretary of State Directions 10 3.3. National policy and operational control 10
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 2

3.4. Area Security Management Specialist 10 4. RESPONSIBILITIES 10 4.1. Chief Executive 10 4.2. Security Management Director 11 4.3. Directors 11 4.4. Heads of Service 11 4.5. Managers 11 4.6. Local Security Management Specialist 12 4.7. Health and Safety Advisor 14 4.8. Employee 14 5. NHS SECURITY MANAGEMENT MANUAL 15 5.1. Reference tool for LSMS 15 5.2. Retained and maintained by the LSMS 15 6. TRAINING 15 6.1. Incorporate good security working practices 15 6.2. Conflict resolution training 15 7. INCIDENT REPORTING 15 7.1. All security incidents to be reported 15 7.2. Reports of criminal matters to the police 15
PART II
LOCAL SECURITY MANAGEMENT PROCEDURES
8. ACCESS CONTROL 17 8.1. Purpose of access control measures 17 8.2. Restricted access to specified areas 17 8.3 Staff to wear ID badges 17 8.4. It’s the badge that matters 17 8.5. Staff responsibility 17 8.6. Tailgating 17 8.7. Ensure doors remain secure 17 8.8. Request unauthorised persons to leave 17 8.9. Summoning assistance 17 8.10. Reporting suspicious behaviour 17 8.11. Reporting faulty access doors 17 8.12. Contractors and visitors should wear badge 17
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 3

8.13. Car parking 17 8.14. No liability for damage or theft 18 9. BOMB THREATS AND SUSPECT PACKAGES 18 9.1. To be used in conjunction with Major Incident Plan 18 9.2. Types of bombs 18 9.3. General guidelines – bomb and suspect packages 18 9.4. Postal bombs and suspect packages 20 9.5. Dealing with telephone warnings of a bomb threat 21 9.6. Internal procedures – dealing with telephone warnings 22 10. CCTV 23 10.1. CCTV Code of Practice 23 10.2. Request for copy or to view CCTV in writing to LSMS 23 10.3. Except if relevant to police investigation of recent crime 23 10.4. Approval of Security Management Director required 23 11. CONFLICT RESOLUTION TRAINING 23 11.1. All frontline staff to receive training 23 11.2. Ten objectives for Conflict Resolution Training 24 11.3. Copy of training handbook on intranet 24 11.4. Refresher training every three years 24 12. GENERAL SECURITY - NHS PROPERTY 24 12.1. Public access 24 12.2. Good lighting and constant supervision 24 12.3. Premises should be checked regularly 25 12.4. Securing premises out of hours 25 12.5. Alarms sounding 25 13. GENERAL SECURITY - PERSONAL EFFECTS 25 13.1 Cash and personal belongings should not be in excess 25 13.2. PCT not responsible for loss of personal property 25 13.3. Staff encouraged to report loss 25 13.4. Advisability of insuring personal property 25 13.5. Advice can be sought from LSMS 25 14. GOOD HOUSEKEEPING PRACTICES 26 14.1. Reduce opportunities 26
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 4
14.2. Senior staff responsibility 26 14.3. Reporting of security incidents 26 14.4. Register of assets 26 14.5. Service Heads responsible for ensuring register up to date 26 14.6. Equipment to be included in register 26 14.7. Equipment checks at least once a year 26 14.8. Lost equipment to be reported 26 14.9. Any damage to equipment to be reported 26 14.10 NHS equipment not to be used for purpose other than intended 26 14.11 Responsibility for security management rest with Service Heads 26 14.12. Staff responsibility 27 14.13 Staff expected to co-operate in any enquiry 27 14.14. Refer to Accident/Incident reporting policy for further advice 27 15. IDENTIFICATION BADGES 27 15.1. Must be worn at all times when conducting duties 27 15.2. Remove from view when off duty 27 15.3. Only identification badges issued and approved 27 15.4. Details of missing identity badges to be reported 27 16. IMPERSONATION 27 16.1. To follow pathway @ Appendix ‘C’ 27 17. INFORMATION SECURITY 27 17.1. Identifiable information should remain secure at all times 27 17.2. Maintaining security 28 17.3. Compliance with Data Protection Act 28 17.4. Electronic access systems 28 17.5. Access to data 28 17.6. Requires approval of Security Management Director 28 17.7. Police requests 28 18. LOCKDOWN PROCEDURES 28 18.1. Lockdown can be total or partial 28 18.2. Five possible actions 28 18.3. Definition of lockdown 29 18.4. Definition of partial lockdown 29 18.5. Lockdown activation 29 18.6. Lockdown deployment 30 18.7. Lockdown maintenance 30 18.8. Lockdown stand-down 30 18.9. External stakeholders 31
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 5

18.10. Mutual aid 31 18.11. Manual lockdown 31 19. MEMORANDUM OF UNDERSTANDING 31 19.1. Guidelines published by the Department of Health 31 19.2. Patient safety incident resulting in unexpected death 31 19.3. Areas covered 31 20. REPORTING AND RECORDING 32 20.1 Staff encouraged to report anything suspicious 32 20.2. Use of Accident / Incident reporting procedures 32 20.3. Action upon discovering a breach of security 32 20.4. National incident reporting system for assaults on NHS staff 32 20.5. Contact police 32 20.6 LSMS to be informed 33 20.7. Staff should not put own safety or that of others in danger 33 21. SECURITY ALERTS 33 21.1. Security alerts received from NHS Protect 33 22. SIEGE OR HOSTAGE SITUATION 33 22.1. Definition of a hostage situation 33 22.2. Contacting the police 34 22.3. Primary action 34 22.4. Secondary action 35 22.5 Ancillary action 36 22.6. Post incident management and review 36 22.7. Guidance for staff – siege or hostage situation 36 22.8. Profile of the hostage taker 37 23. STAFF AWARENESS 37 23.1. Importance of training 37 23.2. All staff should be aware 37 23.3. Employee duty of care 37 24. VIOLENCE AND AGGRESSION 38 24.1 Commitment to tackling violence 38 24.2. Physical assaults 38 24.3. Non-physical assaults 38 24.4 Verbal warnings 40
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 6

24.5. Assaults by Service user/patient 42 24.6. Secondary prevention 42 25. OTHER POLICIES & GUIDANCE 44
PART III
QUICK REFERENCE QUIDE Appendix ‘A DEALING WITH A SUSPECT PACKAGE 46 Appendix ‘B’ CHECK LIST WHEN RECEIVING BOMB THREAT 47 - 50 Appendix ‘C IMPERSONATION / SUSPICIOUS INDIVIDUALS 51 Appendix ‘D GUIDANCE ON LOCKDOWN PROCEDURES 52 - 53 Appendix ‘E SIEGE SITUATION - INITIAL ACTION 54 Appendix ‘F EXAMPLE OF BEHAVIOUR AGREEMENT 55 Appendix ‘G WARNING LETTER TEMPLATE 56 Appendix ‘H PREVENTION AND MANAGEMENT OF VIOLENCE ASSESSMENT TOOL 57 Appendix MANAGEMENT OF VIOLENT/ABUSE INCIDENT 61
’
’
’
’
’
’
’
’J’
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 7

Local Security Management Policy and Procedures
PART I
Security Policy
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 8
1. INTRODUCTION 1.1. Wirral Community NHS Trust is committed to promoting and improving a safe
and secure environment for those who work in or use the NHS so that the highest standards of clinical care can be made available to patients.
1.2. The Trust also aims to ensure that its policies will be compliant with the Human
Rights Act 1998. 1.3. This policy is based on current directions from the Secretary of State for Health
which is as follows:-
Secretary of State Directions to NHS Bodies on work to tackle violence against staff and professionals who work or provide services to the NHS on 20th November 2003.
Secretary of State Directions to NHS Bodies on Security Management
Measures on 24th March 2004.
1.4. Any future changes to the above directions may supersede this policy. 1.5. Senior Managers of the Trust should take a leading role in promoting and
developing a secure environment. 1.6. All Trust employees have a responsibility to ensure that security procedures are
observed at all times. 1.7. This document sets out the framework for managing security within Wirral
Community NHS Trust and will be underpinned by the procedures outlined in part II of this document.
2. STRATEGIC OBJECTIVES
The primary aims of this Policy are: 2.1. The personal safety at all times of staff, patients and visitors as well as other
employers and contractors. 2.2. Protection of NHS property and assets against theft and damage. 2.3. To ensure a safe environment in which the uninterrupted delivery of quality
health care can be provided. 2.4. To work in partnership with local agencies; e.g. police and local authority, for a
safe and secure environment.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 9
2.5. Ensure that appropriate action is taken when security and the contents of this
policy are breached. 2.6. Ensure that in the event of a security incident escalating, any action taken is
commensurate with action required to be taken in accordance with the Major Incident Plan and NHS Protect guidance on lockdown procedures.
2.7. Ensure that breaches of security are reported in accordance with the Incident
Reporting Policy. 2.8. Ensure security of drugs, prescription forms and hazardous materials. 2.9. To describe the remit of NHS Protect and the Local Security Management
Specialist (LSMS) for Security Management within the NHS. 2.10. To ensure the security of all personal information in accordance with the Data
Protection Act. 3. THE ROLE OF NHS PROTECT 3.1. In 2003, the Secretary of State for Health issued directions to the NHS for the
management of security. This created the NHS Counter Fraud and Security Management Service now referred to as NHS Protect and replaces work previously undertaken under the NHS Zero Tolerance campaign.
3.2. The aim of the directions and the campaign, “protecting your NHS Initiative” that
followed is to improve security management within the NHS with particular emphasis on tackling violence against members of the NHS.
3.3. NHS Protect is a division of the NHS Business Services Authority, and is
responsible for national policy and operational control for the management of security within the whole of the NHS structure.
3.4. NHS Protect has allocated an Area Security Management Specialist (ASMS) to
each strategic health authority region to act as a link between NHS Protect and Local NHS Security Management. The ASMS for this region is Gary Blackhurst, telephone number: 07917077589.
4. RESPONSIBILITIES 4.1. Chief Executive 4.1.1. The Chief Executive has the overall responsibility for all matters of
security.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 10

4.2. Security Management Director 4.2.1. The Trust Board member with responsibility for security will be the Director of
Finance and he will keep the Board informed of the major developments on security related issues.
4.3. Directors 4.3.1. It is the responsibility of the Directors to: (i) Disseminate this policy within the area of their responsibility.
(ii) Ensure the implementation of the strategy within the area of their responsibility by providing support and advice to their managers.
(iii) Co-ordinating security issues with other employers who share premises with
Wirral Community NHS Trust. 4.4. Heads of Service
4.4.1. Service Heads need to assess the impact of security within their department. 4.4.2. Ensuring risk assessments are completed within their service area. 4.4.3. Developing local arrangements to reduce the risks.
4.4.4. Ensuring processes are in place to deal with any emergency situation.
4.4.5. Implementing any necessary remedial action identified by incidents, audits or
inspections.
4.4.6. Liaising with controllers of premises where Wirral Community NHS Trust staff are based to ensure their safety in those premises
4.4.7. Ensure that future job descriptions for all managers include, as part of their
duties, the responsibility for security within their department. 4.5. Managers’ Responsibilities 4.5.1 All managers carry a responsibility for security. It is their job to see that the right
policies, procedures and systems are in place in their local areas and that such policies are kept under constant review. They need to carry out risk assessments and ensure staff receive relevant instruction and training.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 11

4.5.2 It is the individual managers’ responsibility to see that safe and secure environments are maintained and that all incidents are fully reported and that action is taken when necessary.
4.5.3 Managers should implement a procedure to record details i.e; make,
model, serial number etc. of valuable or important property within their department/directorate. The Local Security Management Specialist can advise on methods to secure property.
4.5.4 Managers should ensure that arrangements are made to secure the
department/directorate out of working hours together with the safe custody of keys.
4.5.5 Ensure the setting of any security alarm or device to protect the property out of
hours.
4.5.6 Ensure records are kept of all keys issued to staff in their department/directorate and reporting of all losses of keys to the Security Manager.
4.5.7 Seek advice from the Security Manager to ensure that security is maintained
within their Department/Directorate. 4.5.8 Advise the Security Manager of any changes within their department/directorate
that may adversely affect the security of premises. 4.5.9 Ensure all staff employed within the NHS environment have an identification
badge and when appropriate wear them. 4.5.10 Ensure that all staff are made aware of this strategy and understand its content and their responsibilities.
4.6. LOCAL SECURITY MANAGEMENT SPECIALIST 4.6.1. Locally, each NHS organisation is required under Secretary of State Directions to
have access to an accredited Local Security Management Specialist (LSMS).
4.6.2. The role of the LSMS is to implement at a local level, the national policy for Security Management, and to work proactively and reactively with their NHS employers to ensure that staff are supported on Security Management issues and thereby reduce risks.
4.6.3. The LSMS has to undergo training, provided by NHS Protect, and achieve a level
of accreditation.
4.6.4. Your Local Security Management Specialist is:
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 12

Philip Davies
Office telephone number: 0151 514 2888 Ext 1492 Mobile telephone number: 07717766162
Email Address: [email protected]
4.6.5. Under a service level agreement with Wirral NHS Primary Care Trust until April
2013, the LSMS will also provide support for the management of security to all who work in NHS Primary Care in the Wirral area.
4.6.6. The overall objective of the LSMS is to “work on behalf of the local NHS to
deliver an environment that is safe and secure so that the highest standards of clinical care can be delivered to patients.” This objective will be achieved by working in close partnership with staff, patients, their carers, NHS Protect and other stakeholders. The LSMS will aim to provide a comprehensive, inclusive and professional security management service for their NHS organisation, including independent contractors, and work towards the creation of a pro-security culture within the NHS.
4.6.7. A summary of the key objectives of the LSMS are:
To comply with and implement the Secretary of State’s Directions for Security Management in the NHS
To become an accredited LSMS as assessed by NHS Protect and maintain this accreditation
To ensure that all NHS Security Management work is carried out within a professional and ethical framework as provided by NHS Protect
Ensure that all relevant stakeholders are involved in Security Management in the local NHS
To report to the Local Security Management Director on security management work locally
To ensure that strong links are maintained with NHS Protect and the ASMS
To lead on day to day work locally to tackle violence, harassment and abuse against NHS Staff, patients and carers, in accordance with the national framework
To maintain appropriate links with the local risk management process To take steps to promote a pro-security culture at a local level To ensure that security incidents/breaches are investigated, appropriate
actions taken and to publicise the outcome, where appropriate, in accordance with guidelines issued by NHS Protect
To ensure that lessons are learnt from security incidents/breaches and preventative measures introduced to eliminate future occurrences, where possible.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 13

To encourage the reporting of security incidents/breaches, investigate these reports, assess risks, and implement preventative measures
To act professionally at all times, ensuring that a fair, objective and professional approach is taken at all times
To work towards applying a range of sanctions against those responsible for security incidents/breaches, being aware of the law as it applies to each incident/breach
To provide advice regarding the physical security of premises, proposed new premises, alterations to premises and assets
To maintain records of annual risk assessments showing action plans that are in place and changes that have been implemented
To work with the Local NHS and the National Legal Protection Unit to ensure that appropriate redress is sought against those who commit security incidents/breaches, including redress when a loss of resources has occurred
Ensure relevant information about potential security risks is circulated and all relevant staff alerted to the risk.
4.6.8. The LSMS will additionally submit an annual security management report and
plan to the Security Management Director and NHS Protect identifying the process and work programme for security management in the local NHS for each year.
4.7. Health and Safety Advisor 4.7.1. The Trust Health and Safety Advisor and Local security Management Specialist
work closely together on violence and security issues. They will provide assistance to managers undertaking violence at work risk assessments and report to the Health and Safety Committee on the implementation of risk assessments by directorates.
4.8. Responsibilities of the Employee 4.8.1. Employees are expected to co-operate with management to achieve the aims,
objectives and principles of the security strategy. Great emphasis is placed on the importance of co-operation of all staff in observing security and combating crime.
4.8.2. Staff should be aware of their responsibilities in protecting at all times, the
assets/property of patients, visitors and Wirral Community NHS Trust. Where specific security procedures exist, staff must abide by them at all times. When staff know or suspect a breach of security, they must report it immediately to their manager or the Local Security Management Specialist.
4.8.3. All staff are reminded that it is an offence to remove property belonging to Wirral
Community NHS Trust without written authority. Failure to seek authority from
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 14
their line manager could result in disciplinary action or criminal proceedings being taken.
4.8.4. Staff are responsible at all times, for the protection and safe keeping of their
private property. The Local Security Management Specialist will if requested, advise staff on the security of their property. Any loss of private property must be reported without delay. If private property has been stolen, then it is the owner’s responsibility to contact the police.
4.8.5. Wirral Community NHS Trust will not accept liability for the loss of, or damage to
private property. 4.8.6. All staff, official visitors and contractors working on behalf of Wirral Community
NHS Trust are required to wear an approved security identification badge at all times unless medical or operational situations prevent this being possible.
5. NHS SECURITY MANAGEMENT MANUAL 5.1. NHS Protect provides a National NHS Security Manual to be implemented across
the NHS as a whole. This manual is a generic manual that will be used as a reference tool by the LSMS in the performance of their role at a local level. It aims to support the LSMS in the reactive and proactive elements of their role and whenever appropriate, sections will be shared with staff. Sections of the NHS Security Manual have been referred to in this policy. The manual is a living document that will be updated and refined as Security Management initiatives are introduced and improved.
5.2. The manual will be retained, maintained and updated by the LSMS. 6. TRAINING 6.1. All departments must incorporate good security working practices. Wirral
Community NHS Trust recognises the need for effective training of staff likely to deal with security related issues.
6.2. Conflict Resolution Training is available to all staff and further advice and details of training can be obtained from the Local Security Management Specialist.
7. INCIDENT REPORTING 7.1. Any security incident whether actual or perceived should be immediately be
brought to the attention of a manager and recorded upon an accident/incident report. (For further information about accident/incident reporting please refer to policy reference GP8).
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 15

7.2. Reports of theft and other criminal activity should also be made to the police and a police crime/incident reference number obtained.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 16

Local Security Management Policy and Procedures
PART II
Local security Management Procedures
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 17
8. ACCESS CONTROL 8.1. Ideally access control measures that we use, and have confidence in, can help
deter and prevent security related incidents. 8.2. They are designed to ensure that members of staff, patients and public only have
access to areas they need to enter to do their job, obtain treatment or make enquiries.
8.3. Staff should wear identification badges, especially in secure areas. 8.4. Do not think that an NHS lanyard is good enough identification. It’s the badge
that matters. 8.5. Staff should not lend access cards to others or wedge doors open and to be
aware of the possibility of ‘tailgating.’ 8.6. Tailgating is simply the act of following a person through an access controlled
door after they have opened it using their access control card, key or by using a code controlled key pad.
8.7. If necessary staff should pause for a moment and secure doors behind them. 8.8. Anyone present on our sites without due reason should be requested to leave,
having in mind own personal safety when doing so. On some sites assistance will be available, via on site security, to remove unauthorised individuals who are causing a nuisance and/or damage to those sites.
8.9. If unauthorised visitors refuse to leave then staff should take the most
appropriate action, in a safe manner, to remove and/or summon assistance from security, porters, other members of staff, or the police as most appropriate in the circumstances.
8.10. Suspicious behaviour or unauthorised access to restricted or patient treatment
areas should be reported to the manager of that area and an incident report completed.
8.11. Faulty access doors must be reported immediately. 8.12. All contractors and visitors requiring access to restricted areas of NHS premises
should where possible be issued with identification badges that clearly show them as being authorised to access the relevant area. Local procedures will be in place that allows this procedure to be implemented.
8.13. Car Parking: NHS premises are private and there is no right of way. Car parking
is allowed in specified areas and access is conditional on the owners or drivers of
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 18

vehicles observing whatever safety regulations Wirral Community NHS Trust make to ensure the orderly flow of traffic, safety and security of all concerned.
8.14. The NHS accepts no responsibility for damage to or theft of vehicles whilst on
NHS premises. 9. BOMB THREATS AND SUSPECT PACKAGES
(NB: In the event of an emergency; staff should refer to the quick reference guides at Appendix A, B and C).
9.1.1. This procedure is to support staff should there be a bomb threat or a suspect
package (including possible chemical agents). Please note that this section is designed to be used (when appropriate) in conjunction with the Trust’s Major Incident Plan.
9.1.2. While the risk of an individual being caught up in a bomb related incident is low,
bomb threats, be they real or hoax, could cause a great deal of disruption to the NHS.
9.1.3. The priority is to ensure that any such incident is managed effectively so that staff
and visitors are not put at risk and to minimise the impact on the core business of Wirral Community NHS Trust.
9.2. Types of bombs: 9.2.1. It is important to be aware that bombs can easily be disguised to look like
everyday objects. It might not therefore always be possible to recognise a bomb from its outward appearance. Some examples are:
9.2.2. Letter and Parcel Bombs sent through the mail. They will generally contain
only a small amount of explosives. 9.2.3. Anti-personnel bombs for indiscriminate attacks on people, the aim
being to kill or maim as many as possible. These can be nails or other jagged metal having a shrapnel effect.
9.2.4. Anti-property for damaging buildings, especially dangerous in
modern high rise buildings. They vary in size from a few kilograms to 200 kilograms or more.
9.2.5. Incendiaries can be simple devices such as petrol bombs or more
sophisticated including highly flammable and long burning materials.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 19

9.3. General Guidelines - Bomb Threats and Suspect packages 9.3.1. A bomb or incendiary device is easily disguised, and is designed to cause
damage by blast or fire. They can be concealed in a briefcase, handbag and flask or in the case of incendiary devices, in a cigarette pack, cassette tape or similar container. Litterbins and toilets have been favoured for depositing devices in the past. In recent times we have also seen the effects of suicide car bombers.
9.3.2. Report to a manager or head of service any object/person you see which you
consider suspicious. Don’t hesitate or think twice about it. No one will criticise you for a false alarm. (Please use quick reference guide at Appendix ‘A’ ).
9.3.3. Do not touch or attempt to move a suspicious item. 9.3.4. Notify the police and switchboard immediately, giving your name, job title, your
exact location and contact telephone number. 9.3.5. When calling the switchboard please remember to express the seriousness of
the incident and the reason for calling and that action by a Director is needed immediately. The Director will consider implementing the major incident plan, as necessary.
9.3.6. The rota for the on-call Director is held at Arrowe Park Hospital
switchboard, telephone number: 0151 678 5111. 9.3.7. Once the main switchboard has been contacted, consider if it is
appropriate to contact the Communications Department who can assist in alerting as many members of staff as possible, for example:
Ali Hughes, Head of Communications, Marketing and Corporate Affairs, Email: [email protected], Tel: ext. 1440/0151 651 3905
Jane Loughran, Senior Communications and Marketing Manager, Email: [email protected], Tel: ext. 1520/0151 514 2311
Amy Sclater, Communications and Marketing Officer, Email: [email protected], Tel: ext. 1611/0151 651 3961.
9.3.8. Remain at a safe distance from the object and keep others away. Turn off
radios/mobile phones within close proximity of the bomb or suspect package. 9.3.9. The police and bomb disposal will want to talk to you so make yourself known to
the Emergency Services. Your first hand account of what you have seen is essential.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 20

9.3.10.After a safe evacuation procedure from the premises, please ensure that all staff, contractors and visitors remain outside of the premises and a sufficient distance away from the building concerned. A minimum distance is 100 metres from the location of the incident but this will also depend upon police advice and other information available at the time of the event. Please be aware that fire evacuation assembly points may be too close to the property in question. In the case of a lorry or a large van the police may set up a cordon 1000M away.
9.3.11.A check of all personnel should be conducted by managers or senior member of
staff present to ensure that everyone has evacuated the premises. 9.3.12 Staff should not go to their cars nor remove their cars from the car park; this will
take too much time and will lead to confusion. 9.3.13.Do not let anyone re-enter the building until instructed that the building is safe.
9.3.14.Consider the impact on the neighbouring properties and the need to inform them
that a bomb threat has been received; they may then need to instigate an emergency evacuation from their property. The priority is the safety of staff and public and to minimise the risk of injury.
9.3.15.If you notice a package, about which you are suspicious, consider the relevant
risk to both staff and patients within the premises and similar actions to those listed above in this section. If you have a serious concern about a package then, do not touch it and instigate the emergency evacuation procedure. Do not use mobile phones, personal radios or similar electrical devices in close vicinity of such suspect devices.
9.3.16.The person receiving the notification of a bomb, or similar alert, is the key to
dealing with the incident and will be a key liaison for the police and LSMS with whom to make contact with. The details of the threat received, and its accuracy, are key to dealing with the threat. Copies of plans/drawings for each site should be kept in the Major Incident Plan cupboard.
9.3.17.A decision to re-occupy the building should only be taken once instructed to do
so by the Police. 9.4. Postal Bombs – Possible signs and appropriate action to be taken. 9.4.1. Any one of the following signs should alert members of staff to the possibility that
a letter or package may contain an explosive device.
Grease marks on the envelope or wrapping Unusual odour such as marzipan or machine oil
Visible wiring or tin foil, especially if package is damaged Envelope or package may feel heavy for its size
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 21

Weight distribution may be uneven Contents may be rigid inside a flexible envelope May have been delivered by hand from unknown source If a package, it may have excessive wrapping There may be poor handwriting, spelling or typing It may be wrongfully addressed or from an unexpected source There may be too many stamps for the weight of the package
9.4.2. Initial action for dealing with a package that may contain an explosive
device:
Put down gently and walk away from it Evacuate the immediate area and raise the alarm
(Immediate area may mean a room, department or building and will depend upon the size and type of building)
Inform the police via the 999 system Inform your manager Prevent anyone from re-entering the premises. Do not place the package into anything (e.g. water) or place anything on top
of it Do not tamper with or open the package Make a description of the article and its location within the room (e.g. size,
shape, lettering on it) Establish if possible, whether the person to whom the package is addressed
is expecting the package Complete Trust Incident Report Form and forward a copy to the Local
Security Management Specialist. 9.5. Dealing with telephone warnings of a bomb threat 9.5.1. Historically it is switchboard operators who most frequently receive telephone
bomb warnings, but any member of staff with a direct dial facility might also receive a threat.
9.5.2. Terrorists often issue telephone warnings to organisations that would not be
affected by the explosions (i.e. a third party). However, in all cases telephone the police immediately via 999 system with as much information as possible.
9.5.3. A checklist is provided at appendix ‘B st in gathering evidence. This
form should be displayed prominently to reception staff and completed upon receipt of a bomb threat.
9.5.4. There are four key rules:
Keep calm
’, to assi
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 22

Obtain as much information as possible for the caller – make notes
Keep the line open even after the caller has hung up Report the call to the police and your manager/head of service.
9.5.5. If you receive a threat about a bomb at an alternative address then you should:
Contact the police immediately, by dialling 999, and inform them clearly and concisely, of the information you have received, use the checklist at Appe i
Attempt to get in touch with the premises to which the threat has been made
in order for them to instigate their evacuation procedure
Contact the LSMS or a Director of the Community Trust to inform them of the threat you have received and the actions you have taken
9.5.6. It is advised that service heads bring details of this policy to the attention of their
staff and that copies be kept within key staff areas within their
nd x ‘B’
service function. Additionally it is advised that all receptionist staff within the primary care trust will receive a direct copy of this procedure, which should be kept by them, at all times, within their work area. Any new receptionist staff, including bank staff, should receive a copy of this procedure, from their manager, at the commencement of their employment at the primary care trust.
9.6. Internal Procedures - Dealing with telephone warnings of a bomb threat 9.6.1. Member of staff receiving call should notify:
Police 999 Manager / Head of Services Executive Director on call Start log of events (e.g. time calls received)
9.6.2. Role of the Senior Nurse / Manager on call:
Make a quick survey and if necessary arrange evacuation to a safe area Supervise at scene until help arrives In the event of an explosion, survey casualties, arrange call out of doctors,
additional nurses Identify the casualties Liaise with the Executive Director and collate information
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 23

9.6.3. Chief Executive/Executive Director:
Put on stand by or activate the Trust’s Major Incident Plan depending on a threat or explosion.
Take charge and control log of events Liaise with Senior Manager at the scene. Ensure that the Communication lead is briefed on developments Consider if need to make the Strategic Health Authority and NHS Protect are
aware of the threat/incident. Ensure that other health services are put onto alert i.e. Accident and
Emergency and local GP practices. Provide local knowledge of the site to the other emergency services.
10 CCTV 10.1. Wirral Community NHS Trust has external and internal cameras designed to
to safeguard staff, patients, and visitors. To regulate the use of cameras, Wirral Community NHS Trust operates to a CCTV Code of Practice made in accordance with the Data Protection Act. A copy of this guidance can be obtained from the Local Security Management Specialist.
10.2. CCTV recordings are strictly confidential and held solely for the purpose of
detecting or preventing crime or to assist with improving safety. All requests to view or obtain copies of CCTV footage must be made in writing to the Local Security Management Specialist for investigation outlining reasons for request.
10.3. The only exception to this rule is that a police office may view CCTV recordings that are relevant to the investigation of a recent crime.
10.4. All requests will be forwarded to the Security Management Director for approval.
11. CONFLICT RESOLUTION TRAINING (CRT) 11.1. It is a requirement that all “frontline” NHS staff receive Conflict Resolution
Training. Managers should ensure that all staff, deemed to be “frontline” have access to this training as advertised in the KSF development prospectus. This training should be seen as core training for “frontline” staff. Frontline staff is defined as “any member of staff who in the course of their duties comes into contact with the public”. This will include staff providing clinical care to patients, receptionist staff, anyone who gives public talks or attends public events or has course to speak to the public over the telephone. This list is not exhaustive and it is anticipated that most staff will be deemed to be “frontline” at some point in the performance of their duties. It is therefore anticipated that most staff employed by Wirral Community NHS Trust will be expected to have attended Conflict Resolution Training,
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 24
11.2. A national syllabus for Conflict Resolution Training (CRT) has been devised by the CFSMS and agreed to by the member staff side organisation representing NHS staff. This training must include the 10 objectives from the national guidance, which are for delegates to be able to:
Describe common causes of conflict Describe two forms of communication Give examples of how communication can break down Explain three examples of communication models that can assist in conflict
resolution Describe patterns of behaviour they may encounter during different
interactions Explain the different warning and danger signs Give examples of impact factors Describe the use of distance when dealing with conflict Explain the use of reasonable force as it applies to conflict resolution Describe different methods for dealing with possible conflict situations.
11.3. A copy of the training handbook is held on the intranet. 11.4. Once a frontline member of staff has received initial one day training they will be
eligible to attend refresher training once every three years. 12. GENERAL SECURITY - NHS PROPERTY 12.1. It is advised that all NHS premises should remain as secure as possible at all
times, and allow public access to authorised areas only for the purposes of receiving healthcare. The public should not have access to staff only areas and managers should take appropriate measures to ensure that this principle is complied with. Ideally, entrances to restricted areas should display appropriate signs. For example: ‘STAFF ONLY’ or ‘AUTHORISED PERSONS ONLY.’
12.2. Public areas should have a minimum of concealed places; such areas require
good lighting and to be constantly supervised. 12.3. Premises should be regularly checked during the working day and thoroughly
checked prior to closing. All doors and windows should be secured. 12.4. During normal “out of hours” period it is expected that NHS premises will be
alarmed and be locked in accordance with the local security policy in place for those premises. It is also expected that equipment and other assets of the NHS are made appropriately secure, when not in use by NHS staff.
12.5. Across all sites except Riverside and Port Causeway any issues with regards to
alarms sounding will be attended by the external contractor employed to respond. The contact details to respond to any alarms that sound are:
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 25

Arrowe Security, Telephone number: 0151 609 0909.
Separate arrangements are in place for Riverside, Port Causeway and the annexe building known as the White House. In the event of an alarm sounding at these premises, the organisation to contact is: MPS, Telephone number: 07721 539 352.
13. GENERAL SECURITY - PERSONAL EFFECTS 13.1. Within all areas of the NHS, staff are advised against bringing cash or personal
belongings, in excess of their personal daily needs, whilst on duty, and that any cash and personal belongings should where possible remain with the individual at all times. If this is not possible then it is advised that all personal belongings and cash should be stored in an appropriately secure area, within the work place.
13.2. Wirral Community NHS Trust will not be responsible for loss of personal property,
cash and belongings. Each service area is expected to take the most appropriate measures possible to ensure that work areas remain as secure as possible and that appropriate storage facilities are provided to staff.
13.3. Although the Primary Care Trust accepts no responsibility for the loss of personal
belongings, staff are encouraged to report any loss of their property and co-operate in any enquiry which may result in connection with the loss.
13.4. Service heads are encouraged to remind staff of the advisability of insuring
personal property and that the NHS accepts no responsibility for its loss. 13.5. As with all security related issues the advice of the LSMS can be sought on
appropriate security measures to be implemented within specific work areas to ensure the protection of personal belongings.
14. GOOD HOUSEKEEPING PRACTICES 14.1. Managers should encourage good housekeeping both inside and outside
premises belonging to Wirral Community NHS Trust. This will reduce the opportunity for breaches of security to go undetected.
14.2. Senior staff, in all disciplines have a responsibility to apply appropriate routine
security practices in relation to NHS property and assets. 14.3. Breaches of agreed security practices must be brought to the notice of the LSMS
and reported in accordance with the Incident Reporting Policy.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 26

14.4. Registers shall be maintained of assets/equipment used within each service area.
14.5. The Service Head is responsible for ensuring that the register is updated on a
regular basis and that regular audits of assets/equipment registers are undertaken. The responsible person should be clearly identified on the register.
14.6. Evidence that such actions are undertaken should be made available to the
LSMS or the Community Trust auditors on request. The type of equipment included in the register shall be that which is attractive in terms of personal usage, portable and potentially vulnerable to misappropriation. Wherever practicable equipment should be permanently security marked and contain a unique asset identifier.
14.7. Managers responsible for equipment shall carry out a check of all items at least
once per year. This should be carried out by the end of February. Any discrepancies shall be notified in writing to the Director of Finance and LSMS who may also undertake such other independent checks as considered necessary.
14.8. If at any time assets/equipment are known to be lost or misplaced then this
should be reported, via an incident report, and notified to the LSMS. 14.9. Additionally any damage to the assets/equipment should also be reported using
an incident form. 14.10. Service Heads are responsible for ensuring that staff do not use NHS
assets/equipment for purposes other than their intended use. NHS assets exist for the benefit of the NHS and the treatment of patients; they should not be used for personal gain.
14.11. Within each service area, the responsibility for security management rest with the
Service Head. Advice can be sought, at all times, from the LSMS. Good security management, and local security procedures, are the keys to ensuring that we keep the NHS secure and protect staff, patients and carers from adverse incidents.
14.12. Staff, at every level, have a responsibility to take steps to protect assets,
patients, staff, visitors, carers and themselves, to prevent theft, fire, damage and waste and to bring to justice those who offend against the NHS and criminal law. All adverse security incidents, or near misses, should be notified, by staff, to their manager, an incident form and risk assessment completed and reported to the LSMS for investigation, action or advice.
14.13. All staff will be expected to co-operate in any enquiry into incidents particularly
where losses by theft or otherwise, may be anticipated.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 27

14.14. Please refer to the Accident/Incident Reporting Policy (Community Trust
Reference GP8) for further advice. 15. IDENTIFICATION BADGES 15.1. All NHS staff are issued with identification badges, which must be worn at all
times, when conducting their duties as an NHS employee. The identification badge should be in a position on their clothing so that anyone can see the badge and should not be hidden from public view, unless medical or operational situations prevent this being possible.
15.2. When off duty it is advised that NHS staff remove their identification badges from
view, and keep them in a secure place. 15.3. Staff should only display identity badges issued and approved by the NHS. The
use of imitation badges and insignia which has not been assessed by Health and Safety is not permissible.
15.4. Staff must report immediately to their manager any theft or loss of their identity
badge and complete an incident report. Details of a missing identification badge should be circulated so that all members of the trust can be alerted.
16. IMPERSONATION 16.1. If a health professional is advised by a service user that they think they have
been approached/visited by a person who claims to be a health professional, but is thought to be bogus, then the pathway at Appendix should be followed.
17. INFORMATION SECURITY 17.1. Any personal information e.g. patient or staff identifiable information or data,
must remain secure at all times and only be used when it is needed and for the purpose it is being held.
17.2. Any paperwork containing personally identifiable information should be locked away when not in use and any computer systems should contain appropriate security measures to ensure that access is only permitted to those that need to gain access on specific approved grounds. Computer systems should be logged / turned off when not in use for any period of time. Further information in the use and security of “personal information” can be obtained from the relevant Caldicott Guardian, the Information Security Officer within WHIS and/or your LSMS.
17.3. At all times Wirral Community NHS Trust employees must comply with the Data
Protection Act when conducting Trust business.
‘C’
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 28

17.4. During recent years there has been an increasing number of electronic access systems installed which require staff to present a card or fob to a reading device in order to gain access. The majority of these systems identify the card holder and the time of access to a building or area. This information is strictly confidential and held in accordance with the Data Protection Act, solely for the prevention and detection of crime and to ensure safety.
17.5. All requests to view or obtain a copy of access control or CCTV data must be
made in writing to the Local Security Management Specialist outlining the reason(s) for the request.
17.6. Requests will be forwarded to the Security Management Director for approval.
17.7. Staff responsible for maintaining the security of data held on an electronic access system or closed circuit television system must not allow any other person to view the data base unless authorised by the Security Management Director. The only exception is where access is urgently required by a police officer who is investigating a recent crime.
18. LOCKDOWN PROCEDURES 18.1. In the event of pandemic influenza or some other abnormal event, excessive
demand may be suddenly placed upon the normal services that are available. It may become necessary to request a total or partial lockdown of some or all of the trust’s premises.
18.2. This may require:
Enforcement of additional access controls to limit non essential visitors. Closing some facilities. Restricted/controlled access to areas generally open to public visitors. Restricting access to where materials are stored. Restricting visitors to avoid spread of the virus.
18.3. Lockdown: A lockdown is defined by the NHS Security Management Services as the process of controlling the movement and access f people (this includes NHS staff, patients and visitors) around sites or specific buildings/areas in response to an identified risk, threat or hazard.
18.3.1.These buildings will in the main be owned or leased by Wirral Community NHS Trust but in some cases may fall under the control of other organisations such as the Local Authority. In the latter case permission may be required from those organisations concerned.
– both entry and exit o
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 29

18.3.2.A lockdown is achieved through a combination of physical security measures and the deployment of security personnel.
18.3.3. It is important to note that in locking down a trust there are three key elements, that is; preventing the entry, exit and movement of people on a trust site or in a building or part of a building.
18.3.4 In preventing the entry, exit or movement of people, or a combination of the three, the main aim of implementing a lockdown is to either exclude or contain staff, patients and visitors.
18.4. Partial Lockdown: A partial lockdown can be defined in a number of ways. In most instances, a partial lockdown is the locking down of a specific part of a trust site or a specific building or part of a building.
18.4.1.A partial lockdown can also be implemented when entry restrictions are placed on a specific building to control the flow of people into it – via identification checks for example. This is also known as 'controlled access' to a site or building.
18.4.2. On these occasions, the partial lockdown can also be characterised as being ‘static.’ For example; the partial lockdown is sustained at a specific part of a site or building and it remains there.
18.4.3. A decision to implement a partial lockdown will usually be the initial response to an incident. This response will help to ensure that identified critical assets such as personnel and property are protected.
18.5. Lockdown Activation 18.5.1. Following the Major Incident policy the incident commander may call for a partial
or total lockdown of NHS premises within the remit of the trust. 18.6. Lockdown Deployment 18.6.1. Security guards, porters and dedicated staff will be assigned to relevant security duties. 18.6.2.These duties may include guarding specific areas, temporarily securing entrances, affixing additional signs and providing advice and directions to the public.
18.7. Lockdown Maintenance
18.7.1. It is anticipated that some staff will be released from their normal duties to assist
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 30
with dealing with abnormal situations. Estates, and Housekeeping staff will be assigned to designated doors to maintain the lockdown and to give guidance and instruction to those who are attempting either entrance or exit. Printed information will be issued to these staff in order to reduce conflict and confusion. 18.7.2. CCTV and electronic access controls where fitted must be maintained and monitored at all times to provide accurate and up to date reports of all persons on site or attempting to gain access. 18.7.3. Normal porter services will continue to be maintained, staff being assigned to duties on a priority and need basis. 18.7.4. In the event of lockdown all persons entering a building should be in possession of a valid form of identity. 18.7.5. The Head of Capital Projects and Premises must be contacted if additional resources are required. The following is a list of companies who presently provide accredited security patrols and key holder services to this trust: Mitie Security…………………………...Telephone number: 0151 423 5262 Arrowe Security Systems……………..Telephone number: 0151 609 0909 MPS………………………….………….Telephone number: 07721 539 352 Herritage Security……………………...Telephone number: 0151 639 0772
18.8. Lockdown Stand-down
18.8.1. Only the incident control commander is able to instigate the stand-down authority which will be communicated directly to Managers who will verify the instruction before taking any action. 18.8.2. On stand-down all doors and barriers will be removed in an orderly fashion to enable the trust to return to normal services as promptly as possible. Staff will remain on duty until instructed to leave or reassigned to other duties. 18.8.3. A debrief will take place as soon as is practical with those staff who wish to take part. Further debriefs will be communicated using normal trust communication service after the event.
18.9. External stakeholders
18.9.1. Following instruction from the incident commander within the incident control room relevant assistance will be given to the Police, Ambulance and Fire services depending on the priority need. Due consideration will also be given to other stake holders such as County and Local Council Emergency Planning Leads. This again will be communicated from the incident commander under guidance from external incident management remit.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 31

18.10. Mutual Aid
18.10.1. In order to prevent the possibility of individual services such as the walk in centre becoming either contaminated or over-run with casualties, the incident commander may give specific instruction to the lock-down team to concentrate resources to the area to assist and facilitate either temporary or permanent re- location of services.
18.11. Manual Lockdown
18.11.1.Doors which are not able to be locked automatically will have dedicated
staff allocated to each area with the correct keys to physically lockdown the area.
18.11.2. In the event of a manual lockdown, security staff should be fully briefed as to their duties. A briefing sheet is provided at Appendix ‘D’ 19. MEMORANDUM OF UNDERSTANDING – UNEXPECTED DEATH 19.1. The purpose of this protocol is to promote effective working relationships
between the National Health Service (NHS), Association of Chief Police Officers and Health and Safety Executive (HSE). The protocol will take effect in circumstances of unexpected death or serious untoward harm requiring investigation by the police, or the police and the HSE jointly.Guidelines were published by the Department of Health in November 2006 to provide practical and pragmatic advice on the implementation of the Memorandum of Understanding agreed by the NHS with the Health and Safety Executive and the Association of Chief Police Officers.
19.2. The guidelines apply where a patient safety incident has occurred, resulting in
unexpected death or serious untoward harm.
19.3. They cover the following areas:-
When to refer a patient safety incident to the Police and / or HSE.
How to conduct an investigation, including advice on how to preserve and
assess potential evidence and safeguard it.
How to communicate with the Police, HSE, patients, relatives and staff.
The procedure to establish, conduct and manage an Incident Co-ordination Group, including guidance on who should represent an organisation.
Model terms of reference and agenda for the Incident Co-ordination Group, including guidance on the issues that should be considered at the initial meeting.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 32
What information should be shared by the Police and HSE with Trusts.
How to handle communications, including media coverage.
There is no substitute for referring to the Guidelines which can be accessed at: the following internet address:-
://www.dh.gov.uk/PublicationsAndStatistics/Publications/PublicationsPolicyAndGuidance/PublicationsPolicyAndGuidanceArticle/fs/en?CONTENT 20. REPORTING AND RECORDING 20.1. Staff should be encouraged to report anything they consider suspicious to their
line manager or the Local Security Management Specialist. 20.2. All security incidents and near misses must be recorded using the Incident
Reporting System Procedures. 20.3. In the event of discovering that an incident (resulting in a breach of security) has
taken place, staff will take reasonable steps to remedy the situation immediately and must inform their Manager, the LSMS or the appropriate on-call Duty Manager, as soon as reasonably practicable.
20.4. A National NHS Security Incident Reporting System (SIRS) for recording physical
and non physical assaults and the loss or damage of NHS property is operated and coordinated by NHS Protect. The LSMS will be responsible for transferring information from the incident report to the national database.
20.5. If a member of staff sees or suspects that a crime is taking place, they
should (if appropriate) immediately contact the Police via switchboard or direct using 999. Wherever possible the member of staff should keep the situation under surveillance without endangering their own safety or that of others.
20.6. Whenever possible the LSMS should be informed, who will advise of the most
reasonable course of action, as deemed appropriate to the circumstances. 20.7. At no time should a member of staff put their own safety, or that of others, in
danger, and should only attempt to intervene if they believe that their own personal safety is not at risk.
21. SECURITY ALERTS 21.1. NHS Protect will issue Security alerts via the LSMS network when appropriate, to
highlight individuals or circumstances that give cause for concern. The LSMS will distribute such security alerts within Wirral Community NHS Trust as is deemed fit to alert service managers and staff of risks that they may face. Due to the nature of such alerts it is necessary, at times, to put such alerts on restricted
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 33

distribution in order to comply with the Data Protection Act and an individual’s right to confidentiality. Alerts will be distributed by the Governance Department.
22. SIEGE OR HOSTAGE SITUATION (In the event of an emergency, please refer to Appendix ‘Ereference guide) 22.1. Any person held against their will by force or threat of force (expressed or
implied) must be considered a hostage. The taking of hostages is used in an attempt to secure total control in order to gain compliance with the wishes of the hostage-taker(s) in order to bring about the hostages release.
22.1.1.Hostage taking is a serious crime defined in law as;
A person whatever his nationality, who in the United Kingdom or elsewhere,- (a) detains any other person (‘the hostage’), and
(b) in order to compel a state, international governmental organisation or
person to do or abstain from doing any act, threatens to kill, injure or continue to detain the hostage, commits an offence.
(Contrary to: The Taking of Hostages Act 1982, Section 1).
22.1.2. Confusion or mishandling of a hostage incident could lead to avoidable serious
consequences. 22.1.3. Primary objectives during a hostage situation are to:
Preserve life; and Maintain the safety of staff and the public.
22.2. Contacting the Police - Siege or hostage Situation 22.2.1. The taking of hostages is always a matter for the police, and every area of
the United Kingdom has officers on call who are specifically trained in hostage negotiation techniques. The police must therefore be called using 999, as soon as possible. The staff member making this call should make it perfectly clear that there is a suspected hostage situation. At the same time the LSMS or in his absence the most senior member of healthcare staff available must be informed. The LSMS or senior member of staff should ensure that the Director of Finance and Chief Executive are informed and kept updated as to developments. Where the situation includes threats of explosives or other hazards, the guidance given on dealing with bomb threats above must be considered.
’ for quick
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 34

22.2.2. The police will benefit from the following information where available:
The exact location of the incident including access points; Details of the hostage-taker including clinical condition and events leading
up to the incident; Details of hostages; A suitable rendezvous point for police arrival, where they will be met by
appropriate personnel; Any known weapons or items being used as such; and Any known injuries to any party.
22.3. Primary Action - Siege or hostage Situation 22.3.1.The following provides guidance only until the arrival of police officers who, upon
arrival, will take over the control of the situation. The first five to ten minutes of any hostage situation are critical to setting the stage for the subsequent outcome, and tensions will be highest at this stage. It must be understood that the police have overall responsibility for the incident.
22.3.2.Prior to the arrival of the police, no attempt should be made to enter into any
form of discussion with the hostage-taker, unless failing to do so would place the hostage at greater risk. No negotiation should be undertaken and no requests granted. If confronted by the hostage-taker(s) it must be stated that you do not have the authority to grant any of their demands.
22.3.3.No attempt at intervention should be made whatsoever, if there is any doubt as
to its success or places the safety of those concerned. No intervention involving the use of force must be used unless:
Life is in immediate danger; and Forcible intervention has a high probability of success.
22.3.4. If possible and it is safe to do so, the situation should be carefully assessed (for example, through the use of CCTV) in order to determine:
The number of hostages Physical descriptions, especially of the hostage-taker(s) Any specific demands or statements. Make written notes. It is useful to keep
a log of times and actions taken for the information of the police Behaviour patterns Types of weapons; and Any other potentially useful facts.
22.3.5. Steps must be taken to ensure that the police are contacted as soon as possible together with details of any action taken. This should be done in a
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 35
quick, quiet and discreet manner out of sight and hearing of the hostage- taker(s). 22.3.6. Where possible, relevant staff should be directed to secure the location by
establishing an exclusion perimeter around the incident site at an appropriate distance relative to the risk presented. This will prevent the accidental incursion of unwary staff, patients and visitors into the incident scene. The exclusion area should also ensure that the immediate access route to the scene is secure, unobstructed and preferably unobserved from the incident location.
22.3.7. All non-essential staff and mobile patients should be withdrawn from the area, ensuring that this is done in a manner that will not cause alarm to the staff themselves or exacerbate the hostage situation. If this cannot be done without risk of inflaming the incident, no action should be taken. Where practicable, staff and patients should be protected by the securing of doors to relevant areas. 22.3.8. Arrangements should be made for all calls into and out of the hostage area to be diverted to the switchboard and for dedicated lines of communication to be made available to relevant parties. 22.3.9. Consideration should be given to greater risks than those currently present (i.e. access to hazardous materials) and, where it is safe to do so, steps should be taken to prevent access. 22.4. Secondary Action - Siege or hostage Situation 22.4.1. Witnesses to the incident should be asked to remain close to hand in order to provide the best information to the police when they arrive. Consideration should be given to arranging suitable support, such as access to counselling services, for those who may have been traumatised by the incident. 22.4.2. Information held pertaining to hazardous materials and fire hazards present on the site should also be made available to the emergency services. 22.4.3. No one should talk to the media unless the police press officer, who would have obtained the agreement of the police senior investigating officer in charge of the incident, approves the text. The hostage-taker(s) may be listening and could react adversely to media attention. 22.4.4. LSMS or appropriate senior personnel should arrange for the communications manager and NHS SMS to be briefed on the incident and they will liaise with the police press office, as appropriate. 22.5. Ancillary Action - Siege or hostage Situation
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 36
22.5.1. Consideration should be given to the location of other buildings in relation to the security incident, and whether any action needs to be taken in respect of these (i.e. managing unwanted onlookers). 22.5.2. Appropriate personnel and medical records of all parties involved should be made available to the police upon request. 22.5.3. The notification of next of kin for those held hostage is a matter for the police, unless specifically instructed by them otherwise. 22.6. Post Incident Management and Review 22.6.1. As soon as possible after the event, a meeting should be convened between all the agencies involved and the LSMS. The purpose of this debrief is to learn from the experience and to afford the revision of local and national guidelines or procedures in the light of that experience. 22.6.2. Issues about abortion, genetic research, and animal rights along with the more
common issues such as estrangement, insensitivity to human emotion, pain and vulnerability ensure that the healthcare setting is not immune from the possibility of a hostage situation. Avoiding the issue will not cause it to go away. The key to maintaining the safe environment that the law requires and healthcare workers have a right to expect, lies in planning, training and commitment.
22.7. Guidance for Staff - Siege or hostage Situation 22.7.1. The sudden occurrence of a hostage situation can cause fear and panic, but it is important to try and remain as calm and as rational as possible.
If you need medication, ask for it; Otherwise, do not say or do anything that may put you or others at further
risk; Do not lose hope and avoid an open display of despair; Initially, do not speak to anyone unless spoken to; Try to calm the hostage-taker; Do exactly what you are told and do not make suggestions; Try to appear calm but do not turn your back towards the hostage taker; Under no circumstances argue with the hostage-taker; Be observant, you may be released at any time; Expect noise and lights if a rescue attempt is made; and In the case of a rescue attempt drop to the floor and stay there until told
otherwise by one of the rescuers.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 37

22.8. Profile of the Hostage-Taker 22.8.1.Potential hostage-takers who are most likely to be encountered in a healthcare setting come from four groups: 22.8.2.The criminal who is either:
in the process of committing a crime and try to use hostages to achieve their objective or to escape; or
prisoner patient, who may have both the experience and propensity to carry out violent threats and be motivated by the desire to escape.
22.8.3. the aggrieved person who feels wronged by the system and considers that there is no way to address what they perceive is a legitimate grievance. 22.8.4. the estranged individual who is experiencing disruption or disintegration of a significant personal relationship with a loved one. 22.8.5. the acutely mentally ill who may be first diagnosed as such during or after a hostage incident; 22.8.6. Political terrorists must also be considered but their activity in a healthcare setting is generally considered as a low risk. 23. STAFF AWARENESS 23.1. Good training is essential for all members of staff and management must lead by
example. Every employee must know WHAT TO DO, and what NOT to do if there is a need to search or evacuate an area.
23.2. All staff should be aware of their surroundings and be on the look out for
suspicious behaviour, unusual packages or objects. 23.3. Each employee has a responsibility to exercise a duty of care in respect of NHS
property they use during the course of their duties. 24. VIOLENCE & AGGRESSION 24.1.1. Wirral Community NHS Trust is committed to tackling violence, and
aggression against NHS staff and professionals. 24.1.2. In any incident of violence or abuse towards NHS staff the line manager must
ensure that the employee is safe after the incident and where appropriate consider a referral to Occupational Health and/or the staff counselling service (MEDRA) to ensure that the best available support is given to the employee.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 38

24.1.3. The victim of any incident of violence or abuse should be informed of the progress of any investigation or action taken and offered full support and counselling services that are available in the circumstances. 24.2. Physical assaults 24.2.1. Physical assault on NHS Staff is defined as:
‘the intentional application of force to the person of another, without lawful justification, resulting in physical injury or personal discomfort.’
24.2.2. Each case of physical assault upon any member of the NHS in the course of their duties must be reported to the police. This applies to all employees, including volunteers, contractors, and employees of other organisations working on behalf of the Primary Care Trust. 24.2.3. Furthermore, such incidents should be immediately reported to the line manager of the employee concerned, or the appropriate on-call manager. 24.2.4. An incident form should be completed and the LSMS informed, as soon as possible. 24.2.5. The LSMS is responsible for investigating and reporting the incident to NHS
Protect using a national incident reporting system. This is known as the Physical Assault Reporting System (PARS). This system is intended to track and monitor cases from report to conclusion, to increase the prosecution rate of offenders, where appropriate, and to provide feedback and support to those who have been assaulted. 24.3. Non-physical assaults 24.3.1. It is important that patients, relatives and visitors are dealt with in a fair and
objective manner. However, whilst staff have a duty of care, this does not include accepting abusive behaviour.
24.3.2. The following definition of a non-physical assault was introduced in 2003 as part of the Secretary of State’s directions on work to tackle violence against staff and professionals who work in the NHS and replaced any other definitions previously in use across the NHS.
constituting harassment. 24.3.2. Inappropriate behaviour is not defined but some examples are given below:
Offensive or abusive language, verbal abuse and swearing which prevents staff from doing their job or makes them feel unsafe;
‘The use of inappropriate words or behaviour causing distress and/or ’
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 39

Loud and intrusive conversation; Unwanted or abusive remarks; Negative, malicious or stereotypical comments; Invasion of personal space Brandishing of objects or weapons Near misses i.e. unsuccessful physical assaults Threats or risk of serious injury to a member of staff, fellow patients or visitors Bullying, victimization or intimidation Stalking Spitting Alcohol or drug fuelled abuse Unreasonable behaviour and non-cooperation such as repeated disregard for
NHS policy i.e. visiting hours, smoking on premises, or Any of the above which is linked to destruction of or damage to property.
24.3.4. It is important to remember that such behaviour can be either in person, by telephone, letter or e-mail or other form of communication such as graffiti on NHS property. An incident form must be completed and the matter reported to the appropriate line manager or head of service. 24.3.5. The LSMS in conjunction with the Health & Safety Advisor, has responsibility for providing advice, guidance and support to managers in developing local arrangements under this policy. 24.3.6. The appropriate response to such incidents will depend upon the individual circumstances of each incident. Managers must recognise that action is appropriate where non-physical assault or abusive behaviour is likely to:
Prejudice the safety of staff involved in providing the care or treatment; or lead the member of staff providing care to believe that he/she is no longer able to undertake his/her duties properly as a result of fearing for their safety; or
Prejudice any benefit the patient might receive from care or treatment; or
Prejudice the safety of other patients; or
Result in damage to property inflicted by the patient, relative, visitor or as a
result of containing their behaviour. 24.3.7. Measures that can be taken as the result of a report of non-physical assault may include the following:
A verbal warning
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 40

Acknowledgement of responsibilities agreement (ARA) or Behaviour Agreement – an intervention designed to engage an individual in acknowledging his or her antisocial behaviour and its effect on others, with the aim of stopping that behaviour (For further details please see paragraph 18.5.2. and appendix ‘F
A written warning letter signed by a senior member of staff deemed to have
the suitable level of authority. A warning letter may also be sent by the NHS SMS Legal Protection Unit if appropriate. A template of a warning letter which can be amended accordingly can be found at appendix ‘G’
The use of secure environments or security chaperone
Civil injunctions and Anti-Social Behaviour Orders (ASBOs)
Criminal prosecution and police bail conditions
24.4. Verbal Warnings 24.4.1. Verbal warnings are a method of addressing unacceptable behaviour with a view to achieving realistic and workable solutions. 24.4.2. They are not a method of appeasing difficult patients, relatives or visitors in an attempt to modify their behaviour, or to punish them, but used instead to determine the cause of their behaviour so that the problem can be addressed or the risk of it recurring minimised. 24.4.3. Every attempt should be made to de-escalate a situation that could potentially become abusive or worse. Where de-escalation fails, the patient, relative or visitor should be warned of the consequences of future unacceptable behaviour. 24.4.4. Where it is deemed appropriate to speak to a patient, relative or visitor in respect of their behaviour, this should (where practicable) be done informally, privately and at a time when all parties involved are composed. 24.4.5. The aim of the verbal warning is twofold:
to ascertain the reason for the behaviour as a means of preventing further incidents or reducing the risk of it reoccurring; and
ensure that the patient, relative or visitor is aware of the consequences of
further unacceptable behaviour. 24.4.1. A meeting should be arranged and conducted in a fair and objective manner. A formal record should be made and maintained, utilising the Incident Reporting
’)
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 41

System. 24.4.2. Collective responsibility, partnership working and local ownership is essential to the creation of a pro-security culture and it is therefore important for managers to ensure that all relevant parties are involved in the development or review of local procedures and arrangements. Local procedures should therefore reflect:
the views of staff and their union safety representatives or professional representatives
the view of patients, service users and their representatives
clear links to other relevant procedures and policies; and
clear outlines of responsibilities and lines of accountability in respect of any
action to tackle non-physical assaults. 24.4.3. Members of staff should never be prevented or discouraged from reporting non- physical assaults to the police. In appropriate cases the clinical condition of the assailant should be considered as part of the decision making process. The following is a list of possible aggravating factors which should be considered when deciding to report an incident to the police. It is by no means exhaustive:
The effect on the victim and/or others present;
(However, the fact that none of the individuals present are adversely affected does not mean that a criminal offence has not been committed or that the incident should not be reported to the police).
The assailant’s behaviour is motivated by hostility towards a particular group
or individual on the ground of race, religious belief (or lack of), nationality, gender, sexual orientation, age, disability or political affliction;
A weapon, or object capable of being used as a weapon, is brandished or
used to damage property;
The incident was an attempted, incomplete or unsuccessful physical assault;
The incident involves action by more than one assailant;
The incident is not the first to involve the same assailant(s);
There is an indication that a particular member of staff or department/section is being targeted;
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 42

There is a serious concern that any threats made will be carried out;
There is a concern that the individual’s behaviour may deteriorate or that other NHS bodies should be advised or alerted;
The response to the incident has caused significant additional expenditure.
All incidents involving firearms should be reported to the police.
24.5. Service user/patient
24.5.1. Action at the level of the service user/patient relates to individual care planning
and patient expectation. Each service user having treatment within the NHS must have a care plan. Where violence is an issue, this plan must identify underlying problems which will be picked up as part of the patient assessment. Appendix ‘H’ provides an assessment tool template to assist nursing staff when carrying out an assessment for care-planning of patients with a potential for violence. Action in this area also includes participation in and adherence to any behaviour agreement on the part of the service user.
24.5.2. It is recommended by NHS Protect that as best practice, NHS health bodies
should have a behaviour agreement in place. This is a written agreement between staff and patients set by the NHS health body. It gives an opportunity for local issues and concerns to be addressed and allows the patient’s expectations to be managed by staff. An example of such an agreement is given in appendix ‘E’ of this document and lists the type of content needed. It should be noted that this list is not exhaustive. Engaging mental health professionals and psychologists to advise staff on where there is a history of violence will also be beneficial to the individual care-planning.
24.6. Secondary prevention 24.6.1. Secondary prevention is focused on reducing the prevalence of the problem by
minimising known or suspected risk factors and by early intervention i.e. when violence is perceived to be imminent or immediately post-incident. This knowledge can be used proactively to plan positive interventions such as training staff to recognise warning signs and in de-escalation strategies so they can defuse a potentially violent incident.
24.6.2.This involves staff using a dynamic risk assessment immediately before an
Incident occurs or while it is occurring. A dynamic risk assessment can be defined as a continuous process of identifying hazards and risks and taking steps to eliminate or reduce them in the rapidly changing circumstances of an incident. The dynamic risk assessment involves staff:
being alert to warning signs as covered in conflict resolution training
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 43

carrying out a ‘10-second risk assessment’; if staff feel there is a risk of harm to themselves, they should leave immediately placing themselves in a position to make a good escape
making a judgement as to the best possible course of action – for example, whether to continue working or withdraw. At no point should a staff member place themselves, their colleagues or their patients/service users at risk or in actual danger
utilising appropriate physical security measures e.g. triggering panic buttons to call assistance from staff nearby/security/the LSMS/the police, or using a lone worker device such as Identicom
ensuring that when they enter a confined area or room, they make sure they can operate the door lock in case they need to make an emergency exit
avoiding walking in front of a patient/service user, and not positioning themselves in a corner or in a situation where it may be difficult to escape
remaining calm and focused during an incident in order to make rational judgements.
24.6.3. Staff should be aware of their body language (as well as that of the
patient/service user). There is a risk of exacerbating the situation by sending out the wrong signals, particularly; if there are cultural, gender or physical issues to consider. Body language and other forms of non-verbal communication and mannerisms play an important role in how people perceive and behave towards others. Specific training in non-physical intervention skills, customer service and de-escalation is essential and all front-line staff must be trained in the national syllabus for conflict resolution, with additional training provided over and above this, depending on the risks faced and individual needs.
24.6.4. Managers and staff should discuss what actions they should take in the event of
an incident. The flowchart at appendix ‘J’ outlines action when confronted with an incident of violence or abuse.
24.6.5.Initially, this involves notifying the police, LSMS or health body security staff. The
manager responsible for the staff involved and the doctor on call or person in charge of the patient’s care should also be notified. These individuals all have their own responsibilities in the event of an incident:
24.6.6.The police if appropriate, to make an arrest, take witness statements, gather
evidence, conduct an investigation and secure the area if required. 24.6.7.The LSMS – to conduct an investigation, gather evidence and identify security
breaches and any failures in systems and processes. The LSMS should complete a PARS report if there is a physical assault. (Please see paragraph 24.2.5 above).
–
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 44

25. OTHER POLICIES & GUIDANCE 26.1. This policy should be read in conjunction with other Primary Care Trust polices
and guidance, examples include – Human Resource policies Lone Working, (PCT Reference: HS6) Accident/Incident Reporting, (PCT Reference GP8) Withholding Care Policy (PCT Reference: GP3) Counter Fraud and Security Management Service web resources
(www.CFSMS.nhs.uk), NHS Security Manual (held by the LSMS) Wirral Health Informatics Service (WHIS) Information Security and related
policies that are applicable to the PCT. CCTV Code of Practice. Risk assessments (PCT Reference HS9) Fraud and Corruption (PCT Reference: GP32)
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 45

Local Security Management Policy and Procedures
PART III
QUICK REFERENCE GUIDES
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 46

Appendix ‘A’ Quick Reference Guide
Dealing with a suspect package that may contain an explosive device
1. It is important to be aware that bombs can easily be disguised to look like
everyday objects. You are looking for an unidentified objects which: Should not be there Cannot be accounted for Is out of place Ownership cannot be established
2. Report any suspicious looking object to your manager or head of service. 3. Do not touch or attempt to move it.
4. Do not place the package into anything such as water or place anything on top of it. 5. Notify police & switchboard immediately (Switchboard Tel no: 0151 6 78 5111)
Give the operator the following information:
Your full name Your job title Your exact location Your contact telephone number.
6. Evacuate the immediate area and raise the alarm 7. Remain at a safe distance having regard to police advice and other information available at the time of the event. 8. Keep others away and restrict vehicles from entering the area. 9. Do not transmit from a mobile phone or radio within close proximity 10. Make a written description of the article and its location within a room (eg size, shape, lettering on it). 11. Assist police or bomb disposal squad at scene by providing as much information as possible about the threat and the layout of the area.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 47

Appendix ‘B’ Quick Reference Guide
CONFIDENTIAL (When complete)
Check list for recording evidence of a bomb threat (or similar warnings) Please listen carefully to the caller and record the details exactly as YOU hear them. Keep any notes you make of the message that you received, as well as this checklist, the Police will require copies of this information. Current date and time
Telephone number of person making the call (if known) :
Date and time of call or threat was made :
Telephone number at which the call was received :
Details of the exact words spoken in the telephone message/warning
Try and ask the caller the following questions and records their answers 1. Exactly where is the bomb?
2. When is it going to explode?
3. What does the bomb look like ?
4. What kind of bomb is it ?
4. What will cause it to explode?
6. Who placed the bomb?
7. Why did they place the bomb ?
8. Is their a code word? If Yes what is it : Time telephone call ended :
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 48
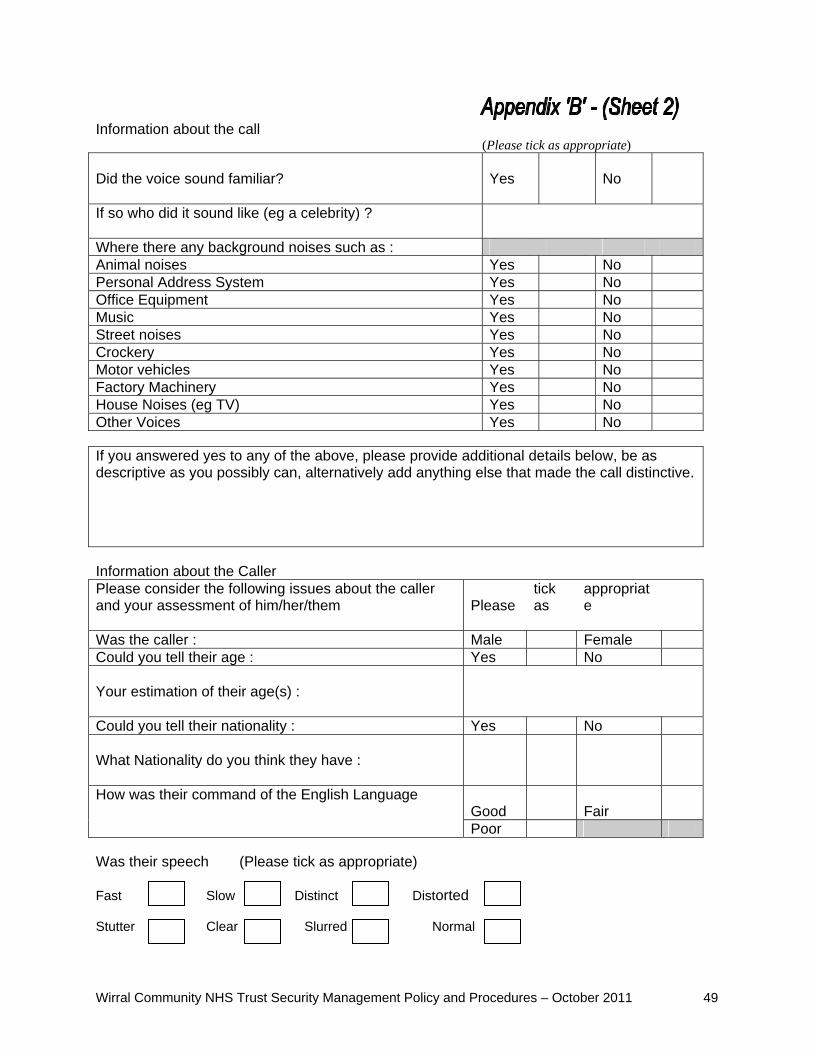
Information about the call (Please tick as appropriate) Did the voice sound familiar?
Yes
No
If so who did it sound like (eg a celebrity) ?
Where there any background noises such as : Animal noises Yes No Personal Address System Yes No Office Equipment Yes No Music Yes No Street noises Yes No Crockery Yes No Motor vehicles Yes No Factory Machinery Yes No House Noises (eg TV) Yes No Other Voices Yes No If you answered yes to any of the above, please provide additional details below, be as descriptive as you possibly can, alternatively add anything else that made the call distinctive.
Information about the Caller Please consider the following issues about the caller and your assessment of him/her/them
Please
tick as
appropriate
Was the caller : Male Female Could you tell their age : Yes No Your estimation of their age(s) :
Could you tell their nationality : Yes No What Nationality do you think they have :
How was their command of the English Language Good
Fair
Poor Was their speech (Please tick as appropriate) Fast Slow Distinct Distorted Stutter Clear Slurred Normal
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 49
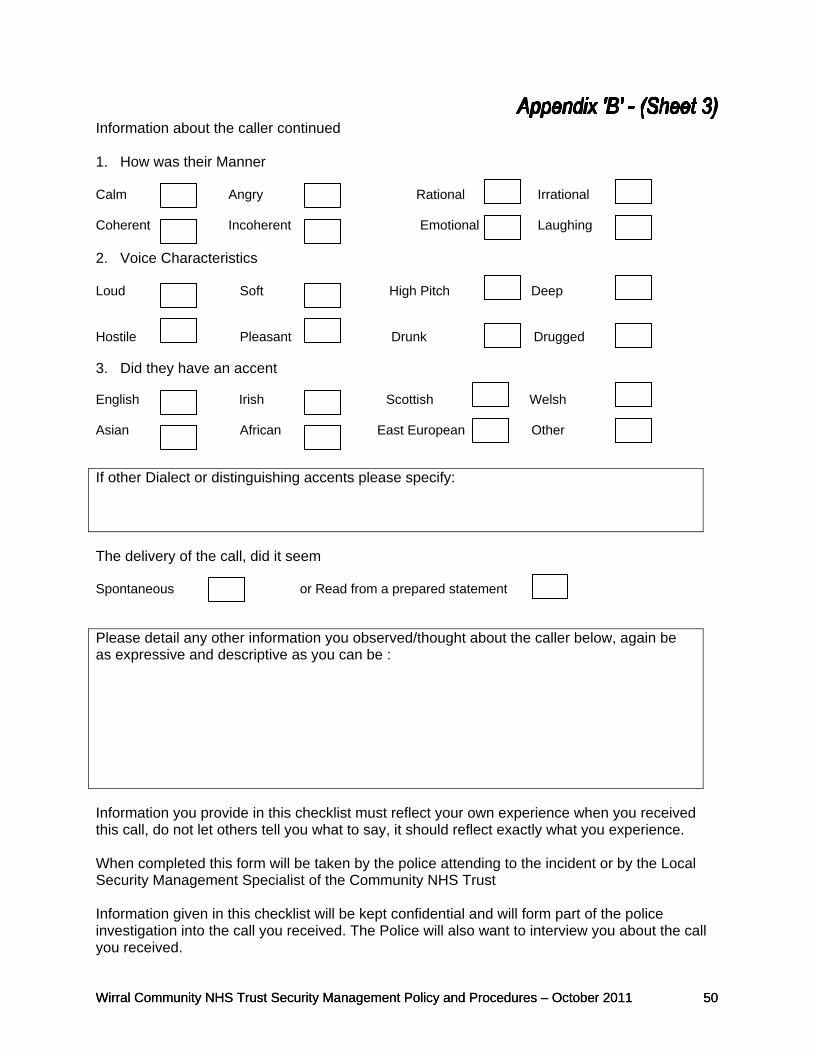
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 50
Information about the caller continued 1. How was their Manner Calm Angry Rational Irrational Coherent Incoherent Emotional Laughing 2. Voice Characteristics Loud Soft High Pitch Deep Hostile Pleasant Drunk Drugged 3. Did they have an accent English Irish Scottish Welsh Asian African East European Other If other Dialect or distinguishing accents please specify:
The delivery of the call, did it seem Spontaneous or Read from a prepared statement Please detail any other information you observed/thought about the caller below, again be as expressive and descriptive as you can be :
Information you provide in this checklist must reflect your own experience when you received this call, do not let others tell you what to say, it should reflect exactly what you experience. When completed this form will be taken by the police attending to the incident or by the Local Security Management Specialist of the Community NHS Trust Information given in this checklist will be kept confidential and will form part of the police investigation into the call you received. The Police will also want to interview you about the call you received.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 50

Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 51
Information about the person receiving the call Your First Name : Your Surname : Your Job Title : Your place of Work (full postal address) Who do you work for : Your contact telephone number: Did anyone else overhear the content of the ca If Yes please provide details: Time and date the police were informed: Did you phone the police or someone else: Yes Someone else If someone else please provide their details below: Details of the first person you informed that you had received this call: Full Name: Job Title: Address or contact details (if known): Signed: Please print your name:
:
ll: Yes No

Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 52
Appendix ‘C’
IMPERSONATION / SUSPICIOUS INDIVIDUALS
If a health professional is advised by a service user that they think they have been approached/visited by a person who claims to be a health professional,
but is thought to be bogus, then the following steps should be taken:
In the first instance, the service user should be advised to contact Merseyside Police on 0151 709 6010 so that any unnecessary delay in safeguarding the general public is avoided.
The member of staff should obtain the following information from the service user without delay: Description of the person/vehicle Name of bogus professional Employing agency Purpose of visit to include if they specifically asked to see a child/adult and if
they named them correctly, e.g. “I have come to see Mrs Jones/baby Lewis.” Date and time of incident Details of client/patient involved
The member of staff should immediately report the incident to their Line Manager/ Manager on call, if out of hours, on
0151-678 5111
The member of staff should complete an Incident Form within that working day and
sent to Line Manager
1. The Line Manager must discuss the situation with the Director of Operations &
Performance. Advice from Merseyside Police may be sought on 0151-709 6010 2. The Director of Operations & Performance will circulate a memo to all the
following by fax and email, giving a brief description of the person and details of their attempted visit to Heads of Service, LHD Leads, CYPD, Safeguarding Team (to include Designated Doctor/Nurse)
Director of Operations & Performance will feed back to Line Manager on outcomes
Line Manager will speak with service user and update action/progress

Appendix ‘D’ Briefing for Security personnel in the event of lockdown The following written guidance should be handed to security guards and read out at briefings. During an abnormal event which places greater demand upon the delivery of NHS services than that which is normally warranted, the primary care trust will endeavour to continue normal service for as long as possible but it may become necessary to close some areas and concentrate resources where they will be most effective. The main aim of security in tackling an abnormal event is:
o The security of medical supplies. o The security of staff, particularly frontline. o The protection of the general public.
Stockpiles of Medicine Dedicated members of staff may be assigned to accompany delivery drivers. Each vehicle must contain a mobile telephone or radio contact. Drivers may require the assistance of security staff with parking and delivery of vital drugs. Drugs must be stored in a secure room which is protected by an alarm. Keys must not be left in the lock. Protecting Staff If a visitor is unable to obtain the medication they seek then security personnel should be mindful that this may result in a dispute with staff. Disputes may be quickly resolved by making sure that all information about how to collect medication is readily available and easily understood. In the event that a minor dispute cannot be resolved then a Manager should be notified immediately and the complainant advised to contact in the first instance the Patient Advice Liaison Service on telephone number: 0151 647 4251 or if a more formal complaint is received, the Complaint’s Manager on telephone number 0151 651 0011. If a dispute escalates out of control then the police must be contacted immediately and the assailant requested to leave the premises. Ensuring queues are orderly.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 53

Length of queues and waiting times can also cause frustration and security personnel should ensure that there is no queue jumping and that signs are not removed. Some events may require the formation of two queues. It is crucial to the success of distributing emergency drugs that people can move through the defined queue system as efficiently as possible and that order is maintained. Regular checks should be made to ensure the following: Are drug storerooms secure and keys removed? Are the alarms, CCTV and electronic access controls working? Are all personnel wearing clearly visible identification badges? Are the issue and assessment areas clearly signposted at all times? Are fire exits clearly signposted and kept clear at all times? Is there a telephone landline immediately accessible in the event that assistance needs to be summoned? Do you know the name of the ACP Manager and where that person can be contacted? Any breach of security must immediately be reported to the Local Security Management Specialist or in his absence the Estates Department
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 54

Appendix ‘E Quick Reference Guide
Siege Situation ~ Initial Action
’
Remember: you and everyone involved is a potential victim or hostage. Initial Action For further advice
refer to section: 1. Immediately telephone 999 Call out emergency service (e.g: police, ambulance, Or fire brigade).
22.2. and 22.3.5.
2. Inform the senior manager on duty and switchboard. Ensure that the Chief Executive, Director of Finance and on call Director are notified.
22.2.1.
3. Do not take unnecessary chances
22.3.3.
4. Try to prevent unwary staff, patients or visitors from accidental entry of the incident scene.
22.3.6.
5. If possible withdraw all non-essential staff, mobile Patients, contractors and visitors from the area.
22.3.7.
10. Arrange for telephone calls into hostage area to be diverted to the switchboard.
22.3.8.
11. Try to contain the situation consider if there are nearby
hazardous materials and the need to secure other buildings in the vicinity.
22.3.6. –
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 55
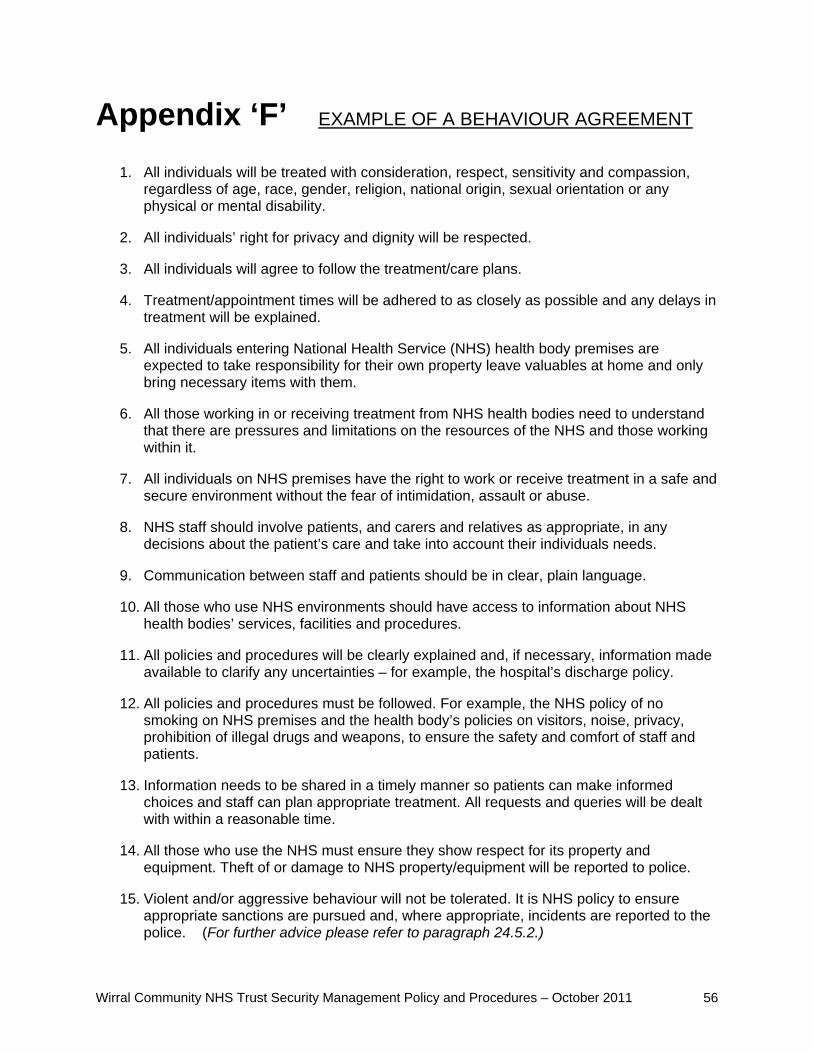
Appendix ‘F EXAMPLE OF A BEHAVIOUR AGREEMENT’
1. All individuals will be treated with consideration, respect, sensitivity and compassion, regardless of age, race, gender, religion, national origin, sexual orientation or any physical or mental disability.
2. All individuals’ right for privacy and dignity will be respected.
3. All individuals will agree to follow the treatment/care plans.
4. Treatment/appointment times will be adhered to as closely as possible and any delays in treatment will be explained.
5. All individuals entering National Health Service (NHS) health body premises are expected to take responsibility for their own property leave valuables at home and only bring necessary items with them.
6. All those working in or receiving treatment from NHS health bodies need to understand that there are pressures and limitations on the resources of the NHS and those working within it.
7. All individuals on NHS premises have the right to work or receive treatment in a safe and secure environment without the fear of intimidation, assault or abuse.
8. NHS staff should involve patients, and carers and relatives as appropriate, in any decisions about the patient’s care and take into account their individuals needs.
9. Communication between staff and patients should be in clear, plain language.
10. All those who use NHS environments should have access to information about NHS health bodies’ services, facilities and procedures.
11. All policies and procedures will be clearly explained and, if necessary, information made available to clarify any uncertaintie for example, the hospital’s discharge policy.
12. All policies and procedures must be followed. For example, the NHS policy of no smoking on NHS premises and the health body’s policies on visitors, noise, privacy, prohibition of illegal drugs and weapons, to ensure the safety and comfort of staff and patients.
13. Information needs to be shared in a timely manner so patients can make informed choices and staff can plan appropriate treatment. All requests and queries will be dealt with within a reasonable time.
14. All those who use the NHS must ensure they show respect for its property and equipment. Theft of or damage to NHS property/equipment will be reported to police.
15. Violent and/or aggressive behaviour will not be tolerated. It is NHS policy to ensure appropriate sanctions are pursued and, where appropriate, incidents are reported to the police. (For further advice please refer to paragraph 24.5.2.)
s –
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 56
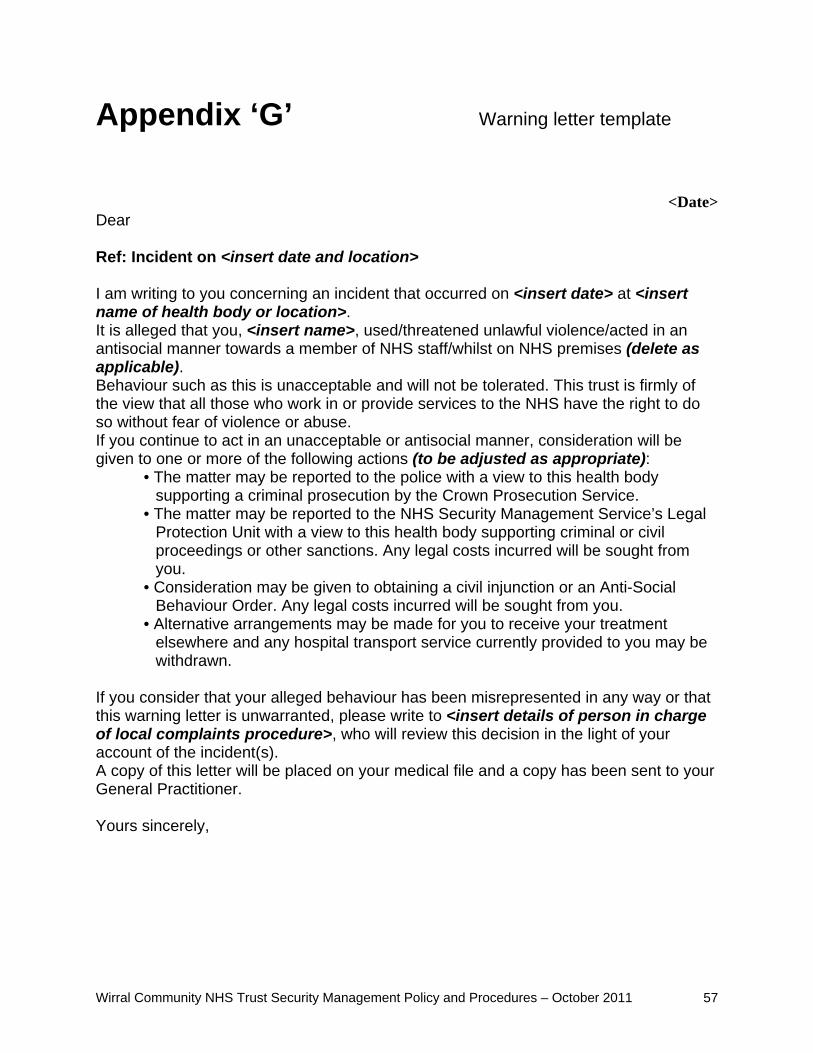
Appendix ‘G Warning letter template
<Date> Dear Ref: Incident on <insert date and location> I am writing to you concerning an incident that occurred on <insert date> at <insert name of health body or location>. It is alleged that you, <insert name>, used/threatened unlawful violence/acted in an antisocial manner towards a member of NHS staff/whilst on NHS premises (delete as applicable). Behaviour such as this is unacceptable and will not be tolerated. This trust is firmly of the view that all those who work in or provide services to the NHS have the right to do so without fear of violence or abuse. If you continue to act in an unacceptable or antisocial manner, consideration will be given to one or more of the following actions (to be adjusted as appropriate):
• The matter may be reported to the police with a view to this health body supporting a criminal prosecution by the Crown Prosecution Service.
• The matter may be reported to the NHS Security Management Service’s Legal Protection Unit with a view to this health body supporting criminal or civil proceedings or other sanctions. Any legal costs incurred will be sought from you.
• Consideration may be given to obtaining a civil injunction or an Anti-Social Behaviour Order. Any legal costs incurred will be sought from you.
• Alternative arrangements may be made for you to receive your treatment elsewhere and any hospital transport service currently provided to you may be withdrawn.
If you consider that your alleged behaviour has been misrepresented in any way or that this warning letter is unwarranted, please write to <insert details of person in charge of local complaints procedure>, who will review this decision in the light of your account of the incident(s). A copy of this letter will be placed on your medical file and a copy has been sent to your General Practitioner. Yours sincerely,
’
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 57

Appendix ‘H’ Prevention and management of violence and abuse Assessment tool template This assessment tool is designed to help nursing staff assess patients with a potential for violence or a history of violence and abuse against NHS staff, and to achieve a consistent approach. It should be used in conjunction with the information and strategies outlined in these procedures. The tool may be used on its own or as part of an overall nursing assessment and the information gathered used to inform the patient’s care plan.
Nursing intervention Guidance Notes 1
Assess patient’s potential for violence and abusive behaviour through history, patient interview (or interview with family and friends, if patient is unable to communicate). Where possible, refer to medical and nursing notes and information provided from other relevant organizations or individuals, such as Social Services, patient’s GP etc.,
• Before meeting with the patient, examine their medical and nursing notes to check for any incidents of violence and abusive behaviour that have been documented and how they were managed. • Introduce yourself and explain any procedure in plain and simple terms. Try to build a rapport with the patient to put them at ease during the assessment interview. • If appropriate and safe to do so, explore the patient’s history with them and explain the health body’s policy regarding violence and abuse against staff.
2
Assess whether patient has any communication difficulties and explore possible reasons for this (e.g. sensory impairment, learning disability or English not being their first language).
• If there are communication difficulties, try to arrange for a family member or significant other person to be present to assist during the assessment. You should always try to obtain the patient’s consent for this first. • If the patient’s hearing is impaired, ensure that hearing aid equipment is set and working properly or arrange for a BSL interpreter to be present for the assessment. • If the patient’s first language is not English, it may be appropriate to arrange for an interpreter to be present.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 58

3
It may be useful to engage with family and/or friends to establish if there is any history of violence or abusive behaviour within the family. To maintain patient confidentiality, establish whether or not the patient has advised any significant persons/family, of their condition. However, be aware that family dynamics may be a cause of patients’ violence and judge whether or not to proceed with engaging with family. Establish level of support available to the patient from family or other significant person.
• Encourage family members and significant persons to enforce message that violence or abuse is not tolerated within the healthcare environment.
4
Assess patient’s attitude to treatment and medical condition.
• Answer any questions the patient may have concerning their admission, treatment or diagnosis and try to alleviate any anxiety. • Arrange for the patient’s doctor, or other relevant members of the multi-disciplinary team (MDT), to discuss their condition with them if necessary.
5
Assess patient’s current physical and mental health, current medication and any substance use and misuse.
• If there are any concerns about the patient’s mental health, refer to the on-call psychiatrist, psychiatric liaison nurse or mental health team. • If there are any signs of substance use or misuse, discuss with the patient the health body policy on the use of substances. Refer the patient to the substance misuse team, if appropriate. • If appropriate, set boundaries with patient and employ the use of a behaviour agreement (see appendix ‘F’ for template). • If there are any organic or other physical health concerns, refer to the appropriate member of the MDT. • Explain policy regarding prescribed medication.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 59
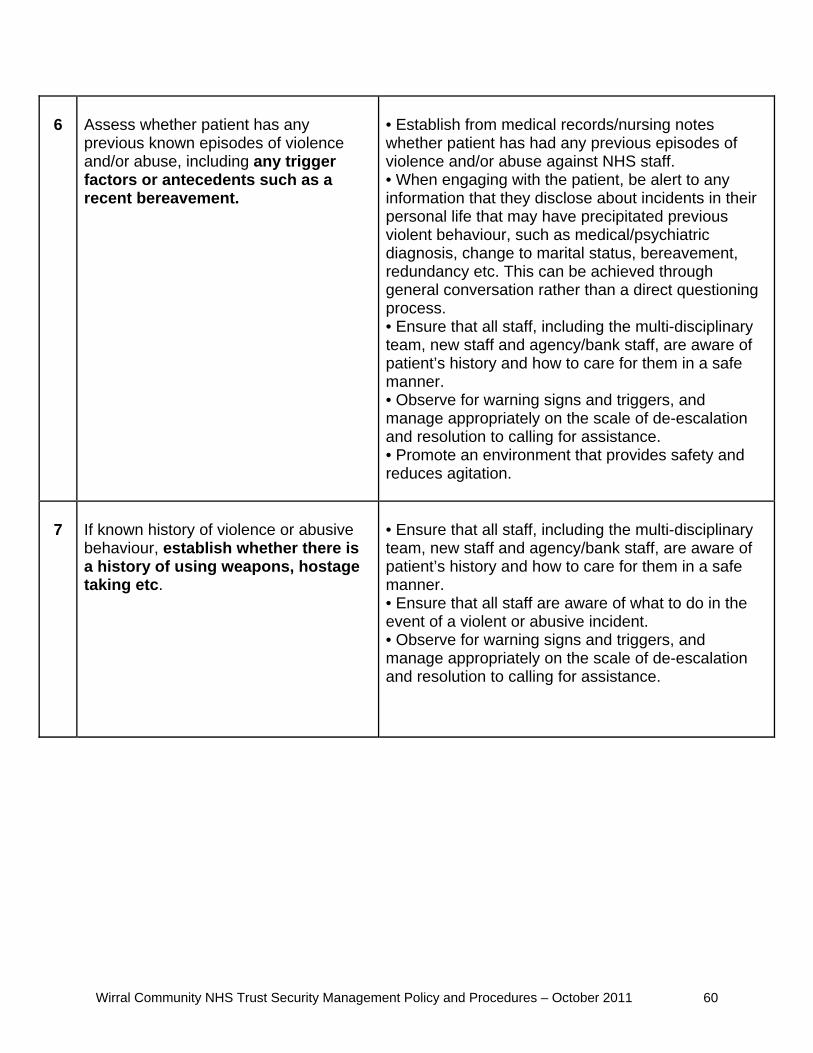
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 60
6
Assess whether patient has any previous known episodes of violence and/or abuse, including any trigger factors or antecedents such as a recent bereavement.
• Establish from medical records/nursing notes whether patient has had any previous episodes of violence and/or abuse against NHS staff. • When engaging with the patient, be alert to any information that they disclose about incidents in their personal life that may have precipitated previous violent behaviour, such as medical/psychiatric diagnosis, change to marital status, bereavement, redundancy etc. This can be achieved through general conversation rather than a direct questioning process. • Ensure that all staff, including the multi-disciplinary team, new staff and agency/bank staff, are aware of patient’s history and how to care for them in a safe manner. • Observe for warning signs and triggers, and manage appropriately on the scale of de-escalation and resolution to calling for assistance. • Promote an environment that provides safety and reduces agitation.
7
If known history of violence or abusive behaviour, establish whether there is a history of using weapons, hostage taking etc.
• Ensure that all staff, including the multi-disciplinary team, new staff and agency/bank staff, are aware of patient’s history and how to care for them in a safe manner. • Ensure that all staff are aware of what to do in the event of a violent or abusive incident. • Observe for warning signs and triggers, and manage appropriately on the scale of de-escalation and resolution to calling for assistance.

8
As regards any previous episodes of violence or abusive behaviour, establish the following if possible: how previous incidents were managed; which interventions were successful and which were not; how long the episode of violence or abusive behaviour lasted; if medication was used to resolve the situation; if the police were involved; and what sanctions, if any, were applied.
• If in previous episodes of violence, particular interventions worked, review these for application locally. If particular interventions did not work, review these for lessons to be learned and ensure that all of the multi-disciplinary team, new staff and agency and bank staff are aware of these. • Observe for warning signs and triggers, and manage appropriately on the scale of de-escalation and resolution to calling for assistance.
9
Where possible, use appropriate advanced
directives1 determined by the patient.
• Staff may wish to consider previous incidents recorded and decide whether it would be helpful to discuss known trigger factors and any preferred intervention with the patient. • Staff may wish to consult their mental health colleagues for advice before engaging in such a discussion with the patient. • Ensure that any advanced directives are communicated to all staff caring for the patient.
1 An advanced directive is a document that contains the instructions of a patient, setting
out their requests in the event of a relapse of a condition or an incident of disturbed/violent behaviour etc. It sets out the treatment that they do not want to receive and any treatment preferences that they may have in the event that they become violent. It also contains the names of people whom they wish to be contacted and any other personal arrangement that they wish to be made.
Wirral Community NHS Trust Security Management Policy and Procedures – October 2011 61

Wirral PCT Security Management Policy – January 2008 62
Appendix ‘J’
Incident of violence or abuse occurs
Immediate Or imminent
danger
Initial incident dealt
with
Primary tasks:
Do not take risks Look for hazards Decide who might be harmed and how Decide whether existing precautions are
adequate Decide whether to continue
operations or evacuate Discreetly remove objects that could
be used as weapon
Contact: (a) Police (if appropriate) (b) Local Security Management Specialist.
Secondary tasks:
Notify manager & complete incident report
• Notify Manager • Complete an incident report
Notify LSMS •
Begin a post-incident review process
Establish if a medical review is required
Investigation & review (as appropriate)
Provide counselling/support Follow up on all witnesses to the
incident Conduct a risk assessment and a
develop strategy for ensuring safety
Provide feedback on process/ systems in place, any
identified weaknesses and Lessons learned
MANAGEMENT OF VIOLENT / ABUSE INCIDENT
Manager to provide support & assistance on dealing with
immediate situation until resolved.
Initiate post-incident review

![Meeting Procedures Local Law No. 17293931: 20436355_1] page 1 MEETING PROCEDURES LOCAL LAW NO.1 OF 2017 1. Title 1.1 This Local Law may be cited as Meeting Procedures Local Law No](https://static.fdocuments.us/doc/165x107/5ab6a8577f8b9ab47e8e1272/meeting-procedures-local-law-no-1-7293931-204363551-page-1-meeting-procedures.jpg)
















