Learning Objectives Managing Surgical Incisions at Risk for Post-Operative …Management.pdf ·...
17
Incision Management: The Final Step for Complex Surgical Procedures Faculty Allen Gabriel, MD, FACS Associate Professor of Surgery Loma Linda University Medical Center Loma Linda, California Peacehealth Southwest Medical Center Vancouver, Washington Devinder Singh, MD Associate Professor of Surgery University of Maryland School of Medicine Section Chief of Plastic Surgery VA Hospital – Baltimore Baltimore, Maryland Learning Objectives • Recognize the impact of surgical care complications as it relates to postoperative infections and identify patient populations at risk for surgical site compromise • Review considerations for steps to take when surgical site disruption occurs with the goal of achieving wound closure • Explore the role of incision management to reduce the risk of wound infection and dehiscence • Employ best practice protocols in preventing surgical site infections Devinder Singh, MD Associate Professor of Surgery University of Maryland School of Medicine Chief of Plastic Surgery, VA Hospital Baltimore Appointed Member, Maryland State Medical Board Baltimore, Maryland Managing Surgical Incisions at Risk for Post-Operative Complications Goals • Recognize the importance of infection control protocols for the prevention of SSIs • Identify patient populations at risk for surgical site compromise • Describe the appropriate use of NPWT on surgical sites to reduce the risk of wound infection and dehiscence • Employ early interventions to reduce the risk of readmissions for SSIs SSI = surgical site infection; NPWT = negative-pressure wound therapy. Skin Is Naturally under Tension • The natural tension from Langer lines cause incisional edges to retract • This internal tension within the skin opposes the closure of incisions • In regions of high movement and in obese patients, tension is increased and sutures or staples experience increased stress Med Art. http://www.med-ars.it/galleries/langer.htm. Accessed September 19, 2013.
Transcript of Learning Objectives Managing Surgical Incisions at Risk for Post-Operative …Management.pdf ·...

Incision Management: The Final Step for Complex
Surgical Procedures
Faculty
Allen Gabriel, MD, FACS Associate Professor of Surgery
Loma Linda University Medical Center Loma Linda, California
Peacehealth Southwest Medical Center Vancouver, Washington
Devinder Singh, MD
Associate Professor of Surgery University of Maryland School of Medicine
Section Chief of Plastic Surgery VA Hospital – Baltimore
Baltimore, Maryland
Learning Objectives
• Recognize the impact of surgical care complications as it relates to postoperative infections and identify patient populations at risk for surgical site compromise
• Review considerations for steps to take when surgical site disruption occurs with the goal of achieving wound closure
• Explore the role of incision management to reduce the risk of wound infection and dehiscence
• Employ best practice protocols in preventing surgical site infections
Devinder Singh, MD Associate Professor of Surgery
University of Maryland School of Medicine Chief of Plastic Surgery, VA Hospital Baltimore
Appointed Member, Maryland State Medical Board Baltimore, Maryland
Managing Surgical Incisions
at Risk for Post-Operative Complications
Goals
• Recognize the importance of infection control protocols for the prevention of SSIs
• Identify patient populations at risk for surgical site compromise
• Describe the appropriate use of NPWT on surgical sites to reduce the risk of wound infection and dehiscence
• Employ early interventions to reduce the risk of readmissions for SSIs
SSI = surgical site infection; NPWT = negative-pressure wound therapy.
Skin Is Naturally under Tension
• The natural tension from Langer lines cause incisional edges to retract
• This internal tension within the skin opposes the closure of incisions
• In regions of high movement and in obese patients, tension is increased and sutures or staples experience increased stress
Med Art. http://www.med-ars.it/galleries/langer.htm. Accessed September 19, 2013.

Closure Options
Standard Closure Techniques for Surgical Incisions
• Sutures
• Staples
• Tissue adhesives
• Tapes
• Combination of the above
Adjunctive Therapies used over Closure Techniques
• Gauze dressings
• Hydrocolloids
• Growth factors
• Cultured skin
• NPWT
Easterlin B, et al. Wounds. 2007;19(12):331-333. Steichen FM, et al. Br J Surg. 1973;60(3):191-197. Reece TB, et al. Am J Surg. 2001;182(2 suppl):40S-44S. Coulthard P, et al. Cochrane Database Syst Rev. 2010;5:CD004287. Atkinson JA, et al. Plast Reconstr Surg. 2005;116(6):1648-1656. Holm C, et al. Eur J Surg. 1998;164(3):179-183. Wu L, et al. Surgery. 1995;117(5):570-576. Veves A, et al. Diabetes Care. 2001;24(2):290-295. Ennis WJ, et al. Ostomy Wound Manage. 2005;51(8):24-39. Stannard JP, et al. J Trauma. 2006;60(6):1301-1306. Stannard JP, et al. J Orthop Trauma. 2012;26(1):37-42. Atkins BZ, et al. Surg Innov. 2009;16(2):140-146. Armstrong DG, et al. Lancet. 2005;366(9498):1704-1710. Blume PA. Diabetes Care. 2008;31(10):e77.
Risk Remains Elevated
• Despite advances in surgical technique and perioperative management, SSO/SSI continues to be a major source of morbidity and mortality
Finan KR, et al. Am J Surg. 2005;190(5):676-681. Dunne JR, et al. J Surg Res. 2003;111(1):78-84. Kaafarani HM, et al. J Surg Res. 2010;163(2):229-234. Houck JP, et al. Surg Gynecol Obstet. 1989;169 (5):397-399. Pauli EM, et al. Surg Infect (Larchmt). 2013;14(3):270-274.
Protocols for Lowering Risk
• Well-established, published guidelines by the CDC and National Institute for Health
– Preoperative hair removal with clippers
– Perioperative administration of intravenous antibiotics
– Surgical team antiseptic techniques
– Surgical techniques
– Pre- and post-operative glycemic control
– Oxygenation, normothermia
National Institutes for Health and Clinical Excellence. http://www.nice.org.uk/CG74. Accessed September 26, 2013. Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20:247–278.
High Risk?
High Risk? Risk Factors That May Compromise Healing
Riou JP, et al. Am J Surg. 1992;163(3):324-330. Wilson JA, et al. Adv Skin Wound Care. 2004;17(8):426-435. Abbas SM, et al. ANZ J Surg. 2009;79(4):247-250.
• Age >65 years
• Wound infection
• Pulmonary disease
• Peripheral vascular disease
• Hemodynamic instability
• Ostomies
• Hypoalbuminemia
• Systemic infection
• Obesity
• Uremia
• Hyperalimentation
• Ascites
• Malignancy
• Hypertension
• Length and depth of incision
• Anemia
• Jaundice
• Diabetes – poor control
• Nicotine use
• Type of injury
• Radiation therapy
• Steroid use
• Malnutrition

Prevalence of Hospital Acquired Infections
• CDC estimates of healthcare-associated infections – US – 1.7 million infections
– US – 99,000 deaths
• 17% to 22% are SSIs
• Patients with multiple comorbidities are at higher risk for surgical site complications
– Obesity
– Diabetes
– Smoking
– Poor vascularization
– Poor nutrition
Klevens RM, et al. Public Health Rep. 2007;122(2):160-166. National Nonsocomial Infections Surveillance (NNIA) Report. Am J Infec Control. 1996;24(5):380-388. Scott RD, II. http://www.cdc.gov/HAI/pdfs/hai/Scott_CostPaper.pdf. Accessed September 20, 2013. Riou JP, et al. Am J Surg. 1992;163(3):324-330. Wilson JA, et al. Adv Skin Wound Care. 2004;17(8):426-435. Abbas SM, et al. ANZ J Surg. 2009;79(4):247-250.
Economic Impact
• Wound complications following surgical procedures can be costly to the healthcare system
• SSIs have been associated with an increased hospital stays that are approximately 9.58 more days and incur an estimated $38,656 more in medical costs
• Postoperative dehiscence can add 9.42 extra days, resulting in additional charges of $40,323 in additional charges
Wong ES. Infect Control Hosp Epidemiol. 1999;20(11):722-724. Holtz TH, et al. Am J Infect Control. 1992;20(4):206-213. Klevens RM, et al. Public Health Rep. 2007;122(2):160-166. Zhan C, et al. JAMA. 2003;290(14):1868-1874.
Hospital Infections Now Cost Billions
• $9.8 billion in Hospital Acquired Infection
• JAMA Internal Medicine Sept 2, 2013
• TOP 5 drivers of cost – 33.7% SSI ($20,785 per case)
– 31.6% VAP ($40,144 per case)
– 18.9% CLABSI ($45,814 per case)
– 15.4% Cdiff ($11,285 per case)
– 1% CA-UTI ($896)
A Factor That Can Improve Healing
Review of Scientific and Clinical Evidence Supporting
NPWT over CLOSED incisions
What Is Incisional NPWT?
• Incision management system
• Different from a traditional open wound NPWT dressing

Prevena™ Incision Management System and Incisional NPWT
Indications • Prevena™
Incision Management System is specifically designed for use over clean, closed incisions that continue to drain
*Brand names are included for clarification purposes only. No product promotion should be inferred.
Incisional NPWT
• NPWT can also be used to manage clean, closed incisions, and when applied as incisional NPWT, it is functionally equivalent to Prevena™ Incision Management
How Does Incisional NPWT Work?
1. Removes fluid through the incisional interspaces that may otherwise percolate and work to break down the incision
2. Acts like a splint for the skin to help resist distracting forces on the incision line
3. Protects the incision from external contamination for the duration of therapy
Wilkes RP, et al. Surg Innov. 2012;19(1):67-75. Agarwal JP, et al. Plast Reconstr Surg. 2005;116(4): 1035-1040. Lessing MC, et al. Presented at: Wound Healing Society Annual Meeting 2011; April 14-17, 2011; Dallas, Texas. Atkins BZ, et al. Int Wound J. 2011;8(1):56-62. Kilpadi DV, et al. Wound Repair Regen. 2011;19(5):588-596.
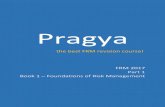
3D Finite Element Computer Modeling Showed Reduced Lateral Tension
Before Incisional NPWT With Incisional NPWT
Lateral tension around suture line was reduced by approximately 50%
Wilkes RP, et al. Surgical Innovations. 2012;19(1):67-75.
Immediate Impact Intermediate Term Impact Longer Term Impact
Bench Study of Appositional Forces
Bonded area of loading plate
Load Loading plate
Incision Sutures/staples
Dressing footprint
Load
Wilkes RP, et al. Surgical Innovations. 2012;19(1):67-75.
Immediate Impact Intermediate Term Impact Longer Term Impact
With Incisional NPWT Therapy: Suture line had 51% stronger approximation Staple line had 43% stronger approximation
Wilkes RP, et al. Surgical Innovations. 2012;19(1):67-75.
In This Bench Top Model, Appositional Forces Were Increased
Immediate Impact Intermediate Term Impact Longer Term Impact
80
60
120
100
40
20
0 Sutured Incision Stapled Incision
Forc
e (N
)
Without NPWT With NPWT
P < .05 P < .05
Force Required to Stretch Incision 10 mm

Data courtesy of Dr. Yaszay.
Porcine Incisions following 5 Days of Incisional NPWT
Immediate Impact Intermediate Term Impact Longer Term Impact
Incision following 5 days of treatment with incisional NPWT
Incision after 5 days
Data courtesy of Dr. Yaszay.
Immediate Impact Intermediate Term Impact Longer Term Impact
Porcine Incisions following 5 Days of Incisional NPWT
Improved Lymph Flow in a Porcine Model
27
Increased nanosphere accumulation in lymph nodes suggested incisional NPWT can help improve lymph flow
Kilpadi DV, et al. Wound Repair Regen. 2011;19(5):588-596.
Immediate Impact Intermediate Term Impact Longer Term Impact
160000 140000
200000 180000
120000 100000
60000
20000
80000
0
40000
30 nm 50 nm
Nan
osph
ere
Qua
ntity
(c
umul
ativ
e), n
g
Nanosphere Size
Incisional NPWT
Semi-Permeable Film Dressing
P = .0406 P = .0526
Nanospheres in Lymph Nodes
Lessing MC, et al. Presented at: Wound Healing Society Annual Meeting 2011; April 14-17, 2011; Dallas, Texas.
Immediate Impact Intermediate Term Impact Longer Term Impact
In a Porcine Study, Incision Apposition Was Increased
0.5
1.5
1.0
0 Superficial Dermis Deep Dermis
Inci
sion
Wid
th (m
m)
Standard of Care Incisional NPWT
N = 3 per group
Representative 40-Day Histology
Histology 40 Days
Clinical Experience Using Incisional NPWT
• Physicians reported use of NPWT over incisions as early as 2006
• Cardiothoracic
• Orthopedic
• Obstetrician/gynecologist
• Hernia
• Vascular
Cardiothoracic Procedures
Incident Rate of Surgical Site Complications and Use of NPWT Postsurgery

Cardiothoracic Surgical Site Complications
• CABG surgeries – 1081 CABG surgeries per million adults per year
• SSI after CABG is serious – Infection of the sternum
– Mediastinitis
– 50% mortality risk
CABG = coronary artery bypass graft. Epstein AJ, et al. JAMA. 2011;305(17):1769-1776. A.D.A.M Medical Encyclopedia. http://www.ncbi.nlm. nih.gov/pubmedhealth/PMH0001145/. Accessed September 20, 2013.
Postoperative CABG and mitral valve replacement via sternotomy on a 65-year-old male patient
Case Study: CABG through Median Sternotomy Incision
A. Day 0: Clean closed surgical incision
B. Day 0: Placement of incisional NPWT
C. Day 0: Application of -125 mm Hg pressure
D. Day 5: Surgical incision following removal
of incisional NPWT
Atkins BZ, et al. Int Wound J. 2011;8(1):56-62.
Retrospective Review
• Retrospective study of 20 adult male patients with clean, closed sternotomy incisions
– 10 NPWT; 10 control (standard dressings)
– The NPWT patients were classified as high risk; control patients were not
– Laser Doppler flowmetry measurements • When obtained after induction of anesthesia
and before surgical incision, there was no difference in baseline sternal perfusion
• When obtained daily after NPWT for a total of 4 days, the NPWT group had a 100±150% increase, where the control group dropped -12.7 ±70% (P=.004)
When the internal mammary artery was harvested for CABG, topical NPWT increased peristernal skin perfusion by 100%,
whereas controls perfusion decreased by 26% (P=.04)
Hernia
Case Study Presentation Intersecting Incisions

RECONSTRUCTIVE SURGERY
Incisional Negative-Pressure Wound Therapy versus ConventionalDressings Following Abdominal Wall Reconstruction
A Comparative Study
Alexandra Conde-Green, MD, FICS,* Thomas L. Chung, MD,* Luther Holton, III, MD,* Helen Hui-Chu, MD,*Yue Zhu, MD, MS,† Howard Wang, MD,‡ Hamid Zahiri, DO,† and Devinder P. Singh, MD*
Background: Improvements in surgical techniques have allowed us toachieve primary closure in a high percentage of large abdominal herniarepairs. However, postoperative wound complications remain common. Thebenefits of negative-pressure wound therapy (NPWT) in the management ofopen abdominal wounds are well described in the literature. Our studyinvestigates the effects of incisional NPWT after primary closure of theabdominal wall.Methods: A retrospective chart review was performed for the period be-tween September 2008 and May 2011 to analyze the outcomes of patientstreated postoperatively with incisional NPWT versus conventional dry gauzedressings. Patient information collected included history of abdominal sur-geries, smoking status, and body mass index. Postoperative complicationswere analyzed using !2 exact test and logistic regression analysis.Results: Fifty-six patients were included in this study; of them, 23 weretreated with incisional NPWT, whereas 33 received conventional dressings.The rates of overall wound complications in groups I and II were 22% and63.6%, respectively (P ! 0.020). The rates of skin dehiscence were 9% and39%, respectively (P ! 0.014). Both outcomes achieved statistical signifi-cance. Rates of infection, skin and fat necrosis, seroma, and hernia recur-rence were 4%, 9%, 0%, and 4% for group I and 6%, 18%, 12%, 9% forgroup II, respectively.Conclusions: This study suggests that incisional NPWT following abdom-inal wall reconstruction significantly improves rates of wound complicationand skin dehiscence when compared with conventional dressings. Prospec-tive, randomized, controlled studies are needed to further characterize thepotential benefits of this therapy on wound healing after abdominal wallreconstruction.
Key Words: incisional negative-pressure wound therapy, abdominal wallreconstruction, conventional dry gauze dressings, outcomes
(Ann Plast Surg 2012;68: 000–000)
Surgeons today are faced with an increasing number of patientswith complex and chronic wounds. This phenomenon is likely a
result of multiple factors. Patient demographic changes such as anaging population and increased prevalence of comorbidities lead todecreased wound healing. The increase in volume and complexity oftrauma, advances in surgery in general, and the stateside care of
international victims of armed conflict have all contributed to themounting complexity of wounds, which plastic surgeons are ex-pected to manage.1 One etiology of these wounds is the repair oflarge ventral hernia, the incidence of which has been on the risebecause of improved techniques and technology, which allows foroperations on higher-risk patients.2 High morbidity and prolongedrecovery time are associated with these complex wounds, and theneed for improved methods of management is apparent.
Many methods, including debriding agents, topical antimicro-bial dressings, and nonadherent dressings, have been used in aneffort to stimulate the proliferative phase of wound healing. How-ever, their use has demonstrated limited efficacy and resulted inminimal improvement.3 The advent of negative-pressure woundtherapy (NPWT) in the 1990s revolutionized acute and chronicwound management.4,5 NPWT acts by promoting a moist wound-healing environment and increasing granulation tissue, fluid evacu-ation, and angiogenesis. Recent studies on the application of subat-mospheric pressure directly on open abdominal wounds after largehernia repair have reported a decrease in wound complications andfaster recovery time.6 However, the use of NPWT on closed inci-sions is not as well characterized.
With advances in preoperative care and surgical techniques,primary wound closure is now often attainable after large herniarepair and complex abdominal wall reconstruction.7 Despite achiev-ing primary closure, management of these patients remains chal-lenging even for experienced surgeons because of the high rates ofpostoperative complications, such as seroma, surgical site infections,skin and fat necrosis, skin and fascial dehiscence, and herniarecurrence.8 Postoperative application of incisional NPWT along thelength of the closed abdominal incision is 1 approach we are takingto minimize complication rates of patients who underwent abdom-inal wall reconstructions. We hypothesized that the patients whowere treated with incisional NPWT would have fewer complicationsthan those who received conventional dry gauze dressings. There-fore, the aim of our study was to analyze and compare the compli-cation rates of these 2 cohorts of patients.
METHODS
Patient SelectionAfter approval by the institutional review board, a retrospec-
tive chart review of patients who underwent abdominal wall recon-struction by a single surgeon from the division of Plastic Surgery atthe University of Maryland Medical Center in Baltimore betweenSeptember 1, 2008 and May 31, 2011 was performed. The followinginclusion criteria were used: primary closure of the abdominalincision at the end of the operation, postoperative wound manage-ment with either NPWT or conventional dressings consisting ofgauze, and age "21 years. All 56 patients in the study presentedwith large ventral hernias. Patient demographics, diagnosis, historyof abdominal surgeries, smoking status, body mass index (BMI), andother comorbidities were noted. Postoperative complications such as
Received October 14, 2011, and accepted for publication, after revision January23, 2012.
From the *Division of Plastic Surgery, University of Maryland Medical Center,Baltimore, MD; †Department of Surgery, University of Maryland MedicalCenter, Baltimore, MD; and ‡University of Maryland Medical Center, Balti-more, MD.
Conflicts of interest and sources of funding: none declared.Reprints: Alexandra Conde-Green, MD, FICS, University of Maryland Medical
Center, Plastic Surgery Division, Room S8D18, 22 South Greene Street,Baltimore, MD 21201. E-mail: [email protected].
Copyright © 2012 by Lippincott Williams & WilkinsISSN: 0148-7043/12/6804-0001DOI: 10.1097/SAP.0b013e31824c9073
balt5/zps-aps/zps-aps/zps00412/zps6131-12z xppws S!1 2/17/12 5:08 4/Color Figure(s): F1-4 Art: SAP202506
Annals of Plastic Surgery • Volume 68, Number 4, April 2012 www.annalsplasticsurgery.com | 1
AQ:1
AQ:4AQ:5
"DOI: 10.1097/SAP.0b013e31824c9073#
RECONSTRUCTIVE SURGERY
Incisional Negative-Pressure Wound Therapy versus ConventionalDressings Following Abdominal Wall Reconstruction
A Comparative Study
Alexandra Conde-Green, MD, FICS,* Thomas L. Chung, MD,* Luther Holton, III, MD,* Helen Hui-Chu, MD,*Yue Zhu, MD, MS,† Howard Wang, MD,‡ Hamid Zahiri, DO,† and Devinder P. Singh, MD*
Background: Improvements in surgical techniques have allowed us toachieve primary closure in a high percentage of large abdominal herniarepairs. However, postoperative wound complications remain common. Thebenefits of negative-pressure wound therapy (NPWT) in the management ofopen abdominal wounds are well described in the literature. Our studyinvestigates the effects of incisional NPWT after primary closure of theabdominal wall.Methods: A retrospective chart review was performed for the period be-tween September 2008 and May 2011 to analyze the outcomes of patientstreated postoperatively with incisional NPWT versus conventional dry gauzedressings. Patient information collected included history of abdominal sur-geries, smoking status, and body mass index. Postoperative complicationswere analyzed using !2 exact test and logistic regression analysis.Results: Fifty-six patients were included in this study; of them, 23 weretreated with incisional NPWT, whereas 33 received conventional dressings.The rates of overall wound complications in groups I and II were 22% and63.6%, respectively (P ! 0.020). The rates of skin dehiscence were 9% and39%, respectively (P ! 0.014). Both outcomes achieved statistical signifi-cance. Rates of infection, skin and fat necrosis, seroma, and hernia recur-rence were 4%, 9%, 0%, and 4% for group I and 6%, 18%, 12%, 9% forgroup II, respectively.Conclusions: This study suggests that incisional NPWT following abdom-inal wall reconstruction significantly improves rates of wound complicationand skin dehiscence when compared with conventional dressings. Prospec-tive, randomized, controlled studies are needed to further characterize thepotential benefits of this therapy on wound healing after abdominal wallreconstruction.
Key Words: incisional negative-pressure wound therapy, abdominal wallreconstruction, conventional dry gauze dressings, outcomes
(Ann Plast Surg 2012;68: 000–000)
Surgeons today are faced with an increasing number of patientswith complex and chronic wounds. This phenomenon is likely a
result of multiple factors. Patient demographic changes such as anaging population and increased prevalence of comorbidities lead todecreased wound healing. The increase in volume and complexity oftrauma, advances in surgery in general, and the stateside care of
international victims of armed conflict have all contributed to themounting complexity of wounds, which plastic surgeons are ex-pected to manage.1 One etiology of these wounds is the repair oflarge ventral hernia, the incidence of which has been on the risebecause of improved techniques and technology, which allows foroperations on higher-risk patients.2 High morbidity and prolongedrecovery time are associated with these complex wounds, and theneed for improved methods of management is apparent.
Many methods, including debriding agents, topical antimicro-bial dressings, and nonadherent dressings, have been used in aneffort to stimulate the proliferative phase of wound healing. How-ever, their use has demonstrated limited efficacy and resulted inminimal improvement.3 The advent of negative-pressure woundtherapy (NPWT) in the 1990s revolutionized acute and chronicwound management.4,5 NPWT acts by promoting a moist wound-healing environment and increasing granulation tissue, fluid evacu-ation, and angiogenesis. Recent studies on the application of subat-mospheric pressure directly on open abdominal wounds after largehernia repair have reported a decrease in wound complications andfaster recovery time.6 However, the use of NPWT on closed inci-sions is not as well characterized.
With advances in preoperative care and surgical techniques,primary wound closure is now often attainable after large herniarepair and complex abdominal wall reconstruction.7 Despite achiev-ing primary closure, management of these patients remains chal-lenging even for experienced surgeons because of the high rates ofpostoperative complications, such as seroma, surgical site infections,skin and fat necrosis, skin and fascial dehiscence, and herniarecurrence.8 Postoperative application of incisional NPWT along thelength of the closed abdominal incision is 1 approach we are takingto minimize complication rates of patients who underwent abdom-inal wall reconstructions. We hypothesized that the patients whowere treated with incisional NPWT would have fewer complicationsthan those who received conventional dry gauze dressings. There-fore, the aim of our study was to analyze and compare the compli-cation rates of these 2 cohorts of patients.
METHODS
Patient SelectionAfter approval by the institutional review board, a retrospec-
tive chart review of patients who underwent abdominal wall recon-struction by a single surgeon from the division of Plastic Surgery atthe University of Maryland Medical Center in Baltimore betweenSeptember 1, 2008 and May 31, 2011 was performed. The followinginclusion criteria were used: primary closure of the abdominalincision at the end of the operation, postoperative wound manage-ment with either NPWT or conventional dressings consisting ofgauze, and age "21 years. All 56 patients in the study presentedwith large ventral hernias. Patient demographics, diagnosis, historyof abdominal surgeries, smoking status, body mass index (BMI), andother comorbidities were noted. Postoperative complications such as
Received October 14, 2011, and accepted for publication, after revision January23, 2012.
From the *Division of Plastic Surgery, University of Maryland Medical Center,Baltimore, MD; †Department of Surgery, University of Maryland MedicalCenter, Baltimore, MD; and ‡University of Maryland Medical Center, Balti-more, MD.
Conflicts of interest and sources of funding: none declared.Reprints: Alexandra Conde-Green, MD, FICS, University of Maryland Medical
Center, Plastic Surgery Division, Room S8D18, 22 South Greene Street,Baltimore, MD 21201. E-mail: [email protected].
Copyright © 2012 by Lippincott Williams & WilkinsISSN: 0148-7043/12/6804-0001DOI: 10.1097/SAP.0b013e31824c9073
balt5/zps-aps/zps-aps/zps00412/zps6131-12z xppws S!1 2/17/12 5:08 4/Color Figure(s): F1-4 Art: SAP202506
Annals of Plastic Surgery • Volume 68, Number 4, April 2012 www.annalsplasticsurgery.com | 1
AQ:1
AQ:4AQ:5
"DOI: 10.1097/SAP.0b013e31824c9073#
pulmonary disease (4.6%), coronary artery disease (10.8%), andtaking immunosuppression drugs (3.1%). Forty percent of patientspresented with an initial diagnosis of ventral hernia, 58.5% withrecurrent ventral hernia, and 1.5% with incarcerated recurrent ven-tral hernia. There were no significant differences between the 2groups with regards to preoperative comorbidities.
The mean follow-up period of these patients was 15 months(range, 4 months–3 years). In group I, 22% (5 of 23) of the patientsdeveloped wound complications overall (comprising skin dehis-cence, skin/fat necrosis, infection), compared with 63.6% (21 of 33)in group II. Two patients of the 23 (9%) presented with skin
dehiscence in group I, whereas 13 of the 33 (39%) in group IIexperienced skin dehiscence. These 2 differences were statisticallysignificant (P ! 0.020 and P ! 0.014, respectively). These datashow that the patients treated with conventional dressings ingroup II were more prone (6.3 times more) to develop woundcomplications than those treated with incisional NPWT in groupI (odds ratio ! 6.3 with 95% confidence interval ! 1.37–34.14).Also patients in group II were 6.83 times more likely to have skindehiscence than patients in group I (odds ratio ! 6.83 with 95%confidence interval ! 1.37–34.14) (Table 2).
The rates of skin and fat necrosis, hernia recurrence, seroma,infection, and hematoma were 9%, 4%, 0%, 4%, 0% for group I and18%, 9%, 12%, 6%, 0% for group II, respectively. The differencesin these variables between the 2 groups trended toward significancebut did not achieve it (Fig. 4).
DISCUSSIONThe benefits of NPWT on wound healing in the management
of complex open wounds after reconstructive procedures have beenwell described. Since the introduction of this therapy delivered by aportable and practical device in the 1990s, the landscape of acuteand chronic wounds management has been drastically altered.NPWT, which functions by applying negative pressure to a sealed,airtight wound, has been shown to promote a moist wound-healingenvironment, reduce bacterial colony counts, increase granulationformation, remove edema, stimulate cell-mediated immune re-sponse, decrease the permeability of blood vessels, and stimulateangiogenesis and blood flow to the wound margins.9–11 Two broadmechanisms are proposed to account for the accelerated rates ofwound healing: a fluid-based mechanism with the removal of ex-cessive interstitial fluid and toxic inflammatory mediators and amechanism consisting of microdeformation at the wound surfaceand drawing of the surrounding skin together causing the release ofgrowth factors, similar to the effects from tissue expansion.12
NPWT is now used in almost every surgical discipline because ofthe versatility and the dramatic improvements in wound healing seenwith this device. This technology has been rapidly introduced into awide array of conditions, such as burns, pressure ulcers, open
TABLE 1. Preoperative Factors of Patients Treated WithIncisional NPWT and Conventional Dressings
IncisionalNPWT (Mean)
ConventionalDressings (Mean)
Age 54 55Prior abdominal surgery 2 2.3BMI 36.4 36.1
TABLE 2. No. Postoperative Complications in PatientsTreated With Incisional NPWT and Conventional Dressings
IncisionNPWT
(n ! 23)
ConventionalDressings(n ! 33) P
OddsRatio
Wound complications 5 21 0.020* 6.3Skin dehiscence 2 13 0.014* 6.83Skin/fat necrosis 2 6 0.45 —Infection 1 2 — —Hernia recurrence 1 3 0.63 —Seroma 0 4 0.14 —Hematoma 0 0 — —
*P " 0.05.
FIGURE 4. Percentage of postoper-ative complications in group I: pa-tients treated with incisional NPWTand group II: patients treated withconventional dry gauze dressings.
balt5/zps-aps/zps-aps/zps00412/zps6131-12z xppws S!1 2/17/12 5:08 4/Color Figure(s): F1-4 Art: SAP202506
Annals of Plastic Surgery • Volume 68, Number 4, April 2012 NPWT versus Conventional Dressings
© 2012 Lippincott Williams & Wilkins www.annalsplasticsurgery.com | 3
AQ:3
T2
F4
Retrospective Chart Review Results
*Statistical significance; P < .05. Condé-Green A, et al. Ann Plast Surg. 2013;71(4):394-397.
Group I Incisional NPWT (n=23)
Group II Conventional Dressings (n=33)
10
70
30
0 Wound
Complications
Po
stop
erat
ive
Com
plic
atio
ns (%
)
20
50
40
60
*
*
Skin Dehicence
Skin/Fat Necrosis
Seroma Hernia Recurrence
Infection
Retrospective Review of Incisional NPWT in High-Risk Abdominal Wound Closures
• 30 patients treated with nonadhering dressing plus NPWT for 5 to 7 days • 30 patients with standard care (retrospective) • Wound complications
– NPWT: 3% – Control: 20%
Vargo D. Abstract presented at 2012 Southwestern Surgical Conference. March 26, 2012.
15
10
25
20
5
0 NPWT Control
P < .05
%
Wound Complications
Perfusion Analysis with ICG Angiography
Average absolute 116 Average absolute 83
P = .003
ICG = indocyanine green.
Perfusion Analysis with ICG Angiography (cont’d)
Orthopedic Procedures
Incident Rate of Surgical Site Complications and Use of NPWT Postsurgery

Orthopedic Trauma Surgical Site Complications
• Stabilizing the bone
• Boney fragments within the wound
• 33% to 50% potential infection rates
• Osteomyelitis
Stannard JP, et al. J Trauma. 2006;60(6):1301-1306.
Case Study: Right Total Hip Arthoplasty
A. Day 0: Clean closed surgical incision
B. Day 0: Application of incisional NPWT
C. Day 5: Surgical incision following removal
of incisional NPWT Dressing
Postoperative right total hip arthroplasty on a 71-year-old female patient
Randomized Controlled Trial of Incisional NPWT after Lower Extremity Fractures
• Incisional NPWT vs standard postoperative dressings (control) for patients with calcaneus, pilon, and tibial plateau fractures
• 141 incisional NPWT patients vs 122 control patients
Stannard JP, et al. J Orthop Trauma. 2012;26(1):37-42.
Randomized Controlled Trial Results
Stannard JP, et al. J Orthop Trauma. 2012;26(1):37-42.
Incisional NPWT Control P Value
Number 141 122
Infection 14 24 < .02
Dehiscence 12 21 < .03
Vascular Procedures
Incident Rate of Surgical Site Complications Use of NPWT Postsurgery
Groin Incision Complications
Potential complications • Massive hemorrhage
• Systemic sepsis
• Severe limb ischemia
• Septic embolization
Atnip RG. Surgery. 1991;110(1):106-108. Patel KR, et al. J Vasc Surg. 1988;8(3):321-328.

• Incidence of SSI at the groin after vascular procedures can be as high as 44%
• Morbidity associated with groin infection includes limb loss, sepsis, increased LOS, and increased mortality
From the Society for Vascular Surgery
Experience with a new negative pressure incisionmanagement system in prevention of groin woundinfection in vascular surgery patientsTim Matatov, MD,a Kaavya N. Reddy, MD,a Linda D. Doucet, RN,a Cynthia X. Zhao, MD, MPH,b andWayne W. Zhang, MD,a Shreveport, La
Objective: Groin wound infection is an important cause of postoperative morbidity in vascular surgery patients, especiallywhen prosthetic grafts are involved. The objective of this study was to investigate if Prevena (Kinetic Concepts, Inc, SanAntonio, Tex), a negative pressure incision management system, could reduce the risk of groin wound infection inpatients after vascular surgery.Methods: Ninety patients (115 groin incisions) underwent longitudinal or transverse femoral cutdown for vascularprocedures. A retrospective chart review was performed on 63 consecutive incisions in patients in the non-Prevena groupfrom December 2009 to November 2010 and on 52 consecutive incisions in patients in the Prevena group from January2011 to December 2011. Prevena was applied intraoperatively and removed 5 to 7 days postoperatively. The non-Prevenagroup received either a skin adhesive or absorbent dressing. Groin incisions were assessed, and infection was gradedbased on Szilagyi classifications. Student t-test and two-sample proportion z test were used for statistical analyses.A P value < .05 was considered statistically significant.Results: Comorbidities and known risk factors for infection were compared; there were no statistically significantdifferences between the two groups. Prosthetic material was used in 34 (65%) incisions in the Prevena group and 29 (46%)incisions in the non-Prevena group. Fifty (96%) incisions within the Prevena group and 60 (96%) in the non-Prevenagroup were classified as clean surgical wounds. Wounds were evaluated at 7 days and 30 days postoperatively. Of63 groin incisions in 49 patients in the non-Prevena group, 19 (30%) incisions had groin wound infections. Woundinfections were classified into Szilagyi grade I (10; 16%), Szilagyi grade II (7; 11%), and Szilagyi grade III (2; 3%). Of52 groin incisions in 41 patients in the Prevena group, three (6%) incisions had Szilagyi grade I wound infections. Nograde II or III infections occurred in this group. Overall incidence of infection between the two groups was statisticallysignificant (P [ .0011).Conclusions: In this clinical study, Prevena negative pressure dressing significantly decreased the incidence of groin woundinfection in patients after vascular surgery. (J Vasc Surg 2013;57:791-5.)
The incidence of surgical site infections (SSIs) at thegroin after vascular procedures is 3% to 44%.1-8 This re-ported incidence is up to five times higher than theexpected incidence of infection in clean cases as predictedby the U.S. Centers for Disease Control and PreventionNational Nosocomial Infections Surveillance System.9
Factors contributing to increased incidence of SSIs in thissubset of patients include disruption of lymphatics, prox-imity of the groin to the perineum, and prosthetic graftplacement.1,10 Morbidity associated with infection includeslimb loss, sepsis, prolonged hospital stay, and increased
mortality. There is no “gold standard” for treatment ofthese infections. Multiple treatment modalities have beenattempted with limited success and increased health carecosts, including rotational flaps, wound vacuum-assistedclosure, and excision of prostheses with extra-anatomicbypass. Standard infection prevention measures such aspreoperative antibiotics have significantly decreased SSIs.However, even when combined with other preventivetechniques, such as oblique incisions, use of antibiotic-impregnated grafts, meticulous wound closure, and closedsuction drain placement, wound infection rates in thissubset of patients remain substantially higher than theaccepted norm for clean cases.7,11 Because most bacterialinfections occur from direct spread of bacteria from thewound, prevention must be given just as much importanceas treatment.11 The aim of this study was to investigate ifa new negative pressure incision management system,Prevena (Kinetic Concepts, Inc, San Antonio, Tex), couldreduce the incidence of groin wound infections aftervascular surgery.
METHODS
This study was approved by institutional reviewcommittee at Louisiana State University Health Sciences
From the Division of Vascular and Endovascular Surgery, Department ofSurgerya and Department of Pathology,b Louisiana State UniversityHealth Sciences Center.
Author conflict of interest: none.Presented at the 2012 Vascular Annual Meeting of the Society for Vascular
Surgery, National Harbor, Md, June 7-9, 2012.Reprint requests: Wayne W. Zhang, MD, Louisiana State University Health
Sciences Center, 1501 Kings Highway, PO Box 33932, Shreveport,LA 71130 (e-mail: [email protected]).
The editors and reviewers of this article have no relevant financial relationshipsto disclose per the JVS policy that requires reviewers to decline review of anymanuscript for which they may have a conflict of interest.
0741-5214/$36.00Copyright ! 2013 by the Society for Vascular Surgery.http://dx.doi.org/10.1016/j.jvs.2012.09.037
791
Matatov T, et al. J Vasc Surg. 2013;57(3):791-795.
Groin Incisions
CentereShreveport, and informed consent was waived. Weretrospectively studied the charts of 90 consecutive patients(115 groin incisions) who underwent femoral cutdown forvascular procedures. The patient population was dividedinto a “Prevena group” and a “non-Prevena group.”From December 2009 to November 2010, 63 consecutiveincisions in the non-Prevena group were reviewed, and 52consecutive incisions were reviewed in the Prevena groupfrom January 2011 to December 2011. In the non-Prevena group, skin was covered using Primapore (Smith& Nephew UK, London, UK), which was removed 3days postoperatively, or Dermabond Adhesive (EthiconInc, Somerville, NJ). In the Prevena group, Prevena wasapplied intraoperatively under sterile conditions (Fig) andremoved 5 to 7 days postoperatively. Patients underwentpreoperative hair clipping and were prepared with iodo-phor (DuraPrep; 3M, St. Paul, Minn) or povidone-iodine(Betadine; Purdue Products L.P., Stamford, Conn) forpre-existing open wounds or chlorhexidine in iodine-allergic patients. Patients received cefazolin, or clindamycinif allergic to penicillin, 30 minutes before incisions. In thepatients who had been receiving antibiotics for lowerextremity open wound infection or sepsis at the time ofthe vascular procedure, therapeutic antibiotic doses weregiven again within 1 hour of skin incision. The orientationof the incision was based on the site of vascular access. Allincisions were reapproximated in three layers of runningpolyglactin 910 suture (Vicryl; Ethicon Inc, Somerville,NJ) for subcutaneous tissue, and skin was closed in a subcu-ticular fashion with poliglecaprone 25 (Monocryl; EthiconInc). After closure, incisions and surrounding skin wereclean and dried with sterile gauzes. The Prevena dressingwas placed by covering the incision with the foam bolsterin the center and then surrounding adhesive dressing tointact skin. Negative pressure was applied, and a completeseal was confirmed.
Attending physicians evaluated wound appearance onpostoperative day 5 to 7 and at 1-month follow-up orsooner if patients presented with symptoms or signs ofwound infection (mean follow-up was 7 days and 33 daysin the Prevena group and 10 days and 40 days in thenon-Prevena group). Groin wound infection in bothgroups was graded according to the Szilagyi gradingsystem. Incidences of infection with different grades wererecorded and analyzed.
All patients who underwent longitudinal or transverseincisions for groin cutdown were eligible for inclusion inthis study. Patients who could not have Prevena placedbecause of the inability to obtain a seal were excluded.Two morbidly obese patients were excluded becausea complete seal with Prevena dressing could not beachieved owing to the patients’ giant pannus.
Szilagyi classification was used to describe SSIs.12 GradeI infections had only dermal involvement. Grade II infec-tions extended to the subcutaneous region but did notinvolve the arterial graft. Infection that involved the arterialgraft was grade III. If a patient presented initially witha lower grade of infection but then developed a higher grade
because of failure of medical or surgical treatment, thepatient was placed into the higher category. Localized infec-tion was defined as acute or chronic ipsilateral lowerextremity infection occurring before vascular surgery. Renalinsufficiency was defined as glomerular filtration rate <50,and anemia was defined as hemoglobin <12 g/dL.
Student t-test and two-sample proportion z test wereused for statistical analyses. A P value < .05 was consideredstatistically significant.
RESULTS
Comorbidities such as diabetes and coronary arterydisease and other known risk factors for infection such ascigarette smoking and body mass index were comparedbetween the two groups, and there was no statisticallysignificant difference (Table I). No patients required hemo-dialysis or peritoneal dialysis. Prosthetic material was usedin 34 incisions (65%) in the Prevena group and 29 incisions(46%) in the non-Prevena group. Prosthetic material wassubdivided further into polytetrafluoroethylene or polyeth-ylene terephthalate (Dacron) (Table II). In the Prevenagroup, 40 incisions (77%) were longitudinal, and 12 inci-sions (23%) were transverse. In the non-Prevena group,47 incisions (75%) were longitudinal, and 16 incisions(25%) were transverse. There was no statistically significantdifference in the incision types of longitudinal vs transversebetween the two groups. Of the 22 infected incisions inboth groups, 16 incisions were longitudinal and six weretransverse.
Groin exposure was performed for revascularization,endovascular, or other vascular procedures (Table II).The number of patients with a history of revascularizationor amputation was greater in the Prevena group (17; 41%)compared with the non-Provena group (12; 24%), but thiswas not statistically significant (P ¼ .0844). The presenceof a localized or systemic infection at the time of operationwas not statistically significant between the two groups.Perioperative risk factors were compared as well
Fig. Intraoperative application of Prevena negative pressuredressing after femoral-femoral bypass.
JOURNAL OF VASCULAR SURGERY792 Matatov et al March 2013
Matatov T, et al. J Vasc Surg. 2013;57(3):791-795.
Intraoperative application of incisional NPWT dressing after femoral-femoral bypass
Results
Prevena Group
Non-Prevena Group P Value
Szilagyi I 3 (6%) 10 (16%)
Szilagyi II 0 7 (11%)
Szilagyi III 0 2 (3%)
Overall infection 3 (6%) 19 (30%) .0011
Matatov T, et al. J Vasc Surg. 2013;57(3):791-795.
Incidence and Szilagyi Grades of Infection Based on Total Number of Incisions
Another Case Study
Massive Localized Lymphedema

Results
Observations
• Mechanical stabilization (immediate reduced lateral tension/increased appositional strength)
• Physical protection of wound
• Early increase in wound-breaking strength
• Narrower zone of scar histologically
• Reduction in edema
• Increased blood flow
• Suggested increase in lymph flow
• Reduction in hematoma/seroma
Wilkes RP, et al. Surg Innov. 2012;19(1):67-75. Agarwal JP, et al. Plast Reconstr Surg. 2005;116(4): 1035-1040. Lessing MC, et al. Presented at: Wound Healing Society Annual Meeting 2011; April 14-17, 2011; Dallas, Texas. Atkins BZ, et al. Int Wound J. 2011;8(1):56-62. Kilpadi DV, et al. Wound Repair Regen. 2011;19(5):588-596.
Summary
Progression from models, bench, histology, animal, clinical, retrospective, and prospective science

Allen Gabriel, MD, FACS Department of Plastic Surgery
Peacehealth Southwest Medical Center Vancouver, Washington
Loma Linda University Medical Center Loma Linda, California
Managing Surgical Incisions
at Risk for Post-Operative Complications Clinical Cases
NOTE: As with any case study, the results and outcomes experienced by the following patients should not be interpreted as a guarantee
or warranty of similar results. Individual results may vary depending on the patient’s circumstances and condition.
Case 1 Chest Defect
Tight Closure of Donor Site

Tight Closure of Donor Site
Flap on Chest Wall Application of Incisional NPWT
Post Dressing Removal POD #7 Follow-up at POD 24

Case 2

Case Study
• We report on postoperative outcomes with a customizable dressing over closed incisions in 13 patients who received immediate postoperative breast reconstruction.
Patient Demographics
Category N = 13 Number of Breasts 25 Average age (range) 44.72 years (27-62 years) Gender Male (%) 0 (0%) Female (%) 13 (100%) Average BMI (range) 29.36 (20-44) Comorbidities Preoperative chemotherapy 2 Obesity 4 Axillary dissection 1 Diabetes mellitus 1 None 9
Results Surgical Incision Management
Mastectomy Type
Average Number of Days with Surgical
Incision Management (range)
Average Number of
Days with Drain (range)
Reduction pattern 4.33 (3-5) 8.50 (7-12
Nipple sparing 4.71 (3-5) 7.93 (6-10)
Skin sparing 3.00 (3) 8.60 (8-9)
Total for all patients 4.28 (3-5) 8.20 (6-12)
Use of Capsular Incision in Normal Prostatic Tissue (ciNPT)?
Closed incisions • Primary use
– To avoid SSI
• Secondary use – To avoid SSI
Case 3
Necrotizing fasciitis following tubal ligation
POD 1 following debridement

Application of Incisional NPWT
3 weeks Post Delayed Primary Closure
4 months Post Delayed Primary Closure
Case 4

Contraindications
• Necrotic tissue with eschar
• Untreated osteomyelitis
• Malignancy in the wound
• Exposed blood vessels organs or nerves
• Non-enteric or unexplored fistulas
Where Does ciNPT Fit in My Practice?
• Closed incisions – At risk for seroma formation
• Large undermining
• High BMI
• Use of biologics/synthetics
– At risk for dehiscence • Tight closure
• Repeated incisions through the same scar
• Risk factors:
– DM, high BMI , smoker, h/o radiation, soiling, immunosuppressed

Conclusion
Improved surgical outcomes in the high risk group of patients can be achieved
with the addition of NPWT when well-planned and executed operative procedures
are carried out based on sound surgical principles
NPWT NPWT instillation
ciNPT
Thank You