
TraitAnxiety Mediated by Amygdala Serotonin Transporter in ...
Upload
giampaolo-pernaCategory
view
212download
0
American Journal of Medical Genetics Part B (Neuropsychiatric Genetics) 129B:41–43 (2004)
Lack of Relationship Between CO2 Reactivity andSerotonin Transporter Gene Regulatory RegionPolymorphism in Panic DisorderGiampaolo Perna,* Daniela di Bella, Elisa Favaron, Michele Cucchi, Laura Liperi, and Laura Bellodi
Anxiety Disorders Clinical and Research Unit, Istituto Scientifico H. San Raffaele, Vita-Salute University, Milan, Italy
Changes in the function of the serotonergicsystem influence both panic phobic symptomsand carbon dioxide (CO2) reactivity in patientswith panic disorder. Schmidt et al. [2000: JAbnorm Psychol 109(2):308–320] recently report-ed a predictive role of the genetic variants of the5-HTTLPR on the fearful response to CO2 inhealthy controls. We tested the hypothesis thatthe heterogeneity of CO2 reactivity in patientswith panic disorder could be related to the allelicvariation of the 5-HTT promoter. Ninety-five pa-tients with panic disorder were challenged with35% CO2. 5-HTTLPR allelic variation in each sub-ject was determined using a PCR-based method.There were no differences for all the measures ofCO2 reactivity among the genotype groups. CO2
reactivity of patients with panic disorder seemsnot to be influenced by the genetic variants of the5-HTTLPR; this finding does not support a role forthe serotonin transporter in the etiopathogenesisof CO2 reactivity in panic disorder.� 2004 Wiley-Liss, Inc.
KEY WORDS: panic disorder; carbon dioxide;panic provocation; serotonin; 5-HTTLPR; polymorphism
Several experimental evidences have identified hyperreac-tivity to carbon dioxide (CO2) as a putative valid marker inpanic disorder, possibly useful in genetic studies. Hyperreac-tivity tohighdoseCO2might bea traitmarker of panic disordersince it is not significantly influenced by the actual age ofsubjects [Gorman et al., 1990; Perna et al., 1994b], nor bybaseline anxiety levels before the test [Gorman et al., 1990;Perna et al., 1994b], nor by the severity of clinical character-istics of panic disorder (panic attacks, anticipatory anxiety,and phobic avoidance) [Perna et al., 1994b]. Familial and twinstudies supported a role of hyperreactivity to CO2 as a markerof a genetic vulnerability to the panic disease [Perna et al.,1995, 1996; Coryell, 1997; Bellodi et al., 1998; van Beek andGriez, 2000].Hyperreactivity toCO2maybe one of themultiplephenotypes calledpanicdisorderandmaybe theexpressionofagenetic dysfunction in one ormore neurotransmitters systems;thus combining panic provoking challenges with geneticstudies may prove a useful strategy in dealing with themultiple phenocopy problem [Klein, 1998].
Serotonergic system function is linked to both PD andhyperreactivity toCO2.Selective serotonin reuptake inhibitorsdecrease hyperreactivity to CO2; however, this effect was nothomogeneousamongpatients [Bertani et al., 2001;Perna et al.,2002]. Reduced 5-HT availability, that might be explained byenhanced activity of 5HT transporter, is associated with thefearful response to the CO2 challenge [Klaassen et al., 1998;Miller et al., 2000; Schruers et al., 2000]. Thus, the geneencoding for the 5-HTT protein might be a strong candidate inthe explanation of the behavioral hyperreactivity toCO2 inPD.A functional polymorphism in the upstream regulatory regionof serotonin transporter gene (5-HTTLPR) has been identified.It consists of a 44-base pair (bp) insertion/deletion and, in vitro,the basal activity of the long (l) variant was more than twicethat of the short (s) one, suggesting that serotonin transportergene transcription is modulated by such variants [Heils et al.,1996;Leschet al., 1996]. Schmidt et al. [2000] recently reporteda significant difference in subjective reactivity to CO2 inhala-tion between 5-HTTLPR genotype groups in healthy subjects.In their sample, subjects homozygous for the long variant (l)appear to be at risk for behavioral hyperreactivity to the 35%CO2 inhalation test. In the present study, we have tested thehypothesis that the genetic profile of the 5-HTTLPR might beassociated with the reactivity to the 35% CO2 challenge in asample of patients with PD.
Ninety-five patients with PD with/without agoraphobiawere included in the study (53 women and 42 men, mean age34.5� 11.2 years, age at onset: 26.6� 9.9). The patients wereconsecutively recruited over 1 year at the Anxiety DisordersClinical and Research Unit at San Raffaele Hospital in Milan.Seventy-two (76%) admitted to the study had a current historyof agoraphobia. Consensus diagnoses according to DSM IVcriteria were made by two experienced psychiatrists whoindependently assessed patients by a clinical interview and bythe MINI International Neuropsychiatric Interview—Plus[Sheehan et al., 1994]. Criteria for exclusion for all subjectswere significant cardiocirculatory and respiratory disorders,personal and family history of cerebral aneurysm, significanthypertension (systolic> 180 mmHg, diastolic> 100 mmHg),pregnancy or epilepsy, according to direct physical examina-tion and to a careful collection of their medical histories. Atthe time of challenge, subjects had to have not taken anypsychotropic medication for at least 1 week before and theywere asked to abstain from drinking alcohol for at least 36 hr,beverages containing xantines for at least 8 hr, and eatingor smoking for at least 2 hr before the test. The severity ofpanic-phobic symptomatology was measured by the PanicAssociated Symptom Scale (PASS) [Argyle et al., 1991] whichassess frequency and intensity of panic attacks, level ofanticipatory anxiety, and phobic avoidance and by the FearQuestionnaire (FQ) [Marks and Mathews, 1979] to assessphobic symptomatology.
Two different gas mixtures were employed: compressed air(placebo) and a mixture of 35% CO2 and 65% O2. All subjectswere tested according to the method described by Griez et al.[1987]. Immediately before and after each inhalation anxiety
*Correspondence to: Giampaolo Perna, M.D., Ph.D., AnxietyDisorders Clinical and Research Unit, Istituto Scientifico H. SanRaffaele, Vita-Salute University, 20 Via Stamira d’Ancona, 20127,Milan, Italy. E-mail: [email protected]
Received 9 June 2003; Accepted 6 January 2004
DOI 10.1002/ajmg.b.30035
� 2004 Wiley-Liss, Inc.
was evaluated by the Panic Symptom List (PSL IV) [Pols et al.,1991], a self-rating questionnaire assessing the 13 panicsymptoms characteristic of PD on a five-point scale and aVisual Analogue Scale for Anxiety (VAS-A) describing thedegree of global subjective anxiety on a continuum from 0(no anxiety at all) to 100 (the worst anxiety ever imaginable).
The reactivity to 35% CO2 inhalation was evaluated as D%VAS-A [Perna et al., 1996].
The symptomatological reaction to CO2 was evaluated asDPSL IV (PSL IV post inhalation—PSL IV before inhalation)and as DRespiration (subgroup of DPSL considering only therespiratory symptoms: sensations of shortness of breath orsmothering and feeling of choking). According to the idealthreshold obtained by Receiver Operating Characteristic(ROC) analysis of the 35% CO2 challenge, the reaction wasconsidered ‘‘positive’’ if D% VAS-A� 26 and ‘‘negative’’ if D%VAS-A< 26 [Battaglia and Perna, 1995].
Genomic DNA was extracted from whole blood by NaClprecipitation [Lahiri and Nurnberger, 1991]. Target DNA wasamplified by PCR analysis and detected as previously de-scribed [Deckert et al., 1997].
Since psychometric scores in our sample were not normallydistributed—according to Shapiro–Wilks test of normality—we decided to use non parametric testing. Baseline clinical anddemographic characteristics of the patients with PD accordingto the genotype were compared with Kruskall–Wallis testson continuous variables and with chi-square statistics ondichotomous variables.
In order to calculate the minimum effect size detectable byour sample, a power analysis was performed using the Statcalcroutine of EpiInfo 2000 v1.0.
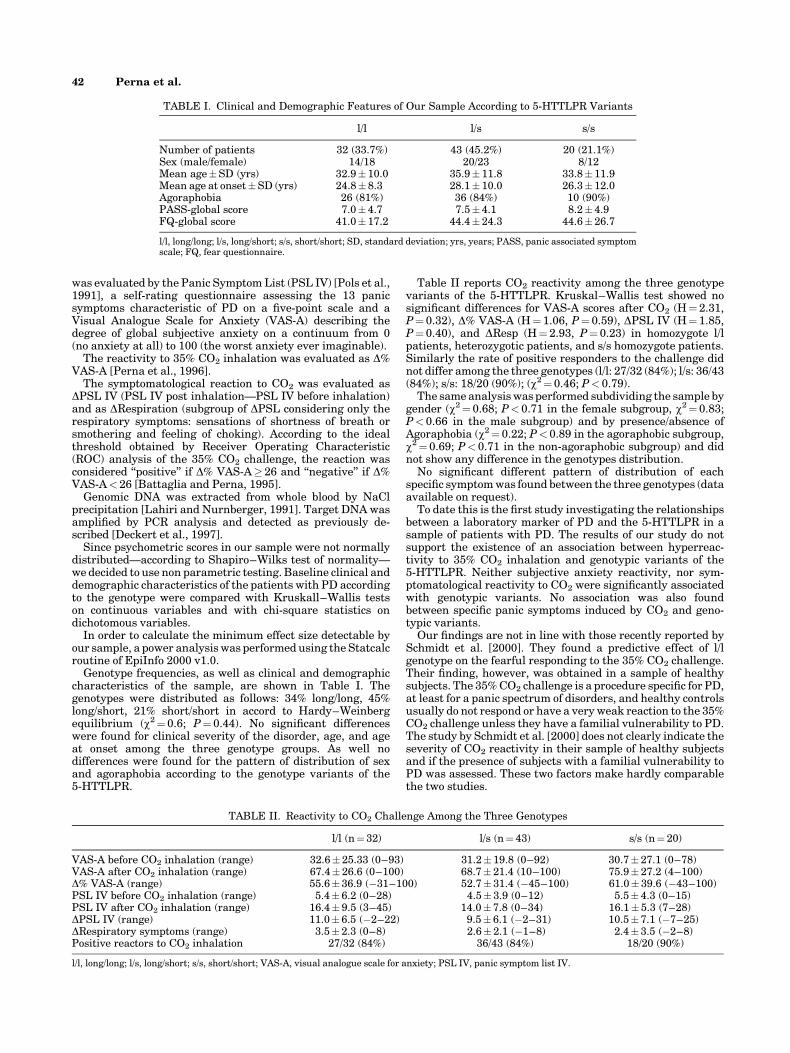
Genotype frequencies, as well as clinical and demographiccharacteristics of the sample, are shown in Table I. Thegenotypes were distributed as follows: 34% long/long, 45%long/short, 21% short/short in accord to Hardy–Weinbergequilibrium (w2¼ 0.6; P¼ 0.44). No significant differenceswere found for clinical severity of the disorder, age, and ageat onset among the three genotype groups. As well nodifferences were found for the pattern of distribution of sexand agoraphobia according to the genotype variants of the5-HTTLPR.
Table II reports CO2 reactivity among the three genotypevariants of the 5-HTTLPR. Kruskal–Wallis test showed nosignificant differences for VAS-A scores after CO2 (H¼ 2.31,P¼ 0.32), D% VAS-A (H¼ 1.06, P¼ 0.59), DPSL IV (H¼ 1.85,P¼ 0.40), and DResp (H¼ 2.93, P¼ 0.23) in homozygote l/lpatients, heterozygotic patients, and s/s homozygote patients.Similarly the rate of positive responders to the challenge didnot differ among the three genotypes (l/l: 27/32 (84%); l/s: 36/43(84%); s/s: 18/20 (90%); (w2¼ 0.46; P< 0.79).
The same analysis was performed subdividing the sample bygender (w2¼ 0.68; P< 0.71 in the female subgroup, w2¼ 0.83;P< 0.66 in the male subgroup) and by presence/absence ofAgoraphobia (w2¼ 0.22; P< 0.89 in the agoraphobic subgroup,w2¼ 0.69; P< 0.71 in the non-agoraphobic subgroup) and didnot show any difference in the genotypes distribution.
No significant different pattern of distribution of eachspecific symptomwas found between the three genotypes (dataavailable on request).
To date this is the first study investigating the relationshipsbetween a laboratory marker of PD and the 5-HTTLPR in asample of patients with PD. The results of our study do notsupport the existence of an association between hyperreac-tivity to 35% CO2 inhalation and genotypic variants of the5-HTTLPR. Neither subjective anxiety reactivity, nor sym-ptomatological reactivity to CO2 were significantly associatedwith genotypic variants. No association was also foundbetween specific panic symptoms induced by CO2 and geno-typic variants.
Our findings are not in line with those recently reported bySchmidt et al. [2000]. They found a predictive effect of l/lgenotype on the fearful responding to the 35% CO2 challenge.Their finding, however, was obtained in a sample of healthysubjects. The 35%CO2 challenge is a procedure specific for PD,at least for a panic spectrum of disorders, and healthy controlsusually do not respond or have a veryweak reaction to the 35%CO2 challenge unless they have a familial vulnerability to PD.The study by Schmidt et al. [2000] does not clearly indicate theseverity of CO2 reactivity in their sample of healthy subjectsand if the presence of subjects with a familial vulnerability toPD was assessed. These two factors make hardly comparablethe two studies.
TABLE I. Clinical and Demographic Features of Our Sample According to 5-HTTLPR Variants
l/l l/s s/s
Number of patients 32 (33.7%) 43 (45.2%) 20 (21.1%)Sex (male/female) 14/18 20/23 8/12Mean age�SD (yrs) 32.9�10.0 35.9� 11.8 33.8�11.9Mean age at onset�SD (yrs) 24.8�8.3 28.1� 10.0 26.3�12.0Agoraphobia 26 (81%) 36 (84%) 10 (90%)PASS-global score 7.0�4.7 7.5� 4.1 8.2�4.9FQ-global score 41.0�17.2 44.4� 24.3 44.6�26.7
l/l, long/long; l/s, long/short; s/s, short/short; SD, standard deviation; yrs, years; PASS, panic associated symptomscale; FQ, fear questionnaire.
TABLE II. Reactivity to CO2 Challenge Among the Three Genotypes
l/l (n¼32) l/s (n¼ 43) s/s (n¼ 20)
VAS-A before CO2 inhalation (range) 32.6�25.33 (0–93) 31.2�19.8 (0–92) 30.7� 27.1 (0–78)VAS-A after CO2 inhalation (range) 67.4�26.6 (0–100) 68.7� 21.4 (10–100) 75.9� 27.2 (4–100)D% VAS-A (range) 55.6� 36.9 (�31–100) 52.7� 31.4 (�45–100) 61.0�39.6 (�43–100)PSL IV before CO2 inhalation (range) 5.4� 6.2 (0–28) 4.5�3.9 (0–12) 5.5� 4.3 (0–15)PSL IV after CO2 inhalation (range) 16.4�9.5 (3–45) 14.0�7.8 (0–34) 16.1�5.3 (7–28)DPSL IV (range) 11.0�6.5 (�2–22) 9.5�6.1 (�2–31) 10.5�7.1 (�7–25)DRespiratory symptoms (range) 3.5� 2.3 (0–8) 2.6� 2.1 (�1–8) 2.4�3.5 (�2–8)Positive reactors to CO2 inhalation 27/32 (84%) 36/43 (84%) 18/20 (90%)
l/l, long/long; l/s, long/short; s/s, short/short; VAS-A, visual analogue scale for anxiety; PSL IV, panic symptom list IV.
42 Perna et al.
The serotonergic systemmodulates the reactivity to the 35%CO2 challenge. Moreover our results do not support a role forthe serotonin transporter in this modulation. Serotonin trans-porter is onekey element in themodulation of the 5-HTsystem,however, the possibility that other polymorphisms in the genecoding for 5-HTT or in the genes coding for other structuresinvolved in serotonergic modulation may be contributing toinfluencing CO2 reactivity, cannot be disregarded.
Moreover, we cannot exclude that our negative finding couldbe related to bias linked to thedimension of our sample or to therecruitment strategy. For a frequency of the risk allele of the5-HTTLPR of 60% and assuming a power of 80% and avalue¼ 0.05, the minimum detectable risk of our sample is 7:consequently we cannot exclude that 5-HTTLPR has a minoreffect in conferring susceptibility to CO2 reactivity.
The genotype distribution of the 5-HT transporter variants,however, is comparable to that of previous studies both inhealthy subjects [Lesch et al., 1996] and in PD [Deckert et al.,1997]. The distribution of genotypes in our sample is alsocomparable to the one observed in the study of Schmidt et al.[2000] that examined the relationships betweenCO2 reactivityand genetic variants of the 5-HTTLPR in healthy controls. Sexand agoraphobia distribution as well as the severity of panic-phobic symptomatology in our patients, which are similar tothose reported in other studies, support the idea that thesample examined represents thegeneral population of patientswith PD.
A possible implication of 5-HTTLPR in panic disorder hasbeen suggested by a positive association between the 5-HTTpolymorphism and anxiety-related personality traits such asneuroticism and harm avoidance, characteristics frequentlyreported in PD [Lesch et al., 1996]. The absence of an asso-ciation between PD and the genotypic variants of the 5-HTTLPR [Deckert et al., 1997; Hamilton et al., 1999], theabsence of a significant relationships between reactivity toCO2
and harm avoidance [Perna et al., 1994a] together with theresults of the present study suggest that 5-HTTLPR is notspecifically related to panic disorder and might have a nonspecific effect on avoidance and anxiety.
ACKNOWLEDGMENTS
We thank Prof. Enrico Smeraldi for sharing his original andinnovative ideas on psychiatric genetics.
REFERENCES
Argyle N, Deltito J, Allerup P, Maier W, Albus M, Nutzinger D, RasmussenS, Ayuso JL, Bech P. 1991. The panic-associated symptom scale:Measuring the severity of panic disorder. Acta Psychiatr Scand 83(1):20–26.
Battaglia M, Perna G. 1995. The 35% CO2 challenge in panic disorder:Optimization by receiver operating characteristic (ROC) analysis.J Psychiatr Res 29(2):111–119.
Bellodi L, PernaG,CaldirolaD,Arancio C, Bertani A,Di BellaD. 1998. CO2-inducedpanic attacks:A twin study.AmJPsychiatry155(9):1184–1188.
Bertani A, Caldirola D, Bussi R, Bellodi L, Perna G. 2001. The 35% CO2
hyperreactivity and clinical symptomatology in patients with panicdisorder after 1week of treatmentwith citalopram:Anopen study. JClinPsychopharmacol 21(3):262–267.
Coryell W. 1997. Hypersensitivity to carbon dioxide as a disease-specifictrait marker. Biol Psychiatry 41(3):259–263.
Deckert J, Catalano M, Heils A, Di Bella D, Friess F, Politi E, Franke P,Nothen MM, Maier W, Bellodi L, et al. 1997. Functional promoterpolymorphism of the human serotonin transporter: Lack of associationwith panic disorder. Psychiatr Genet 7(1):45–47.
Gorman JM, Papp LA, Martinez J, Goetz RR, Hollander E, Liebowitz MR,Jordan F. 1990. High-dose carbon dioxide challenge test in anxietydisorder patients. Biol Psychiatry 28(9):743–757.
Griez EJ, Lousberg H, van den Hout MA, van der Molen GM. 1987. CO2
vulnerability in panic disorder. Psychiatry Res 20(2):87–95.
Hamilton SP, Heiman GA, Haghighi F, Mick S, Klein DF, Hodge SE,Weissman MM, Fyer AJ, Knowles JA. 1999. Lack of genetic linkage orassociation between a functional serotonin transporter polymorphismand panic disorder. Psychiatr Genet 9(1):1–6.
Heils A, Teufel A, Petri S, Stober G, Riederer P, Bengel D, Lesch KP. 1996.Allelic variation of human serotonin transporter gene expression.J Neurochem 66(6):2621–2624.
Klaassen T, Klumperbeek J, Deutz NE, van Praag HM, Griez E. 1998.Effects of tryptophan depletion on anxiety and on panic provoked bycarbon dioxide challenge. Psychiatry Res 77(3):167–174.
Klein DF. 1998. Panic and phobic anxiety: Phenotypes, endophenotypes,and genotypes. Am J Psychiatry 155(9):1147–1149.
Lahiri DK, Nurnberger JI Jr. 1991. A rapid non-enzymatic method for thepreparation of HMW DNA from blood for RFLP studies. Nucleic AcidsRes 19(19):5444.
Lesch KP, Bengel D, Heils A, Sabol SZ, Greenberg BD, Petri S, Benjamin J,Muller CR,HamerDH,MurphyDL. 1996.Association of anxiety-relatedtraits with a polymorphism in the serotonin transporter gene regulatoryregion. Science 274(5292):1527–1531.
Marks IM, Mathews AM. 1979. Brief standard self-rating for phobicpatients. Behav Res Ther 17:263–267.
Miller HE, Deakin JF, Anderson IM. 2000. Effect of acute tryptophandepletion on CO2-induced anxiety in patients with panic disorder andnormal volunteers. Br J Psychiatry 176:182–188.
Perna G, Arancio C, Bertani A, Gabriele A, Bellodi L. 1994a. Personalitydimensions and 35% CO2 reactivity in panic patients and healthycontrols. European Psychiatry 9:236–240.
Perna G, Battaglia M, Garberi A, Arancio C, Bertani A, Bellodi L. 1994b.Carbon dioxide/oxygen challenge test in panic disorder. Psychiatry Res52(2):159–171.
Perna G, Cocchi S, Bertani A, Arancio C, Bellodi L. 1995. Sensitivity to 35%CO2 in healthy first-degree relatives of patients with panic disorder. AmJ Psychiatry 152(4):623–625.
Perna G, Bertani A, Caldirola D, Bellodi L. 1996. Family history of panicdisorder andhypersensitivity toCO2 in patientswith panic disorder. AmJ Psychiatry 153(8):1060–1064.
Perna G, Bertani A, Caldirola D, Gabriele A, Cocchi S, Bellodi L. 2002.Antipanic drug modulation of 35% CO2 hyperreactivity and short-termtreatment outcome. J Clin Psychopharmacol 22(3):300–308.
Pols H, Zandbergen J, de Loof C, Griez E. 1991. Attenuation of carbondioxide-induced panic after clonazepam treatment. Acta PsychiatrScand 84(6):585–586.
Schmidt NB, Storey J, Greenberg BD, Santiago HT, Li Q, Murphy DL.2000. Evaluating gene x psychological risk factor effects in the patho-genesis of anxiety: A new model approach. J Abnorm Psychol 109(2):308–320.
Schruers K, Pols H, Overbeek T, Griez E. 2000. 10 microg CCK-4premedication and 35% CO2 challenge in healthy volunteers. ProgNeuropsychopharmacol Biol Psychiatry 24(3):409–418.
Sheehan DV, Lecrubier Y, Janavs J, Knapp E,Weiler E, Bonora P, SheedanM, Amorim P, Baker R, Sheehan KH, et al. 1994. Mini InternationalNeuropsychiatric Interview. Paris/Tampa: MINI.
van Beek N, Griez E. 2000. Reactivity to a 35% CO2 challenge in healthyfirst-degree relatives of patients with panic disorder. Biol Psychiatry47(9):830–835.
Polymorphism in Panic Disorder 43


















