LOCAL ANAESTHESIA
77
-
Upload
anonymous-fodvgcw -
Category
Documents
-
view
16 -
download
2
description
BASIC OF LA
Transcript of LOCAL ANAESTHESIA


Local anesthetics (LAs) prevent or relieve pain by
interrupt- ing nerve conduction. They bind to specific
receptor sites on the sodium (Na+) channels in nerves
and block the movement of ions through these pores

Electric potential of
60-70mV

Mechanical,chemical thermal stimuli
Miniscule electric current
Electric potential become less negative
Threshold potential Achieved
Action potential results
-sudden influx of Na ions
depolarization
-depolarization generates the current that
-depolarizes the adjacent segment of NV
Thus occur sequential polarization
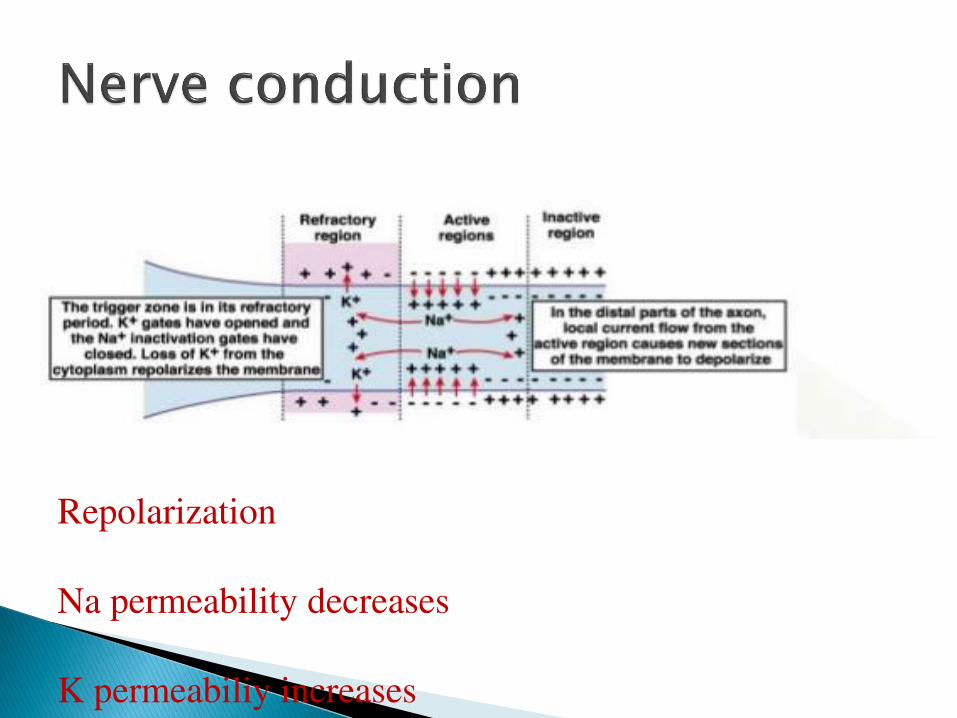
Repolarization
Na permeability decreases
K permeabiliy increases

LAs prevent the generation and conduction of nerve
impulse by binding to the alpha sub unit of voltage gate
sodium channel and preventing the influx of Na ions

Block duration is JUST related to protein binding
Extend of period to which local anaesthetic remain in
vicinity of nerve
-lipid solubility
-vascularity of tissue
- presence of vasoconstrictors
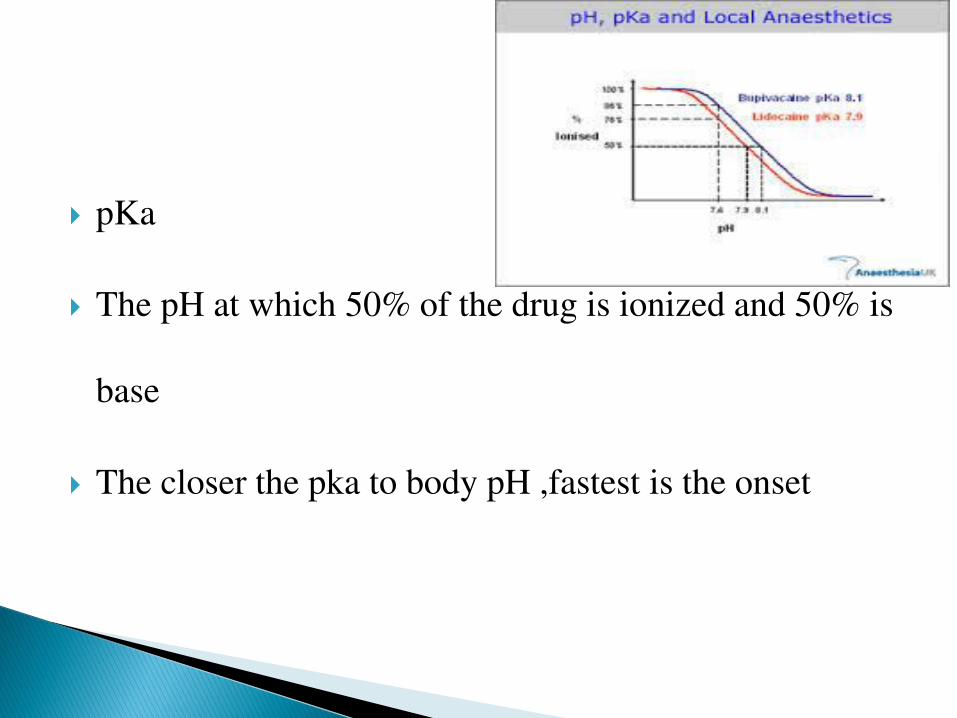
pKa
The pH at which 50% of the drug is ionized and 50% is
base
The closer the pka to body pH ,fastest is the onset
The degree of protein binding of a particular LA is
influenced by the pH
The binding decreases from 95% to 70% with acidosis,
the amount of free drug bupivacaine increases from 5% to
30%
Acidosis renders the drug more toxic

• Short acting(45-90 minutes)
• -2-chloroprocaine
• Intermediate acting(90-180 MINUTES)
• -lidocaine
• ,mepivacaine
• Long acting(4-18 HOURS)
• -BUPIVACAINE
• LEVOBUPIVACINE
• ROPIVACAINE

Smaller nv fibers are more susceptible to the action
of LA than large fibers’
Myelinated are easily blocked than unmyelinated
C fibers ,small in diameter, unmyelinated are most
resistant to block

Loss of pain sensation
Cold
Warmth
Touch
Deep pressure
Motor function
NV BLOCK ONSET
B
A DELTA
A GAMMA
A BETA
A ALPHA
C
NV BLOCK RECOVERY
• Is proportional to concentration of LA in circulation
• Which depends on • dose of drug administered
• Rate of absorption of drug
• -site injected.
• Vasoactivity of drug.
• vasoconstrictors
• Biotransformation and elimination of drug in circulation
Short acting ester linked local anaesthetic are
inherently safer with respect to systemic toxicity due
to their clearance by pseudo cholinesterase

Appparent stimulaqtion
followed by depression
of neuronal activity
• No current monitoring method can prevent systemic toxicity.
cases have been reported despite (1) negative aspiration
for blood, (2) the use of recommended dosages, and (3) the
observation of local anesthetic spread in a tissue plane and
not intravascularly
• Thus constant vigilance and preparation for treatment is essential
during all regional anesthetic procedures.

• Lidocaine
• onset of seizures 10 to 12 µg/mL
• respiratory depression (20-25 µg/mL)
• Bupivacaine,
• 4 µg/mL result in seizures,
• 4 - 6 µg/mL cardiac toxicity.
• This is reflective of a much lower therapeutic index for
bupivacaine compared with lidocaine in terms of cardiac toxicity.
• The symptoms of CNS toxicity associated with LAs are a
function of their plasma level
• Toxicity is typically first expressed as stimulation of the
CNS, producing restlessness,disorientation, and tremor
• central stimulation is followed by depression and
respiratory failure, culminating in coma

However, rapid systemic administration of a LA may
produce death with no, or only transient, signs of CNS
stimulation

occurs at high systemic concentration than required for CNS
toxicity
Predominantly CNS signs may or may not occur prior to
cardiac symptom
Due to action on pacemaker cell
Bupivacaine causes
◦ Progressive Prolongation of ventricular conduction,
widening of QRS COMPLEX,VF

Bupivacaine, which is four times more potent than
lidocaine in blocking nerves, is also four times more
potent in depressing cardiac contractility.

PLASMA CONCENTRATION of AAG is decreased
in pregnancy and newborns
Increases the free fraction of bupivacaine thus more
cardio toxic

No current monitoring method can prevent systemic oxicity
Midazolam-0.05—0.1mg/kg
Propofof—0.5—1mg/kg
Ventilation wih 100% oxygen
If ventilation inadequate than intubation with aid of a
muscle relaxant
Cardiotoxicity-cardiac resuscitative measure

Act as lipid sink; that draws drug out of the solution
Its possible role in overriding the inhibition of
mitochondrial carnitine-acylcarnitine translocase, thereby
providing the myocardium with fatty acid for fuel
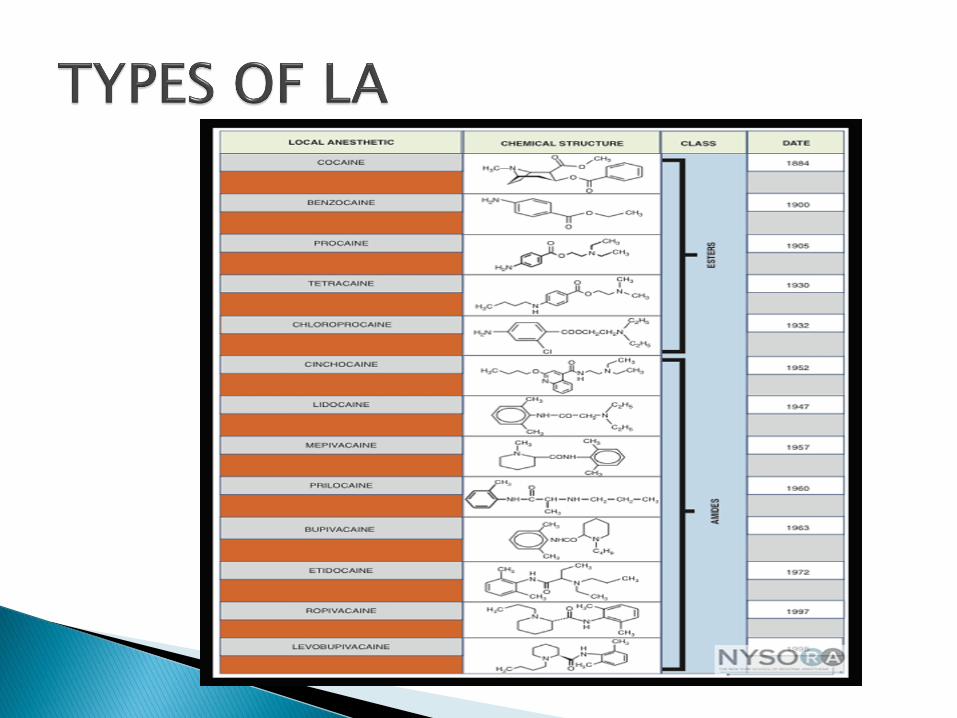
ESTER LINKED AMIDE LINKED
Hydrolyzed at ester linkage by
pseudocholine esterase
Hydrolysis lead to formation
of PABA(POTENTIAL OF
ALLERGIC RECTION)
LIVER[dealkylation]
Allergic reaction due to
PABA as preservative

Short acting ester linked local anaesthetic are
inherently safer with respect to systemic toxicity due
to their clearance by pseudo cholinesterase

Leaves of coca shrub
local vasoconstrictor
Only LA THAT inhibit uptake of norepinephrne and do
not produce sensitization to catecholamine
Mydriatic
Use topical anaesthesia
vasocostrictor
INFILTERATION ANAESTHESIA

Chlorine derivative of procaine
Rapid break down

Most toxic
Used in combination with lidocaine as
‘super caine’

• Prilocaine is an intermediate-duration amino amide LA with a
pharmacologic profile similar to that of lidocaine
• . The primary differences are a lack of vasodilatation.
• methemoglobinemia, an effect of metabolism of the aromatic
ring to o-toluidine
• IV administration of methylene blue (1-2 mg/kg). Prilocaine is
used infrequently in peripheral nerve blockade
• Etidocaine
• Etidocaine is a long-acting amino amide introduced in
1972.
• profound motor blockade outlasts sensory blockade.
• not used for peripheral nerve blockade.

• introduction in 1963,
• commonly used in regional and infiltration anesthesia.
• producing prolonged anesthesia and analgesia
• . At least part of the cardiotoxicity of bupivacaine may be
mediated centrally because direct injection of small quantities of
bupivacaine into the medulla can produce malignant ventricular
arrhythmias.
• Bupivacaine-induced cardiotoxicity can be difficult to treat.

S-enantiomer of 1-propyl-2', 6'-pipecolocylidide
The S-enantiomer, has a lower toxicity than the R-enantiomer.
. Ropivacaine undergoes extensive hepatic
. Ropivacaine is slightly less potent than bupivacaine
reduced CNS toxicity and cardiotoxic potential
For these reasons, ropi- vacaine has become one of the most commonly
used long acting LAs in peripheral nerve blockade.

Levobupivacaine
Levobupivacaine contains a single enantiomer of
bupivacaine hydrochloride, and is less cardiotoxic than
bupivacaine

• The addition of a vasoconstrictor to a LA delays its
vascular absorption, increasing the duration of drug
contact with nerve tissues. The net effect is
prolongation of the blockade by as much as 50% and a
decrease in the systemic absorption of LA.


• opioid receptors are present in the substantia gelatinosa
of the spinal cord.
• successfully used in neuraxial blockade to both
enhance the blockade and prolong analgesia.
• However, in peripheral nerves, similar receptors are
absent.
• For this reason, opiates do not have a significant
clinical role in peripheral nerve blockade.
• Clonidine.FENTANYL,MORPHINE

• Mixing of Local Anesthetics
• . Unfortunately, when LAs are mixed, their onset,
duration, and potency become much less predictable,
and the end result is far from expected
• results in little clinical advantage.
0.5% is 5mg /ml
2% is 20mg/ml

EMERGENCY DRUGS

There is limited evidence to suggest that one particular
inotrope is better than another.
• Dobutamine is predominantly a ß1 agonist and
therefore increases cardiac contractility and heart rate.
• It also acts at ß2 receptors causing vasodilatation and
decreasing afterload.

Because of this vasodilatation, and to ensure adequate MAP is
achieved, it may be necessary to administer dobutamine in
combination with a vasopressor (eg, noradrenaline).
side effects
• increased heart rate,
• arrhythmias
• raised myocardial oxygen demand.
These can cause myocardial ischaemia.
Dobutamine is not a vasopressor but rather a inotrope
that causes vasodilation –
increasea inotropy and chronotropy and
reduces LV filling pressure
Dopamine is a complicated inotrope
it has dose-dependent pharmacological effects
. Low-dose dopamine (2–5µg/kg/min) exerts mainly
dopaminergic effects
medium doses (5–10µg/kg/min) the ß1 inotropic effects
high doses (10–20µg/kg/min) a1 vasoconstriction
predominates.

Epinephrine also serves as a marker of intravenous
injection of local anesthetic. An increase in heart rate of
20 bpm or greater and/or an increase in systolic blood
pressure of 15 mmHg or greater after a dose of 15 mg
of epinephrine is should raise a suspicion of
intravascular injection.

For postoperative analgesia (often in concert with
general anesthesia) do not require a high concentration
of LA.
Ropivacaine 0.2% is usually sufficient to provide
excellent sensory analgesia but spare any motor
blockade.

In 1903, Braun suggested using
adrenaline as a “chemical tourniquet” to
prolong the duration of local anesthetics

Phenylephrine has purely Alpha-adrenergic agonist
activity and therefore results in vasoconstriction with
minimal cardiac inotropy or chronotropy. MAP is
augmented by raising SVR

Isoproterenol
is also primarily an inotropic and chronotropic agent
rather than a vasopressor.[ Beta-1]
Utility limited to hypotensive patients, where
hypotension results from bradycardia.
Norepinephrine
acts both on Alpha-1 and Beta-1 adrenergic receptors,
thus producing potent vasoconstriction as well as a less
pronounced increase in CO.
A reflex bradycardia ususally occurs in response to
increased MAP
Most commonly used in septic shock.
•
• Route: IVDosage: For acute myocardial infarction 6 mg IV bolus followed by 54
mg within the first hour, followed by 20 mg/hour for 2 hours for a total dose of 100
mg.
• Patients <65 kg should receive a total of 65 mg.
• Alternatively: 15 mg IV bolus then 50 mg IV over 30 minutes, followed by 35 mg
over 60 minutes ("front loading" regimen).
•
Anistreptase (Eminase, Iminase)
Route: IV Dosage: For acute myocardial infarction 30 units IV over 2-5 minutes

Atenolol (Tenormin, Atenil, Atenolan, Betatop, and others)
Route: IV
Dosage: Following acute myocardial infarction, 5 mg IV over 5 minutes
every 10 minutes for a total IV dose of 10 mg.
Oral atenolol therapy should be initiated immediately after the second IV
bolus with 50 mg, followed by another 50 mg oral dose 12 hours later. Oral
maintenance therapy is continued with 100 mg daily for at least 10 days.
• Route: IV
• Hyperkalemia
Magnesium intoxication:.
• Hypocalcemic tetany:
• Calcium channel blocker overdosage:
• 5-10 mL (6.8-13.6 mEq) of 10% calcium chloride
• 10-20 mL (4.65-9.3 mEq) of 10% calcium gluconate IV
over 5 minutes.
• Repeat after 1-2 minutes as necessary.

Magnesium sulphate
Route: IV, IM
Dosage: Seizure prevention and control in pre-
eclampsia or eclampsia:
4-5 gm of 50% solution IM every 4 hours.

• Metoprolol (Lopressor, Betaloc, Arbralene, Beprolo, and
others)
• Route: IV, PO
Dosage: Following acute myocardial infarction, 5 mg IV push
every 2 minutes for a total IV dose of 15 mg.
• Oral metoprolol at a dose of 50 mg every 6 hours should be
started 15 minutes after the last IV bolus dose and continued for
48 hours.
• The maintenance dose is 100 mg twice daily for at least 3
months.
•
Streptokinase (Kabikinase, Streptase)
Route: IV
Dosage: For acute myocardial infarction 1.5 million
units IV over 1 hour

Vasopressin (Pitressin)
Route: IV
Dosage: For bleeding oesophageal varices (unlabeled
use in U.S.), 0.2 units/minute initially.
The infusion rate may be increased by 0.2 units/minute
every hour if bleeding continues and up to 1
unit/minute,

• Verapamil
• Route: IV
• Dosage: For Supraventricular tachyarrhythmias 5-10 mg
IV push over 2 minutes.
• A second bolus dose of 10 mg may be administered after
30 minutes