Lister Ios Is

of 6
Transcript of Lister Ios Is
-
8/10/2019 Lister Ios Is
1/6
Listeriosis
Klara M. Posfay-Barbe a,*, Ellen R. Wald b
a Department of Pediatrics, Childrens Hospital of Geneva, University Hospitals of Geneva, 6 rue Willy-Donze, 1211 Geneva 14, Switzerlandb Department of Pediatrics, University of WisconsinMadison, School of Medicine and Public Health, 600 Highland Avenue, Box 4108, Madison, WI 53792, USA
Keywords:
Early-onset sepsis
Late-onset sepsis
Listeriosis
Neonates
Perinatal infection
s u m m a r y
Listeria monocytogenes, a small, facultative anaerobic, Gram-positive motile bacillus, is an important
cause of foodborne illness which disproportionately affects pregnant women and their newborns. Lis-teria infects many types of animals and contaminates numerous foods including vegetables, milk,
chicken and beef. This organism has a unique proclivity to infect the fetoplacental unit with the ability to
invade cells, multiply intracellularly and be transmitted cell-to-cell. The organism possesses several
virulence factors, including internalin A and internalin B, which facilitate the direct invasion of cells. Cell-
to-cell transmission is promoted by the bacterial surface protein ActA which is regulated by a tran-
scriptional activator known as positive regulatory factor A. Both innate and adaptive immune responses
enable the host to eliminate this pathogen. Clinical manifestations of infection in the newborn fall into
the traditional categories of early- and late-onset sepsis. Therapeutic recommendations include ampi-
cillin and gentamicin for 1421 days.
2009 Elsevier Ltd. All rights reserved.
1. Microbiology
Listeria monocytogenesis a small, facultatively anaerobic, Gram-
positive, motile bacillus. It grows well in broth and on blood agar;
some species produce a narrow zone of beta-hemolysis.1 In clinical
specimens, the organism may be Gram-variable and look like cocci,
diplococci, or diphtheroids, thereby misleading the laboratory
technician. The organism tolerates low temperatures as well as
high pH and high salt concentrations, which allow it to replicate in
soil, water, sewage, manure, animal feed, and contaminated
refrigerated foods. It can survive many months in soil and 2030
days in tap water. Although persisting on environmental surfaces,
pasteurization and most disinfecting agents eliminateListeria.
Only four of the seven species ofListeria infect humans. Most
diseases are due to three primary serotypes: 1a, 1b and 4b. The last
is responsible for almost all outbreaks of listeriosis.2
2. Epidemiology
Listeria spp. are distributed worldwide, but human illness is
reported most frequently in developed countries. Listeria spp. are
an important cause of zoonoses, infecting many types of animals
(domestic pets, livestock, other mammals, rodents, amphibians,
fish, and arthropods) and more than 17 avian species. In
mammals,L. monocytogenes can cause spontaneous abortions and
is the cause of circling disease, a manifestation of basilar
meningitis in which animals move incessantly in a circle. Fecal
oral transmission is the probable means by which organisms are
spread in animals. The pathogen can be transmitted directly from
animals to humans and has been documented in veterinarians,
farmers, and abattoir workers. Vertical transmission from mother
to neonate occurs transplacentally or through an infected birth
canal. Cross-infection in a neonatal unit through contact with
contaminated mineral oil used to bathe infants led to one noso-
comial outbreak.3
Most cases of listeriosis appear to be foodborne, including those
acquired during pregnancy. Many foods can be contaminated by L.
monocytogenes, including raw vegetables, raw milk, fish, poultry,
processed chicken, and beef. Approximately 1570% of hot dogs are
reported to be contaminated withListeriaspp.Listeriaspp. also are
found in the stools ofw5% of healthy adults.4 The infectious dose isestimated to be 104106 organisms per gram of ingested product
but may be lower in immunocompromised hosts and patients who
have diminished gastric acidity or have undergone ulcer surgery.5
The incubation period has not been well-established, but is esti-
mated to be three weeks.
The first clearly documented foodborne (coleslaw) outbreak
was in Nova Scotia in 1981.5 It was associated with a case fatality
of 27%. In other sporadic outbreaks, 11% of all food samples
retrieved from the refrigerator were contaminated, and 64% of the
refrigerators of patients contained at least one contaminated food
item.2* Corresponding author. Tel.: 41 22 382 5462; fax: 41 22 382 5490.
E-mail address: [email protected](K.M. Posfay-Barbe).
Contents lists available atScienceDirect
Seminars in Fetal & Neonatal Medicine
j o u r n a l h o m e p a g e : w w w . e l s e v i e r . c o m / l o c a t e / s i n y
1744-165X/$ see front matter 2009 Elsevier Ltd. All rights reserved.
doi:10.1016/j.siny.2009.01.006
Seminars in Fetal & Neonatal Medicine 14 (2009) 228233
mailto:[email protected]://www.sciencedirect.com/science/journal/1744165Xhttp://www.elsevier.com/locate/sinyhttp://www.elsevier.com/locate/sinyhttp://www.sciencedirect.com/science/journal/1744165Xmailto:[email protected] -
8/10/2019 Lister Ios Is
2/6
-
8/10/2019 Lister Ios Is
3/6
was the first identified virulence factor ofL. monocytogenesand is
required for bacterial escape from endocytic vacuoles. LLO-defec-
tive strains are five to 10 times less invasive than wild-type
strains.22 LLO is required in vivo for bacterial growth in tropho-
blastic cells, and for subsequent fetal invasion.8 It is also known as
a modulator of the innate immune response by inducing new
cytokine synthesis in different immune cells and activating
different immune-response-associated pathways, such as the NF-
kappaB pathway.23 The mechanisms behind this activation process
are, however, still unclear.
3.3. Cell-to-cell transmission
Once in the cytoplasm, listeria multiplies rapidly, migrates to the
host cell periphery and into cell-wall protrusions, which will be
taken up and ingested by neighboring cells where a new cycle will
start again (Fig. 1). This migration to the surface of the hosts cell
depends on ActA, a bacterial surface protein.
3.3.1. ActA
ActA is a virulence factor required for cell-to-cell spread of lis-
teria. It uses components of the host cells actin cytoskeleton to
generate a comet-tail which is rich in actin, enabling bacterialpropulsion in the cytosol leading to the infection of uninfected
neighbor cells.24 Strains lacking ActA retain the ability to grow in
the placenta although at a lower rate than wild-type strains but
arestronglycurtailed in their ability to spread from cell to cell.8 This
was demonstrated in an animal model, in which neonatal mice
injected with an isolate ofL. monocytogenes lacking ActA induced
a strong primary and secondary Th1 CD4 and CD8 T-cell response,
but were protected against death from infection with listeria.
Interestingly, motility can be conferred upon other non-motile
micro-organisms (such asL. innocua) by adding ActA.25
3.3.2. Positive regulatory factor A
The expression of nearly all bacterial gene products that
contribute to the survival and virulence of L. monocytogenes,including LLO and ActA, are regulated by a transcriptional activator
known as positive regulatory factor A (PrfA). Strains lacking func-
tional PrfA are not virulent. The effect of PrfA seems to be reduced
at low temperature, but increased at low pH, probably explaining
the increased virulence of strains in a warm, acidic environment
after oral ingestion.26,27 Post-transcriptional mechanisms control-
ling PrfA expression have also been described and contribute to the
synthesis of Int1A, Int1B, and LLO.11
In summary, it is currently believed that: In1A (especially) and
In1B play a key role in the entry of listeria into host cells; LLO
punches holes to allow the organism to multiply inside the cyto-
plasm of the host cell; ActA produces a rocket-like mechanism to
penetrate into neighboring cells; and that all these mechanisms are
co-ordinated by PrfA. New virulence factors forL. monocytogenesaswell as genes involved in virulence or stress-response are described
regularly, increasing the complexity of the bacteriums pathoge-
nicity and its regulatory mechanisms.28
4. Immunology
4.1. Innate and adaptive immune response
L. monocytogenes has been used for decades as a model
organism to study innate and adaptive immune responses against
intracellular pathogens. The innate immune response is immediate
and involves multiple cellular types, cytokines, and bactericidal
effector mechanisms. Monocytes and resident macrophages,
Kupffer cells for example, are known to ingest and destroy listeria.
Production of cytokines, such as interleukin (IL)-1, IL-6, and tumor
necrosis factor (TNF)-a are central in decreasing susceptibility to
disease by recruiting neutrophils. On the other hand, the adaptive
immune response against infection induced by L. monocytogenes
peaks about one week after infection, and is mainly a CD8 T-cell
response. This response has twomain functions: the specific lysis of
infected cells and rapidproduction of IFN-g in response to IL-12 and
IL-18.29 It is now hypothesized that early IFN-gproduction leads to
an accelerated formation of granulomas at sites of infection,
thereby walling off the infection. In mouse strains of listeria that
do not elicit an early IFN-gresponse, acute inflammation continues
and listeria spreads between cells. Clearance ofL. monocytogenesis
believed to be mediated through a Th1 immune response. IFN-gis
a crucial contributor to the Th1 response by activating macro-
phages, increasing antigen presentation via the MHC class I and II
pathways, and by inhibiting the expansion of Th2 cells.30
A number of research groups have been focused on describing
the cells which produce IFN-g in infections caused by L. mono-
cytogenes. It seems likely that several cells, including natural killer
(NK) cells, dendritic cells during the early phase of innate immu-
nity, antigen-specific CD4 TH1 cells,and effector and memory CD8
T-cells during the later phase of adaptive immunity, produce IFN-g
during infection.29,31 Tocomplicate ourunderstanding of the role ofIFN-gin listerial infection, it appears that IFN-gboth promotes the
control of bacterial replication and also induces (paradoxically), the
erosion of CD8 T-cell memory during infection, thereby impairing
subsequent protective mechanisms.32 In summary, IFN-g plays
a critical role in both innate and adaptive immune responses to L.
monocytogenes.
4.2. Toll-like receptors and autophagy
Toll-like receptor (TLR) 2 and TLR5 have been reported to
recognize L. monocytogenes.33 TLR recognition of listerias lip-
oteichoic acid, lipoproteins, peptidoglycans and flagellin leads to
the production of cytokines which inturn directly activate innate
effectors and recruit other cells.34,35 Interestingly, however, ina murine model in which animals lack myeloid differentiation
factor 88 (MyD88), an adaptor molecule downstream from TLRs, it
was shown that the animals are highly susceptible to infectionwith
listeria and that a MyD88-independent innate and adaptive
immune response exists.36
Macro-autophagy, also referred to as autophagy, is a recently
described mechanism involved in the immune response of
mammals to micro-organisms.37 Briefly, through autophagy, an
infected cell can target an invading micro-organism and restrict its
growth by destroying it in the lysosome. It then induces an adaptive
immune response via presenting peptides on MHC Class I and II
molecules. Recent studies have shown that autophagy targets L.
monocytogenes before bacterial escape into the cytosol. However,
listeria is capable of using alternate strategies, including ActA-dependent polymerization mentioned earlier, to avoid
destruction.38
4.3. Specific relation to immunology of pregnant woman and child
The maternal immune system faces an important challenge
during pregnancy, i.e. to prevent rejection of the semi-allogenic
fetus and to protect itself and also the fetus from infection. Many
observations suggest that pregnancy is associated with a shift from
Th1 to Th2 cellular response and that the maternal immune system
is biased toward humoral immunity and away from cell-mediated
immunity (that could be harmful to the fetus). However, these
changes appear mostly to occur locally, as there is no strong
evidence suggesting that the maternal immune system is
K.M. Posfay-Barbe, E.R. Wald / Seminars in Fetal & Neonatal Medicine 14 (2009) 228233230
-
8/10/2019 Lister Ios Is
4/6
compromised overall during pregnancy. New immunomodulating
mechanisms, not specific to L. monocytogenes, have been studied
extensively and are reviewed elsewhere.39,40 L. monocytogenes, on
the other hand, has to develop different strategies against the
defence mechanisms of the host to survive. While some of these
defences are not specific to pregnancy, such as gastric acidity, lis-
teria has mastered manipulating the differences related to the
immaturity of the immune system of the fetus. Neonatal immunity
is reported to be Th2-biased. This avoids maternal rejection of fetal
antigens induced by Th1-type inflammation that may result in
spontaneous abortion or premature delivery.41 Furthermore, it
appears that (murine) neonates have a lower expression of
mannose-binding lectins and certain TLRs than adults.42 These
mediators are necessary to develop Th1 immune responses and
might explainwhy neonates are highly susceptible to infectionwith
listeria. This fact has been questioned by others who believe that it
is not a decreased expression of TLRs, but instead a TLR-induced
TNF-a production which is significantly decreased in neonates.43
Interestingly, the same authors acknowledge that neonates are
capable of a robust IL-6 production, indicating that the intrinsic TLR
pathway is functional at birth, and suggesting an abnormal, still
unclear, TLR defect related to Th2.
L. monocytogenes can also gain access to the neonate via oralexposure during the passage through the birth canal. Enteric anti-
microbial peptides derived from Paneth cells provide protection
from intestinal infection. However, these cells are not present
during the first weeks of life. Recently, Menard et al. described an
antimicrobially active form of peptide, called CRAMP (cathelin-
related antimicrobial peptide), in the epithelium of neonatal mice,
which is expressed constitutively during the first weeks of life
only.44 CRAMP provides significant protection against bacterial
growth in the gut. This developmental switch in innate immune
effector expression (i.e. CRAMP being functional only while Paneth
cells are lacking) is a newly described mechanism in the early
protection against infection with listeria. Enhanced understanding
of the specificity of the immune system in neonates may lead to
novel treatment strategies in years to come.
5. Neonatal disease
Worldwide,L. monocytogenesis one of the three major causes of
meningitis in neonates. Clinical manifestations may be very similar
to those seen with group B streptococcal disease, and there is a high
fatality rate (350%). There are two forms of neonatal listeriosis.
5.1. Early onset
The mothers of affected children often have a flu-like illness
a few days before delivery, which may be preterm. Listeria
bacteremia presents with an acute febrile illness, which is often
accompanied by myalgias, arthralgias, backache and headache.Maternal illness is observed most often in the third trimester.
Neonatal death and stillbirth occur in approximately one-fifth of
maternal infections. Two-thirds of the infants who survive delivery
to a woman who experiences listeriosis in pregnancy will develop
neonatal infection. The infants are believed to be infected in utero
because of the bacteremic phase of their mothers, but ascending
infections have been described. The highest concentrations of L.
monocytogenes are found in the lung and gut, suggesting that
infection also can be acquired in utero via inhalation and ingestion
of infected amniotic fluid as well as via the hematogenous route.
During labor, brown-stained amniotic fluid is seen and maternal
fever may be present. Serotypes 1a and 1b are most common.
The mean onset of symptomsis 1.5 days after birth. A sepsis-like
picture predominates, but other common manifestations are acute
respiratory distress, pneumonia, and more rarely, meningitis or
myocarditis. Strategies implemented to prevent group B strepto-
coccal sepsis in the newborn may have secondarily decreased the
rate of early-onset listerial infection.
Granulomatosis infantisepticum is a widely disseminated
granuloma characteristic of severe listerial disease. The lesions are
more common in the liver, skin and placenta, but also appear in the
brain, adrenal glands, spleen, kidney, lungs and gastrointestinal
tract. Aspiration of infected fluid can contribute to acute respiratory
failure and hemodynamic compromise in the neonate.
5.2. Late onset
This form of neonatal listeriosis is less common than the early-
onset form, but it occurs more frequently in term infants who are
the products of uncomplicated pregnancies. The babies are healthy
at birth, and the maternal history is usually normal. The first
manifestations of infection appear several days to weeks after birth,
with a mean onset of illness at 14.3 days after birth. The clinical
manifestation in this group is more likely to be meningitis than
sepsis, but it can be subtle, with fever, irritability, anorexia, diar-
rhea, and lethargy. Postpartum transmission is assumed to occur
either during delivery or nosocomially. Serotype 4b is mostfrequent in late-onset disease.
6. Diagnosis
Listeriosis usually presents with leukocytosis, but unlike its
name, rarely with monocytosis. Isolation of Listeria spp. from
a normally sterile site defines the disease. Thirty-six hours of
incubation usually are necessary for sufficient growth for identifi-
cation. The pathogen often is observed on the Gram stain of the
meconium of infected newborns. Carriage in the gastrointestinal
tracts of older children may be common but difficult to demon-
strate because the organism is fastidious and normal flora are
plentiful. Screening of rectal or vaginal cultures is not clinically
useful.Cold enrichment is not as good as selective media to isolate the
organism from specimens containing multiple species (e.g. in food
or stools). Rapid detection tests are based on the use of either
monoclonal antibodies or nucleic acid hybridizations, but they only
identify the genus Listeria.45
When the central nervous system is infected, cerebrospinal fluid
(CSF) is usually purulent, with leukocyte counts of 10010 000/mL
(0.110 109/L). Polymorphonuclear leukocytes predominate in
70% of cases, but the severity of the inflammatory response does
notcorrelate with the prognosis. The Gram stain of CSFis positive in
-
8/10/2019 Lister Ios Is
5/6
L. monocytogenes can multiply within macrophages, several
prerequisites must be fulfilled to inhibit these hidden bacteria.
Antibiotics must penetrate into and distribute within host cells and
remain stable within this environment. Recommmendations are
based on data obtained from in-vitro susceptibility testing, animal
models, and clinical experience with small numbers of patients
who were compared with historic controls.
No controlled trials have established a drug of choice or duration
of therapy for listeriosis. L. monocytogenes is sensitive in vitro to
penicillin G, ampicillin, erythromycin, sulfamethoxazole, trimeth-
oprim, chloramphenicol, rifampin, tetracyclines, and aminoglyco-
sides. Bactericidal antibiotics include sulfamethoxazole,
trimethoprim, and aminoglycosides. Gentamicin and tobramycin
have been reported to have greater in-vitro activity than strepto-
mycin, kanamycin, and amikacin. Listeria always are resistant to
cephalosporins.48 Chloramphenicol should not be used because of
unacceptable failure and relapse rates, and quinolones do not havegood in-vitro activity. Ampicillin, which is superior to penicillin,
and gentamicin have shown synergistic effects in some studies.48
Accordingly, gentamicin with ampicillin is recommended for
treatment of listerial meningitis.
If the patient is allergic to ampicillin or gentamicin, sulfame-
thoxazole-trimethoprim is recommended because it is bactericidal
and reaches adequate levels in the serum and CSF.48 No systematic
study has examined the duration of therapy, but the current
recommendations are 1421 days of treatment for meningitis due
toL. monocytogenes.
8. Prevention
There is no vaccine for listeria infection. Dietary recommenda-
tions for preventing foodborne listeriosis were established by the
Centers for Disease Control and Prevention (CDC) in 1992. They are
similar to those for other foodborne illnesses and include thorough
cooking of raw food from animal sources; washing of raw vegeta-
bles; avoidance of unpasteurized dairy products; keeping uncooked
meats separate from vegetables; washing hands, knives, and
cutting boards after exposure to uncooked food; and regular
cleaning and disinfection of the insides of refrigerators. Persons at
high risk for listeriosis should avoid soft cheeses, reheat (until
steaming hot) leftover and ready-to-eat foods, and avoid cold cuts if
unable to reheat them thoroughly.
TheUS Department of Agriculture began surveillance in 1989 for
L. monocytogenes in ready-to-eat processed meats and enforced
regulations prohibiting the sale of contaminated meats. Since then,
the number of cases of listerial infection has dropped substantially.
The CDCs Division of Foodborne, Bacterial and Mycotic Diseases
tracks the annual incidence of certain foodborne illnesses,
including listeria, in 10 states through Food Net Surveillance.49
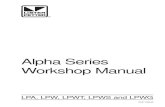
Between 1996 and 2006, the incidence of listeria declined by 36%,
although an outbreak in 2002, related to contaminated turkey
meat, resulted in 54 illnesses, eight deaths and three fetal deaths in
nine states (Fig. 2).49
References
1. Swaminathan B, Hayes PS, Przybyszewski VA, Plikaytis BD. Evaluation ofenrichment and plating media for isolating Listeria monocytogenes. J Assoc Off
Anal Chem 1988;71:6648.2. Pinner RW, Schuchat A, Swaminathan B, et al. Role of foods in sporadic liste-
riosis. II. Microbiologic and epidemiologic investigation. The Listeria StudyGroup. J Am Med Assoc1992;267:204650.
3. Schuchat A, Lizano C, Broome CV, Swaminathan B, Kim C, Winn I. Outbreak ofneonatal listeriosis associated with mineral oil. Pediatr Infect Dis J 1991;10:1839.
4. Schlech III WF. Foodborne listeriosis. Clin Infect Dis2000;31:7705.5. Schlech III WF. Listeria gastroenteritis old syndrome, new pathogen.N Engl J
Med1997;336:1302.
6. Kaur S, Malik SV, Vaidya VM, Barbuddhe SB. Listeria monocytogenes in spon-taneous abortions in humans and its detection by multiplex PCR. J ApplMicrobiol2007;103:188996.
7. Redline RW, Lu CY. Specific defects in the anti-listerial immune response indiscrete regions of the murine uterus and placenta account for susceptibility toinfection. J Immunol 1988;140:394755.
8. Le Monnier A, Autret N, Join-Lambert OF, et al. ActA is required for crossing ofthe fetoplacental barrier by Listeria monocytogenes. Infect Immun 2007;75:9507.
9. DOrazio SE, Troese MJ, Starnbach MN. Cytosolic localization of Listeria mono-cytogenestriggers an early IFN-gamma response by CD8 T cells that correlateswith innate resistance to infection. J Immunol 2006;177:714654.
10. Seveau S, Pizarro-Cerda J, Cossart P. Molecular mechanisms exploited by Lis-teria monocytogenes during host cell invasion. Microbes Infect2007;9:116775.
11. Gray MJ, Freitag NE, Boor KJ. How the bacterial pathogenListeria monocytogenesmediates the switch from environmental Dr. Jekyll to pathogenic Mr. Hyde.Infect Immun 2006;74:250512.
12. Hamon M, Bierne H, Cossart P. Listeria monocytogenes: a multifaceted model.Nat Rev Microbiol 2006;4:42334.
13. Lecuit M, Dramsi S, Gottardi C, Fedor-Chaiken M, Gumbiner B, Cossart P.A single amino acid in E-cadherin responsible for host specificitytowar ds the h uman p athogen Listeria monocytogenes. EMBO J 1999;18:395663.
14. Pentecost M, Otto G, Theriot JA, Amieva MR.Listeria monocytogenesinvades theepithelial junctions at sites of cell extrusion. PLoS Pathog2006;2:e3.
15. Lecuit M, Nelson DM, Smith SD, et al. Targeting and crossing of the humanmaternofetal barrier by Listeria monocytogenes: role of internalin interactionwith trophoblast E-cadherin. Proc Natl Acad Sci USA 2004;101:61527.
16. Bonazzi M, Veiga E, Cerda JP, Cossart P. Successive post-translational modifi-cations of E-cadherin are required for InlA-mediated internalisation ofListeriamonocytogenes. Cell Microbiol 2008; 10: 220822.
17. Jacquet C, Doumith M, Gordon JI, Martin PM, Cossart P, Lecuit M. A molecularmarker for evaluating the pathogenic potential of foodborne Listeria mono-cytogenes. J Infect Dis 2004;189:2094100.
18. Bakardjiev AI, Stacy BA, Fisher SJ, Portnoy DA. Listeriosis in the pregnant guineapig: a model of vertical transmission. Infect Immun 2004;72:48997.
19. Shen Y, Naujokas M, Park M, Ireton K. InIB-dependent internalization of Listeriais mediated by the Met receptor tyrosine kinase. Cell 2000;103:50110.
2.0
1.0
0.5
0.4
1996-1998
1999 2000 2001 2002 2003
Year
Relative
rate(logscale)
2004 2005 2006 2007
0.9
0.8
0.7
0.6
Fig. 2. Relative rates of laboratory-confirmed infections with listeria compared with
19961998 rates, by year (Foodborne Diseases Active Surveillance Network, USA,
19962007).
Research directions
To understand better how this quiet saprophyte
becomes a deadly agent.
To determine the infectious dose of listeria and to define
the extent of human illness by searching for listeria inoutbreaks of febrile gastroenteritis where no other
pathogens are identified.
To identify new bacterial and host effectors.
To examine interaction and activation processes
between bacteria and host, especially in vulnerable
populations, such as neonates.
K.M. Posfay-Barbe, E.R. Wald / Seminars in Fetal & Neonatal Medicine 14 (2009) 228233232
-
8/10/2019 Lister Ios Is
6/6
20. Greiffenberg L, Goebel W, Kim KS, et al. Interaction of Listeria monocytogeneswith human brain microvascular endothelial cells: InlB-dependent invasion,long-term intracellular growth, and spread from macrophages to endothelialcells.Infect Immun 1998;66:52607.
21. Sabet C, Lecuit M, Cabanes D, Cossart P, Bierne H. LPXTG protein InlJ, a newlyidentified internalin involved inListeria monocytogenesvirulence.Infect Immun2005;73:691222.
22. Dramsi S, Cossart P. Listeriolysin O-mediated calcium influx potentiates entry ofListeria monocytogenes into the human Hep-2 epithelial cell line. Infect Immun2003;71:36148.
23. Park JM,Ng VH,Maeda S,RestRF,Karin M.AnthrolysinO andother gram-positivecytolysins are toll-like receptor 4 agonists. J Exp Med2004;200:164755.
24. Portnoy DA, Auerbuch V, Glomski IJ. The cell biology ofListeria monocytogenesinfection: the intersection of bacterial pathogenesis and cell-mediated immu-nity. J Cell Biol 2002;158:40914.
25. Kocks C, Marchand JB, Gouin E, et al. The unrelated surface proteins ActA ofListeria monocytogenesand IcsA ofShigella flexneriare sufficient to confer actin-based motility on Listeria innocua and Escherichia coli respectively. Mol Micro-biol 1995;18:41323.
26. Johansson J, Mandin P, Renzoni A, Chiaruttini C, Springer M, Cossart P. An RNAthermosensor controls expression of virulence genes in Listeria mono-cytogenes.Cell 2002;110:55161.
27. Ferreira A, Sue D, OByrne CP, Boor KJ. Role ofListeria monocytogenes sigma(B) insurvival of lethal acidic conditions and in the acquired acid tolerance response.
Appl Environ Microbiol2003;69:26928.28. Chaturongakul S, Raengpradub S, Wiedmann M, Boor KJ. Modulation of stress
and virulence in Listeria monocytogenes. Trends Microbiol2008;16:38896.29. Berg RE, Crossley E, Murray S, Forman J. Memory CD8T cells provide innate
immune protection against Listeria monocytogenes in the absence of cognateantigen.J Exp Med 2003;198:158393.
30. Pamer EG. Immune responses to Listeria monocytogenes. Nat Rev Immunol2004;4:81223.
31. Plitas G, Chaudhry UI, Kingham TP, Raab JR, DeMatteo RP. NK dendritic cells areinnate immune responders to Listeria monocytogenes infection. J Immunol2007;178:44116.
32. Dudani R, Murali-Krishna K, Krishnan L, Sad S. IFN-gamma induces the erosionof preexisting CD8 T cell memory during infection with a heterologous intra-cellularbacterium. J Immunol 2008;181:17009.
33. Torres D, Barrier M, Bihl F, et al. Toll-like receptor 2 is required for optimalcontrol ofListeria monocytogenes infection. Infect Immun 2004;72:21319.
34. Hayashi F, Smith KD, Ozinsky A, et al. The innate immune response to bacterialflagellin is mediated by Toll-like receptor 5. Nature 2001;410:1099103.
35. Machata S, Tchatalbachev S, Mohamed W, Jansch L, Hain T, Chakraborty T.Lipoproteins of Listeria monocytogenes are critical for virulence and TLR2-mediated immune activation. J Immunol 2008;181:202835.
36. Way SS, Kollmann TR, Hajjar AM, Wilson CB. Cutting edge: protective cell-mediated immunity to Listeria monocytogenes in the absence of myeloiddifferentiation factor 88. J Immunol 2003;171:5337.
37. Kirkegaard K, Taylor MP, Jackson WT. Cellular autophagy: surrender, avoidanceand subversion by microorganisms. Nat Rev Microbiol 2004;2:30114.
38. Birmingham CL,Canadien V, Gouin E, et al. Listeria monocytogenes evades killingby autophagy during colonization of host cells. Autophagy2007;3:44251.
39. Poole JA, Claman HN. Immunology of pregnancy. Implications for the mother.Clin Rev Allergy Immunol 2004;26:16170.
40. Seavey MM, Mosmann TR. Immunoregulation of fetal and anti-paternalimmune responses. Immunol Res2008;40:97113.
41. Adkins B, Leclerc C, Marshall-Clarke S. Neonatal adaptive immunity comes ofage. Nat Rev Immunol 2004;4:55364.
42. Byun HJ, Jung WW, Lee JB, et al. An evaluation of the neonatal immune systemusing a listeria infection model. Neonatology2007;92:8390.
43. Levy O, Coughlin M, Cronstein BN, Ry RM, Desai A, Wessels M. The adenosinesystem selectively inhibits TLR-mediated TNF-a production in the humannewborn. J Immunol 2006;144:195666.
44. Menard S, Forster V, Lotz M, et al. Developmental switch of intestinal antimi-crobial peptide expression. J Exp Med 2008;205:18393.
45. Sontakke S, Farber JM. The use of PCR ribotyping for typing strains ofListeriaspp. Eur J Epidemiol 1995;11:66573.
46. Dalton CB, Austin CC, Sobel J, et al. An outbreak of gastroenteritis and fever dueto Listeria monocytogenes in milk. N Engl J Med 1997;336:1005.
47. Marget W, Seeliger HP. Listeria monocytogenes infections therapeutic possi-bilities and problems. Infection 1988;16:S1757.
48. Espaze EP, Reynaud AE. Antibiotic susceptibilities ofListeria: in vitro studies.Infection1988;16:S1604.
49. Anonymous. Preliminary foodnet data on the incidence of infection withpathogens transmitted commonly through food 10 states, 2007.MMWR MorbMortal Wkly Rep2008;57:36670.
K.M. Posfay-Barbe, E.R. Wald / Seminars in Fetal & Neonatal Medicine 14 (2009) 228233 233