

LifeCourse: An Innovative Approach to Late Life Care in the Community
24
LifeCourse TM : An innovative approach to late life care in the community Eric Anderson, MD, Principal Investigator Allina Health September 29, 2015
-
Upload
allina-health -
Category
Health & Medicine
-
view
290 -
download
1
Transcript of LifeCourse: An Innovative Approach to Late Life Care in the Community

LifeCourseTM: An innovative approach
to late life care in the community
Eric Anderson, MD, Principal Investigator
Allina Health
September 29, 2015
Disclosure
There are no conflicts of interest or relevant financial interests in
making this presentation.
I have indicated that my presentation does not include discussion of
an unlabeled use of a commercial product, or an investigational use
not yet approved for any purpose.
2

Learning Objectives
• List the key activities of a lay healthcare worker providing patient-
centered and family-oriented care to individuals with advanced
serious illness.
• Describe how late life support several years before death impacts
- Quality of life for patients,
- The experience of care for families,
- Use of hospital and hospice in the last 6 months of life
- Completion of advance directives, and
- Total cost of care
3

7 out of 10 Americans
will die from serious
illness with an end-of-
life period that can be
drawn out over years,
not just weeks or
months.
Too often, serious illness
care is fragmented and
doesn’t support our
nonmedical needs.
With limited resources and
pressure to reduce
healthcare spending, we
have an opportunity to
make sure we are spending
our healthcare dollars as
wisely as possible – on the
care that matters most to
individuals.
Serious Illness Care Today
4
Home & Community
HospitalsService Lines& Specialties
Clinics
Allina Health Impact
5
• Individuals living with serious illness touch all parts of Allina
Health.
• They interact with multiple providers in different settings in
order to manage their increasingly complex care.
The Felt Experiences of Care
• A wife of a chronically ill husband: “We’ve been in the
hospital and five different care centers. It’s like starting over
every time.”
• A son caring for his father at home: “The only time I felt out
of control of my dad’s care was when we went into the
hospital.”
• A surgeon at Abbott Northwestern Hospital: “How can we
reclaim the heart of medicine?”
6

An Opportunity
“…our most cruel failure in how we treat the sick and the aged is the
failure to recognize that they have priorities beyond merely being
safe and living longer;
that the chance to shape one’s story is essential to sustaining
meaning in life;
that we have the opportunity to refashion our institutions, our
culture, and our conversations in ways that transform the
possibilities for the last chapters of everyone’s lives.”
- Atul Gawande, Being Mortal: Medicine and What Matters in the End
7

LifeCourse
LifeCourse is a late life supportive care approach that helps
individuals and families navigate serious illness.
It is part of a system strategy for addressing complex, serious
illness so that we can be more responsive as a health system to
the things that matter most to our patients.
8

Timeline
9
2012 2013 2014 2015 2016 – 2020
Pilot PhaseResearch and Program
DevelopmentProgram Expansion and
Community Impact
• Develop model
• Enroll 23 patients
• Enroll and study
over 1500 patients
plus family
members and
comparison patients
• Develop program
evaluation
• Test model with early
adopters
• Integrate LifeCourse across
Allina Health
• Promote public engagement
around late life care issues
• Pursue government policy
and reimbursement agenda

Key Components
Whole Person
Care
Care Guide
Family-Oriented Approach
What Matters
Most
10

Identified by multiple factors in the EHR
Screened by a research nurse
Target Population
Study Participants
11
Recent clinic or hospital
encounter
1 or more chronic
illnesses in an advanced
stage
Allina Health
provider
Comorbidity score ≥ 4
Electronic eligibility report
Individuals living with serious illness who may be in the last two to three
years of life

Visit Approach
Care guides have monthly, in-person visits with patients
and their caregivers.
Care guides discuss patient goals, and they review what
matters most.
In their Excellian notes, care guides reflect the whole
person.
12

Implementing Whole Person Care
13
Visit #1
Visit #2
Visit#3
Visit #4
Visit #5
Visit #6 On-going
Qu
est
ion
Set
s
Physical Social Cultural Financial & Legal
Revisit and Update
Questions
Revisit and Update
Questions
Revisit and Update
QuestionsPsychological Cultural Spiritual
Family Legacy
Care at End of Life
Ass
ess
me
nts
Physical Physical Ethical Reassess-ment:
Physical
Reassess-ment:
Physical
Revisit Assessments
Social
Financial & Legal
Supplemental Visits: Advance Care Planning, Supportive Family Conference

Implementing Whole Person Care
14
Visit #1
Visit #2
Visit#3
Visit #4
Visit #5
Visit #6 On-going
Qu
est
ion
Set
s
Physical Social Cultural Financial & Legal
Revisit and Update
Questions
Revisit and Update
Questions
Revisit and Update
QuestionsPsychological Cultural Spiritual
Family Legacy
Care at End of Life
Ass
ess
me
nts
Physical Physical Ethical Reassess-ment:
Physical
Reassess-ment:
Physical
Revisit Assessments
Social
Financial & Legal
Supplemental Visits: Advance Care Planning, Supportive Family Conference
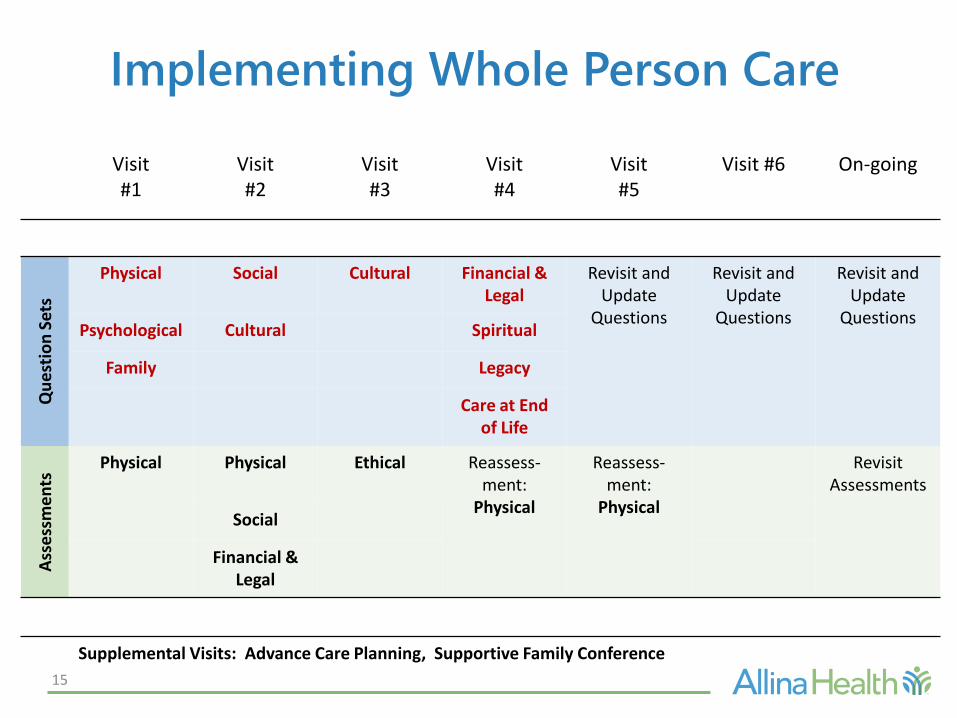
Implementing Whole Person Care
15
Visit #1
Visit #2
Visit#3
Visit #4
Visit #5
Visit #6 On-going
Qu
est
ion
Set
s
Physical Social Cultural Financial & Legal
Revisit and Update
Questions
Revisit and Update
Questions
Revisit and Update
QuestionsPsychological Cultural Spiritual
Family Legacy
Care at End of Life
Ass
ess
me
nts
Physical Physical Ethical Reassess-ment:
Physical
Reassess-ment:
Physical
Revisit Assessments
Social
Financial & Legal
Supplemental Visits: Advance Care Planning, Supportive Family Conference

Outcomes
Participant Outcomes
Quality of Life1
Experience3
Goals honored
Caregiver Outcomes
Quality of Life2
Experience3
System Outcomes
Care Team wellbeing4
Hospice Days
Hospital Days
Emergency Visits
Total Cost of Care
1. FACIT-PAL (Functional Assessment of Chronic Illness Therapy - Palliative Care)2. PROMIS-29 (Patient Reported Outcome Measurement Information System)3. LifeCourse Experience tool4. Maslach Burnout Inventory
Goal: maintain patient & family quality of life while decreasing overall cost
16

Participant Outcomes
Measure Hypothesis Early Results
Quality of Life
LifeCourse participants quality of life will remain stable or decrease at a slower rate than patients receiving
usual care.
+
ExperienceLifeCourse participants will have more positive care experiences than patients
receiving usual care.+
GoalsExploratory: To understand patient
goals late in life.
Patients prioritize both medical and
nonmedical goals.
17

Caregiver Outcomes
18
Measure Hypothesis Result
Quality of Life
Quality of life for caregivers participating in LifeCourse will remain stable or
decrease at a slower rate than caregivers of patients receiving usual care.
+/-(+ for Anxiety and Global - Health)
Experience
Caregivers participating in LifeCourse will have more positive experiences as compared to caregivers of patients
receiving usual care.
+

System Outcomes
19
Measure Hypothesis Early Results
Palliative Care Utilization
LifeCourse participants utilize community and inpatient palliative care services more frequently than patients receiving usual care.
Inpatient DaysLifeCourse participants will have fewer inpatient days than participants receiving usual care.
Advance Directive LifeCourse participants will have increased advance directive completion compared to patients receiving usual care.
Hospice EnrollmentLifeCourse participants will choose to enroll in hospice at an increased rate compared to patients receiving usual care.
ED VisitsLifeCourse participants will utilize the ED less frequently than patients receiving usual care.
Total Cost of CareLifeCourse participants will have lower total cost of care than patients receiving usual care.

• One article published in the American Journal of Hospice and Palliative
Medicine, with several other manuscripts in progress
• Presentations at 11 conferences in 2015, including a symposium at the
Gerontological Society of America Annual Scientific Meeting
• One presentation confirmed for 2016 at American Academy of Hospice
and Palliative Medicine
• LifeCourse included in a presentation on HHS Delivery System Reform
given by Senator Amy Klobuchar and Allina EVP Robert Wieland
• Eight late life documentaries broadcast on Twin Cities Public Television
Dissemination
20

• Fortin AH, Dwamena FC, Frankel RM, Smith RC. Smith’s Patient-Centered Interviewing;
An Evidence-Based Method. 3rd ed. New York, NY: McGraw-Hill Companies, Inc.
• Gawande A. Being Mortal; Medicine and What Matters in the End. New York, NY:
Metropolitan Books, 2014.
• National Consensus Project for Quality Palliative Care. Clinical Practice Guidelines for
Quality Palliative Care, Third Edition. Published 2013.
• National Quality Forum. A National Framework and Preferred Practices for Palliative
and Hospice Care Quality: A Consensus Report. Published 2006.
• RAND Corporation. Redefining and Reforming Health Care for the Last Years of Life.
http://www.rand.org/pubs/research_briefs/RB9178/index1.html. Published 2006.
• Schellinger S, Cain CL, Shibrowski K, Elumba D, Rosenberg E. Building New Teams for
Late Life Care: Lessons from LifeCourse. American Journal of Hospice & Palliative
Medicine. 2015: 1049909115574692.
21
References

22

In case you missed Speaking of Being Mortal: A Life Changing
Conversation with Dr. Atul Gawande on September 18,watch
the broadcast in November on Twin Cities Public Television.
– Also available on www.lifecoursemn.org
– Event sponsored by Allina Health and LifeCourse
24
To Contact Me












![Lifecourse Health Development: Past, Present and Future · Lifecourse Health Development: Past, Present and Future ... ness, injury, and infectious diseases [1–3]. As evidence subsequently](https://static.fdocuments.us/doc/165x107/5f0c6b3e7e708231d4354e4a/lifecourse-health-development-past-present-and-lifecourse-health-development.jpg)





