Laurie Fouser, MD Pediatric Nephrology Swedish Pediatric ...
30
Hematuria and Proteinuria in the Pediatric Patient Laurie Fouser, MD Pediatric Nephrology Swedish Pediatric Specialty Care
Transcript of Laurie Fouser, MD Pediatric Nephrology Swedish Pediatric ...

Hematuria and Proteinuria in the Pediatric Patient
Laurie Fouser, MD Pediatric Nephrology
Swedish Pediatric Specialty Care

Hematuria in the Child
• Definition • ³ 1+ on dipstick on three urines over three weeks • 5 RBCs/hpf on three fresh urines over three weeks
• Prevalence • 4-6% for microscopic hematuria on a single
specimen in school age children • 0.3-0.5% on repeated specimens

Sources of Hematuria
• Glomerular or “Upper Tract” – Dysmorphic RBCs and RBC casts – Tea or cola colored urine – Proteinuria, WBC casts, renal tubular cells
• Non-Glomerular or “Lower Tract” – RBCs have normal morphology – Clots/ Bright red or pink urine

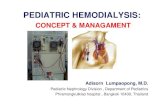
The Glomerular Capillary Wall

The Glomerular Capillary Wall

Glomerular Causes of Hematuria
• Benign or self-limiting – Benign Familial Hematuria – Exercise-Induced Hematuria – Fever-Induced Hematuria

Glomerular Causes of Hematuria
• Acute Glomerular Disease – Poststreptococcal/ Postinfectious – Henoch-Schönlein Purpura – Sickle Cell Disease – Hemolytic Uremic Syndrome

Glomerular Causes of Hematuria
• Chronic Glomerular Disease – IgA Nephropathy – Henoch-Schönlein Purpura or other Vasculitis – Alport Syndrome – SLE or other Collagen Vascular Disease – Proliferative Glomerulonephritis

Non-Glomerular Hematuria
• Extra-Renal • UTI • Benign urethralgia +/- meatal stenosis • Calculus • Vesicoureteral Reflux, Hydronephrosis • Foreign body • Rhabdomyosarcoma • AVM • Coagulation disorder

Non-Glomerular Hematuria
• Intra-Renal • Hypercalciuria • Polycystic Kidney Disease • Reflux Nephropathy with Renal Dysplasia • Sickle Cell Crisis • Renal Vein Thrombosis • Renal Hemangioma • Tumor or Leukemia • Nutcracker syndrome/Loin Pain Hematuria

Evaluation – Phase I
• Complete History – Duration, color, discrete clots vs diffuse? – In males, change during stream? – Pain or painless (dysuria, abdominal, flank) – Recent or current infection? – Rashes, joint, or GI symptoms?

Evaluation – Phase I
• Complete Physical – Blood pressure – Volume status (“dry or wet”, rales, gallop) – Edema (periorbital, pretibial, ascites) – Rash

Urinalysis with Microscopy

Evaluation - Phase I
• Complete H&P • Urinalysis with microscopy • Urine culture • Urine calcium: urine creatinine ratio • CBC with platelets (+/-Sickle prep), BUN,
Creatinine, albumin, C3 • Ultrasound of kidneys and bladder • Urine dipsticks on parents and siblings

Evaluation - Phase II
• C3, C4, ANA, Hepatitis B & C • Streptozyme • BUN, creatinine, electrolytes, albumin,
calcium, phosphorus • Hearing evaluation • VCUG or CT

Evaluation - Phase III
• Other laboratory
• Renal biopsy
• Cystoscopy

When to Refer • Family history of kidney disease • Gross hematuria or clots • RBC casts • Proteinuria ³ 1+ • Elevated creatinine or BUN • Hypertension • Imaging abnormalities • Parental anxiety

Proteinuria in the Child

Proteinuria
• Definition – 1+ or more on dipstick – Urine protein:creatinine
• >0.2 mg/mg if over 2 yrs • >0.6 mg/mg ages 6 months-
2yrs • Nephrotic range is >2 mg/mg
– Timed urine protein excretion
• >96 mg/m2/24 hrs • >150 mg/1.73m2/24hrs • Nephrotic range is >3
gm/1.73m2/24 hrs

Causes of Proteinuria
• Physiologic or Intermittent • Postural or Orthostatic • Pathologic
– Glomerular – Tubular

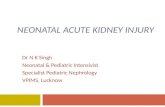
Glomerular Permeability Barrier

Physiologic or Intermittent Proteinuria
• Mechanism is change in glomerular capillary wall permeability – Increased luminal
hydrostatic pressure – Increased blood
flow
• Causes – Acute elevations in BP
or intraglomerular volume
– Catecholamines/stress – Metabolism

Physiologic or Intermittent Proteinuria
• Clinical Settings – Fever – Physical stress (march
proteinuria) – Pregnancy – Immediately post op
unilateral nephrectomy – Acute hypertension or
CHF
• Duration – Transient (hours-
days) – Self-remitting – No need for referral

Postural or Orthostatic Proteinuria
• Two patterns – Fixed, reproducible (15-20%) – Transient (75-80%)
• Accounts for 60% of children and 75% of adolescents with proteinuria
• Incidence – 2-5% of adolescents • MUST DISTINGUISH FROM PATHOLOGIC
PROTEINURIA WITH A POSTURAL COMPONENT

Postural or Orthostatic Proteinuria
• Evaluation:
– Blood pressure, edema should not be present, UA/UC
– First am void for urine protein:creatinine (patient must be sure to go to bed with empty bladder)
• If <0.2 mg/mg, likely orthostatic – Normal renal function panel and renal
ultrasound

Postural or Orthostatic Proteinuria
• Protein in 24 hr fractional urine collection – Supine: <50-75 mg for 8-12 hrs – Upright: 200-1000 mg
• Etiology – Variant of normal permeability or renal vein
kink/entrapment • Long term follow-up
– 10-20 years: resolution or benign outcome

Pathologic Proteinuria

Pathologic Proteinuria
• Fixed proteinuria >150-300 mg/24hrs or
• First am void has urine protein:creatinine >0.2 or
• Edema
– PE (edema, rash, volume), Ht, Wt, BP
– UA (?hematuria), 24 hr urine protein &creatinine
– BUN, creatinine, albumin, lytes, calcium, phosphorus, lipids, C3, C4
– CBC

Causes of Pathologic Proteinuria
• Nephrotic syndrome – Minimal change, FSGS, membranous
• Glomerulonephritis – Henoch-Schonlein purpura, IgA nephropathy,
Alport nephritis • Tubular Proteinuria
– Dent’s disease, Fanconi syndrome

When to Refer
• Parental anxiety or confirmation of orthostatic proteinuria
• Any pathologic proteinuria • ASAP for edema/anasarca,
hypoalbuminemia, hypertension, associated hematuria, elevated creatinine