Lipids: Is Lower Better For Diabetic Patients? Prof. Samir Helmy Assaad -Khalil Department of...
22
Lipids: Is Lower Better For Diabetic Patients ? Prof. Samir Helmy Assaad -Khalil Department of Internal Medicine Unit of Diabetes, Lipidology & Metabolism Alexandria University, Alexandria, Egypt MGSD Morocco; Friday, April 29, 2011
-
Upload
miles-obrien -
Category
Documents
-
view
215 -
download
0
Transcript of Lipids: Is Lower Better For Diabetic Patients? Prof. Samir Helmy Assaad -Khalil Department of...

Lipids: Is Lower Better For Diabetic Patients?
Prof. Samir Helmy Assaad -KhalilDepartment of Internal Medicine
Unit of Diabetes, Lipidology & Metabolism
Alexandria University, Alexandria, Egypt
MGSD Morocco; Friday, April 29, 2011

Agenda
Epidemiological data EBM derived from clinical trials Evidence in patients with T2DM What is Desirable Cholesterol?

Elevated Cholesterol Is a Risk Factor for Cardiovascular Disease (CVD)
Elevated serum cholesterol is associated with increasedrisk of1–3
CHD Reinfarction CVD mortality4
All-cause CHD Stroke
CHD=coronary heart disease; MRFIT=Multiple Risk Factor Intervention Trial.
1. Kannel WB. Am J Cardiol. 1995;76:69C–77C; 2. Anderson KM et al. JAMA. 1987;257:2176–2180; 3. Kannel WB et al. Ann Intern Med. 1971;74:1–12; 4. Neaton JD et al. Arch Intern Med. 1992;152:1490–1500.
0
10
20
30
40
50
<160(4.13)
160–199(4.13–5.14)
200–239(5.17–6.18)
240(6.20)
CV
D M
ort
alit
y R
atea
MRFIT (N=350,977)4
Serum Cholesterol,
mg/dL (mmol/L)

Correlation Between LDL-C & Cardiovascular
Mortality: The Framingham Study1
aNs refer to person-years.1. Wilson PWF et al. Circulation. 1998;97:1837–1847.
<130 mg/dL(<3.4 mmol/L)
(n=11,142a) (n=10,384a) (n=8,628a)(n=15,835a) (n=10,455a) (n=11,767a)
7.3
2.3
0
5
10
15
20
Ag
e A
dju
sted
10-
Yea
r D
eath
R
ates
, %
of
Po
pu
lati
on
Men
Women
130–159 mg/dL(3.4–4.11 mmol/L)
≥160 mg/dL(≥4.14 mmol/L)
11.3
6.5
17.3
10.6

Log Linear Relationship Between LDL-C and Relative Risk of CHD1
CHD=coronary heart disease.
Log-linear relationship between LDL-C levels and relative risk of CHD. This relationship is consistent with a large body of epidemiologic data and with data available from clinical trials of LDL-lowering therapy. These data suggest that for every 30 mg/dL change in LDL-C, the relative risk of CHD is changed in proportion by about 30%. The relative risk is set at 1.0 for LDL-C=40 mg/dL.
1. Grundy SM et al. Circulation. 2004;110:227–239.
Reprinted with permission ©2004, American Heart Association, Inc.
Rel
ativ
e R
isk
of
CH
D,
Lo
g S
cale
0
3.7
2.9
2.2
1.3
1.7
LDL-C, mg/dL (mmol/L)
40(1.0)
100(2.6)
130(3.4)
160(4.1)
190(4.9)
70(1.8)
1.0

Is Lower LDL-C Better?1
CHD=coronary heart disease.
1. Grundy SM et al. Circulation. 2004;110:227–239.
Reprinted with permission ©2004, American Heart Association, Inc.
1
3.7
2.9
2.2
1.3
1.7
Rel
ativ
e R
isk
of
CH
D,
Lo
g S
cale –30 mg/dL
–30% CHD risk
40(1.0)
100(2.6)
130(3.4)
160(4.1)
190(4.9)
70(1.8)
LDL-C, mg/dL (mmol/L)

Correlation Between LDL-C Lowering & Decreased CHD Risk in Primary & Secondary Prevention Trials With Statins1–3
Reproduced from Rosenson. (2004).1
CHD=coronary heart disease; Atv=atorvastatin; Pra=pravastatin; Sim=simvastatin; PROVE-IT=Pravastatin or AtorVastatin Evaluation and Infection Therapy; IDEAL=Incremental Decrease in Endpoints through Aggressive Lipid Lowering; ASCOT=Anglo-Scandinavian Cardiac Outcomes Trial; AFCAPS=Air Force Coronary Atherosclerosis Prevention Study; 4S=Scandinavian Simvastatin Survival Study; CARE=Cholesterol And Recurrent Events Trial; HPS=Heart Protection Study; LIPID=Long-term Intervention with Pravastatin in Ischaemic Disease; TNT=Treating to New Targets: WOSCOPS=West of Scotland Coronary Prevention Study.
1. Rosenson RS. Expert Opin Emerg Drugs. 2004;9(2):269–279; 2. LaRosa JC et al. N Engl J Med. 2005;352(14):1425–1435; 3. Pedersen TR et al. JAMA. 2005;294(19):2437–2445.
Eve
nt,
%
0
30
25
20
15
10
5
StatinPlacebo
Mean Treatment LDL-C at Follow-up, mg/dL (mmol/L)
0 80(2.1)
140(3.6)
200(5.2)
100(2.6)
40(1.0)
120(3.1)
180(4.7)
60(1.6)
160(4.1)
4S
4S
CARE
HPS
LIPID
HPS
CARELIPID
PROVE-IT (Atv)
PROVE-IT (Pra)
ASCOT
AFCAPS
ASCOT
AFCAPS
WOSCOPS
WOSCOPS
SecondaryPrevention
PrimaryPrevention
IDEAL (Atv)
IDEAL(Sim)
TNT(Atv
80 mg)
TNT (Atv 10 mg)
NCEP 2001
NCEP 2004

Correlation Between LDL-C Lowering & Decreased CHD Risk According to Treatment Modality in a Meta-Regression Analysis1,a
Reprinted from Journal of the American College of Cardiology, 46(10), Robinson JG, Smith B, Maheshwari N, et al, Pleiotropic effects of statins: benefits beyond cholesterol reduction? A meta-regression analysis, 1855–1862, Copyright © (2005), with permission from Elsevier.
CHD=coronary heart disease; MI=myocardial infarction; MRC=Medical Research Council; LRC=Lipid Research Clinics; NHLBI=National Heart, Lung, and Blood Institute; POSCH=Program on the Surgical Control of the Hyperlipidemias; 4S=Scandinavian Simvastatin Survival Study; WOSCOPS=West of Scotland Coronary Prevention Study; CARE=Cholesterol And Recurrent Events Trial; LIPID=Long-term Intervention with Pravastatin in Ischaemic Disease; AF/TexCAPS=Air Force/Texas Coronary Atherosclerosis Prevention Study; HPS=Heart Protection Study; ALERT=Assessment of LEscol in Renal Transplantation; PROSPER=PROspective Study of Pravastatin in the Elderly at Risk; ASCOT-LLA=Anglo-Scandinavian Cardiac Outcomes Trial–Lipid Lowering Arm; CARDS=Collaborative Atorvastatin Diabetes Study.aAnalysis included 19 trials of high-risk primary prevention and secondary prevention (CHD, cardiovascular disease, renal transplant, diabetes) patients; bStatin trials.
Robinson JG et al. J Am Coll Cardiol. 2005;46(10):1855–1862.
No
nfa
tal M
I an
d C
HD
Dea
th
Rel
ativ
e R
isk
Red
uct
ion
, %
–20
100
80
60
40
20
0
LDL-C Reduction, %
25 3015 35 4020
London
Oslo
MRC
Los Angeles
Upjohn
LRC
NHLBI
POSCH
4Sb
WOSCOPSb
CAREb
LIPIDb
AF/TexCapsb
HPSb
ALERTb
PROSPERb
ASCOT-LLAb
CARDSb

Each LDL-C Reduction of 1 mmol/L (39 mg/dL) Reduced CHD Risk by Over 20% in a MetaAnalysis1,a
CHD=coronary heart disease.aMeta-analysis of 62 randomized, controlled clinical studies that included 216,616 patients with CHD (secondary prevention), without CHD (primary prevention), or with or without CHD.bFatal or nonfatal myocardial infarction.
1. Gould AL et al. Clin Ther. 2007;29(5):778–794.
Rel
ativ
e R
isk
Red
uct
ion
, %
–26.6
–28.0–28.8
–27.5
–26.5
–25.5
0CHD Eventsb CHD Mortality
–26.0
–27.0
–28.0

Each LDL-C Reduction of 1 mmol/L (39 mg/dL) Reduced Major Coronary Eventsa by 23% in a Meta-Analysisb of Statin Trials1
Each 1 mmol/L (39 mg/dL) reduction also reduced
All-cause mortality (P<0.0001)
CHD mortality (P<0.0001)
Nonvascular mortality (P=NS)
CHD=coronary heart disease.aMajor coronary event=nonfatal myocardial infarction or death due to CHD. bMeta-analysis of 14 trials of patients with CHD (47%), history of diabetes (21%), and history of hypertension (55%).cIn the 14 trials analyzed, the control group was placebo in 11 trials, lower statin doses in 1 trial, no treatment in 1 trial, and usual care in 1 trial.
1. Cholesterol Treatment Trialists’ (CTT) Collaborators. Lancet. 2005;366:1267–1278.
Pooled Statin Groups
(n=45,054)
Pooled Controlc Groups
(n=45,002)
P<0.001
Statin vs Control
7.4
9.8
0
2
4
6
8
10
12
Pat
ien
ts W
ith
Maj
or
Co
ron
ary
Eve
nts
, %

Reducing LDL-C by 1 mmol/L Continued to Reduce IHDa Risk During Each Year of Treatment in a Meta Analysis1,b
IHD=ischemic heart disease.aIHD death and nonfatal myocardial infarction.bMeta-analysis of 58 trials.
1. Law MR et al. BMJ. 2003;326:1423–1427.
Ris
k R
edu
ctio
n,
%
–11
–33–40
–30
–20
–10
0
–24
–36
Year 1 Year 2 Years 3–5Year 6
and After
Years of Treatment

The 4S Diabetes Sub-study
(n=202)
P=0.087 P=0.002 P=0.018

The Role of Lipid-lowering Therapy in Preventing CHD in
Patients with Type 2 Diabetes : A Meta-analysis
D.G. Karalis. Clin. Cardiol. 31, 6, 2008: 241–248
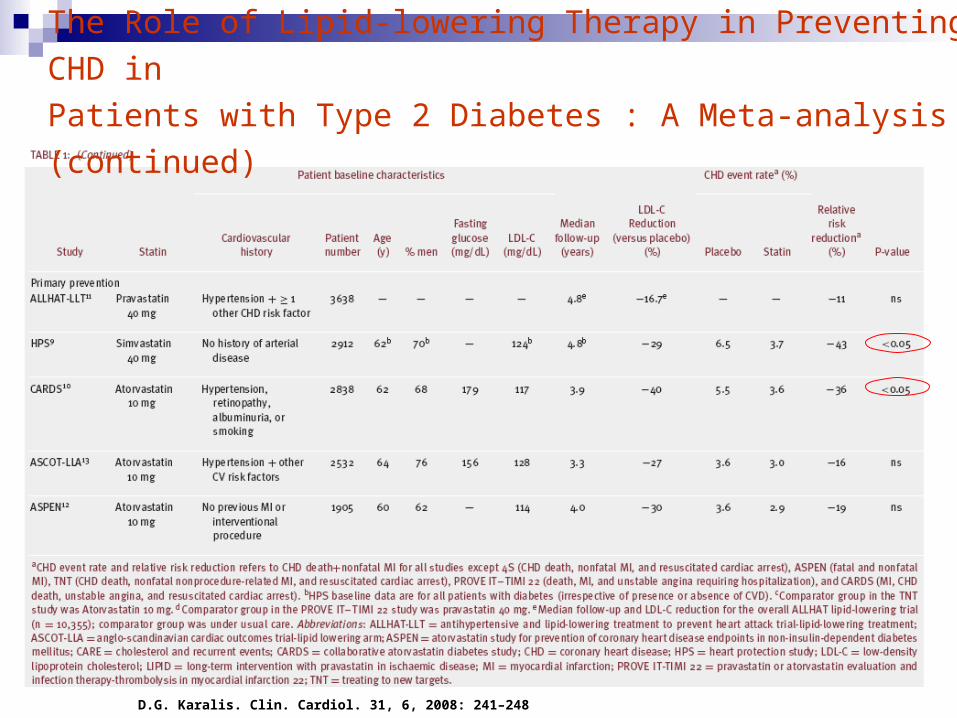
The Role of Lipid-lowering Therapy in Preventing CHD in
Patients with Type 2 Diabetes : A Meta-analysis (continued)
D.G. Karalis. Clin. Cardiol. 31, 6, 2008: 241–248

An Ideal Level of LDL Cholesterol should be between 40-70 mg/dL
What Is the Ideal Level of LDL Cholesterol
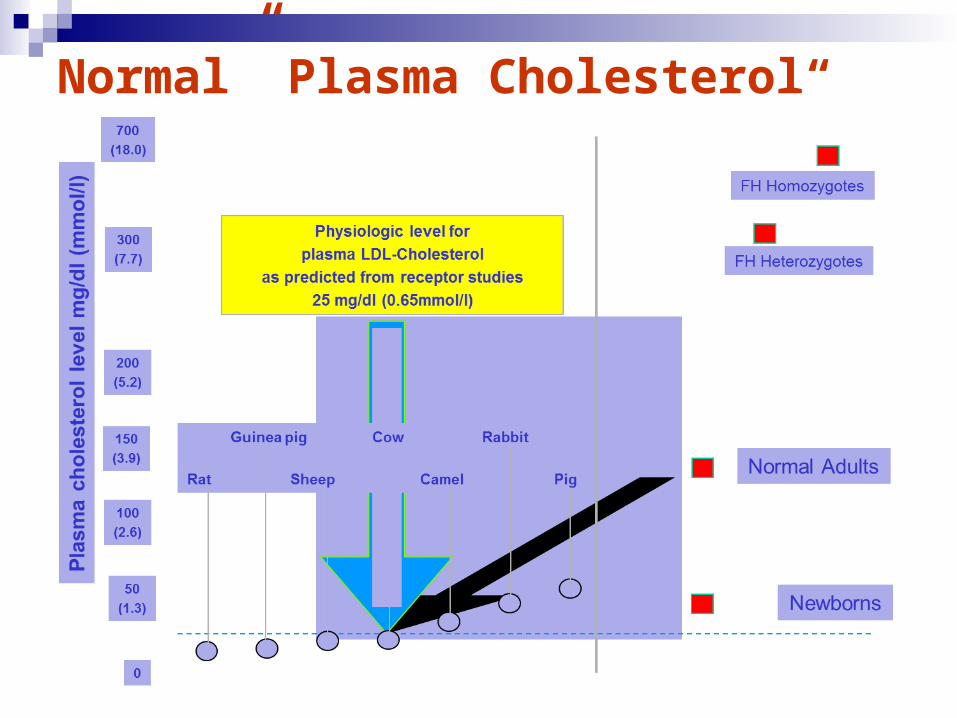
“Normal” Plasma Cholesterol

What is Desirable Cholesterol?
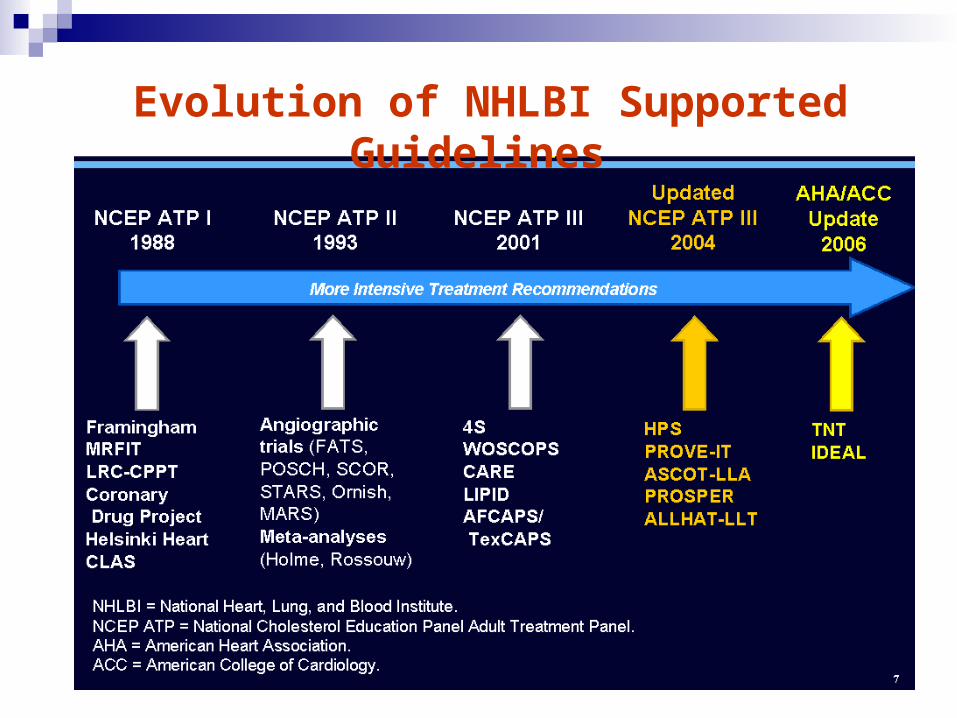
Evolution of NHLBI Supported Guidelines

Intensive LDL-C Goals for High Risk Patients
* And other forms of atherosclerotic disease.2
† Factors that place a patient at very high risk: established cardiovascular disease plus: multiple major risk factors (especially diabetes); severe and poorly controlled risk factors (e.g., cigarette smoking); metabolic syndrome (triglycerides ≥200 mg/dL + non–HDL-C ≥130 mg/dL with HDL-C <40 mg/dL); and acute coronary syndromes.1
1. Grundy SM et al. Circulation 2004;110:227–239.2. Smith SC Jr et al. Circulation 2006; 113:2363–2372.
<100 mg/dL
<70 mg/dL
Recommended LDL-C treatment goals
If it is not possible to attain LDL-C <70 mg/dL because of a high baseline LDL-C, it generally is possible to achieve LDL-C reductions of >50% with more intensive LDL-C lowering therapy, including drug
combinations.
ATP IIIUpdate 20041
<100 mg/dL:Patients with CHD or CHD risk equivalents(10 year risk >20%)1
<70 mg/dL:Therapeutic option for very high risk
patients1
AHA/ACC guidelinesfor patients with
CHD*,2
<100 mg/dL:Goal for all
patients with CHD†,2
<70 mg/dL:A reasonable goal
for all patients with CHD2

-1
-0.5
0
0.5
1
1.5
2
50 60 70 80 90 100 110 120
ASTEROID3 rosuvastatin
A-Plus2 placebo
ACTIVATE1 placebo
CAMELOT4 placebo
REVERSAL5 pravastatin
REVERSAL5 atorvastatin
Mean LDL-C (mg/dL)
The relationship between mean LDL-C and change in
percent atheroma volume (PAV) in IVUS studies†
Change in
Percent Atheroma
Volume*(%)
†ASTEROID and REVERSAL investigated active statin treatment; A-PLUS, ACTIVATE AND CAMELOT investigated non-statin therapies but included placebo arms who received background statin therapy (62%, 80% and 84% respectively).
*Median change in PAV from ASTEROID and REVERSAL; LS mean change in PAV from A-PLUS, ACTIVATE AND CAMELOT
1 Nissen S et al. N Engl J Med 2006;354:1253-1263. 2 Tardif J et al. Circulation 2004;110:3372-3377. 3 Nissen S et al. JAMA 2006;295 (13):1556-1565 4 Nissen S et al. JAMA 2004;292: 2217–2225. 5 Nissen S et al. JAMA 2004; 291:1071–1080
Progression
Regression
Conclusion
Epidemiological data Findings in other species EBM derived from clinical trials Evidence in patients with T2DM Studies aiming at regression of atheroma volume
All support the view of: “The lower the better in the context of lipids in patients with diabetes”

Thank You!