Liver
26
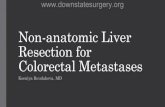
[Alterations in Metabolic and Endocrine Functions] LIVER CIRRHOSIS Precipitating Factors: Predisposing Factor: - Excessive alcohol - LAENNEC’S CIRRHOSIS - Biliary Atresia - Complication of viral, toxic / idiopathic hepatitis - Genetic digestive disorder - POSTNECROTIC CIRRHOSIS - Chronic biliary obstruction and infection - BILIARY CIRRHOSIS - Autoimmune hepatitis - Severe right-sided heart failure 94 Liver Cell Inflammation Activation of Hepatic Expansion of Myofibroblasts- Pool Fibrosis/Scarring of Obstruction of Blood Flow Increased pressure in the venous and sinusoidal channels Portal Splanchnic vascular and Peripheral arterial Effective blood volume Cardiac output SNS Renal Arterial Hepatorenal Splanchnic Lymph Formation of collateral circulation pressure to nearest Esophageal Hypersplenis Caput Hemorrhoids Thrombocytope Anemia Leukopenia Prolonged weakne infectio Increased circulating Jaundic Pain Fever Anorex Nausea & Fatig Increased *Oliguria *Increased BUN and Creatinine levels - azotemia *Increased osmolality and urine
-
Upload
jorie-roco -
Category
Documents
-
view
216 -
download
0
description
medical surgical nursing
Transcript of Liver
[Alterations in Metabolic and Endocrine Functions]LIVER CIRRHOSIS
Precipitating Factors:Predisposing Factor:
- Excessive alcohol - LAENNECS CIRRHOSIS - Biliary Atresia- Complication of viral, toxic / idiopathic hepatitis - Genetic digestive disorder- POSTNECROTIC CIRRHOSIS- Chronic biliary obstruction and infection - BILIARY CIRRHOSIS - Autoimmune hepatitis- Severe right-sided heart failure
PainLiver Cell Injury
Increased WBCs
FeverFatigueInflammation
Nausea & VomitingActivation of Hepatic Stellate cellsAnorexia
Expansion of Myofibroblasts-Pool
Fibrosis/Scarring of the Liver
Obstruction of Blood FlowIncreased pressure in the venous and sinusoidal channels
Portal Hypertension( 10mmHg)
Increased circulating bilirubinSplanchnic vascular and Peripheral arterial vasodilationFormation of collateral circulation
Caput medusae
pressure to nearestsusceptible organ/sorgans
Jaundice
Hemorrhoids
Esophageal varices
Hypersplenism
Splanchnic Lymph production
LeukopeniaAnemiaThrombocytopenia
Prolonged bleedinginfectionweakness
Hepatorenal Syndrome
Effective blood volume decreased
*Oliguria*Increased BUN and Creatinine levels - azotemia*Increased osmolality and urine specific gravity*Low blood sodium*Low urine sodium concentration
Cardiac output decreased
SNS
Renal Arterial Vasoconstriction
Renal blood flowADH
Na+ & WaterRetention
Ascites formationRAAS A BSources:Gressner, O., Weiskirchen, R., & Gressner, A. (2007). Medscape Nurses: Evolving Concepts of Liver Fibrogenesis Provide New Diagnostic and Therapeutic Options. Retrieved March 2015, from http://www.medscape.com/viewarticle/573027.Lewis, S. and et.al. (2008). Medical Surgical Nursing: Assessment and Management of Clinical Problems. Singapore: Mosby Elsevier Inc.Mayo Foundation for Medical Education and Research. (2015). Cirrhosis. Retrieved March 2015, from http://www.mayoclinic.org/diseases-conditions/cirrhosis/basics/causes/con-20031617.Udan, J. (2002). Medical Surgical: Concepts and Clinical Application (First Edition). Philippines: Guiani Prints House.Wolf, D. (2014, December 10). Medscape: Cirrhosis. Retrieved March 2015, from http://emedicine.medscape.com/article/185856-overview.
[Alterations in Metabolic and Endocrine Functions]
A B
Activation of vasoconstrictorsArterial underfilling
Release of endothelin-1 and combines to capillary cellsDecreased bile in Gastrointestinal tract and increase urobilinogen
Clay-colored stools and dark urineNitric oxide secreted causing to vasodilate and increased blood flow
Increased RBC causing insufficient O2 supply and different pressure d/t different pressure in capillary and alveolus
Hepatic Pulmonary Syndrome
*Exhaustion*Fatigue
Decrease ADH & aldosterone detoxificationDecrease androgen and estrogen detoxificationDecrease metabolism of protein and carbohydratesDecreased emulsification of fatsPoor Vitamin K absorption
Edema* Palmar erythema* Testicular atrophy* Gynecomastia* Spider Angiomas* Loss of body hair* Menstrual changesHypoglycemiaMalnutritionOsmotic pressureBleeding tendencies
Inability to metabolize ammonia to urea
Ascites
Ammonia levelsin the bloodBacterial Peritonitis
SepsisBrain edemaAstrocyte swelling Neurotransmitter and receptor alterationAltered brain glucose metabolism
Hepatic Encephalopathy
* Inability to concentrate* Loss of memory* Confusion* Depressed level of consciousness* Asterixis* Foul breath* Respiratory acidosis* Alteration in sleep
DeathHepatic Coma
Sources:Gressner, O., Weiskirchen, R., & Gressner, A. (2007). Medscape Nurses: Evolving Concepts of Liver Fibrogenesis Provide New Diagnostic and Therapeutic Options. Retrieved March 2015, from http://www.medscape.com/viewarticle/573027.Lewis, S. and et.al. (2008). Medical Surgical Nursing: Assessment and Management of Clinical Problems. Singapore: Mosby Elsevier Inc.Mayo Foundation for Medical Education and Research. (2015). Cirrhosis. Retrieved March 2015, from http://www.mayoclinic.org/diseases-conditions/cirrhosis/basics/causes/con-20031617.Udan, J. (2002). Medical Surgical: Concepts and Clinical Application (First Edition). Philippines: Guiani Prints House.Wolf, D. (2014, December 10). Medscape: Cirrhosis. Retrieved March 2015, from http://emedicine.medscape.com/article/185856-overview.
[Alterations in Metabolic and Endocrine Functions]LIVER CIRRHOSISCirrhosis is the final stage attained by various chronic liver diseases after years or decades of slow progression.The liver cells attempt to regenerate, but the regenerative process is disorganized, resulting in abnormal blood vessel and bile duct architecture. The overgrowth of new and fibrous connective tissue distorts the livers normal lobular structure, resulting in lobules of irregular size and shape with impeded blood flow. Eventually, irregular, disorganized regeneration; poor cellular nutrition; and hypoxia caused by inadequate blood flow and scar tissue result in decreased functioning of the liver. Cirrhosis may be having an insidious, prolonged course.[1]
ETIOLOGY AND RISK FACTORSExcessive alcohol (Laennecs Cirrhosis) the first change in the liver from excessive alcohol intake is an accumulation of fat in the liver cells. Uncomplicated fatty changes in the liver are potentially reversible if the person stops drinking alcohol. If the alcohol abuse continues, widespread scar formation occurs throughout the liver.Complication of viral, toxic or idiopathic hepatitis (Postnecrotic Cirrhosis) called as post necrotic cirrhosis. Chronic biliary obstruction and infection due to gallstones, inflammation of bile ducts, trauma, biliary strictures (abnormal narrowing of the ducts), cysts, enlarged lymph nodes, pancreatitis, and injury related to gallbladder or liver surgery, tumors of bile ducts or pancreas, hepatitis, or parasites. (Biliary Cirrhosis) Severe right-sided heart failure in patients with corpulmonale, constrictive pericarditis, and tricuspid insufficiency.[2] Biliary Atresia Genetic digestive disorder Autoimmune hepatitis[3]
1 Wolf, D. (2014, December 10).Medscape: Cirrhosis. Retrieved March 2015, from http://emedicine.medscape.com/article/185856-overview2 Udan, J. (2002).Medical Surgical: Concepts and Clinical Application (First Edition). Philippines: Guiani Prints House.3 Lewis, S. and et.al. (2008). Medical Surgical Nursing: Assessment and Management of Clinical Problems. Singapore: Mosby Elsevier Inc.
[Alterations in Metabolic and Endocrine Functions]PATHOPHYSIOLOGYIn cirrhosis, continuous liver damage can result to cell destruction and fibrosis of hepatic tissues.Fibrosis within the cirrhotic liver obstructs the flow of blood through the liver and to the liver cells. As a result of the obstruction to the flow of blood through the liver, blood backs-up in the portal vein, and the pressure in the portal vein increases, a condition calledportal hypertension. Because of the obstruction to flow and high pressures in the portal vein, blood in the portal vein seeks other veins in which to return to the heart, veins with lower pressures that bypass the liver. Unfortunately, the liver is unable to add or remove substances from blood that bypasses it. It is a combination of reduced numbers of liver cells, loss of the normal contact between blood passing through the liver and the liver cells, and blood bypassing the liver that leads to manyof the manifestations of cirrhosis. In an attempt to reduce the high portal pressure and to reduce the increased plasma volume and lymphatic flow, collateral circulation develops. The common area for collateral circulation includes the veins in the esophagus, anterior abdominal wall, parietal peritoneum and the mesenteric veins in the intestines specifically in the rectum. Varicosities develop in the collateral areas, resulting to esophageal and gastric varices, caput medusa and haemorrhoids. These varices can lead to massive haemorrhage if the varices are being ruptured because of some factors such as acid regurgitation from the stomach, ingestion of coarse food, swallowing of poorly masticated food, and increased abdominal pressure.[4]The spleen normally acts as a filter to remove older red blood cells, white blood cells, and platelets. The blood that drains from the spleen joins the blood in the portal vein from the intestines. As the pressure in the portal vein rises in cirrhosis, it increasingly blocks the flow of blood from the spleen. The blood turns back accumulating in the spleen, and the spleen swells in size, a condition referred to as hypersplenism.[5] Sometimes, the spleen is so enlarged that it causes abdominal pain. As the spleen enlarges, it filters out more and more of the blood cells and platelets until their numbers in the blood are reduced called as thrombocytopenia, leukopenia, anemia and coagulation disorders. The anemia can cause weakness, the leukopenia can lead to infections, and the thrombocytopenia can impair the clotting of blood and result in prolonged bleeding.[6]
4 Lewis, S. and et.al. (2008). Medical Surgical Nursing: Assessment and Management of Clinical Problems. Singapore: Mosby Elsevier Inc.5 Mayo Foundation for Medical Education and Research. (2015). Cirrhosis. Retrieved March 2015, from http://www.mayoclinic.org/diseases-conditions/cirrhosis/basics/causes/con-20031617.6 Wolf, D. (2014, December 10). Medscape: Cirrhosis. Retrieved March 2015, from http://emedicine.medscape.com/article/185856-overview.[Alterations in Metabolic and Endocrine Functions]Some of the protein in food that escapes digestion and absorption is used by bacteria that are normally present in the intestine. While using the protein for their own purposes, the bacteria make substances that they release into the intestine. These substances then can be absorbed into the body. Some of these substances, for example, ammonia, can have toxic effects on the brain. Ordinarily, these toxic substances are carried from the intestine in the portal vein to the liver where they are removed from the blood and detoxified. When cirrhosis is present, blood are not detoxified and ammonia and other substances are present in the systemic circulation. When the toxic substances accumulate sufficiently in the blood, the function of the brain is impaired, a condition called hepatic encephalopathy. Symptoms include irritability, inability to concentrate or perform calculations, loss of memory,confusion, or depressed levels of consciousness, asterixis, foul breath, respiratory acidosis, and alteration in sleep. Hepatic encephalopathy will further complicate to hepatic coma if not well managed that will lead to death.[7]Rarely, some patients with advanced cirrhosis can develop hepatopulmonary syndrome. These patients can experience difficulty breathing because certain hormonesspecifically the endothelin-1, a portent vasoconstrictor, released in advanced cirrhosis cause the lungs to function abnormally. The basic problem in the lung is thatnot enough blood flows through the small blood vessels in the lungs that are in contact with the alveoli of the lungs. Blood flowing through the lungs is shunted around the alveoli and cannot pick up enough oxygen from the air in the alveoli. As a result the patient experiences shortness of breath, particularly with exertion.[8]In uncontrolled multiplication of liver cells for recovery of lost cells, cancer of the liver develops. The most common symptoms and signs of primary liver cancer are abdominal pain and swelling, hepatomegaly,weight loss, and fever.[9]The liver cells and the channels through which bile flows are also affected in cirrhosis. Bile is a fluid produced by liver cells that has two important functions: to aid in digestion and to remove and eliminate toxic substances from the body. The bile that is produced by liver cells is secreted into very tiny channels that run between the liver cells that line the sinusoids, called canaliculi. The canaliculi empty into small ducts which then join together to common bile duct.[10]
7 Gressner, O., Weiskirchen, R., & Gressner, A. (2007).Medscape Nurses: Evolving Concepts of Liver Fibrogenesis Provide New Diagnostic and Therapeutic Options. Retrieved March 2015, from http://www.medscape.com/viewarticle/573027.8 Lewis, S. and et.al. (2008). Medical Surgical Nursing: Assessment and Management of Clinical Problems. Singapore: Mosby Elsevier Inc.9 Mayo Foundation for Medical Education and Research. (2015). Cirrhosis. Retrieved March 2015, from http://www.mayoclinic.org/diseases-conditions/cirrhosis/basics/causes/con-20031617.10 Wolf, D. (2014, December 10). Medscape: Cirrhosis. Retrieved March 2015, from http://emedicine.medscape.com/article/185856-overview.
[Alterations in Metabolic and Endocrine Functions]Ultimately, all of the ducts combine into one duct that enters the small intestine. In this way, bile gets to the intestine where it can help with the digestion of food. At the same time, toxic substances contained in the bile enter the intestine and then are eliminated in the stool. In cirrhosis, the canaliculi are abnormal and the relationship between liver cells and canaliculi is destroyed, just like the relationship between the liver cells and blood in the sinusoids. As a result, obstructive jaundice may also occur and is usually accompanied by pruritus, an accumulation of bile salts underneath the skin. The liver is not able to eliminate toxic substances normally, and they can accumulate in the body. To a minor extent, digestion in the intestine also is reduced. Jaundice occurs as a result of decreased ability to conjugate and excrete bilirubin. If obstruction of the biliary tracts occurs,obstructive jaundice may also occur and is usually accompanied by pruritus, an accumulation of bile salts underneath the skin.[11]Patients with worsening cirrhosis can develop hepatorenal syndrome. This syndrome is a serious complication in which the function of the kidneys is reduced. It is a functional problem in the kidneys, meaning there is no physical damage to the kidneys. Instead, the reduced function is due to changes in the way the blood flows through the kidneys themselves. Due to the portal hypertension along with liver decompensation results in splanchnic and systemic vasodilation and decreased arterial blood volume, renal vasoconstriction occurs and renal failures occur.This syndrome consists of progressive oliguria and azotemia in the absence of structural damage to the kidney. There will be an increase BUN and Creatinine levels in the urinalysis result. There will be also an increase osmolality and urine specific gravity, low blood sodium and low urine sodium concentration due to sodium reabsorption.[12]As cirrhosis of the liver becomes severe, signals are sent to the kidneys to retain salt and water in the body. The excess salt and water first accumulates in the tissue beneath the skin of the ankles and legs because of the effect of gravity when standing or sitting. Thisaccumulation of fluid is called edema or pitting edema. Fluid also may accumulate in the abdominal cavity between the abdominal wall and the abdominal organs. This accumulation of fluid, called ascites causes swelling of the abdomen, abdominal discomfort, and increased weight. When BP is elevated in the liver, proteins move from the blood vessels via the large pores of sinusoids into the lymph space. When the lymphatic system is unable to carry off the excess proteins and water, they leak through the liver capsule into the peritoneal cavity. The osmotic pressure of the proteins pulls additional fluid into the peritoneal cavity. Another mechanism is hypoalbuminemia resulting from inability of the liver to synthesize albumin.[13] The hypoalbuminemia results in
11 Wolf, D. (2014, December 10).Medscape: Cirrhosis. Retrieved March 2015, from http://emedicine.medscape.com/article/185856-overview.12 Gressner, O., Weiskirchen, R., & Gressner, A. (2007).Medscape Nurses: Evolving Concepts of Liver Fibrogenesis Provide New Diagnostic and Therapeutic Options. Retrieved March 2015, from http://www.medscape.com/viewarticle/573027.13 Lewis, S. and et.al. (2008). Medical Surgical Nursing: Assessment and Management of Clinical Problems. Singapore: Mosby Elsevier Inc.
[Alterations in Metabolic and Endocrine Functions]decreased colloidal oncotic pressure. Another mechanism is hyperaldosteronism which occurs when aldosterone is not metabolized by damaged hepatocytes. The increased level of aldosterone causes increased sodium reabsorption by the renal tubules. This retention of sodium as well as the increased in antidiuretic hormone, causes additional water retention. When this ascites will rupture, usually at the abdominal part, this may lead to bacterial peritonitis, sepsis and may progress and lead to death.[14]Several signs and symptoms relating to the metabolism and inactivation of adrenocortical hormones, estrogen and testosterone occur in cirrhosis. When the liver is unable to metabolize the hormones, various manifestations occur. In men, gynecomastia, loss of axillary and pubic hair, testicular atrophy, and impotence with loss of libido may occur as a result of increased estrogen levels. In younger women, amenorrhea may occur, and in older women there may be vaginal bleeding. The liver fails to metabolize aldosterone adequately, resulting in hyperaldosteronism with subsequent sodium and water retention and potassium loss.[15]
Jaclyn Mae T. Alviola, RN MSN Student
14 Lewis, S. and et.al. (2008). Medical Surgical Nursing: Assessment and Management of Clinical Problems. Singapore: Mosby Elsevier Inc.15 Wolf, D. (2014, December 10). Medscape: Cirrhosis. Retrieved March 2015, from http://emedicine.medscape.com/article/185856-overview.
[Alterations in Metabolic and Endocrine Functions]CHOLECYSTITIS
Precipitating factors:- Pregnancy- Diabetes- Tumor surrounding the Gallbladder- Hyperlipidemia- Losing weight rapidly and diet- Obesity- Gallstones- Oral contraceptivesPredisposing factor:- Female (estrogen levels)- Pregnancy - Hormone therapy- Family History- Ethnicity
Bile stasisDecreased contractility of Bile Flow
Contraction of substances present in bile
Precipitation of bile substances
Bile substances will increase in size
Kinking/compression of common bile duct/pancreatic ductStones migrate to gallbladder
Obstruction to gallbladder
Stimulates smooth muscle contraction
RUQ abdominal painIncrease intraluminal pressureObstruction of flow of bile
Increase tension to duodenum
Pain radiates to lower backGallbladder distention
Presence of bile in the circulation
Wall edema
No bile reaches the GIT Collection of soluble bilirubin in the urineImpaired Hepatic uptake of bilirubin
Vascular compromise
Ischemia to Gallbladder
Cholesterol salts in the skin No bile in small intestine for fat digestionDecrease bile in the duodenum
Necrosis to Gallbladder
Invasion of bacteriaDecreased sterobilin Jaundice Escape of bilirubin to GUT
Realease of toxic metabolites into bloodEmulsification of fatsPresence of bile in the urine
Clay-colored stool
ShockPulmonary InsufficiencyAcute renal failureDissemenated Intravascular Coagulation
Nausea and Vomiting Dark yellow urine
Sources:Intuit and Docstoc. (2014). Cholecystitis Pathophysiology. Retrieved March 2015, from http://img.docstoccdn.com/thumb/orig/113462569.png.Mayo Foundation for Medical Educationand Research. (2015). Cholecystitis. Retrieved March 2015, from http://www.mayoclinic.org/diseases-conditions/cholecystitis/basics/symptoms/con-20034277.Nursing Crib. (2015). Pathophysiology of Cholelithiasis/Cholecystitis. Retrieved March 2015, from http://nursing crib.com/pathophysiology/pathophysiology-of-cholelithiasischoleccsytitis/.
[Alterations in Metabolic and Endocrine Functions]CHOLECYSTITIS
Cholecystitisis inflammation of thegallbladder, a small organ near the liverthat plays a part in digesting food. It is usually associated with cholelithiasis. Normally, fluid called bile passes out of thegallbladderon its way to the small intestine. If the flow of bile is blocked, it builds up inside the gallbladder, causing swelling, pain, and possible infection. Cholecystitis may be acute or chronic. These conditions usually occur together.[1]ETIOLOGY AND RISK FACTORSCholecystitis occurs when gallbladder becomes inflamed. Gallbladder inflammation can be caused by gallstones, the result of hard particles that develop in gallbladder from imbalances in the substances in bile such as cholesterol and bile salts. Gallstones can block the cystic duct, the tube through which bile flows when it leaves the gallbladder, causing the bile to build up and resulting in inflammation. Also, it is caused by tumor that may prevent bile from draining out of the gallbladder properly, causing the buildup that can lead to cholecystitis. Kinking or scarring of the bile ducts can cause also blockages that lead to cholecystitis.[2]Risk factors in developing cholecystitis include increasing age, female gender, obesity and rapid weight loss, using hormonal therapies, pregnancy, having diabetes and being Native American or Hispanic.[3]Sometimes the bile duct becomes blocked temporarily. When this occurs repeatedly, it can lead tochronic cholecystitis. This is swelling and irritation that continues over time. Eventually, the gallbladder becomes thick and hard. It also does notstore and release bile as well.[4]PATHOPHYSIOLOGYThe initial event in acute cholecystitis (ACC) is believed to be obstruction to gallbladder drainage. This causes an increase in intraluminal pressure, gallbladder distention, and wall edema that may progress to venous and lymphatic obstruction, ischemia, and necrosis. A number of potential mediators have been identified including cholesterol-supersaturated bile, lysolecithin,phospholipase A, and prostaglandins. Enhanced production of prostaglandins is
1 Mayo Clinic Health Letter-Online Edition. (2014, August 28). Disease and Conditions: Cholecsytitis. Retrieved March 2015, from http://www.mayoclinic.org/diseases-conditions/cholecystitis/basics/symptoms/con-20034277.2 Mayo Foundation for Medical Educationand Research. (2015). Cholecystitis. Retrieved March 2015, from http://www.mayoclinic.org/diseases-conditions/cholecystitis/basics/symptoms/con-20034277.3 Udan, J. Medical Surgical: Concepts and Clinical Application (First Edition). Philippines: Guiani Prints House. (2002).4 Black, J.M., & Hawks, J.H. Medical-Surgical Nursing Clinical Management for Positive Outcomes. Philippines: Elsevier. (2005).
[Alterations in Metabolic and Endocrine Functions]believed to play a key role in mediating inflammation, and agents that reduce prostaglandin production have been shown to block the inflammatory response and reduce the pain of cholecystitis. Bile is sterile in the early stages of acute cholecystitis and infection is believed to be a secondary event. Indeed, although ACC is often considered an infection. The organisms most commonly cultured are enteric bacteria including Escherichia coli, Klebsiella, and Enterococcus.[5]Cholelithiasis develops when the balance that keeps cholesterol, bile salts, and calcium in solution is altered so that precipitation of these substances occurs. Conditions that upset this balance include infection and disturbances in the metabolism of cholesterol. It is known that in patients with cholethiasis, the bile secreted by the liver is supersaturated with cholesterol. The bile in the gallbladder also becomes supersaturated with cholesterol. When bile is supersaturated with cholesterol, precipitation of cholesterol will occur.[6]The main symptom is pain in the upper right side or upper middle of your belly that usually lasts at least 30 minutes. You may feel: Sharp, cramping, or dull pain, steady pain, pain that spreads toyour back or belowyour right shoulder blade. Other symptoms that may occur include: clay-colored stools, steatorrhea, fever, nausea and vomiting, yellowing of skin and whites of the eyes (jaundice), and hronic diarrhea (4 - 10 bowel movements every day for at least 3 months) may be a common symptom of gallbladder dysfunction.[7]
Jaclyn Mae T. Alviola, RN MSN Student
5 Mayo Clinic Health Letter-Online Edition. (2014, August 28). Disease and Conditions: Cholecsytitis. Retrieved March 2015, from http://www.mayoclinic.org/diseases-conditions/cholecystitis/basics/symptoms/con-20034277.6 Black, J.M., & Hawks, J.H. Medical-Surgical Nursing Clinical Management for Positive Outcomes. Philippines: Elsevier. (2005).7 Lewis, S. and et.al. Medical Surgical Nursing: Assessment and Management of Clinical Problems. Singapore: Mosby Elsevier Inc. . (2008).
[Alterations in Metabolic and Endocrine Functions]PANCREATITIS
Damage to pancreatic cellsInflammation of the parenchymaEdema of the pancreas and pancreatic ductActivation of pancreatic enzymes inside pancreasAutodigestion of the pancreasObstruction to the flow of pancreatic enzymeElastaseNecrosis of blood vessels and ductal fibersHemorrhagePhospholipase AFat necrosisCell membrane disruptionLipaseFat NecrosisKalikreinFurther inflammation of pancreasPrecipitating factors:- Alcohol abuse- Drugs (antihypertensives, diuretics, antimicrobials, immunosuppresives, oral contraceptives)- Biliary obstruction- Hypercalcemia- Hypertriglyceridemia- Abdominal trauma- Tumors- IschemiaPredisposing factors:- Genetic/ Family History- Anatomical variantsAcute PancreatitisChronic Pancreatitis
EdemaVascular permeabilitySmooth muscle contractionVasodilationHypoperfusionPeripancreatic exudation or pancreatic ductal leakage
NecrosisPseudocyst
Compresses nearby organsInvasion of bacteria
Constant pain or deep ache in the abdomen which felt in the back Infected necrotic pancreas or abscess
Realease of toxic metabolites into peritoneal space
Ruptured due to trauma to the sac
Realease of toxic metabolites into blood
DEATHHemorrhageShockPulmonary InsufficiencyAcute renal failureDissemenated Intravascular Coagulation
Hypovolemia
Sources:Fisher, T. & Raton, B. (2015, March 16). MedlinePlus: Pancreatic Pseudocyst. Retrieved March 20, 2015, from http://www.nlm.nih.gov/medlineplus/ency/article/000272.htm.Freedman, S. (2013, October).The Merck Manual: Acute Pancreatitis. Retrieved March 2015, from http://www.merckmanuals.com/professional/gastrointestinal_disorders/pancreatitis/acute_pancreatitis.html.Gardner, T. (2014, December 8). Medscape: Acute Pancreatitis. Retrieved March 2015, from http://emedicine.medscape.com/article/181364-overview.Pancreatitis.(2015). InEncyclopdia Britannica.Retrieved from http://www.britannica.com/EBchecked/topic/441022/pancreatitis.
[Alterations in Metabolic and Endocrine Functions]PANCREATITIS
Pancreatitisis a disease in which the pancreas becomes inflamed. Pancreatic damage happens when the digestive enzymes are activated before they are released into the small intestine and begin attacking the pancreas.[1]There are two forms ofpancreatitis: acute and chronic.Acute pancreatitis.Acute pancreatitis is a sudden inflammation that lasts for a short time. It may range from mild discomfort to a severe, life-threatening illness. Most people with acute pancreatitis recover completely after getting the right treatment. In severe cases, acute pancreatitis can result in bleeding into the gland, serious tissue damage, infection, andcystformation. Severe pancreatitis can also harm other vital organs such as theheart,lungs, andkidneys.[2]Chronic pancreatitis.Chronic pancreatitis is long-lasting inflammation of the pancreas. It most often happens after an episode of acute pancreatitis. Heavy alcohol drinking is another big cause. Damage to the pancreas from heavy alcohol use may not cause symptoms for many years, but then the person may suddenly develop severe pancreatitis symptoms.[3]ETIOLOGY AND RISK FACTORSAcute pancreatitis has many causes, such as alcohol abuse, cholelithiasis, abdominal trauma, virus infection, drugs, and metabolic factors. The mechanisms by which these conditions trigger pancreatic inflammation have not been identified.[4]Acute pancreatitis is thought to result from inappropriate intrapancreatic activation of proteases, which causes autodigestion of the pancreas. Exactly how this occurs is unknown.[5]It is thought that alcohol-induced pancreatitis may include a physiochemical alteration of protein that results in plugs that
1 Pancreatitis.(2015).InEncyclopdia Britannica.Retrieved from http://www.britannica.com/EBchecked/topic/441022/pancreatitis..2 Freedman, S. (2013, October).The Merck Manual: Acute Pancreatitis. Retrieved March 2015, from http://www.merckmanuals.com/professional/gastrointestinal_disorders/pancreatitis/acute_pancreatitis.html.3 Lewis, S. and et.al. Medical Surgical Nursing: Assessment and Management of Clinical Problems. Singapore: Mosby Elsevier Inc. . (2008).4 Gardner, T. (2014, December 8). Medscape: Acute Pancreatitis. Retrieved March 2015, from http://emedicine.medscape.com/article/181364-overview.
[Alterations in Metabolic and Endocrine Functions]block the small pancreatic ductules. Biliary pancreatitis occurs when edema or an obstruction blocksthe ampulla of Vater, resulting in reflux of bile into pancreatic ducts or direct injury to the acinar cells.Other causes include the following: hyperlipidemia, which may occur secondary to nephritis, castration, or exogenous estrogen administration, or as hereditary hyperlipidemia, hypercalcemia arising as a result of hyperparathyroidism, cholecystitis and cholelithiasis, familial cases with no definite mechanism defined, pancreatic tumor, pancreatic trauma or pancreatic duct obstruction, such as penetrating or blunt external trauma, intraoperative manipulation, or ampullar manipulation, and pancreatic ductal overdistention during endoscopic retrograde cholangiopancreatography (ERCP), pancreatic ischemia during episodes of hypotensive shock, cardiopulmonary bypass, visceral atheroembolism, or vasculitis, drugs; although azathioprine and estrogens have been directly linked with the disease, many other drugs are believed to have an association (e.g., antibiotics, anticonvulsants, thiazide diuretics, sulfonamides, valproic acid), and ther general causes, such as pancreatic duct obstruction, obesity, duodenal obstruction, viral infection (e.g., mumps), carcinoma, scorpion venom, ERCP, peritoneal dialysis, and factors still to be determined.[5]PATHOPHYSIOLOGYPancreatitis occurs when digestive enzymes produced in your pancreas become activated while inside the pancreas, causing damage to the organ.[6]During normal digestion, the inactivated pancreatic enzymes move through ducts in your pancreas and travel to the small intestine, where the enzymes become activated and help with digestion.[7]
5 Pancreatitis.(2015).InEncyclopdia Britannica. Retrieved from http://www.britannica.com/EBchecked/topic/441022/pancreatitis.6 Udan, J. (2002).Medical Surgical: Concepts and Clinical Application (First Edition). Philippines: Guiani Prints House.7 Ibid
[Alterations in Metabolic and Endocrine Functions]In pancreatitis, the enzymes become activated while still in the pancreas. This causes the pancreas to undergo the process of inflammation. It is thought that alcohol increases the production of digestive enzymes in the pancreas and/or increases the sensitivity to the hormone cholecystokinin (CKK). CCK stimulates the production of pancreatic enzymes. Other and most common pathologic mechanism is autodigestion of the pancreas that may lead to further damage to thepancreas. One possible cause is the reflux of the bile acids into the pancreatic ducts through an open or distended sphincter of Oddi. This causes the enzymes to irritate the cells of your pancreas, causing inflammation and the signs and symptoms associated with pancreatitis.[8]Regardless of the etiology, pancreatic enzymes (including trypsin, phospholipase A2, and elastase) become activated within the gland itself. The enzymes can damage tissue and activate the complement system and the inflammatory cascade, producing cytokines. This process causes inflammation, edema, and sometimes necrosis. In mild pancreatitis, inflammation is confined to the pancreas. In severe pancreatitis, there is significant inflammation, with necrosis and hemorrhage of the gland and a systemic inflammatory response. After 5 to 7 days, necrotic pancreatic tissue may become infected by enteric bacteria.[9]Activated enzymes and cytokines that enter the peritoneal cavity cause a chemical burn and third spacing of fluid; those that enter the systemic circulation cause a systemic inflammatory response that can result in acute respiratory distress syndrome and renal failure. The systemic effects are mainly the result of increased capillary permeability and decreased vascular tone, which result from the released cytokines and chemokines. Phospholipase A2is thought to injure alveolar membranes of the lungs.[10]In about 40% of patients, collections of enzyme-rich pancreatic fluid and tissue debris form in and around the pancreas. In about half, the collections resolve spontaneously. In others, the collections become infected or form pseudocysts. Pseudocysts have a fibrous capsule without an epithelial lining. Pseudocysts may hemorrhage, rupture, or become infected.[11]
8 Pancreatitis.(2015).InEncyclopdia Britannica.Retrieved from http://www.britannica.com/EBchecked/topic/441022/pancreatitis..9 Freedman, S. (2013, October).The Merck Manual: Acute Pancreatitis. Retrieved March 2015, from http://www.merckmanuals.com/professional/gastrointestinal_disorders/pancreatitis/acute_pancreatitis.html.10 Gardner, T. (2014, December 8). Medscape: Acute Pancreatitis. Retrieved March 2015, from http://emedicine.medscape.com/article/181364-overview.11 Fisher, T. & Raton, B. (2015, March 16). MedlinePlus: Pancreatic Pseudocyst. Retrieved March 20, 2015, from http://www.nlm.nih.gov/medlineplus/ency/article/000272.htm.[Alterations in Metabolic and Endocrine Functions]With repeated bouts of acute pancreatitis, damage to the pancreas can occur and lead to chronic pancreatitis. Scar tissue may form in the pancreas, causing loss of function. A poorly functioning pancreas can cause digestion problems and diabetes.[12]Signs and symptoms of pancreatitis may vary, depending on which type you experience.Acute pancreatitis signs and symptoms include: upper abdominal pain, abdominal pain that radiates to your back Abdominal pain that feels worse after eating, nausea and vomiting, tenderness when touching the abdomen. Chronic pancreatitis signs and symptoms include: upper abdominal pain, losing weight without trying, oily, smelly stools (steatorrhea)The following uncommon physical findings are associated with severe necrotizing pancreatitis: cullen sign (bluish discoloration around the umbilicus resulting from hemoperitoneum), Grey-Turner sign (reddish-brown discoloration along the flanks resulting from retroperitoneal blood dissecting along tissue planes); more commonly patients may have a ruddy erythema in the flanks secondary to extravasated pancreatic exudates, and erythematous skin nodules, usually no longer than 1 cm and typically located on extensor skin surfaces; polyarthritis.[13]Pancreatitis can cause serious complications, including: Infection.Acute pancreatitis can make your pancreas vulnerable to bacteria and infection. Pancreatic infections are serious and require intensive treatment, such as surgery to remove the infected tissue.[14] Pseudocyst.Acute pancreatitis can cause fluid and debris to collect in cyst-like pockets in your pancreas. A large pseudocyst that ruptures can cause complications such as internal bleeding and infection,[15] reathing problems.Acute pancreatitis can cause chemical changes in your body that affect your lung function, causing the level of oxygen in your blood to fall to dangerously low levels.[16] Diabetes.Damage to insulin-producing cells in your pancreas from chronic pancreatitis can lead to diabetes, a disease that affects the way your body uses blood sugar.[17] Kidney failure.Acute pancreatitis may cause kidney failure, which can be treated with dialysis if the kidney failure is severe and persistent.[18]
12 Gardner, T. (2015, April 1). Medscape: Acute Pancreatitis. Retrieved April 15, 2015, from http://emedicine.medscape.com/article/181364-overview.13 Ibid14 Ibid15 Fisher, T. & Raton, B. (2015, March 16). MedlinePlus: Pancreatic Pseudocyst. Retrieved March 20, 2015, from http://www.nlm.nih.gov/medlineplus/ency/article/000272.htm.16 Freedman, S. (2013, October).The Merck Manual: Acute Pancreatitis. Retrieved March 2015, from http://www.merckmanuals.com/professional/gastrointestinal_disorders/pancreatitis/acute_pancreatitis.html.17 Ibid18 Ibid
Malnutrition.Both acute and chronic pancreatitis can cause your pancreas to produce fewer of the enzymes that are needed to break down and process nutrients from the food you eat. This can lead to malnutrition, diarrhea and weight loss, even though you may be eating the same foods or the same amount of food.[19] Pancreatic cancer.Long-standing inflammation in your pancreas caused by chronic pancreatitis is a risk factor for developing pancreatic cancer.[20]
Jaclyn Mae T. Alviola MSN Student
19 Gardner, T. (2014, December 8). Medscape: Acute Pancreatitis. Retrieved March 2015, from http://emedicine.medscape.com/article/181364-overview.20 Ibid110