Lactulose, Disaccharides and Colonic Flora · 2017. 8. 28. · Department of Medicine CA, Division...
13
REVIEW ARTICLE Lactulose, Disaccharides and Colonic Flora Clinical Consequences Mette Rye Clausen and Per Brebech Mortensen Department of Medicine CA, Division of Gastroenterology, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark Contents Drug s 1997 Jun: 53 (6) : 930-942 00 12-6667/97/ rJ:XJO-O<I3O/ S13.00/ 0 © Ad isInterna tional lim ited . AUrights reserved . Summary . 1. Dietary Carbohydrate . 1.1 Lactulose ..... 2. Colonic Fermentation and Producti on of Short-Chain Fatty Acids (SCFA) 2.1 Fermentation of Lactulose . 3. Lactul ose in the Management of Constipation ........ 3.1 Colonic Compensation in Carb ohydrate Malabsorption 3.2 Fermentation Capacity Threshold : Individual Variability . 3.3 DoesLactu lose Exert Its La xative Effect Through the Osmotic Act ivity of Unferme nted Carbohydrate? . 3.4 Capacity of the Colon to Absorb Fluid . 3.5 Possible Me chanisms of A ct ion of Lactul ose in the Treatment of Const ipation. 4. Lactulose in the Management of Hepatic En cephal opathy ............ 4.1 Effects of Lactulose on Ammonia and Nitrogen Meta bolism .......... 4.2 Role of Short- and Mediu m-Chain Fatty Acids in Hepat ic Encephalopathy . 4.3 Effe ct of Lactulose on Colonic SCFA Production in Hepatic En cephal opathy 4.4 Possible Mechanisms of Acti on of Lactulose in the Treatment of Hepati c En cephal opathy 5. Conc lusions .................................. 930 931 931 931 932 933 933 934 935 936 936 937 937 938 939 940 940 Summary Lactulose is one of the most frequently utilised agents in the treatment of constipation and hepatic encephalopathy because of its efficacy and good safety profile. The key to understanding the possible modes of action by which lactulose achieves its therapeutic effects in these disorders lies in certa in pharmacological phenomena: (a) lactulose is a synthetic disaccharide that does not occur naturally; (b) there is no disaccharidase on the microvillus membrane of enterocytes in the human small intestine that hydrolyses lactulose; and (c) lactulose is not absorbed from the small intestine. Thus, the primary site of action is the colon in which lactulose is readily fermented by the colonic bacterial tlora with the production of short-chain fatty acid s and various gases.The purpose of this review is to focu s on some pertinent basic aspects of the clinical pharmacology of lactulose and to discuss the possible mechanisms by which lactulose benefits patients with con- stipation and hepatic encep ha lopat hy.
Transcript of Lactulose, Disaccharides and Colonic Flora · 2017. 8. 28. · Department of Medicine CA, Division...

REVIEW ARTICLE
Lactulose, Disaccharides andColonic FloraClinical Consequences
Mette Rye Clausen and PerBrebech Mortensen
Department of Medicine CA, Division of Gastroenterology, Rigshospitalet,Universi ty of Copenhagen, Copenhagen, Denmark
Contents
Drug s 1997 Ju n: 53 (6) : 930-9420012-6667/97/rJ:XJO-O<I3O/ S13.00/0
© Ad isInterna tional lim ited . AUrights reserved .
Summary .1. Dietary Carbohydrate .
1.1 Lactulose . . . . .2. Colonic Fermentation and Producti on of Short-Chain Fatty Acids (SCFA)
2.1 Fermentation of Lactulose .3. Lactulose in the Management of Constipation . . . . . . . .
3.1 Colonic Compensation in Car bohydrate Malabsorption3.2 Fermentation Capac ity Threshold : Ind ividual Variability .3.3 Does Lactulose Exert Its La xa tive Effec t Through the Osmotic Activity of
Unferme nted Carbohydrate? .3.4 Capac ity of the Colon to Absorb Fluid .3.5 Possible Me chanisms of Action of Lactulose in the Treatment of Constipation.
4. Lac tulose in the Management of Hepatic Encephalopathy . . . . . . . . . . . .4.1 Effects of Lac tulose on Ammonia and Nitrogen Metabolism . . . . . . . . . .4.2 Role of Short- and Medium-Chain Fatty Acids in Hepatic Enc ephalopathy .4.3 Effect of Lactulose on Colon ic SCFA Produc tion in Hepatic Encephalopathy4.4 Possible Mechanisms of Action of Lactulose in the Treatment of
Hepatic Encephalopathy5. Conc lusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
930931931931932933933934
935936936937937938939
940940
Summary Lactu lose is one of the mos t freq uen tly utilised age nts in the treatment ofconstipation and hepatic ence pha lopat hy because of its efficacy and good safe typrofile. The key to understanding the possible modes of action by which lactuloseac hieves its therapeutic effects in these diso rders lies in certain pharmaco logicalphe nomena: (a) lactu lose is a sy nthetic disaccharide that does not occur naturally;(b) there is no disaccharidase on the microvi llus membrane of enterocytes in thehuman small inte sti ne that hydrolyses lactulose; and (c) lactulose is not absorbedfrom the small intestine. Thus, the primary site of action is the colon in whichlactulose is readi ly fermented by the co lonic bacterial tlora with the produ ctionof short-chain fatty acid s and various gases. T he purpose of this review is to focu son some pertinent basic aspects of the clinica l pharmacology of lactulose and todiscu ss the possible mec hanisms by which lactulose benefits patients with co nstipation and hepatic encephalopat hy.

Disaccharides and Colonic Flora 931
1.Dietary Carbohydrate
Dietary carbohydrates may be divided intomonosaccharides, disaccharides, oligosaccharidesand polysaccharides. Their physiological properties and health benefits depend on the site, rate andextent of their digestion or fermentation in the human gastrointestinal tract. The polysaccharidefraction of plant cell walls (dietary fibre) and someforms of starch (resistant starch) are resistant tohydrolysis in the small intestine. These carbohydrate polymers as well as indigestible oligosaccharides, e.g. stacchyose and raffinose, enter the colonthrough the ileocaecal valve to be fermented by thecolonic bacterial flora. Monosaccharide and disaccharide sugars are absorbed as they pass throughthe healthy small intestine and only become available to the colonic flora as a consequence of deficiencies in the transport system, or, more usually,specific disaccharidase deficiencies, e.g. lactasedeficiency. Physiological carbohydrate malabsorption, that is, the fermentable carbohydrate enteringthe colon in healthy individuals, is in the range of30-60 g/day in Western communities.l!l This loadis normally fermented by the vast numbers of colonic bacteria.
1.1 Lactulose
Lactulose is a synthetic disaccharide composedof the monosaccharides galactose and fructose [p( 1-4)-galactosido-fructose] . The disaccharidasesthat split naturally occurring disaccharides intotheir hexose moieties do not include a lactulase,and lactulose is not metabolised or absorbed in the
human small intestine.Pv' Once in the caecum,lactulose is a fully fermentable carbohydrate.Lactulose is widely considered to be an effectiveagent in the management of constipation and hepatic encephalopathy. It is the purpose of this review to discuss the interaction of lactulose with thebacterial flora of the colon and the possible modesof action by which it achieves its therapeutic effectsin patients with constipation and hepatic encephalopathy. The review deals almost exclusively withlactulose. The principles expressed, however, areapplicable to any malabsorbed and fermentable disaccharide, e.g. lactitol, a disaccharide analogue oflactulose for which there is also no disaccharidaseon the microvillus membrane of enterocytes, orlactose when it is administered to lactase-deficientindividuals.
2. Colonic Fermentation and ProductionofShort-Chain Fatty Acids (SCFA)
Fermentation, the process whereby the microbial population that inhabits the human colonbreaks down carbohydrates in order to obtain energy for maintenance of cellular function andgrowth, is an important component of normalcolonic activity (fig . I) . Short-chain fatty acids(SCFA) and the gases H2, CO 2 and, in some individuals, CH4, are the principal end products of car bohydrate fermentation.l!' The major SCFA foundin the human colon are the C2 (acetate), C3 (propionate) and C4 (butyrate) members of the ali phatic monocarboxylic acid series. Formate (C I) ,valerate (C5), hexanoate (C6), and the branched-
Dietary mono·, di- and oligosaccharides
SCFA,H2,C02,CH.andincreased bacterial mass
BacterialenzymesIPolysaccharides 1- - - - -- ICarbohydrates Ir-- - -
Fig. 1. Bacterial fermentation in the human colon . Abbrevialion: SCFA = short-chain fatty acids .
<0Adis International Limited. Ail rights reserved. Drugs 1997 Jun; 53 (6)

932
chain fatty acids isobutyrate (iC4) and isovalerate(iC5) , whi ch are produced during amino acid ferment ation ,14's1are also present in the co lon, thoughin smaller quantities. Oth er orga nic ac ids such aslactate and succ inate are ferment ati on intermediates. Th ey can be further metaboli sed to SC FA, anddo not usually accumulate to any extent, exceptduring rapid carbohydrate breakd own. P"!
Th e SCFA are weak acid s and their pKa valuesare very similar, rangin g from 4.76 to 4 .87 . Thu s,more than 95% of the SCFA are present in theirdi ssociated form at the phy siological pH of the colon (pH 6-8) . Total co ncentrations of SCFA are lowin the sma ll intestine, but in the co lon and faecesSCFAco nstitute the predominant ani ons at concentration s ranging from about 80 to 130 mmol/Lp ·IOIConcentrati ons are highest in the caecum, wheresubstra te avai lability is grea tes t, and fa ll progressive ly towards the dista l co lon. By co ntras t, pH islowest in the right colon and rises in the distalbowel .l?' SC FA are av idly abso rbed by the co lonicepithe lium,II I.1 21 and used as a source of energy,e ither locall y (co lonic mucosa)113. 151 or syste mica lly (l iver, peripheral tissues).' 161 In the colon, absorpt ion of SCFA is accompanied by luminal bicar bon ate acc umulatio n and inc reased sodium andwate r absorption.t'I -P!Thu s, the micro bia l processco nve rts unabsorb able materi al to rapidly absorbedSCFA, thereby redu cing the effective osmo tic pressure of the co lonic co ntents, enhanci ng water andelectrol yte abso rption, and sa lvag ing calo rieswhi ch wo uld otherwise be lost in the faeca l strea m.
2.1 Fermentation of Lactu lose
Lactul ose, after arriving in the colon, is digestedby bacteri al disaccharidases and metaboli sed to orga nic aci ds, mainl y acetate and lactate , H2 andC02.1 61 A variety of studies have show n that lactulose is usuall y vigorously fermented . In an ill vitroex pe rime nt using human faecal homogen ates,Vince et aLI171showed that co mplete fermen tatio nof 10 giL (30 mmol/L ) of lactul ose occurred within6 hours. By use of a similar tech nique, Mortensenet aLII X.191 showed tha t the total product ion ofSCFA in faeca l homoge nates was increased 2- to
e Ad is Interna Nonal Umited . All rights reserved .
Clausell & Mor!('//s('//
3-fo ld by the additio n of 100 mmol/L lactulose orits mon osacch ari de co ns tituents, ga lac tose andfructose, during inc ubation for 6 hours , secondaryto an iso lated 4- to 6-fo ld increase in the synthes isof acetate. In patient s undergoing elective cholecystectomy, caecal insti lla tio n of lactulose ca usedan immediate inc rea se in por tal plasma SCFAco nce ntrations, principally acetate; peak co ncentrations were achieve d in 15 to 45 minutes, co nfirming efficient fermen tatio n of lactulose and absorption of the resultant SCFAP ol
Th e various gases ge nerated in the co lon are either absorbed and ex pired in breath or expelled asflatu s, and excess gas production may ca use bor borygm i and flatul ence. Sin ce H2 produced in thehuman bod y deri ves entire ly from bacter ial ferment ation of nonabsorbed carb oh ydrate, brea th H2
exc retion in the abse nce of sma ll intes tinal bacterial ove rgrowth ca n be used as a marker of carbohydrate rnalabsorpt ion .F! ' Th e extent of ma labsorption may be quantified by co mparing breath H2
excretion following a test dose of lactulose withtha t after ingestion of a different carbohydrate.l->'
Fermentation of a readily fermen tab le carbohydrate result s in acidification of co lonic co ntent s.Using a pH-sensitive rad iotelem etry de vice, Bownet aL/231 showed that lactul ose 30 to 40g da ily decreased the pH of the right co lon fro m contro l levels of 6.0 to 4.8 5. As the intes tinal co ntent reachedthe left co lon and rectum, the median pH rose,probab ly as a res ult of SCFA absorpt ion and bicar bonate sec retion. Th e effect of lactulose on faeca lpH depend s on the dose employed, and the drop inpH is usually maint ain ed throughout the co lon andthe stool when larger doses of lactul ose are ad ministered.124.261
Alth ough co ns istent cha nges in the relat ive pro por tion s or in the abso lute numbers of differe ntbacterial species have been difficul t to ide ntify inpat ient s treated with lactul ose,1 27-291this co mpou nddoes appea r to have a significant effect on the metaboli c ac tivities of the microb es. In healthy volunteers, faeca l levels of ~-galactosidase activity increased significantly after an 8-da y period o f anon diar rhoeogeni c dose of lactu lose (20g twice
Drugs 1997 Jun: 53 (6)

Disacchari des and Colonic Flora
daily j.!'" Co mpared with day I , caecal co ntentssampled on day 8 afte r lactul ose administ ration exhibit ed a mar ked fall in pH, a faster disappearanceof lactulose and its co nstitutive hexoses, and increased co ncentrations of SCFA and lactate.l'" Theco lonic microflora therefore are able to adapt toferment lactul ose, and the more efficie nt bacteri alfermentation of lactul ose mod ifies the diarrhoeaindu ced by a larger load of this sugar.P'!'
Th e co lonic bacter ia use ferme ntable carbohydrate, e.g . lactul ose, as a so urce of ene rgy, thu sprom oting their growth and multipl ication. P!' It isbel ieved that bacteri al growth ass imilates the ammoni a produ ced by degradation and putrefactionof ingested prot ein s as a source of nitrogen , andfaeca l nitrogen exc retion increas es 2- to 4-fo ld after lactul ose administration.tv-P!
3. Lactulose in the Managementof Constipation
Lactul ose is frequently used as an effective laxative in the management of constipation.P"! Basedon the absence of its respecti ve disaccharidase, therationale for the use of lactulose as a laxative wasto indu ce disacch aride malab sorption, a we llknown cause of diarrh oea. In spite of the freq uencyand importan ce of ca rbo hydrate-i nduce d diar rhoea, its pathophysiology is not full y understood .Until re lative ly rece ntly, SC FA were thought to bepoorly abso rbed and to functi on as an irrit ating andos motic force stimula ting intes tina l motilit y andimp eding co lonic water and elec tro lyte absorption .135.3xl Early work on carbohydrate malabsorption therefo re impli cated bacter ial fermentation asthe prim ary mechani sm for diarrhoea in disaccharide malabsorption (' ferme ntative diarrhoea ' ). Th estro ng co rre lation between faecal water output andoutput of SCFA135.371 was thought to incriminateSCFA in the path ogenesis of diarrhoea. As co lonicSCFA levels remain more or less co nstant despitedietary changes, any fac tor increasing stool we ightwill, however, increase their output. Later in vivostudies of intes tinal SCFA abso rption have consistent ly de mo nstrated efficient absorption of SCFAfrom the human colon.' I 1.1 21 Th is absorption mark-
© Adis Internationa l Umited. All rights reserved.
933
edly enha nces net sodi um and water abso rptio nand bicarb onate secretion into the lumen. Thu s, theintracolonic fer mentation of nonabsorbed suga rsinto readily absorbable SCFA reduces the osmoticload , and suppresses or mit igates the diarrhoeawh ich would have resulted from unm odified ilealoutput.
3.1 Colonic Compensation inCarbohydrate Ma labsorption
Th e protect ive role of coloni c fermentation inreducing the severity of carbohydrate-induced diarrhoea has been demonstr ated in studies co mparingthe output of faecal water in response to a nonfe rme ntable os mo tic load with a load of ferm entable carbohydrate. Hammer et al.1391co mpared thediarrh oea res ulting fro m increasin g iso -os mo larloads of the nonabsorbable, nonferment able andelec trically neut ral co mpound polyeth ylene glyco l(PE G) and lactulose in healthy individuals. Increasing osmotic loads of PEG caused a near-li nearincrease in stool wa ter output. At any load,lac tu lose ind uced less diarrhoea than did PEG.With low (45 g/day) or moderate (95 g/day ) dosesof lact ulose, stool water losses were redu ced by asmuch as 600 g/day (co mpared with equimo lar osmotic loads of PEG ). As lactulose doses of >45g/day were ingested, faecal ca rbohydrate exc retionrose progressively, thereb y contributing more andmore to the osmotic dr iving force for diarrh oea.With the largest dose of lactul ose (125 g/day) thedifferen ce between lactulose- and PEG-induceddiarrh oea markedly decreased . In lactulose- inducedd iarrhoea, daily stoo l collections co nta ined anaverage of I, 12 and 45g of carbohyd rate when theparticipant s were ingesting 45 , 95 and 125g oflactul ose/d ay, respecti vely, indi catin g a maximumca pacity of the co lonic bacteria to met aboli selactulose of approximately 80 g/day.' 39I
Saunders and Wiggi nsl' ! obtained dose-responsecurves fo r mann itol (a poorly absorbed sugar alco hol ), raffi nose, lactulose and magnesium sulfate inrelation to faecal water ou tput over 48 hours afte rthe dose of test substance. With magnesium sulfatethere was an immediate inc rease in faecal output,
Drugs 1997 Jun; 53 (6)

934
whereas a lag period was observed for the nonabsorbed sugars. When an increase in faecal wateroccurred after ingestion of mannitol, lactulose orraffinose, the sugar or its constitutive hexoses appeared in the stools. The dose-response experiments indicated that the colonic flora can normallyconvert 40 to 60g of single doses of carbohydrateto SCFA without the individual experiencing diarrhoea.I"
3.2 Fermentation Capacity Threshold:Individual Variability
The human colon is obviously capable of removing appreciable amounts offermentable carbohydrates from colonic contents, even in patientswith malabsorbed carbohydrate.Ue'" If, however,the fermentative capacity of the colonic microflorais exceeded, unmodified and osmotically activesugars may produce an osmotic diarrhoea. The response threshold when a given amount of carbohydrate is malabsorbed differs among individuals, Inthe study by Saunders and Wiggins.U' one participant tolerated a 73 mmol (25g) dose of lactulosewhereas another tolerated 176 mmol (60g) beforefaecal water output rose above 400 ml/48 hours andtest carbohydrate appeared in the stool. Similarly,doses of 120 mmol (22g) and 350 mmol (64g) ofmannitol were tolerated by different participants.
The individual variability may, at least in part,be explained by differences in the fermentation capacity of the bacterial flora. Individuals with a limited fermentation capacity or a high dependence onthe existing capacity for colonic carbohydrate degradation might be especially susceptible to an increased carbohydrate load. A similar situation mayapply to the development of microbial fermentation in newborn animals. Argenzio et al.1401 produced carbohydrate malabsorption by administration of corona virus to newborn pigs. This resultedin diarrhoea in 3-day-old pigs, with high concentrations of carbohydrate and low concentrations ofSCFA in colonic contents. Pigs 3 weeks of ageshowed no diarrhoea, with negligible amounts ofcarbohydrate and normal levels of SCFA in coloniccontents, indicating that the more mature micro-
'£JAdis International limited. All rights reserved.
Clausell & Mortellsell
flora in these older piglets were capable offermenting the osmotic load to SCFA, which could then berapidly absorbed from the colonic contents. Oncethe microbial process is well established, prolonged ingestion of carbohydrate results in an improved colonic fermentation capacity.l'v'"
The higher capacity to ferment carbohydratesmay be a result of enzymatic induction in existingrnicro-organisms!''! and/or an alteration in microbial populations.lv-'!' Flourie et al.1301 studiedhealthy volunteers for 2 test periods, at the beginning of which they ingested a diarrhoeogenic load(60g) of lactulose; the 2 periods were separated bya lactulose feeding period of 8 days, during whicha nondiarrhoeogenic load (20g) of lactulose wastaken twice daily. Stool weight and frequency, andfaecal outputs of carbohydrates after the ingestionof lactulose 60g, dropped significantly after thelactulose maintenance period (20g twice daily for8 days), indicating that the colonic flora can adaptto a nondiarrhoeogenic load of lactulose, and thatthis adaptation has a beneficial effect on the diarrhoea induced by a larger load of this sugar.
Similarly, Launiala!"!' reported on a 3-weekperiod during which an infant with congenital lactose malabsorption was maintained on a lactosecontaining diet. In comparison with the first day oftreatment, continued treatment resulted in a decreased stool volume and disaccharide output, anda sharp rise in faecal lactate concentration. No adaptation occurred in the small intestine.H!'
Hypothetically, regular consumption of carbohydrates malabsorbed in the small bowel may result in a more efficient colonic carbohydratefermentation and an increased response thresholdwhen a given amount of carbohydrate is malabsorbed. In addition to differences in colonic bacterial fermentation capacity, variations among individuals in the buffering capability of the colonmay contribute to individual differences in the response to identical amounts of nonabsorbable carbohydrates. It is known that caecal pH decreaseseven with the amounts of unabsorbed carbohydratenormally entering the colon .F" Furthermore, patients with severe carbohydrate malabsorption, ei-
Drugs 1997 Jun; 53 (6)

Disaccharides and Colonic Flora 935
::J150
::,0E.s 1002l!!"0>- 50JC::.0
of?IIIU 0
8
7
J: 60-
5
4 )2280)2100
1500)2300)1678
.EOJ
.~
~8: 500
i 1000
~
o 20 40 80 160 320 0 20 40 80 160 320
Lactulose (g/day)
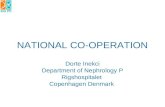
Fig. 2. Faecal weight,pH and carbohydrateconcentrationin faeces of 12 individualstaking increasingdoses of lactulose. The resultshave been divided in accordancewith the response in faecal output to low doses of lactulose (from Holtug et al.,126] with permission).
ther due to disaccharidase deficiency or due to ingestion of excessive amounts of lactulose, have decreased faecal pH in the range of 4 to 5.124,26,35]
This decrease in pH is sufficient to inhibit bacterial fermentation and SCFA production as shownin vivo and in vitro.126,42,43 j In subjects with a restricted colonic buffering system, the tolerance ofcarbohydrate malabsorption may be decreased asthe low pH decreases fermentation leading to accumulation of undigested sugars and osmotic diarrhoea early on in the process .
3.3 Does Lactulose Exert ItsLaxative EffectThrough the Osmotic Activity ofUnfermented Carbohydrate?
Many physicians believe that the change instool output in the diarrhoea of carbohydrate malabsorption is due to the osmotic effect of malabsorbed and nonfermented sugars. This assumptionseems to be supported by the studies mentionedabove (sections 3.1 and 3.2) in which diarrhoeaensued when carbohydrate appeared in the stools.The study by Holtug et aI.,126 1however, queries this
© Adis lnternottonol Limited. All rights reserved . Drugs1997Jun; 53 (6)

936
assumption. Healthy individuals were given lactulose twice daily for 3 consecutive days in each experimental period. Doses were doubled (20, 40,80,160 and 320 g/day) from each period to the next,with the end-point being diarrhoea in excess of1000 g/day. Faecal output responded differentlyamong individuals, and 2 types of behaviour wereidentified (fig . 2).
In accordance with the interpretation that carbohydrate-induced diarrhoea is due to the osmotic effect of nonfermented mal absorbed sugars, diarrhoea occurred suddenly in six of 12 individuals inassociation with the appearance of carbohydrate infaeces . In the 6 other subjects, however, faecal output gradually increased with increasing doses oflactulose and diarrhoea occurred before the appearance of faecal carbohydrates.P''! How does unabsorbed carbohydrate cause diarrhoea in thosecases?
3.4 Capacity of the Colon to Absorb Fluid
The mechanism of action of lactulose as a laxative is probably multifactorial, involving effects onboth the colon and the small bowel. Under normalcircumstances, about 1500ml of fluid is estimatedto enter the colon each day.14411ndisaccharide malabsorption an increased volume of fluid is retainedin the lumen of the small intestine by the osmoticeffect of disaccharide.141,451 Analysis of distal ilealfluid collected during the passage of a lactose mealin lactase-deficient people and a lactulose load inhealthy people indicates that about two-thirds ofthe osmotic load entering the colon consists ofendogenous electrolytes.130,41,45] Thus, the waterload delivered to the colon is about 3 times thatcalculated to be osmotically held by the nonabsorbed sugar.
A logical extension of the above observations isto ask what the colon can accomplish under stress.In fact, the colon has a surprisingly large capacityto adapt to fluid overload. When the healthy humancolon was subjected to a slow, continuous infusionof isotonic fluid (1.4 to 2.8 ml/min), net absorptionof water increased markedly, up to 5 to 6 L/day.1461
The rate and pattern of t1uid entry are , however, of
© Adi s International Limited . All rights reserved.
Clausen & Mortensen
major importance. Rapid infusion (8.3 ml/min) ofa single bolus of 250ml of t1uid did not influencefaecal output whereas 500ml delivered at the samerate overwhelmed the absorptive capacity of thecolon and produced liquid stools.U''!In healthy human volunteers, Chauve et al.1471investigated pressure recordings in the right , transverse and left colon, while isotonic saline was continuously infusedin the caecum. The data obtained indicated thatonce a certain volume of content is reached in theproximal part of the colon, it contracts and propelsits content.l''?' which may explain the different colonic responses comparing slow continuous andrapid bolus infusions of t1uid into the caccum .lv '
The extra volume load to the colon due tolactulose can be estimated to be 1.65L at a lactuloseintake of 60g,130,41,451and the sudden arrival in thecaecum of this considerable amount of ileal discharge might lead to colonic 'decompensation ' andprompt colonic evacuation.
3.5 Possible Mechanisms of Action ofLactulose in the Treatment of Constipation
A single primary mechanism for the laxative effect of lactulose cannot be determined because ofmultiple possible effects . Most likely , the laxativeeffect of lactulose results from the combination of:• water retention in the small intestine through the
osmotic activity of the unabsorbed disaccharide; and
• interference with net t1uid absorption in the colon due to the osmotic effect of malabsorbed andintact sugars when the bacterial fermentationcapacity is exceeded.Whether or not the laxative effect of lactulose is
accomplished is probably just a matter of dose . Itis, however, important to realise that the responsethreshold when lactulose is prescribed differsamong individuals (fig . I) . A gradual increase infaecal output with increasing amounts of lactuloseoccurs in some individuals, while others suddenlyrespond with severe diarrhoea.P'" Unfortunately, itis not possible to predict the response of a givenindividual, and firm guidelines for dosage recommendations are impossible.
Drugs 1997 Jun: 53 (6)

Disaccharides and Colonic Flora
4. Lactulose in the Management ofHepatic Encephalopathy
Lactulose has been successfully used in thetreatment of hepatic encephalopathy ever sincethe pioneering experiments of Bircher et al. in1966.'241 The exact mechanisms whereby lactuloseexerts its beneficial effect on hepatic encephalopathy are not fully understood, but several hypotheses have been suggested.
Hepatic encephalopathy is a complex neuropsychiatric syndrome that appears to be characterisedpredominantly by augmented neuronal inhibition.The syndrome is associated with hepatocellularfailure, increased portal-systemic shunting ofblood and multiple metabolic changes, and is generally considered to be a potentially reversible metabolic encephalopathy. The precise pathogeneticmechanism responsible for the CNS dysfunctionremains to be determined.
Products of bacterial metabolism in the colon,which are normally absorbed and extracted by theliver, tend to accumulate in the peripheral blood ofpatients with liver disease either because the diseased liver is unable to remove these compoundsfrom the portal blood perfusing it, or because portal hypertension has led to the development of venous collaterals which transmit portal blood directly into the systemic circulation. If one or moreof these metabolites can cross the blood-brain barrier and promote neural inhibition, they may contribute to hepatic encephalopathy. Despite decadesof research endeavour, the nature of the toxic, gutderived, substances defies identification. Threecandidate toxins seem likely pathogenetic factorsbecause they are present to excess in patients withliver failure and cause coma experimentally in animals. These are ammonia, SCFA and medium-chainfatty acids (MCFA), and mercaptans; of these, ammonia probably plays the most central role.'48I
4.1 Effects of Lactulose on Ammonia andNitrogen Metabolism
Ammonia occupies a central position in nitrogenmetabolism in the colon, both as an end-product of
© Adi s International Limited . All right s reserved.
937
bacterial metabolism of amino acids , peptides andproteins.P?' and as the simplest nitrogenous compound which can be used by bacteria as a startingmaterial in the synthesis of their own nitrogenousconstituents. In the absence of active colonic fermentation most of the ammonia formed is absorbed to be converted to urea in the liver.
When lactulose was first used in the treatmentof hepatic encephalopathy, it was presumed thatthe colonic acidification favoured the growth ofacid-tolerant lactobacilli and other acidophilic, fermentative bacteria and reduced the growth ofacidophobic, proteolytic bacteria responsible forammonia formation .P'! However, quantitativestudies failed to confirm this rearrangement of gutf1ora.127,281 Alternatively, luminal acidificationwould reduce the proportion of ammonia availablefor reabsorption by passive nonionic diffusion byincreasing the ratio of ionised to unionised ammonia, thereby enhancing the faecal excretion of ammonia.P'!' Attempts to demonstrate increases instool ammonia caused by lactulose administrationhave failed,151 ,521 except when excessive amountsof lactulose (>80 g/day) have been given.F'l ln thatcase, stool ammonia increases approximately 3fold .1331The main point is, however, that ammoniaconstitutes only a small percentage (3 to 5%) oftotal faecal nitrogen. The debate on whether or notlactulose increases faecal excretion of ammonia istherefore of minor importance in the context of total nitrogen excretion. Of more importance for faecal nitrogen clearance are other sources of nitrogen, constituting about 95% of total stool nitrogen.
By use of an anaerobic faecal incubation system, Vince et al. I171demonstrated that net generation of ammonia by faecal bacteria can be converted to net utilisation of ammonia by theprovision of a fermentable source of energy, e.g.lactulose, ammonia disappearing from the incubation system. The results may be explained by acombination of factors: (a) the availability of areadily fermentable substrate may encourage bacterial proliferation and assimilation of ammonia asa nitrogen source;' 17,31 I (b) preferential use oflactulose as a carbon and energy source may exert
Drugs 1997 Jun; 53 (6)

938
a sparing effect on the metabolism of both exogenous and endogenous aminated compounds with asubsequent decrease in the generation of ammoniaby colonic bacteria;117, 191 and, (c) low pH valuessuch as are induced in the colon by lactulose maybring about a general reduction in bacterial metabolism, including that of ammonia-producing bacteria.l 17,19,26,421 If, in the presence of lactulose, incorporation of ammonia into bacterial protein isstimulated, faecal nitrogen excretion should increase and hepatic urea production and total bodyurea pool should decrease during administration oflactulose.
This is exactly what Weber l321and Mortensen'Vlhave shown. Administration of lactulose caused a2- to 4-fold increase in faecal nitrogen content inpatients with cirrhosisl321and in healthy individuals,1331 and the increase in nitrogen excretion wasaccompanied by a significant reduction in the ureaproduction rate leading to a reduction in the totalbody urea pool.1321Using recently developed techniques that permit quantitative separation of faecalsolids into bacterial, soluble and fibre fractions,Weber et al.1531analysed the effects of lactulose onthe compartmentalisation of faecal nitrogen. In patients with cirrhosis, administration of lactulose(56 ± 6 g/day) caused a marked increase in both thesolid weight and nitrogen content of the bacterialand soluble fractions of stool ; lactulose administration increased nitrogen excretion in the bacterialand soluble fractions by 165 and 135%, respectively. The major increment in nitrogen content ofthe bacterial fraction indicated that lactulose stimulated bacterial growth and multiplication significantly, and thereby increased the incorporation ofnitrogenous compounds such as ammonia into bacterial protein.
The increase in faecal soluble nitrogen may beexplained by reduced bacterial catabolism of nitrogenous compounds to absorbable metabolites,e.g. ammonia, due to: (a) the introduction of a carbohydrate which is preferentially used as a carbonand energy source;117,191 (b) an increase in thehydrogen ion concentration which may bringabout a general reduction in bacterial metabo-
<0Adi s International Limited . All right s reserved.
Clausen & Mortensen
lism;117,19,26,421 or (c) both. A direct effect of lactulose in reducing the colonic transit time may alsobe a factor contributing to an increase in faecal soluble nitrogen.
4,2 Role of Short- and Medium-Chain FattyAcids in Hepatic Encephalopathy
The suggestion that SCFA and MCFA may playa role in the pathogenesis of hepatic encephalopathy is mainly based on animal experiments. Samson et aI.i541 investigated the narcotic action ofSCFA (acetate, propionate, butyrate, valerate andhexanoate) and MCFA (heptanoate and octanoate)in experimental animals , Intravenous or intraperitoneal injection of the sodium salt s of theseacids produced a reversible coma with a definiterelationship between the amount of the fatty acidwhich would produce unconsciousness and thecarbon length of the compound; i.e . the longer thecarbon chain, the more potent the encephalopathiceffect, acetate being almost nontoxic.P'l
In a subsequent experiment, White and Samson l551demonstrated that intravenous injection ofpropionate, butyrate, valerate and hexanoate immediately induced electroencephalographic (EEG)changes from a resting type to one of sleep in unanaesthetised rabbits . During these EEG alterations, overt signs of drowsiness or sleep alwaysoccurred and the typical 'alert' EEG responses tonociceptive and auditory stimuli were diminishedor absent. Again , the longer the carbon chain, themore potent the effect. In rats , the rate of bloodbrain barrier penetration of straight-chain saturatedmonocarboxylic acids has also been shown to increase with chain length and is virtually completeat lengths greater than that of hexanoate (C6).1561
In humans, octanoate has been shown to cross theblood-brain barrier in both normal individuals andpatients with cirrhosis.lV'
The mechanisms by which SCFA and MCFA interfere with CNS functions are not entirely clear.In vitro and in vivo stud ies have shown that SCFAand MCFA inhibit cerebral Na+,K+-ATPase activity,15X,591and, as for the narcotic potency, the inhibitory capacity increases with increasing chain
Drugs 1997 Jun; 53 (6)

Disaccharides and Colonic Flora
length.P'" The con sequences of inhibiting this enzyme would include an increase in intracellular sodium and possibl y impaired neurotransmi ssion.
Muto and Takahashi t'v ' were the first to sugges ta role of SCFA in the pathogenesis of hepatic en cephalopathy. In patients with hep ati c coma, pla sma level s of SCFA of 4- to 6-carbon length wereincreased 3- to 4-fold compared with controls andpatients with other kind s of coma. Significantlyelevated levels of SCFA in peripheral venous bloodof patients with fulminant hepatic failure and portal systemic encephalopathy have been confirmedrecently. Lai et al.1611investigated 6 patients withfulminant hepatic failure due to paracetamol (acetaminophen) intoxication and hepatitis. All patientswere in grade IV coma. Pla sma levels of SCFAwere significantly elevated in patients with encephalopathy (2034 ± 11341lmo1/L; mean ±2 SO )compared with 10 healthy controls ( 1113 ± 662um ol/L), but a correlation between SCFA con centrations and the clinical course could not be demonstrated.
Clausen et al.1621inve stigated 32 patients withcirrhosis, 15 patients with and 17 patients withouthepatic ence phalopathy, and II health y indi viduals. Plasma concentrations of SCFA were significantly elevated in patients with hepatic encephalopathy (362 ±831lmo1/L; mean ±SEM) comparedwith patients without encephalopathy ( 178 ± 57umol/L) and healthy controls (60 ± 8IlmoI/L). Repetitive sampling from the encephalopathic patients showed no relationship between SCFA concentrations and the grade of encephalopathy.I '<'
In comparison with the encephalopathy associated with inborn errors of organic acid metabolism, el evated levels of SCFA in patients withhepatic encephalopathy are modest. Massive elevations of propionate are found in severe and fatalca ses of propionic acidaemias (5400 to 38 000IlmoI/L ),1 63-651 and levels of isovalerate in therang e of 340 to 2990 umol/L are associ ated withstupor and unconsciousne ss in children with isovaleric ac idaemia.166,671 Moreover, an 8- to IO-foldrise of venous propionate and oct an oate (C8) isseen in pat ients with liver cirrhos is after duodenal
<D Adis Internat iona l Umited . All rights reserved .
939
or rectal instill ation without any influence on themental or neurological state.16X.691 It thereforeseems unlikely that the elevated level s of SCFA inpatients with hepatic encephalopathy are the pri mary cause of the neurological deterioration ,
A secondary role for SCFA, however, cann ot beexcluded as the coma-producing potential of separate toxic substances may be multiplied severalfold when they are pre sent together. In experimental anima ls the coma-producing effects ofammonia, fatty acid s (octanoate) and mercaptanshave been shown to be strikingly interdependent.170,7!I In healthy animals, the dose of ammonium salt required to produce coma is sharply reduced by the presence of a subcoma dose of eithera fatt y acid (octanoate) or mercaptan.Fv-" Iand theincidence of coma can be raised from zero to 100%by injection of subcoma doses of any of these substances simultaneously. In rats with acute experimental hepatic co ma resulting from massive livernecrosis, the average blood level s of ammoni a, freefatty acids (oc tanoa te) and methanethi ol are muchlower than blood levels required to produce co main health y rats with each of these substances indi vidually. !" I When , however , health y rats are give na combination of doses of ammonia, octan oat e andmercaptan which produce blood level s in the rangeof those obse rved in rats with experiment al hepaticcoma, they becom e cornato se.P!'
4,3 Effect of Lactulose on Colonic SCFAProduction in Hepatic Encephalopathy
Although SCFA may not be the major ca use ofencephalopathy in patients with cirrhosis, the evidence of synergism in animalsl70.71 I sugges ts thatSCFA may playa role as an augmenter or intensifier of other putativ e neurotoxins, e.g. amm oni aand mercaptans. In incubated stool samples, fermentation of lactulose results in the form ation ofacetate prim aril y, whereas bacterial degradation ofblood, albumin and am ino acids significa ntly increases the production of all C2-6-SCFA, es pecially the potentially toxic C4-6-fatt y ac ids .119,431When lactul ose is added to incubations of aminoac ids, protein and blood, the SCFA produ ction is
Drugs 1997Jun: 53 (6)

940
shifted almos t co mpletely toward s the nontox icC2-fatty acid, acetate. At lactul ose concen trationsof 10 to 25 mmol/L, corres ponding to a pH of approximately 5, this effec t is largely mediated by theacidifying effect of lactulose.F'J pH-Independ entinhibition of blood and amino acid degradation toSCFA requires conce ntrations of lactulose exceeding 50 to 100 mmol/L.1431Th e co nce ntratio n oflactul ose after a sing le dose of 20g is 50 to 100mmol/L in the caecum.l''l with a co rres ponding decrease in pH to values in the range of 3.5 to 6.1 inthe prox imal co lon.'6.231
In co ntras t, redu ction of faecal pH by 20 to 40gof lactul ose is small in magnitudelV' or eve n negligiblel'" due to the rapid fermentation of lactul oseand the neutralisation ofluminal co ntents by bicarbonate secretion. The result s obtained in vitro l431
indicate that lactul ose should be given in doses thatnot only acidify the caec um but also exceed thebuffer ing capac ity in the left co lon.
Enemas of lactul ose or glucose may be beneficia l supplemen ts to aid in obtaining this effect.
4,4 Possible Mec hanisms of Ac tion ofLactulose in the Treatment ofHepa tic Encephalopathy
Several mechani sms of action of lactulose in thetreatm ent of hepat ic ence pha lopathy apparentlyex ist (ta ble I). Th ey inc lude: (a) provision of areadi ly fermentable substrate, whic h enco uragesbacteri al proli feration and converts the norm al balance betw een ammonia generation and utili sat ionfrom a net increase to a net decrease (assimil ation) ;(b ) a preferenti al use of lactulose as a carbon andenergy source, which exerts a sparing effect on thebacter ial metabol ism of both exogenous and endogenou s aminated co mpo unds with subsequentdecrease in the generation of ammonia; (c) an acidifyi ng effec t, which brings abo ut a general reductio n in bacterial metabol ism, including that of ammoni a-p rodu cin g bact eria; (d) a laxative ac tion,which reduces the time for the production and absor ption of ammonia and increases the so luble nitrogen content of faeces ; and, (e) an ability to alterthe productio n of SCFA towards the non toxic ace-
'" AdisInternational Umited. All rightsreserved.
Ciali sen & Mortell sen
tate at the ex pense of the potent ially toxic C4-6SCFA.
5. Conclusions
A single primary mech an ism of ac tio n oflactul ose in the treatment of co nsti patio n and hepat ic ence phalopathy cannot be determined due toseveral possible effects the dru g may have. In patient s with consti pation, the laxative effect of lactulose possibly res ults from the combination of: (a)flu id retenti on in the small intestine through theosmo tic act ivity of the unabsorbed disaccharide;and (b) interference with net flu id absorpti on in thecolon due to the osmotic effect of malabso rbed andintact sugars when the bacteri al fermentatio n capacit y is exceeded. However, indivi dual sensi tivities to the drug should be recogni sed, i.e. the therapeutic dose sho uld start at a relat ively low levelwi th a gradual increase according to the frequencyand consistency of the stoo ls.
Th e possibl e mec hanisms by whic h lactulosebenefits patient s with hepat ic encephalopathy incl ude: (a) increased faecal nitrogen excretion; (b)colonic acidification; (c) decreased tra nsit time;and (d) redu ced production of potentially toxicSCFA . In order to ob tain these effects it is recommend ed that the faeca l pH be measured in pat ientswith hepat ic ence phalopathy treated with lactu -
Table I. Possible mechanisms of action of lactulose in the treatmentof hepatic encephalopathy
Effect Result
Utilisation Stimulates bacterial growth and increasesincorporation of ammonia into bacterial protein(assimilation), and exerts a sparing effect on themetabolism of aminated compounds withsubsequent decrease in ammonia generation bycolonic bacteria
Acidifying Brings about a general reduction in bacterialmetabolism, including that of ammonia-producingbacteria
Laxative Reduces the colonic transit time. therebydecreasing the time available both for productionand absorption of ammonia and other potentiallytoxic substances
SCFA Enhances the production of the nontoxic acetatemodification at the expense of the potentially toxic C4-6-SCFA
Abbreviation: SCFA - short-chain fatty acids.
Drugs 1997 Jun: 53 (6)

Disaccharides and Colonic Flora
lose, and that the lactulo se dose should be titratedto pH levels <6 .0. Acidifying enemas, e.g. oflactulo se, lactitol or glucose, may be a beneficialsupplement in obtaining this effect.
ReferencesI. Cummings JH, Macfarlan e GT. The control and consequences
of bacterial fermentation in the human colon . J Appl Bacteriol199 1; 70: 443-59
2. Carulli N, Salv io lo GF, Manent i F. Ahsorpti on of lactulose inman. Digestion 1972; 6: 139-45
3. Saunders DR, Wiggins HS. Co nservation of mannitol , lactulose, and raffinose by the human co lon. Am J Physiol 1981;241 : G397 -402
4. Zarling EJ, Ruchim MA. Protein origin of the volatile fattyacids isobutyrate and isovalerate in human stool. J Lab ClinMed 1987; 109: 566- 70
5. Rasmussen HS, Holtug K, Morten sen PB. Degradat ion ofamino acids to short chain fatty acids in humans: an in vitrostudy. Scand J Gas troentero l 1988; 23: 178-82
6. Florent C, Flourie B, Leblond A, et al. Influence of chroniclactulo se ingestion on the colonic metabol ism of lactulo se inman (an in vivo study). J Cl in Invest 1985; 75: 608-13
7. Hove H, Morten sen PB. Colonic lactate metabolism and D-Iactate acidosis. Dig Dis Sci 1995; 40 : 320-30
8. Bustos D, Pons S, Pernas JC, et al. Fecal lactate and short bowelsyndrome. Dig Dis Sci 1994; 39: 23 15-9
9. Cu mmings JH, Pomare EW, Branch WJ, et al. Short chain fattyacids in human large intes tine, portal, hepatic and venousblood . Gut 1987; 28: 1221-7
10. Mortensen PB, Hove H, Clausen MR, et al. Fermentation toshort-chain fatty acids and lactate in human faecal batch cultures. lntra- and inter-individual var iation s versus variationscaused by changes in ferment ed saccharides. Scand J Gastroenterol 199 1; 26: 1285-94
II. McNeil NI, Cummings JH, James WPT. Short chai n fatty acidabsorption by the human large intestine. Gut 1978; 19: 819-22
12. Ruppin H, Bar-Meir S, Soergel KH, et al. Absorption of shortchain fatty acids by the colon. Gastroenterol ogy 1980; 78:1500-7
13. Roediger WEW. Role of anaerobic bacteria in the metabolicwelfare of the coloni c mucosa in man. Gut 1980; 21: 793-8
14. Clausen MR, Mortensen PB. Kinetic studies on the metaboli smof short-chain fatty acids and gluco se by isolated rat co lonocytes. Gastroenterolo gy 1994 ; 106: 423-32
15. Claus en MR, Morte nsen PB. Kinetic studies on colonocyte metabolism of short -chain fatty acids and glucose in ulcerat iveco litis. Gut 1995; 37: 684- 9
16. McNeil NI. The contribution of the large intestine to energysupplies in man. Am J Clin Nutr 1984 ; 39: 338-42
17. Vince A, Killingley M, Wrong OM. Effect of lactulose on ammonia production in a fecal incubat ion sys tem. Gastroentero logy 1978; 74: 544- 9
18. Mortensen PB, Holtug K, Rasmus sen HS. Short-chain fattyacid producti on from mono- and disaccharides in a fecal incubation system: implication s for colon ic fermentati on of die tary fiber in human s. J Nutr 1988; 118: 321-5
19. Mortensen PB, Rasmus sen HS, Holtug K. Lactulose detoxifi esin vitro short- chain fatty acid production in colonic contentsinduced by blood : implications for hepatic coma. Gastroenterology 1988; 94: 750-4
<0 AdisInternati onal Limited . All rights reserved .
941
20. Peters SG, Poma re EW, Fisher CA. Portal and peripheral bloodshort chain fatty acid concentrations after caecal lactuloseinstillati on at surgery. Gut 1992; 33: 1249-52
21. Bond JH, Levitt MD. Use of pulmonary hydrog en measurements to quantitate carboh ydrate absorption: study of partially gas trectomized patient s. J Clin Invest 1972; 51:1219-25
22. Strocchi A, Cora zza G, Ellis CJ, et al. Detection of malabsorption of low doses of carbohydra tes: accu racy of var ious brea thH2 criteria. Gastroenterology 1993; 105: 1404-10
23. Bown RL, Gibson JA, Siaden GE, et al. Effects of lactu lose andother laxatives on ileal and colonic pH as measured by aradiotelemetry device. Gut 1974; 15: 999- 1004
24. Bircher J, Muller J, Guggenheim P, et al. Treatment of chronicportal- system ic encephalopathy with lactulose. Lancet 1966;I: 890-3
25. Co nn HO, Leev y CM , Vlahcev ic ZR, et al. Co mparison oflactulose and neomycin in the treatment of chronic portal-sys temic encephalopathy: a doubl e blind controlled trial. Gastroentero logy 1977; 72: 573-83
26. Holtug K, Clausen MR, Hove H, et al. The colon in carbohydrate malabsorption: short-chain fatty acid s, pH, and osmoticdiarrhoea. Scand J Gastroenterol 1992; 27: 545-52
27. Conn HO, Floch MH. Effects of lactulose and lactobacillus acidophilus on the fecal flora. Am J Clin Nutr 1970; 23:1588-94
28. Vince A, Zeegen R, Drinkw ater JE, et al. The effect of lactuloseon the faecal nora of patients with hepatic encephalopathy. JMed Microbiol 1974; 7: 163-8
29. Riggio 0 , Varriale M, Testore GP, et al. Effect of lactitol andlactul ose administration on the fecal flora in cirrhotic patients. J Clin Gastroe nterol 1990; 12: 433-6
30. Flourie B, Briet F, Florent C, et al. Can diarrhea induced bylactu lose be reduced by prolonged ingestion of lactulose'? AmJ Clin Nutr 1993; 58: 369-75
3 1. Stephen AM, Cu mmings JH. Mech anism of action of d ietaryfibre in the huma n colon. Nature 1980; 284: 283-4
32. Weber FL. The effect of lactulose on urea metabolism and nitrogen excre tion in cirrhotic patie nts. Gastroe ntero logy 1979;77: 5 18-23
33. Mortensen PB. The effe ct of ora l-administered lactulose on colonic nitrogen metaboli sm and excre tion. Hepatolo gy 1992:16: 1350-6
34. Kot T V, Pett it-Young NA. Lactulose in the management ofconstipation : a cu rrent review. Ann Pharm acother 1992; 26:1277-82
35. Weijers HA, van de Kamer JH, Dicke WK, et al. Diarrhoeacau sed by deficiency of suga r splitting enzymes. ActaPaediatr 1961; 50: 55-71
36. Haemmerli UP, Kistler H, Ammann R, et al. Acquired milkintolerance in the adult caused by lactose malabsorption dueto a selective deficiency of intestinal lactase activity. Am .IMed 1965; 38: 7-30
37. Bustos Fernandez L, Gon zale z E, Marzi A, et al. Feca lacidorrhea. N Engl J Med 1971; 284: 295-8
38. Christopher NL, Bayless TM. Role of the small bowel and colon in lactose-induced diarrh ea . Gastroenterology 1971; 60:845-52
39. Hamm er HF, Santa Ana CA, Schill er LR, et " I. Studies of osmotic diarrhea induced in normal subjects by ingestion ofpolyethylene glycol and lactulose. J Clin Invest 1989; 84:1056-62
Drugs 1997 Jun: 53 (6)

942
40 . Argenzio RA, Moon HW, Kemeny LJ, et al. Colonic compensa tion in transmissible gastroenteritis of swine. Gastroenterology 1984; 86: 1501-9
4 J. Launiala K. The mechanism of diarrhoea in cong enital disaccharide malabsorption. Acta Paediat Scand 1968; 57: 425-32
42 . Perman JA , Modler S, Olson AC. Role of pH in production ofhydrogen from carbohydrates by colonic bacterial flora: studies in vivo and in vitro. J Clin Invest 1981; 67: 643-50
43 . Mortensen PB, Holtug K, Bonnen H, et al. The degradation ofamino acid s, protein s, and blood to short-chain fatty acids incolon is prevented by lactulose. Gastroenterology 1990; 98 :353-60
44 . Phillips SF, Giller J. The contribution of the colon to electrolyteand water conservation in man . J Lab Clin Med 1973; 81:733-46
45 . Bond JH , Levitt MD. Quantitative measurement of lactose absorption. Gastroenterology 1976; 70 : 1058-62
46. Debongnie JC, Phillips SF. Capacity of the human colon toabsorb fluid . Gastroenterology 1978; 74: 698-703
47 . Chauve A, Devroede G, Bastin E. Intraluminal pressures duringperfusion of the human colon in situ. Gastroenterology 1976;70 : 336-40
48 . Zieve L. The mechanism of hepatic coma. Hepatology 1981; I:360-5
49 . Vince A, Down PF, Murison J, et al. Generation of ammoniafrom non-urea sources in a faecal incubation system. Clin SciMol Med 1976; 51 : 313-22
50 . Haemmerli UP, Bircher J . Wrong idea , good results. (Thelactulose story .) N Engl J Med 1969; 281 : 441-2
51 . Zeegen R, Drinkwater JE, Fenton JCB , et al. Some observationson the effects of treatment with lactu lose on patients withchronic hepat ic encephalopathy. Q J Med 1970; 39: 245-63
52. Agostini L, Down PF, Murison J, et al. Faecal ammonia and pHduring lactulose admin istration in man : comparison withother cathartics. Gut 1972; 13: 859-66
53 . Weber FL, Banwell JG , Fresard KM, et al. Nitrogen in fecalbacterial, fiber, and soluble fractions of patients with cirrhosis : effects of lactulose and lactulose plus neomyci n. J LabClin Med 1987; 110: 259-63
54 . Samson FE, Dahl N, Dahl DR. A study on the narcotic actionof the short chain fatty acids. J Clin Inves t 1956; 35 : 1291-8
55. White RP, Samson FE. Effects of fatty acid anions on the electroencephalogram of unanesthetized rabbits. Am J Physiol1956; 186: 271-4
56. Oldendorf WH oCarrier-mediated blood-brain barrier transportof short-chain monocarboxylic organic acids . Am J Physiol1973; 224: 1450-3
57 . Linscheer WG, Blum AL, Platt RR. Transfer of medium chainfatty acids from blood to spinal flu id in patients with cirrhosis.Gastroenterology 1970; 58 : 509- J5
© Adi s International Limited . All right s reserved.
Clausell & Mortellsell
58. Dahl DR. Short chain fatty acid inhibition of rat brain Na-Kadenosine triphosphatase. J Neurochem 1968; 15: 815 -20
59 . Trauner DA. Regional cerebral Na+K+ ATPase activity following octanoate administration. Pediatr Res 1980; 14: 844-5
60 . Muto Y, Takahashi Y. Gas chromatographic determination ofplasma short chain fatty acids in diseases of the liver. J JpnSoc Int Med 1964; 53 : 828-39. Cited in Postgrad Med 1965;37: A 158
61. Lai JCK , Silk DBA , Williams R. Plasma short-chain fatty ac idsin fulminant hepatic failure . Clin Ch im Acta 1977; 78: 305- 10
62 . Clausen MR, Mortensen PB, Bendt sen F. Serum levels of shortchain fatty ac ids in cirrhosis and hepat ic com a. Hepatology1991; 14: W40-5
63. Hommes FA, Kuipers JRG , ElemaJD, et al. Propionicacidemia,a new inborn error of metabolism . Pediatr Res 1968; 2: 519-24
64 . Bran ski D, Gale R, Gross-Kieselstein E, et al. Propion ic acidemia and anorectal anomalies in three siblin gs . Am J Dis Child1977; 131: 1379-81
65 . Hillman RE. Simple, rapid method for determination of propionic acid and other short-chain fatty acids in se rum. ClinChern 1978; 24 : 800-3
66. Budd MA, Tanaka K, Holmes LB, et al. Isovaleric ac ide mia:clinical features of a new genetic defect of leucine metabolism . N Engl J Med 1967; 277 : 321-7
67. Duran M, Sprang FJ van, Drewes JG , et al. Two sisters withisovaleric acidaemia, multiple attacks of ketoac idosis andnormal development. Eur J Pediatr 1979; 131: 205-11
68. Scheppach W, Richter F, Joeres R, et al. Systemic avail abilityof propionate and acetate in liver cirrhosis. Am J Gastroenterol 1988; 83 : 850-3
69. Linscheer W, Castell DO, Platt RR. A new method for evaluation of portosystemic shunting. Gastroenterology 1969; 57:415-23
70. Zieve FJ, Zie ve L, Doi zaki WM, et al. Synergism between ammon ia and fatty acids in the production of coma: implicationsfor hepatic coma. J Pharmacol Exp Ther 1974; 191: 10-6
71. Zieve L, Doizaki WM , Zieve FJ. Synergism between rnercaptans and ammonia or fatty acids in the production of com a: apossible role for mercaptans in the pathogenesis of hepaticcoma. J Lab Clin Med 1974; 83: 16-28
Correspondence and reprints: Dr MetteRyeClausell, Department of Medicine CA 2101, Division of Gastro enterology,Rigshospitalet, Blegdamsvej 9, DK-2100 Cop enhagen 0,Denmark.
Drugs 1997 Jun; 53 (6)