Laboratory diagnosis of herpesvirus infections of the cns
18
Laboratory diagnosis of herpesvirus infections of the CNS Giorgio Palù, MD Padova University,
-
Upload
carlos-rene-espino-de-la-cueva -
Category
Health & Medicine
-
view
1.705 -
download
1
description
Transcript of Laboratory diagnosis of herpesvirus infections of the cns

Laboratory diagnosis of herpesvirus infections of the CNS
Giorgio Palù, MD Padova University, Italy

Herpesvirus Infections of the CNSVirus Clinical diagnosis
• HSV-1 & 2 Encephalitis, meningitis, Mollaret’s (benign recurrent lymphocytic) meningitis, neonatal
meningoencephalitis and disseminated disease
• VZV Zoster sine herpete, aseptic meningitis, encephalitis, transverse myelitis, CNS vasculitis, cerebellitis
• CMV Encephalitis, polymyeloradiculitis, ventriculitis, myelitis, inflammatory polyneuropathy (predominantly in
AIDS/HIV), congenital CMV
• HHV-6 & 7 Meningoencephalitis, recurrent febrile seizures of childhood, possible association with multiple
sclerosis
• EBV Meningoencephalitis, acute cerebellar ataxia, asepticmeningitis, transverse myelitis, autonomic neuropathy,
primary CNS lymphoma in AIDS
• HHV-8 ???

Diagnosis of CNS Infection
• Standard neurodiagnostic procedures include: – CSF examination– EEG – scanning
• These can be normal in early stages of the disease
Other diagnostic evaluations should be initiated immediately

Role of PCR of CSF
• PCR is the standard method of laboratory diagnosis for many viral CNS infections
• CSF PCR testing may antedate clinically recognizable disease
• Quantitative CSF-PCR may also be useful for monitoring therapy.
• Must be performed by a reliable laboratory

Sensitivity and Specificity of PCR
Virus Sensitivity and specificity
HSV-1 and 2 >95% sensitivity and specificity; quantitative PCR available; potential use in determining course of iv therapy (especially in neonatal disease)
VZV Sensitivity and specificity >95%
CMV Sensitivity nearly 100% in immunosuppressed patients with neurological symptoms; can be quantitated (range:10–104 copies/ml); possible use to monitor therapy. Positive results in 60% of affected infants; correlates with poor neurological outcome
HHV-6 Excellent sensitivity, but poor positive predictive value in clinical disease (30–40% of asymptomatic controls positive)
EBV 98.5% sensitive and 100% specific as a tumour marker

HSV-1/-2 Infection of the CNS
• Serological procedures performed on serum or CSF are not helpful early in the disease course when therapeutic decisions are needed
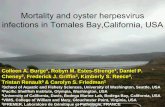
• Detection of viral CSF-PCR is the diagnostic method of choice for confirmation of HSV involvement in CNS disease
• The use of CSF-PCR instead of brain biopsy has expanded awareness of mild or atypical cases (16%-25%)

0%
20%
40%
60%
80%
100%
0% 10% 20% 30%
anti-HSV-2 prevalence
Po
siti
ve P
red
icti
ve V
alu
e
Gull
MRL
POCkit
(Palù et al. Scand.J.Infect.Dis. 2001)
Positive predictive values at different anti-HSV-2 prevalence in the
population

VZV Infection of the CNS
Serum anti-VZV antibody is of no value since VZV antibodies persist in the serum of nearly all adults
BUT
• Testing of CSF for VZV antibodies helps to confirm the role of VZV in producing clinical syndromes of the CNS.
• Diagnosis of VZV infection of the CNS is supported by the detection of VZV antibody in the CSF, even in the absence of PCR-amplifiable VZV DNA
Clinicians should request both PCR and antibody analysis

CMV Infection of the CNS
Diagnosis of CMV-related CNS disease is based upon clinical presentation, neuroradiological studies, CSF chemistries, serological testing, and culture and PCR of CSF
• Clinical presentations of CMV-related CNS disease can be nonspecific
• CSF viral culture can be insensitive • Qualitative DNA PCR can detect both latent and
replicating virus
RT- PCR for specific viral transcripts and quantitative PCR are useful

Measuring HCMV viral load • High systemic CMV load is generally correlated with
CMV disease
• Measuring the viral load at specific sites may help diagnosis when systemic viral load correlates poorly with disease activity
• Quantitation of DNA in both CSF and brain tissue sensitively diagnoses and monitors antiviral treatment, e.g.
– AIDS patients with HCMV-related CNS disease have high quantities of HCMV DNA in their CSF
– Copies of HCMV DNA in CSF are higher in persons with HCMV-related polyradiculopathy than encephalitis
• More data are required on the correlation between changes in viral load, development of resistance, and clinical outcome

HCMV quantitation (methods)
• CMV quantitation can be performed in different fractions of the blood (i.e., cellular fractions and plasma) and organ fluids (e.g., CSF, urine, throat wash, and semen)
• Methods available:– Quantitative viral cultures: plaque assay, determination of TCID50,
shell vial centrifugation cultures– Quantitative pp65 antigenemia– Quantitative PCR– Branched-DNA (bDNA) signal amplification assay – Hybrid capture CMV DNA assay
• The pp65 antigenemia assay appears to be useful as well, especially for patients with polyradiculopathy

Diagnostic accuracy indexes
Gold standard: real-time PCRconcordance kappa sensitivity specificity OR P
pp65 antigen 0.72 0.45 0.65 0.91 19.50 0.0000pp67 RNA 0.41 0.11 0.18 1.00 10.92 0.0137
Gold standard: pp65concordance kappa sensitivity specificity OR P
real-time PCR 0.72 0.45 0.95 0.50 19.50 0.0000pp67 RNA 0.57 0.12 0.20 0.93 3.15 0.0483
Mengoli et al., 2003

HHV-6/-7 Infection of the CNS• Virus Isolation and Assay
• Serological Assays
• Genomic Detection by PCR– Numerous PCR primer sets available for HHV-6 – Reverse transcription–PCR (RT-PCR) assay - latent or
replicating virus?– Quantitative PCR assay - persistence of a high HHV-6 load in
the absence of apparent disease– Multiplex PCR method - simultaneous detection of HHV-6 and
HHV-7CSF-PCR is the technique of choice for the diagnosis of the CNS infection
Brain biopsy recommended to confirm diagnosis in conflicting cases

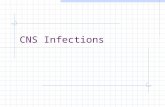
mannitol
ampicillin, acyclovir doxycycline
ceftizoxime, netilmicin
EEG: diffuse irritation chest x-ray: lung consolidation CT: normal LP: bacterial / viral cultures, PCR
CT: diffuse edema LP
extubation
EEG: fewer signs chest x-ray: normal CT: normal LP
1 2 3 4 5 6 12 Days
225
100
75
CS
F c
ells
/l
39.0 38.5 38.0 37.5 37.0
M. pneumoniae: 1:5,120
°C
HHV-6/7: DNA+
M. pneumoniae: DNA+, mRNA - HHV-6/7: mRNA -
(Sgarabotto D. et al, Scand J Infect Dis 2000, 32(6):689-92)
A T
WO
PA
TH
OG
EN
C
AS
E O
F
MEN
ING
OEN
CEP
HA
LIT
IS

EBV Infection of the CNS
• EBV is rarely cultured from CSF during CNS infection
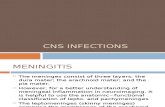
• Quantitative PCR - EBV DNA copy numbers are significantly higher in patients with active EBV infection
• Analysis by RT-PCR of specific viral mRNA
Discrimination between lytic and latent infection is important

0
2
4
6
8
10
12
14
0 20 40 60 80
time (days)
EB
V t
iter
/100
,000
PB
MC
s,
nat
ura
l lo
gar
ith
m
EBV DECAY, RAPID (EARLY) AND SLOW (LATE) COMPONENT
t1/2 early = 29.6 hr
t1/2 late = 111.6 hr
(Biasolo et al, JMedVirol. 2003)

HHV-8???
• The high frequency of HHV-8 in AIDS-related primary CNS non-Hodgkin’s lymphoma in patients with Kaposi's sarcoma suggests that this virus could play a role in the pathogenesis of some cerebral lymphomas.
• This finding needs to be more extensively studied

Conclusions• Herpesvirus infections of CNS are a difficult diagnostic
problem for both clinicians and microbiologists
• As effective antiviral drugs are available, rapid and reliable diagnosis is mandatory
• The isolation of the etiological agent is still important
• The introduction of the non-invasive, rapid and specific CSF-PCR revolutionized the diagnosis of these infections
• Due to the peculiar biological characteristics of the herpesvirus infections, quantitative PCR and discrimination between lytic and latent infection are in many cases essential for the diagnosis