Lessons Learned Report II March 2015 - Health Partners...
72
Lessons Learned Report II March 2015 NU Health Programme PO Box 11161 Plot 31B Bukoto Crescent Kampala Uganda Funded by: Managed by: In support of:
-
Upload
phungthien -
Category
Documents
-
view
214 -
download
2
Transcript of Lessons Learned Report II March 2015 - Health Partners...

Lessons Learned Report II
March 2015
NU Health Programme
PO Box 11161
Plot 31B Bukoto Crescent
Kampala
Uganda
Funded by: Managed by: In support of:

2
NU Health Lessons Learned II Report
TABLE OF CONTENTS
Table of Contents ........................................................................................................................ 2
Abbreviation and Acronyms ......................................................................................................... 3
1 Executive Summary ............................................................................................................. 5
2 Introduction .......................................................................................................................... 6
3 Study Design ........................................................................................................................ 8
4 Experience working with District Health Teams .................................................................. 11
5 Experience working with PNFP Health Facility Staff ........................................................... 15
6 Quality of Care ................................................................................................................... 18
7 Health Outcomes................................................................................................................ 32
8 Value for Money ................................................................................................................. 42
9 Operation / Management Processes .................................................................................. 56
10 Risk, particularly Fiduciary Risks, and its Mitigation ........................................................ 61
11 Conclusions: Good and Bad Practices in RBF ................................................................ 64
References ................................................................................................................................ 68
Annexes .................................................................................................................................... 69
Annex 1: Indicators Assessed and the Associated Calculations for Payments - Year 2 ......... 69
Annex 2: Standard Unit of Output (SUO) formula used by UCMB .......................................... 71

3
NU Health Lessons Learned II Report
ABBREVIATION AND ACRONYMS
ANC
BP
CI
Antenatal Care
Business Plan
Confidence Interval
CL Credit Line
CSP
DCV
DFID
DHIS2
DHT
DQA
DR
EMHS
Capacity Strengthening Plan
Direct Client Verification
Department for International Development
District Health Information System
District Health Team
Data Quality Assessment
Discrepancy Rate
Essential Medicines and Health Supplies
FGD Focus Group Discussion
HC
HF
Health Centre
Health Facility
HMIS Health Management Information System
HPI
IBF
Health Partners International
Input-Based Financing
IMNCI Integrated Management of Newborn and Childhood Illnesses
JMS
KII
LL
LLU
Joint Medical Stores
Key Informant Interviews
Lessons Learned
Lower Level Unit
MNCH
MoH
NAO
NU Health
Maternal, Newborn and Child Health
Ministry of Health
National Audit Office
Northern Uganda Health Programme
OPD Out-Patient Department
OR Odds Ratio
PCDP
PMTCT
Post-Conflict Development Programme
Prevention of Mother to Child Transmission (of HIV)
PNFP Private-not-for-Profit
PO
QoC
QQA
RBF
Purchase Order
Quality of Care
Quarterly Quality Assessment
Results-Based Financing (Health Facility)
RDT Rapid Diagnostic Test
SUO
ToC
UCMB
UGX
Standard Unit of Output
Theory of Change
Uganda Catholic Medical Bureau
Ugandan Shilling
UHC Universal Health Coverage

4
NU Health Lessons Learned II Report
UKaid
VfM
United Kingdom Aid
Value for Money

5
NU Health Lessons Learned II Report
1 EXECUTIVE SUMMARY
This report summarises lessons learned in the implementation of the Department for International
Development (DFID) funded study Northern Uganda Health Programme (NU Health). It covers a
set of topics identified as areas of substantive interest to DFID as well as the larger Results-Based
Financing (RBF) community. Drawing on a range of methodologies, these lessons learned build
on data collected specifically for this report, as well as analysis of existing programme-generated
data. Each section of this report is largely self-standing to enable the discerning reader to review
specific topics consistent with his or her own particular interest. The final section serves as a
conclusion on what has been learned and what might be done with that learning going forward.
Following the completion of its inception period, NU Health underwent a significant revision shifting
from a demonstration project to an operations research study with the aim of generating evidence
and insight into how RBF can contribute to improving health outcomes for the poor. The
programme was refocused to attend to some of the evidence gaps in the current debate on
achieving universal health coverage through RBF, better accountability and improved health
sector performance. NU Health is contributing to the policy discussion in Uganda and it aspires
to make contributions to the larger global debate. This report does not aim to provide the final
word on what has worked and at what price, rather it does aspire to share relatively unvarnished,
practical insights into what seems to work and lessons learned that others active in this area may
benefit from adapting or avoiding in their own efforts.
The report seeks to capture lessons learned along the programme’s value chain, from inputs
through processes, to outputs and outcomes. It is structured to address specific aspects of the
study and their role in the programme and the evidence it generates.
1. Executive Summary
2. Introduction
3. Programme design
4. Experiences working with District Health Teams
5. Experiences of Health Facility Staff and Management
6. Quality of Care
7. Health Outcomes
8. Value for Money (VfM)
9. Operational/Management Process
10. Risks, including fiduciary risk and mitigation in both RBF and Input-Based Financing (IBF)
11. Good and bad practices in RBF
Given the multiple stakeholder groups or constituencies involved in NU Health, many sections of
this report highlight points around perspective, timing and time horizon. Stakeholders at both the
District Health Team (DHT) and Private-Not-For-Profit (PNFP) facility levels appreciate that the
fundamental focus of NU Health as a study is to generate evidence. Still, at the DHT level, though
NU Health may have represented an interesting opportunity to improve health system
performance, it is seen as another priority to juggle by many DHTs who already feel under-

6
NU Health Lessons Learned II Report
resourced and over-burdened. At the facility level, NU Health was generally appreciated as a
vehicle for improving quality of care, and coming as it did with the cessation of humanitarian
support to the health sector, it was seen as a lifeline by many health facilities. In reviewing the
lessons learned outlined in this report, the view point of these stakeholder groups is highlighted
where relevant.
As NU Health looks toward its final months, and the prospects for evidence uptake, it is worth
noting that accompanying the strengthening of the programme’s research study design, DFID also
advised the programme managers to curtail advocacy and communications activities. While the
proscription on advocacy in the absence of evidence certainly made sense, the proscription on
communications was, with hindsight, less helpful: NU Health was off the radar screen for many
key stakeholders and certainly at a policy level. More recently, as restrictions on communication
have eased, stakeholders are taking a real interest in the initial insights arising from the NU Health
experience, while sharing their concerns about how NU Health and similar efforts will feed into
Uganda’s roadmap for establishing more accountable and higher functioning health services
through Results-Based Financing (RBF).
2 INTRODUCTION
The Northern Uganda Health programme (NU Health 2011 - 2015) is part of the UKaid-supported
Post-Conflict Development Programme (PCDP) which aims to strengthen local and national
mechanisms for governance and accountability to improve access to health care, particularly for
the most vulnerable populations in the Acholi sub-region. NU Health focuses on generating
evidence on RBF and the extent to which this is an efficient and effective financing mechanism for
improving accountability and access to quality health care with faith-based PNFPs. Following its
recent contract amendment, the programme will run to the end of October 2015.
After the programme’s inception period, major changes were made to programme design and
implementation approach in consultation with DFID, and the programme was modified to better
assess the cost effectiveness of RBF, by introducing an input-based financing (IBF) comparison,
or control arm, in addition to the RBF intervention. Rather than running the programme in
“implementation mode” to maximise prospects for positive outcomes associated with RBF, NU
Health would adopt a “hands off” approach to avoid influencing how RBF facilities would use any
financing they received for attaining targeted results. Other programme variables aside from the
financing mechanism, such as the provision of a funded credit line and supportive supervision,
are kept constant for the RBF and IBF facilities to isolate the main effort of the funding modality
and strengthen the validity of results.
Prior to refining the study design, the programme had five outputs:

7
NU Health Lessons Learned II Report
Output 1 Improve availability of essential medicines in participating PNFP health facilities
through the provision of a funded credit line for essential medicines and health
supplies (EMHS) for all participating PNFP facilities through the Joint Medical
Stores (JMS)
Output 2 Support improvements in service delivery and quality at PNFP facilities through
the implementation of a RBF model in the Acholi sub-region and for comparison
an input-based financing (IBF) model in Lango
Output 3 Strengthen the capacity of the District Health Teams (DHTs) to monitor and
provide supportive supervision to PNFP facilities
Output 4 Generate stakeholder engagement on the project, the evidence it generates, and
the concept of Results Based Financing at local & national levels
Output 5 Ensure the verification role within the RBF scheme is effectively fulfilled by the
DHTs with support from the NU Health team
With the refined study design, Output 4 was significantly curtailed. While stakeholders directly
involved with the study, i.e. DHTs and diocese and PNFP staff, would be engaged, DFID advised
that NU Health should not proceed with advocacy or communications with the broader stakeholder
group, particularly those at the national level, during the course of the study. Networking and
communications with these groups recommenced following approval of Contract Amendment 3 in
January 2015.
The Lessons Learned report originated from discussions between DFID and NU Health on key
themes for a series of Technical and Policy Briefs to be produced by the programme, exploring
specific areas of interest and programme findings in greater detail. Following further discussion, it
was agreed that two longer Lessons Learned documents would be developed and in March 2014
NU Health produced the first report which summarised lessons learned in the implementation of
the programme to date. That report covered a number of topics identified as areas of substantive
interest relevant to DFID as well as the larger RBF community. Drawing on a range of
methodologies, these lessons learned built on data collected specifically for the report, as well as
alternative analysis of existing programme-generated data. This second report draws additional
attention to implementation issues and their potential implications for any roll out or scale up of
RBF programming.
As working papers, there are limitations to these Lessons Learned documents. A principle
limitation is the reliance on data from the broader Health Management Information System (HMIS)
for some areas of comparison between NU Health-supported facilities and others in the ten
districts, as well as the use of qualitative methodologies on some issues which do not necessarily
provide a basis for wider inference. The findings, therefore, should be interpreted with some
caution and within their specific context. Specific limitations are noted in each section where
relevant. Evidence generated by an independent assessment undertaken by Liverpool School of
Tropical Medicine/LATH will augment these data and may provide a basis for more robust
inference.

8
NU Health Lessons Learned II Report
The objective of this report is to build on the findings in the first report and further examine the role
of RBF or IBF in affecting changes through individual and collective behaviour at facility and district
levels, ultimately in the provision of health services.
This report is structured around the following nine key themes in sections 3 – 11 of this report:
3. Study design
4. Experiences working with DHTs
5. Experiences of Health Facility Staff and Management
6. Quality of Care
7. Health Outcomes
8. Value for Money (VfM)
9. Operational/Management Process
10. Risks, including fiduciary risk and mitigation in both RBF and IBF
11. Good and bad practices in RBF
3 STUDY DESIGN
In its assessment of the costs and benefits of RBF versus IBF, NU Health was designed to isolate
the main effect on financing modality, i.e. RBF versus IBF, on health output. Both this study design
and the inclusion of an evaluation are intended to generate robust evidence. NU Health is
designed to help address key gaps in the body of evidence on the relative value added of RBF.1
One of the assumptions outlined in the project design was that supported PNFP would reduce
their user fees as (i) this loss of funding from patients contribution would be compensated by DFID
funding and (ii) reduced fees would serve the purpose of increasing affordability and thus
accessibility. However, during the inception period this assumption revealed to be impractical as
PNFP were not prepared to remove their user fee levels. The reasons given by PNFP were that,
as NU Health support was limited in time, facilities would have to re-introduce their user fees after
NU Health’s exit. This would likely turn away patients/clients and risk the PNFP’s ability to provide
quality services with any degree of sustainability.
With the aim of isolating the main effect of the financing modality, there were several revisions to
NU Health’s design. First, there was the addition of a control or comparison group, a set of
facilities in Lira which by a range of indicators were similar to those in the Acholi intervention
districts. Secondly, the study adopted inclusion criteria related to facility readiness: despite some
modest investment to reach sample size, most facilities were included “as is” with minimal
intervention to affect facility systems or capabilities. Thirdly, the study emphasised providing
significant capacity development support to the DHTs to enable them to fulfil their
regulator/verifiers function in the study. Finally, there was a decision to be “hands off” in advising
the RBF facilities how they might use their results payments; such that each facility within the
1 For example; Eldridge, C & Palmer, N. Health Policy & Planning. 24 (3):160-166. (2009)

9
NU Health Lessons Learned II Report
strictures of their own standard operating procedures could use the funds it earned as it deemed
fit.
The Theory of Change (ToC) behind the study design is summarised graphically as follows:
Following an assessment to identify PNFPs that met standards of functional service delivery, 21
facilities were originally enrolled in Acholi sub-region and these facilities were matched with ten
control PNFPs in neighbouring Lango sub-region. The Lango region was chosen as it is also post-
conflict and shares a similar socio-cultural and economic setting to Acholi. The range of levels of
health facilities within the RBF and IBF regions are represented in Table 1 below:
Table 1: Range of PNFPs in RBF and IBF regions
Level Acholi/RBF
region
Lango/IBF
region
Hospital /
Health Centre (HC) 4
3 2
HC3 3 6
HC2 15 2
After the disqualification of one facility, St Joseph Minakulu HC2 in July 2014, the 20 Acholi
facilities receive a variable payment each quarter based upon their performance over the
preceding three months. The ten control PNFPs in Lango each prepare a work plan to address
core areas of service improvement and receive input-based funding to support implementation of
these plans. The amount of funding allocated per level of facility roughly matches the amount
anticipated for the RBF PNFPs at the same level over the course of the programme.
A key feature of RBF design is the separation of the roles of Funder, Purchaser, Provider and
Regulator/Verifier. In NU Health these roles are defined as follows:
The Funding Agency is DFID, who transfers funds to NU Health.
The Purchaser is NU Health on behalf of DFID. NU Health oversees the transparency of
the RBF system, and controls the checks and balances. Total system oversight rests
physically at the NU Health Gulu office, with oversight from the NU Health team based in
Kampala.
The Providers are the PNFPs providing health services. They each hold a contract with
the purchaser which is contractually binding in terms of remuneration/incentive payments.
5 Outputs 1. Credit line 2. Financial support 3. DHT strengthening 4. Advocacy 5. Verification/ M&E
Outcome Increased access to quality health care services by the poor in Northern Uganda
Impact Increase in the economic, social and political opportunities that improve the lives of people affected by conflict in Northern Uganda

10
NU Health Lessons Learned II Report
The Regulator/Verifier is the DHT in each district, which has the primary responsibility of
providing guidance and oversight to the PNFPs in implementation of RBF and general
troubleshooting, largely through feedback on HMIS reporting and planned supervisions.
Initially NU Health supported all the participating DHTs in this role both financially and with
the provision of secondees to support capacity, whilst gradually building their capacity to
fulfil their supervision/verification role independently. The programme design aims to see
DHT secondees becoming absorbed within, and financed by, the formal DHT team.
For the purposes of the study, a key aspect of NU Health is an intensive and rigorous verification
process to validate the service delivery data provided by PNFPs. This is a fundamental component
of the NU Health model as the value of RBF payments is calculated on the basis of verified
performance data. Data quality assessments (DQA) are undertaken by DHTs in collaboration with
NU Health staff and are complemented by a quarterly quality assessment (QQA) in each health
facility. The indicators selected to assess PNFP performance include the following:
Antenatal care with defined quality parameters – starting before 16 weeks, 4+ visits,
including provision of tetanus vaccination and malaria prevention, with appropriate
measures for the prevention of mother-to-child transmission (PMTCT) of HIV.
Delivery in the health facility – using a partograph, with emergency obstetric care provided
as needed, early breastfeeding,
appropriate postnatal care.
Child care – full vaccination,
appropriate diagnosis and
treatment of common illnesses.
Adult care – appropriate
diagnosis and treatment of
common illnesses.
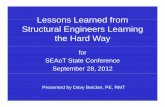
Based on the results of the DQA and
QQA, RBF PNFPs receive payment
according to the formula in Figure 1.
Details of all indicators assessed and the
associated calculations for payments
are provided in Annex 1.
In the IBF control or comparison group, facilities received grants matched to facility-level specific
levels of RBF payment. In contrast to the RBF “hands off” approach, the use of grant funds are
highly regulated, with extensive scrutiny related to adherence to plan and procurement procedure.
P RBF Payment to a PNFP for the quarter
S Standard Subsidy for a particular indicator
z Quality Multiplier determined by the PNFP quality score
x Base Incentive per level of care
y Quality Incentive per level of care
n Number of patients seen by the PNFP for that particular indicator
P = S ( x + (y z)) nRBF INCENTIVE
PAYMENT
FORMULA
RBF Formula
13
Figure 1 RBF Formula

11
NU Health Lessons Learned II Report
4 EXPERIENCE WORKING WITH DISTRICT HEALTH TEAMS
This section reviews the perspective of the DHTs along with those of the facilities and NU Health
Staff to summarise the experience of working with DHTs. As the most decentralised levels of
regulation within the Uganda Ministry of Health (MoH), the DHTs and Health Sub-District
authorities have played a critical function in the role as regulator/verifier in the RBF intervention
area, as well as assessor in the IBF control area. In addition, the DHTs have a set of tasks around
guidance and supervision of health facilities located within their area of responsibility, data
collection and analysis, the planning of health service delivery, and the coordination of
stakeholders at district level (across both public and private sectors). Determinants of DHT
performance relate to, among others, adequate staffing to cover these core functions, appropriate
skills levels among those staff, and the availability of key support measures, for example, funding
for activities and equipment such as vehicles, computers, power supply and so on.
At the time of programme inception, the most prominent obstacle to DHTs carrying out their
responsibilities were the capacity constraints. There was a combination of understaffed district
health offices, under-skilled DHT members, and a lack of transport to enable outreach to the
facilities. Both the lack of transportation and the shortage of qualified district health officials stems
from budget constraints, including staff attrition, unattractive employment packages and the
absence of facilities at the remote areas where some officials should be posted.
NU Health sought to address these issues by supporting three key areas:
Human resources strengthening;
Improved supportive supervision;
Improved data collection, analysis and utilization.
NU Health’s interventions in the aforementioned areas have resulted in improvements in DHT
overall effectiveness and efficiency, including the quality of health facility assessment and
supportive supervision.
Assessment Methodology
Focus Group Discussions (FGDs) and Key Informant Interviews (KIIs) were conducted with 48
District Health Team members according to a predetermined questionnaire. The interview
questions focused on the participants’ perceptions and opinions of:
the impact of support to the DHTs and health facilities on the delivery of services;
the main challenges and successes experienced during the life span of the NU Health
project;
the sustainability of the changes made; and,
recommendations for future RBF initiatives.
In addition, FGD were conducted with NU Health Staff which helped to inform the agenda for a
broader workshop convening key DHT with PNFP personnel, to discuss these issues in greater

12
NU Health Lessons Learned II Report
depth. Many of the core issues raised are expanded with quantitative programme findings
throughout the remaining report sections.
Findings
Overall, the district health officials continued to report a positive view of the support provided by
the NU Health programme both at the district and facility levels. District health officials observed
many improvements at the PNFP health facilities particularly in the following areas:
quality of care provided;
patient attendance and satisfaction with services rendered;
staff management and motivation;
data management & reporting;
investment in equipment and capital development;
financial management;
drug management; and,
prescription habits.
The sections below present the district health officials’ experience in working with the NU Health
study in the three key areas of support provided.
Human Resources Strengthening
In most districts NU Health filled critical staffing gaps at the district health office by seconding staff
to support maternal, newborn and child health (MNCH) related activities. In cases such as Nwoya
district, DHT performance improved greatly with the support from much needed team members
and resulted in the district rising from 20th to 1st position in health sector performance nationwide
due to improved reporting. Despite the assistance that NU Health provided to the various districts
in this regard, many remain understaffed and it is likely that without support from the central
government or other external interventions, many of these positions will remain unfilled.
Supportive Supervision Capacity
NU Health supported each DHT to draw its Capacity Strengthening Plan (CSP) outlining the
support that each DHT would require to enhance its ability to play its expected supervisory role
and also to perform the additional role of independent verifier of the NU Health programme and to
eventually roll out the DQA/QQA process to other public or private facilities within its jurisdiction if
deemed relevant by the DHT. With Uganda Health policy which keeps on changing, most of the
CSP were aimed at mentoring health facility staff on implementing new health policies.
Participants reported that the DHTs’ capacities had been strengthened and that the support from
NU Health now prepared them for the management of RBF programmes. However, some felt that
the recruitment of additional vacant positions within the DHTs and further capacity building could
have resulted in a greater positive impact in supervision and consequently better health service
delivery and would certainly be necessary if RBF programming were expanded. One of the
recommendations made was that there be increased inter-district DHT dialogue and exchange
visits to make up for lack of capacity in some areas. District health officials also recommended

13
NU Health Lessons Learned II Report
that PNFP staff be trained to do a “peer” QQA supportive supervision in other facilities to sustain
the positive impact of the programme on health service delivery. One of the obstacles in achieving
positive results from the DHTs was the attitude among some DHT members who are mainly
motivated by additional allowances given by the programme.
Logistics
Transport to and from the facilities during the quarterly assessments remained a challenge for the
DHTs. This was primarily a result of the competing claims on the limited availability of well-
maintained vehicles at the district health offices.
Conducting Supportive Supervision in Non-NU Health Supported Facilities
Many of the health officials interviewed reported that they had used the NU Health supervision
tools with facilities outside the NU Health study area. It was reported that although the MoH has a
supervision tool, the NU Health tools were preferable as they are more comprehensive. At the
same time, despite the shortcomings of the MoH tool, some officials felt that NU Health should
have harmonised their tools with the pre-existing ones for the purposes of uniformity and ease of
transition in a post-NU Health setting. District health officials also noted that seconded staff
performed their routine duties outside of NU Health study activities and that there were sometimes
conflicting priorities between fulfilling routine responsibilities related to their role within the DHT
and those associated with the NU Health study. Additionally the DHT personnel, including the
secondees, are being solicited by many implementing partners for various programmes and thus,
their availability is often limited.
Data collection, analysis and utilization
With the NU Health study requirements for verification in RBF facilities and assessment in the IBF
facilities, DHT participation in data collection, analysis and utilization increased tremendously.
Over time, a number of DHT members became conversant with data management and use,
particularly in the RBF areas.
As reported in the final section of this report, over time NU Health observed improvements in
reporting, data management and utilisation. Report accuracy increased over time, especially in
the RBF group, as did, to some extent, their completeness. However, the timeliness of reporting
remains a challenge with an average timeliness rate of reporting shown on District Health
Information System (DHIS2) below 70% in both groups (see section 11 for further details).
The demands of the study also served to highlight capacity constraints at both the systems and
individual levels. There were challenges in working with DHIS2 -- including familiarity with the
programme, lack of regular electrical supply, and unreliable internet connectivity. Although the
DHTs were mindful of the time bound nature of the study, many noted the critical gaps in staffing
as well as finance for transport which would adversely affect the DHTs’ ability to verify quality
indicators in the future. It was also noted that in some districts there were relatively low levels of
motivation of DHT members to supervise the facilities let alone review their data.

14
NU Health Lessons Learned II Report
Feedback on process improvements suggested by DHTs
Participants stressed the importance of documenting NU Health’s activities, analysing the
changes made in the facilities and from this, making informed decisions and recommendations for
future RBF initiatives. District health officials also felt that it would have been beneficial for the
programme to have run over a longer period of time since the facilities are just starting to have
consistent performance in the delivery of quality health services.
There is also a general sense that a similar programme should be designed for government health
facilities since the PNFPs are mostly situated in urban and peri-urban areas. Supporting
government facilities in this way would have made a greater difference in rural and underserved
communities. In some areas where only one facility was supported in the whole district, it was
recommended that in future programmes, multiple facilities be supported to be able to better
assess programme impact on service delivery.
PNFP Perspectives
Principle observations from PNFP staff about the DHTs related both to their technical capabilities
and their ability to independently assess and verify facility performance and provide supportive
supervision. This first point, confirmed by NU Health staff, points to the limited capacity of many
DHTs and their absence of redundant capability on issues, such as MNCH, as well as broader
technical and policy concerns such as the role out and use of DHIS2.
The second point was slightly more sensitive. By design, RBF established a segregation of
responsibility that entails a tension between providers and regulators of services. PNFP staff
noted the difficulty at a human level of both assessing performance and defining payment, while
also providing supportive supervision, without being drawn into any gaming of the system. The
PNFP suggestion was to have these two functions separated in the future if possible, which would
have further implications for the, already limited, DHT staff time.
NU Health Staff Perspectives
NU Health field staff also flagged the technical and managerial capacity constraints described by
PNFP staff. In addition, they highlighted the absence of financial analytic and management skills
on the part of DHT staff.
Their more salient observation however was of a strain placed on the DHTs by donor and NGO
programme fragmentation contributing to competing demands on their time. They were clear that
the range of initiatives and their associated level of effort was beyond what the DHTs could
reasonably accommodate. The NU Health field team noted the risk of the largely unregulated
development assistance project market and the tendency for DHT staff to participate in activities
that yielded better allowances, rather than on the basis of policy priority or other system level
criteria.
Policy implications for future RBF initiatives
Overall, the district health officials are supportive and enthusiastic about government
implementing the RBF model. However, some of the district health officials interviewed

15
NU Health Lessons Learned II Report
commented that the central MoH was not fully engaged with the programme. They felt that had
they been more engaged and therefore witnessed some of the changes that the programme has
influenced in the facilities, there would be greater support for government to push for RBF at a
policy level. District health officials have found the interventions and tools introduced by NU Health
useful, and expressed a willingness to use them beyond the life of the programme. However, it is
important to note that future RBF programmes would need to integrate and encourage increased
involvement of the MoH and other stakeholders to be able to push the RBF model as a policy, if
the final evidence gained from the programme evaluation (and other similar initiatives) supports
the intervention model. It was noted that district local government authorities and politicians should
have been better informed about the progress of the study activities to raise awareness and
support for the RBF model. There is a general appreciation that DHTs will need significant
capacity strengthening if they are to support a roll out of RBF to public as well as PNFP facilities.
5 EXPERIENCE WORKING WITH PNFP HEALTH FACILITY STAFF
This section reviews the perspective of the PNFP staff along with those of the DHTs and NU
Health Staff to summarise the experience of working with PNFP staff. A key early insight related
to the relative operational autonomy of the PNFP and the often modest level of oversight that the
dioceses or medical boards had on PNFP operations. Although general observations are valid on
functionality at a particular level of facility, e.g. HC2 or HC3, there was a high level of variation
within any particular level in how facilities functioned.
Many of the PNFPs supported by NU Health were new to the idea of business planning. Yet for
health facilities to participate in NU Health, they had to develop individual plans to outline their
spending priorities. The potential value of a business plan is clear to most, in so far as it aims to
support providers to assess where they are and plan realistic targets; and supports purchasers to
understand in which resources the facility may invest and which strategies they were likely to
apply. However, despite these apparent benefits, many facilities struggled with the exercise. While
many higher level facilities, such as hospitals, already had an established annual planning
process, most lower-level facilities did not, and required substantial assistance. The study’s
“hands off” approach, however, limited the level of support provided to the facilities for the
implementation of their business planning as no advice was provided on the allocation of funds
and there was no monitoring on the use of the funds in the RBF region. This meant that the
expected improvement in business planning from Year 1 to Year 2 was somewhat erratic.
The NU Health study tracked how well the supported health facilities under both models of
financing developed, monitored and revised their business plans to prioritise their spending and
improve service delivery. The NU Health team assessed how participatory the business planning
process was and what incentives exist for employees when the targets were met. As noted in the
first Lessons Learned Report, there were no significant differences in the business planning
process between the IBF and RBF health facilities. Most of the health facilities had participatory
business planning processes and were implementing the plans and making appropriate revisions
to reflect the facility’s evolving needs.

16
NU Health Lessons Learned II Report
Assessment Methodology
FGDs were conducted with health facility staff in three areas of interest listed below:
Business planning;
Staff motivation; and,
Perceptions on financing.
Findings
Overall, staff from both RBF and IBF health facilities reported an improvement in their work
environment and the quality of services that their facilities are now providing. Many reported an
increase in the number of patients, a reduction in drug stock outs and the upgrade or renovation
of health facility infrastructure. Although there were improvements observed in how healthcare
services are delivered at the health facilities, it was noted that some of these improvements would
not be sustainable without NU Health support once the programme ends. For example, most
health facilities reported that staff salaries or salary increments were being paid out of the funds
being provided by the NU Health programme to boost staff motivation. Concern also included how
subsidies for medicines will be maintained in the absence of credit line support.
Business planning and monitoring
It was found that health facility staff did not always participate in the development of the business
plans which were perceived to fall under their financial teams’ roles. This undermined the staff’s
ownership of the changes being made at the health facilities in the interest of meeting assessment
targets. The limited interaction between the financial and health management also affected efforts
to improve conditions at the facilities since the financial teams did not typically have the technical
knowledge about health facility operations. In the RBF health facilities where staff participated in
the business planning to some degree, staff felt that not enough incentives accrued to them
individually when the health facilities were awarded good scores by the NU Heath teams and
DHTs.
Motivation
Some of incentives provided to health workers and staff in return for achievement of health facility
targets included:
Allowances for or provision of accommodation: such as Minakulu HC3 providing a rent
allowance to the staff or Aber Hospital providing accommodation to the staff;
Allowances for or provision of meals to the staff during working days; and,
Bonuses or salary increments such as Alanyi HC3 providing bonuses once last year while
in Aduku HC2 bonuses are provided once a quarter.
However in some of the health facilities, staff remained demotivated. Some staff were displeased
with how facility leadership apportioned funding. It was noted that in some cases staff’s living
conditions were unimproved or salaries unchanged. Staff continually stressed the importance of
health facilities allocating some funds towards further professional development and other
employment benefits such as retirement packages or more bonuses.

17
NU Health Lessons Learned II Report
Perceptions on Financing: Funding autonomy and innovation
Supported facilities invested the NU Health funds in a number of areas that they felt needed
improvement including:
Procurement of medical equipment;
Payment of staff salaries and salary increments;
Construction or upgrading of health facility infrastructure;
Accommodation allowances; and,
Recruitment of additional staff.
Health workers in the RBF health facilities were aware of the new funding model and in some
cases they shared in the success of their health facility. In the cases where this was practised,
better teamwork was fostered and health workers reported increased accountability amongst
themselves and to management. In some cases, the staff reported receiving bonuses depending
on how well the health facility had performed during its assessments. When and where health
facility (HF) staff were not receiving what Management had planned or promised, there were some
examples of disgruntled staff sabotaging the QQA process by reducing quality of services to
ensure that the following QQA results would be poor, which would eventually penalise the HF.
Despite their recognition of the NU Health Study’s purpose, many staff were concerned about the
sustainability of the changes brought about once the study comes to an end. There were concerns
about shortages of essential medical equipment that the facilities needed to be able to provide
better quality health services. Sustaining the rates of subsidised medication was also cited as one
of the challenges that the health facilities would struggle with when the NU Health study closes.
There was a concern that in the absence of other support, the provision of improved quality
healthcare may not be sustained beyond the end of NU Health study.
Feedback on process improvements suggested by PNFPs
Respondents generally reported that health facility management would have benefitted from more
guidance in the investment or budgeting of received programme funds. For example in the RBF
facilities where improved delivery of health services did not reflect in any additional benefits for
employees, health workers suggested that future RBF programmes set a standard salary or that
more stringent conditions be put in place that provide for staff welfare.
Many also recommended that the programme be extended to run over a longer period of time for
it to have a longer lasting impact on the provision of healthcare services in this region. Some
suggested that the DHTs’ capacities should have been strengthened further to enable them to
have the same knowledge on quality health service delivery as the NU Health team. Some health
facility staff also felt that health facilities in more remote areas should have been awarded more
support given the difficulties in providing health services especially with the high staff turn-over
rate experienced in such settings.

18
NU Health Lessons Learned II Report
DHT Perspectives
One of the larger tensions with NU Health from the DHT perspective was the projects focus solely
on PNFPs. Understandably, the DHTs have an allegiance based on affiliation with the public
sector facilities. Despite their stated appreciation about the scope of the NU Health study, many
expressed an underlying resentment that the PNFPs get preferential treatment vis-à-vis public
facilities.
That said, many DHT staff noted their real appreciation for the opportunity to engage substantively
with the PNFPs. A number noted that they had applied their new skills and tools in results
verification and supportive supervision to facilities not participating in the study.
NU Health Staff Perspectives
NU Health staff noted the absence of financial analytic and management skills on the part of many
of the PNFPs. In the lower level facilities, there were also basic concerns about quality of care in
addition to data management/ utilisation capabilities.
NU Health staff had more salient observation however was around the “hands off” approach in the
RBF intervention facilities. As facilities came to focus on quality of care—which was good—and
to improve their results payments, staff were too frequently disappointed with the way many
PNFPs opted to use their results payments and often frustrated that they could do nothing about
it. By contrast, in the IBF facilities, where payments were necessary for business plan priorities
according to proscribed procurement process, there may have been some frustration with the
pace at which these business processes were adopted, but less with how funds were actually
used.
Policy implications for future RBF initiatives
While there are a range of implications for any future RBF initiatives working with PNFPs, the most
significant of these will be the parameters attached to the use of results payments. While the
“hands off” approach made sense for the purposes of the study, incite would have come with
tracking how facilities use their funds. There is a general view among participating stakeholders
that such a carte blanche approach would be neither desirable nor politically acceptable in an
operational context. Defining how to regulate the use of results payments, without inadvertently
creating perverse incentives or other unintended consequences will warrant significant attention.
6 QUALITY OF CARE
Background
In NU Health’s ToC, Quality of Care (QoC) is a critical factor on the path to better health. For the
purpose of the study, QoC is considered in terms of availability of essential equipment and
supplies, the availability of qualified and skilled human resources and how those personnel
performed in terms of prescription practice and adherence to clinical guidelines. The study also
considered client satisfaction including verification of service provision.

19
NU Health Lessons Learned II Report
QoC is dependent on the alignment of a range of critical inputs including adequate number, skills
and motivation of staff, as well as the availability of essential commodities that are necessary to
provide basic, routine health services and emergency treatment. To this end, the Ministry of Health
of Uganda has set out standards for the number of staff and the required skills mix for a given
level of facility to offer the required minimum level of health care delivery, without which the level
of quality of service will not be satisfactory. The baseline survey conducted by NU Health,
however, confirmed that many health facilities lacked essential drugs and equipment, as well as
the requisite number of appropriately skilled personnel for the particular level of service delivery
according to minimum government standards.
One of the inputs of the study was to increase availability, improve stock management and rational
use of essential medicines and health supplies (EMHS) in the 31 supported PNFP facilities in
both RBF and IBF regions. A credit line system for the EMHS was instituted with the Joint Medical
Stores, where the 31 PNFP facilities were able to order and receive EMHS directly to the facility.
During the first year of the study, laboratory and health facility equipment was procured and
distributed to category two facilities in both the RBF and IBF regions. The rationale was to ensure
that the level two facilities2 were in a position to provide basic laboratory and medical procedures
as a requirement of the minimum health care package hence creating a level ground to perform
the RBF/IBF experiment. The equipment provided in the seed grant included delivery beds,
autoclaves, delivery sets, drip stands, and examination couches, amongst others.
Having the requisite number and type of staff according to MoH norms was an inclusion criteria
for the study. The NU-Health human resource intervention is two pronged with direct support to
the District Health Team (DHT) through recruitment of vital staff and indirectly to the facilities
through the creation of a viable financial environment for the facilities to recruit the required
number of staff with the right skills mix. Ongoing availability of EMHS, equipment and appropriate
staffing levels is monitored regularly throughout the programme.
The programme established a range of verification mechanisms to monitor the data provided
by health facility managers. These are used to determine the level of funding received in RBF
facilities which is then matched for the IBF facilities. Firstly, a monthly check of the claimed
performance in service provision (Data Quality Assessment or DQA) is undertaken by external
verifiers from the programme in collaboration with the DHT. Secondly, to complement the DQA, a
Quarterly Quality Assessment (QQA) is conducted at each health facility and a quality score is
given. This score acts as an additional factor in calculating the level of funding attained by the
facility. A third mechanism of verification was Direct Client Verification (DCV) of a sample of clients
from each health facility who were contacted by mobile phone to verify whether or not they actually
received the service they were recorded as receiving. The main objectives of the verification were
to ensure the validity of facility reported data; complement Quarterly Quality Assessment (QQA)
data on client satisfaction; and understand from a patient viewpoint the cost incurred for different
services. The QQAs, undertaken by NU Health staff with DHT members, exposed on-going
2 These were lower level facilities which were close to but did not meet standard with respect to basic medical
equipment and infrastructure at the time of project start up.

20
NU Health Lessons Learned II Report
problems with adherence to appropriate clinical practices and MoH standard protocols. NU
Health put in place a range of measures to address these weaknesses in the health system,
monitored the effects of these actions and subsequently assessed the impact on clinical practice
regarding common illnesses and client satisfaction.
Assessment Methodology
Different methodologies were used to monitor the various aspects of quality of care:
Concerning availability of EMHS, health facilities were assessed on a quarterly basis to
see whether or not a particular item of equipment or commodity was available on the day
of the survey. Equipment availability was checked once a year and included in an
assessment of the level of functionality in order to monitor maintenance practices.
The level of staffing of qualified and skilled people was assessed annually according to
the MOH staffing norms for each level of care. A facility passes the required staffing
number and skills mix if they have the recommended number and personnel per position
at a given level of care.
Prescription practices for common childhood illnesses (malaria, pneumonia and
diarrhoea) are regularly monitored during the DQA/QQA process. In addition, they were
compared between the RBF and IBF health facilities during the baseline year (2011/12),
after one year of implementation (2012/13) and again after two years of implementation
(2013/14) through the conducting of a clinical audit. This audit also assessed the
competence of the most senior clinician to manage sick children by observing them during
up to ten consultations per health facility and scoring them according to the Integrated
Management of Newborn and Childhood Illnesses (IMNCI) parameters of good care. A
detailed methodology of the entire clinical audit study is provided in the full clinical audit
report (available on request).
Client satisfaction was gauged directly by conducting exit interviews with clients present
at the health facilities during the QQAs. This feedback was incorporated into the overall
QQA score. The DCV method was based on telephone interviews with clients sampled
from a range of clinic registers and followed a structured questionnaire guideline. The
interviews were conducted by independent non-clinical staff that were not engaged in the
usual day-to-day running of the field activities or engaged in clinical care, in order to
preserve confidentiality and avoid bias. The sample of patients who had attended services
relevant to NU Health was developed.3 A lower sampling percentage was used for
hospitals than in lower level facilities, with 1% of patients who received care at Hospital
level being sampled, 2% of patients who received care at HC3 level and 3% of patients
who received care at HC2. An exception was made for St. Mary’s Lacor Hospital that has
a large number of patients and as a result only 0.5% of eligible patients were sampled.
3 Cordaid, Sina (2010) PBF in action – theory and instruments. Performance Based Financing Course Guide. Cordaid.

21
NU Health Lessons Learned II Report
Table 2 illustrates the methodology used for each component:
Table 2 Methodology Summary
Area of
assessment
Methodology Sample size / scope Period
covered
Essential
equipment/
supplies
Facility
Survey
- Assessment of the availability and functionality of
selected equipment once annually:
i) delivery beds; ii) sterilisation equipment; iii) Rapid
Diagnostic Tests (RDTs); iv) ORT Corner; v)
microscope;
vi) oxygen cylinder; vii) oxygen delivery
equipment/oxygen concentrator
-Availability of 20 Essential Medicines and Health
Supplies
-31 health facilities (21 Acholi/RBF & 10 Lango/IBF)
2012/13/14
Skilled human
resources
Facility
Survey
- 31 health facilities (21 Acholi/RBF & 10 Lango/IBF)
- Staff availability according to MoH norms for each level
of care
2012/13/14
Prescription
habits
DQA/QQA
Clinical audit
IMNCI
31 health facilities (21 Acholi/RBF & 10 Lango/IBF).
Quarterly verification of data and quality scored against
comprehensive set of indicators (see NU Health’s DQA
and QQA tools)
Review of clinical practices at baseline, and after one
and two years of implementation using three cross
sectional studies for malaria (n=2,911), pneumonia
(n=1,520) and diarrhoea (n=2,608) case management
from Health Management Information System data in
the 31 PNFPs.
Observation of 247 child examinations in RBF PNFPs
and 105 examinations in IBF PNFPs.
2012/13/14
2011/12
2012/13
2013/14
2014
Client
Satisfaction
Exit
interviews
during QQA
Direct Client
Verification
Around 200 interviews held on average each quarter
from PNFPs assessed in that quarter with a total of 1520
interviews to date.
1,995 records were collected across all health facilities.
2012/13/14
Feb to Oct
2014
Findings
Highlights
Overall availability of EMHS items improved from 72% at baseline to 97% in the latest
assessment.
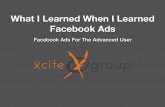
Average availability of seven items of essential equipment increased from 78% in 2013 to
82% in 2014.

22
NU Health Lessons Learned II Report
Availability of appropriately skilled staff increased from 52% to 90% in the RBF region and
from 70% to 100% in the IBF region.
Average QQA scores increased during programme implementation from around 60% to 80%
in the RBF region and from under 50% to over 60% in the IBF region, with the highest
increases occurring at HC3 level.
A clinical audit showed that after two years of programme implementation and after adjusting
for confounding factors, compared to a child in the IBF region, a child in the RBF region was:
three times more likely to be treated correctly for malaria;
almost seven times more likely to be treated correctly for pneumonia; and,
over eight times more likely to be treated correctly for diarrhoea.
Clinical management of sick children, assessed using the IMNCI checklist, improved over
time in both RBF and IBF regions.
The direct client verification exercise to assess satisfaction revealed that 78% of those
contacted were satisfied with the service received.
Availability of EMHS and Equipment
The average availability of EMHS items improved to 96.5% in the most recent assessment with a
slightly higher availability recorded in the intervention RBF facilities (97%) compared to in the IBF
facilities (96%). This is higher than the overall availability results in the baseline and the first
Lessons Learned (LL) report which were 72% and 94% respectively.
All RBF facilities and 90% IBF facilities had over 90% of the basket of EMHS available on the day
of the survey; this is an improvement from the 81% and 70% in the last LL report respectively.
This is presumably still a direct reflection of the impact of monetary incentives which are provided
to facilities that score 100% in availability of the priority EMHS in the RBF health facilities during
the QQA. It is, however, worth noting that despite the provision of incentives to facilities that score
highly in the pharmaceutical indicators, some RBF facilities have failed to score 100% while some
facilities in the IBF region have scored 100%. The good performance in the IBF region can be
attributed to the regular supportive supervision and the credit line which is provided in both arms
of the study. The stock-out incidence of Insecticide treated mosquito nets and vitamin A has
continued to be registered in the IBF region with their stock out rate at 30% and 20% respectively.
Three commodities registered the highest incidence of stock outs in the RBF region, namely;
mosquito nets, suphadoxine-pyramethamine (SP) and measles vaccine, all at 10% on the day of
the survey. It is worth noting that the EMHS which were out of stock are those that are provided
fully by the government structures. There is sometimes a break in the supply chain of these
commodities hence rendering a stock-out in ill-prepared facilities. Availability has continued to be
better at higher level facilities compared to the lower level facilities; this is due to a better skill set
of pharmacists, dispensers and trained pharmacy staff who run this department. Hospitals also
have much bigger budgets than lower health facilities and prioritization is given to good
pharmaceutical practices.
In both the first (2013) and second (2014) annual follow-up rounds of assessment, availability of
essential equipment was highest in hospitals and decreased by level of care. Hospitals and HC4
had a 100% availability of the seven commodities assessed, followed by HC3 and lastly HC2. The

23
NU Health Lessons Learned II Report
average availability of equipment was 78% in 2013 and increased to 82% in 2014 with a higher
availability recorded in the intervention RBF facilities on both occasions (81% and 86% in the first
and second rounds respectively) compared to the control IBF facilities (78% and 81%
respectively). This minimal difference in availability may reflect the impact of monetary incentives
in the RBF health facilities. Oxygen cylinders, oxygen delivery equipment and oxygen
concentrators were least available in both occasions for both the RBF and IBF regions. It is
presumed that this reflects the relative cost of these items which meant only hospitals and large
HC3s purchased them. Sterilizers, delivery beds, RDTs and ORS were provided as a seed grant
and quarterly through the credit line; this explains their high percentage availability in both rounds
of assessment.
Figure 2 Availability of equipment in the intervention and control facilities
Availability of qualified and skilled human resources
The findings showed that there were tremendous improvements in the recruitment and retention
of skilled staff for both the RBF and IBF health facilities. The Lango region demonstrated a better
staffing skills mix for 10/10 (100%) of the facilities compared to 18/20 (90%) in the Acholi RBF
region. Both regions registered an improvement from the first LL period from 52% and 70%
respectively for RBF and IBF regions. St Francis Akia, PAG and Aber hospital that were lagging
in the last LL period have since improved in their recruitment for the required personnel and skills

24
NU Health Lessons Learned II Report
mix. In the RBF Acholi region the recommended staffing and skills mix was recorded in 90% of
the facilities with gaps only noted in the lower level facilities of Wi Anaka and St Luke HC2, which
both lack a midwife and yet conduct deliveries. It is worth noting that there is no association
between funding mechanism and the adequate numbers of the appropriate skilled staff. All
hospitals and HC3 across both the RBF and IBF regions had the required number of staff and skill
mix to offer the minimum standard of care.
Prescription practices in health service delivery
QQA Scores
The QQA is one of the tools used to monitor the provision of quality services: it includes an
assessment of the quality of ANC services, delivery care, under-five Out-Patient Department
(OPD) services, immunisation, general OPD services, hygiene and infection prevention,
laboratory standards, pharmaceutical management, inpatient care and data management. The
QQA scores obtained by PNFPs have gradually increased over time as shown in the graphs
below. The most significant improvement has been made at the HC3 level in both regions while
hospitals have made the least impressive progress. While this assessment looks at broader quality
issues rather than simply clinical practice, it includes areas such as use of the partograph,
appropriate treatment of malaria, pneumonia and diarrhoea cases, and rational antibiotic use.
Figure 3 QQA scores in Acholi/RBF region Figure 4 QQA scores in Lango/IBF region
Clinical Audit
The clinical audit found discernible improvement after two years of implementation for all clinical
practices assessed by the audit. These changes occurred mostly in the second year, and were
generally more pronounced in the RBF health facilities. The key findings regarding prescription
practices for common illnesses are described below, along with a summary of IMNCI-related
clinical practice.
Malaria
A malaria prescription was considered correct when each definitive diagnosis was supported by
either positive microscopy or Rapid Diagnostic Test (RDT) and the choice of medication matched
the illness classification. The first line of treatment for uncomplicated malaria is a combination of
artemether and lumefantrine (Ministry of Health Uganda, 2010). Until recently, the first line for
complicated malaria was oral or injectable quinine but artesunate is now recommended as a safer
and more efficacious option (Dondorp, et al., 2010).

25
NU Health Lessons Learned II Report
At baseline and during year one and two of implementation, the distribution of correctly treated
malaria cases was different between RBF and IBF health facilities. In all periods, the proportion of
correctly treated cases was higher in the RBF setting and the difference between RBF and IBF
widened in the second year of implementation.
Figure 5 Proportion of correctly treated malaria cases in RBF and IBF regions
Multivariate analysis looked at the effect of age and sex of the child, and level of health facility:
only the latter was a confounding factor. After adjusting for this effect, the odds of a child being
correctly treated showed an increasing trend from baseline (Odds Ration [OR] 1.71; Confidence
Interval [CI] 1.21-2.40) through to year one (OR 1.80; CI 1.33-2.44) and year two (OR 3.15; CI
2.13-4.65) in the RBF as compared to the IBF region. These differences were statistically
significant.
Figure 6 Trends in correct treatment of malaria cases at different facility levels in RBF and
IBF regions
In summary, after adjusting for confounding factors, a child in the RBF region was three times
more likely to be treated correctly for malaria than a child in the IBF region after two years of

26
NU Health Lessons Learned II Report
programme implementation. This suggests that the RBF mechanism is having a positive effect on
influencing clinical practice of health care providers.
Pneumonia
The national clinical guidelines recommend that each child with a diagnosis of pneumonia should
receive an antibiotic and Vitamin A supplementation (Ministry of Health Uganda, 2010). At
baseline and during year one and two of implementation, the distribution of correctly treated
pneumonia cases varied between RBF and IBF health facilities. In all periods, the proportion of
correctly treated pneumonia cases was higher in the RBF setting, and the difference between RBF
and IBF widened in the second year of implementation
Figure 7 Percentage of pneumonia cases treated correctly in RBF vs IBF regions
Multivariate analysis looked at the effect of age and sex of the child, and level of health facility: as
was the case for malaria, only the latter was a confounding factor. After adjusting for this effect,
the odds of a child being correctly treated were still higher in the RBF region when compared to
IBF at baseline (OR 22.14 CI 7.75-63.24), year one (OR 4.16 CI 2.80-6.17) and year two (OR 6.63
CI 3.34-13.17). These differences were statistically significant.

27
NU Health Lessons Learned II Report
Figure 8 Trends in correct treatment of pneumonia cases at different facility levels in RBF
and IBF regions
In summary, after adjusting for the influence of the health facility level, a child in the RBF region
was almost seven times more likely to be treated correctly for pneumonia than a child in the IBF
region after two years of programme implementation. This suggests that the RBF mechanism is
having a positive effect on influencing clinical practice of health care providers.
Diarrhoea
The national clinical guidelines recommend that each child with diarrhoea should receive
rehydration therapy and Zinc supplementation (Ministry of Health Uganda, 2010). At baseline and
during year one and two of implementation, the distribution of correctly treated diarrhoea cases
varied between RBF and IBF health facilities. In all periods, the proportion of correctly treated
diarrhoea cases was higher in the RBF setting and the difference between RBF and IBF widened
in the second year of implementation
Figure 9 Percentage of diarrhoea cases treated correctly in RBF vs IBF regions

28
NU Health Lessons Learned II Report
Multivariate analysis looked at the effect of age and sex of the child, and level of health facility:
once again, only the latter was a confounding factor. After adjusting for this effect, the odds of a
child being correctly treated were higher in the RBF compared to the IBF region at baseline (OR
2.41; CI 1.71-3.39), in the first year of implementation (OR 5.34 CI 3.84-7.42) and in the second
year (OR 8.34 CI 4.95-14.08). These differences were statistically significant.
Figure 10 Trends in correct treatment of diarrhoea cases at different facility levels in RBF
and IBF regions
In summary, after adjusting for the influence of the health facility level, a child in the RBF region
was over eight times more likely to be treated correctly for diarrhoea than a child in the IBF region
after two years of programme implementation. This suggests that the RBF mechanism is having
a positive effect on influencing clinical practice of health care providers.
IMNCI-related Clinical Practice
Clinician competence in both RBF and IBF health facilities was observed and assessed against
IMNCI parameters of good clinical practice (assessment tool available in clinical audit report)
during consultations in OPD. The first round of observations for each health facility was conducted
in early 2014 and subsequently repeated after a minimum period of three months. The scores are
given for a total of 227 cases observed in the RBF and 74 in the IBF health facilities.
Table 3 below summarizes the number of cases seen in each health facility by level of care and
region during the second year of implementation and shows the summary of scores for the three
rounds of assessment in the RBF region and two rounds in the IBF region.

29
NU Health Lessons Learned II Report
Table 3 Summary of overall scores in clinical management of sick children in OPD using
IMNCI checklist in the RBF & IBF health facilities
RBF % (range) IBF % (range)
Type of
Health
Facility Round 1 Round 2 Round 3 Round 14 Round 2
HC2
54 (22-83
n=53)
57 (31-92
n=42) 64 (54-85 n=15) 38 (n=10) 71 (61-82 n=20)
HC3
53 (37-80
n=18)
80 (65-89
n=19) 74 (65-80 n=20) 48 (n=5) 64 (47-89 n=22)
Hospitals
36 (13-48
n=20)
69 (53-68
n=20) 68 (53-84 n=20) 79 (75-83 n=2) 66 (62-71 n=15)
In general, there was an improvement among all health facilities in the RBF group from the
assessment in the first round to the second round, which was more or less maintained in the third
round. In the IBF health facilities, improvement between the first and second rounds was observed
only at HC2 and HC3 level of care but not in hospitals. The apparent lack of improvement on
average at hospital level in the IBF hospitals is attributed to the lower performance by Aber
Hospital in the second round where high staff turnover seems to have influenced the lack of
continuity in adhering to the recommended clinical practices.
The following graphs compare the trends in changes and shows that the improvements have been
equally impressive (and more so in the case of HC2 level) in IBF facilities compared to RBF
facilities, apart from hospital level as noted above. The effect of observation itself, rather than the
incentive mechanism in RBF facilities, is therefore likely to be the main reason for improvements
although there could be additional external factors influencing change that are unrelated to the
programme effect. In any case, the third round of assessment in RBF facilities shows that these
improvements may not be maintained as there was a levelling off in average scores at HC3 and
hospital level. This could be due to some level of complacency after a period of time or the limited
capacity of the clinical staff to improve without more training.
4 Only one facility each was included at HC2 and HC3 levels.

30
NU Health Lessons Learned II Report
Figure 11 Changes in average IMNCI assessment scores across RBF and IBF health
facilities at HC2, HC3 and hospital level
Client Satisfaction
In the DCV exercise, 40% of 1,995 patients sampled could be contacted by telephone. The two
most common reasons for unsuccessful calls were that the number was not available on the
network/did not connect (71.7%) or that the phone was switched off (13.5%). When a number
could not be reached, it was dialled again twice over the next 24h. The vast majority of clients
(78%) who were contacted, reported that they had received the service in question and that they
were satisfied with the service. Reasons given for satisfaction included provision of
comprehensive services and positive staff attitudes. Reasons for dissatisfaction with services
included long waiting times, overcrowding of facilities, lack of medicines and poor facility
upkeep/cleanliness. Information on costs incurred highlighted a wide range of fees; however, there
was insufficient detail gathered to draw conclusions. More in-depth analysis would be required to
achieve this, such as comparing receipts given to patients with health facility accounting records.
A broader look at the client satisfaction is outlined in the recent NU Health Client Verification
report, December 2014).
Policy Implications for Future RBF Initiatives
The widespread improved availability of essential equipment, drugs and other supplies is
associated with positive changes in prescription practices and adherence to national protocols,
particularly in the RBF region. It is also associated with high levels of client satisfaction in general.
As the availability of commodities was similar and consistent in both RBF and IBF regions, the
significant improvement in malaria, pneumonia and diarrhoea treatment practices suggests that
RBF may specifically contribute to some aspects of improved clinical behaviour. In the first LL
period, compliance to recommended malaria treatment was not significantly better in the RBF
region compared to the IBF region and this was attributed to malaria requiring more complex

31
NU Health Lessons Learned II Report
management. However, over time this improved substantially in the RBF region, suggesting that
one year is too short a time period for more extensive change in clinical practice to take place.
The improvement noted in the use of recommended treatment protocols for malaria, diarrhoea
and pneumonia in the RBF relative to IBF region is not surprising. This observation is also
supported by the generally positive trend in compliance to good clinical practice among clinicians
seeing children aged less than five years in the Out-Patient Department during the IMNCI
assessment. The scale of improvement is quite large, illustrating how quickly incentives in the
RBF context can turn around quality of care for a range of clinical practices. Secondly, the rapid
improvement for lower level facilities relative to hospitals is attractive for strategies such as
universal health coverage that aim to increase access to quality health care with a relatively low
additional level of inputs.
As noted in the clinical audit report after year one, there is clearly scope to stimulate change in
ways other than using RBF mechanisms since improvements were also observed in the IBF
region. Important inputs in this case include regular supportive supervision, and a regular supply
of essential drugs and other commodities to all health facilities.
Concerning client verification, a high level of concurrence between health facility records and client
feedback was observed. It was also established that where records are available, client verification
can be conducted using telephone calls. Furthermore, the methodology used with telephone-
based validation was documented, providing a framework that might be adopted for use in similar
settings. However, given the current pattern of phone ownership and network coverage, this
approach will not likely provide a statistically representative indication of the experience of the
overall patient/client population.
Identifying specific reasons for satisfaction or dissatisfaction with services requires detailed
probing as clients generally report high levels of satisfaction which may simply be reluctance to
criticise people of power. Understanding the specific needs and desires of clients could be helpful
in orienting health care providers to be more responsive and considerate towards their clientele.
The DCV method can, therefore, complement other measures of eliciting client satisfaction by
providing more detailed information so long as its current biases are taken into account.
Institutionalising the use of telephones as a means of validation of service provision and
performance may have a place in low resource rural settings. The MoH has already revised
registers to include a phone contact. Further investigation, however, is in order to assess whether
the relatively low response rates have biases in phone based DCV findings. If Uganda adopts
plans to take RBF to scale, the cost of verification will need to be considered very seriously. A
comparison of phone versus the gold standard of physical verification in the client’s home might
provide an indication, even on a flawed sample basis, of whether phone-based DCV is good
enough to fulfil its purpose.

32
NU Health Lessons Learned II Report
7 HEALTH OUTCOMES
In this section NU Health examines three aspects of health outcomes, namely: disease
presentation patterns for clients attending health facilities in the RBF and IBF regions (case load);
the client profile by age and sex (case mix); and perinatal outcomes from a clinical audit.
Background
Uganda still faces a high burden of preventable communicable diseases in the vulnerable
populations of women and children aged less than five years as well as a growing problem with
non-communicable disease. Amongst many other factors, quality of care is an important supply
side barrier that influences the use of services by the general population (Ministry of Health
Uganda & Macro International, 2007). For example, there is a known association between
improved monitoring during labour and better perinatal outcomes (Tayade & Jadhao, 2012); yet
use of the partograph, a key tool in monitoring the progress of labour, is still low in Northern
Uganda.
The NU Health programme targets the greatest weaknesses in the health system and the most
commonly occurring illnesses by providing inputs to essential medicines and commodities and
supportive supervision to promote adherence to the best clinical practices. This is enhanced by
additional financing coupled with facility autonomy that is bound in an agreement to ensure the
maintenance of basic health system inputs for participating providers.
Assessment methodology
The electronic DHIS2 that captures data at the district health office from all facility based providers
was used as the source to examine disease ranking patterns and changes in numbers of clients
attending services at NU Health supported health facilities from baseline (2011/12) through the
first year (2012/13) and second year (2013/14) of implementation.
The practice of labour monitoring and associated perinatal outcomes was assessed in a clinical
audit which examined records from the previous three years in all NU Health-supported PNFPs.
Cases constituted a sample of mothers in each year with perinatal death (neonatal death, fresh
still birth, macerated still birth) as an outcome. The cases were matched with controls with live
births of similar maternal age and parity. The study looked at correlations with the level of partial
or complete monitoring using partographs.
Findings
Disease Presentation Patterns
Clients attending the health facilities supported by NU Health in both the Acholi (RBF) and Lango
(IBF) regions were ranked by age and sex for the top ten most prevalent conditions in the baseline
year 2011/12, the first year of implementation 2012/2013 and the second year of implementation
2013/2014. The data presented have been extracted from DHIS2 and are been based on OPD
figures reported by the facilities.

33
NU Health Lessons Learned II Report
Children
Among children aged less than five years, the top ten conditions were similar for both boys and
girls and in the two regions (tables below), especially after injuries dropped from the girls’ ranking
after the baseline. Malaria, pneumonia and diarrhoea remain among the top five conditions in both
regions over the last three years. In the Acholi region, the ranking for the top five conditions was
consistent across the three years for both boys and girls with pneumonia and cough being more
prominent and malaria less prominent in the last year. This is consistent with the findings of the
clinical audit which shows improving clinical management of malaria in RBF facilities. The ranking
for the top five conditions was similar in the Lango region except that anaemia featured more
prominently, being ranked as either the 2nd or 3rd for all three years for both boys and girls. Malaria
remained the most prevalent disease in Lango for boys in the latter two years and for girls for all
three years.
Table 4 Top 10 ranking for U5 boys over three years
Acholi Lango
Disease 2011/12 2012/13 2013/2014 2011/12 2012/13 2013/2014
Cough or cold 1 1 2 4 3 3
Malaria 2 2 4 2 1 1
Pneumonia 3 3 1 5 5 5
Acute Diarrhoea 4 4 3 1 4 4
Skin diseases 5 5 5 6 7 6
Ear, Nose,
Throat (ENT)
conditions
6 10 7 10 6 10
Intestinal Worms 7 6 8 9 8 8
Urinary Tract
Infections
8 9 10 8 11
Other eye
conditions
9 8 6 10
Anaemia 10 3 2 2
Gastrointestinal
disorders (non-
infective)
7 9 7 9 7
Table 5 Top 10 ranking for U5 girls over three years
Acholi Lango
Disease 2011/12 2012/13 2013/2014 2011/12 2012/13 2013/2014
Cough or cold 1 1 1 3 3 2
Malaria 2 2 4 1 1 1
Pneumonia 3 3 2 5 5 5
Acute Diarrhoea 4 4 3 4 4 4
Skin diseases 5 5 5 6 7 6
Ear, Nose,
Throat (ENT)
conditions
6 10 7 8 6 9

34
NU Health Lessons Learned II Report
Intestinal Worms 7 6 8 9 9 8
Urinary Tract
Infections
9 10 10 10
Other eye
conditions
9 8 6 10
Anaemia 10 2 2 3
Gastrointestinal
disorders (non-
infective)
7 9 7 8 7
Injuries 8
Adults
The most prevalent health conditions among adults in the two regions (tables below) are malaria
and cough although anaemia and diabetes are prevalent in Lango and to a lesser extent in Acholi,
while pneumonia and cardiovascular diseases are more prevalent in Acholi and less so in Lango.
Reproductive health problems (Pelvic Inflammatory Disease) represent an increasing non-
communicable condition reported among adult female patients in both regions over the last three
years. This pattern of conditions remains consistent with the emerging national profile of a double
burden of both communicable and non-communicable illnesses.
Table 6 Top 10 ranking for male adults over three years
Acholi Lango
Disease 2011/12 2012/13 2013/2014 2011/12 2012/13 2013/2014
Cough or cold 1 1 1 3 2 3
Malaria 2 2 2 1 1 2
Injuries 3 3 3 10 8 5
Pneumonia 4 8 8
Intestinal Worms 5 5 6 8 10 8
Urinary Tract
Infections
6 6 5 6 6 6
Anaemia 2 3 1
Gastrointestinal
disorders (non-
infective)
4 4 7 7 4
Skin diseases 7 7 7 9 9 10
Cardiovascular
diseases
8 10 10
Hypertension 9 9 9 4 4 7
Diabetes Mellitus 5 5 9
Acute Diarrhoea 10

35
NU Health Lessons Learned II Report
Table 7 Top 10 ranking for female adults over three years
Acholi Lango
Disease 2011/12 2012/13 2013/2014 2011/12 2012/13 2013/2014
Cough or cold 1 1 1 4 3 3
Malaria 2 2 4 1 1 1
Injuries 4 9 9 10
Pneumonia 6 10 10
Intestinal Worms 3 6 8 10 10 9
Skin diseases 7 7 7 9 9
Urinary Tract
Infections 5 5 5 6 6 4
Anaemia 2 2 8
Gastrointestinal
disorders (non-
infective)
3 2 3 5 2
Cardiovascular
diseases 9
Hypertension 10 8 6 5 4 5
Diabetes
Mellitus 7
Pelvic
Inflammatory
Disease (PID)
8 4 3 8 8 6
Malaria in
Pregnancy 7 7
Acute Diarrhoea
Rankings have been relatively consistent over the three years, particularly for children. Some
exceptions have occurred in adults in relation to non-communicable diseases as noted above. A
hypothesis around ranking was that initially more vulnerable children with illnesses constituting
the larger burden of disease would attend health care services at facilities supported by NU Health
and increasingly occupy the top rankings. Although in the longer term, one might see a reduction
in illnesses that are being better managed and where more effective prevention measures are
being provided, NU Health is not conducting enough targeted preventive level efforts to claim any
attribution in the short to medium term.
The information in the DHIS2 used to rank health-related conditions is reported data and, although
discrepancy rates between reported and verified data have improved significantly over time, they
are still subject to variation, especially in the IBF region where hospital/HC4 level data currently
shows a discrepancy rate of -19%. It is possible that the changes in rankings observed reflect
seasonal variations in the prevalence of illness and that the time period studied may also be too
short to draw substantive conclusions. It is furthermore unclear whether these changes observed
are in any way related to the funding mechanism or to changes in the quality of care provided or
other contributory factors.

36
NU Health Lessons Learned II Report
The data used reflect service statistics from all NU Health supported facilities in the two regions. These facilities provided approximately 17% of overall services delivered in Acholi and just under 10% in the Lango sub-region after one year of implementation. In the second year of implementation, these proportions fell in both regions to 12% and just under 6% as shown below in Table 8.
Table 8 Contribution of OPD Consultations by NU Health Supported Health Facilities in
Acholi and Lango
OPD contribution of 20* PNFP to each Acholi District
(FY13-14) from DHIS2
0-4 Years 5 and Over Total
Agago 8.77% 8.62% 8.66%
Amuru 30.62% 7.82% 15.16%
Gulu 27.83% 12.98% 16.68%
Kitgum 17.51% 13.08% 14.22%
Nwoya 8.36% 3.22% 4.45%
Pader 2.84% 1.41% 1.78%
Average 19.54% 9.74% 12.33%
OPD contribution of 10 PNFP to each Lango District (FY13-14)
0-4 Years 5 and Over Total
Alebtong 4.49% 3.73% 3.94%
Apac 1.11% 0.56% 0.66%
Lira 11.32% 8.20% 9.03%
Oyam 6.13% 6.70% 6.58%
Average 7.02% 5.21% 5.63%
*It should be noted that the FY13-14 figures in Acholi are based on 20 and not 21 PNFP due to
the suspension of St Joseph Minakulu HC2.
When comparing the two years of data, we see that OPD attendance has increased slightly in the
Acholi districts (8%) but much more significantly (51%) in the Lango districts while OPD
attendance in PNFP supported by NU Health has decreased in both regions. Clearly this is a
matter of concern as one of the objectives of NU Health is to increase access to services and thus,
we would expect the OPD numbers to increase. However, these figures are based on DHIS2 data
and our assumption is that the DHIS2 OPD data of FY12-13 were seriously inflated while the
FY13-14 ones are more realistic due to the NU Health intervention and for rewarding/stimulating
more reliable reporting of data.

37
NU Health Lessons Learned II Report
Table 9 Service Utilisation Change
ANALYSIS OPD ATTENDANCE FY12-13 versus FY13-14
AT DISTRICT LEVEL FY12-13 FY13-14 DIFFERENCE ∆%
6 districts in Acholi 1,893,473 2,051,957 158,484 8%
4 districts in Lango 1,101,675 1,667,525 565,850 51%
AT PNFP LEVEL FY12-13 FY13-14 DIFFERENCE ∆%
20 Acholi PNFP 309,800 252,991 -56,809 -18%
10 Lango PNFP 107,394 93,827 -13,567 -13%
In support of this, the figures below shows the verified OPD figure trend which has increased
substantially in Acholi PNFP but less so in Lango facilities:
Figure 12 Verified OPD numbers
Client Profile
The patients attending health facilities participating in the NU Health programme in both regions
were compared by age and gender for the top fifteen most prevalent health conditions in the
baseline year 2011/12 and the two years of implementation 2012/2013 and 2013/2014. Error!
eference source not found.In both regions, adult males formed the lowest proportion of
attendance (figure below), except in Lango region during the last year where they represent the
second largest group. The relative contribution of each of the gender and age categories remained
similar from baseline to end of year two in the Acholi region, apart from a slight increase in the
adult female category over the three years. In the Lango region there was a sharp drop in the
proportion of younger (<5 years) males reported to have attended health care services from
baseline (49%) to end of year one (21%); this reducing trend continued in year two (18%) but was
less pronounced. There was also a sharp increase in the proportion of adult females (>5 years)
reported to have attended health care services from baseline (26%) to the end of year one and
year two (to 39%). There is no obvious association between these changes and the funding
mechanism.

38
NU Health Lessons Learned II Report
Table 10 Client Profile by region, age and gender based on the top fifteen prevalent health
conditions
RBF IBF
2011-12 2012-13 2013-14 2011-12 2012-13 2013-14
Fem 24% 29% 31% 26% 39% 39%
Male 17% 17% 16% 12% 19% 26%
Girl <5 29% 26% 24% 13% 21% 17%
Boy <5 30% 28% 29% 49% 21% 18%
U5 Male29%
U5 Fem24%
Adult Male16%
Adult Fem31%
Client profile of 20 Acholi PNFPFY 13-14
U5 Male18%
U5 Fem17%
Adult Male26%
Adult Fem39%
Client profile of 10 Lango PNFPFY 13-14

39
NU Health Lessons Learned II Report
Perinatal Outcomes
Neonatal mortality, defined as death of an infant during the first 28 days of life, is a major aspect
of infant and child mortality. In 2013 it accounted for 44% of deaths in children under the age of
five years globally5 and 33% in Uganda6. The bulk of neonatal deaths occur during labour or in
the first week of life, with half of these occurring within the first 24 hours after birth. About 70% of
these deaths could be prevented if emergency and obstetric care interventions were made
available and used by 90% of mothers and babies (Lawn and Kerber, 2006). Instituting and
maintaining the correct use of partographs has been associated with up to 50% improvement in
both maternal and perinatal outcomes (WHO, 2012).
The clinical audit undertaken in NU Health assessed the use of the partograph during labour and
its association with perinatal outcomes. The figure below illustrates that the overall level of
complete labour monitoring improved over time and this was more pronounced for mothers (both
cases and controls) in the RBF region. In the IBF region, improvements were higher for live births
(controls) than for perinatal deaths (cases) but the absolute levels of monitoring were lower for
both groups compared to the RBF region.
Figure 13 Percentage of labour cases (perinatal deaths) and controls (live births) that
received complete monitoring with a partograph
Figure 14 below further summarises the comparison in performance between RBF and IBF regions
for any type of labour monitoring among mothers with perinatal deaths (cases) and those with live
births (controls) from baseline to year 2 of implementation. In both the RBF and IBF regions, there
was steady improvement in any type of labour monitoring for cases and controls. Overall, the
improvements in absolute levels of labour monitoring were consistently better in the RBF region
although the relative improvements were also impressive in the IBF region.
5 UNICEF 2014, http://data.unicef.org/child-mortality/neonatal 6 Countdown to 2015 - Uganda 2014 report

40
NU Health Lessons Learned II Report
Figure 14 Percentage of labour cases (perinatal deaths) and controls (live births) that received any
monitoring (partial or complete) with a partograph
The difference in means calculation (summarised in the table below) suggests that after the first
and second years of implementation, there were increases in the proportion of all mothers (cases
and controls combined) that had been completely monitored during labour. The increases in labour
monitoring were more pronounced in the RBF region.
Table 10 Difference in means calculation for complete monitoring of labour progress combined for
mothers with live births (controls) and perinatal deaths (cases) in the RBF and IBF health facilities
RBF IBF
Mean % with
Confidence
Interval
% Difference in
means between
years
Mean % with
Confidence
Interval
% Difference in
means between
years
Baseline
(2011/2012)
9.3 (7.1-11.7) 0.0 0.0 0.0
Year 1
(2012/2013)
27.2 (22.7-31.6) 27.2 2.5 (1.0-4.0) 2.5
Year 2
(2013/2014)
54.4 (49.6-59.2) 28.0 19.9 (15.3-24.5) 17.4
Total after two
years
55.2 19.9
As summarised in Table 11 the difference in mean increase of the proportion of all mothers that
received any monitoring during labour was slightly more in the IBF region after two years.

41
NU Health Lessons Learned II Report
Table 11 Difference in means calculation for any monitoring of labour progress for mothers with
live births (controls) and perinatal deaths (cases)
RBF IBF
Mean % with
Confidence
Interval
% Difference in
means between
years
Mean % with
Confidence
Interval
% Difference in
means between
years
Baseline
(2011/2012)
19.2 (16.2-22.3) 0.0 0.0 0.0
Year 1
(2012/2013)
36.2 (31.4-40.9) 17.0 26.9 (22.7-31.0) 26.9
Year 2
(2013/2014)
64.0 (59.4-68.7) 27.8 50.2 (44.4-56.0) 23.3
Total after two
years
44.8 50.2
In summary, at baseline in the RBF region, mothers with perinatal deaths were more likely to have
received complete or any (including partial or complete) labour monitoring compared to those with
live births. In the IBF region there was no evidence that either mothers with perinatal deaths or
live births had been partially or completely monitored during labour as no partograph records were
found. During the first and second years of implementation, although there were substantial
increases in the overall level of monitoring during labour, there was no significant difference in the
level of any or complete labour monitoring between mothers with live births and those with
perinatal deaths in the RBF region. Similarly there was no significant difference between the level
of any or complete labour monitoring for live births and perinatal deaths in the IBF region for the
first year, but in the second year, mothers with perinatal deaths were only half as likely to have
received complete or any monitoring during labour as compared to those with live births.
Policy Implications for Future RBF Initiatives
There is a considerable and growing burden of non-communicable diseases, as well as the
existing communicable ones and RBF programmes targeting adult populations will increasingly
need to take this into account. The general trend emerging in NU Health-supported PNFPs shows
an increase in the volume of services which supports the hypothesis that improvements in quality
are associated with increased use. Better perinatal outcomes are associated with improved
monitoring during labour and the clinical audit demonstrated that complete labour monitoring
improved substantially after two years of implementation. The lack of variation between mothers
with live births and perinatal deaths is suggestive of systematic institutionalisation of the practice
in the RBF region. The relatively lower monitoring of mothers with perinatal deaths compared to
those with live births in the IBF region could potentially be explained in part by the lack of incentive
for faster change. The quality of labour monitoring in the RBF health facilities was monetarily
incentivised whereas this was not so in the IBF region. Lack of consistent use of the partograph
as a monitoring tool to assess progress during delivery should be of serious concern to health
managers and facility staff, as it prevents mothers receiving quality obstetric care and endangers
the lives of both mothers and babies.

42
NU Health Lessons Learned II Report
8 VALUE FOR MONEY
The UK’s National Audit Office (NAO) defines good value for money as “the optimal use of
resources to achieve the intended outcomes”, where ‘optimal’ is taken to be “the most desirable
possible given expressed or implied restrictions or constraints.” (NAO)
To achieve the optimal use of resources, value for money approaches tend to be guided by
aspects of economy -spending less, efficiency - spending well, and effectiveness - achieving
greatest possible outcomes from output, or, spending wisely. These concepts are now the
generally accepted starting point for Value for Money (VfM) analysis, along with the cross-cutting
considerations of equity and sustainability.
Economy Getting the best value inputs
Efficiency Maximising outputs for a given level of inputs
Effectiveness Ensuring that the outputs deliver the desired outcome
Equity Ensuring that the benefits are distributed fairly (ICAI 2011)
Cost
effectiveness
A measure of impact that the programme interventions achieve
relative to inputs
Sustainability A programme approach which aims to achieve high intervention
coverage as a means to lasting impact
£ Inputs Outputs Outcomes Impact
Economy Efficiency
Effectiveness
Cost Effectiveness
Equity

43
NU Health Lessons Learned II Report
VFM can be seen as a simple, but continuous, iterative process of identifying and implementing
further efficiencies and cost savings, applied consistently to an intervention to achieve lasting
impact, while maintaining programme effectiveness.
Value for Money (VfM) is also important for public accountability, and particularly in the Ugandan
context for maximising the prospects towards achieving Universal Health Coverage (UHC). In
addition to increasing absolute levels of investment and expenditure, countries like Uganda need
to ensure that the existing investment/expenditure is well utilised and leads to the desired
outcomes in terms of approaching UHC in addressing people’s health needs in an affordable and
sustainable way.
The aim of the NU Health study is to generate greater evidence about costs and benefits of RBF
as a means of achieving better VfM and accountability in health. The theory is that aligning
incentives will stimulate improved performance within the health system, while accountability is
ensured by making the ‘incentive to performance’ link visible to beneficiaries. Therefore, to
demonstrate what is being achieved at what cost, NU Health monitors financial inputs provided to
both RBF and IBF facilities, and the associated health outputs and outcomes.
Assessment Methodology
This section aims to take a broad look at the VfM ‘Three ‘e’s’ principles to draw out:
What limitations are built into the programme design which would restrict full VfM
analysis?
How can each of the ‘three ‘e’s’ be applied in a NU Health context?
What programmatic lessons have emerged?
What are the implications for policy development stemming from the programmatic
example?
Throughout the review the NAO’s analytical framework on VfM depicted below, will underline the
review.

44
NU Health Lessons Learned II Report
Figure 15 - NAO Analytical Framework for assessing Value for Money
Limitations
VfM – A controlled study vs a national programme? The NU Health programme provides a
degree of verification, data collection and analysis which is significantly more robust and resource
intensive than would be anticipated in a more routine ‘implementation only’ model, or indeed a
national system. This not only increases the financial inputs but also, adds a confounding factor
to the overall impact assessment. It is unclear the degree to which the frequent, intensive and
interactive verification visits in themselves incentivise improved quality and performance. The
assumption is that by comparing IBF with RBF the impact of the financial incentive can be
measured. However, at a national level the budgetary implications of the verification process may
limit the replicability of the study at national programme level.
Additional factors which are built in as controls for the NU Health programme must be examined
when considering a possible national level intervention. A few examples include:
Impact of the timeliness of payments on the facilities’ investment decisions and service
provision – what is the minimum level of financial responsiveness required to incentive
improved performance?
Impact of predictable and appropriate drug credit line – what is the minimum standard for
drug supply management for a facility to function effectively, and how long after a
predictable drug supply has commenced, do health facilities begin to make longer term
investment decisions?
Impact of DHT level engagement – besides the supervision question, to what extent does
the coordination function of the DHT add to the facilities ability and willingness to improve

45
NU Health Lessons Learned II Report
performance, and to what extent does the DHT’s official role allow for time to support and
coordinate facility performance?
Control or oversight of inputs: It is worth noting that in the Acholi (RBF) group, NU Health did
not have either control over, or feedback about, the choice of inputs or investment options made
by the facilities, besides the credit line which was directly controlled by the programme. In the
Lango (IBF) group the programme had both veto control if expenditures did not align to previously
agreed criteria, and full access to the investment data. This limits the degree to which the
‘economy’ analysis can quantitatively reflect the difference in investment choices between the two
financing models.
Complexity of outcomes: As with any systems-wide health intervention, the complete picture of
outcomes and impact is highly complex. In order to fully map the cost-effectiveness of the
intervention, some core proxy indicators have been identified which can provide a highlight of the
impact the intervention is having. If a full mapping were to be attempted, the potential health impact
of every treatment made (across a range of medical departments), would be required. Even this
would only capture a partial impact assessment, as the systems approach also aims to embed
long term quality improvements, which means the outcome at the systems and infrastructure
levels would also need to be mapped (from the impact of health worker knowledge and practice,
to improvements in lab practices, increases to service provision through capital investment in
drugs & equipment). In summary, the long term positive impact of the intervention could be greater
than the immediate impact mapped at facility level.
Alignment between the quality controls and health outcomes: On a practical level the
verification process maps the ability of any facility to hit standard quality indicator targets for
service provision and to increase footfall. This relates directly to an increased resource envelop in
the RBF facilities. However, unless the indicators mapped at the verification stage are those which
will most effectively lead to the longer term health outcomes measured for VfM purposes, there
remains a risk that the benchmark for success shifts between implementation and analysis.
Timeframe: A basic but important note to stress throughout the subsequent analysis is that due
to the short programme timeframe, in most cases the programme has only two time related data
points, which severely limits the ability to determined trends effectively.
Data availability: HMIS data was extracted from the DHIS2 website for each facility in order to
obtain the number of cases for each of the six indicators included in the SUO formula which are
numbers of OPD patients, ANC visits, deliveries, family planning contacts, immunisation contact
and IPD patients. The NU Health team also requested the Annual Reports from each PNFP and
extracted the annual income and expenditure data that were analysed in the VfM section. The
quality of financial data from the RBF HF could not be wholly assessed as financial monitoring is
not directly carried out by NU Health and lower level units (LLUs) do not have a legal obligation to
be scrutinised by an external audit. Expressing the total health output of different levels of care in
a comparable way brings additional limitations.

46
NU Health Lessons Learned II Report
1. Economy
An economy analysis aims to analyse the degree to which inputs both demonstrate, and contribute
to, value for money. While the programme has access to the input decisions of the IBF facilities
through the financial accounts, the variety of inputs is so diverse that no core trends can be
identified. This stems in part from the freedom for each facility to determine whether it uses UKaid
funding to pay salaries, buy drugs and equipment, capital investment or for other allowable
expenses as defined by the contract with NU Health and the annual Business plan. For RBF
facilities the challenge is even greater as the ‘hands-off’ approach prevents the programme
knowing in what inputs the facility chose to invest in order to deliver improved health services.
There are, however, key ‘economy’ areas that the programme can directly analyse and use to
provide insights into potential policy recommendations. These include:
Credit line
DHT resources
Overall investment
1.2 Credit Line inputs
The chart below show the average Credit Line (CL) support from NU Health to PNFP per level of
care in the two regions over the two years of implementation (in GBP). The red lines show the
average CL ceilings per level of care of Acholi PNFPs and the green lines the CL of Lango’s.
While levels of support are similar in the LLU, the average CL support to RBF Hospital exceeds
the one for IBF hospitals due to the inclusion of PAG HC4 which required lower CL support than
a hospital. Variation overtime is also due to the exchange rate between the GBP and the UGX as
CL ceilings were labelled in UGX while this table reflect the actual value of the ceilings in GBP.
£0
£5,000
£10,000
£15,000
£20,000
£25,000
Y1Q1
Y1Q2
Y1Q3
Y1Q4
Y2Q1
Y2Q2
Y2Q3
Y2Q4
Average CL support to Hospital/HC4 PNFP
Per RBF Hospital*
Per IBF Hospital/HC4
£0
£200
£400
£600
£800
£1,000
£1,200
£1,400
£1,600
£1,800
£2,000
Y1 Q1Y1 Q2Y1 Q3Y1 Q4Y2 Q1Y2 Q2Y2 Q3Y2 Q4
Average CL support to LLU PNFP
Per RBFHC3Per RBFHC2Per IBFHC3Per IBFHC2
Figure 16 Credit line Support to PNPF per level of Care

47
NU Health Lessons Learned II Report
From a VfM perspective, the economy argument for the CL comes not from the cost per facility
model, but would rather sit at the procurement stage, as the cost per drug was fixed and in no way
affected by which facility it was going to. From a programme side, during the inception period NU
Health identified JMS as the most cost and context appropriate provider for its own credit line set-
up. Up to the end of December 2011, DANIDA had directed its contribution to PNFPs through
JMS. What the analysis does confirm is that both facility groups maintain a predictable drug supply
which responded to increases in service usage and contributed to the facilities ability to provide
quality care.
From a policy perspective, given the goal of increased access to services, there is an assumption
that not only would facilities require a consistent and predictable supply of drugs to function, but
that the cost of this would increase as service uptake improves. This requirement would likely
remain constant for both an IBF and an RBF model.
1.3 DHT inputs
Figure 17 below show the average financial support from NU Health to DHT for carrying out the
verification process in the two regions over the two years of implementation (in GBP). These
figures include the fees and allowances paid to the DHT personnel and fees-for-service provided
to the DHT after they have submitted the QQA report. These are maximum estimates based on
the agreed fees when reports are submitted in a timely manner.
Figure 17 Average financial support to DHT per level of care
The red lines show the average payment to Acholi DHT per level of care and the green lines the
same for Lango DHT. Variation between Year 1 and Year 2 trends is due to the correction of the
fee-for-service agreement with DHT in order to better reflect the costs really occurred by the DHT
to carry out the DQA/QQA.
£0
£50
£100
£150
£200
£250
£300
£350
£400
Y1 Q1Y1 Q2Y1 Q3Y1 Q4Y2 Q1Y2 Q2Y2 Q3Y2 Q4
Average financial support to DHTper level of care and per quarter
Per Hospital*
Per HC3
Per HC2
Per Hospital/HC4
Per HC3
Per HC2

48
NU Health Lessons Learned II Report
Again from a VfM perspective, this does not demonstrate a significant differential between RBF
and IBF as the financials were controlled by the model. However, linking this with the earlier DHT
feedback around conflicting priorities, large roles and limited district resources, it does help to
raise sustainability questions as to the extent to which resourcing similar activity would be
essential for any future intervention. It is not clear whether the DHT involvement could have been
maintained without this external financial support to operations.
1.4 RBF payments and IBF grants
Figure 18 below shows the average financial support from NU Health to PNFP per level of care in
the two regions over the two years of implementation (in GBP).
Figure 18 Average Financial Support to PNFP per level of care
The red lines show the average RBF payments per level of care and the green lines the average
IBF grants. Efforts were made to achieve facility patient load weighted parity. The average RBF
payments exceed the average IBF grants for all three levels of care during the two years of
implementation (except at Year 1 Quarter 2 at HC2 level). This is because IBF grants were
calculated prospectively at the beginning of each implementation year, based on the average
estimated performance results of the experiment group of Acholi PNFPs and according to the
available IBF budget.
The sudden increment of the green lines between Y1 Q4 and Y2 Q1 is due to the revised IBF
grant after the first year of implementation in order to better match the level of funding with the
RBF payments made to Acholi PNFP.
We see the gap in financing increasing as the RBF facilities begin to provide consistently higher
quality scores during verification than the anticipated average. In essence the analysis at the
economy level clarifies a skewing at effectiveness level. If the financial input rises proportionate
£0
£10,000
£20,000
£30,000
£40,000
£50,000
£60,000
£70,000
£80,000
£90,000
Y1 Q1 Y1 Q2 Y1 Q3 Y1 Q4 Y2 Q1 Y2 Q2 Y2 Q3 Y2 Q4
Average financial support to PNFPper level of care and per quarter
Per RBF Hospital*
Per RBF HC3
Per RBF HC2
Per IBF Hospital/HC4
Per IBF HC3
Per IBF HC2

49
NU Health Lessons Learned II Report
to quality, with the assumption that this relationship will be steady, there is no way for a facility to
demonstrate improved cost effectiveness – as the additional quality is undermined by the
additional input.
If the pilot were to be expanded elsewhere, there could be merit in determining the quality impact
of two different RBF scenarios compared to the IBF. In one, the financing would work as in NU
Health, increasing in line with quality, in the other, a deduction model could apply. This would help
to highlight the degree to which the financial value has the greatest impact on quality, compared
to ‘grant vs potential’ concept in which staff are incentivised by an improving quality score.
1.5 NU Health inputs as proportion of facility revenue
The final economy analysis looks at the degree to which the inputs from NU Health contribute to the facilities’ overall purchasing power. Table 12 NU Health Support as % of Total Income by facility below summarises the average
annual income per level of care against the average NU Health financial support, thus providing
an indication of the NU Health contribution to their annual activities. This gives us an indication
that while we look for trends in activity across the two study groups, the weight of the contribution
and therefore likely attribution, varies considerably.
The NU Health contribution to the HC3 budget is significant (70%) and modest for Hospital/HC4s
(around 20%). At HC2 there is a major difference between the NU health contribution in the two
groups, being significant in the RBF group (70%) and less so in the IBF ones (40%), the latter
charging higher user fees ensuring a better sustainability ratio as analysed later.
Table 12 NU Health Support as % of Total Income by facility
Av. annual
income
FY13-14 (UGX)
Av. RBF/IBF
grant
FY13-14 (UGX)
Av. % NU
Health
contribution to
income
Per RBF Hospital* 4,432,299,991 797,614,480 18.04%
Per RBF HC3 728,110,549 485,149,883 69.46%
Per RBF HC2 180,949,534 108,030,679 69.11%
Per IBF Hospital/HC4 3,028,387,342 590,316,007 22.16%
Per IBF HC3 398,226,247 279,712,421 71.54%
Per IBF HC2 137,634,921 55,525,525 42.17%
Overall, the key economy lessons learned relate to the necessary inputs required for a similar
intervention to succeed. These include:
An adequate, consistent and predictable drug supply;
A financial governance procedure to ensure costs are captured at facility level (whether or
not investment decisions are controlled);
Clarity around the roles, budget and priorities of the DHT;
Clarity around the level of freedom with which the facility may invest;

50
NU Health Lessons Learned II Report
Clarity around any ‘quality cap’ for highly successful facilities.
2. Efficiency
This section analyses how well these inputs are turned into outputs. Key areas for review in this
section include:
Relative cost to run the programme
Comparative investment across IBF / RBF groups
Identification of core cost drivers and recommendations
2.1 NU Health Milestone Payments
The table below summarises the overall support to facilities (including facility grants and credit line
costs) and compares them to the wider cost of running the study. As an implementation based
research piece, these include amounts paid each quarter by DFID to Health Partners International
(HPI)/Montrose for delivering pre-agreed milestones that covered a range of costs including DHT
mentoring and organisational support through business planning, development of capacity
strengthening plans, provision of secondees to support DHTs; data collection & management
through extensive DQA / QQA activities; actual management costs and overheads. The bottom
row shows the value of the milestones relative to direct support to the facilities.
Figure 19 Milestone value proportion of total budget
The initial ratios are higher due to the staggered approach implemented by NU Health at the
beginning of the programme. Considerable improvements in efficiency have been demonstrated
both by facilities achieving higher performance and operational savings allowing the study to
streamline as the model becomes more established.
Economy analysis of inputs Y1 Q1 Y1 Q2 Y1 Q3 Y1 Q4 Y2 Q1 Y2 Q2 Y2 Q3 Y2 Q4TOTAL
2 YEARS
Total inputs to PNFP (Grants and CL) £388,210 £456,127 £483,960 £562,773 £734,001 £857,576 £882,559 £956,514 £5,321,721
NUH costs (MS value) £357,015 £329,060 £292,138 £465,188 £354,920 £511,120 £265,013 £246,875 £2,821,329
Grand Total £745,225 £785,187 £776,098 £1,027,961 £1,088,921 £1,368,696 £1,147,572 £1,203,389 £8,143,050
Ratio MS / Grand total 48% 42% 38% 45% 33% 37% 23% 21% 35%
0%
10%
20%
30%
40%
50%
60%
Y1 Q1 Y1 Q2 Y1 Q3 Y1 Q4 Y2 Q1 Y2 Q2 Y2 Q3 Y2 Q4

51
NU Health Lessons Learned II Report
IBF vs RBF efficiency measures
While the full array of health outcomes cannot be captured for a programme as broad as NU
Health, the programme has been able to identify proxies by using the Standard Unit of Output
model identified by the UCMB. This monitors a wealth of indicators including OPD patient visits,
ANC visits, deliveries, family planning contacts, immunisation contact and IPD patient visits,
weighting each and coming up with an aggregate scoring (more of which is shown in Annex 2).
Analysis for FY13/14 demonstrates that by facility type, the RBF group provided a greater
proportion of the overall SUO score than the IBF group for higher level facilities with approximately
equal impact at the HC2 level. While it is impossible to draw full conclusions at this stage, we may
be seeing a situation in which the routine support, a predictable grant, drug credit line and DHT
inputs provide as much of a boost in lower facilities, as performance based incentives. It does,
however, also point to an inherent flaw in the model which includes many of the services which
HC2s do not perform.
Limitations & Recommendations
One core limitation for a balanced VfM assessment is that the incentivisation of performance in
RBF facilities masks the ability of the facility to demonstrate savings. If the model directly links
performance with increased input, and provides a specific payment per service, the efficiency of
the system will be inherently linked to the value placed on each service, and will not freely
demonstrate the efficiency or inefficiency of the facility.
For instance, if a facility is rewarded $x per ANC visit but only uses $(0.7x) to achieve it, the
assumption from an efficiency side is that the facility has still used $x for a single ANC visit. The

52
NU Health Lessons Learned II Report
saving is only demonstrated if the remaining $(0.3x) goes directly towards another ANC visit.
However, if the saving instead goes to something less tangible, such as a staff incentive,
construction etc, the change in output may not be seen for some time after the investment.
Therefore, without understanding the way in which the facility invests, and the impact of a RBF
model over a longer time period, it is not possible to accurately determine comparative efficiencies
across IBF and RBF. Investments directly into ‘score-able’ areas will naturally be regarded as
more ‘efficient’ than longer term investments in the system. This is particularly important when
looking at the external learning from the programme, as with all health investments, the apparent
efficiency of each model could vary considerably over time. This is particularly compounded when
the NU Health grant forms a varying proportion of the overall facility revenue.
From a policy perspective, another key VfM learning is that operational savings are feasible as
both the RBF and IBF models become more established. However, in planning discussions the
operational budget would need to remain a key component. Further savings could be sourced by
reducing the robustness (frequency / on site time etc) of the verification exercises, however,
ultimately a balance would need to be struck to ensure appropriate quality and cost.
3. Effectiveness & Cost Effectiveness
This section aims to analyse whether the ‘right outputs’ have been invested in to achieve the
intended outcomes. Following the discussion above around the feasibility of mapping efficiency
without a full picture of inputs and outputs, a similar issue arises at the effectiveness level. The
effect is more pronounced as for efficiency there are at least consistent data elements coming
from the DQA/QQA, even if the input picture is less clear of RBF. At the output-to-outcome
transition, limitations stem from the lack of a full mapping of potential outcomes with associated
timeframe.
As clinical outcome data are not available, analysis consists of the cost per quality-adjusted SUO
to give an impression of relative cost effectiveness in RBF versus IBF facilities, across the different
levels of the system. As discussed above, with only two data points this presents only a tentative
finding, however, if the trend were to continue, one would expect to see improving effectiveness
and perhaps cost effectiveness.
Figure 20 provides a snapshot of the relative quality adjusted cost ratio per SUO for the two groups
by facility type. This figure shows a dramatic shift in the relationship between RBF and IBF cost
effectiveness, when the differential improvement in quality, as measured by the QQA is taken into
account. While the IBF appeared far more cost effective in year one for lower level facilities and
reasonably more cost effective for hospitals, RBF appeared to be the more cost effective model
for HC3s. A year further along, we can see a dramatic improvement in relative cost effectiveness
for RBF HC2s and a moderate adjustment for hospitals. At the end of the first full year of
implementation, the grant formula was shifted to help address weaker performing areas.
“The increases proposed would still represent a subsidy towards the total cost of service delivery,
but would allow facilities greater flexibility for innovation. The indicators proposed for increase
included: i) 1st ANC visit, ii) LLIN distribution iii) Caesarean Sections iv) Measles vaccination, and,

53
NU Health Lessons Learned II Report
v) Vitamin A supplementation. Meeting participants suggested that the increments be spread out
across a broader selection of indicators, and nominated areas where they felt greater
incentivisation was needed most. The NU Health team agreed to look into the suggestions raised
when revising subsidy levels for implementation Year 2.”7
It is possible that by amending the performance contract formula, the incentivisation overtook the
facilities’ capacity to invest which would explain why HC3 facilities appeared to move from a RBF
to IBF as the most cost effective model. A third data point would provide an interesting comparator
to examine the extent to which facilities ‘settled’ into the new grant formula and were able to once
again reinvest more effectively in the RBF group.
Figure 20 Quality adjusted RBF v IBF Cost Ratio per SUO by Facility Type
4. Equity & User Fees
This section describes the shifts seen in the socioeconomic profile of beneficiaries through a
description on user fee policy. Despite the recognition that user fees can prove a barrier to access
for the poor, they often end up providing a significant level of necessary health facility revenue.
Although this has a regressive implication with the poor paying proportionally more than the better-
off, the revenue associated with user fees provides a level of health service sustainability which is
analysed below.
Table 13 summarises user fees per SUO per facility type in FY13-14 and FY12-13.
7 NU Health Quarterly Progress Report Jul-Sept 2013.
-
0.50
1.00
1.50
2.00
2.50
3.00
FY12-13 FY13-14
HospitalRatio
HC3 Ratio
HC2 Ratio

54
NU Health Lessons Learned II Report
Table 13 User Fees by Facility Type
Av SUOAv User fees
collected
Av user fees
per SUOAv SUO
Av User fees
collected
Av user fees
per SUO
Per Hospital* 214,465 550,820,851 2,568 Per Hosp./ HC4 164,484 569,122,605 3,460
Per HC3 39,451 42,225,283 1,070 Per HC3 17,479 65,464,242 3,745
Per HC2 7,272 8,594,679 1,182 Per HC2 8,866 60,797,800 6,858
Acholi PNFP - FY13-14 Lango PNFP - FY13-14
Av SUOAv User fees
collected
Av user fees
per SUOAv SUO
Av User fees
collected
Av user fees
per SUO
Per Hospital* 225,455 449,282,513 1,993 Per Hosp./ HC4 144,051 673,524,425 4,676
Per HC3 56,412 39,743,967 705 Per HC3 16,875 61,248,262 3,630
Per HC2 4,201 12,379,791 2,947 Per HC2 9,043 37,620,775 4,160
Acholi PNFP - FY12-13 Lango PNFP - FY12-13
The Acholi Hospitals and HC3 collected more user fees this year, despite lowering their output
while HC2 have decreased their collection of user fees while increasing their output. This
translates into a higher average user fee per output at Hospital and HC3 level compared to the
previous year while being divided by three at HC2 level. This could be explained by the increased
incentive provided by NU Health to that level of care which allowed them to reduce their use fees
to attract more patients and thus boost their output.
In Lango the opposite has been observed, with HC2 almost doubling their collected amount of
fees while slightly reducing their output, but Hospital/HC4 collecting fewer fees while increasing
their output. HC3 figures remained stable over the two FY. This translates into an increment of
average fees at HC2 level and a decrease at Hospital level.
When comparing the two regions, Lango PNFP charge their patients more than the Acholi ones,
with 5 times more at HC2 level and 3 times more at HC3 level, which reflects the same difference
as that noticed last year.
While this analysis is useful, the implications for broader policy or operational learning would be
strengthened by additional review of the following areas:
Key drivers for access (do people seek the facility nearest them first and then progress
through the facility levels or self-refer to the facility level providing the care they need?
Duplicability of user fees – if an individual is referred, must they always pay a second round
of user fees?
Drivers behind user fees – to what degree are user fees set by the owner or diocese vs
the in-charge? How does this link to planned income generation and budget mapping?
What is the socio-economic spread of patients for each level of care, and from this would
an equitable user fee policy look at having a flattened spread of costs to prevent anyone
from being unable to access the suitable level of care based on cost comparative to a lower
level facility? Or would it rather look to have a lower user fee rate at the lower level of
facility on the grounds that not only would this be more likely to be accessed by lower

55
NU Health Lessons Learned II Report
socio-economic groups, but that an individual household would likely require more lower
level services than higher ones in a given time period?
While many of these questions are market driven, there is a broader equity question behind the
user fee analysis.
5. Sustainability & User Fees
The sustainability ratio of PNFP shows the portion of annual income that is covered by the collection of user fees. Table 14 summarises user fees as a proportion of the facilities’ income across facility types in
FY13-14 and FY 12-13.
Table 14 User Fees and Facility Income
Av IncomeAv User fees
collected
Av % user
fees vs
income
Av IncomeAv User fees
collected
Av % user
fees vs
income
Per Hospital* 4,432,299,991 550,820,851 12.43% Per Hosp./ HC4 3,028,387,342 569,122,605 18.79%
Per HC3 728,110,549 42,225,283 5.80% Per HC3 398,226,247 65,464,242 16.44%
Per HC2 180,949,534 8,594,679 4.75% Per HC2 137,634,921 60,797,800 44.17%
Acholi PNFP - FY13-14 Lango PNFP - FY13-14
Av IncomeAv User fees
collected
Av % user fees
vs incomeAv Income
Av User fees
collected
Av % user fees
vs income
Per Hospital* 3,738,416,177 449,282,513 12.02% Per Hosp./ HC4 2,001,454,620 673,524,425 33.65%
Per HC3 390,014,987 39,743,967 10.19% Per HC3 175,978,784 61,248,262 34.80%
Per HC2 82,839,952 12,379,791 14.94% Per HC2 66,947,232 37,620,775 56.19%
Acholi PNFP - FY12-13 Lango PNFP - FY12-13
On average, Lango/IBF HF are collecting more user fees per annum compared to those in Acholi.
When comparing these amounts with the average income per level of care, it shows higher
sustainability ratios in the Lango/IBF region compared to the Acholi one (all three percentages are
higher in Lango), and more so at LLU level.
The average incomes (which include the NU Health contribution) in both regions and at all three
levels of care increased from last year. When comparing these figures, it appears that on average
Acholi facilities collected more user fees this year than last year, though these constitute a smaller
proportion of overall budget. In Lango, by contrast, Hospitals/HC4 collected fewer fees and HC2
more fees, but that these represented a significant decline in their contribution to the overall
budget.

56
NU Health Lessons Learned II Report
9 OPERATION / MANAGEMENT PROCESSES
This section describes the key operations and management processes that were established during the programme and the core lessons learned. Figure 21 illustrates the seven stages of the RBF programme process.
Figure 21 RBF Programme Process
1. Facility Selection
As the PNFPs in Northern Uganda were at different levels of functionality and preparedness to
engage in RBF, they were assessed by NU Health during the inception phase, using the five
following criteria:
1. Staffing norms;
2. Functioning equipment as required per level of care;
3. Functioning infrastructure;
4. Registered with UCMB, UPMB or have other legal status8;
5. Provide most of the preventive and curative maternal and/or child health services as
specified in the Health Sector Strategic and Investment Plan as appropriate for the
level of care.
Based on the above, the PNFP were classified by NU Health in three categories:
Category 1 when all five criteria were in place
Category 2 when two of the criteria were missing
Category 3 when more than 2 criteria were missing
In Acholi sub-region, 9 PNFP were in Category 1 and 12 in Category 2, while in Lango sub-region
there were 5 PNPF in Category 1 and 5 in Category 2. Facilities falling under Category 3 were
excluded from the RBF and IBF scheme as they were deemed too weak for consideration.
Following this selection, RBF implementation was phased with Category 1 HF joining immediately
into the RBF scheme without delay and without a seed grant; and Category 2 HF joining during
the second quarter after receiving a seed grant (explained below). This was to enable the PNFPs
in less-prepared classifications to enhance their level of service and capacity to set thresholds
which allowed them to participate on an equal footing with better-prepared health facilities.
2. Development of business plans by the PNFPs
8 Licensed with the Medical and Dental Practitioners Council and with the Medical Bureau or under the NGO status,
and recommended by the DHT.
Facility Selection
Capacity Building
Business Plan
Seed grantsMOU
Cycles &
Batches
Scale up
app-roach

57
NU Health Lessons Learned II Report
Business plans formed the basis on which health facilities were able to plan improvements in
service delivery/quality which would be funded by the RBF or IBF funds. The business plans state
targets for improvements in quality and the resulting expected volume of services, as well as the
investments needed to attain these. Thus, unlike action plans, the business plan reflects realistic
goals which have financial implications for the health facility and the programme.
The business plan is an essential element of the RBF process as it outlines how the facility plans
to respond to the financial incentives provided, how it plans to achieve improvements in both levels
of service provision and quality of services, and hence meet its targets and receive funding.
A lesson learned from the business plan (BP) process is that most HF, especially LLU, had no
idea of the concept of a BP and were unable to prepare one prior to the programme. Therefore,
NU Health organised several training sessions aimed at explaining to all the PNFP and DHT the
BP concept, use, modalities, etc. as well the overall RBF concept.
Whilst NU Health was facilitating and supporting the BP process, the PNFP had autonomy over
what it did or did not include in the business plan and complete freedom for innovation to ensure
they met their objectives. As a result the PNFP subsequently bears the risk for non-performance
against targets.
The facilities were then able to prepare their business plans detailing scope and volume of
services which were shared with the DHT.
The business plan included the following information:
For the initial entry into the RBF scheme, facilities had to outline their plans for the Seed
Grant, which is an initial investment to prepare the health facility adequately for the
introduction of RBF. This grant was based on a case by case negotiation with NU Health,
and was available for activities or inputs related to improving quality of services and/or
implementation/management of an RBF scheme. This did not cover additional staffing.
Thereafter, NU Health negotiated with each facility to agree a set of services and quality
and quantity indicators (in line with the list of services and indicators included above)
against which their performance will be monitored. The following outlines the structure of
the business plan per service:
Selected services denote those services which each facility will include in line with
their core values and key competencies
Operations targets aimed at compliance with national minimum norms covering for
example human resources, infrastructure, essential medicines, medical equipment,
office equipment
Facilities were asked to outline for each service selected
Monthly targets
Issues arising with achieving targets
Strategies/steps to solve these issues to allow for achievement of targets

58
NU Health Lessons Learned II Report
Finally, facilities were asked to plan revenues and expenses against current revenues and
expenses.
It is also worth noting here that while the initial plan had been to use the BP as a monitoring tool
for the PNPF usage of RBF funding, the revised hands-off approach applied by DFID on the
programme, rendered the BP somewhat irrelevant as a monitoring tool. On the other hand, in the
Lango sub-region, the annual BP has been a useful tool as it formed the basis for the quarterly
business plan and budget reviews which were approved and closely monitored by NU Health.
3. Capacity Building
Based on the above, the first training/capacity building focus was on Business Planning for both
the PNFP and the DHT.
This was followed by Financial Management training in the IBF/Lango region as IBF grants were
to be managed and monitored by NU Health. The existing financial guidelines from the Diocese
of Lira were used to roll out to all the Lango PNFP. Additional procurement guidelines were added
by NU Health to complement these existing procedures.
With NU Health providing medical supplies to all PNFPs, training on drug supply management
was also organised by NU Health twice over the lifespan of the programme. Following a baseline
survey assessing the gaps and weaknesses in drug management, training sessions tailored to
tackle the most pressing gaps were organised by NU Health.
Finally, as a new tool had been introduced by NU Health, the Quality of Care checklist, the tool
had been explained to PNFP and DHT in each District with theoretical and practical training
sessions.
4. Seed grants provided to Category 2 HF
As mentioned above, the PNFPs were in variable states of readiness to undertake the RBF
initiative. There were gaps in infrastructure, equipment, supplies, and human resources which
required attention before PNFPs could provide the services identified in the RBF programme as
triggers for payment. Seed grants were therefore provided by NU Health prior to engaging in the
RBF programme in order to enable them to participate effectively.
The initial assessment indicated that the capital needed to support equipment needs was relatively
small. Seed grant for equipment was used to procure equipment items such as instrument drums,
delivery sets, delivery beds, adult weighing scales, examination couches, drip stands, centrifuges,
autoclaves and dressing kits. These seed grant equipment items were sourced directly from JMS.
The human resource gaps were more substantial. A critical assumption was that with an enhanced
salary package (from the overall increased funding through the RBF/IBF mechanism), the facilities
would be able to attract the required staff mix during the first six to 12 months of implementation.
In reality PNFPs were not willing to change their human resource policies because the NU Health
support was limited in time. PNFP therefore consistently struggled to retain staff and often lost

59
NU Health Lessons Learned II Report
staff to GoU recruitment campaigns to staff the public facilities. This was broadly seen to be a
reflection of the fact that in private facilities, staff have to do more work for less pay, while
performance is much laxer in public facilities and so it is seen to be a more attractive role for many.
5. MoU signed with each HF and DHT
Once the business plans had been endorsed by NU Health, the RBF modalities were sealed into
legal agreements with each PNPF. As PNFPs belonging to a Diocese had no legal status in their
own right as entities capable of entering into a legally binding contract (while the Diocese had),
legal agreements were therefore signed between NU Health, the Dioceses (as legal owners) and
the PNFP; the Dioceses taking legal responsibility for the participation of the PNFPs in the RBF
scheme.
It is worth noting here that the Medical Bureaus were not involved in the RBF scheme and thus
not in the legal agreements signed with PNFP, despite their technical role in the health sector
supporting the Dioceses. It is also worth noting that the Diocesan Health Coordinator Office was
not supported by NU Health –technically or financially - despite their legal responsibility as
representative of the legal owner of the HF.
6. Planning the verification in cycles and batches
The following processes are being followed in the RBF verification process:
On a routine basis, the PNFP records data on levels of service provision;
On a quarterly basis, data is being verified by the DHT with NU Health’s support;
DHT and NU Health also assess the quality of the health care services being provided by
the PNFP, using the Quality of care checklist;
NU Health then calculates performance-based payments due to PNFP;
PNPF prepares an invoice;
Invoices are crosschecked by NU Health and passed to HPI for payment;
HPI to match invoice with purchase order (PO) to check the amount is within agreed
maximum quarterly incentive payment per PNFP, however overall responsibility for
correctness of incentive invoice rests with NU Health;
The raising of a PO per PNFP allow HPI to monitor independently the actual funds
disbursement per PNFP versus target;
Funds are transferred by HPI directly to PNFPs;
PNPF raise a receipt.
The fund flows process for both RBF and the credit line are summarised in the following diagram.

60
NU Health Lessons Learned II Report
Due to the above process based on quarterly verification, the supported PNPF HF in Acholi were
shared into three equivalent batches with each batch composed of one hospital, one HC3 and 5
HC2. In Lango, due to a different level of care composition, two batches had one Hospital or one
HC4, one HC3 and one HC2 while the third batch had four HC3. The aim was to spread as much
as possible the workload evenly across each month of verification.
As illustrated in Table 15, due to the above, one RBF quarter, broken into three cycles would then
spill over a five-month period as follows: Cycle 1 starting 1st September while the last cycle of that
quarter, Cycle 3, ending on 31st January, with the verification process (highlighted in red below)
being organised at the end of the three-month cycle.
Table 15 NU Health Planning Cycle
NU Health - CYCLE PLANNING
Quarter 1 Quarter 2 Quarter 3
Batch Sept Oct Nov Dec Jan Feb Mar Apr May
A Cycle 1 DQA/QQA DQA/QQA
Figure 24 NU Health Fund Flow Diagram

61
NU Health Lessons Learned II Report
B Cycle 2 DQA/QQA DQA/QQA
C Cycle 3 DQA/QQA DQA/QQA
With the extension of the contract, NU Health support will continue to the facilities through the end
of June 2015. The final round of DQA/QQA will be completed in two rather than three months.
10 RISK, PARTICULARLY FIDUCIARY RISKS, AND ITS MITIGATION
This section examines the potential risks related to the different components of the programme:
the implementation of the RBF scheme, the IBF component, the Credit Line, and support to the
DHT. Given the “hands off” policy, where no advice was provided on the allocation of funds and
there was no monitoring on the use of the funds in the RBF region, particular emphasis is placed
on fiduciary risks. This section also examines the potential consequences of these risks and
mitigation measures taken by NU Health.
1. Fiduciary risk
Fiduciary risk is the risk that funds are not used for the intended purposes; do not achieve value
for money; and/or are not properly accounted for. Fiduciary risk arises due to a variety of factors,
including lack of capacity, competency or knowledge; bureaucratic inefficiency; and/or active
malfeasance and corruption.
By design, the RBF’s hands-off approach on fund management use entails risk. By design, DFID
and NU Health accepted this risk to ensure the methodological integrity of the study.
Nevertheless, the programme has criteria and standards related to how facilities adhere to their
own standard operating procedures, and there was one case brought to NU Health and DFID over
the potential mismanagement of RBF funding in one HC2. Additional financial monitoring carried
out subsequently by NU Health and the Diocesan Health Office indicated that there was poor
adherence to financial guidelines in that HF. Per its agreement, the facility was provided with an
opportunity to make corrections and was subsequently suspended from the programme when it
failed to make these corrections.
In the IBF group, by contrast, the fiduciary risk was mitigated by a range of actions. Basic
expenditure plans were based on NU Health approved business plans. Procurement and
payments, including accounting for project funds were closely monitored on a routine basis. IBF
facilities were audited by an external firm selected by NU Health. NU Health also received
management responses from each facility on issues from these audits.
2. Corruption
The likelihood and magnitude of corruption occurring, as opposed to the other factors (lack of
capacity, inefficiency, etc.) is a key aspect of fiduciary risk. Defined by Transparency International

62
NU Health Lessons Learned II Report
as ‘the abuse of entrusted power for private gain,’ corruption is a problem in Uganda, as reflected
in the UK government’s suspension of direct funding in 2012. Building on the RBF segregation of
authority model, risk is mitigated by ensuring a high level of transparency among the DHT, the
PNFP and NU Health in the verification process with three parties jointly verifying the PNFP
performance which triggered RBF payment.
3. Displacement of existing funding
NU Health’s inception came at the time when humanitarian financing for health was tailing off,
according to many participating facilities. With NU Health funding flowing to PNFPs, there was a
risk that GoU and Districts might use NU Health support as an opportunity to displace some of the
Primary Health Care grants allocated to PNFP by the GoU. While tracking these fund flows was
beyond the scope of NU Health, no report of fund interruption was received, although there were
reports of delays.
4. Data reliability and gaming
Reported service delivery figures were generally higher than the verified figures because of poor
adherence to data collection and reporting procedures. As performance payment came on line,
there was also some tendency to inflate the performance. For the purpose of the study, primary
data were employed rather than those reported in the HMIS. Data triangulation was carried out
by the DHT and NU Health in order to obtain the verified numbers. Primary data was then
compared in order to assess the discrepancy rate. In addition, data quality assessment was
incorporated within the QQA tool.
5. DHT capacity
As the regulator/verifier of the RBF intervention arm as well as the IBF comparison arm, the DHT
plays a crucial role in the study. In Northern Uganda, however, the range of demands by externally
supported programmes and projects outstrips the capacity of the DHTs to deliver. Often the DHTs
were stretched thin to perform the results verification with consistent teams having the right skill
set.
Mitigation measures taken by NU Health included training all DHT personnel on the DQA and
QQA tools so that all of them were able to verify the data quantity and to a certain extent the
quality of health care services being provided. A second measure was to also train the District
Sub-District personnel (public health workers from HC4) on the tools so that they also could be
included when needed.
6. Management of medical supplies
The risks related to the Credit Line of EMHS can be divided into two main types:
1) Risks at the drug supplier level—JMS:
Changing prices of EMHS: there is a risk of EMHS prices rising beyond the agreed upon
price maximum in the MOU. This may lead to budget increase for EMHS.

63
NU Health Lessons Learned II Report
There is a risk of JMS not being able to stock enough EMHS in terms of quantity, quality
and variety. This may eventually lead to very low order fill rates for the facilities and poor
quality drugs may be delivered to facilities
There is a potential risk in the delay in distribution of EMHS due to inadequate quantity of
EMHS available to transport at JMS, transport break down due to mechanical failure of the
trucks.
There is a risk of loss due to theft of some or all the EMHS being transported by the third
party transporters. Though it is a risk of JMS it eventually affects the PNFPs too.
The probability of the JMS risks occurring is minimal as JMS has a sound supply chain
management system in place that minimizes the occurrence of these risks. The impact of
these risks would be organisational and financial as other sources of supply would have to be
sourced which might have a financial implication.
The mitigation actions put in place by NU Health were to:
Signing a detailed MoU with JMS that clearly stipulates the roles and responsibilities
between NU Health and JMS.
There are procedures in place at NU Health to check the actions of JMS during execution
of the EMHS process with a routine back and forth communication between JMS, NU
Health and the PNFP about the purchase orders, the unavailability of some items at JMS,
suggested replacements, progress in the delivery rate, etc.
2) Risks at PNFP level:
Risk of theft of EMHS by the staff
responsible.
There is potential risk of a facility not
practicing good pharmaceutical
management practices hence leading to
loss due to expiries of medicines or
damage of EMHS due to poor storage
practices.
There is a risk of a facility not honouring
the terms of its NU Health MOU leading
to its suspension from the study.
The probability of loss occurring at facility level is
lower in higher level facilities due to their more
robust supply management procedures in place.
That probability is higher (medium) but
consequences lower in LLU that lack trained
staff, have weak supervision and poor
infrastructure. The impact of these risks might be
serious for beneficiary health services.
Despite the “hands off” policy, DHT and NU
Health keep their “ear to the ground.” Over the
course of the last three years, the programme
has received two notifications of potential
financial impropriety. With the first of these,
NU Health conducted an assessment, and
reported back to the Facility Management
Committee on matters that were inconsistent
with their NU Health agreement. Per
agreement, the facility was provided an agreed
period to implement the agreed changes in
management and control procedures. The
agreed changes were not made, and the
facility was excluded from the programme.
In the second instance, the programme
received an anonymous report of procurement
impropriety. In this case, there were apparent
weaknesses in adherence to procurement
procedure, but with no apparent malfeasance.
After further review by DFID, NU Health was
instructed not to certify the payment requested.
Figure 22 Risks & Consequences

64
NU Health Lessons Learned II Report
The mitigation actions put in place by NU Health were to:
Train facility staff in good pharmaceutical management;
Conduct routine supportive supervision and EMHS audits at facilities;
Incentivise good pharmaceutical practises by adding two pharmaceutical management
indicators added to the QQA tool; and,
Use “the stick” in case of mismanagement of EMHS with the possibility of suspension of
credit line support.
11 CONCLUSIONS: GOOD AND BAD PRACTICES IN RBF
Background
This final section of the Lesson Learned paper will serve as its conclusion. Building on and
synthesizing points made in other sections of this report, evidence, insight and impression are
brought together to summarise NU Health’s observation on what has happened in health facilities
in the provision of services and the implications of those observations on policy and programming.
Management Process
With NU Health’s “Hands Off” policy the responsibility of the programme focused on ensuring
requisite inputs were in place, the appropriate reporting was undertaken, and, in the case of the
IBF control facilities, that procurement was carried out in accordance with facility plans and facility
procedures. While facilities were provided support for business planning at the beginning of the
programme, there was neither technical assistance nor supportive supervision to assist them in
using their plans in routine operations.
NU Health had a mandate not to guide the development or use of facility plans. Informally,
however, it received reports on heterogeneity on both how plans were developed and how they
were used. Some facilities actively overcame the management-clinical divide and achieved
success in increasing ownership of staff involved in clinical care as well as management and
administration. In these facilities, it seemed that there was a higher level of transparency in
communication with both organisational performance and incentive payments. Though it was
beyond the scope of this study, it would be interesting to better characterise the determinants of
more participatory and transparent planning and management.
Clinical Care
In interpreting what happened in terms of clinical care in facilities enrolled in the NU Health Study
it is important to note that although the study was designed around isolating the effect of funding
modality on provider behaviour, there are many other considerations that affect provider behaviour
outside the scope of the study. It is also interesting that anecdotally, at least, the health sectors
in Acholi and Lira are said to have different cultures born out of their differential experiences during
the conflict.
As noted in the Quality of Care and Health Outcomes sections of this report, data generated by
the programme provide possible preliminary insight into how financing modality affected clinical

65
NU Health Lessons Learned II Report
care. Overall, facilities in the RBF arm of the study provided higher quality of care as measured
by adherence to treatment guidelines and maintenance of tracer medicine stocks.
Reporting
Discrepancy Rates in data
The discrepancy rates in the NU Health study refer to the discrepancy between service data reported in the HMIS and those verified by NU Health. As summarised in
Figure 26, while a general tendency toward under-reporting is noted, there is a trend toward lower
discrepancy rates over the life of the study overall and, not surprisingly, in the RBF facilities in
particular.
Figure 26 Discrepancy Rates
Discrepancy rate (DR) = (number of verified cases – number of reported cases by the PNFP) / number of reported
cases. A DR within a +-5% margin is considered acceptable and therefore incentivised in the RBF scheme in the quality
assessment tool.
Despite the absence of baseline data on reporting discrepancy, the pattern observed over the life
of the project is noticeably different in RBF versus IBF facilities. It no surprise that the discrepancy
rates are better in the RBF facilities, by virtue of their role in defining performance payment. No
doubt the intensity of QQA also reinforced the importance of good data management. Even with
the relatively more reliable HMIS of the RBF facilities, these data do underscore the need to
strengthen HMIS to strengthen service delivery and accountability, by enabling better targeting of
scarce resources to under-served or under-performing areas and facilities.
Completeness and Timeliness of data entry
In addition to managing accurate data, HMIS function is improved with complete and timely
information. While this exercise had some implications for the programme, it serves more as a
diagnostic on the state of HMIS in Uganda, or at least Northern Uganda in general.

66
NU Health Lessons Learned II Report
Table 17: Average Completeness and Timeliness of Reporting rate of supported PNFP per
Level of Care during FY 13-14
Level of care Sub-
region
Actual
Reports
received
per year
Expected
Reports
per year
Completeness
Ratio
Reports
On
Time
per
year
Timeliness
Ratio
AVG PER
HOSPITAL*/HC4
ACHOLI 132.5 183 72% 89.5 49%
LANGO 152 182.5 83% 124 68%
AVG PER HC3 ACHOLI 153 235 65% 126 54%
LANGO 140 182 77% 116 64%
AVG PER HC2 ACHOLI 90 123 73% 71 58%
LANGO 119 146 82% 94 64%
AVG PER PNFP
(all level)
ACHOLI 104 147 71% 82 56%
LANGO 138 175 79% 113 65%
* excluding Lacor Hospital
In both intervention and comparison areas, performance was relatively low. It is interesting to
note that the Lango intervention area generally had more complete and timely submission.
Nevertheless, the larger point relates to how well HMIS can support effective and efficient delivery
of sectoral oversight and health services without good enough or timely enough information as
this is an essential factor in deciding on appropriate allocation of resources to those areas most
in need.
Financial Management
Financial management, including the mitigation of fiduciary risk, is vital to any project or
programme. When it is the substantive focus of the intervention, in this case the assessment of a
service financing mechanism, it becomes the central focus of interest.
When NU Health was realigned to provide a stronger basis of evidence, the project was advised
to adopt a “hands off” approach with relation to how RBF funds might be used. IBF facilities, which
received grants matching the value of similar situated RBF facilities, had facility specific plans and
specific procurement and documentation requirements guiding the use of NU Health funds. The
RBF facilities received payment on the basis of their verified results without investment
qualification from NU Health. It was stipulated that performance payments be used in a manner
consistent with any non-NU Health existing governance arrangements.
To this end, there were a range of ways facilities opted to utilise their funds. Although NU Health
did not track it, we have some impressions about investment tendencies. In general, in the larger
facilities, finance from NU Health was pooled with other facility operating funds. Funds also seem
to have flowed towards investment rather than consumption in many of these larger institutions.

67
NU Health Lessons Learned II Report
In general lower level facilities are using NU Health finance to fund operating expenses and
allowances rather than choosing broader investment options. It was also noticed that IBF facilities
in general invested more in infrastructure and equipment than the RBF facilities.
That said, there were some RBF facilities who opted to save some of their results payments. A
number of HC2s such as New Life, St Monica and Wi Anaka adopted saving strategies in part for
concern about what happens after the end of NU Health.
Conclusion
Over the last three years, NU Health has developed into a quasi-experimental study focused on
isolating, to the extent possible, the different practices, management methods and cost-
effectiveness of RBF with non-state PNFPs vis-à-vis a conventional IBF model. Some significant
lessons can be drawn from this experiment as can be seen through the two Lessons Learned
documents prepared.
It is expected that with its formal evaluation, NU Health will contribute important evidence to inform
policy and programming in Uganda and beyond. In terms of effectiveness, preliminary data
suggest that RBF can lead to better quality of care along with improvements in a number of the
critical pathways that result in accessible quality care regardless of gender or socio-economic
status. The programme is also working with cost data to develop preliminary models of the extent
to which a similar intervention design, with the research elements and some data management
functions stripped out, could serve as an appropriate financing model for public facilities in
Uganda.

68
NU Health Lessons Learned II Report
REFERENCES
CORDAID & SINA (2010) PBF in Action Theory and Instruments Course Guide
COUNTDOWN TO 2015 (2014) Fulfilling the Health Agenda for Women and Children: The 2014
Report
DONDORP AL, FANELLO CI, HENDRIKSEN ICE, GOMES E, SENI A, CHHAGANLAL KD, et al.
(2010) “Artesunate versus quinine in the treatment of severe falciparum malaria in African children
(AQUAMAT): an open-label, randomised trial”. The Lancet 376(9753): 1647-1657
ELDRIDGE, C & PALMER, N (2009) Performance-based payment: some reflections on the
discourse, evidence and unanswered questions. Health Policy and Planning 24(3): 160-166
ICAI (2011) ICAI’s report on Approach to effectiveness and Value for Money
LAWN JE & KERBER K (Eds) (2006) Opportunities for Africa’s Newborn. Practical data, policy
and support for newborn care in Africa, Cape Town, PMNCH, Save the Children, UNFPA,
UNICEF, USAID, WHO
MINISTRY OF HEALTH UGANDA & MACRO INTERNATIONAL INC. (2007) Uganda Service
Provision Assessment Survey 2008
MINISTRY OF HEALTH UGANDA (2010) Uganda Clinical Guidelines: National Guidelines on
Management of Common Conditions
NAO (Date unknown) Analytical Framework for assessing Value for Money -
http://www.bond.org.uk/data/files/National_Audit_Office__Analytical_framework_for_assessing_
Value_for_Money.pdf
TAYADE S & JADHAO P (2012) The Impact of Use of Modified WHO Partograph on Maternal and
Perinatal Outcome International Journal of Biomedical and Advance Research 256
UNICEF (2014) http://data.unicef.org/child-mortality/neonatal

ANNEXES
ANNEX 1: INDICATORS ASSESSED AND THE ASSOCIATED CALCULATIONS FOR PAYMENTS - YEAR 2

70
NU Health Lessons Learned II Report

71
NU Health Lesson Learned II Report
ANNEX 2: STANDARD UNIT OF OUTPUT (SUO) FORMULA USED BY UCMB
As the range of health care services provided by the PNFP is very broad and varies substantially
across the different levels of health care, from HC2 to hospital, it was suggested by NU Health
that the total health output of facilities be limited to a certain number of indicators, for which cases
will be collected from DHIS2 for each PNFP.
To make the data meaningful, it is presented under the form of Standard Unit of Outputs (SUO)
which is a method used by the UCMB (Uganda Catholic Medical Bureau)9 , by hospitals in their
annual reports and by Cordaid to reflect the health output of facilitates supported by its
Performance Based Financing scheme in Jinja and Kamuli Districts.
As described in the UCMB documents, this method is a composite index calculated with a
combination of the six following parameters which are then converted and expressed into their
outpatient equivalents to determine the health output of a HF:
In-patients episodes (IP);
Out-patient contacts (OP);
Deliveries carried out (DEL);
Immunisation doses administered (IMM);
Antenatal contact (ANC); and
Family Planning contacts (FP).
The composite indicator of activity, called Standard Unit of Output (SUO), is calculated by
attributing to each output a relative weight according to the level of care. The weighting attributed
to each of the 6 parameters, based on relevant literature described in the UCMB report, is
equivalent in terms of costs for managing one outpatient, when you manage for example one
inpatient from admission to discharge. Because the costs for managing patients vary with the
level of care, two different weighting scales have been designed by UCMB to reflect this
difference, as shown in the table below:
Equivalent weighting of each
parameter of the SUO formula
Hospital
and HC4
LLU (HC2
and HC3)
IP *15 *5
DEL *5 *2
OP *1 *1
9 PUBLIC PRIVATE PARTNERSHIP IN HEALTH. WHAT IS ITS EFFECT ON THE PERFORMANCE OF THE HEALTH SECTOR? Daniele Giusti, MD DTM&H MPH, Peter Lochoro, MB ChB MHSM, Andrea Mandelli, BA Economics http://www.ucmb.co.ug/data%20on%20ucmb/Reports/ARTICLES/Article%20Effect%20of%20PPP%20on%20Health%20System.pdf

72
NU Health Lesson Learned II Report
ANC *0.5 *0.3
IMM *0.2 *0.2
FP *0.2 *0.2
In other words, SUO provides a general idea of the volume of the main services produced by a
health unit by using the following two formulas:
- SUO for a hospital and HC4 = [15*IP+5*DEL+1*OP+0.5*ANC+0.2*IMM+0.2*FP]
- SUO for a LLU = [5*IP+2*DEL+1*OP+0.3*ANC+0.2*IMM+0.2*FP]
Using this formula and based on data extracted from DHIS2 on these 6 indicators for each PNFP
for the FY 2013-14, NU Health has calculated the Total Health Output for each HF, and been able
to compare the two groups of PNFP. The two PNFP groups of Lango and Acholi sub-regions are
sufficiently homogenous to ensure that the SUO method for comparison of Total Health Output is
adequate and useful.
Limitations of this method
One of the limitations of this method is the quality of the data presented by DHIS2. As per NU
Health experience, the reported figures are not totally accurate due to miscalculation or
misclassification by PNFP in the way their data are submitted to the DHT. A second limitation is
due to the SUO formula which, as any indicator, is limited to certain factors while excluding others.
Finally, it also does not differentiate weighting between HC3 and HC2 and between hospitals and
HC4, while in reality the higher the level of care, the higher the cost of delivering the same health
care services.
It should also be noted here that Lacor Hospital is excluded from this study as there is no
comparable institution in the Lango region offering a similarly large range of services. See page
18 of NU Health’s inception report for more detailed background on this statement.