LNCS 8149 - Constructing an Un-biased Whole Body Atlas ......j∈RTE cc j for Fi.This estimateisused...
8
Constructing an Un-biased Whole Body Atlas from Clinical Imaging Data by Fragment Bundling Matthias Dorfer 1, , Ren´ e Donner 1 , and Georg Langs 1,2 1 CIR Lab, Department of Radiology, Medical University of Vienna, Austria 2 CSAIL, Massachusetts Institute of Technology, Cambridge, MA, USA {matthias.dorfer,rene.donner,georg.langs}@meduniwien.ac.at Abstract. Atlases have a tremendous impact on the study of anatomy and function, such as in neuroimaging, or cardiac analysis. They provide a means to compare corresponding measurements across populations, or model the variability in a population. Current approaches to construct atlases rely on examples that show the same anatomical structure (e.g., the brain). If we study large heterogeneous clinical populations to capture subtle characteristics of diseases, we cannot assume consistent image acquisition any more. Instead we have to build atlases from imaging data that show only parts of the overall anatomical structure. In this paper we propose a method for the automatic contruction of an un-biased whole body atlas from so-called fragments. Experimental results indicate that the fragment based atlas improves the representation accuracy of the atlas over an initial whole body template initialization. Keywords: Anatomical atlas construction, Medical imaging fragments, Average shape and intensity model, Landmark transformation accuracy. 1 Introduction Models that represent common characteristics of a specific anatomical structure, or atlases are at the center of medical imaging analysis in the context of quanti- tative morphometric population analysis, or as a reference frame to summarize functional data across large cohorts. In computational anatomy anatomical at- lases have been constructed for single organs such as the brain [3], or for entire body regions such as the abdomen [6]. Anatomical atlases help to automati- cally distinguish between healthy and pathological subjects [4] or to segment or annotate anatomical structures contained in the imaging data [8]. Existing approaches commonly rely on the presence of the same anatomical structure of interest in all examples that form the training data for the atlas, and the target data the atlas is applied to. This is feasible for organ specific studies, such as in This work has received funding from the Austrian Sciences Fund (P 22578-B19, PULMARCH), EU (FP7/2007-2013) under grant agreements 318068 (VISCERAL), 257528 (KHRESMOI). K. Mori et al. (Eds.): MICCAI 2013, Part I, LNCS 8149, pp. 219–226, 2013. c Springer-Verlag Berlin Heidelberg 2013
Transcript of LNCS 8149 - Constructing an Un-biased Whole Body Atlas ......j∈RTE cc j for Fi.This estimateisused...

Constructing an Un-biased Whole Body Atlas
from Clinical Imaging Data by FragmentBundling
Matthias Dorfer1,�, Rene Donner1, and Georg Langs1,2
1 CIR Lab, Department of Radiology, Medical University of Vienna, Austria2 CSAIL, Massachusetts Institute of Technology, Cambridge, MA, USA{matthias.dorfer,rene.donner,georg.langs}@meduniwien.ac.at
Abstract. Atlases have a tremendous impact on the study of anatomyand function, such as in neuroimaging, or cardiac analysis. They providea means to compare corresponding measurements across populations, ormodel the variability in a population. Current approaches to constructatlases rely on examples that show the same anatomical structure (e.g.,the brain). If we study large heterogeneous clinical populations to capturesubtle characteristics of diseases, we cannot assume consistent imageacquisition any more. Instead we have to build atlases from imaging datathat show only parts of the overall anatomical structure. In this paper wepropose a method for the automatic contruction of an un-biased wholebody atlas from so-called fragments. Experimental results indicate thatthe fragment based atlas improves the representation accuracy of theatlas over an initial whole body template initialization.
Keywords: Anatomical atlas construction, Medical imaging fragments,Average shape and intensity model, Landmark transformation accuracy.
1 Introduction
Models that represent common characteristics of a specific anatomical structure,or atlases are at the center of medical imaging analysis in the context of quanti-tative morphometric population analysis, or as a reference frame to summarizefunctional data across large cohorts. In computational anatomy anatomical at-lases have been constructed for single organs such as the brain [3], or for entirebody regions such as the abdomen [6]. Anatomical atlases help to automati-cally distinguish between healthy and pathological subjects [4] or to segmentor annotate anatomical structures contained in the imaging data [8]. Existingapproaches commonly rely on the presence of the same anatomical structure ofinterest in all examples that form the training data for the atlas, and the targetdata the atlas is applied to. This is feasible for organ specific studies, such as in
� This work has received funding from the Austrian Sciences Fund (P 22578-B19,PULMARCH), EU (FP7/2007-2013) under grant agreements 318068 (VISCERAL),257528 (KHRESMOI).
K. Mori et al. (Eds.): MICCAI 2013, Part I, LNCS 8149, pp. 219–226, 2013.c© Springer-Verlag Berlin Heidelberg 2013

220 M. Dorfer, R. Donner, and G. Langs
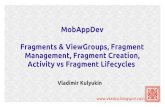
Fig. 1. Overview of fragment to WB reference space registration. The goal is to find atransformation TFi,R which registers a fragment Fi with the WB reference template R.
neuroimaging, where the brain is the focus of analysis [1]. It is not feasible forbuilding a representative model of the entire human body. In clinical practice,only those parts of the anatomy relevant for diagnosis are imaged [2]. We callthese imaging data fragments. To use this data for population studies, to repre-sent anatomical variability, or to identify characteristics of pathologies we needmethodology to build an atlas from fragment data.
The contribution of this work is an atlas construction framework to constructan un-biased template from clinical medical imaging fragment data. Fragmentsacquired during clinical routine cover the human body in overlapping regions.The proposed atlas construction allows for the dense sampling of a wide range ofanatomical regions in a clinical population. It goes beyond building and stitchingindividual atlases that represent individual anatomical regions. Furthermore, theatlas adds structure to arbitrary clinical imaging data examples, that constituteits training population. The framework provides functionality to localize theregion of a fragment in relation to a Whole Body (WB) reference template andto register the fragment within the WB reference space. Based on the fragmentsthe average shape and intensity template is updated. The method is closelyrelated to Guimond et. al. [3] but extends it to image fragments. This fragmentbased model enables the bundling of imaging fragments within a single commonWB reference space.
The results indicate that our approach is feasible, and is able to constructan atlas in situations where a large fraction of the data shows only part ofthe structure of interest. After an initial fit to a WB template the fragmentregistrations, and the template are updated and refined in an iterative processthat further reduces bias.
2 Methods
Given a set of fragments F1, ...,FN , where Fi ∈ Rmi×ni×hi , we seek to find
a reference template R ∈ Rm×n×h and corresponding transformations TFi,R so
thatTFi,R maps each position between the reference template and the individualfragment. To initialize the group-wise registration, all fragments are registeredto a WB volume, that can either be a single individual, or the result of group-wiseregistration of multiple WB volumes. For each fragment the corresponding region(reference space fragment) FR,i in R is determined. Then, the fragments Fi are

Constructing an Un-biased Whole Body Atlas from Fragments 221
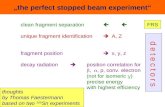
Fig. 2. Overview of miniature similarity based robust center estimation
registered to their corresponding region FR,i. After initialization the templateis updated to represent both shape and appearance variation in the fragmentpopulation, and the fragments are registered to the updated template iteratively.This leads to an increasinlgy un-biased template RF representing the populationof fragments [3]. Fig. 1 illustrates all components contributing to the registrationproblem addressed. The main computation steps of the algorithm are: (1) Foreach fragment Fi estimate the center ci in R. (2) Estimate the correspondingreference fragment FR,i. (3) Non-rigidly register Fi to FR,i. (4) Compute up-dated fragment based shape and intensity population model RF based on theregistered fragments. In the following we describe the steps in detail.
2.1 Fragment Center Estimation
The first step to register Fi to R is to estimate its center position ci in R. Thisis based on calculating the appearance similarity of the fragment Fi and a set offragments Fc
j with known center points ccj , following an approach proposed in[2]. Fig. 2 provides an overview of the center estimation algorithm. For each Fc
j
we construct a miniature Mj by resizing it to dimensions of 32× 32× 32 voxels.Fi is downscaled analogously. We compute the Normalized Cross Correlation(NCC) and select those k miniatures for whom this similarity is highest.
Given the centers cc1, ..., cck of of the k top ranked miniatures, we calculate the
median position, and keep the 50 percent of estimates closest to the median. Theregion containing these estimates is denoted as Region of Trimmed Estimates(RTE). From this set we calculate the center estimate by ci =
1k/2
∑ccj∈RTE ccj
for Fi. This estimate is used to initialize the transformation and the fragmentregion in the WB template.
2.2 Fragment Region Estimation
Based on ci we estimate the region inR corresponding to the fragment. We refinethe fragment center estimate ci as well as the region IFR,i (voxel coordinates)of the reference fragment FR,i (intensity volume) with respect to R iteratively.The initial region IFR,i corresponding to the fragment is spanned by the bound-ing box, with same dimensions as the fragment, centered around ci, defined bycoordinates of two opposite corners xcor1,i and xcor2,i. The input fragment Fi is

222 M. Dorfer, R. Donner, and G. Langs
affinely registered to the corresponding reference fragment FR,i = R(IFR,i) re-sulting in an affine transformation Ta
Fi,R. Based on Ta
Fi,R, we update IFR,i . For
the region update the two homogeneous corner coordinates xcor1,i and xcor2,i are
transformed by the inverse of TaFi,R
. i.e., x1cor l,i = Ta,−1
Fi,R(xcor l,i) with l = 1, 2.
The updated corresponding region I1FR,iof the fragment is now spanned by the
transformed corner points x1cor1,i and x1
cor2,i leading to an updated reference
space fragment F1R,i and a rigid component Tr
Fi,Rof the transformation TFi,R.
The updated center position c1i is computed as the arithmetic mean of the trans-formed corner points.
The localization procedure is iterated with the updated reference fragmentuntil the region estimate IkFR,i
converges. We keep the affine transformationTa
Fi,Rof the final iteration k as initialization for the non-rigid registration.
2.3 Non-rigid Registration of the Fragment to the WB Template
The previous computation step estimates the corresponding reference space frag-ment FR,i and region IFR,i of the input fragment Fi in the WB template R.The final step of fragment to WB registration is the non-rigid registration of thequery fragment Fi with the reference space fragment FR,i yielding the non-rigidtransformation Tnr
Fi,R. For registration B-spline based Free Form Deformation
(FFD) is used [7],[5]. The final result is an embedding of the non-rigidly regis-tered fragment F′
i in the WB reference template R as well as the correspondingtransformation TFi,R = Tnr
Fi,R◦Ta
Fi,R◦Tr
Fi,R.
2.4 Fragment Based Un-biased WB Reference Template Update
With the algorithm described in the previous subsections, we register fragmentsFi with i = 1, ..., N to a common reference template R ∈ R
m×n×h. In the firststage fragments are registered to an initial template R0. After the first iteration,this template is updated based on the fragment appearance, and deformationinformation, to obtain an un-biased template. For each fragment Fi we have thecorresponding region IFR,i in R, the reference fragment FR,i, the transformation
TFi,R, and the transformed fragment F′i = Fi(T
−1Fi,R
(x)).Based on these components the shape and intensity averaging, proposed by
Guimond et. al. [3] is enhanced to a fragment based model. For a region con-strained shape and intensity averaging we calculate for every voxel x in R, theset of fragments I(x) = {i|T−1
Fi,R(x) ∈ Fi} that contribute to it as well as the
corresponding number of contributors N(x) = |I(x)|. Based on N(x) the aver-
age fragment registration F′ ∈ R
m×n×h is formalized as F′(x) = 1
N(x)
∑i∈I(x)
Fi(T−1Fi,R
(x)). The transformations of the fragments towards R are averaged
in each voxel x, i.e., TF = M(TnrFi,R
) where i ∈ I(x). In practice we followGuimond et. al [3] and estimate the mean by averaging the vector fields ofthe non-rigid transformations. We exclude rigid and affine transformations fromun-biasing, since they mainly capture variability in image acquisition (e.g., body

Constructing an Un-biased Whole Body Atlas from Fragments 223
Fig. 3. Construction results of the fragment based WB shape and intensity model RF
on 60 head, thorax, and abdomen fragments
region imaged, resolution), and assume that the population variability is encodedin the non-rigid component of the transformations. The fragment based averageshape and intensity model R1
F of iteration one is computed by applying the re-
gion dependent inverse average deformationT−1
F to the region dependent average
intensity registration image F′. This results in R1
F (x) = F′(T
−1
F (x)) and draws
the shape of the average intensity registration F′towards the geometric popu-
lation center of the training fragments [3]. The result is an un-biased fragmentbased model R1
F representing the underlying fragment population F1, ...,FN .We proceed by again registering the fragments to this template, and updatingthe template Rk
F iteratively, until convergence.
3 Experimental Results
We evaluate the fragment based WBA construction on data that includes a sin-gle initial WB Computed Tomography (CT) volume R and 60 CT fragmentsFi encompassing parts of the body including head, thorax, or abdomen. Allvolumes are isotropic and have a voxel dimension of 2 mm. In each fragmentexpert annotated bone landmarks are placed for evaluation, if present. They areused as reference for validation of registration accuracy, and the representationalpower of the atlas. The aim of the experiment is to show, (1) that the proposedmethod is capable to register medical imaging fragments containing locally lim-ited anatomical regions to a common WB reference template R and (2) that thefragment based model RF improves the representation of the imaging data incomparison to the initialization R.
3.1 Experimental Setup
All 60 fragments Fi are registered with the WB template R resulting in theregistered fragments F′
i and the corresponding transformations TFi,R (see sub

224 M. Dorfer, R. Donner, and G. Langs
section 2.2 and Subsection 2.3). Fragment center estimation was based on 1200annotated fragments. The registrations are used to compute the average frag-ment model RF as described in sub section 2.4. Fig. 3 summarizes the resultsand shows the resulting fragment based model RF . Additionally the contribu-tion of each training fragment Fi to the respective region of RF is highlighted.In Fig. 3(c) blue rectangles indicate the bounding boxes of the fragments in thereference space.
After model computation all fragments are registered to the updated, un-biased fragment based template RF . The registration transformations TFi,R
and TFi,RF are applied to the coordinates of the landmarks annotated in therespective fragments. This yields landmark distributions containing the positionestimates for each of the landmark positions in the two reference spaces R andRF . As evaluation measure the centroid of these landmark distributions as wellas the mean distance of all landmarks in a distribution to their centroid arecomputed. If the method proposed is valid, the average distance to the centroidsis expected to decrease for the fragment based model RF .
3.2 Evaluation of Landmark Transformation Accuracy
Fig. 4 shows the initial WB template R in comparison to the fragment basedmodel RF . In addition to the maximum intensity projections the one, two, andthree standard deviation areas of the transformed landmark distributions arevisualized as ellipses. The numbers identify individual landmarks, annotated inthe fragments. For both cases we registered the individual fragments to the tem-plate. We interpret a lower spread of the mapped positions as an indicator thatthe template is a better representative of the population. The fragment basedmodel provides an improved representation of the fragment data, in particular inthe abdominal region (landmark 32, 47-52). The bar plot in Fig. 5a presents themean distances of the landmarks in a distribution to their centroid. The originalWB template R is shown in blue; the fragment based model RF in red.
In the abdominal region the transformation error decreases for the fragmentbased model in each of the seven landmarks (32, 47-52). The average distanceover all seven landmarks decreases from 8.7 mm to 7.1 mm (-1.6 mm). Landmark52 shows a maximum decrease of -2.58 mm. For the thorax region, the averagedistance shows a decrease for the first four landmarks (29, 30, 31, 33) and anincrease for the remaining four of the eight landmarks (34, 47, 48, 49). Theaccuracy improvement over all thorax landmarks is summarized by an averagetransformation error decrease from 6.23 mm to 6.08 mm (-0.15 mm). The aver-age distance to the center of the landmark distribution in the head fragmentsdecreases for landmark 35, 36, 37, 41 and 42. The average distance of landmark40 and 50 is not effected by the model. Landmark 38 and 39 show an increaseddistance. The accuracy improvement over all head landmarks is summarized byan average transformation error decrease from 3.96 mm to 3.82 mm (-0.14 mm).
Fig. 5b summarizes the average landmark transformation improvementachieved by the fragment based model for each landmark. Values below zero in-dicate that the model performs correct in the region of the respective landmark.

Constructing an Un-biased Whole Body Atlas from Fragments 225
(a) Initial WB template R. (b) Fragment based WB model RF .
Fig. 4. Landmark distributions before and after fragment based un-biased WB tem-plate computation. The ellipses indicate the distribution of landmarks mapped fromall fragments the template. Ideally they should coincide. The fragment based modelimproves the agreement.
35 36 37 38 39 40 41 42 50 29 30 31 33 34 47 48 49 32 52 53 54 55 56 570
5
10
Landmark
AV
G D
ista
nce
to C
entr
oids
(m
m)
(a) Average distance of landmark distributions to their centroids.
(b) Average improvement of landmark transformation accuracy.
Fig. 5. Landmark transformation accuracy of abdominal fragments before and afterfragment based WB template update. (blue: initial WB reference R, red: fragmentbased WB template RF ).
The landmark transformation accuracy is increased for 16 landmarks, remainsthe same for landmark 40 and 50, and decreases for 6 of the 24 landmarks. Thebest results are achieved in the abdominal region.
This increased landmark transformation accuracy indicates that it is feasibleto construct a whole body template from fragments. All fragment positions werelocated reliably during the initial center estimate. The decreased registrationerror of the landmarks shows that the fragment based WB model improves therepresentation of the underlying fragment population. Note that we did notexplicitly evaluate the effect of pathologies present in the fragments at this point.

226 M. Dorfer, R. Donner, and G. Langs
4 Conclusion
We propose methodology for constructing a WBA from fragments. The fragmentbased atlas is motivated by the fact, that typically individual medical imagingdata recorded in hospitals do not cover the entire body region, while their inclu-sion into atlas building is necessary if we aim for a representative model of a largepopulation [2,3]. This is relevant to represent the natural variability for modellearning [3], disease characterization [4], or epidemiological research [9]. Existingapproaches take only examples that cover identical anatomical structures intoaccount (e.g., the brain [4]). The present work overcomes this limitation. Themethod estimates the position as well as the precise mapping between coordi-nates of a fragment and the WB reference fully automatically. In an iterativeprocedure the fragments are registered to a WB template, and this template isupdated to reduce bias. The results show that our approach is feasible if themajority of the data consists of fragments, and reduces bias compared to aninitial WB template.
References
1. Dale, A.M., Fischl, B., Sereno, M.I.: Cortical surface-based analysis – i. segmentationand surface reconstruction. Neuroimage 9, 179–194 (1999)
2. Donner, R., Haas, S., Burner, A., Holzer, M., Bischof, H., Langs, G.: Evaluation offast 2d and 3d medical image retrieval approaches based on image miniatures. In:Muller, H., Greenspan, H., Syeda-Mahmood, T. (eds.) MCBR-CDS 2011. LNCS,vol. 7075, pp. 128–138. Springer, Heidelberg (2012)
3. Guimond, A., Meunier, J., Thirion, J.P.: Average brain models: A convergence study.Computer Vision and Image Understanding 77(2), 192–210 (2000)
4. Joshi, S., Davis, B., Jomier, B.M., Gerig, G.: Unbiased diffeomorphic atlas construc-tion for computational anatomy. Neuroimage 23 (suppl. 1), 151–160 (2004)
5. Modat, M., Ridgway, G.R., Taylor, Z.A., Lehmann, M., Barnes, J., Hawkes, D.J.,Fox, N.C., Ourselin, S.: Fast free-form deformation using graphics processing units.Comput. Methods Prog. Biomed. 98(3), 278–284 (2010)
6. Park, H., Bland, P.H., Meyer, C.R.: Construction of an abdominal probabilistic atlasand its application in segmentation. IEEE TMI 22(4), 483–492 (2003)
7. Rueckert, D., Sonoda, L.I., Hayes, C., Hill, D.L.G., Leach, M.O., Hawkes, D.J.:Nonrigid registration using free-form deformations: application to breast MR im-ages. IEEE TMI 18(8), 712–721 (1999)
8. Sabuncu, M.R., Yeo, B.T.T., Van Leemput, K., Fischl, B., Golland, P.: A GenerativeModel for Image Segmentation Based on Label Fusion. IEEE TMI 29(10), 1714–1729(2010)
9. Sabuncu, M.R., Balci, S.K., Shenton, M.E., Golland, P.: Image-driven populationanalysis through mixture modeling. IEEE TMI 28(9), 1473–1487 (2009)