Latex allergy Jay E. Slater, MD CBER/OVRR/DBPAP Laboratory of Immunobiochemistry.
36
Latex allergy Jay E. Slater, MD CBER/OVRR/DBPAP Laboratory of Immunobiochemistry
-
Upload
egbert-hood -
Category
Documents
-
view
215 -
download
0
Transcript of Latex allergy Jay E. Slater, MD CBER/OVRR/DBPAP Laboratory of Immunobiochemistry.
Latex allergy
Jay E. Slater, MDCBER/OVRR/DBPAP
Laboratory of Immunobiochemistry
Symptoms of latex allergy Urticaria Rhino-conjunctivitis Wheezing Anaphylaxis
A systemic, multisystem allergic reaction that may include any and all of the above, plus hypotension
Other types of latex allergy
Contact urticaria
Contact dermatitis
Irritant dermatitis

IgE-mediated responsesIgE-mediated responses
Mast cellsMast cells
Initial reports Germany, 1930’s
Europe, 1980’s
US/Canada, 1989

Items that elicit latex allergic responses gloves condoms catheters cofferdams surgical drains latex stoppers adhesives other
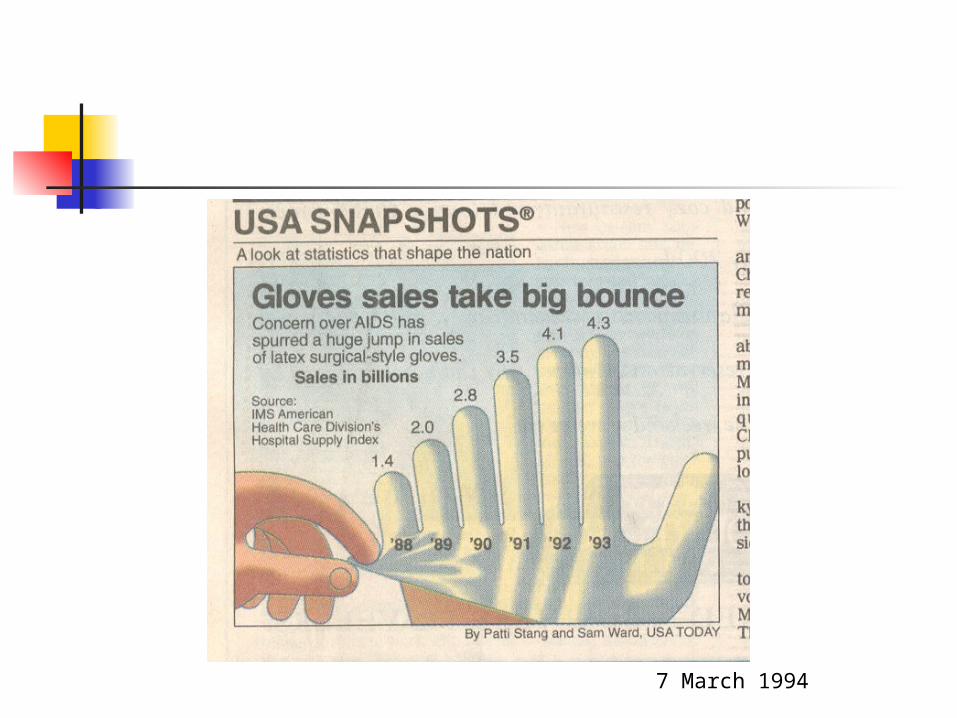
7 March 1994

Risk groups Meningomyelocele Urogenital abnormalities Health care workers Rubber industry workers
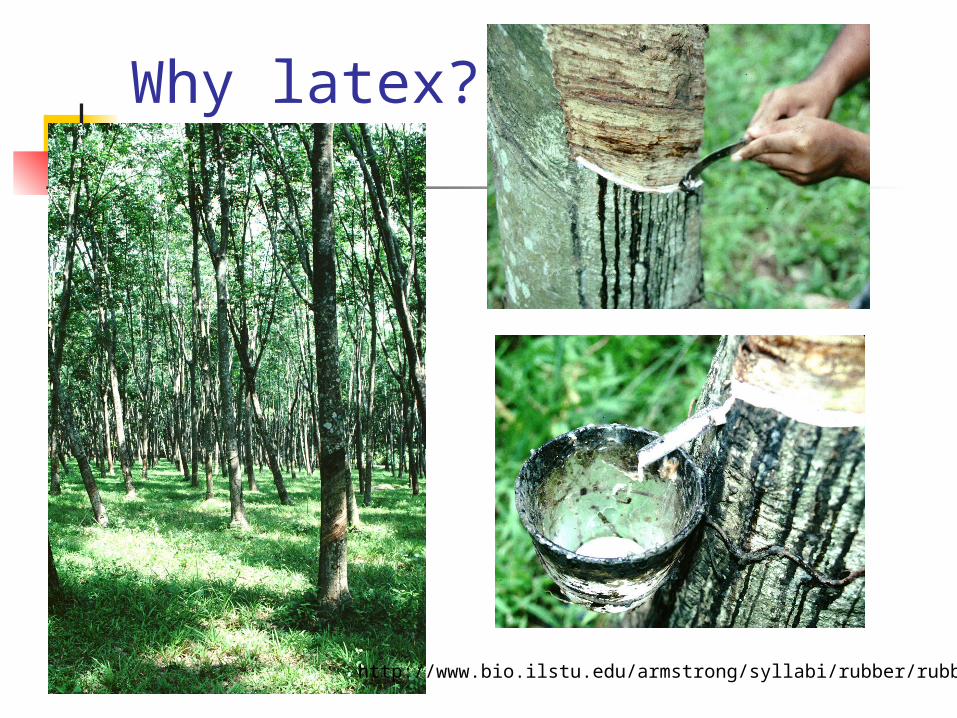
Why latex?
http://www.bio.ilstu.edu/armstrong/syllabi/rubber/rubber.htm

Why latex?
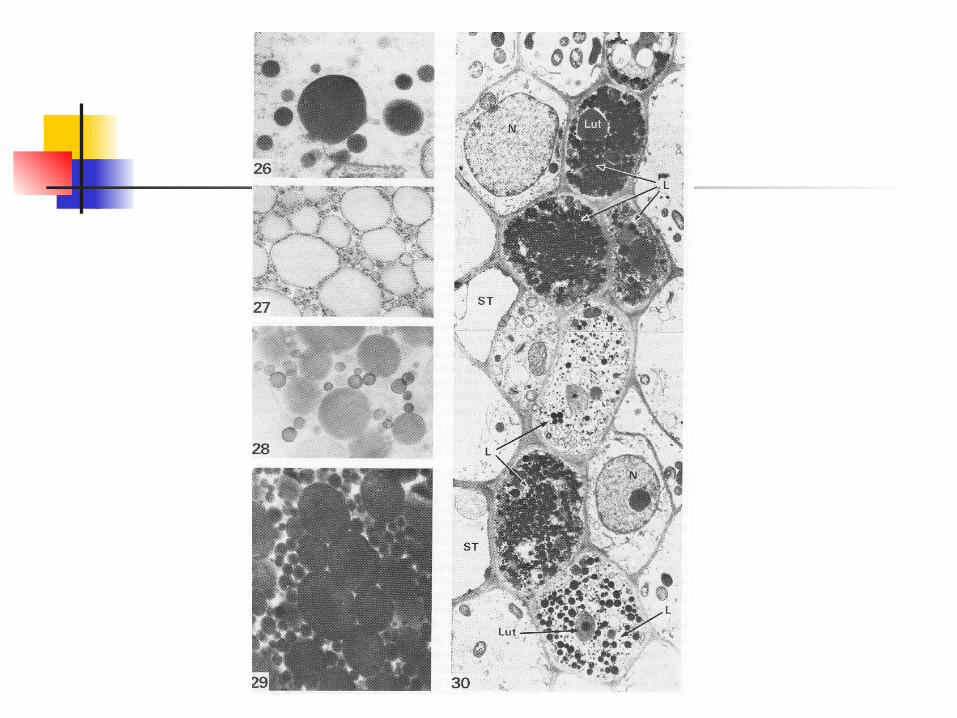
From D’Auzac et al, Physiology of rubber tree latex, CRC Press, Boca Raton, 1989, p. 6

Latex gloves are “dipped” products

Hevea latex antigens Hev b 1 (REF) Hev b 2 (-1,3-
glucanase) Hev b 3 (microhelix
component) Hev b 4 Hev b 5 Hev b 6 (prohevein) Hev b 7 (patatin
analogue)
Hev b 8 (profilin) Hev b 9 (enolase) Hev b 10 (Mn-
superoxide dismutase)
Hev b 11 (class 1 chitinase
Hev b 12 (lipid transfer protein)
Hev b 13 (esterase)
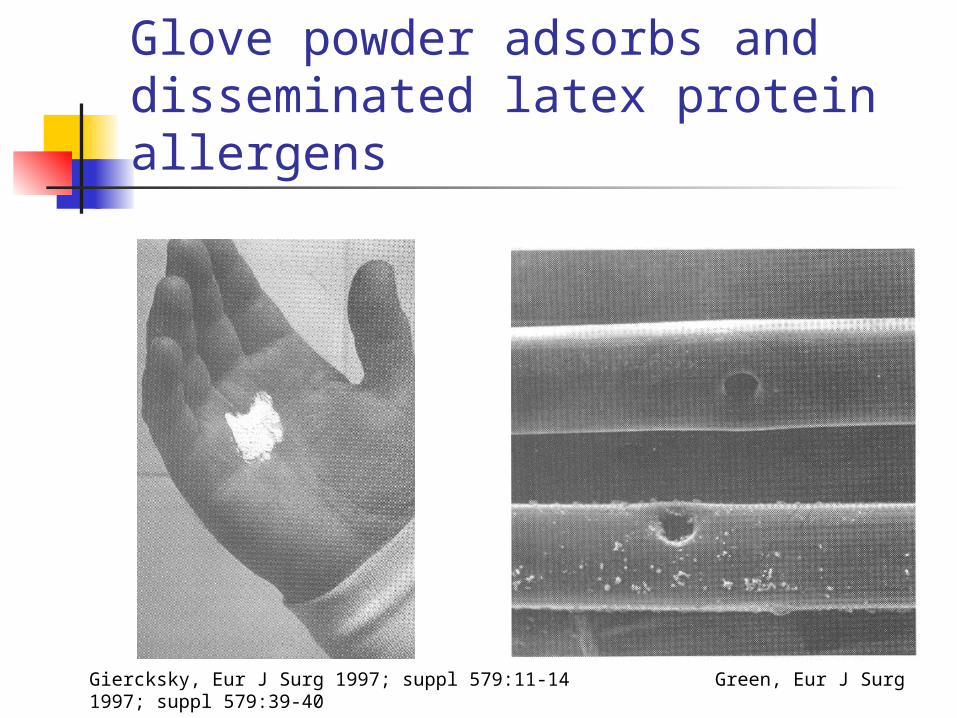
Glove powder adsorbs and disseminated latex protein allergens
Giercksky, Eur J Surg 1997; suppl 579:11-14 Green, Eur J Surg 1997; suppl 579:39-40

Diagnosis of latex allergy History
Events Risk factors
Latex-specific IgE skin test serum
Intervention (challenge and/or avoidance)

Prevalence of latex allergy Questionnaire Latex-specific IgE
skin test serum
Predictive value is questionable
Skin tests none licensed in US Outside the US:
Western Allergy Services (Canada) Stallergenes S.A. (France) Lofarma (Italy) ALK Abello (Denmark)
Serum specific IgE tests Available tests (Hamilton, JACI 2002; 110(2 suppl):S47-S56) :
Pharmacia CAP (sens 70-80%, spec >90%) Hycor HyTECH (sens 70-80%, spec >90%) DPC AlaSTAT (sens 90%, spec 70%)
Specific allergens important Adding Hev b 5 to CAP increases sensitivity by 1-
2% (Lundberg, Allergy 2001; 56:794-795) Hev b 2 + 3 + 7 is 100% sensitive for spina bifida
(Kurup Clin Exp Allergy 2000; 30:359-369)

General population Seroprevalence
Reinheimer (1995): 12% Garabrant (2001) : 8-37% Grzybowski (2002): 8%
Skin tests Buckland (2002): 5% Jensen (2002): 9%
Health care worker data Multiple initial estimates: 5-10% Workers compensation claim data:
not a significant cause of work-associated disability (Horowitz et al. 2000-2002)
NHANES II : modest increased risk (OR up to 2.53 (1988-1991)

Health care workers – incidence data
769 apprentices dental, animal care, pastry-making Skin tests (for latex and program-specific
allergens) and questionnaire <44 month follow-up
Incidence of latex allergy Dental: 2.5%/year Animal: 0.4%/year Pastry: 1.6%/year
Garabrant et al. 2001
Urogenital abnormalities Spina bifida <37% bladder exstrophy, cerebral palsy,
and spinal cord injury spina bifida, atopy, and the
number of surgical interventions are independent risk factors (OR 6.76, 3.37 and 1.14/operation) (Hochleitner, et al. 2001)
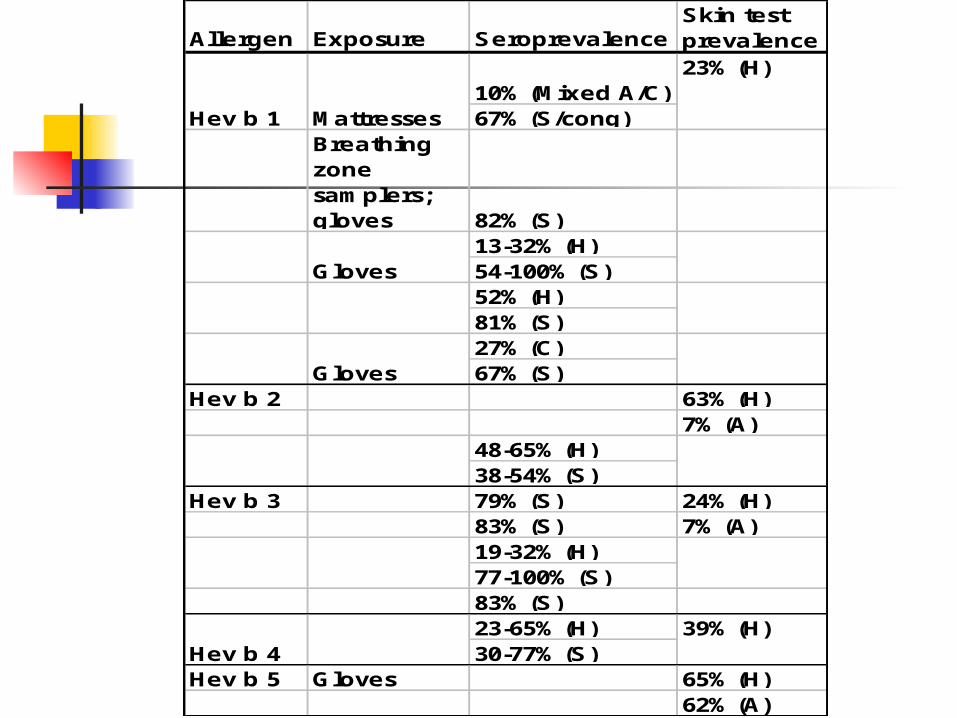
Allergen Exposure SeroprevalenceSkin test prevalence
10% (Mixed A/C)67% (S/cong)
Breathing zone samplers; gloves 82% (S)
13-32% (H)54-100% (S)52% (H)81% (S)27% (C)67% (S)
Hev b 2 63% (H)7% (A)
48-65% (H)38-54% (S)
Hev b 3 79% (S) 24% (H)83% (S) 7% (A)19-32% (H)77-100% (S)83% (S)23-65% (H)30-77% (S)
Hev b 5 Gloves 65% (H)62% (A)
Hev b 1 Mattresses
23% (H)
Gloves
Gloves
Hev b 439% (H)
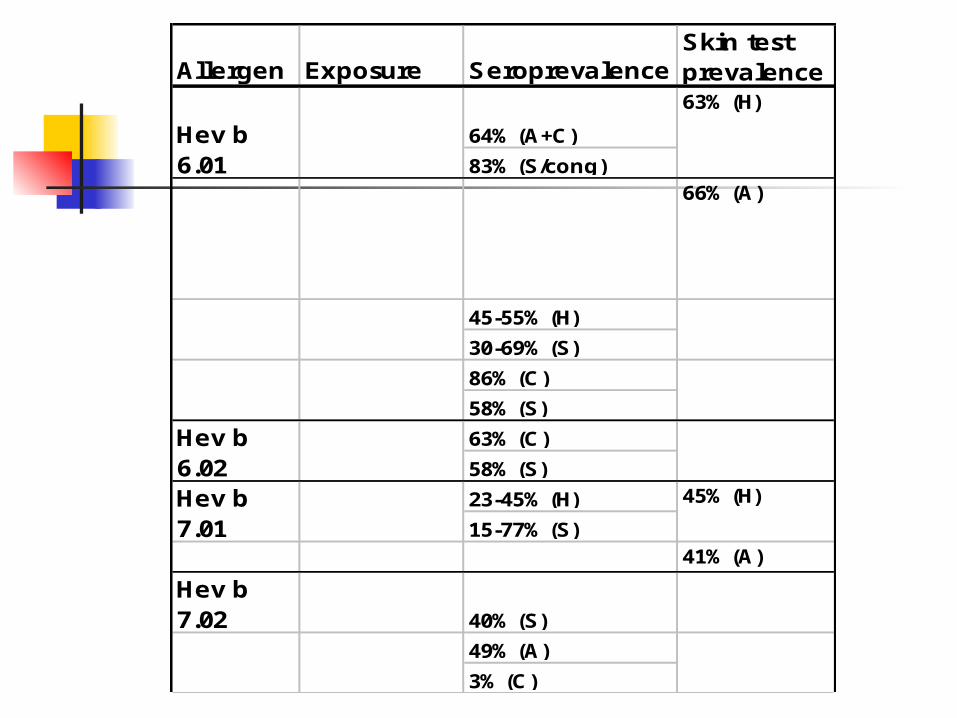
Allergen Exposure SeroprevalenceSkin test prevalence
64% (A+C)
83% (S/cong)66% (A)
45-55% (H)
30-69% (S)
86% (C)
58% (S)
63% (C)
58% (S)
23-45% (H)
15-77% (S)41% (A)
49% (A)
3% (C)
Hev b 6.01
Hev b 7.01
63% (H)
Hev b 6.02
45% (H)
Hev b 7.02 40% (S)
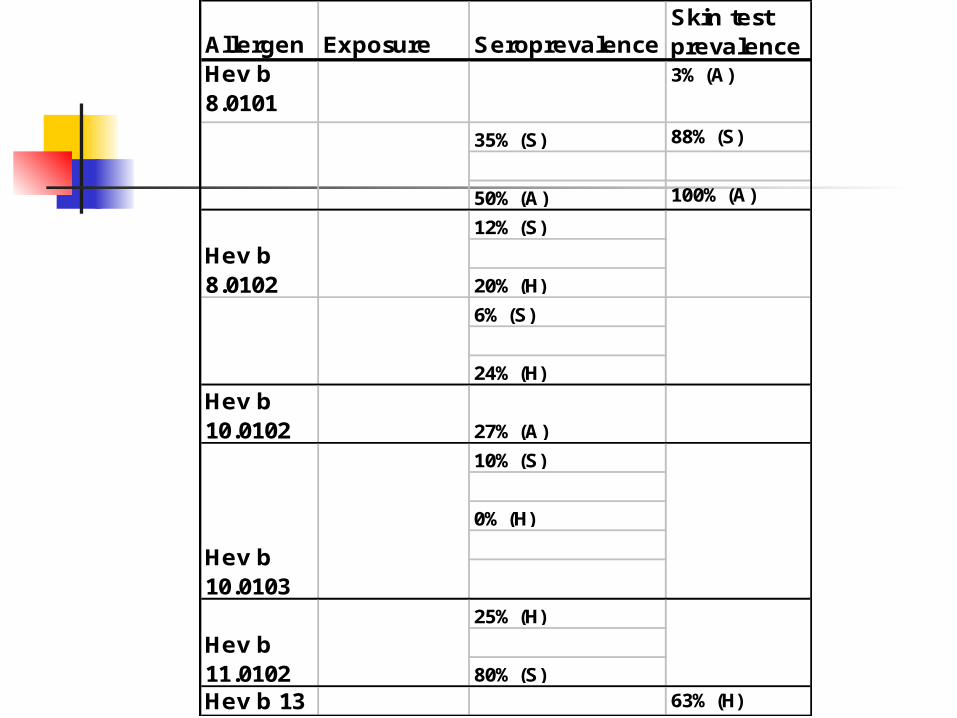
Allergen Exposure SeroprevalenceSkin test prevalence
Hev b 8.0101
3% (A)
35% (S) 88% (S)
50% (A) 100% (A)
12% (S)
20% (H)
6% (S)
24% (H)
Hev b 10.0102 27% (A)
10% (S)
0% (H)
25% (H)
80% (S)
Hev b 13 63% (H)
Hev b 8.0102
Hev b 10.0103
Hev b 11.0102

Modes of treatment 1. Avoidance 2. Avoidance 3. Avoidance 4. Other

Avoidance is hard because latex is ubiquitous in the health
care environment labeling has been erratic threshold doses (for sensitization
and reactivity) are unknown cross-reactivity with foods

Cross-reactivity banana chestnut avocado other fruits
Cross-reactivity of Hevea latex antigens Hev b 3 : red kidney bean Hev b 5 : kiwi Hev b 6 : wheat germ agglutinin Hev b 7 : potato Hev b 8 : profilins Hev b 9 : fungal enolases Hev b 10 : fungal superoxide
dismutases lysozymes: ubiquitous

Other approaches better methods of prevention premedication regimens immunotherapy
classical peptide based naked DNA
Premedication H1 antagonist (H2 antagonist) glucocorticoid (sympathomimetic)
Premedication Plausible efficacy, but No evidence that it works Anecdotal reports of
failure May lead to breach of latex
precautions

Final points…1. At this time, prevention is the only effective
treatment for latex allergy. 2. Latex allergens are ubiquitous, but 3. Gloves are the most important source of latex
allergen in the health care environment. Deal with the gloves first. Catheters are also important.
4. All latex allergy tests, whether RAST, ELISA, skin tests or challenges, are only as good as the allergens that are used. The allergens must be intact, and all significant specific allergens must be represented in the allergen mix used.
Final points…5. Testing is readily available now. The
predictive value of testing as a diagnostic tool is excellent. However, the value of such tests as a screening tool is uncertain.
6. Premedication does not prevent antigen-induced anaphylaxis.
7. Consider food allergy. 8. There is probably no way to construct a
latex-free environment in the healthcare setting, but it is certainly possible to construct a latex-safe environment.

Final points…
9. All latex avoidance measures come with a price (money, resources, risk of contamination, diminished barrier protection). Latex avoidance should be consonant with the risk.
10. History alone is a poor predictor of latex allergy, but the predictive value of not obtaining a history is zero. Asking your patients if they have symptoms consistent with latex allergy is simple and quick, and should be part of routine screening for all medical and dental practitioners.