Lecture 63 Rabies

of 6
-
Upload
paijo-suseno -
Category
Documents
-
view
213 -
download
0
Transcript of Lecture 63 Rabies
-
7/31/2019 Lecture 63 Rabies
1/6
1
COURSE: MEDICAL MICROBIOLOGY, MBIM 650/720 FALL 2001TOPIC: Zoonotic viruses II viruses with vertebrate vectors LECTURE:63
FACULTY: Dr. Margaret Hunt (Tel: 733-3293; e-mail: [email protected])
REFERENCE: Murray et al., Microbiology, 3rd Ed., Chapter 58 (Rhabdoviruses, appropriateparts of chapters 60 (Bunya- and Hanta- viruses) and 64 (Filo- and Arena-viruses).
WEB SITES: http://www.cdc.gov/ncidod/dvrd/rabies/introduction/intro.htm (rabies, excellent)http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5008a1.htmhttp://www.cdc.gov/ncidod/diseases/hanta/hps/index.htm (hantaviruses)
TEACHING OBJECTIVES: Introduction to viral zoonoses. Brief overview of general features ofrhabdoviruses, bunyaviruses (including hantaviruses), arenaviruses and filoviruses. Discussion of
ecology, epidemiology and public health. Discussion of: rabies; rodent borne hemorrhagic feverand arenaviruses; hemorrhagic fever with renal syndrome, hantavirus pulmonary syndrome andhantaviruses; filovirus-associated hemorrhagic fevers and Ebola and Marburg viruses..
RABIES
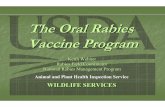
Rabies virus: Single-stranded RNA virus, negative-sense, non-segmented genome.Member of the Lyssavirus genus (lyssa = frenzy) of the Rhabdovirus family.Virus is enveloped, the nucleocapsid has helical symmetry.
TRANSMISSION:
Usually obtained by a bite from an infected animal. In rare cases, has been transmitted bycorneal transplant, or through contact of infected saliva with mucosal membranes or an openwound.. CDC: Inhalation of aerosolized rabies virus is also a potential non-bite route ofexposure, but other than laboratory workers, most people are unlikely to encounter an aerosol of
rabies virus. It has been suggested that people in infected bat caves may be exposed toaerosolized virus. Most bats are not infected.
helical nucleocapsid (RNA plusN protein)
G glycoprotein
SPIKES
lipid bilayer membrane
polymerase(2 proteins)
M protein
-
7/31/2019 Lecture 63 Rabies
2/6
2
PATHOGENESIS AND DISEASE:The virus replicates at the site of inoculation and then enters a peripheral nerve. It then travels
along the nerve (retrograde axoplasmic flow) to the dorsal root ganglia. It replicates here andgains entry to the central nervous system and spreads to various parts of the brain. From here itcan spread out via the nerves to various sites in the body (there is no viremia). The antibody
response in an unvaccinated person is not seen until after the disease develops. If there isdisease, it almost inevitably results in death.The incubation period is variable, from two weeks to eighteen months, with an average of about
two months. The distance from the muscle to the CNS and the amount of virus in the wound playa role in determining the length of the incubation period.Since it takes a considerable period of time for the virus to get to the CNS, there is time for post-
exposure prophylaxis in rabies. If a humoral immune response can be raised by vaccination whilethe virus is in transit, this can prevent the disease.
Symptoms can vary, and cases may often be misdiagnosed at first. There may be tingling or
paresthesia at the site of the bite. In the initial phase there is fever, headache, malaise, anorexia.Later symptoms include: nausea, vomiting, myalgia, hydrophobia (in 20-50% of patients), and avariety of neurological symptoms such as confusion, hallucinations, seizures and paralysis. This
is followed by coma, respiratory failure and death. Not all patients show all of these symptomsand the fact that rabies was the cause of the encephalitis may not be realized until post mortem.
DIAGNOSISNeutralizing serum or cerebrospinal fluid antibodies in an unvaccinated person are diagnostic but
usually are only detectable late in disease. A corneal impression or nuchal skin biopsy or brainbiopsy can be examined for rabies antigen using a direct fluorescent antibody test. Saliva may betested for rabies virus RNA by RT-PCR (reverse transcription-polymerase chain reaction).
Eosinophilic, cytoplasmic inclusion bodies (Negri bodies) are seen in post-mortem staining ofbrain sections in ~50-80% of cases. They are typical of rabies, but the results need to be read by
Murray et al., Medical Microbiology
-
7/31/2019 Lecture 63 Rabies
3/6
3
someone experienced with rabies and there can be false positives - so all such results need to beconfirmed by another method.
There is a single serotype of rabies, however, there are subtle differences in nucleotide sequencebetween strains. The virus RNA is therefore amplified by RT-PCR and sequenced. This can givea clue as to the likely origin of the virus.
EPIDEMIOLOGY
Usually transmitted by animal bite. Worldwide most cases arise from a dog bite. Canine rabies isprevalent in Latin America, Asia and Africa. In recent years (1990-2000) in the US the majority of cases (74%) have been associated with batrabies; of the 8 remaining cases, all were from dog/coyote like-strains of virus and 7/8 of thosewere acquired outside the US.
Many animals in the US are infected with rabies viruses, including raccoons (especially along theeastern seaboard states), skunks, coyotes, and foxes. Small rodents are rarely infected, but there
have been cases reported, especially in woodchucks. Dogs, cats and cattle are potential vectors -in the US immunization of pets has lessened the risk of pets acquiring rabies from wild animals.Bats also carry rabies, although most bats are not infected. Bats have very small, sharp teeth,
and people who are bitten may not be aware of the bite, or not bother to do anything about it.With most bites from other rabid animals, the victim will get treatment because the bite is moreserious and also because the animal appeared to behave in a suspicious fashion, the level of
awareness seems to be lower for suspiciously behaving bats. Thus immunization of pets andprompt response for bites from most suspicious animals may explain why bat-transmission ofrabies has been the predominant mode of transmission in recent years.
In many cases of bat-associated rabies, there is no record of a bite. In some cases, the victim or
their family may be aware that they handled a bat or that an oddly behaving bat was found in e.g.a bedroom (e.g. a bat which is active by day, is easily approached, is unable to fly, is in a room ina house or on a lawn). However, as mentioned above, if the victim is not sufficiently lucid toanswer questions it may be difficult to obtain a history of bat contact since they may not have
found the incident remarkable enough to mention to anyone.
Human to human transmission has occurred in a few cases of corneal transplants (when it was
not realized that the encephalitis was due to rabies). This has led to stricter criteria in screening ofpotential donors for encephalitis so that those who might have rabies (or Creutzfeld-Jakob
-
7/31/2019 Lecture 63 Rabies
4/6
4
disease) are not accepted. Apart from these cases, no human-human spread of the disease hasever been documented.
PREVENTION AND TREATMENT OF A PERSON WHO MAY HAVE BEEN EXPOSED
The wound is immediately and thoroughly washed with soap and water, then treated with 40-70%ethyl alcohol or an antiseptic such as benzyl ammonium chloride. The State Health authoritiesshould be promptly informed. The risk of exposure to rabies and whether prophylactic treatment
should be given are determined in consultation with the State Health Department. If the animal isavailable, the brain is examined for rabies virus antigen by fluorescent antibody. (In some cases,if the bite was from a domesticated cat or dog, the animal may be kept under close observation).
Post-exposure prophylaxisRabies vaccine. This is an inactivated vaccine and is strongly immunogenic. It is grown in
human diploid cells or rhesus monkey lung cells and is more potent and has fewer side effectsthan the vaccine used in the early 1980s. A purified chick embryo cell grown vaccine is alsoavailable. The vaccine is administered as a series of injections over a 4-week period.
Human rabies immunoglobulin (HRIG). HRIG is prepared from the plasma of hyperimmunedonors. Up to half of the recommended dose is infiltrated into the wound area if possible. Theremainder is given as an intramuscular injection. A separate syringe and a separate site are used
for the HRIG and the vaccine so that the HRIG does not neutralize the vaccine.
So far there has never been a case of someone who received post-exposure prophylaxis in the
US developing rabies.
Pre-exposure prophylaxis
People at risk for rabies infection may be vaccinated as a preventive measure. Such individualsinclude rabies-laboratory workers; certain people in areas with enzootic rabies who are at risk forexposure to rabid animals: veterinarians and their staff, wildlife control workers, spelunkers;
travelers who will be spending more than a month in areas with enzootic rabies. People at highrisk for exposure to rabid animals should have regular serologic testing and booster vaccinationswhen necessary.
If a vaccinated person is exposed to rabies, they still need to get post-exposure prophylaxis, but
the number of post-exposure vaccination shots is reduced and HRIG is not used.
TREATMENTThere is no specific anti-viral treatment once symptoms develop. Intensive supportive care isgiven. However, there have only ever been three cases of documented recovery from rabies.
-
7/31/2019 Lecture 63 Rabies
5/6
5
VIRAL DISEASES TRANSMITTED BYRODENTS
ARENAVIRUS FAMILY
HF=hemorrhagic fever
All of the above viruses have a rodent vector (there are other disease-associated arenaviruses).
The arenavirus-associated hemorrhagic fevers have a high case-fatality rate (5-35%). Thearenaviruses seem to easily establish persistent infections in certain rodents, which get a viruria.Humans are thought to acquire infection from contact with rodent urine contaminated materials.
Disease in humans: dehydration, hemoconcentration, hemorrhage, shock syndrome,cardiovascular collapse. Recently (1999-2000) there have been reports of three deathsapparently due to a North American arenavirus (Whitewater Arroyo). It is not clear if there are
other unrecognised cases of this virus or what the case fatality rate is.
BUNYAVIRUS FAMILY HANTAVIRUS GENUS
i) Associated with hemorrhagic fever with renal syndrome (HFRS)Korean hemorrhagic fever has a case-fatality rate of about 7%, other members of the
hantaviruses which cause HFRS (hemorrhagic fever with renal syndrome) tend to have a lowerfatality rate. Transmission appears to be via inhalation of, or contact with, rodent excreta.
FAMILY ENVELOPE
yes
yes
SYMMETRY
helical
helical
GENOME
ssRNA
ambi-sensesegmented
ssRNA (-ve)segmented
Hantavirus genus
VIRUS
Lassa
Machupo
Junin
Whitewater Arroyo
DISEASE
Lassa fever (HF)
Bolivian HF
Argentine HF
Whitewater Arroyo HF
OCCURRENCE
Africa
South America
South America
Western US
-
7/31/2019 Lecture 63 Rabies
6/6
6
ii) Associated with severe pulmonary syndromeA newly recognized (1993) group of hantaviruses in North and South America are transmitted by
rodents (by inhalation or contact with excreta) and cause Hantavirus Pulmonary Syndrome (HPS)rather than hemorrhagic fever. These hantavirus pulmonary syndrome viruses have a high casefatality rate of ~40%. The viruses are widely distributed throughout the US but relatively rarely
cause human disease - about 280 known cases so far in the US. Initial symptoms often includefever, myalgia, nausea, vomiting and a cough, this may progress to dizziness and shortness ofbreath and then acute respiratory distress. There are a several hantaviruses which have been
associated with this syndrome, one of the best known of the US HPS-associated viruses is SinNombre virus.
VIRAL DISEASES IN WHICH RESERVOIRAND VECTOR ARE UNCLEAR
Ebola and Marburg viruses are filoviruses and cause hemorrhagic fevers. The case-fatality ratecan be as high as 60-70% for certain strains of these viruses. These viruses occur in Africa, but
the natural reservoir is unknown. They occasionally infect humans, but the means by which thisoccurs is usually not clear. Patients have severe hemorrhages and there is a lot of virus present,so stringent barrier nursing techniques are needed to prevent further spread. There have been a
few cases where humans have been infected by apparently healthy laboratory monkeys.
NAME
Korean HFRS
HFRS
Hantavirus
pulmonarysyndrome (HPS)
TYPE OF DISEASE
hemorrhagic fever withrenal syndrome (HFRS)
hemorrhagic fever withrenal syndrome
hantavirus pulmonary
syndrome
OCCURRENCE
S.E.Asia
Europe, Asia
North and
South America
VECTOR UNKNOWN
FAMILY ENVELOPE
yes
SYMMETRY
helical
GENOME
ssRNA (-ve)