Laboratory Blood Tests Useful in Monitoring Renal Function ...be altered renal function during the...
6
N EONATAL N ETWORK Lab Values Accepted for publication May 2013. Continuing Nursing Education (CNE) Credit A total of 2.1 contact hours may be earned as CNE credit for reading the articles in this issue identified as CNE and for completing an online posttest and evaluation. To be successful the learner must obtain a grade of at least 80% on the test. Test expires three (3) years from publication date. Disclosure: The author/planning committee has no relevant financial interest or affiliations with any commercial interests related to the subjects discussed within this article. No commercial support or sponsorship was provided for this educational activity. ANN/ANCC does not endorse any commercial products discussed/displayed in conjunction with this educational activity. The Academy of Neonatal Nursing is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. Provider, Academy of Neonatal Nursing, approved by the California Board of Registered Nursing, Provider #CEP 6261; and Florida Board of Nursing, Provider #FBN 3218, content code 2505. The purpose of this article is to describe the importance of monitoring renal laboratory values in detecting renal impairment caused by pathophysiology or drug interference for the lab value column. VOL. 33, NO. 1, JANUARY/FEBRUARY 2014 © 2014 Springer Publishing Company 35 http://dx.doi.org/10.1891/0730-0832.33.1.35 Laboratory Blood Tests Useful in Monitoring Renal Function in Neonates Robin B. Knobel, PhD, RN Jennifer Marie Smith, RN, MSN, CPNP T HROUGH A COMPLEX NETWORK OF filtration, secretion, and absorption, the kidneys are largely responsible for main- taining homeostasis in the extracellular envi- ronment. Individuals with poor renal function are at risk for the overaccumulation of waste products and electrolytes (such as potassium [K 1 ]) and subsequent cardiac rhythm distur- bances, metabolic acidosis, hypertension, and fluid overload. 1 In the neonate, where fluid balance is already exquisitely sensitive, kidney malfunction and/or failure can have grave consequences. Because nephrogenesis is still in process when many preterm infants exit fetal development to deliver early, there can be altered renal function during the neona- tal period. It is imperative to monitor renal function and glomerular filtration primarily through laboratory testing of blood creat- inine levels. Blood urea nitrogen (BUN) is another marker of renal function; however, it is largely affected by dietary intake of protein. It is also necessary to assess renal function through laboratory testing during drug treatment because many drugs are toxic to the infant with immature renal function. DEVELOPMENTAL PHYSIOLOGY OF THE RENAL SYSTEM The kidneys are paired organs that lie on opposite sides of the vertebral column near the posterior abdominal wall. The functional unit of the kidney is the nephron; there are approximately a million nephrons in each kidney. 1 Most nephrons are formed from about 20 weeks onward, with nephrogen- esis plateauing around 36 weeks gestational age (GA), which means that interruption of fetal development by premature birth places the infant at risk for alterations in kidney function. 2,3 Within each nephron are a glomerulus, afferent and efferent arterioles, and a series of tubules. Despite nephron weight compromis- ing less than 0.5 percent of the body’s total mass, these highly vascular organs receive 83 mL/minute/1.73m 2 plasma flow by term gestation for filtration. 4 As the infant ages, effective renal plasma flow increases greatly, reaching 650 mL/minute/1.73m 2 by 12–24 months of age. One of the primary functions of the kidney is urine formation, consisting of four basic processes: glomerular filtration, tubular reabsorption, tubular secretion, and urinary excretion (Figure 1). To begin, blood enters the kidneys through the renal arteries and via afferent arterioles (a subdivision of the renal artery) and is brought to the glomerulus for filtration. Once inside the glomerulus, blood encounters the glomerular capillaries, which have pores large enough to facilitate the ABSTRACT It is important to monitor renal function in the neonate, especially in premature infants where nephrogenesis is still in process upon birth. The kidneys are responsible for maintaining homeostasis in the extracellular environment by preventing overaccumulation of waste products and electrolytes. This review describes developmental physiology of the renal system as well as laboratory testing to monitor renal function and glomerular filtration in neonates. Drugs that may affect renal function in infants are also discussed. Keywords: renal function; creatinine; GFR; BUN; neonatal renal lab tests
Transcript of Laboratory Blood Tests Useful in Monitoring Renal Function ...be altered renal function during the...

N E O N A T A L N E T W O R K
Lab Values
Accepted for publication May 2013.
Continuing Nursing Education (CNE) Credit
A total of 2.1 contact hours may be earned as CNE credit for reading the articles in this issue identified as CNE and for completing an online posttest and evaluation. To be successful the learner must obtain a grade of at least 80% on the test. Test expires three (3) years from publication date. Disclosure: The author/planning committee has no relevant financial interest or affiliations with any commercial interes ts related to the subjects discussed within this article. No commercial support or sponsorship was provided for this educational activity. ANN/ANCC does not endorse any commercial products discussed/displayed in conjunction with this educational activity.
The Academy of Neonatal Nursing is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center ’s Commission on Accreditation.
Provider, Academy of Neonatal Nursing, approved by the California Board of Regis tered Nursing, Provider #CEP 6261; and Florida Board of Nursing, Provider #FBN 3218, content code 2505.
The purpose of this article is to describe the importance of monitoring renal laboratory values in detecting renal impairment caused by pathophysiology or drug interference for the lab value column.
V O L . 3 3 , N O . 1 , J A N U A R Y / F E B R U A R Y 2 0 1 4 © 2 0 1 4 S p r i n g e r P u b l i s h i n g C o m p a n y 3 5 http://dx.doi.org/10.1891/0730-0832.33.1.35
Laboratory Blood Tests Useful in Monitoring Renal Function in NeonatesRobin B. Knobel, PhD, RN Jennifer Marie Smith, RN, MSN, CPNP
Through a complex neT wor k of
filtration, secretion, and absorption, the kidneys are largely responsible for main-taining homeostasis in the extracellular envi-ronment. Individuals with poor renal function are at risk for the overaccumulation of waste products and electrolytes (such as potassium [k1]) and subsequent cardiac rhythm distur-bances, metabolic acidosis, hypertension, and fluid overload.1 In the neonate, where fluid balance is already exquisitely sensitive, kidney malfunction and/or failure can have grave consequences. Because nephrogenesis is still in process when many preterm infants exit fetal development to deliver early, there can be altered renal function during the neona-tal period. It is imperative to monitor renal function and glomerular filtration primarily through laboratory testing of blood creat-inine levels. Blood urea nitrogen (Bun) is another marker of renal function; however, it is largely affected by dietary intake of protein. It is also necessary to assess renal function through laboratory testing during drug treatment because many drugs are toxic to the infant with immature renal function.
DEVELOPMENTAL PHYSIOLOGY OF THE RENAL SYSTEM
The kidneys are paired organs that lie on opposite sides of the vertebral column near
the posterior abdominal wall. The functional unit of the kidney is the nephron; there are approximately a million nephrons in each kidney.1 most nephrons are formed from about 20 weeks onward, with nephrogen-esis plateauing around 36 weeks gestational age (ga), which means that interruption of fetal development by premature birth places the infant at risk for alterations in kidney function.2,3
within each nephron are a glomerulus, afferent and efferent arterioles, and a series of tubules. Despite nephron weight compromis-ing less than 0.5 percent of the body’s total mass, these highly vascular organs receive 83 ml/minute/1.73m2 plasma f low by term gestation for filtration.4 as the infant ages, effective renal plasma f low increases greatly, reaching 650 ml/minute/1.73m2 by 12–24 months of age.
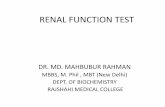
one of the primary functions of the kidney is urine formation, consisting of four basic processes: glomerular filtration, tubular reabsorption, tubular secretion, and urinary excretion (figure 1). To begin, blood enters the kidneys through the renal arteries and via afferent arterioles (a subdivision of the renal artery) and is brought to the glomerulus for filtration. once inside the glomerulus, blood encounters the glomerular capillaries, which have pores large enough to facilitate the
AbstrAct
It is important to monitor renal function in the neonate, especially in premature infants where nephrogenesis is still in process upon birth. The kidneys are responsible for maintaining homeostasis in the extracellular environment by preventing overaccumulation of waste products and electrolytes. This review describes developmental physiology of the renal system as well as laboratory testing to monitor renal function and glomerular filtration in neonates. Drugs that may affect renal function in infants are also discussed. Keywords: renal function; creatinine; gfr; Bun; neonatal renal lab tests

3 6 J A N U A R Y / F E B R U A R Y 2 0 1 4 , V O L . 3 3 , N O . 1N E O N A T A L N E T W O R K
passage of water and solutes (but not red blood cells [RBCs], white blood cells [WBCs], or platelets) out of the blood and into the glomerulus. Here the fi ltration process begins. The functional measurement of this process is called the glomeru-lar fi ltration rate (GFR), which is the volume of fi ltrate pro-duced per minute by both kidneys. After birth, renal blood fl ow increases because of an increased cardiac output and decreased vascular resistance that increases GFR. 5 The GFR doubles in the fi rst two weeks of life in a term newborn. 6,7
Preterm and very low birth weight (VLBW) infants have higher GFRs because nephron development is not complete until 35 weeks gestation, and those born before this time will be defi cient in the overall number of nephrons. 8
Fluid enters the glomerular capsule under hydrostatic pres-sure and begins its journey through Bowman’s space and into the proximal tubule. Once inside the proximal tubule, fl uid is isosmotic with the plasma, and a concentration gradient must be established for fi ltration. Sodium (Na � ) is actively transported out of the fi ltrate and into the plasma. Glucose is cotransported with Na � , and chloride (Cl � ) follows into the
plasma because of the electrical gradient. Water additionally follows passively because of osmosis. This movement leaves approximately one-third of the total volume of the ultrafi ltrate remaining to travel onward to the loop of Henle. 9
Once in the ascending loop of Henle, Na � once again is actively removed from the filtrate. Just as in the proximal tubule, Cl � passively follows; however, the ascending loop is not permeable to water, which causes the remaining ultrafi l-trate to become more dilute. As the ultrafi ltrate then travels into the descending loop of Henle, permeability reverses. Here, the thick walls of the loop are permeable to water but not to solutes. Water is removed by osmosis; thus the remaining fi ltrate becomes more concentrated. Ultimately, the concentration of Na � at the conclusion of the descending loop of Henle is even higher than the initial concentration prior to its arrival in the ascending loop. 10 In the neonate as well as a premature infant, tubular thresholds are reduced, and thus more electrolytes such as Na � and glucose are excreted into the urine. 10
Fluid then moves through the distal tubule into the col-lecting ducts. The medullary tissue surrounding the ducts is
FIGURE 1 � Kidney nephron function in urine formation.
Illustration by Michal Komorniczak (Poland).

V O L . 3 3 , N O . 1 , J A N U A R Y / F E B R U A R Y 2 0 1 4 3 7N E O N A T A L N E T W O R K
hypertonic compared with the ultrafiltrate, which promotes the passage of the remaining water back into systemic circula-tion. Permeability of the distal tubules can be altered by the amount of antidiuretic hormone (ADH) in the blood. In the case of dehydration, ADH secretion will rise, increasing the permeability of the collecting ducts, which leads to increased water absorption to rehydrate the body. The distal tubules are also regulated by aldosterone, which stimulates the reabsorp-tion of Na1 and subsequent wasting of K1.11
From the distal tubules, the ultrafiltrate travels through the collecting ducts and ultimately through the ureters to the urinary bladder, where it is then excreted through the urethra out of the body as urine. Fetal urine production begins at nine to ten weeks gestation and makes up much of the amniotic fluid.12,13
Many different factors may affect preterm kidney func-tion including intrauterine and extrauterine growth restric-tion, administration of maternal steroids, postnatal exposure to oxygen, and administration of nephrotoxic drugs during the neonatal period.2 Clinical diagnoses and conditions asso-ciated with renal dysfunction are vasopressor use during the first week of life, Grade 3 or 4 intraventricular hemorrhage, a patent ductus arteriosus (PDA), necrotizing enterocolitis, use of indomethacin, positive blood cultures, and use of high- frequency ventilation.14 GFR can also be decreased as the result of a profound stimulation of the sympathetic nervous system, such as with hypoxic ischemic brain injury or as the result of other defensive mechanisms in the body, which the neonate may employ during stress reactions.15 Because these factors are usual occurrences in the neonatal period, we must assess renal function with laboratory testing. By evaluating renal function through serial testing, we can adjust medication dosing, plan fluid management, and provide electrolyte support.
Glomerular Filtration Rate (GFR)Renal function can be assessed through measurement of
the GFR. The GFR can be measured directly using inulin or indirectly through creatinine and BUN. Efficacy of the renal clearance system or GFR is the sum of the filtration rates in all functioning nephrons. The GFR varies with gender, body size, and gestational and postnatal age.16 The GFR is sig-nificantly decreased in preterm infants compared with term infants and will reach adult levels by one to two years of age (please see Table 1 for GFR rates).
The GFR can be assessed by measuring inulin clearance, a substance that is freely filtered with a stable plasma concen-tration, to estimate the actual number of functioning neph-rons.1 This exogenous starch-like fructose polymer is not metabolized, reabsorbed, or secreted by the renal tubules, making it a good marker for glomerular filtration.17 However, inulin measurement can be difficult and often inaccurate. It is also said to contain bacteria, which is not suitable for use in the neonatal population. Because of this, creatinine, another substance with a stable plasma concentration, is often used as an indirect measure of renal function.
CreatinineCreatinine is released into circulation following the metab-
olism of creatine and phosphocreatine in the muscles17 and correlates with muscle mass.1 It is used as a gross estimate of the GFR because it is secreted into the blood at a steady rate and is freely filtered at the glomerulus.10
The GFR is usually measured using serum creatinine (SCr) levels in most neonatal intensive care units (NICUs) based on the Schwartz formula,17,18 which relates creatinine clearance to body length and plasma creatinine values. Historically, the Jaffe reaction had been the standard for most routine assays of creatinine19; however, this method can substantially over-estimate SCr levels because of the presence of pseudochro-mogenic constituents in the blood such as proteins,1 and bilirubin presence causes a major problem when the Jaffe reaction is used in neonates. Modern testing is now achieved with enzymatic methods.20 The GFR is estimated from SCr and infant characteristics such as weight, gender, and age. The amount of creatinine filtered is approximately the same as the amount excreted (plus a small amount secreted by the kidney tubules).15 Creatinine levels and GFR are inversely related. When GFR declines, creatinine increases propor-tionally; thus, a high creatinine level is indicative of a poorly functioning kidney. In addition, creatinine takes seven to ten days to stabilize with a declining GFR and is therefore a good indication of chronic rather than acute kidney function.21,22
Immediately after birth, infant SCr levels reflect maternal levels and can be as high as 1.1 mg/dL (97 mol/L).17,22,23 In infants, normal values are 0.2–1 mg/dL (17.6–88.4 mol/L) on DOL 1 to 3 and decreasing to 0.2–0.5 mg/dL (17.6–44.2 mol/L) by one year.9 Levels in the first week of life may vary according to the infant’s hydration and clinical status. Creatinine levels undergo a rapid decline from birth through the first year of life, reaching values 50 percent less than those at birth.19 Assessing creatinine levels as a marker for GFR in premature infants can be difficult. Creatinine clearance increases with increased GA7; however, there is no significant relationship between creatinine levels and gender, weight, and height.19 In VLBW infants, SCr levels are found to peak at DOL 2 to 3 and then decrease postnatally with a plateau at four to five days of age.17,24 However, plasma creat-inine levels may take a month to normalize in VLBW infants. Auron and Muhanna found that newborn infants less than
TABLE 1 n Glomerular Filtration Rates by Gestational Age and Postnatal Age5,10,17
Infant Glomerular Filtration Rate
Term newborn 20–25 mL/min/1.73m2
Term 2–4 weeks old 50 6 10 mL/min/1.73m2
Term .30 days 100–130 mL/min/1.73m2
Preterm 25 weeks GA 2 mL/min/1.73m2
Preterm 27–31 weeks GA by 7 days 8–29 mL/min/1.73m2
Preterm 27–31 weeks GA by 21 days 13–35 mL/min/1.73m2

3 8 J A N U A R Y / F E B R U A R Y 2 0 1 4 , V O L . 3 3 , N O . 1N E O N A T A L N E T W O R K
29 weeks GA had a delay in the decrease of SCr, but by DOL 5, SCr levels began to decrease with increased GA and weight.24 Until DOL 4, SCr levels increase in preterm infants because of tubular reabsorption. SCr levels may also underestimate GFR in VLBW infants because of the passive reabsorption of fil-trated creatinine across the premature kidney because of leaky renal tubules.17 Premature infants have short renal tubules that limit reabsorption ability, high renal artery resistance, low renal blood flow, and low permeability to the glomerular membrane. Therefore, without efficient renal tubules, creati-nine leaks through the tubules and is elevated in the blood. For these reasons, it is better to periodically measure SCr levels for trends rather than diagnose renal problems based on a single creatinine measurement. Researchers have suggested that a persistent elevated SCr level more than 1.5 mg per 100 mL (132.5 mol/L), especially after values have normalized early in the neonatal period, is suggestive of acute renal failure.25,26
Blood Urea Nitrogen (BUN)The BUN is another marker of kidney function that repre-
sents glomerular filtration and urine-concentrating capacity.10 Urea, a by-product of protein metabolism that is formed in the liver from amino acids and ammonia, is filtered through the glomerulus; thus, as GFR decreases, BUN increases. An elevated BUN is indicative of an infant’s limited ability to con-centrate urine with urea solute and may also be associated with increased protein intake through hyperalimentation or formula. The urinary urea solute content of an infant is about half that of an adult.27 Researchers have found that, despite attempts to increase urinary urea solute content in infants through increased dietary intake of protein, infants are unable to concentrate their urine. Balakrishnan and colleagues found that, for every gram per kilogram of protein intake per day, they saw an increase in BUN of 3.3 mg/dL (urea 1.17 mmol/L).28 These research-ers found BUN values were also increased in association with increased age in premature infants. They saw a range of BUN values from 6 to 43 mg/dL (urea 2.14–15.4 mmol/L) with a mean of 20.9 mg/dL (urea 7.45 mmol/L) on DOL 1 and a range from 8 to 110 mg/dL (Urea 2.86–39.27 mmol/L) with a mean of 36 mg/dL (12.85 mmol/L) on DOL 7. Normal values are 7–20 mg/dL (2.49–7.15 mmol/L) in adults and 5–17 mg/dL (1.78–6.07 mmol/L) in children one to three years. It is very difficult to state “normal ranges” for infants because of the association between BUN, postnatal age, and dietary intake of protein, but, once infants are able to concentrate urine with urea solutes equally to adults, BUN values should approach lower ranges. BUN may be elevated because of a lower GFR as a result of dehydration and hypotension; however, BUN may also be elevated in response to increased protein intake and catabolism. Therefore, it is not the first choice for estimating GFR.29 BUN measurement has also been discounted as an ade-quate estimation of protein intake in extremely low birth weight (ELBW) infants because researchers have found such wide vari-ations in the correlation between BUN and protein intake, with some studies reporting no correlation.27–29
MEDICATIONS AND RENAL FUNCTIONPremature infants have decreased GFR and tubular func-
tion and are slower to metabolize drugs when compared with term infants. Infants do not have the ability to metab-olize drugs as efficiently as adults until they reach approxi-mately one year of age.16,30 Some drugs are nephrotoxic and, when administered to an immature kidney with decreased renal function, can cause permanent damage. Therefore, it is important to monitor renal function in relationship to GA and SCr levels to assess drug clearance in the neonatal period to prevent drug toxicity. Drug dosing is based on recom-mended doses for GA and postnatal age obtained through research studies and specified in neonatal drug books. Care providers then calculate expected peak and trough levels of each antibiotic and draw drug levels at the appropriate time for each drug to assess dosing and clearance of the drug.
Aminoglycosides and Glycopeptide AntibioticsAminoglycosides and glycopeptide antibiotics are elimi-
nated through the kidneys.31 Amikacin and vancomycin clear-ance can also be predicted with GFR related to GA. These drugs are almost exclusively cleared by glomerular filtration because of decreased ability of immature renal tubules to secrete drugs.32 Prematurity is not the only factor limiting glo-merular filtration and renal tubule function. Being small for gestational age (SGA) or growth restricted has an effect on the kidney size, the number of nephrons, the GFR, and the tubular function. Thus, these infants also have an inefficient ability to clear drugs. In a study of 531 infants by Allegaert and col-leagues,31 SGA preterm infants had a decreased renal clearance by 16.2 percent of amikacin and vancomycin up to four weeks of age. This decreased renal clearance was comparable to the decreased creatinine clearance documented in SGA preterm infants.31 Administration of ibuprofen to infants on vanco-mycin reduces the clearance of vancomycin by 50 percent.33 Concurrent administration of indomethacin has a higher effect than ibuprofen on reducing clearance of vancomycin.34
Gentamicin is frequently used in early and late sepsis for such gram-negative organisms as Escherichia Coli, Enterococci, Pseudomonas, and Klebsiella and as adjunct therapy for Group B streptococci.35 Gentamicin impairs bac-terial protein synthesis, is able to penetrate cell walls of gram-negative bacteria, and leads to cell death of these bacterial microorganisms. The goal of any antibacterial therapy is to achieve therapeutic ranges as quickly and efficiently as pos-sible without toxic side effects. Increased peak concentrations of gentamicin are associated with an increased chance of sur-vival and a better therapeutic response. Gentamicin is largely processed through glomerular filtration; however, some gen-tamicin is processed through the renal tubules. High levels of gentamicin can accumulate in the renal tubules and lead to tubular cell necrosis.36 In addition, too high a concentration of gentamicin can impair protein synthesis of infant cells and manifests as nephrotoxicity and/or ototoxicity. Therefore, we monitor peak blood levels to achieve the concentration

V O L . 3 3 , N O . 1 , J A N U A R Y / F E B R U A R Y 2 0 1 4 3 9N E O N A T A L N E T W O R K
needed to cause cell death in the bacteria without exceeding the concentration that may cause toxicity. The peak level is drawn right after the drug is administered to find the highest blood level. The trough blood level is drawn right before the next dose to confirm that the lowest acceptable therapeutic level is achieved. If levels are not in the desired range, dosing and administration times can be adjusted by the care pro-vider to maximize efficacy and minimize toxicity.
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)Nonsteroidal anti-inflammatory drugs (NSAIDs), such as
ibuprofen and indomethacin, are known to have a deleteri-ous effect on the developing kidney.37 These drugs have been shown to delay the normal increase in GFR that happens as a premature infant advances postnatal age, which can lead to a decreased urinary output. Research on clearance of ibuprofen given for prophylaxis or treatment of a PDA during the neona-tal period showed that the GFR was significantly decreased in the infants treated with ibuprofen and the reduction in GFR could persist through one month of age.38 These researchers also found that ibuprofen was more nephrotoxic than ami-noglycosides, glycopeptides, and other drugs usually given during the first week of life.39 Nurses should watch urine output during the administration of NSAIDs and monitor creatinine levels to assess GFR.
RENAL MONITORING THROUGH ASSESSMENT OF URINE OUTPUT AND LABORATORY TESTING
In healthy nonhospitalized full-term neonates, an assess-ment of renal function is merely the number of wet diapers per day. By DOL 5, infants should have 6–8 colorless voids/day.9 In hospitalized neonates where there is concern about renal function, more specific measures should be taken to assess for adequate urine output (at least 0.5–1.0 mL/kg/h). Output can be monitored through catheterization, urine bags, or preferably by weighing diapers. In addition, weight, serum Na1, serum K1, and creatinine should be moni-tored in high-risk infants.40 BUN is not included on this list because it reflects nutritional status and nitrogen load rather than fluid status (which is a truer indication of renal function in the neonate).
SUMMARYRenal development is a vital contributor to overall fetal
health because of its close link with pulmonary development and the central role of the kidneys in regulation of homeosta-sis. At birth, renal perfusion is greatly increased, resulting in decreased GFR and increased levels of BUN and creatinine. As the renal system matures, the GFR will increase and BUN and creatinine will decrease to adult levels. Monitoring the GFR through creatinine levels as well as monitoring clinical factors and assessing GA, postnatal age, weight, and gender will improve proper assessment of renal status and apprecia-tion of drug dosing and clearance.
REFERENCES 1. Guignard J. Postnatal development of glomerular filtration rate in neonates.
In: Polin RA, Fox WW, Abman SH, eds. Fetal and Neonatal Physiology. Vol 2. 4th ed. Philadelphia, PA: Elsevier Saunders; 2011:1339-1349.
2. Gubhaju L, Sutherland MR, Black MJ. Preterm birth and the kidney: implications for long-term renal health. Reprod Sci. 2011;18:322-333.
3. Hinchliffe SA, Sargent PH, Howard CV, Chan YF, van Velzen D. Human intrauterine renal growth expressed in absolute number of glomeruli assessed by the disector method and Cavalieri principle. Lab Invest. 1991;64:777-784.
4. Solhaug MJ, Jose PA. Postnatal maturation of renal blood flow. In: Polin RA, Fox WW, Abman SH, eds. Fetal and Neonatal Physiology. Vol 2. 4th ed. Philadelphia, PA: Elsevier Saunders; 2011:1323-1329.
5. Hunley TE, Kon V, Ichikawa J. Glomerular Circulation and Function. Philadelphia, PA: Springer Publishing Company; 2009.
6. Aperia A, Broberger O, Elinder G, Herin P, Zetterström R. Postnatal development of renal function in pre-term and full-term infants. Acta Paediatr Scand. 1981;70:183-187.
7. Bueva A, Guignard J. Renal function in the preterm neonate. Pediatr Res. 1994;36:572-577.
8. Baum M, Quigley R, Satlin LM. Postnatal renal development. In: Alpern RJ, Hebert SC, eds. Seldin and Giebisch’s the Kidney: Physiology and Pathophysiology. 4th ed. New York, NY: Saunders Elsevier; 2008:707-722.
9. Blackburn S. Maternal, Fetal, & Neonatal Physiology. St. Louis, MO: Saunders Elsevier; 2007.
10. Huether SE. Structure and Function of the Renal and Urologic Systems. 5th ed. Philadelphia, PA: Elsevier Mosby; 2006.
11. Feld LG, Corey HE. Renal transport of sodium during early development. In: Polin RA, Fox WW, Abman SH, eds. Fetal and Neonatal Physiology. Vol 2. 4th ed. Philadelphia, PA: Elsevier Saunders; 2011:1349-1361.
12. Engle W. Development of fetal and neonatal renal function. Semin Perinatol. 1986;10(2):113-124.
13. Chevalier R. Developmental renal physiology of the low birth weight pre-term newborn. J Urol. 1996;156(2, pt 2):714-719.
14. Walker MW, Clark RH, Spitzer AR. Elevation in plasma creatinine and renal failure in premature neonates without major anomalies: terminology, occurence and factors associated with increased risk. J Perinatol. 2011;31:199-205.
15. Guyton A, Hall J. Textbook of Medical Physiology. 10th ed. Philadelphia, PA: W.B. Saunders Co; 2005.
16. van der Heijden AJ, Grose WF, Ambagtsheer JJ, Provoost AP, Wolff ED, Sauer PJ. Glomerular filtration rate in the preterm infant: the relation to gestational and postnatal age. Eur J Pediatr. 1988;148:24-28.
17. Hoseini R, Otukesh H, Rahimzadeh N, Hoseini S. Glomerular function in neonates. Iran J Kidney Dis. 2012;6:166-172.
18. Schwartz GJ, Brion LP, Spitzer AR. The use of plasma creatinine concentration for estimating glomerular filtration rate in infants, children, and adolescents. Pediatr Clin North Am. 1987;34:571-590.
19. Boer DP, de Rijke YB, Hop WC, Cranberg K, Dorresteijn EM. Reference values for serum creatinine in children younger than 1 year of age. Pediatr Nephrol. 2010;25:2107-2113.
20. Cobbaert CM, Baadenhuijsen H, Weykamp CW. Prime time for enzymatic creatinine methods in pediatrics. Clin Chem. 2009;55:549-558.
21. Guignard JP, Drukker A. Why do newborn infants have a high plama creatinine? Pediatrics. 1999;103:e49.
22. Miall LS, Henderson MJ, Brownlee KG, Brocklebanck JT, Newell SJ, Allgar VL. Plasma creatinine rises dramatically in the first 48 hours of life in preterm infants. Pediatrics. 1999;104:e76.
23. Lao TT, Loong EP, Chin RK, Lam YM. Renal function in the newborn: newborn creatinine related to birth weigh, maturity and maternal creatinine. Gynecol Obstet Invest. 1989;28:70-72.

4 0 J A N U A R Y / F E B R U A R Y 2 0 1 4 , V O L . 3 3 , N O . 1N E O N A T A L N E T W O R K
24. Auron A, Mhanna MJ. Serum creatinine in very low birth weight infants during their first days of life. J Perinatol. 2006;26:755-760.
25. Chevalier RL, Campbell F, Brenbridge AN. Prognostic factors in neonatal acute renal failure. Pediatrics. 1984;74:265-272.
26. Stapleton FB, Jones DP, Green RS. Acute renal failure in neonates: incidence, etiology and outcome. Pediatr Nephrol. 1987;1:314-320.
27. Linshaw MA. Concentration and dilution of the urine. In: Polin RA, Fox W, Abman SH, eds. Fetal and Neonatal Physiology. Vol 2. 4th ed. Philadelphia, PA: Elsevier Saunders; 2011:1392-1418.
28. Balakrishnan M, Tucker R, Stephens BE, Bliss JM. Blood urea nitrogen and serum bicarbonate in extremely low birth weight infants receiving higher protein intake in the first week after birth. J Perinatol. 2011;31:535-539.
29. Roggero P, Gianni ML, Morlacchi L, et al. Blood urea nitrogen concentrations in low-birth-weight preterm infants during parenteral and enteral nutrition. J Pediatr Gastroenterol Nutr. 2010;51:213-215.
30. Mannan MA, Shahidulla M, Salam F, Alam MS, Hossain MA, Hossain M. Postnatal development of renal function in preterm and term neonates. Mymensingh Med J. 2012;21:103-108.
31. Allegaert K, Anderson BJ, van den Anker JN, Vanhaesebrouck S, de Zegher F. Renal drug clearance in preterm neonates: relation to prenatal growth. Ther Drug Monit. 2007;29:284-291.
32. Allegaert K, Verbesselt R, Naulaers G, et al. Developmental pharmacology: neonates are not just small adults. Acta Clin Belg. 2008;63:16-24.
33. Asbury WH, Darsey EH, Rose WB, Murphy JE, Buffington DE, Capers CC. Vancomycin pharmacokinetics in neonates and infants: a restrospective evaluation. Ann Pharmacother. 1993;27:490-496.
34. Allegaert K. The impact of ibuprofen or indomethacin on renal drug clearance in neonates. J Matern Fetal Neonatal Med. 2009;22(suppl 3):88-91.
35. Touw DJ, Westerman EM, Sprij A. Therapeutic drug monitoring of aminoglycosides in neonates. Clin Pharmacokinet. 2009;48:71-88.
36. Martinez-Salgado C, Lopez-Hernandez FJ, Lopez-Novos JM. Glomerular nephrotoxicity of aminoglycosides. Toxicol Appl Pharmacol. 2007;223:86-98.
37. Giniger R, Buffat C, Millet V, Simeoni U. Renal effects of ibuprofen for the treatment of patent ductus arteriosus in premature infants. J Matern Fetal Neonatal Med. 2007;20:275-283.
38. Vieux R, Desandes R, Boubred F, et al. Ibuprofen in very preterm infants impairs renal function for the first month of life. Pediatr Nephrol. 2010;25:267-274.
39. Vieux R, Fresson J, Guillemin F, Hascoet JM. Perinatal drug exposure and renal function in very preterm infants. Arch Dis Child Fetal Neonatal Ed. 2011;96:F290-F295.
40. Hartnoll G. Basic principles and practical steps in the management of fluid balance in the newborn. Semin Neonatol. 2003;8:307-313.
About the AuthorsRobin Knobel, PhD, RN, is an assistant professor at Duke
University School of Nursing where she teaches in the graduate nursing programs. Dr. Knobel practiced as a neonatal nurse for 13 years and then as a neonatal nurse practitioner for 15 years. Her interdisciplin-ary research focuses on basic physiologic processes related to body temper-ature and perfusion in extremely premature infants. She has a research grant from the National Institutes of Health (National Institute of Nursing Research), and she is a Robert Wood Johnson Foundation Nurse Faculty Scholar (2010–2013).
Jennifer Marie Smith, RN, MSN, CPNP, received her BA at the University of Notre Dame and both her BSN and MSN at Duke University. She is currently a pediatric nurse practitioner at Western Wake Pediatrics in Cary, North Carolina.
For further information, please contact: Robin B. Knobel, PhD, RN Duke University School of Nursing Box 3322 DUMC, 307 Trent Dr. Durham, NC 27710 E-mail: [email protected]_Layout 1 12/16/13 11:33 AM Page 1