Insert: Presenter Name Insert: Presenter Title / Organization.

Learning Objectives
• Discuss individualization of therapy in Type Diabetes mellitus
• Identify relevant aspects each new class of drugs
• Assess cardiovascular effects of the new class of drugs

Conflict of Interest Declaration: Nothing to Disclose
Presenter: DR. A. ABU-BAKARE
Title of Presentation: CHOOSING THE RIGHT DRUG FOR TYPE 2 DIABETES
I have no financial or personal relationships to disclose

Faculty/Presenter Disclosure
• Faculty: Dr Asiru Abu-Bakare
• Relationships with commercial interests:– Grants/Research Support: None
– Speakers Bureau/Honoraria: Astra Zeneca: BoehringerIngelheim Pharmaceuticals, Inc.: Elil Lilly and Company: Janssen Pharmaceuticals, Inc.; Merck & Co., Inc.: Novo Nordisk: Sanofi: Amgen Inc.: Abbott Laboratories:
– Consulting Fees: Novo Nordisk; Boehringer IngelheimPharmaceuticals; Eli Lilly; Sanofi
– Other: None

Disclosure of Commercial Support
• This program has received financial support from no organization.
• This program may have received support indirectly because of inclusion of materials I have used in previous talks sponsored by several Companies listed earlier.
• Potential for conflict(s) of interest:– Dr. Abu-Bakare has received no payments from any
organization supporting this program AND/OR organization whose product(s) are being discussed in this program].

28%
50%
67%
78%86%
91%
0%
20%
40%
60%
80%
100%
Target Achieved
≤6.5%
Target Achieved
≤7.0%
≤7.5% ≤8% ≤8.5% ≤9.0%
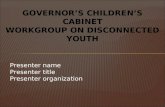
DM-SCAN: A1C Values Achievedin Primary Care
N=5123
% o
f P
ati
en
ts
A1C (%)
Leiter LA et al. Can J Diabetes. 2013;37(2):82-9.



CDA Treatment Algorithm
CDA: Canadian Diabetes Association. 1. CDA. Can J Diabetes. 2013;37(suppl 1):S61-8.
8
A1C <8.5% Symptomatic hyperglycemia with metabolic decompensation
A1C 8.5%
If not at glycemic target (2-3 mos)
Start/Increase metformin
L
I
F
E
S
T
Y
L
E
Patient CharacteristicsDegree of hyperglycemia
Risk of hypoglycemiaOverweight or obesity
Comorbidities (renal, cardiac, hepatic)Preferences & access to treatment
Other
AT DIAGNOSIS OF TYPE 2 DIABETES
Agent CharacteristicsBG lowering efficacy and durability
Risk of inducing hypoglycemiaEffect on weight
Contraindications & side-effectsCost and coverage
Other
Initiate insulin +/- metformin
Start metformin immediately
Consider initial combination with another antihyperglycemic agent
If not at glycemic targets
Make timely adjustments to attain target A1C within 3 to 6 months
Add an agent best suited to the individual:
Start lifestyle intervention (nutrition therapy and physical activity) +/- Metformin




Noninsulin Agents Available for T2D
Class Primary Mechanism of Action Agent(s) Available as
-Glucosidase inhibitors
Delay carbohydrate absorption from
intestine
AcarboseMiglitol
Precose or genericGlyset
Amylin analogue
Decrease glucagon secretion
Slow gastric emptying
Increase satiety
Pramlintide Symlin
Biguanide Decrease HGP
Increase glucose uptake in muscleMetformin Glucophage or generic
Bile acid sequestrant Decrease HGP?
Increase incretin levels?Colesevelam WelChol
DPP-4 inhibitors
Increase glucose-dependent insulin
secretion
Decrease glucagon secretion
AlogliptinLinagliptinSaxagliptinSitagliptin
NesinaTradjentaOnglyzaJanuvia
Dopamine-2 agonist Activates dopaminergic receptors Bromocriptine Cycloset
Glinides Increase insulin secretionNateglinideRepaglinide
Starlix or genericPrandin
DPP-4 = dipeptidyl peptidase; HGP = hepatic glucose production.
Garber AJ, et al. Endocr Pract. 2013;19(suppl 2):1-48. Inzucchi SE, et al. Diabetes Care. 2012;35:1364-1379.
Continued on next slide

Noninsulin Agents Available for T2D
Class Primary Mechanism of Action Agent(s) Available as
GLP-1 receptor agonists
Increase glucose-dependent insulin
secretion
Decrease glucagon secretion
Slow gastric emptying
Increase satiety
AlbiglutideDulaglutideExenatideExenatide XRLiraglutide
TanzeumTrulicityByettaBydureonVictoza
SGLT2 inhibitors Increase urinary excretion of glucoseCanagliflozinDapagliflozinEmpagliflozin
InvokanaFarxigaJardiance
Sulfonylureas Increase insulin secretion
GlimepirideGlipizideGlyburide
Amaryl or genericGlucotrol or genericDiaeta, Glynase, Micronase, or generic
Thiazolidinediones
Increase glucose uptake in muscle
and fat
Decrease HGP
PioglitazoneRosiglitazone
ActosAvandia
GLP-1 = glucagon-like peptide; HGP = hepatic glucose production; SGLT2 = sodium glucose cotransporter 2.
Garber AJ, et al. Endocr Pract. 2013;19(suppl 2):1-48. Inzucchi SE, et al. Diabetes Care. 2012;35:1364-1379.
Continued from previous slide

Effects of Agents Available for T2D
Met GLP1RA SGLT2I DPP4I TZD AGI Coles BCR-QRSU/
GlinideInsulin Pram
Renal impair-ment/ GU
Contra-indicated in stage 3B, 4, 5
CKD
Exenatide contra-
indicated CrCl <30 mg/mL
GU infection
risk
Dose adjust-ment
(except lina-
gliptin)
May worsen
fluid retention
Neutral Neutral Neutral
Increased hypo-
glycemia risk
Increased risks of hypo-
glycemia and fluid retention
Neutral
GI adverse effects
Mod Mod* Neutral Neutral* Neutral Mod Mild Mod Neutral Neutral Mod
CHF Neutral Neutral Neutral Neutral† Mod Neutral Neutral Neutral Neutral Neutral Neutral
CVDPossible benefit
Neutral Neutral Neutral Neutral Neutral Neutral Safe ? Neutral Neutral
Bone Neutral Neutral Bone loss NeutralMod bone
lossNeutral Neutral Neutral Neutral Neutral Neutral
Continued from previous slide
AGI = -glucosidase inhibitors; BCR-QR = bromocriptine quick release; Coles = colesevelam; CHF = congestive heart failure; CVD =
cardiovascular disease; DPP4I = dipeptidyl peptidase 4 inhibitors; GI = gastrointestinal; GLP1RA = glucagon-like peptide 1 receptor
agonists; GU = genitourinary; Met = metformin; Mod = moderate; SGLT2I = sodium-glucose cotransporter 2 inhibitors; SU =
sulfonylureas; TZD = thiazolidinediones.
*Caution in labeling about pancreatitis.†Caution: possibly increased CHF hospitalization risk seen in CV safety trial.








Individualizing A1C Targets
1. CDA. Can J Diabetes. 2013;37(suppl 1):S61-8.
Consider 7.1-8.5% if:
22

Food
intake
Stomach
GI tract
Intestine
Increases and prolongs GLP-1
effect on α-cells:
α-cells
Pancreas
Insulin release
Net effect:
Blood glucose
Beta-cells
Increases and prolongs GLP-1
and GIP effects on β-cells:
DPP-4
inhibitor
Glucagon secretion
Incretins
DPP-4

AEY
GT
FI
SD
YS
IA
MD
KI
H
HN
QT
I
Q
QD
FV
NW
LL
AQKG
KK
NDW
K
EFIWLVK
GR
GA K
AEH T
FT
SD
VS
SY
LE
GQ
AA
G
GIP: Glucose-dependent insulinotropic polypeptide
GLP-1: Glucagon-like peptide-1
The Incretins
DPP-4
DPP-4 Dipeptidyl Peptidase-4

1. Hansen L, et al. Endocrinology. 1999;140:5356–5363; 2. Deacon CF, et al. Am J Physiol. 1996;
271(3 pt 1):E458–E464.
More Than 50% of Secreted GLP-1 Is Degraded Before Plasma Absorption
– GLP-1 (green) released into intestinal capillaries is immediately exposed to DPP-4 (red)1
– > 50% of secreted GLP-1 is already degraded before it reaches the general circulation2
– > 40% of circulating GLP-1 is already degraded before it reaches β-cells2
Histochemistry by C. Ørskov, Panum Institute, Copenhagen. Copyright © 1999, The Endocrine Society.

GLP-1 (incretin)
Meal
(gut peptide hormone released from L-cells in the jejunum and ileum)
Inactive GLP-1
DPP-4
↓ glucagon secretion↑ insulin secretion
(glucose dependent)
↑ β-cell mass (long-term animal
studies)
DPP-4 Inhibitor
XGLP-1 analogue
GLP-1 analogues pharmacological level of GLP-1 action
DPP-4 inhibitors physiological level of GLP-1 action
↓ gastric emptying↓ food intake
↑ satiety
Effects of GLP-1 analogues and DPP-4 inhibitors


Sitagliptin Saxagliptin Linagliptin
Dosage 100 mg qd 5 mg qd 5 mg qd
Earliest approval 2005 2009 2011
Approximate half-life 12 hours 2 hours > 120 hours
Elimination Renal clearance (75%) Hepaticmetabolism to active metabolite( half as potent) Renal excretion ( 12% -29 % unchanged pant and 21%-52% as metabolite)
Entero-hepatic Eliminated unchangedin feces via biliary excretion (85%)
Important drug interactions
Low clinically meaningful interactions
Low clinicallyMeaningfulinteractions
Efficacy may be limited in patients receiving concurrent inducers of CYP3A4 or P-gp (eg, rifampicin)
Effect on weight Neutral Neutral Neutral
Adverse events Low Low Low
Currently Available DPP-4 Inhibitors Approved for Use in Patients with T2DM in Canada

Sitagliptin Saxagliptin Linagliptin
Usual dosage 100 mg qd 5 mg qd 5 mg qd
CrCl ≥ 50 mL/min No dose adjustment required
No dose adjustment required
No dose adjustment required
CrCl ≥ 30 to <50 mL/min
Dose reduction to 50 mg/day
Dose reduction to 2.5 mg/day
No dose adjustment required
CrCl < 30 mL/min Dose reduction to 25 mg/day
Dose reduction to 2.5 mg
No dose adjustment required
End-stage renal disease Dose reduction to 25 mg/day
2.5 mg administered following dialysis
No dose adjustment required
Peritoneal dialysis Dose reduction to 25 mg/day
No data available No dose adjustment required
Summary of Dose Reductions Recommended in Patients With Renal Impairment

Antihyperglycemic Agents and Renal Function
eGFR (mL/min/1.73 m2): <15 15–29 30–59 60–89 ≥ 90CKD Stage: 5 4 3 2 1
Acarbose Not recommended 25
Dapagliflozin 60Empagliflozin 45
Thiazolidinediones 30Contraindicated Caution and/or dose reduction
Canagliflozin 25 60†100 mg45
60†10 or 25 mg
Not recommended
Metformin 30 60
15Linagliptin
Sitagliptin 5030 50 mg25 mg
Saxagliptin 5015 2.5 mg
Alogliptin Not recommended 506.25 mg 12.5 mg30
Exenatide (BID/QW) 30 50Liraglutide* 50
Albiglutide 50
30
Repaglinide
Gliclazide/Glimepiride 15 30Glyburide 30 50
SGLT2 inhibitors
GLP-1R agonists
Alpha-glucosidaseInhibitors
Biguanide
DPP-4 inhibitors
Insulin Secreta-gogues
Dulaglutide 50
*Based on Saxenda Product Monograph June 2015; †Do not initiate if eGFR <60 ml/min.
1. CDA. Can J Diabetes. 2015;39:250-252; 2. Respective Product Monographs as of Nov 2015.
SafeNo dose adjustment but close monitoring of renal function




DPP-4 Inhibitors vs. Sulfonylureas
(added to Metformin): Efficacy by Baseline A1C
-0.14
-0.59
-1.11
-1.76
-0.26
-0.53
-1.13
-1.68
-2
-1.8
-1.6
-1.4
-1.2
-1
-0.8
-0.6
-0.4
-0.2
0
-0.3
-0.58
-0.81
-1.72
-0.32
-0.45
-0.84
-1.05
-2
-1.8
-1.6
-1.4
-1.2
-1
-0.8
-0.6
-0.4
-0.2
0
Sitagliptin 100 mg QD + MET
Glipizide + MET
Cha
nge
fro
m B
ase
line in A
1C
(%
)
Saxagliptin 5 mg QD + MET
Glipizide + MET
Ch
an
ge
fro
m B
ase
line in A
1C
(%
)
Sitagliptin vs. Glipizide1
52 weeks (n=793)
Saxagliptin vs. Glipizide2
52 weeks (n=858)
p values not available.
1. Nauck et al. Diabetes Obes Metab. 2007;9:194-205; 2. Goke et al. Int J Clin Pract. 2010;64:1619-31.
<7% 7-<8% 8-<9% ≥9% <7% 7-<8% 8-<9% ≥9%
112n= 117 167 179 82 82 21 33 n= 99 186 190 105 93 34 46105
Not head-to-
head trials











Nausea was generally mild to moderate, transientand rarely led to discontinuation of therapy.
Percentage of subjects with nausea through 26 weeks of treatment.
† † † p<0.05
† † p<0.001
† p<0.0001
Frequency of Nausea (LEAD 2)
Nauck et al. Diabetes Care 2009;32:84–90;
Gallwitz B et al. Int J Clin Pract. 2010;64(2):267-276.



0.0
-0.2
-0.4
-0.6
-0.8
-1.0
-1.2
-1.4
-1.6
-1.8
-2.0
*
Significant vs. comparator.
DULA vs.
Glargine
(AWARD-2)5
78 weeks
-1.1*
-0.6
BL~8.1%
DU
LA
1.5
GL
AR
EXE QW vs.
Glargine
(DURATION-3)4
26 weeks
-1.3
-1.5*
BL~8.3%
GL
AR
EX
E Q
W
LIRA vs.
Glargine
(LEAD-5)2
26 weeks
-1.3*
-1.1
BL~8.3%
GL
AR
LIR
A 1
.8
-1.9
-1.8*
LIRA vs.
Glargine
(EAGLE)3
24 weeksBL~9.1%
GL
AR
LIR
A 1
.8
ALBI vs.
Glargine
(HARMONY-4)6
52 weeks
-0.7-0.8
Noninferior
p=0.146
BL~8.3%
GL
AR
AL
BI
EXE BID vs.
Insulin
(4-Trial Analysis)1
26 weeksBL: N/A
-1.1-1.2
Noninferior
p=0.09
Δ in Wt. (kg): -1.9* 1.4-2.6* 1.4-1.8* 1.6 -3.0* 2.0 -1.1* 1.6-2.0 1.8
Ins dose (U/d): 293124 52 30NA
GL
AR
/ P
rem
ix
EX
E B
ID
p=0.0015
GLP-1R Agonists vs. Basal Insulin: Head-to-Head Trials
p=0.019 p=0.017 p<0.001
230 232 470 474 233 223 273 262 496 239n= 721 702
Me
an
ΔA
1C
Fro
m B
ase
line (
%)


R
Median Duration of Follow-upa
aApproximate median duration of follow-up for TECOS, based on the expected event rate at study initiation. EXAMINE = Examination of Cardiovascular Outcomes: Alogliptin vs Standard of Care in Patients With Type 2 Diabetes Mellitus and Acute Coronary Syndrome;SAVOR-TIMI = Saxagliptin Assessment of Vascular Outcomes Recorded in Patients With Diabetes
Mellitus Trial-Thrombolysis in Myocardial Infarction; TECOS = Trial Evaluating Cardiovascular Outcomes With Sitagliptin. CV = cardiovascular; MI = myocardial infarction; UA = unstable angina.
EXAMINE, SAVOR-TIMI, and TECOS
50
SAVOR-TIMI2
TECOS3
EXAMINE1
6.5–8.0
CV death, Nonfatal MI, Nonfatal stroke, or UA
req. hospitalization
RandomizationUp to Year 4
Year 3Year 2Year 1
CV death, Nonfatal MI, orNonfatal stroke
CV death, Nonfatal MI, orNonfatal stroke
Saxagliptin
Alogliptin
Placebo
Placebo
Placebo
6.5–12.0
6.5–11.0
HbA1c Range, % Primary End pointDuration of Treatment (as part of usual care)
Sitagliptin
1. White WB et al. N Engl J Med. 2013;369:1327–1335. 2. Scirica BM et al. N Engl J Med 2013;369:1317–1326. 3. Green JB et al. Am Heart J. 2013;166:983–989.e7.
R
R

EXAMINE, SAVOR-TIMI, and TECOS
EXAMINE1 SAVOR-TIMI2 TECOS3
Alogliptin vs Placebo
Saxagliptin vs Placebo
Sitagliptin vs Placebo
Sample size, N 5,380 16,492 14,724
Median duration of diabetes, y
≈7.2 10.3 9.4
Baseline HbA1c, % 8.0 8.0 7.3
Number of events 621 1,222 >1,300
Median duration of exposure, y
1.5 2.1 ≈ 3.0
51
EXAMINE = Examination of Cardiovascular Outcomes: Alogliptin vs Standard of Care in Patients With Type 2 Diabetes Mellitus and Acute Coronary Syndrome; SAVOR-TIMI = Saxagliptin Assessment of Vascular Outcomes Recorded in Patients With Diabetes Mellitus Trial-Thrombolysis in Myocardial Infarction; TECOS = Trial Evaluating Cardiovascular Outcomes With
Sitagliptin.

Endpoint
2-year KM rate (%)
HRp value for superiorityPlacebo
(n = 8,212)Saxagliptin(n = 8,280)
CV death 2.9 3.2 1.03 (0.87-1.22) 0.72
MI 3.4 3.2 0.95 (0.80-1.12) 0.52
Ischemic stroke 1.7 1.9 1.11 (0.88-1.39) 0.38
Hosp. for cor.revasc.
5.6 5.2 0.91 (0.80-1.04) 0.18
Hosp. for UA 1.0 1.2 1.19 (0.89-1.60) 0.24
Hosp. for HF 2.8 3.5 1.27 (1.07-1.51) 0.007
All-cause mortality 4.2 4.9 1.11 (0.96-1.27) 0.15
SAVOR TIMI-53: Individual Endpoints
52Scirica BM, et al. N Engl J Med 2013; 369(14):1317-26.

Relevant Baseline Characteristics
Characteristic SAVOR-TIMI1 EXAMINE2 TECOS3
# patients 16492 5380 14724
Males (%) 67 68 71
Mean age (SD) 68.1 (8.5) 61 66 (8)
BMI 31.1 (5.5) 28.7 30.2 (5.7)
A1C % 8.0 8.0 7.3 +/-0.7
Duration of DM 10.3 7.2 9.4
North America 31.9% 15.9 18%
Western Europe 26.0% 11.3* 14%
531.Scirica BM et al, N Engl J Med 2013. DOI: 10.1056/NEJMoa1307684. 2.White W. et al N Engl J Med 2013. DOI: 10.1056/NEJMoa1305889.
3.Bethel M.A. et al. DOM 2015 Jan 20. doi: 10.1111/dom.12441.
* Western Europe, Australia, New Zealand, and Middle East ** Eastern Europe, Western Europe

Relevant Baseline Characteristics (2)
Characteristic SAVOR-TIMI1 EXAMINE2 TECOS3
Established CVD 78.4% 100% 100%
MI 37.8% 88% 43%
CABG TBD 12.8% 25%
Stroke/TIA TBD 7.2% 21%
PAD TBD 9.6% 17%
CHF (all patients) 12.8% 28.5%4 18%
CHF (NYHA Class 3-4) 1.4% 5.65%4 2.5%
541-Scirica BM et al, N Engl J Med 2013. DOI: 10.1056/NEJMoa1307684. 2-White W. et al N Engl J Med 2013. DOI: 10.1056/NEJMoa1305889
3- Bethel M.A. et al. DOM 2015 Jan 20. doi: 10.1111/dom.12441. 4-Zannad F. et al. Lancet 2015. Published online March 10, 2015. http://dx.doi.org/10.1016/S0140-6736(14)62225-X

Days
Pat
ien
ts W
ith
En
dp
oin
ts (
%)
14
12
10
8
6
4
2
00
180 360 540 720 900
HR 1.00; 95% CI, 0.89–1.12P<0.001 (NI)P=0.99 (superiority)
Saxagliptin: 7.3%*Rate/100 person-yrs – 3.7
Placebo: 7.2%*Rate/100 person-yrs – 3.7
SAVOR: Kaplan – Meier Rates of the Primary Composite Endpoint – CV Death, MI, or Stroke
55
SAVOR: n = 16,492 patients (mean age 65 years) with type 2 diabetes (median duration 10.3 years) and established CVD or multiple risk factors. Median duration of follow-up: 2.1 years. A1C at 2 yrs: Saxa, 7.6%, PBO 7.9%
*K-M event rates are presented after 2 yrs., HR: hazard ratio; K-M: Kaplan-Meier; Pbo: placebo; Saxa: saxagliptin, Scirica BM, et al. N Engl J Med. 2013;369:1317-1326.

0
8
0
6
4
180 360 540 720 900
Days
Ho
spit
aliz
atio
n f
or
HF
(%)
Saxagliptin
2
Placebo
n = 16,492
HR 1.80(1.29 – 2.54)
p = 0.001
Overall HR 1.27(1.07 – 1.51)
p = 0.007
HR 1.48(1.14 – 1.87)
p = 0.003
HR = hazard ratio1.1%
0.6%
1.9%
1.3%
3.5%
2.8%
SAVOR TIMI – 53: Rates of Risk of Hospitalization For Heart Failure Over Time
56
• Saxagliptin neither increased nor decreased the risk of the 1° and 2° endpoints in these high-risk populations
• There were no specific subgroups in which the RR associated with saxagliptin was particularly high or low
• The absolute risk with saxagliptin was smallest in patients at low risk of HF and correspondingly larger in patients at highest risk
HF, heart failure. Scirica BM et al. Circulation. 2014; 130:1579-88.


Renal Handling of Glucose in Healthy Patients
SGLT = Sodium-dependent glucose transporter
Adapted from:1. Bailey CJ. Trends in Pharmacol Sci. 2011;32:63-71.
2. Chao EC. Core Evid. 2012;7:21-28.
GlomerulusDistal tubule
Collecting duct
Loop of
Henle
Proximal tubule
S3 segment of proximal tubule
• ~10% glucose reabsorbed
• Facilitated by SGLT1
S1 segment of proximal tubule
• ~90% glucose reabsorbed
• Facilitated by SGLT2
Glucosereabsorption
S3~10%
S1
~90%Glucosefiltration
(180 L/day) (1000 mg/L)=180 g/day
No/minimalglucose
excretion

SGLT2 Inhibitors: Mechanism of Action
GLU = facilitative glucose transporter. SGLT = sodium-dependent glucose transporter.Adapted from: Abdul-Ghani MA, et al. Endocr Pract 2008; 14(6):782-90. Bays H. Curr Med Res Opin 2009; 25(3):671-81. Wright EM. Am J Physiol Renal Physiol 2001; 280(1):F10-8. Lee YJ, et al. Kidney Int Suppl 2007; 106:S27-35. Han S, et al. Diabetes 2008 ; 57:1723-9.
Proximal tubuleS1
GlomerulusDistal tubule
Collecting duct
Glucosefiltration
S3
SGLT2 and GLUT2 SGLT1 and GLUT1
Increasedglucose
excretion
SGLT2 inhibitor
SGLT2 inhibition reduces renal glucose reabsorption and increases glucose elimination
Loop of Henle
Reduced glucosereabsorption

0
25
50
75
100
125
150
Healthy RTG
~10 mmol/L
0 2 4 6 8 10 12 14
Glucose Excretion (g/day)
Plasma glucose (mmol/L)
16
Above the RTG , glucosuria occurs
Under the RTG , no or minimal glucosuria occurs
Adaptationin patients
with diabetes
Under treatment with SGLT2 inhibitors
Effects of SGLT2 Inhibitors on RTG
RTG= Renal Threshold of Glucose

Targeting Hyperglycemia: Insulin-Dependent vs Insulin-Independent Approaches
Insulin action• TZDs• Metformin
Adipose Tissues
Muscles
Liver
Insulin release• Sulfonylureas• GLP-1R agonists• DPP-4 inhibitors• Meglitinides
Pancreas
Insulin-Dependent Mechanisms Insulin-Independent Mechanism
Insulin-independent renal SGLT2
Insulin replacement• Insulin

Osmotic diuresis• Initial weight loss2
• Decrease in blood pressure2
Loss of excess calories2,3
• Sustained weight loss2
• Mitigation of weight gain caused by antihyperglycemics of other classes2
Insulin-independent mechanism3
• Efficacy at all stages of the disease• Possibility of combination with
antihyperglycemics of other classes2
• Stable control in combination with insulin and insulin secretagogues2
Treatment with an SGLT2 Inhibitor: Clinical Benefits in T2DM
1. Holman RR, et al. N Engl J Med 2008; 359:1577-89. 2. Neumiller JJ. Drugs 2010; 70:377-85. 3. Lo MC, et al. Am J Ther 2013; 20(6):638-653.
Sustained glucose lowering• Potential prevention of
microvascular morbidity1
• Decrease in glucotoxicity2
SGLT2

-0.78 -0.8
-0.7
-0.85
-0.64
-1.03
-0.95
-0.79
-1.06
-0.72
0.14
-0.17
0.04
-0.13
0.01
-1.25
-1
-0.75
-0.5
-0.25
0
0.25
Mono + Met + SU + Met + SU + Insulin
Canagliflozin 100 mg/d Canagliflozin 300 mg/d Placebo
Baseline A1c 8.0% 7.9% 8.4% 8.1% 8.3%
A1
c %
mm
ol/
LCanagliflozin – Summary of Clinical Studies
A1c Reduced: 0.64 to 1.06% (0.63 to 1.17% PBO Corrected)
CANA: Adapted from: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/EndocrinologicandMetabolicDr
ugsAdvisoryCommittee/UCM336236.pdf. Accessed January 23, 2013

5.1 6.84.1
38.8
63.3
3.6
6.8
12.5
36.5
58.4
3.6 4.15.8
17.9
50.1
0
10
20
30
40
50
60
70
Mono + Met + SU + Met + SU + InsulinBaseline A1c 8.0% 7.9% 8.4% 8.1% 8.3%
Canagliflozin 100 mg/d Canagliflozin 300 mg/d Placebo
%
hyp
ogl
yce
mia
Canagliflozin – Summary of Clinical Studies
Rare Hypoglycemia Except When Combined with Secretagogues or Insulin
CANA: Adapted from: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/EndocrinologicandMetabolicDr
ugsAdvisoryCommittee/UCM336236.pdf. Accessed January 23, 2013

-2.7
-3.5
-0.6
-2.0
-1.5
-3.8 -3.9
-2.0
-2.6-2.4
-0.6
-1.0
-0.2
-0.7
-4
-3
-2
-1
0
1
-0.1
We
igh
t -
kg
Mono + Met + SU + Met + SU + Insulin
Baseline 86.8 kg 87.2 kg 83.0 kg 94.1 kg 97.0 kg
Canagliflozin – Summary of Clinical StudiesWeight Reduced by 0.6 to 3.9 kg (0.4-3.2 kg PBO Corrected)
CANA: Adapted from http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/EndocrinologicandMetabolicDr
ugsAdvisoryCommittee/UCM336236.pdf. Accessed January 23, 2013
Canagliflozin 100 mg/d Canagliflozin 300 mg/d Placebo

Mono + Met + SU + Met + SU + Insulin
Baseline SBP 127.7 128.2 136.2 130.5 137.8
Canagliflozin 100 mg/d Canagliflozin 300 mg/d Placebo
-3.3
-3.9-3.5
-3.7
-5.15.0 -5.1 -5.2
-4.3
-6.9
0.4
1.5
-3.4
-2.6 -2.5
-7
-6
-5
-4
-3
-2
-1
0
1
2
mm
Hg
Canagliflozin – Summary of Clinical StudiesSystolic BP Decreased by 3.3 - 6.9 mmHg (0.1-6.6 PBO Corrected)
CANA: Adapted from: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/EndocrinologicandMetabolicDr
ugsAdvisoryCommittee/UCM336236.pdf. Accessed January 23, 2013

A1c - Comparative DataCanagliflozin vs Sitagliptin in Triple Therapy MET + SU
Superior A1c reduction
observed with CANA
compared to SITA
Cana Sita% achieving A1c < 7.0% 47.6% 35.3%
Sita 100 mg
Cana 300 mg


Mean Change in FPG and PPG Canagliflozin vs Sitagliptin in Triple Therapy MET + SU
Schernthaner G, et al. Diabetes Care. 2013;36(9):2508-2515.

Weight - Comparative DataCanagliflozin vs Sitagliptin in Triple Therapy MET + SU
Schernthaner G, et al. Presentation 243. Presented at: The 48th Annual EASDMeeting, Oct. 2012.

Blood Pressure - Comparative DataCanagliflozin vs Sitagliptin in Triple Therapy MET + SU
Schernthaner G, et al. Presentation 243. Presented at: The 48th Annual EASD
Meeting, Oct. 2012.
* Statistical comparison for CANA 300 mg vs SITA 100 mg not performed (not pre-specified)†p < 0.001 vs PBO.mITT, LOCF

Pla
ceb
o-0
.23
10
mg
-0.8
9
5m
g-0
.77
*
Pla
ceb
o-0
.30
10
mg
-0.8
4
5m
g-0
.70
*
Pla
ceb
o-0
.13
10
mg
-0.8
2
5m
g-0
.63
*
Pla
ceb
o-0
.30
10
mg
-0.9
0
5m
g-0
.82
*
A1C Reductions Across Continuum of T2DM
= 0.6-1.1% from Baseline with Dapa and Cana
1. Ferrannini E, et al. Diabetes Care 2010; 33:2217-24. 2. Bailey CJ, et al. Lancet 2010; 375:2223-33. 3. Strojek K, et al. Diabetes Obes Metab 2011; 13:928-38. 4. Wilding JP, et al. Ann Intern Med. 2012 Mar 20;156(6):405-15. 5. INVOKANA Product Monograph. Janssen Inc., November 2014.
*p < 0.0001 vs. placebo. **p = 0.0005 vs. placebo. ***p < 0.001 vs. placebo.
Bargraph denotes individual trials and is not intended for comparisons between dapagliflozin and canagliflozin.
Ch
ange
fro
m
bas
elin
e A
1C
(%
)
0
-1.25
-0.25
0.25
Baseline A1C
Monotherapy1
7.92
Add-on to Ins4
8.53
Add-on to Glim3
8.11
Add-onto Met2
8.06
Dapagliflozin
Pla
ceb
o0
.14
30
0 m
g-1
.03
10
0 m
g-0
.78
Pla
ceb
o-0
.17
30
0 m
g-0
.77
10
0 m
g-0
.62
Pla
ceb
o0
.04
30
0 m
g-0
.83
10
0 m
g-0
.74
Pla
ceb
o-0
.13
30
0 m
g-1
.06
10
0 m
g-0
.85
Monotherapy
8.0
Add-on toMet + SU
8.1
Add-on to SU
8.4
Add-onto Met
7.9
Canagliflozin5
Pla
ceb
o0
.01
30
0 m
g-0
.72
10
0 m
g-0
.64
Add-on to Ins
8.3
-0.5
-0.75
-1.0 **
**
****
***
***
*** ******
***
***
***
***





Body Weight Reductions Across Continuum of T2DM = 1.0 - 3.9 kg from Baseline with Dapa and Cana
Pla
ceb
o-2
.19
10
mg
-3.1
6
5m
g-2
.8
NS
Pla
ceb
o-0
.89
10
mg
-2.8
6
5m
g-3
.04
*
Pla
ceb
o-0
.72
10
mg
-2.2
6
5m
g-1
.56
*
Pla
ceb
o0
.02
10
mg
-1.6
7
5m
g-0
.98
*Ch
ange
fro
m
bas
elin
e b
od
y w
eig
ht
(kg)
0
-4
-1
1.0
Baseline weight
24-wkmonotherapy1
90.2 kg
24-wk add-on to Ins4
93.8 kg
24-wk add-on
to Glim3
81.1 kg
24-wk add-on to Met2
88 kg
Dapagliflozin
Pla
ceb
o-0
.6
30
0 m
g-3
.9
10
0 m
g-2
.7
Pla
ceb
o-1
.2
30
0 m
g-4
.2
10
0 m
g-3
.7
Pla
ceb
o-0
.2
30
0 m
g-2
.0
10
0 m
g-0
.6
Pla
ceb
o-0
.7
30
0 m
g-2
.6
10
0 m
g-2
.1
Monotherapy
86.8 kg
Add-on toMet + SU
94.1 kg
Add-on to SU
83.0 kg
Add-onto Met
87.2 kg
Canagliflozin5
Pla
ceb
o-0
.0
30
0 m
g-2
.7
10
0 m
g-1
.9
Add-on to Ins
97.0 kg
-2
-3
1. Ferrannini E, et al. Diabetes Care 2010; 33:2217-24. 2. Bailey CJ, et al. Lancet 2010; 375:2223-33. 3. Strojek K, et al. Diabetes Obes Metab 2011; 13:928-38. 4. Wilding JP, et al. Ann Intern Med. 2012 Mar 20;156(6):405-15. 5. . INVOKANA Product Monograph. Janssen Inc., November 2014.
*p < 0.0001 vs. placebo. **p = 0.0091 vs. placebo. ***p < 0.001 vs. placebo. ****p < 0.05.
Bargraph denotes individual trials and is not intended for comparisons between dapagliflozin and canagliflozin.
*
**
*
***
***
***
***
***
***
***
***
****
NS
NS

Sustained Body Weight Reduction withAdd-on Dapagliflozin vs. Add-on Glipizide* in Patients Taking
Metformin (104 weeks)
*Glipizide is approved and authorized for use but is not marketed in Canada.Nauck M, et al. Diabetes Obes Metab 2014; 16(11):1111-20.
Week 104 weight
+1.36 kg (0.88, 1.84)
-3.70kg (-4.16, -3.24)
GLI + MET (n = 401)
DAPA + MET (n = 400)
0
400401
-5.0Ch
ange
in t
ota
l bo
dy
we
igh
t (k
g)
6 12 18
369361
26 34 42 52
323315
65 78 91 104
234211
-4.0
-3.0
-2.0
-1.0
2.0
3.0
Baseline weightDAPA + MET: 88.4 kgSulfonylrea + MET: 87.6 kg
-0.0
1.0
Between-group difference:
−5.06 kg (95% CI; −5.73, −4.4)
Sample size per time pointDAPA + METSU + MET

Placebo+ METN=79
Dapa10 mg + MET
N=82
Body Fat and Lean Mass (kg)at Week 24 by DXA (SE)
SGLT2 Inhibitors:
Predominant Fat Loss
DXA= Dual-energy X-ray Absorptiometry. ** Statistically significant vs. placebo by Hochberg’s method (p<0.001)
1. Toubro S et al. EASD Annual Meeting 2012. Poster 762.2. Bolinder J et al. J Clin Endocrinol Metab 2012;97:1020-1031.
Fat MassLean Mass
Canagliflozin1Dapagliflozin2
Body Fat and Lean Mass (kg)at Week 52 by DXA
CANA 100 mgN=71
GlimepirideN=68
CANA 300 mgN=69
1.0
1.3
-1.3
-2.5
-0.9
-2.9
1
-5
-3
3
-4
0
-1
-2
2
Ch
ange
fro
m B
ase
line
(kg
)
Fat MassLean Mass
-1.1
-0.6
1
-5
-3
3
-4
0
-1
-2
2
Ch
ange
fro
m B
ase
line
(kg
)
-2.22**
-0.74

Dapagliflozin Pooled Data: Genital Mycotic Infections
• More in women than men
• All events were mild to moderate in intensity
• Rarely led to discontinuation (0.2%)
• Most events responded to the initial course of standard therapy and rarely re-occurred
Pe
rce
nta
ge o
f su
bje
cts
wit
h c
linic
ald
iagn
osi
s o
f ge
nit
al in
fect
ion
MenWomenTotal
0.9
5.7
4.8
1.5
8.4
6.9
0.3
2.8 2.7
Johnsson KM, et al. J Diabetes Complications 2013; 27(5):479-84.
0
8
6
4
2
10
DAPA 5 mg
DAPA 10 mg
Placebo
Higher rates of GMI in dapagliflozin treatment groups than placebo

MenWomenTotal
DAPA 5 mg
DAPA 10 mg
Placebo
• More frequent in women than men
• All events were mild to moderate in intensity
• Rarely led to treatment discontinuation (0.3%)
• Most events responded to the initial course of standard therapy and rarely reccurred
Dapagliflozin Pooled Data: UTI
5.7
4.3
6.6
9.6
7.7
1.0
1.6
0.8
Johnsson KM, et al. J Diabetes Complications 2013; 27(5):473-8.
Pe
rce
nta
ge o
f su
bje
cts
wit
h
clin
ical
dia
gno
sis
of
UTI
0
8
6
4
2
12
10
3.7
Rates of clinically diagnosed UTI higher in the dapa groups than placeboUpper UTI were rare and balanced between groups

Volume-related AEs
• Polyuria dapagliflozin 10 mg (0.9%) vs. placebo (0.2%)
• Pollakiuria dapagliflozin 10 mg (2.1%) vs. placebo (0.7%)
• Rarely led to discontinuation from dapagliflozin
Johnsson et al. Presented at EASD 2014. Abstract 800-P.

Events of Volume Depletion with SGLT2 Inhibitors: Pooled Analyses
*Including dehydration, hypovolemia, or hypotension.
Serious events occurred in < 0.2% of patients and were comparable between groups.
Volume depletion AEAll
events*
Dapagliflozin 10 mg 0.8%
Dapagliflozin 5 mg 0.6%
Control 0.4%
INVOKANA Product Monograph. Janssen Inc., November 2014.FORXIGA Product Monograph. AstraZeneca. December 2014.
Volume depletion AEAll
events**
Canagliflozin 300 mg 1.3%
Canagliflozin 100 mg 1.2%
Control 1.1%
**Including postural dizziness, hypotension, orthostatic hypotension, dehydration and syncope.
• SGLT2 inhibitors not recommended for initiation in volume depleted patients.
• Temporary interruption of SGLT2 inhibitors is recommended for patients who develop volume depletion until the depletion is corrected.

Volume-related Adverse Effects: Which Patients Are More At Risk?
eGFR measured in mL/min/1.73m2
1. Johnsson et al. Presented at EASD 2014. Abstract 800-P.2. Adapted from: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/EndocrinologicandMetabolicDrugsAdvisoryCommittee/UCM336236.pdf. Accessed January 23, 2013.
Pat
ien
ts (
%)
0
8
6
4
2
10
DAPA 10 mg
Placebo
Dapagliflozin1
Yes
2.5
1.5
8.8
3.2
4.7
Yes
Loop diureticLoop diureticeGFR
≥30-<60
1.91.5
<60
8.1
4.7
eGFR
2.5
≥75<65
0.90.7
3.1
1.2
≥65
1.7
0.8
Age (years)
<75 ≥75
3.1
2.2
8.7
4.9
Age (years)
2.6
1.4
CANA 100
CANA 300
All non-cana
Canagliflozin2
Not intended for comparisons between trials

Efficacy of SGLT2 Inhibitors is Reduced
in Patients with Moderate Renal Impairment
1. Kohan D et al. Kidney Int. 2014;85: 962-971.2. Yale JF et al. Diabetes Obesity & Metabolism 2013;15:463-473.
*p < 0.001; †p <0.05
BL Mean A1C (%)BL Mean eGFR (mL/min/1.73m2)
LS m
ean
ch
ange
fro
m
bas
elin
e (
±9
5%
CI)
A1
C (
%)
0
-0.8
-0.2
-0.4
-0.6
0.2
Dapagliflozin ineGFR 30 to < 60 (N =
252)2
8.444.6
-0.32
-0.44
-0.11
8.039.4
Canagliflozin ineGFR 30 to < 50 (N = 269)1
-0.03
-0.33
-0.44
-0.30†
-0.40*
PlaceboCANA 100 mg CANA 300 mgDAPA 10 mgDAPA 5 mg
-0.41
-0.08

eGFR Changes in Normal Renal Function and in CKD
Weeks
Me
an c
han
ge f
rom
bas
elin
ee
GFR
(m
L/m
in/1
.73
m2)
10
-15
5
0
-5
-10
15
Baseline
Note: These are separate pooled analysis for Dapagliflozin and Canagliflozin.1. Ptaszynska, et al. Presented at EASD 2014. 2. Yale JF, et al. Presented at ADA 2013. Abstract 1075-P.
BL Mean eGFR (mL/min/1.73m2)
81.0
Dapagliflozin in normal eGFR1
80.7
841 10289766350372416
38.539.440.1
Canagliflozin in low eGFR2
eGFR decreases slightly at initiation of SGLT2 inhibitors, then returns slowly towards baseline

Canagliflozin Pooled Analysis: Hyperkalemia-related Endpoints
eGFR ≥ 60
PBO Cana 100
Cana 300
Mean % change from BL 0.5% 0.6% 1.0%
AE – blood K+ increased 0.2% 0.8% 0.7%
K+ level meeting outlier criteria* 4.7% 4.5% 6.8%
K+ level meeting outlier criteria*among patients on RAAS blockers or K-sparing diuretics
4.6% 5.1% 6.1%
*outlier criteria = potassium > 5.4 mmol/L with a > 15% increase from baseline
• In both populations, K+ elevations were usually < 6.5 mmol/L• Elevations ≥ 6.5 mmol/L were rare but more frequent in patients taking antihypertensive
agents that affect K+ excretion, in both the canagliflozin and placebo groups
Weir MR, et al. Curr Med Res Opin 2014; 30:1759-68.
eGFR ≥ 60 eGFR ≥ 45 and < 60
PBO Cana 100
Cana 300
PBO Cana 100
Cana 300
Mean % change from BL 0.5% 0.6% 1.0% 0.7% 1.7% 2.8%
AE – blood K+ increased 0.2% 0.8% 0.7% 1.5% 1.4% 2.1%
K+ level meeting outlier criteria* 4.7% 4.5% 6.8% 5.5% 5.2% 9.1%
K+ level meeting outlier criteria*among patients on RAAS blockers or K-sparing diuretics
4.6% 5.1% 6.1% 5.6% 4.9% 10.5%

Dapa: Changes in Lipids From Baseline
Hardy E, et al. Presented at ADA 2013. Poster 1188-P.
% c
han
ge f
rom
bas
elin
e (w
ith
95
% C
I)
8
-10
6
10
n =
4
2
0
BL mean =
Unit =
-2
-4
-6
-8
TC
989
5.04
mM
-0.4
834
5.06
mM
1.4
888
5.03
mM
1.1
838
0.56
mEq/L
-5.7
694
0.56
mEq/L
1.2
732
0.58
mEq/L
-0.5
984
2.12
mM
-0.7
831
2.19
mM
-5.4
886
2.15
mM
-3.2
985
2.96
mM
-1.9
828
2.95
mM
2.7
884
2.93
mM
0.6
990
1.15
mM
3.8
834
1.16
mM
5.5
889
1.16
mM
6.5
HDL-C LDL-C TG FFAs
Placebo (N = 1,393)DAPA 5 mg (N = 1,145) DAPA 10 mg (N = 1,193)

Bladder Cancer
• Across 22 clinical trials, newly diagnosed cases of bladder cancer were reported in 10/6,045 patients treated with dapagliflozin (0.17%) and 1/3,612 patient (0.03%) treated with placebo/comparator.
• Risk factors: 10/11 were male, 9/11 were > 55 years and 8/11 had smoking history.
• Pre-existing?
– 8/11 had hematuria at baseline
– 6/11 were diagnosed within 6 months of the start of treatment
PM: Dapagliflozin should not be used in patients with active bladder cancer and should be used with caution in patients with a prior history of bladder cancer.
DAPAGLIFLOZIN BMS-512148 NDA 202293. US Food & Drug Administration (FDA) Endocrinologic & Metabolic Drug Advisory Committee (EMDAC) Background Document. 2013. Available at: http://www.fda.gov/downloads/drugs/endocrinologicandmetabolicdrugsadvisorycommittee/ucm378079.pdf.FORXIGA Product Monograph. AstraZeneca. December 2014.


SGLT2 Inhibitors:Ongoing CV Outcome Trials
www.clinicaltrials.gov.
Treatment n Population Endpoints Results
CANVAS
Canagliflozin
vs.Placebo
4,363CVD or high risk for CVD
CV death, nonfatal MI or nonfatal CVA
June 2018
EMPA-REG
OUTCOMES
Empagliflozinvs.
Placebo7,000 CVD
CV death, nonfatal MI or nonfatal CVA
April
2015
DECLAREDapagliflozin
vs.Placebo
17,150CVD or high risk for CVD
CV death, nonfatal MI or nonfatal CVA
April 2019

EMPA-REG OUTCOMES: Trial design
• Study medication was given in addition to standard of care
– Glucose-lowering therapy was to remain unchanged for first 12 weeks
• Treatment assignment double masked
• The trial was to continue until at least 691 patients experienced an adjudicated primary outcome event
92
Randomised and treated(n=7020)
Empagliflozin 10 mg(n=2345)
Empagliflozin 25 mg (n=2342)
Placebo (n=2333)
Screening(n=11531)

93
EMPA-REG Outcome: n=7020 patients (mean age 63 years) with type 2 diabetes and established CVD. Median duration of follow-up: 3.1 years. Mean diff in A1C: 0.4% at wk 94. Mean diff in SBP 4 mm Hg.
EMPA-REG Outcome: Primary Composite
Endpoint CV Death, MI, or Stroke
CI: confidence interval; CV: cardiovascular; EMPA: empagliflozin; HR: hazard ratio; MI: myocardial infarction; PBO: placebo.
1. Zinman B et al. N Engl J Med. 2015;373:2117-28.
0
5
10
15
20
0 6 12 18 24 30 36 42 48
Placebo
Months
Pa
tie
nts
With
Eve
nt
(%)
Empagliflozin
PBO EMPA HRp
value
CV death, MI, stroke (%) 12.1 10.5 0.86 0.04
CV deaths (%) 5.9 3.7 0.62 <0.001
Nonfatal MI (%) 5.2 4.5 0.87 0.22
Nonfatal stroke (%) 2.6 3.2 1.24 0.16
Hosp. heart failure (%) 4.1 2.7 0.65 0.002
All-Cause mortality (%) 8.3 5.7 0.68 <0.001
4687
2333
4580
2256
4455
2194
4328
2112
3851
875
2821
1380
2359
1161
370
166
1534
741
No. of patients
Empagliflozin
Placebo
HR 0.86 (95% CI 0.74, 0.99)
p<0.001 for noninferiority
p=0.04 for superiority

4687
2333
4651
2303
4608
2280
4556
2243
4128
2012
3079
1503
2617
1281
414
177
1722
825
9
8
7
6
5
4
3
2
1
0
HR 0.62
(95% CI 0.49, 0.77)
p<0.001
Pa
tie
nts
With
Eve
nt (%
)
0 126 18 24 30 36 42 48
No. at riskMonths
Empagliflozin
Placebo
Placebo
Empagliflozin
Cumulative incidence function. HR: hazard ratio.
1. Zinman B et al. N Engl J Med. 2015;373:2117-28.
EMPA-REG Outcome: Death from CV cause
94

Patients with event/analysed
Empagliflozin Placebo HR (95% CI) p-value
3-point MACE490/468
7282/2333 0.86
(0.74, 0.99)*
0.0382
CV death 172/4687 137/2333 0.62(0.49, 0.77)
<0.0001
Non-fatal MI 213/4687 121/2333 0.87(0.70, 1.09)
0.2189
Non-fatal stroke 150/4687 60/2333 1.24(0.92, 1.67)
0.1638
0.25 0.50 1.00 2.00
EMPA-REG OUTCOMES: CV death, MI and stroke
Cox regression analysis. MACE, Major Adverse Cardiovascular Event; HR, hazard ratio; CV, cardiovascular; MI, myocardial infarction *95.02% CI95
Favours empagliflozin Favours placebo

• T2DM is associated with considerable CV risk• Some classes of antihyperglycemics are associated with off-target
effects (eg, weight gain, fluid retention, hypoglycemia) that may elevate CV risk• Other classes(e.g., GLP-1 RAs, SGLT2 inhibitors) have shown benefit on
those risk factors (eg, weight loss, BP reduction)
• CV safety studies in DPP-4 inhibitors have demonstrated CV neutrality, with perhaps a slight HF signal
• EMPA-REG, the first trial in the SGLT2 inhibitor class, reported a substantial reduction in CV mortality
• The first GLP-1 RA trial, with lixisenatide, showed CV neutrality• All CV safety studies have been conducted in high risk populations• A number of other GLP-1 RA CV safety trials (eg, LEADER) will be
reporting soon
Summary