Lecture 3. Secondary glomerular diseases and diseases of large blood vessels.
26
Lecture 3. Secondary glomerular diseases and diseases of large blood vessels
-
Upload
ashlyn-welch -
Category
Documents
-
view
233 -
download
1
Transcript of Lecture 3. Secondary glomerular diseases and diseases of large blood vessels.

Lecture 3. Secondary glomerular diseases and diseases of large blood vessels

Crescentic Glomerulonephritis and Vasculitis
• VASCULITIS: Inflammation and necrosis of blood vessels
• Large vessel vasculitis eg Giant cell (Temporal) arteritis
• Medium sized vessel arteritis eg Polyarteritis Nodosa
• Small vessel vasculitis*– *Capillaries, venules, arterioles +/- small arteries
– Skin only e.g. drugs
– Multiple organs, tissues, kidney: systemic vasculitis
• Crescentic glomerulonephritis is typical of systemic vasculitis involving the kidney
• (renal-limited crescentic GN also occurs)

Vasculitis

Vasculitis - artery in Polyarteritis Nodosa
Lumen

Crescentic Glomerulonephritis, vasculitis
• Crescent: Proliferation of cells inside Bowman’s capsule - obliterates urinary space
Glom
CRESCENT

Systemic small vessel Vasculitis
• Microscopic polyangiitis (micro PAN)
– Vasculitis in small, med blood vsls; glomerulonephritis
• Wegener’s granulomatosis
– Necrosis and granulomas in upper/lr resp tract
– Vasculitis in small, med blood vsls; glomerulonephritis
• Henoch-Schlonlein purpura
• Cryoglobulinemia
• Goodpasture’s syndrome and anti-GBM nephritis
– Anti-GBM, anti-alveolar BM antibodies
– Pulmonary haemorrhage, glomerulonephritis

Wegener’s granulomatosis
• Multinucl Giant cell• Granulomas, necrosis,
vasculitis in respiratory tract
• Crescents, focal necrosis in glomeruli
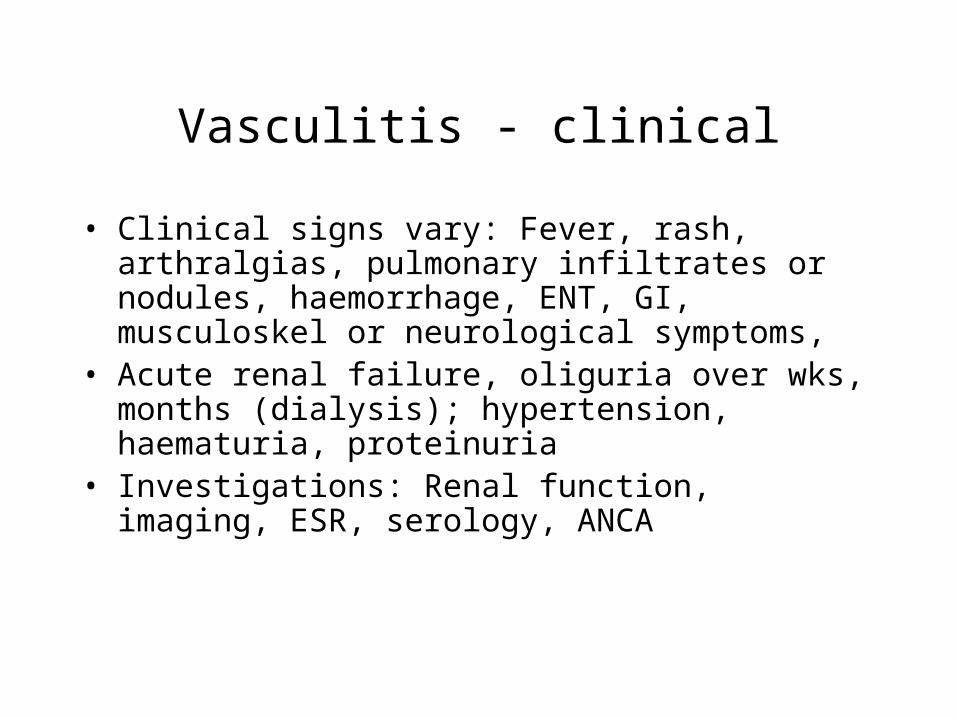
Vasculitis - clinical
• Clinical signs vary: Fever, rash, arthralgias, pulmonary infiltrates or nodules, haemorrhage, ENT, GI, musculoskel or neurological symptoms,
• Acute renal failure, oliguria over wks, months (dialysis); hypertension, haematuria, proteinuria
• Investigations: Renal function, imaging, ESR, serology, ANCA

Anti-neutrophil cytoplasmic antibodies (ANCA)
• Serum antibodies to enzymes in neutrophil granules, monocyte lysosomes
• Immunofluorescence: Cytoplasmic or Perinuclear
• P-ANCA (anti-myeloperoxidase) in 80% of micro polyangiitis; more often indolent, renal limited
• C-ANCA (anti-proteinase 3) in 90% of Wegener’s
• Very useful in diagnosis; follow up of disease activity in Wegener’s with C-ANCA

Crescentic GN, vasculitis
• Crescent
• Necrosis and crescentN
Cr

Crescentic GN, vasculitis: Immunofluorescence findings
65% “pauci-immune” – pauci = few or no IC
• 20% immune complex
• 15% anti-GBM
. .. ,.

Crescentic GN, vasculitis - pathology
• LM: Glomerular crescents, inflammation and necrosis• Crescent: Proliferation of cells inside Bowman’s capsule -
obliterates urinary space (-> oliguria)• Focal glomerular inflammation, necrosis
– Immune complex deposits FM & EM 20% e.g. SLE, cryoglob
– anti-GBM 15% Goodpature’s syndrome, anti-GBM nephritis
– pauci-immune 65% (in ANCA+ microscopic polyangiitis, Wegener’s)
– Adverse prognosis: >80% crescents, anti-GBM
• Summary: Crescentic GN typical of systemic small vessel vasculitis; sometimes limited to kidney

Secondary glomerular diseases
• Glomerular disease an important feature of multisystem diseases - vasculitis, diabetes, SLE, amyloidosis
• DIABETES MELLITUS– Relative/absolute deficiency of insulin secretory response; leading
cause of end-stage renal disease in US, Europe (40%)
– Type 1: autoimmune destruction of insulin secreting beta cells
– Type 2 (90%) decreased insulin secretion; insulin resistance
• Gradual onset of proteinuria, glycosylation of proteins, microangiopathy thick leaky GBM, and increased mesangial matrix synthesis; also suscept to pyelonephritis
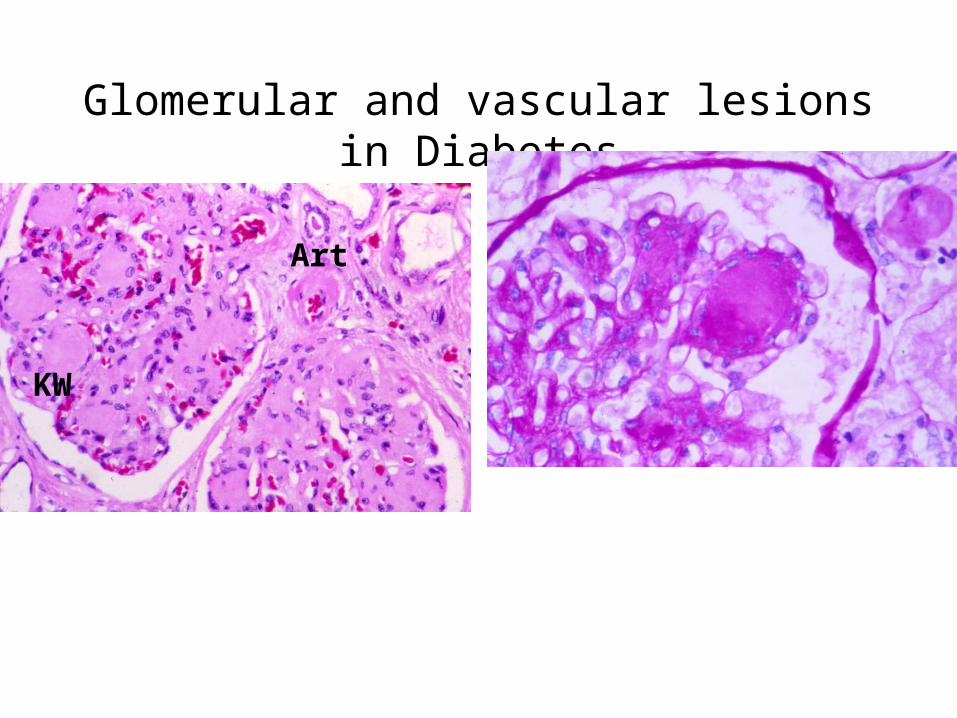
Glomerular and vascular lesions in Diabetes
Art
Art
KW
Art

SLE (Lupus) nephritis
SLE (Lupus) nephritis
• Chronic auto-immune disease; females 20-30 yrs
• Rash, connective tissues, kidney etc
• Antinuclear (e.g. anti-ds DNA), anticytoplasmic & antiphospholipid antibodies
• Lupus nephritis in 90% - variable proteinuria, haematuria
• Immune Complex Glomerulonephritis ranges from very mild to severe
• Glomerulonephritis a major cause of morbidity, mortality

Lupus nephritis

Amyloidosis
• Abnormal beta-fibrillar protein (15 classes)
• (A-beta in Alzheimer’s)
• AA amyloid (chronic infection, inflammation) or AL amyloid (Ig derived) deposited in glomeruli, renal vessels
• Proteinuria
• Poor prognosis

Amyloidosis

Clinical Presentations of glomerular disease

Clinical Presentations of glomerular disease• CRESCENTIC GN and VASCULITIS (“Rapidly progressive GN”)
• HAEMATURIA– IgA nephropathy
• PROTEINURIA & NEPHROTIC SYNDROME– Minimal change disease
– Membranous glomerulonephritis
– SLE, diabetes, renal amyloidosis
• ACUTE NEPHRITIS – Post-streptococcal glomerulonephritis -
• Haematuria, hypertension, raised serum creatinine, oedema
• Immune complexes to streptococcal antigen
• Most patients recover fully
• CHRONIC RENAL FAILURE– Abnormal renal function tests. Raised se Cr, reducd Cr Cl & clinical signs
– Develops slowly, chronically over years
– Glomerular disease not the only cause (nephrosclerosis, APCKD)
Lesions of large blood vessels
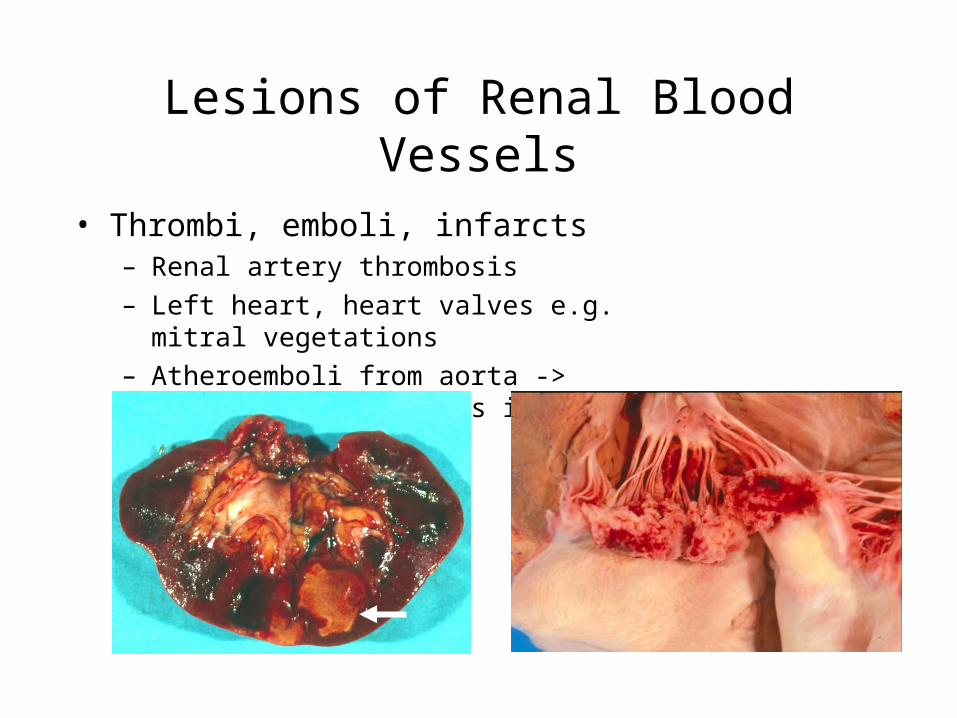
Lesions of Renal Blood Vessels
• Thrombi, emboli, infarcts– Renal artery thrombosis
– Left heart, heart valves e.g. mitral vegetations
– Atheroemboli from aorta -> interlobular arteries in kidneys

Lesions of Renal Blood Vessels
• Vasculitis (other than small vessel vasculitis)– Large and medium sized blood vessels, small
arteries.
– Temporal (Giant cell) arteritis - head and neck
– Takayasu’s - coronaries
– (Vasculitis a/w infection include fungal)
• Polyarteritis Nodosa – aneurysms in coeliac, mesenteric, coronary and renal
arteries; hepatitis B in 30%; ANCA negative

Lesions of Renal Blood Vessels
• Renal artery stenosis– Proximal renal artery atherosclerosis– Fibromuscular dysplasia– GFR afferent arteriole pressure -> Renin, BP
• Nephrosclerosis– Age change worsened by hypertension– Thick arterioles (“hyaline” arteriolosclerosis) & thickened
small, medium sized arteries – Small kidneys, granular suface +/- larger scars
• Malign BP and thrombotic microangiopathies– Endothelial injury, necrosis of media, thrombi
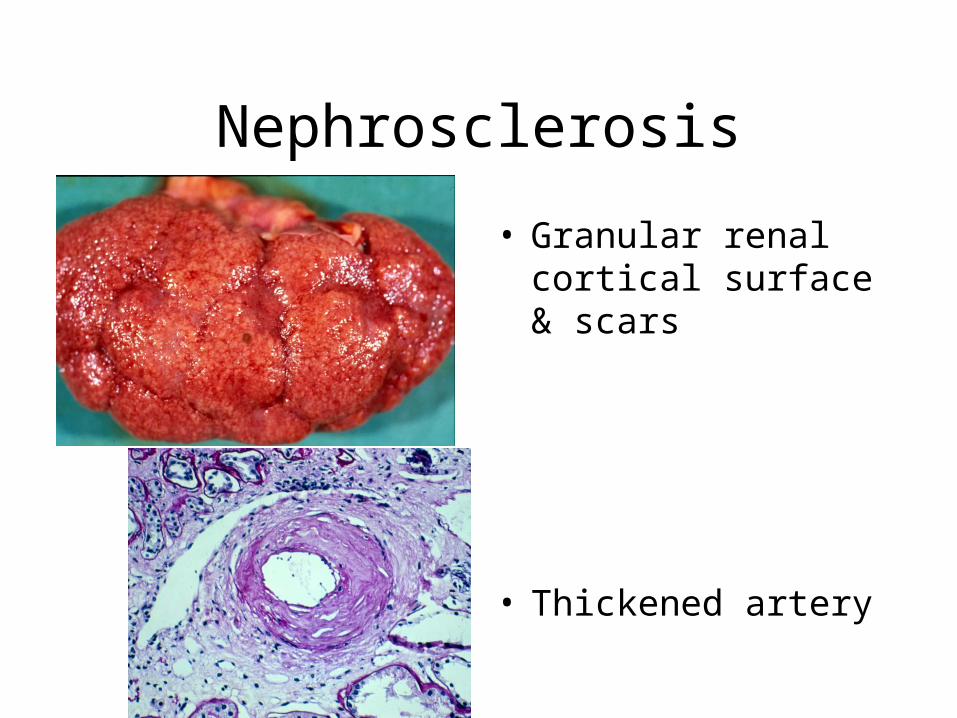
Nephrosclerosis
• Granular renal cortical surface & scars
• Thickened artery