
LA CHEMIOTERAPIA DI I LINEA -...
30
Michele Reni Department of Medical Oncology IRCCS Ospedale San Raffaele Milan, Italy DECIDERE LA CHEMIOTERAPIA ADIUVANTE E DELLA MALATTIA METASTATICA LA CHEMIOTERAPIA DI I LINEA
Transcript of LA CHEMIOTERAPIA DI I LINEA -...

Michele Reni
Department of Medical Oncology
IRCCS Ospedale San Raffaele
Milan, Italy
DECIDERE LA CHEMIOTERAPIA ADIUVANTE E
DELLA MALATTIA METASTATICA
LA CHEMIOTERAPIA DI I LINEA

THE HISTORY OF PC TREATMENT
Whipple refines the PD procedure
Italian surgeons develop the pylorus-preserving PD
Chemo added to RT improved survival vs RT alone in LAPC
The 1st chemotherapeutic agent receives FDA approval in advanced metastatic disease
1st study to demonstrate OS benefit with ADJ CHEMO for resectable disease
1st targeted agent approved for LA or
metastatic PC
Multidrug regimen shows significant
OS benefit in metastatic disease
19
30
19
40
19
50
19
60
19
70
19
80
19
90
20
00
20
10
1st combination chemotherapy showing superiority over GEM

mSv 1y OS
5-FU 4.41 2%
GEM 5.65 18%
P = .0025
1.0 –
0.9 –
0.8 –
0.7 –
0.6 –
0.5 –
0.4 –
0.3 –
0.2 –
0.1 –
0.0 –
0 4 8 12 16 20
1ST-LINE OPTIONS IN MPC: GEMCITABINE ?
Burris et al. JCO 1997;15:2403-13
100
80
60
20
0
40
20 0 2 6 8 12 14 18 4 10 16
Time (months)
Patients
surv
ivin
g (
%)
Log rank test p=0.0025
Gemcitabine
5-FU
N 126
Stage IV 93 (74%)
KPS 50-70 87 (69%)
KPS 80-100 39 (31%)

Unresectable PDA Countless negative trials over last
decades
Drug G +X G P value
bolus 5FU 6.7 mo 5.4 mo 0.11
c.i. 5FU 5.9 mo 6.2 mo 0.683
pemetrexed 6.2 mo 6.3 mo 0.85
capecitabine 8.4 mo 7.3 mo 0.314
irinotecan 6.3 mo 6.6 mo 0.789
cisplatin 7.6 mo 6.0 mo 0.12
oxaliplatin 9.0 mo 7.1 mo 0.13
….
1ST-LINE OPTIONS IN MPC: GEMCITABINE ?

GEM+erlotinib : 1 positive phase III trial
level 1 evidence :
CLINICALLY IRRELEVANT benefit (HR 0.82)
GEM+platinum salt: 5 negative phase III trials
level 1 evidence :
LACK OF any relevant BENEFIT (HR>0.85)
GEM+capecitabine : 2 negative phase III trials
level 1 evidence :
LACK OF any relevant BENEFIT (HR 0.86)
1ST-LINE OPTIONS IN MPC ?


10 days ! 0% 18 mo
1ST-LINE OPTIONS IN MPC: GEMCITABINE + ERLOTINIB ?
Moore et al JCO 2007;25:1960-6;

phase II-III trial
Metastatic pancreatic
cancer
(n 342)
R
A
N
D
O
M
I
Z
E
FOLFIRINOX
gemcitabine
No prior chemo
PS 0-1
<76 y
T. Bilirubin < 1.5x ULN
Conroy T, et al. NEJM 2011
1ST-LINE OPTIONS IN MPC : FOLFIRINOX

FFX: 11.1 mo Gem: 6.8 mo
Conroy T, et al. NEJM 2011
1ST-LINE OPTIONS IN MPC : FOLFIRINOX

• This study enrolled 861 pts at 151 sites in North America, Europe, and Australia
1:1, stratified by KPS, region, liver metastasis
nab-P 125 mg/m2 IV qw 3/4
+
Gem 1000 mg/m2 IV qw 3/4
Gem 1000 mg/m2 IV qw 7/8
then qw 3/4
Planned N = 842 •Stage IV •No prior treatment for M+ disease •KPS ≥ 70 •Measurable disease •Total bilirubin ≤ ULN •No age limitation
Von Hoff DD, et al. N Engl J Med. 2013; 369: 1691-1703.
1ST-LINE OPTIONS IN MPC : NAB-PACLITAXEL-GEMCITABINE

Von Hoff DD, et al. N Engl J Med. 2013; 369: 1691-1703.
1ST-LINE OPTIONS IN MPC : NAB-PACLITAXEL-GEMCITABINE

ORR mOS 1y OS 18-mo OS
FOLFIRINOX 32% 11.1 48% 19%
GEM 9% 6.8 21% 6%
GEM 7% 6.7 22% 9%
GEM-nab 24% 8.5 35% 16%
Nab-paclitaxel + gem vs FolfIrinOx

ACCORD 11 and MPACT cannot be directly compared
(regional vs global settings; differences in eligibility
criteria, in 2nd-line use and efficacy …)
1st-line treatment: what criteria to select one treatment or the other?

Nab-paclitaxel + gem vs FolfIrinOx Comparable populations ?

FFX: 11.1 mo Gem: 6.8 mo
BEWARE of APPLES
FOLFIRINOX

#259 ASCO GI 2015 who is eligible ?
N=473 M+ treated with GEM in Canada
mOS
1) Eligible for FOLFIRINOX 24.7% 8.6
2) Eligible for nab-Gem 45.2% 6.7
Nab-paclitaxel + gem vs FolfIrinOx Comparable populations ?
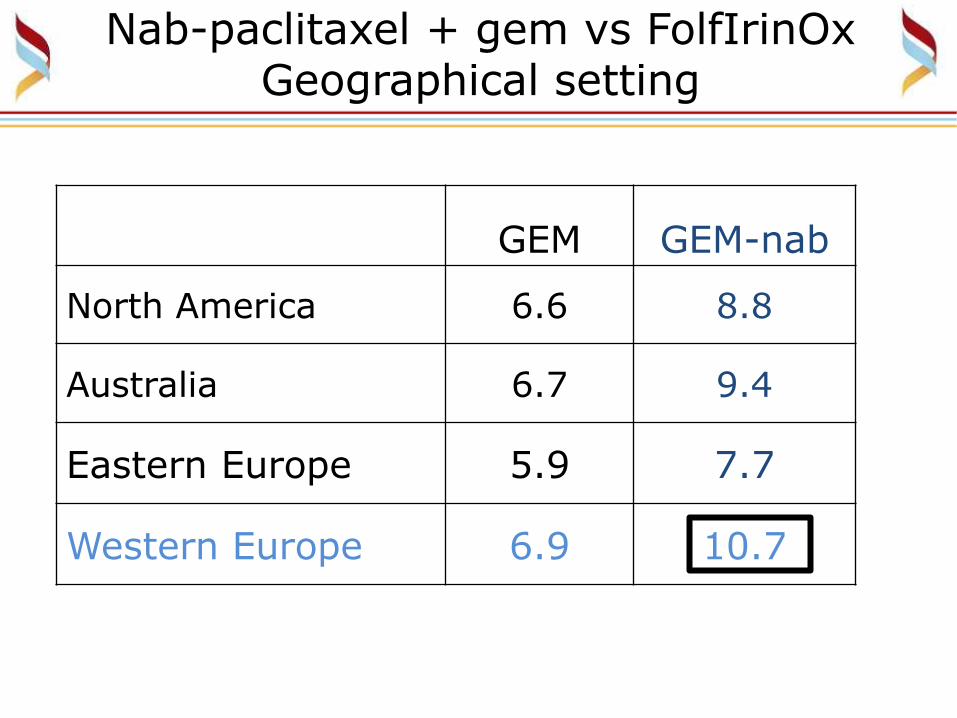
GEM GEM-nab
North America 6.6 8.8
Australia 6.7 9.4
Eastern Europe 5.9 7.7
Western Europe 6.9 10.7
Nab-paclitaxel + gem vs FolfIrinOx Geographical setting

Gem-nab FolfIrinOx
mPFS 5.5 mo 6.4 mo
6-mo PFS 44% 53%
1-y PFS 16% 12%
45.4%
Conroy T, et al. NEJM 2011; 364: 1817-1825
Nab-paclitaxel + gem vs FolfIrinOx is FOLFIRINOX better ?

nabP+gem mOS phase II 12.1 phase III 8.7
FOLFIRINOX is median OS correctly calculated ?
Conroy T, et al. NEJM 2011

2nd line
FOLFIRINOX 47%
Gem-nab 38%
Nab-paclitaxel + gem vs FolfIrinOx Comparable populations ?

is modified FolfIrinOx equally effective ?
Stein1 Uesugi2 Conroy (# 395) (#422) (NEJM) N 37 19 171 ECOG 0 46% nr 37% M+ liver 54% nr 88% CA19.9 <59 ULN 49% nr 44%
mOS 10.2 10.32 11.1
PR 35% nr 31.6% (stage III) 17% na na 1. Stein S. ASCO GI 2016 #395. IRI 135 includes locally advanced
2. Uesugi K. ASCO GI 2016 #422. FU 0+2400; IRI 150

Maroun J ESMO 2015 302P
Median OS is overestimated ? Modified FOLFIRINOX is less effective ?

Gem-nab FolfIrinOx PEXG
neutropenia 38% 46% 35%
PLT 13% 9% 10%
neutrop fever 3% 5% 1%
Hb 13% 8% 13%
vomiting nr 15% 4%
fatigue 17% 24% 9%
diarrhea 6% 13% 8%
neuropathy 17% 9% 0%
COMBINATION CHEMOTHERAPY G3-4 ADVERSE EVENTS

mOS 1y 2y
GEM-nab1 8.7 (10.7)4 35% (39%)4 9%
FolfIrinOx2 11.1 48% 11%
PEXG3 10.6 41% 17%
1) VanHoff DD, et al N Engl J Med. 2013;369(18):1691-703 2) Conroy T, et al N Engl J Med 2011; 364: 1817-1825 3) Reni M, et al Cancer Chemother & Pharmacol 2012: 69: 115-123 4) Tabernero J, et al OncoTargets and Therapy 2017; 10: 591-596
1ST-LINE OPTIONS IN MPC

R
Gem+nab-paclitaxel
PAXG
p0=45%; p1=65%, α=0.05, power=80%;
N=42 eligible patients
If ≥ 25/42 PFS-6, the regimen will be considered active
Reni M, et al. BJC 2016; 115: 290-296
Chemo-naive patients
age 18-75 yr
Karnofsky PS ≥ 70
Metastatic disease
PACT-19 - PHASE II
randomised, monocentric

RESULTS
CR PR SD PD ↓CA19.9 ≥90%
↓CA19.9 50-89 %
PAXG 1
(2%) 20
(48%) 14
(33%) 7
(17%) 12 (38%) 10 (31%)
AG* 2
(5%) 10
(24%) 18
(44%) 8
(20%) 13 (42%) 6 (19%)
VonHoff 29% 31%
*3 patients not assessable

RESULTS (Apr 2014 – May 2016)
Baseline Characteristic A: PAXG B: AG
Number 42 41
Male/female 19/23 24/17
KPS 80-100 40 (95%) 38 (93%)
Age median 66 64
range 44-75 29-75
CA19.9 >ULN 32 (76%) 31 (76%)
median 2230 1201
range 53-36645 46-739108
Biliary Stent 12 (29%) 7 (17%)
NLR ≥5 6 (14%) 8 (19%)
Liver metastasis 29 (69%) 32 (79%)
Peritoneal metastasis 9 (21%) 6 (15%)

RESULTS
AG VonHoff2
PFS6 49% 44%
mPFS 6.1 5.5
mOS 11.2 8.5
1y OS 44% 35%
2y OS 12% 9%
PAXG AG VonHoff2
PFS6 31 (74%) 49% 44%
mPFS 8.1 6.0 5.5
mOS 14.4 11.2 8.5
1y OS 62% 44% 35%
2y OS 24% 12% 9%

OSR stage IV – by REGIMEN
N mOS 1y 2y
PEFG 96 8.7 39 12
PEXG 134 10.2 41 17
AG 41 11.2 44 12
PAXG 42 14.4 62 24

LINEE GUIDA AIOM
Qualità dell’evidenza
SIGN
Raccomandazione clinica Forza della raccomandazione
clinica
A
Nei pazienti affetti da PDAC M+ KPS>70 età ≤ 70 anni, una chemioterapia di 1° linea con 3 o 4 farmaci può essere presa in considerazione come opzione di 1° intenzione in alternativa alla monoterapia con gemcitabina
Positiva debole
A
In pazienti con PS ≥ 70 ed età >18 anni una chemioterapia di I linea con
gemcitabina-nab-paclitaxel dovrebbe essere preso in considerazione come
opzione terapeutica di 1° intenzione in termini di incremento di PFS e OS
Positiva forte
B
La gemcitabina settimanale può essere presa in considerazione come opzione terapeutica di 1° intenzione in pazienti con malattia avanzata e KPS <70
Positiva debole


















