
La Risonanza Magnetica Cardiaca: quando usarla come gold ... · XV Congresso nazionale SIEC 2011...
57
XV Congresso nazionale SIEC 2011 Uso dell’Imaging nella pratica clinica: dalla diagnosi alla tecnologia La Risonanza Magnetica Cardiaca: quando usarla come gold standard G. Di Bella (Messina) Napoli, 16 Aprile 2011 Università di Messina Dipartimento Clinico Sperimentale di Medicina e Farmacologia
-
Upload
doannguyet -
Category
Documents
-
view
215 -
download
0
Transcript of La Risonanza Magnetica Cardiaca: quando usarla come gold ... · XV Congresso nazionale SIEC 2011...

XV Congresso nazionale SIEC 2011
Uso dell’Imaging nella pratica clinica: dalla diagnosi alla tecnologia
La Risonanza Magnetica Cardiaca:
quando usarla come gold standard
G. Di Bella (Messina)
Napoli, 16 Aprile 2011
Università di Messina Dipartimento Clinico Sperimentale di Medicina e Farmacologia

CMR: Advantages
•No Ionizing Radiation==>Virtually Safe
•Multiplanarity
•Flow and Velocity Measurement
•Not conditioned by presence of Bone
•Controindications (PM dependent,device, Claustrophobia..)
•Long time of execution
•Need for Cardiac Gating
•Need for Compatible instrument
CMR: Disadvantages
CMR

CMR as gold standard
Accuracy
Differential diagnosis
Reserch tool

High spatial and temporal resolution
standardization of acquisition
high quality images
no geometric assumptions
high accuracy
good inter and intra-observer reproducibility
Relative high costs
Not available at bed side of patients
CMR: left ventricular function

SSFP cine MRI:
10-16 slices, 8 mm thickness, no
spacing (or 2 mm gap),
R-R: 30 phases,
CMR: left ventricular function
Starting from a horizzontal long axis view
using planes orthogonal to major left ventricular
axis (from center of mitral valve to apex)
QUANTITATIVE ASSESSMENT

• End-diastolic frame and end-systolic frame for each slice
• Trace left ventricular endocardial contour
• Trace left ventricular epicardial contour
• Trace right ventricular endocardial contour
Phase 1 Phase 10
Post-processing
CMR: left ventricular function
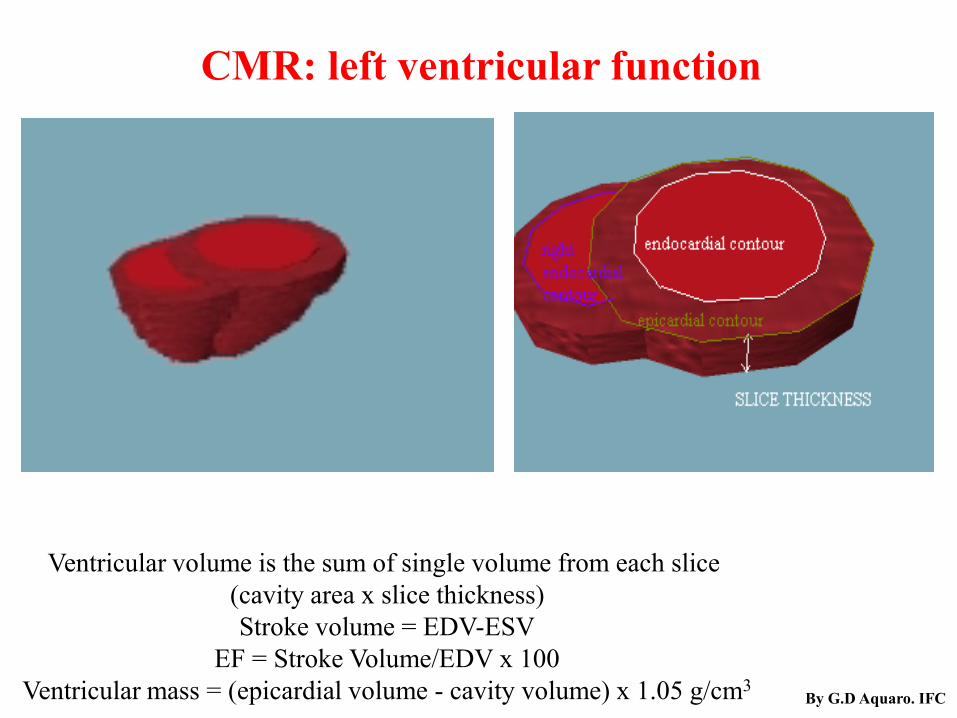
Ventricular volume is the sum of single volume from each slice
(cavity area x slice thickness)
Stroke volume = EDV-ESV
EF = Stroke Volume/EDV x 100
Ventricular mass = (epicardial volume - cavity volume) x 1.05 g/cm3 By G.D Aquaro. IFC
CMR: left ventricular function

Maceira et al JCMR 2006
CMR: left ventricular function

ARVC/D

ARVC/D



Ev
ent-
free
Su
rviv
al(%
)
0 200 400 600 800 1000 1200
Event-free Survival curve of RVA vs no-RVA
Time (days)
no-RVA
RVA
P<0.0001
100
98
96
94
92
90
88
86
Aquaro GD et al JACC 2010

Ev
ent-
free
Su
rviv
al(%
) no-RVA
RVA
100
98
96
94
92
90
88
86
Event-free Survival curve: no-RVA, Intermediate group, ARVC/D group
0 200 400 600 800 1000 1200
Time (days)
RVA-1 group
RVA-2 group
P<0.0001
P<0.003
Aquaro GD et al JACC 2010

Echocardiography 2010
Additive data from strain imaging

Semiautomatic Quantification of Left Ventricular Function by
2D Feature Tracking Imaging Echocardiography.
A Comparison Study with Cardiac Magnetic Resonance Imaging
Gianluca Di Bella, M.D., Ph.D., Concetta Zito, M.D., *Michele Gaeta, M.D., Maurizio Cusmà Piccione, M.D., *Fabio Minutoli, M.D.,
*Rocco Donato, M.D., Antonino Recupero, M.D., Antonio Madaffari, M.D., Sebastiano Coglitore, M.D., Scipione Carerj M.D.
Echocardiography 2010

Di Bella G, et Al. Echocardiography


Stroke volume can be assessed also
by measuring total flow
across ascending aorta or pulmonary
trunk in one heartbeat
CMR: left ventricular function

Stroke volume can be assessed also
by measuring total flow across
ascending aorta or pulmonary
trunk in one heartbeat
CMR: left ventricular function
Absolute Flow 86 ml/beat
Retrograd Flow 32 ml/beat
Regurgitant fraction 37%

Quantitative assessment of absolute aortic flow
(LV stroke volume)
CMR: left ventricular function
Quantitative assessment of absolute pulmonary flow
(RV stroke volume)
QP/QS

CMR: Flow measurements
Clinical Implication……………………..
Congenital heart diseases
Study of Left Ventricle volume and mass:
EndDiastolic Volume: 210 ml
EndSystolic Volume: 94ml
Stroke volume: 115 ml
EF 55%
Mass: 175 g
Phase Contrast at Ascending Aorta
Real Stroke volume 73.5 ml
REAL EF=SV/EDVx 100%
73.5/210x100
EF 35%
Regurgitant Volume=
115 ml-73.5 ml=41.5 ml Mitral regurgitation


CMR as gold standard
Identification and
extent of scar tissue

Scar tissue in myocardial infarction
Scar tissue in myocarditis

A. Wagner et al. Lancet 2003
necrosis as small as 1g can be detected with CE-IR-MRI
<=> 10 g with SPECT
Noninvasive Gold for Infarct Imaging ?

CE-IR MRI rationale: scarred myocardium strongly enhances
after Gd-DTPA administration, and can be used to
determine presence, extent, and transmurality, and
to differentiate with normal myocardium
(Kim et al. N Engl J Med, 2000)
likelihood of segmental recovery of function
paralles infarct transmurality




Il valore prognostico additivo dell’integrazione funzione/necrosi
HR P de=1 & wm=0 vs de=0 & wm=0 2,285 ns de=0 & wm=1 vs de=0 & wm=0 2,129 ns
de=1 & wm=1 vs de=0 & wm=0 7,784 0.007
de=1 & wm=1 vs de=1 & wm=0 3,347 0.05
de=1 & wm=1 vs de=0 & wm=1 3,407 0.05 Di Bella et al.
Submitted
237 pts con infarto miocardico pregresso con e senza
disfunzione ventricolare sinistra Eventi: n=19 (morte cardiaca, arresto resuscitato, scarica
DEF appropriata
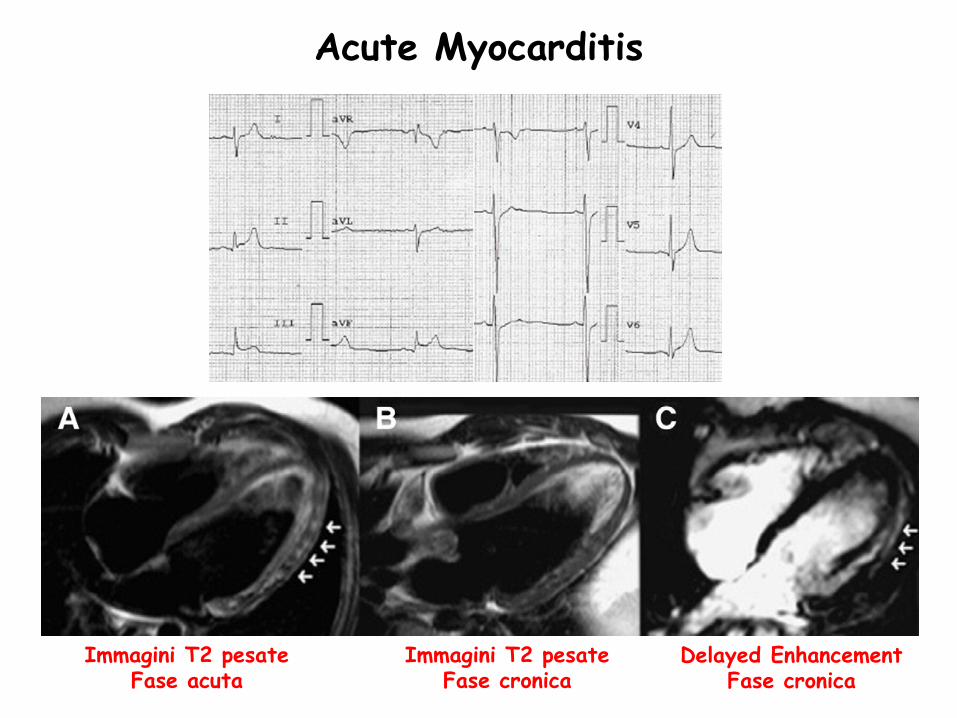
Immagini T2 pesate Fase acuta
Immagini T2 pesate Fase cronica
Delayed Enhancement Fase cronica
Acute Myocarditis

CMR as gold standard
Tissue characterization
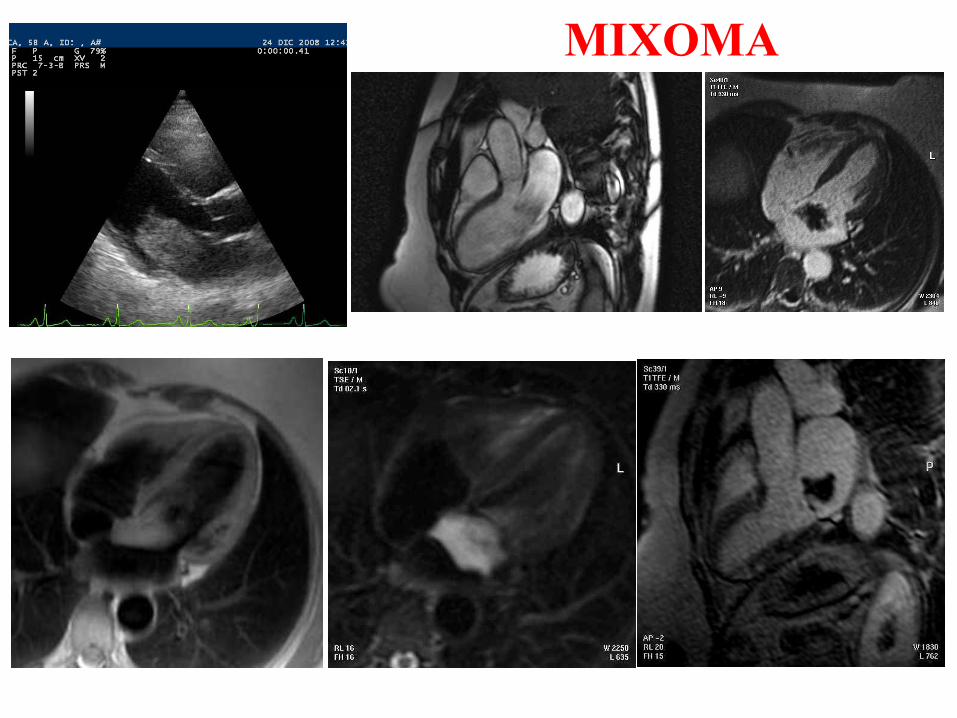
MIXOMA

Di Bella G et al. Rev Esp Cardiol. 2010;63(11):1383-9 ANGIOSARCOMA

Di Bella G et al. Circulation 2008

CMR as gold standard
Tissue characterization (scar tissue)
Myocarditis
Viability
Cardiac tumors
Cardiomyopathies
Cardiac Morphology andFunction
RV function
Congenital heart diseases


CMR is gold standard in
Right ventricular function
Identification of scar tissue in MI and
Myocarditis
Tissue caracterization of cardiac tumors
and in other many cardiomyopaties

Gianluca Di Bella
Grazie
University of Messina Clinical and Experimental Department of Medicine and Pharmacology
PhD course on Cardiovascular Imaging Methodologies and Techniques


Post-Infarction Ventricular
Arrhythmia
• Characterization of the peri-infarct zone by CE-MRI is a powerful predictor
of post-myocardial infarction mortality (Yan AT et al. Circulation 2006;114:32)
• Presence and extent of tissue heterogeneity in the peri-infarct zone increases
susceptibility to ventricular arrhythmias in patients with prior LV infarction
and LV dysfunction (Schmidt A et al. Circulation 2007;115:2006)


RV infarction

Grasso e Displasia aritmogena VD
“Un caso senza sospetti”
Immagini T1 pesate Immagini T1 pesate con fat suppression
Delayed enhancement

CMR: left ventricular function By G.D Aquaro. IFC

Epidemiologic data
•2% of population < 65 years
•10% of population > 65 years
have reduction of LV systolic function
CMR: left ventricular function

1 R-R
8-16 View per segm.
30 N° Phase
1 NEX
0.0 SPACING
8 mm THICKNESS
~40 FOV
125 kHz RBw
45° FLIP ANGLE
In base
freq.cardiaca TR
Minimun TE
SSFP
CMR: left ventricular function

dia
sto
le
sis
tole
Tagging RM
E1: ispessimento sistolico
E2: accorciamento circonferenziale
Alfa: angolo di deformazione della direzione di E1 rispetto alla
direzione radiale
E1
E2
Alfa

Clinical Implication……………………
• LV
• >>>>>> RV
• Global function
• >>> regional function
CMR as gold standard in
function

MRI tagging
Con una sequenza di
impulsi viene generata
una modulazione spaziale
di magnetizazzione.
Le righe generate si
muovonoi con il tessuto e
si analizza il movimento
delle righe (deformazione)
su più immagini


La sequenza di impulsi in CINE viene
preceduta da una modulazione spaziale di
magnetizzazione (demagnetizzazione)
Le righe generate (tags) si muovono con il
tessuto
viene analizzato la deformazione delle tags
line nelle fasi del ciclo cardiaco
mappe di deformazione del miocardio
MRI: STUDIO DI FUNZIONE
TAGGING
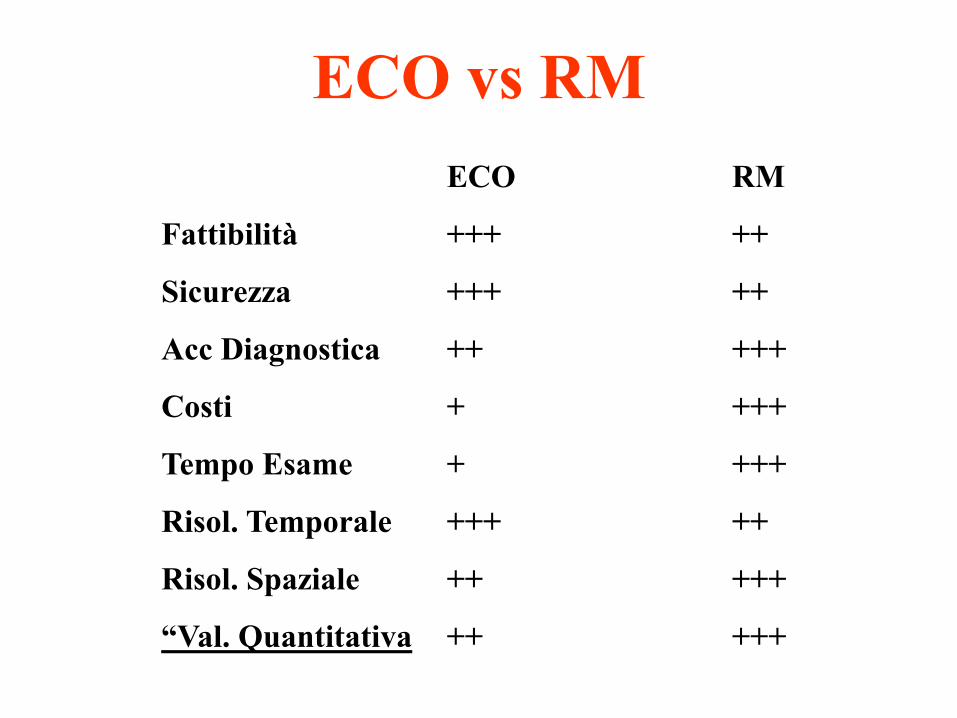
ECO RM
Fattibilità +++ ++
Sicurezza +++ ++
Acc Diagnostica ++ +++
Costi + +++
Tempo Esame + +++
Risol. Temporale +++ ++
Risol. Spaziale ++ +++
“Val. Quantitativa ++ +++
ECO vs RM

Study of Left Ventricle volume and mass:
EndDiastolic Volume: 210 ml
EndSystolic Volume: 94ml
Stroke volume: 115 ml
EF 55%
Mass: 175 g
Phase Contrast at Ascending Aorta
Real Stroke volume 73.5 ml
REAL EF=SV/EDVx 100%
73.5/210x100
EF 35%
Regurgitant Volume=
115 ml-73.5 ml=41.5 ml
CMR: Flow measurements
Mitral regurgitation
Clinical Implication……………………..

Di Bella G, et Al. In press Echocardiography
Semiautomatic Quantification of Left Ventricular Function by
2D Feature Tracking Imaging Echocardiography.
A Comparison Study with Cardiac Magnetic Resonance Imaging

MR in VALVULOPATIE
EDV: 328 ml; ESV: 140 ml;
ejection fraction: 57%; mass: 195 g
EF= 188/328*100= 57%
Real EF= 81/328*100= 25%
Regurgitation flow volume: 77 ml;
regurgitation fraction: 46%.
Effective aortic SV (156-77) = 81 ml;


















