Local Intraarterial Thrombolysis in Vertebrobasilar ... · Local Intraarterial Thrombolysis in...
4
401 Local Intraarterial Thrombolysis in Vertebrobasilar Thromboembolic Disease H. Zeumer,1 W. Hacke ,2 and E. B. Ringelstein 2 The poor prognosis of basilar artery occlusion is well known. Systemic anticoagulation rarely prevents a lethal outcome . A new therapeutic approach involves selective perfusion of strep- tokinase through the vertebrobasilar artery via a coaxial catheter system . Three of five reported cases demonstrated successful vascular recanalization with clinical improvement. Between 1976 and 1981 , 17 patients with angiog r aphica ll y di- ag nosed basilar ar t ery thr ombos is were treated at our clinic. Ten patients died within 2 weeks, while six patients survived more than 6 weeks but less than 3 months. Only one patient survived a 1 year period. All the patients had severe neurologic defic its and died from secondary comp li ca ti ons suc h as pulmonary thr o mboembo li sm, myocardial infarction, or pneumonia . These results parallel the experiences of oth ers [1-4] in document ing the poo r prognosis of basi lar artery thrombosis . In our view, the st anda rd regimen using heparin and other anti coagu lants offered no proven therapeutic advantage. With this in mind, we felt challenged to deve lop a new therapy, despite the possible dangers involved. The systemic administr ation of the fibrinolytic agent streptoki- nase in doses of 2,500,000 IU / day is reported to be hazardou s and fraught with comp li cat ions [5]. Moreover , this therapy ca nnot be applied soon aft er angiograp hy because of the certainty of local bleeding. However, card iologists [6-8] have demonstrated that in patients with co ronary art ery thrombosis, th e local use of fibrinolyti c agents is superior to systemic app li cat ion and that even in hi gh local conce ntr ations, the systemic effect is minimal. Our approach involved selec tive perfusion of streptok in ase through the vert ebro- basi lar artery by means of a coaxial cat heter system. Results of the treatment if") five cases are reported. Methods The technique used to perform loca l fibrinolysis in the vertebro- bas il ar system is relatively simpl e: A 6 French Torcon catheter (William Cook Europe, DK-2860 Sbbo rg, Denmark) is introduced via a femoral sheath into the vertebra l ar teri es and angiog r aphy is performed. The same cat het er is th en used to guide a 3 French Teflon catheter (which comp letely occludes the lumen of the Torcon catheter) into the vert ebra l artery chosen for perfusion . The tip of this catheter is placed just below the atlas loop and the guiding catheter is then removed to the descending aorta. The drug is administered with a high-acc ur acy infusion pump . The dose of str eptokinase (200,000 IU) used in our first four cases was comparable to doses used by cardiologists; however, we administered the drug more slow ly. When perform ing coronary artery thromboly sis, one must t ake into co nsideration the great loss of streptokinase to the aortic arc h. In compar ison, the leakage that takes place in the vertebrobasilar system is less signi fi cant. In view of our recent expe rience using lower doses (50 ,000 IU) of strepto- kinase, we are no longer sure th at the initial dose of 200,000 IU over a period of 2 hr is either the op timal amount or th e best time co urse for administration of the drug. The fibrinolytic therapy is acco mpanied by low-dose heparin treatment ca lculated to prolong thrombin time by a factor of 2 or 3. Case Reports Case 1 A 27-year-o ld woman, aft er an initial transient hemihypesthesia and hemiataxia, experienced deterioration . Symptoms included somnolence, tetraparesis, and multiple co mplic ated ocu lomotor disturbances. The details have been described elsewhe re [9]. An upper bas il ar occlusion was found (fig. 1 A) in co njun ct ion with intracrania l vertebral artery occ lu sion. After admi nistration of 200,000 IU strept ok inase, reca nali zation was angiograph ica ll y demonstrated. Furt her angiographic improvement was noted th e next day and normalization was ac hieved after a second adminis- tr ation of 70,000 IU streptok in ase (fig. 1 B). We be li eve an embo lu s from the stump of the occ lu ded vertebra l art ery was dissolved before further thrombosi s occurred in the basilar artery. The patient was disc harged at 8 weeks with minimal motor disturbances of th e hands and was report ed to be well at 11 months posttreatment. Case 2 A 62-year-old woman showed minimal r ecana lization of the bas- il ar artery after administrat ion of 200,000 IU str ep tokin ase. How- ever, a co mplete reocclus ion occurred at 12 hr posttreatment co ncomitant with a severe deterio ration in ge neral co ndition . The patient died a few hour s later. Case 3 A 57-year-old woman, initia ll y comatose and suffering from oc- clusion of the lower and middle basilar artery. was treated with I Neuroradiological Service. Klinikum der Rheini sc h-Westfalischen, Techni sc hen Hochsc hule. Goethestr. 27-29 . 5 100 Aac hen. West Germany . Address reprint requests to H. Zeumer . 2 Department of Neurology , Klinikum der Rheinisch-Westfalischen. 5100 Aachen. West Germany . AJNR 4:401-404, May / June 1983 0195-6108 / 83 / 0403-0401 $00 .00 © Ameri ca n Roentgen Ray Soc iety
Transcript of Local Intraarterial Thrombolysis in Vertebrobasilar ... · Local Intraarterial Thrombolysis in...

401
Local Intraarterial Thrombolysis in Vertebrobasilar Thromboembolic Disease H. Zeumer, 1 W . Hacke,2 and E. B . Ringelstein2
The poor prognosis of basilar artery occlusion is well known. Systemic anticoagulation rarely prevents a lethal outcome. A new therapeutic approach involves selective perfusion of streptokinase through the vertebrobasilar artery via a coaxial catheter system. Three of five reported cases demonstrated successful vascular recanalization with clinical improvement.
Between 1976 and 1981 , 17 patients with angiog raphically diagnosed basilar artery thrombosis were treated at our c linic. Ten patients d ied within 2 weeks, while six patients su rvived more than 6 weeks but less than 3 months. Only one pat ient survived a 1 year period. All the patients had severe neurologic deficits and died from
secondary complications such as pulmonary thromboembolism, myocardial infarc tion, or pneumonia. These results parallel th e experiences of others [1-4] in documenting the poor prognosis of basi lar artery thrombosis. In our view, the standard reg imen using heparin and other anticoagu lants offered no proven therapeutic advantage. With this in mind , we fe lt challenged to develop a new therapy, despite the possible dangers involved.
The system ic administrat ion of the fibrinolytic agent streptokinase in doses of 2,500,000 IU / day is reported to be hazardous and fraught with complicat ions [5]. Moreover, this therapy cannot be applied soon after angiog raphy because of the certainty of local bleeding. However, card iologists [6-8] have demonstrated that in pat ients wi th coronary artery thrombosis, th e local use of fibrinolyti c agents is superior to system ic applicat ion and that even in high
local concentrat ions, the systemic effect is minimal. Our approach involved selecti ve perfusion of streptok inase through the vertebrobasi lar artery by means of a coaxial catheter system. Results of the treatment if") five cases are reported.
Methods
The technique used to perform local fibrinolysis in the vertebrobasilar system is relatively simple: A 6 French Torcon catheter (William Cook Europe, DK-2860 Sbborg, Denmark) is introduced via a femoral sheath into the vertebra l arteries and angiography is performed. The same catheter is th en used to gu ide a 3 French Teflon catheter (which completely occludes the lumen of the Torcon
catheter) into the vertebral artery chosen for perfusion . The tip of this catheter is placed just below the atlas loop and the gu id ing catheter is then removed to the descending aorta. The drug is administered with a high-accuracy infusion pump.
The dose of streptokinase (200,000 IU) used in our first four cases was comparable to doses used by cardiologi sts; however, we administered the drug more slowly. When perform ing coronary artery thrombolysis, one must take into consideration the great loss of streptokinase to the aorti c arch. In comparison, the leakage that takes place in the vertebrobasilar system is less signi fi cant. In view of our recent experience using lower doses (50,000 IU) of streptokinase , we are no longer su re that the initial dose of 200,000 IU over a period of 2 hr is either the optimal amount or th e best time course for administrat ion of the drug. The fibrinolyti c therapy is accompanied by low-dose heparin treatment calculated to prolong thrombin time by a facto r of 2 or 3.
Case Reports
Case 1
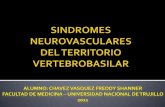
A 27-year-old woman, after an initial transient hemihypesthesia and hemiataxia, experienced deterioration . Symptoms included somnolence, tetraparesis, and multiple complicated ocu lomotor disturbances. The details have been described elsewhere [9]. An upper basilar occlusion was found (fig. 1 A) in conjunct ion with intracranial vertebral artery occ lusion. After administration of
200,000 IU streptokinase, recanalizat ion was ang iograph icall y demonstrated. Further angiographic improvement was noted the next day and normalization was achieved after a second administration of 70,000 IU streptok inase (fig . 1 B). We believe an embolus from the stump of the occluded vertebra l artery was dissolved before further thrombosis occurred in the basilar artery . The patient was discharged at 8 weeks with minimal motor disturbances of the hands and was reported to be well at 11 months posttreatment.
Case 2
A 62-year-old woman showed minimal recanalization of the basilar artery after administrat ion of 200,000 IU streptokinase. However, a complete reocclus ion occurred at 12 hr posttreatment concom itant with a severe deterioration in general condition . The pat ient died a few hours later.
Case 3
A 57-year-old woman , initially comatose and suffering from occ lusion of the lower and middle basi lar artery. was treated with
I Neuroradiological Service. Klinikum der Rheinisch-Westfalischen, Technischen Hochschule. Goethestr . 27-29 . 5 100 Aachen. West Germany. Address
reprint requests to H. Zeumer. 2 Department of Neurology, Klinikum der Rheinisch-Westfalischen. 5100 Aachen. West Germany.
AJNR 4:401-404, May/ June 1983 0195-6108 / 83 / 0403-0401 $00 .00 © American Roentgen Ray Society

402 INTERVENTIONAL PROCEDURES AJNR:4, May / June 1983
.. A 8
A 8
200,000 IU streptokinase. Recanalization was not achieved. In this case, we decided against repeat thrombolysis because 36 hr after the c linical onset a hypodense lesion of the pons had been detected by computed tomography (CT) . This patient survived for 3 months in a state of " locked-in " syndrome. Later CT scans showed an increase in the size of the hypodense lesion of the pons .
Case 4
Fig. 1.-Case 1. A, Subtota l upper basi lar artery occ lusion. B, Recanalization after local in traarterial fibrinolYSis .
Fig. 2.-Case 4. A, Left vertebral angiogram (oblique projection) . Subtotal stenosis of upper segments of left vertebral artery (arrows). B , Recanlization after local intraarterial fibrinolysis.
A 54-year-old woman with a 5 year history of quadrantanopsia complained of intermittent exacerbat ion of her visual defects and developed complete corti cal blindness 48 hr later. Immediate angiography demonstrated normal blood flow in the right vertebral

AJNR :4 , May / June 1983 INTERVENTIONAL PROCEDURES 403
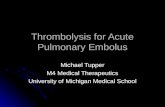
Fig . 3. - Case 5. Init ial angiograms show bilateral stenoses of the intracranial vertebral arte ri es (A) w ith lower basilar artery occlusion (B, arrow). Posttreatment angiog rams demonstrate normal fl ow in both vertebral arteri es (C) and in basilar artery (0, arrow).
A
c
artery, th e basilar artery, and the major branches of the posterior
cerebral arteries. The left vertebral artery showed subtotal stenosis at the loop above th e atlas (fig . 2A) and in th e intracranial segment. Because of th e possibility of further embolization from the left vertebral artery, it was dec ided to apply local fibrinolysis. The procedure was successful in effecting recanalization after 2 hr (fig . 2B) . The patient' s blindness rapidly vanished and no further brainstem or visual symptoms have since occurred .
Case 5
A 33-year-old woman with a history of transient hemihypesthesia suffered a brainstem infarction 7 days before admission with severe right hemiparesis, a left-sided Babinski refl ex, impaired hori zontal eye movements, dysarthria, and dysphagia . Angiography demon
strated severe bilateral stenoses of both intracranial vertebral artery segments with lower basilar artery occlusion (figs. 3A and 3B) . It was dec ided to administer a lower dose of streptoki nase over an extended period of therapy. At 12 hr intervals, the right and left vertebral arteries were altern ately perfu sed, each for a 1 hr period , with 50,000 IU of streptokin ase. Recanalization was achieved after 25 hr. The Teflon catheter was subsequently left in place in the left vertebral artery , and an infusion of 15,000 IU / hr of streptokinase was administered over 12 hr. Th e increasing fl ow in both vertebral
8
D
arteries was monitored by Doppler sonography. The fi nal resul ts of therapy are shown in fi gures 3C and 3D. With normalization of flow a slight worsening of hemiparesis was noted, but this cond ition resolved within 1 week. The patient was able to walk with assistance after 3 weeks. The oculomotor d isturbances were minimal at this time.
Discussion
In our first patient , who initially suffered from severe neuro log ic defi c its, earl y implementation of therapy was very important in promoting c linica l recovery. However, the value of earl y commencement of therapy should not be overestimated. Neurons will die if exposed to 10 min total ischemia. Such neuronal death is impossible to treat, since no available therapy can be initiated quick ly enough to salvage these neurons. Clinical symptoms in stroke-prone patients may be caused not only by ce ll death , but also by reversible functional disturbances . Neu rons in the so-called ischemic penum
bra may be resuscitated and rega in normal fu nction after restoration of blood fl ow. Clin ically, it is impossible to tell whether a c linica l neurolog ic defi c it is caused by ce ll death or functi onal insuffic iency. Ischemic arterial walls are penetrated by red blood ce ll s after a few hours. The clin ica l experi ence in our last patient , who had transient

404 INTERVENTIONAL PROCEDURES AJNR:4, May / June 1983
deterioration, suggests hemorrhage into an existing necrotic lesion with su rrounding edema. No bleeding was demonstrated by CT. Nevertheless we are always concern ed about the possibility of secondary bleeding.
In all five cases, our main intention was to prevent further progression of local thrombosis in the vertebrobasilar system with resultant c linical deterioration. In three of our five patients, improvement of func tional distu rbances as well as the prevention of further ischemic necrosis was achieved. Of course preex ist ing neurologic deficits are not influenced by thrombolysis.
At present, we advise using small quantit ies of streptokinase with long administration times. It is suggested that con tinuou s perfusion of abou t 10,000-15,000 IU / hr will provide optimal lysis and minimal ri sk, but the optimum dose and time course are still under evaluation .
It seems desirable to reduce th e number of angiog rams obtained during therapy. Doppler sonography of the vertebral arteries was used in all our patients, and results compared favorably with angiography. In our experience, Doppler-sonographic flow studies provide a high ly re liable way of monitoring the effects of therapy.
REFERENCES
1. Kubik CS, Adams RD. Occlusion of the basilar artery-a clinical and pathological study. Brain 1946;69: 73-1 2 1
2. McDowell F, Potes H, Grosch S. The natural history of internal carotid and vertebral-basilar artery occlusion. Neurology (N Y) 1961 ;11 : 153-160
3 . Dorndorf W, Giinshirt H. Die Klinik der arteriellen zerebralen Verschlusse. In: Giinshirt H, ed. Der Hirnkreislauf. Stuttgart:
Thieme, 1972 4 . Archer CR, Horenstein S. Basi lar artery occlusion . Clinical and
radiological correlation. Stroke 1977;8: 383- 390 5. Brogden LN , Speight TM , Avery GS. Streptokinase. A review
of its c linical pharmacology , mechanism of action, and therapeutic use. Drug 1973;5: 3 57 -365
6. Rentrop KP, Blanke H, Karsch KR, et al. Wiedererbffnung des Infarktgefiisses durch transluminale Rekanalisation und intracoronare Steptokinase-Applikation . Dtsch Med Wochenschr 1979;104 : 1438-1440
7. Rentrop KP , Blanke B, Rahlf G, Leitz K. InfarktgrbBenbegrenzung durch nicht-chirurgische Rekanalisat ion der Koronararterien. Dtsch Med Wochenschr 1981 ;106: 765-770
8. Merx W, Dbrr R, Rentrop P, et al. Evaluation of the effectiveness of intracoronary streptokinase infusion in acute myocardial infarction: Postprocedure management and hospital course in 204 patients. Am Heart J 1981; 102 : 11 8 1 -11 87
9. Zeumer H, Hacke W, Kolmann HL, Poeck K. Lokale FibrinoIyse-Therapie bei Basilaris Thrombose. Dtsch Med Wochenschr 1982;107: 728-731
Addendum
Recent experience has shown that an intermittent application of streptokinase is superior to a continuous perfusion. Starting with bolus inject ions of 4 ,000 IU streptokinase every 15 min, the dosage shou ld be reduced to 2,000 IU / injection, when the plasma fibrinogen level has fallen to half the initial level. Using this reg imen , therapy can be performed over a period of 12-24 hr in an intensive care unit.