Lecture 1 Gastrointestinal Pharmacology(Powerpoint)
30
GASTRO-INTESTINAL Pharmacology Peptic ulcer disease/dyspepsia GORD Inflammatory bowel disease Irritable bowel syndrome Diarrhoea Constipation Pancreatitis
Transcript of Lecture 1 Gastrointestinal Pharmacology(Powerpoint)

GASTRO-INTESTINAL Pharmacology
Peptic ulcer disease/dyspepsia GORD Inflammatory bowel disease Irritable bowel syndrome Diarrhoea Constipation Pancreatitis
Dyspepsia / Peptic ulcer disease
Dyspepsia: upper abdo pain/discomfort (fullness, bloating, distension, nausea)
Peptic ulcersdefects in mucosa extending through muscularis mucosae
PrevalencePUD 5-10% lifetimedyspepsia 25-40%
Aetiology (most common) H.pylori NSAIDs

Parietal cell and acid regulation
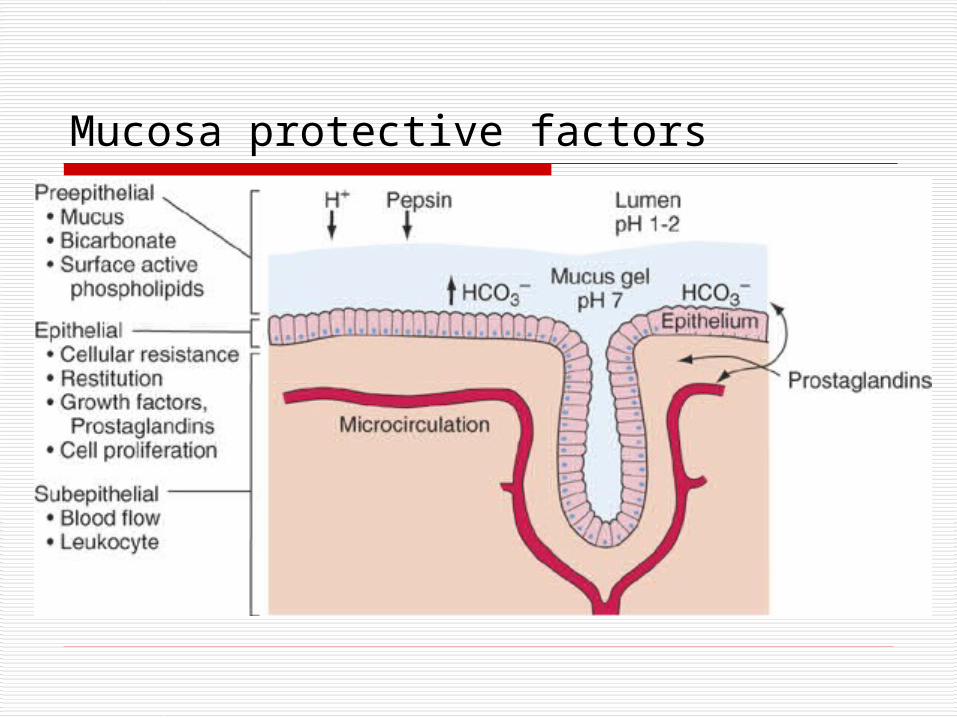
Mucosa protective factors
Introduction• Means self remedy
• Naturally occurring substances
• Localized in tissues
• Do not normally circulate
• Diverse physiological and pharmacological activities
• Differ from hormones and neurotransmitters
• Short duration of action
• Usually involved in a response to injury
• Sites of action restricted to the synthesis area

Mecanism of mucosal cells protection against acid digestion
- Secretion of a barrier of adherent mucus gel from the cells
- Secretion of bicarbonate into the mucus layer- Intrinsec resistance of the cell membranes to
hydrogen ion back-diffusion- High mucosal blood flow, which removes H+ from the
mucosa and provides additional bicarbonate- The phospholipid hydrophobic barrier

Antisecretory agents
Rising of intragastric pH above 3 for few hours - promote healing of most ulcers
Proton pump inhibitors - Omeprazole, Lansoprazole, Pantoprazole, Esomeprazole, Rabeprazole
H2 receptor antagonists- Cimetidine, Ranitidine, Famotidine, Nizatidine

Proton pump inhibitors - Omeprazole, Lansoprazole, Pantoprazole, Esomeprazole, Rabeprazole
Prodrugs activated in acidic secretory canaliculi Inhibit gastric H+K+ ATPase irreversibly Decrease acid secretion by up to 95% for up to 48
hours Use:Ulcers, GORD, Zollinger-Ellison Syndrome, reflux
oesophagitis Side effects
Generally well tolerated headache, headache dizziness Omeprazole – impotence, gynaecomastia May increase risk of GI infections (reduced acidity)
Note: pH > 6 necessary for platelet aggregation Give high dose PPI in active GI bleed (eg Omeprazole 8mg/hr for 72 hrs)

H2 receptor antagonists - Cimetidine, Ranitidine, Famotidine, Nizatidine
Competitive and selective inhibition of histamine H-2 receptor Suppress 24 hr gastric secretion by 70% Less effective than PPI Caution: renal failure, pregnancy, breast feeding Interaction: Cimetidine binds to CYP 450 (retards oxidative
drug metabolism) note interactions with warfarin, phenytoin, theophylline.
Side effects Well tolerated, less than 3% adverse effects Diarrhoea, headache, drowsy, fatigue, constipation, CNS Rarely pancreatitis, bradycardia, AV block, confusion
(elderly, especially cimetidine) Rarely blood dyscrasias

Antiacids - aluminium hydroxide, magnesium trisilicate
Neutralise gastric acidity; more prolonged effect if taken after food
Maqnesium salts neutralise acid much more rapidly than aluminium salts
Most are relatively poorly absorded from the gut May chelate other drugs (avoid concomitant
administration of other drugs) Side effects: diarrhoea (Mg), constipation (Al) Milk alkali syndrome (alkalosis, renal insufficiency,
hypercalcemia)
Cytoprotective agents
Sucralfate Forms sticky polymer in acidic environment Inhibits hydrolysis of mucous proteins by pepsin 1 g bd to 1g qds SE: constipation, aluminium absorption (avoid in
severe renal impairment due to risk of encephalopathy)
Bismut salts- Precipitate in the environment of the stomach and then
bind to glycoprotein on the base of an ulcer – complex with similar effects of sucralfate
- Suppress H. Pylori- Risc of accumulation of bismuth - limited of 6 weeks
Cytoprotective agents
Misoprostol Analogue of prostaglandine E1 Increased gastric mucus production Enhanced duodenal bicarbonate secretion Increased mucosal blood flow, which aids buffering of H+
that diffuses back across the mucosa Direct effect on gastric acid secretion, reduse endogenous
histamine secretion Limit the damage caused by agents such as acid and alcohol
to superficial mucosal cell Used to reduce NSAID induced gastric damage SE: diarrhoea and abdominal cramps, uterine contractions,
menorragia, postmenopausal bleedings

Cytoprotective agents
Carbenoxolone Synthetic derivative of a constituent of
liquorice – it has a steroid structure Enhances the synthesis of gastric mucus -
stimulating prostaglandin secretion Increases the protective barrier in the stomach
aganist acid and peptic digestion SE: aldosterone like actions – water retention
and hypokalaemia, hypertention, heart failure
H. pylori eradication
Eradication increases ulcer healing Reduces recurrence MALT, Ca (can lead to resolution)
Triple therapyFor 7 (14) days twice daily eg
full dose PPI + Amoxicillin + Clarithromycin/Metronidazole
Effective in 80-85%

GORD
Definition Abnormal reflux of gastric contents into oesophagus ± mucosal damage
Prevalence > 50% of population > once a year 50% of patients have erosive oesophagitis
Pathophysiology Antireflux barrier (sphincter…) Acid, pepsin, trypsin, bile acids, hiatus hernia
GORDTreatmentLifestyle advice
Dietary habits (fat, alcohol, caffeine, timing) Smoking Weight loss Raising head But little evidence for all those
Medication H-2 receptor antagonists PPI Antacids Prokinetics

Prokinetics
Metoclopramide Dopamine receptor-blocking agent Peripheraly it enhances gastric motility –
stimulating Ach release, sensitising receptors
bioavailability 80% SE: sedation, extrapiramidal effects,
increased prolactin and aldosterone release

Inflammatory Bowel Disease
Ulcerative colitis Diffuse mucosal inflammation limited to the colon
Crohn's disease patchy transmural inflammation May affect any part of GI tract
Features UC bloody diarrhoea, colicky pain, urgency,
tenesmus CD abdominal pain, diarrhoea, weight loss
intestinal obstructionsystemic symptoms

Drugs in IBD
Aminosalicylates Corticosteroids Thiopurines Methotrexate Ciclosporin Infliximab

Constipation
Stool: 70-85% water (100ml/d)
Normal stool frequency ≥ 3/week
Causes Dietary (fibre), drugs, hormonal disturbances, neurogenic
disorders systemic illnesses, IBS colonic motility disorder of defecation or evacuation (outlet)
Management Diet, fluid, fibre rich diet Avoidance of constipating drugsOnly then consider medication (haemorrhoids, exacerbation of
angina from straining…)

Laxatives
Bulk-forming Stimulant Faecal softeners Osmotic laxatives Bowel cleansing solutions
Oral Rectal-suppositories, enemas
General Contraindications: intestinal perforation and obstruction

Bulk-forming laxatives
Increase faecal mass which stimulates peristalsis
Bulk/softness/hydration dependant on fibre Ensure adequate fluid intake (obstruction) Effect can be delayed by a few days
Try dietary fibre first! Wheat bran, oat bran, bran buiscuits Pectins/hemicellulose (fruits, vegetables)
Ispaghula (Fybogel, Isogel) Methylcellulose (Cevelac) Sterculia (Normacol) Contraindication: intestinal obstruction, colonic
atony, faecal impaction Side effects: flatulence, abdominal distension, GI
obstruction, rarely hypersensitivity

Stimulant Laxatives Increase intestinal motility
Diphenylmethane derivatives Sodium picosulfate, hydrolyzed by bacteria to active form, effects vary Bisacodyl (Dulco-lax), usually 5-10mg nocte
Anthraquinone Laxatives Require activation in colon (bacteria), onset of action delayed (6-12 hours) Senna (Senokot), plant derivative Danthron (Co-danthramer) possibly carcinogenic, only use in terminally ill
Docusate Sodium stimulant and softening
Glycerol suppositories(Parasympathomimetics such as bethanechol, neostimin rarely used)
Side effects: cramps, diarrhoea, hypokalaemia

Osmotic laxativesOsmotically mediated water retention
Nondigestible sugars and alcohols synthetic disaccharide, resists intestinal disacharidase draw water in osmotically, not absorbed Lactulose Use: elderly, opioids, hepatic encephalopathy (↓ ammonia
production)
Magnesium salts Phosphates (rectal, Fleet) Sodium citrate (rectal, Micralax Micro-enema)
Polyethylene Glycol-Electrolyte Solutions - Macrogels Sequester fluid in bowel, poorly absorbed Movicol

Faecal softeners - Emollients Sodium docusate (stimulant and softening)
Arachis oil enema for impacted faeces
Liquid Paraffin (oral solution)Side effects: anal irritation, interference with absorption of fat soluble vitamins, granulomatous reactions

Bowel cleansing solutions Before colonic surgery, colonoscopy and
radiological examinations
eg Fleet, Klean-Prep, Picolax
Contraindications: obstruction, GI-ulceration, perforation, CCF, toxic colitis or megacolon, ileus
Side effects: nausea, bloating, cramps, vomiting

DiarrhoeaDefinition
Excessive fluid weight (200g/day)Mechanism
Increased osmotic load Excessive secretion (electrolytes and water) Exudation of protein and fluid Altered motility (rapid transit) Often combined
Management Rehydration, maintain fluid and electrolyte balance NaCl absorption linked with glucose uptake (rehydr.
solutions) Antimicrobial therapy. May mask clinical picture,
delay clearance of organism, increase risk of systemic invasion.

Antimotility drugsOpioids
μ (motility) and δ (secretion) receptors, absorption (both)
Loperamide – Imodium 40-50x more potent than morphine Poor CNS penetration Increases transit time and sphincter tone Antisecretory against cholera toxin and some E.coli toxin T½ 11 hours, dose: 4 mg followed by 2mg doses (16mg/d max) Overdose: paralytic ileus, CNS depression Caution in IBD (toxic megacolon)
Codeine phosphate
Other Bismuth subsalicylate Adsorbents such as Kaolin (not recommended), charcoal
(insufficient data for adsorbents)

Diarrhoea
Clostridium difficile Clinical suspicion, test for
toxins (stool) Metronidazole PO Vancomycin PO

Irritable bowel syndrome Recurrent abdominal pain with disturbed bowel habits 9-12% of population affected ? Pathophysiology
Treatment Dietary modification Psychological therapies Fibre – binding water (diarrhoea and constipation) Antispasmodics
Anticholinergic – Hyoscyamine, methscopolamine Calcium channel antagonists and peripheral opioid receptor
antagonists Mebeverine: direct effect on smooth muscle cell
Tricyclic antidepressants Analgesic and neuromodulatory properties Loperamide, codeine

Antispasmodics
Antimuscarinics Reduce motility Quaternary amines
eg hyoscine butylbromide (Buscopan) less lipid soluble and thus less well absorbed than atropine
CI: angle-closure-glaucoma, mysthenia, paralytic ileus, pyloric stenosis and prostatic enlargement
SE: constipation, transient bradycardia, reduced bronchial secretions, urinary urgency etc
Other Direct relaxants of intestinal smooth muscle No serious side effects but avoid in paralytic ileus Alverine Mebeverine Peppermint oil (Colpermin)
.






![[Product Monograph Template - Schedule D]€¦ · ACTION AND CLINICAL PHARMACOLOGY ... Use of GLP-1 receptor agonists may be associated with gastrointestinal adverse reactions. This](https://static.fdocuments.us/doc/165x107/5af75f887f8b9ae948900933/product-monograph-template-schedule-d-action-and-clinical-pharmacology-.jpg)