Lecture 3 2012 (1)

of 22
-
Upload
leyla-majunda -
Category
Documents
-
view
215 -
download
0
Transcript of Lecture 3 2012 (1)
-
7/27/2019 Lecture 3 2012 (1)
1/22
Natural Products
Dr Suzanne Fergus
-
7/27/2019 Lecture 3 2012 (1)
2/22
MorphineExcellent Analgesic
Serious Side Effects:Respiratory depression
Addiction
Nausea
Drowsiness
Constipation
Euphoria
Source:
Opium Poppy
1803 Isolated main alkaloid
-
7/27/2019 Lecture 3 2012 (1)
3/22
Administered by
injection
(subcutaneous orintramuscular)
10mg every 4 hours
What can you say
about solubility of
morphine?
SIDE EFFECTS??
-
7/27/2019 Lecture 3 2012 (1)
4/22
Blood Brain Barrier
The blood-brain barrier (BBB) is formed by the braincapillary endothelium and excludes from the brain 100%
of large-molecule neurotherapeutics and more than 98%
of all small-molecule drugs
Example: Histamine readily crosses the porouscapillaries perfusing all peripheral tissues but is excluded
from entry into the brain or spinal cord by the BBB.
-
7/27/2019 Lecture 3 2012 (1)
5/22
Morphine
-
7/27/2019 Lecture 3 2012 (1)
6/22
Opioid Receptor Interactions
Ionic Bond interaction with protonated 3
amine
Hydrogen Bond with phenol
Van der Waals with aromatic ring
-
7/27/2019 Lecture 3 2012 (1)
7/22
Opioid Receptor Interactions
-
7/27/2019 Lecture 3 2012 (1)
8/22
Structure Activity Relationships
Mask or remove a functional group
Test the analogue for activity
Determines the importance or otherwise of afunctional group for activity
-
7/27/2019 Lecture 3 2012 (1)
9/22
Codeine
Only 0.2-0.7% codeine
available in opium
Methylation of morphine
Non-addictive
Codeine 20% active (injected
peripherally) 0.1% active (injected into brain)
Prodrug-partly demethylated in liver to producemorphine
-
7/27/2019 Lecture 3 2012 (1)
10/22
Removing the oxide bridge (and hydrogenating
double bond, removing one alcohol) produces
levorphanol, which has enhanced analgesicproperties over morphine.
O
HO
H
NH
CH3
HO1
23
4
5
6
7
8
9
1011
12
1314
15 16
H
NH
CH3
HO1
23
4
5
6
7
8
9
10
11
12
1314
15 16
Levorphanol
Levorphanol is used to treat severe pain and has several
brand names.
-
7/27/2019 Lecture 3 2012 (1)
11/22
Levorphanol
Removing the oxide bridge (and hydrogenating double
bond, removing one alcohol) produces levorphanol,which has enhanced analgesic properties over morphine
-
7/27/2019 Lecture 3 2012 (1)
12/22
Mirror image has antitussive properties,
but no analgesic properties
H
NH
CH3
HO1
2
3
4
5
6
7
8
9
10
11
12
1314
15 16
Levorphanol
H
NH
H3C
OH1
2
3
4
5
6
7
8
9
10
11
12
1314
1516
dextrorphan
Mirror
analgesic + antitussiveAntitussive only
Dextromethorphan (DM orDXM) is an antitussive drug that
is found in many over-the-counter cold and cough
preparations, usually in the form of dextromethorphanhydrobromide.
-
7/27/2019 Lecture 3 2012 (1)
13/22
Pethidine
-
7/27/2019 Lecture 3 2012 (1)
14/22
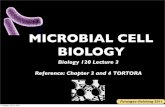
Fentanyl (A Piperidine)
100 times more active than morphine!
Most potent agonist for opioid
receptor
Can efficiently cross the BBB
Lacks phenolic group and is
therefore LIPOPHILIC
-
7/27/2019 Lecture 3 2012 (1)
15/22
Fentanyl is most lipid-soluble andmorphine is the least lipid-soluble.
The octanol-water partition coefficient for
morphine is 6 and 9550 for fentanyl.
This difference in lipid solubility has
profound effects on how we can use these
2 drugs in clinical practice.
-
7/27/2019 Lecture 3 2012 (1)
16/22
Elimination half-lives: 2-4 hours formorphine and 3-7 hours for fentanyl.
Morphine lasts longer because once it
enters the central nervous system it has a
difficult time exiting the cellular lipid barrier
(blood-brain barrier). It is this retention in
the central nervous system that makes
morphine longer-acting than fentanyl.
-
7/27/2019 Lecture 3 2012 (1)
17/22
Heroin (Diamorphine)
2 x more active
than morphine 4 x more active
than morphineHow do we explain
this ?
-
7/27/2019 Lecture 3 2012 (1)
18/22
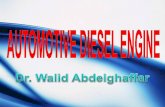
What structural elements are
necessary for activity ?
O
HO
H
NH
CH3
HO1
23
4
5
6
7
8
9
10
11
12
1314
15 16
R3R1
N
CH3
Basic NitrogenQuaternary Carbon Center
Spacer
R2
Aromatic Ring
-
7/27/2019 Lecture 3 2012 (1)
19/22
Methadone
Orally active
Side Effects less severe (sedation,
Euphoria & withdrawal symptoms
-
7/27/2019 Lecture 3 2012 (1)
20/22
10,000 more potent !!
Etorphine can cross BBB
300x more easily than
morphine as ishydrophobic and has 20x
better receptor binding
-
7/27/2019 Lecture 3 2012 (1)
21/22
-
7/27/2019 Lecture 3 2012 (1)
22/22
The impact of natural products on the well
being of mankind has been enormous andtheir study continues to influence research
in the fields of chemistry, biology and
pharmacy. (J. Med. Chem., 2008)
Critically discuss using relevant examples.