
Knowledge-based ergonomic assessment of working conditions ... · As mentioned OWAS, RULA and REBA...
11
Knowledge-based ergonomic assessment of working conditions in surgical ward – A case study Joanna Bartnicka ⇑ Silesian University of Technology, Faculty of Organization and Management, Institute of Production Engineering, 26-28 Roosevelta Street, 41-200 Zabrze, Poland article info Article history: Received 10 June 2013 Received in revised form 30 April 2014 Accepted 21 July 2014 Available online 10 September 2014 Keywords: Surgery Musculoskeletal disorders Ergonomics Integrated assessment Knowledge management mechanisms abstract This article aims at identifying the mechanisms of knowledge management in the selection and integra- tion of ergonomic methods for the evaluation of working conditions of nursing staff and surgeons in sur- gical wards. The criterion for choice of given category of work was specified for individual workstation based on the results of empirical research taking into account a case study of trauma and orthopaedics. There were established procedures of ways for integrating methods and tools depending on appointed category of work. In the study there were used such ergonomic methods and evaluation factors as: OWAS, REBA, RULA, NIOSH, monotype tasks, energy expenditure and computing tools: 3D Static Strength Prediction Program 3D SSPP, Energy Expenditure Prediction Program EEPP, Anthropos ErgoMax, CAPTIV L2100. In addition, the tool of competence matrix and decision tables are used to identify the category of work as well as to select an integrated ergonomic assessment. The presented research methodology of ergonomic assessment has been performed along with contin- uation of works on the development project titled: Knowledge-based shaping of working conditions in health care units, funded by the National Centre for Research and Development in Poland. The aim of the project was to establish a computer system based on ICT technologies for supporting hospital processes, which was called ‘‘Virtual hospital’’. Ó 2014 Elsevier Ltd. All rights reserved. 1. Introduction Use of ergonomic methods provides a lot of information on the assessment of the degree of adjustment of working conditions to properties and human predispositions. The more comprehensive assessment is expected, the more ergonomic methods and the more information relevant to the application of these methods are needed. Hence, it seems to be necessary to manage information recourses in such a way, that they will replenish the ergonomic assessment process in an effec- tive way and analyse the assessment results together and depend- ing on each other. Only such action will give a complete overview of the ergonomic state of workstation and work operations, con- tributing to an effective improvement of working conditions. The subject of research is the activity of the trauma and ortho- paedic surgery wards (TOSW), in particular work processes carried out by medical personnel. The premise for the choice of such research subject is the numerous ergonomic problems manifested by an excessive load of musculoskeletal system during surgery operations, whereby this problem affects both the surgical staff as well as nursing staff. The reason for the excessive load is to long-lasting staying in the forced body positions and necessity for using a large force. Numerous studies confirm the existence of such problem around the world. They are based inter alia on information from medical staff, who gave their opinions during dif- ferent surveys. Such research was e.g. conducted in reference to scrub nurses in Sheikhzadeh et al. (2009) where there was indi- cated as the main problem the low back pain (LBP), and right after it ankle/foot and shoulder pain. Many research related to the problem of incorrect working con- ditions in surgical theatres including the problem of poor ergo- nomic surgical instruments mainly concern low-invasive surgery. The outcomes of such research are published inter alia in: Trejoa et al. (2007), where it is presented the results from a comparative analysis of two laparoscopic instruments in terms of physical workload of wrists; (Marcos et al., 2006; Wichert et al., 2004) which contain the results of research on using computer-aided tools: CATIA, PCMAN, RAMSIS for analysing and designing an oper- ating room dedicated to perform laparoscopic surgery; (Albayrak et al., 2007) where is described the design of special equipment for body support which reduces the loads in spine and neck during surgery; (Xiao et al., 2012) which aim was to investigate the http://dx.doi.org/10.1016/j.ssci.2014.08.010 0925-7535/Ó 2014 Elsevier Ltd. All rights reserved. DOI of original article: http://dx.doi.org/10.1016/j.ssci.2014.07.020 ⇑ Tel.: +48 32 2777311. E-mail address: [email protected] Safety Science 71 (2015) 178–188 Contents lists available at ScienceDirect Safety Science journal homepage: www.elsevier.com/locate/ssci
Transcript of Knowledge-based ergonomic assessment of working conditions ... · As mentioned OWAS, RULA and REBA...

Safety Science 71 (2015) 178–188
Contents lists available at ScienceDirect
Safety Science
journal homepage: www.elsevier .com/locate /ssc i
Knowledge-based ergonomic assessment of working conditionsin surgical ward – A case study
http://dx.doi.org/10.1016/j.ssci.2014.08.0100925-7535/� 2014 Elsevier Ltd. All rights reserved.
DOI of original article: http://dx.doi.org/10.1016/j.ssci.2014.07.020⇑ Tel.: +48 32 2777311.
E-mail address: [email protected]
Joanna Bartnicka ⇑Silesian University of Technology, Faculty of Organization and Management, Institute of Production Engineering, 26-28 Roosevelta Street, 41-200 Zabrze, Poland
a r t i c l e i n f o
Article history:Received 10 June 2013Received in revised form 30 April 2014Accepted 21 July 2014Available online 10 September 2014
Keywords:SurgeryMusculoskeletal disordersErgonomicsIntegrated assessmentKnowledge management mechanisms
a b s t r a c t
This article aims at identifying the mechanisms of knowledge management in the selection and integra-tion of ergonomic methods for the evaluation of working conditions of nursing staff and surgeons in sur-gical wards. The criterion for choice of given category of work was specified for individual workstationbased on the results of empirical research taking into account a case study of trauma and orthopaedics.
There were established procedures of ways for integrating methods and tools depending on appointedcategory of work. In the study there were used such ergonomic methods and evaluation factors as:OWAS, REBA, RULA, NIOSH, monotype tasks, energy expenditure and computing tools: 3D Static StrengthPrediction Program 3D SSPP, Energy Expenditure Prediction Program EEPP, Anthropos ErgoMax, CAPTIVL2100. In addition, the tool of competence matrix and decision tables are used to identify the category ofwork as well as to select an integrated ergonomic assessment.
The presented research methodology of ergonomic assessment has been performed along with contin-uation of works on the development project titled: Knowledge-based shaping of working conditions inhealth care units, funded by the National Centre for Research and Development in Poland. The aim ofthe project was to establish a computer system based on ICT technologies for supporting hospitalprocesses, which was called ‘‘Virtual hospital’’.
� 2014 Elsevier Ltd. All rights reserved.
1. Introduction
Use of ergonomic methods provides a lot of information on theassessment of the degree of adjustment of working conditions toproperties and human predispositions.
The more comprehensive assessment is expected, the moreergonomic methods and the more information relevant to theapplication of these methods are needed. Hence, it seems to benecessary to manage information recourses in such a way, thatthey will replenish the ergonomic assessment process in an effec-tive way and analyse the assessment results together and depend-ing on each other. Only such action will give a complete overviewof the ergonomic state of workstation and work operations, con-tributing to an effective improvement of working conditions.
The subject of research is the activity of the trauma and ortho-paedic surgery wards (TOSW), in particular work processes carriedout by medical personnel. The premise for the choice of suchresearch subject is the numerous ergonomic problems manifestedby an excessive load of musculoskeletal system during surgery
operations, whereby this problem affects both the surgical staffas well as nursing staff. The reason for the excessive load is tolong-lasting staying in the forced body positions and necessityfor using a large force. Numerous studies confirm the existenceof such problem around the world. They are based inter alia oninformation from medical staff, who gave their opinions during dif-ferent surveys. Such research was e.g. conducted in reference toscrub nurses in Sheikhzadeh et al. (2009) where there was indi-cated as the main problem the low back pain (LBP), and right afterit ankle/foot and shoulder pain.
Many research related to the problem of incorrect working con-ditions in surgical theatres including the problem of poor ergo-nomic surgical instruments mainly concern low-invasive surgery.The outcomes of such research are published inter alia in: Trejoaet al. (2007), where it is presented the results from a comparativeanalysis of two laparoscopic instruments in terms of physicalworkload of wrists; (Marcos et al., 2006; Wichert et al., 2004)which contain the results of research on using computer-aidedtools: CATIA, PCMAN, RAMSIS for analysing and designing an oper-ating room dedicated to perform laparoscopic surgery; (Albayraket al., 2007) where is described the design of special equipmentfor body support which reduces the loads in spine and neck duringsurgery; (Xiao et al., 2012) which aim was to investigate the

J. Bartnicka / Safety Science 71 (2015) 178–188 179
influence of ergonomic factors on task performance during laparo-scopic training, and to evaluate the trainee posture under twoergonomic conditions: optimal and non-optimal.
This paper is dedicated to the equally important issue of opensurgery, although less accentuated in the research. Here the litera-ture calls attention on LBP and much more frequent movements ofback flexion than during laparoscopic surgery, in turn, in a lesserextent on a static loads of neck, shoulder and wrists (Nguyenet al., 2001). Nevertheless, in the research conducted by Szetoet al. (2012) it is indicated that surgeons generally maintained aflexed neck posture during open surgery and a more extended neckposture during laparoscopic procedures. Other studies described inSoueid et al. (2010) concerning the assessment of the load ofsurgical personnel of various specialties showed that nearly 80%of them described pains on a regular basis and the back and neckwere the most common areas of pain. It should be noted that opensurgery may be characterized by varying degrees of dynamicoperational activities and higher frequencies of movements thatrequire additional methods of assessment, apart from the statisti-cal analysis.
The aim of this article is to present the research methodologyon how to manage the information for an integrated ergonomicassessment. The basis for developing the methodology was a casestudy from two hospitals in which the orthopaedic surgeries areperformed as a standard procedure.
The methodology includes the following specific objectives:
O1: identification of problems and pain in the musculoskeletalsystem of medical staff and identification of factors affectingthe workload.O2: selecting the ergonomic assessment method depending onthe work category.O3: gaining, transforming, collecting and integrating informa-tion resources for conducting a comprehensive ergonomicassessment using different configurations of methods.O4: integration of outcomes from ergonomic assessment andtheir analysis.
The article presents the results of ergonomic assessment of pro-cedures performed during the surgeries: total knee replacementand hip replacement. These procedures require using relativelygreat force by the surgeons. Therefore it is proposed to use an addi-tional method of physical load assessment apart from the analysisof static load. Integration of both static and dynamic assessmentprovides a more complete outlook of working conditions duringsurgery and allows to diagnose ergonomic problems.
2. A review of ergonomic assessment methods and theirapplications
The intensive development of ergonomics in the past few dec-ades has been resulting in numerous different methods for ergo-nomic assessment and improve working conditions. The problemof workload associated with excessive static load has become areason for the development of methods to assess the correctnessof body position. These methods are based on the codification ofthe arrangement of individual body segments and assignment ofindicated codes for a particular category of load. The body positionis defined in different ways and with different degree of specificity,depends on the type method.
In the OWAS method (OVAKO Working posture Analysing Sys-tem) (Karhu et al., 1977) the body posture is evaluated by positionof three body segment: back, arms and legs. Additionally there istaken into account the weight of the load handled and the timeof maintaining the certain position during a workday. There is
defined the degree of harmfulness (to one from four different cat-egory of postural stress) for the musculoskeletal system accordingto the code of the body posture. Such definition is developed for allposture combination indicating the urgency for changes in the areaof the way of performing certain tasks.
There are similar methods to OWAS like: RULA (McAtamneyand Corlett, 1993) and REBA (Hignett and McAtamney, 2000) butthey are more complex due to taking into account additionallyposition of wrist, neck and body balance.
As mentioned OWAS, RULA and REBA methods take intoaccount the value of external load and the time factor, but in theOWAS method the factor is expressed in % time in certain task,while in the RULA and REBA in the repeatability of operations.The RULA and REBA methods were used inter alia to assess the sta-tic load of shoulder and wrist while performing sonographic exam-inations (Burnett and Campbell-Kyureghyan, 2010) whileminimally invasive surgical techniques requiring performing theprecision manual tasks, like an endoscopic technique (Lee et al.,2005), laparoscopic technique (Youssef et al., 2011).
The comparative study of OWAS, RULA and REBA methods (Keeand Karwowski, 2007) does not indicate the superiority of any ofthem, but points out rather their strengths and weaknesses associ-ated with the degree of details describing observed body positionsand work activities. Here are described inter alia the outcomesfrom analysis of working postures in the general hospital, wherewas observed the underestimated postural loads for this posturesestimated by REBA, compared with RULA. Similarly, OWAS showeda tendency to underestimated postural loads.
In other research on selection of ergonomic assessment meth-ods for the analysis of a hospital, the OWAS and RULA were ratedlower in comparison with the REBA which additionally includesdata on leg positions and foot support while standing (Janowitzet al., 2006).
The REBA method was also chosen as a basic method for assess-ment of workload of nurses in: Hignett and McAtamney (2000),although the authors suggested the use of additional methods forconfirming and verifying assessments like OWAS, NIOSH (Waterset al., 1993) or empirical measurement in a laboratory setting.
Nevertheless, analysing the literature, it can be concluded thatfrom the collection of aforementioned three methods: OWAS, RULAand REBA, OWAS method is the most widespread and used inde-pendently of the type of industry and type of work. The researchwith using OWAS method were conducted inter alia in: chemicalindustry (Väyrynen et al., 1994) in particular by fibre spinning, pay-ing additionally attention to the mode of conducting the research,which were based on the monitoring of employees by video cam-eras (Vedder, 1998); agricultural industry for the analysis of bodypostures of stoctworker by operating in perchery system (Scottand Lambe, 1996), on the farms by milking, cow brushing or silagehandling (Groborz et al., 2011; Nevala-Puranen, 1995; Nevala-Puranen et al., 1996; Perkiö-Mäkelä and Hentilä, 2005); in storageindustry by operating forklift truck (Hoy et al., 2005); buildingindustry by two types suspended scaffolds: light and heavy(Saurin and de Macedo Guimarães, 2008), etc.
The OWAS method was repeatedly used to the analyses of pos-tural load in health care, for care activities carried out by nursingstaff, especially for: tasks connected with lifting and moving thepatients or services of hospital instrumentation (Best, 1997;Engels et al., 1994; Hignett, 1996) for evaluation of the accuracyof the methods used by health-care workers while cleaning, bath-ing or folding and unfolding wheelchairs (Pohjonen et al., 1998;Whitea and Kirby, 2003); physiotherapists work drawing specialattention to the problems of handling large forces related to man-ual handling operations with patients (Hignett, 1995).
In Poland, the OWAS method has legislative implications. In Acton early retirement from 19 December 2008, the method has been

Table 2Outcomes from survey about MSDs.
Localization of MSDs Number of persons Response rate (%)
Lumbosacral spine n = 30 71.43Thoracic spine n = 20 47.62Cervical spine n = 27 64.29Arm joints n = 17 40.48Hip joints n = 17 40.48Knee joints n = 15 35.71Ankle joints n = 5 11.90Wrists n = 11 26.19Non-MSDs n = 4 9.52
180 J. Bartnicka / Safety Science 71 (2015) 178–188
used to define the concept of work in the forced body posture as awork that requires a significant slope and (or) twist back whileexerting forces in excess of 10 kG for men and 5 kG for women(according to the method OWAS it is category 4) for at least 50%of the work shift (Dz. U. Nr 237, poz. 1656, 2008).
All three methods have their implementations in the form ofcomputer programs, such as ErgoLAB (OWAS), ErgoFellow (OWAS,RULA, REBA), WinOWAS (OWAS), etc.
Apart from the mentioned methods there are many other toolsfor ergonomic assessment based on computer-aided design forboth static and dynamic kinds of workload e.g.: EEPP (EnergyExpenditure Prediction Program) which estimates energy expendi-ture rates and based on model described in Garg et al. (1978); soft-ware which allow for predicts static strength requirements fordefined tasks and provides an approximate job simulation thatincludes posture data, force parameters and anthropometric suchas: Anthropos-Ergomax; 3D SSPP (Three Dimensional StaticStrength Prediction Program) (3D Static Strength PredictionProgram, 2011; Chaffin, 1969); SAMMIE (System for AidingMan-Machine Interaction Evaluation) (Porter et al., 1996); JACK(Badler, 1993), DELMIA (Digital Enterprise Lean ManufacturingInteractive Application) (Xinhua et al., 2011) and many otherswhich are mentioned inter alia in Karwowski et al. (2008).
3. Methodology and results description
The research are generally divided into four stages:
1st stage – examination of working conditions in TOSW withusing survey methods and recording video – the objective O1.2nd stage – analyses of functionality of ergonomic assessmentmethods with using competency matrix tool – the objective O2.3rd stage – categorization of the work of medical staff anddeveloping a scheme of selection of ergonomic methods withusing decision tables – the objective O2.4th stage – development of information resources managementmodel for integrated ergonomic assessment – the objectives O3,O4.
3.1. 1st stage – Examination of working conditions in TOSW
The empirical study included:
– surveys which allowed for a subjective, based on experience ofthe respondents, assessment of the working conditions andidentification of key factors of workload,
– analysis and assessment of working conditions on the basis ofphotographic and video recording of two kinds of surgeries:hip replacement and knee replacement which allowed to verifyand objectify the survey results and identify additional keyfactors of workload.
The specification of the research is presented in Table 1.
Table 1Specification of empirical study in hospitals.
Research methods Number of hospitals Number of pein research
Survey n = 2 Total n = 42Nurses n = 24Doctors n = 1Management
Analysis of video and photo recordingsof surgeries
n = 2 Total n = 14Nurses n = 5Doctors n = 9male n = 8)
3.1.1. Survey outcomesThe purpose of the survey was to assess the hardship work, tak-
ing into account: the structure of the musculoskeletal disorders(MSDs), the most common body postures adopted during the work,activities causing the greatest difficulty, as well as technical andorganizational conditions, which have negative impact on workprocesses. A survey was conducted in two hospitals in TOSW.Table 2 presents the synthetic results connected with MSDs fromthe survey.
Only four people of all respondents did not complain of MSDs.Other 38 individuals claimed that they suffer from MSDs, but themost in the lumbosacral spine and cervical spine (LBP), slightly lessin the thoracic region of spine. Almost the half of respondents com-plains of arm and hip disorders. It should also note the pain in theknee joints and wrists.
MSDs should be linked with the mode of operating activitiesespecially with hard and forced body position which additionallyreinforces static load. Table 3 shows the most commonly bodypositions of the staff during job tasks, and the organizational andtechnical conditions which, according to respondents, may affectthe workload and MSDs.
The survey indicated a need to direct an ergonomic assessmentto analyse the somatic relations connected with the manner ofoperations, particularly operations with the static nature relatedto the necessity of maintaining specific body position. The respon-dents who took part in the survey did not indicate the time as afactor which can enhance the hardship of work - this importantaspect of an ergonomic assessment emerged from the direct obser-vation combined with the video recording of work in the TOSW.According to the survey the dynamic operations causing workloadconcern mostly the activities related to lifting and movement ofpatients. The key elements which influence on the workload areawkward positions of back, head and legs as well as work withloads.
3.1.2. Video and photo recordings analysis outcomesIn the study there were taken into account two surgical
procedures: hip replacement and knee replacement. The surgerieswere carried out in two different hospitals by two different surgical
rsons participating Number of body positions
n/a
4staff n = 4
Total n = 94Handle of tools and equipment n = 17
(female n = 1, Process of surgery n = 77 (standing position n = 70,sitting position n = 7)

Table 3Outcomes from survey about position and environmental issues.
Working conditionsfactors
The opinions of respondents
Body positions duringwork processes
Standing positionBent backBent headSeated positionTwo bent legs
Organizational andtechnical conditions
Limited working spaceMaladjusted height of bedsInsufficient number support equipment forhandling the patient and thus the need formanual lifting and movement of patientsMaladjustment toilets for people moving onwheelchairsSlippery ground
J. Bartnicka / Safety Science 71 (2015) 178–188 181
teams. The surgeries were fully invasive. The duration for singleprocedure was �2 h.
There was identified two main processes in surgical procedure:the main process containing direct operational activities and sup-port processes containing preparation of the patient for surgery,the use of equipment and surgical instruments including handingand drawing the instruments during the procedure.
From the recorded video material there were separated for fur-ther analyses the body positions, which were inconsistent fromneutral position, but for one activity it could be attributed severalpositions. The basis for the selection of the inconsistent fromneutral positions was the procedure for static load assessmentaccording to the REBA method. In particular in this method suchnon-natural positions are defined taking into account the anglevalue between a body segment and the reference plane (sagittal,frontal and lateral) and are following:
– for wrist when is bent more than 15� from straight position,– for upper and lower arm when are bent more than 20� from
straight position,– for neck when is bent more than 20� from straight position,– for back when is bent more than 20� from straight position,– for leg when the position is unstable or the legs are bent more
than 30� from straight position.
The angle values are specified in the 3DSSPP software whichenables the modelling of anthropometric features of human bodyand somatic relations based on photographic or video registration.Fig. 1 presents the procedure of the identification of body segmentangles.
The next step was describing in details the state of selectedpositions. Whereby it was taken into account the following set ofelementary states S e {ssi, sst, snh, sba, sar, swr, sle, slo, sfo, sre} chosenbased on the survey and additionally completed by frequencyfactor, where:
– seated position ssi,– standing position sst,– neck/head position snh,– back position sba,– arms position (shoulders position) sar,– wrist position swr,– legs position sle,– lifting slo,– the force sfo,– action frequency sfr.
Table 4 presents the results of analysis. For the defined elemen-tary states, there were adopted the following attributes indicatinga possible qualitative assessment of body position:
– hardship, i.e. the position diverges largely from neutral position(non-neutral positions according to REBA method),
– no hardship i.e. the position is neutral or diverges slightly fromneutral position (non-neutral positions according to REBAmethod),
– no data.
If the attribute is: no data, the simplification is adopted consist-ing in assigning an attribute to: hardship.
During both the operational and support activities (i.e. handleof tools and equipment) there are highlighted the deficiencies inmaintaining the position of the head (bent in the sagittal and/orcoronal plane, twisted), back (bent in the sagittal and/or coronalplane, twisted) and wrist including the max. range of movementsin joints. Maintaining the body position, which can lead to posturalstress, is caused by the following features:
– for snh, sba, sar and sle: stationary position of the patient withoutthe possibility to change it to another during surgery; inade-quate height of the surgical table; the necessity of maintainthe interactions between surgeon’s eyes and limited operatingfield, different anthropometric features of medical staff,
– for swr: inadequate grip design of surgical instruments, the lackof sizes for surgical instruments, stationary position of thepatient without the possibility to change it to another duringsurgery; inadequate height of the surgical table.
In turn, to the dynamic features causing the maintaining bodyin non-ergonomic position and hence the physical burdens of sur-geons (sfo and sfr) should be included the instruments manipula-tions like hitting, milling, drilling, sawing with a high precisionand in different directions.
Lifting operations (slo) during surgery occur occasionally, how-ever. This kind of activities is characterized by the stage of prepa-ration for surgery, as well as during patient care before and aftersurgery and concern mainly operations performed by nursing staff.
Concluding, the study results enabled to specify the musculo-skeletal system disorders of medical staff and identify the key fac-tors affecting the workload. Thus it was possible to build theinformation recourses needed for next stages of proposed method-ology of integrated ergonomic assessment.
3.2. 2nd stage – Analysis of functionality of ergonomic assessmentmethods with using competency matrix tool
High degree of differentiation of working methods by medicalpersonnel makes it impossible to select a single universal ergo-nomic method, which can be used to evaluate and make correc-tions in the working conditions at the hospital. Concurrently acomprehensive ergonomic assessment is a prerequisite to diagnosethe working conditions and determine the corrective guidance.
Table 5 presents the functionality of the popular methods ofergonomic assessment in the form of matrix of competence.
Competence matrix identified as the most functional 3DSSPPmethod which based on models described in Chaffin et al.(2006). The principle of application of the method is based on com-puter models of anthropometric features with the implementedcomputational models from the range of the biomechanics. Themain advantage that distinguishes it from other methods is theability to assessing the operations with using force which is differ-ent than lifting force. In addition, the method has the advantages of

Fig. 1. The mode of the identification of body segment angles with use of 3DSSPP software.
Table 4The results of the analysis of body positions during surgical procedures.
Elementary state ofbody position
The number of hardship positions, rate of all positions
Operational activities Support activities Total
Standing position Seated position
snh n = 59, 84% n = 6, 86% n = 12, 71% n = 77, 82%sba n = 60, 86% n = 7, 100% n = 8, 47% n = 75, 80%sar n = 28, 40% n = 3, 43% n = 10, 59% n = 41, 44%swr n = 66, 94% n = 7, 82% n = 9, 53% n = 82, 87%sle n = 37, 53% n = 0, 0% n = 7, 41% n = 44, 47%slo n = 1, 01% n = 0, 0% n = 1, 06% n = 2, 02%sfo n = 43, 61% n = 2, 29% n = 4, 24% n = 49, 52%sfr n = 3, 04% n = 2, 29% n = 4, 24% n = 9, 10%
182 J. Bartnicka / Safety Science 71 (2015) 178–188
visualization of different ways of presenting computer models, aswell as the possibility of building a simple computer animation.The method does not take into account time factor, which meansthat operations carried out in forced positions without externalload will not be interpreted as negative affecting on the musculo-skeletal system. Hence the complementary methods in this casemay be the methods OWAS, RULA or REBA. Similar characteristicsto 3DSSPP applies computer-aided method Anthropos-ErgoMAX(AN.ER), where the additional advantage of this method is the abil-ity of accurate modelling of the position of the wrists, and evenindividual phalanges bones. The quality of visualization and ani-mation is higher compared to the 3DSSPP method, but conse-quently there is a higher degree of difficulty in handling thesoftware.
3DSSPP and Anthropos-ErgoMAX are excellent computer toolsfor designing and modernization of workplace and work methods.
As mentioned OWAS, RULA and REBA methods are based on asimple codification of the body position and can be used to assesspostural stress with or without external load. The advantage ofRULA and REBA methods is taking into account the position ofthe wrists, which significantly affects the final evaluation of thestatic load and discomfort at work.
In turn the algorithm used in these methods does not includesitting position, which limits the scope of application (Sá et al.,2006). These methods should be considered mainly as a supportfor the risk assessment, especially when there are adverse wristspositions, and a lesser extent, as a tool for helping by formingthe working conditions.

Table 5Matrix of competence containing the functionality of methods for ergonomic assessment.
Set of features F Feature OWAS RULA REBA NIOSH 3DSSPP EEPP AN.ER.
Anthropometric features fa Gender x x xPercentile 5, 50, 95 x xWeight x x xHeight x x
Body position fp Position of forearm x x x xPosition of upper arm x x x xPosition of shoulder x x xPosition of upper leg x x xPosition of lower leg x x xPosition of foot xPosition of hip xPosition of back x x x x x xPosition of wrist x x xPosition of neck/head x x x xSeated position x x x xStanding position x x x x x x xWalking x xOther x x
Manner of support fs Support for leg x x x x xSupport for arm x x x
Right/left body side fl/r Distinction between right/left body side x x
External load fl Hand load/ranges x x x x x x xLifting x x x x xThe force xQuality of coupling x xExternal forces x
Time ft % Time in certain position xDuration x xFrequency x x x xPosition holding min. 1 min x x x
Static load assessment frs Low back pain LBP x xRisk x x x xMain body segment load x xWrist load xBody balance assessment x
Dynamic load assessment frd Energy expenditure xMonotype
Recommendations Recommended weight limit xRecommended coefficient of friction xRanges of limbs xField of view xDesign x x x
Visualization Computer animation/simulation x xSimplicity of use x-Simple
xx-Difficult x x x x x x xx
J. Bartnicka / Safety Science 71 (2015) 178–188 183
NIOSH method supports the analysis associated with heavy lift-ing, and above all is a simple tool for the selection of the maximumweight of lifted object. Taking into account the work processes ofmedical staff, NIOSH method has its application in the analysis ofactivities related to lifting and moving surgical instruments as wellas medicines, dressings and other accessories used during surgery.Whereby these accessories are placed both in and on hospitalcabinets.
The independent method in relation to the others is EEPP,which supports the calculation of energy expenditure workerbased on the time study of work. Evaluation of energy expenditureis concerned basically with the activities carried out with signifi-cantly dynamics of the motion.
Similarly, an independent tool is a tool for assessment of work-load related to monotype of activities.
From the group of analysed methods you can distinguish meth-ods dedicated for specific ways of performing actions such as lift-ing or work in forced postures (3DSSPP, NIOSH, RULA, REBA), aswell as methods which are independent of the type of work(OWAS, EEPP, assessment of monotype of work).
Summarizing the body posture analysis it can be concluded thatthe features differentiating the ways of activities are: body posi-tion, a manner of body support (standing, sitting position) and loadoperating.
3.3. 3rd stage – Categorization of the work
Taking into account the results of empirical studies conductedin hospitals and analysis of functionality of ergonomic methodsthe work categorization was performed. In consequence, the workcategorization became the basis for elaboration of decision tablessupporting the selection of ergonomic methods. The process of cat-egorization is based on division of objects into groups, character-ized by relative homogeneity, whereby, these objects must notbe identical.
In the process of work categorization the following assumptionswere made:
– each category is represented by unique collection of workfeatures,

184 J. Bartnicka / Safety Science 71 (2015) 178–188
– each category is self-definable,– each category possesses an essential feature that characterizes
all objects belonging to it,– affiliation to a certain category is defined by the logical rules.
The following essential features classifying affiliation to a cer-tain type of work category were defined:
– activities carried out without external load – Category A,– lifting activities in standing position – Category B,– lifting activities in seated position – Category C,– activities that require using force different than lifting force –
Category D.
Identification methods assigned to a given work category werebased on decision tables. The essence of decision tables is to graph-ically represent a set of decision rules. These, in turn, represent anexpression that describes a set of conditions that must be fulfilledin order to realize the operations.
Table 6 presents in a simplified way decision rules supportingselection of methods for the assessment of ergonomic workstationsin surgical wards.
The recommended method R demonstrates the best functional-ity from the characteristics of the certain work category point ofview. And so, for Category A it is recommended to use the methodof Anthropos-ErgoMAX, which allows to conduct static analysiswithout external load for any given body position and to analysethe field of view and the ranges of limbs, which, as demonstratedby the research conducted in hospitals, significantly affects themanner of operations. Since this method does not include the timefactor that is crucial in assessing tasks without external load, as acomplementary method C OWAS has been chosen. Because of itsversatility, ease of use and the importance of legislation (seeSection 2), this method was considered to be complementary toall work categories. Similarly, EEPP methods and monotypeassessment are not dedicated to specific categories of work, butare complementary to all R methods.
The results of assessment with use of the EEPP methods andmonotype assessment significantly supplements the knowledgeabout the hardship of the workstation, and also supports the assess-ment of organization of work, regardless of its categorization.
In case of lifting operations in standing position there arefollowing methods recommended: 3DSSPP methods because ofthe detailed biomechanical analysis, including analysis of the bodystability and Anthropos-ErgoMAX method. Method C in this case isNIOSH, which enables the analysis of environmental factors, suchas design features of workstation. This method also works wellas a simulation tool for the modernization of working conditions.
Table 6Decision table supporting selection of ergonomic method.
Rule 1 Rule 2 Rule 3 Rule 4
If Category A xCategory B xCategory C xCategory D x
Then OWAS C C C CRULA, REBA S S SNIOSH C3DSSPP S R R REEPP C C C CAssessment of work monotype C C C CAnthropos-ErgoMAX R R R S
R – recommended method.C – complementary method.S – supported method.
If the work is performed with an external load but it is not a lift-ing task, then it is recommended to use the 3DSSPP method. Thismethod allows to define additional external forces acting on theemployee, so it is possible to simulate the actual somatic relationsoccurring in the workplace. 3DSSPP method cannot model thewrists, but it contains a calculation formulas for determining thedegree of hardship of this part of the body.
It is recommended to use support methods S in a situationwhere it is necessary to verify the results received by other assess-ment methods or to focus an assessment on any particularsegment of the body, e.g. the use of RULA and REBA method forthe analysis of static load of wrists.
3.4. 4th stage – Development of information resources managementmodel for integrated ergonomic assessment
The model of integration of ergonomic methods was developedusing knowledge management principles. The model includes inparticular a unified procedure how to gain, organize, collect andtransform information for the implementation of an integratedergonomic assessment and procedure of the analyses of the resultsfrom the assessment. Fig. 2 presents a schematic diagram describ-ing the various steps of the procedure as well as the methods andtools to perform a given stage.
The essence of the procedure is to use a common software envi-ronment as a place for data acquisition and ordering informationfor the ergonomic assessment and analysis of the results of thisassessment. The selected software environment is CAPTIV L2100(produced by TEA, France).
CAPTIV L2100 is a computer program for analysing data onworkplace based on video registration of work activities and relatedencoded information. Such encoded information can be e.g. thetypes of movements, body postures, types of activities, the valueof the load, environment parameters etc., creating a kind of elec-tronic timing work. It is proposed that the encoded informationwere the features belonging to the set F. Synchronization of suchinformation in connection with video footage, allows the cross-sec-tional analyses of the work in unit time, expressed graphically ashistograms, graphs and summary tables, and simultaneously servesas a structured common database of related data representing theinput data for ergonomic assessment methods. Similarly, it is possi-ble to perform comprehensive analysis, which includes additionallyencoded information in frame of the ergonomic assessment resultswith the use of R and C methods. The encoded results appear on thebackground of a set of features F describing the process of work intime unit. Fig. 3 presents in a model way the essence of linksbetween video records with graphic description of, in this case,the changing body position of surgeon over time.
In Table 7 a model manner of using the procedure, for the caseof work category A is presented.
Cross-sectional analysis containing varying threads of an ergo-nomic evaluation and factors influencing the working conditionscan provide new knowledge in the fields of organization and ergo-nomics, which would be difficult to identify in case of any particu-lar study with these methods using separately. Visualsynchronization of cross-sectional data makes it possible toperform a comparative analysis of the hardship of work of differentemployees at different stages of surgery procedure and the assess-ment of teamwork. It allows to identify the weak points of thewhole work process.
4. Discussion
Working in a hospital at a surgical ward is characterized by highdynamics. The surgical activities performed by medical staff
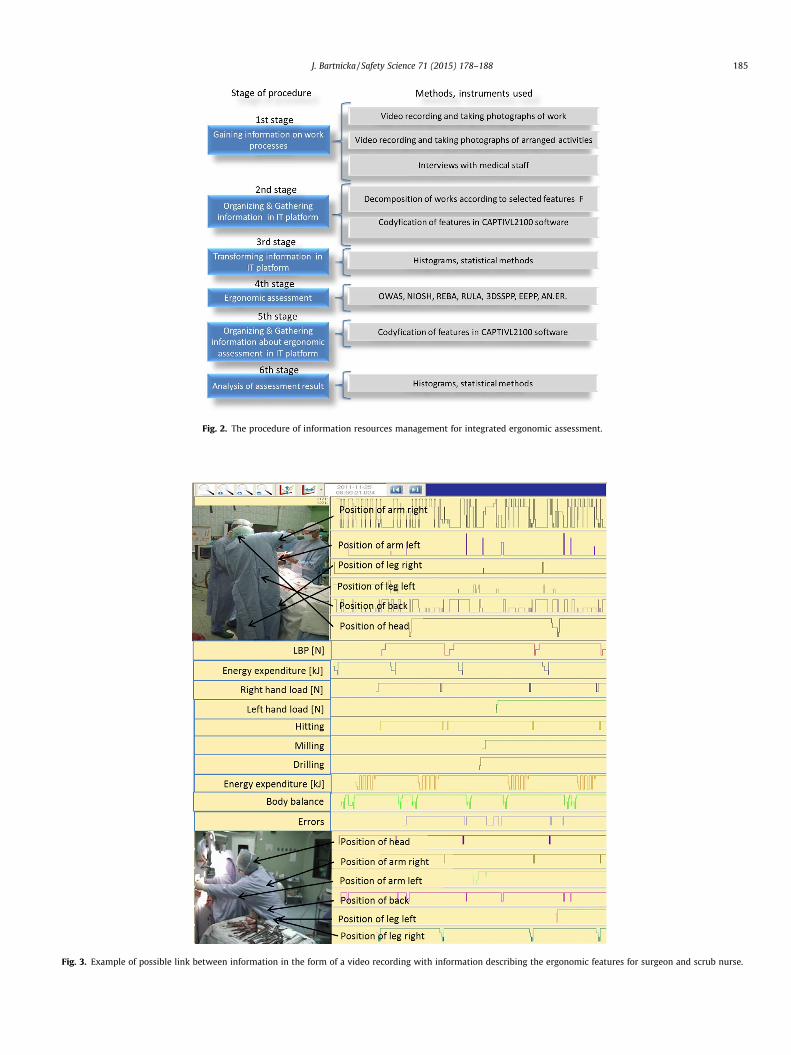
Fig. 2. The procedure of information resources management for integrated ergonomic assessment.
Fig. 3. Example of possible link between information in the form of a video recording with information describing the ergonomic features for surgeon and scrub nurse.
J. Bartnicka / Safety Science 71 (2015) 178–188 185

Table 7The model way of using the procedure for the work category A.
Stage Description Information stored in CAPTIV L2100
1 Gaining information on work processes – video recording AVI files2 Codifying features F F 2 {fa, fp, fs, fl/r, fl}3 Ordering information Body position
Time of position maintenanceType of activitiesLasting time of activitiesInformation about forced position
4 Ergonomic assessment with using methods: OWAS, EEPP,monotype, AN.ER (REBA, RULA, NIOSH – if needed)
n/a
5 Codifying features F F 2 {frs, frd}6 Integrated ergonomic assessment Visualization of cross-analysis of assessments in the form of histograms, graphs and summary
tables:– dynamic load of the musculoskeletal system in unit time– degree of intensity of work, including the particular segments of the body, in unit time– uniformity of the load on the right and left hand– average duration of specific types of activities– relation between the size of the static load [N], and load category and risk in the OWAS
method and energy expenditure in the EEPP method– identification and duration of errors activities, unnecessary extra procedures resulting not
from surgical procedures, and their impact on the load of musculoskeletal system– other
186 J. Bartnicka / Safety Science 71 (2015) 178–188
require considerable physical and postural effort, which is associ-ated with maintaining awkward position at work. The nursing staffis exposed mainly to static loads associated with both work inforced body positions, as well as the necessity of lifting and han-dling external loads. However, the appropriate harmony betweena medical staff and the other components of working conditions,which is the ergonomics purpose, is not only the factor for keepingwork safety for workers but also is a part of patient safety(Carayon, 2010; Buckle et al., 2006). The attention is drawn to rela-tion of ergonomics and patient safety in operating room. In theresearch, which outcomes are described in Matern and Koneczny(2007), the elementary ergonomic deficiencies within such fieldsas the architectural situation, the devices and instruments as wellas working posture and associated pain (MSDs) were showed onthe background of potential hazards for patients and personnel.For instance the growing number of complex devices has led toincreased difficult or unnecessary interactions between humansand machines disturb the work flow, often to the detriment ofthe patient. In addition, the non-ergonomic instruments causinguncomfortable hand and arm postures can lead to decreasedpatient safety because of reduced tactile sensitivity (Büchel et al.,2010). The another ergonomic aspect affecting safety for patientand doctors is improperly designed operating room leading tocrowded workplaces, floors cluttered with tubing and wires(Alarcon and Berguer, 1996). Because of the fact, that ergonomicsis one of the important factor (next to the surgeon factors) inachieving safe and high-quality performance in surgery (Carayonet al., 2014; Douglas et al., 2010; ElBardissi and Sundt, 2012;Vincent et al., 2004) it is advisable to continually asses andimprove working condition taking into account ergonomic criteria.
It should be highlighted however that apart from above men-tioned research, there is the lack of extensive clinical studies indi-cated the direct relations between patient safety and MSDs ofsurgical staff from trauma and orthopaedic wards. Furthermore,there are no epidemiological tests in range of orthopaedic sur-geons’ MSDs noted in the literature which could be the base forrecognizing these disorders as the formal occupational diseases.
Regarding the ergonomics in the operating rooms, the vastmajority of publications in this field are related to minimallyinvasive surgery. Relatively little research is conducted in the areaof open surgery, in which the staff is faced with both static anddynamic loads. Thus the challenges for ergonomics are huge and
attention of researchers should also be focused on this aspect ofsurgical operations.
Despite the multitude of ergonomic assessment methods it isdifficult to choose the right one for the total ergonomic issues inthe surgical ward.
There are no clear indications for the choice of methods basedon the codification of the position of work, i.e. OWAS, RULA, REBA.Important factor in favour of an ergonomic assessment based onobservation and further transformation of information is non-con-tact manner of such measurement. The use of additional measuringequipment, like the EMG method is not recommended in such ademanding and sterile conditions prevailing in the operating room.
In Polish conditions, the OWAS method has the legitimacy (seeSection 2) which can be a factor in favour of the choice of thismethod from the above mentioned group of ergonomic methods.In turn, 3DSSPP method should be supplemented by auxiliarymethods: OWAS, RULA, REBA, which take into account the timefactor.
It is suggested to use the advanced computer tool Anthropos-ErgoMAX in the study. It should be noted, however, that any othertools with similar functionality, which have already supported theanalysis of ergonomic operating room in other research (see Sec-tion 2), can be used.
Elaborating new methods, which duplicate the principles ofother methods, should rather be refocused on the study of howto integrate them as well as how to standardise the ergonomicassessment. The development of information technologies createsnew opportunities for the integration of differentiated informationresources on working conditions and thus generation of newknowledge which can be useful in the ergonomic design and man-agement of occupational safety and health.
Despite the obvious benefits of implementation of ergonomicsin working conditions, the possible adverse effects of ergonomicrecommendations in surgical wards should be discussed. Theyare located at least in three aspects:
1. The reduction of work effectiveness after implementation ofergonomic principles (a longer operating time, errors) causedby such features like: the necessity of using new work proce-dures or work organization, the natural reluctance of employeesto changes, the difficulty in changing multiannual habits, favor-ing medical staff at the expense of patient comfort.

J. Bartnicka / Safety Science 71 (2015) 178–188 187
2. Worsening the working conditions of the certain surgical teammembers at the expense of improving work conditions of oneemployee (e.g. main operator) caused by the unbalanced imple-mentation of ergonomic principles within the whole team work.
3. The adverse financial consequences of implementation of ergo-nomic principles caused by purchasing costs of new equipment,modernisation of workspace, trainings of workers, etc.
The adverse effects are associated with the serious, problematicand in the same time little recognized area which is the examinationof the relations: costs-benefits of ergonomics implementation. Inthis context, a study should be conducted on the basis of the systemapproach, which is the fundamental element of above presentedresearch methodology for an integrated ergonomic assessment.
5. Conclusion
The essence of the proposed approach to knowledge-basedergonomic assessment is the possibility to re-use the same infor-mation resources depending on the purpose and the method ofergonomic analysis. It is shown that these resources are stored ina common software environment. In the same environment theresults of ergonomic studies are stored, which, thanks to integra-tion of them, allow cross-sectional analysis of the results and iden-tification of weak points in the work process, that would beimpossible or more difficult using traditional analytical procedurebased on separate ergonomic assessment methods.
The research has shown that most laborious and simulta-neously relatively difficult stage in the presented procedure isthe stage of acquisition and codification of many of the data inCAPTIVL2100. Therefore it seems reasonable to develop a formalprocedure for data coding, which will be a repeatable scheme forfuture analyses, as well as for elaborating scenarios of differentvariants of ergonomic analyses.
Summarizing the literature review, it can be concluded thatnumerous ergonomic analyses conducted in different areas oflabour activity, both in industry and health care, prove the keepingproblem of hardship of working conditions related to the bodyposition and manual tasks with external loads.
5.1. Relevance to industry
The present work aimed at identifying how to integrate ergo-nomic assessment methods for the synergy of knowledge in theprocess of forming correct working conditions. The presented pro-cedure of integrated ergonomic assessment can be used as a modelfor creating professional procedures by the ergonomics teams incompanies of different industries.
Acknowledgements
The author would like to thank all of the hospitals, the doctors,nurses and the decision makers who have agreed to participate inthe study.
References
3D Static Strength Prediction Program. User Manual, 2011. The University ofMichigan Center for Ergonomics.
Alarcon, A., Berguer, R., 1996. A comparison of operating room crowding betweenopen and laparoscopic operations. Surg. Endosc. 10, 916–919.
Albayrak, A., van Veelen, M.A., Prins, J.F., Snijders, C.J., de Ridder, H., Kazemier, G.,2007. A newly designed ergonomic body support for surgeons. Surg. Endosc. 21,1835–1840.
ANTHROPOS – ErgoMax: User Guide, Version 3.0, 1999. IST GmbH, Keiserslautern.Badler, N., 1993. Computer Graphics Animation and Control. Simulating Humans.
Oxford University Press, New York, USA.
Best, M., 1997. An evaluation of manutention training in preventing back strain andresultant injuries in nurses. Saf. Sci. 25, 207–222.
Büchel, D., Mårvik, R., Hallabrin, B., Matern, U., 2010. Ergonomics of disposablehandles for minimally invasive surgery. Surg. Endosc. 24, 992–1004.
Buckle, P., Clarkson, P.J., Coleman, R., Ward, J., Anderson, J., 2006. Patient safety,systems design and ergonomics. Appl. Ergon. 37, 491–500.
Burnett, D.R., Campbell-Kyureghyan, N.H., 2010. Quantification of scan-specificergonomic risk-factors in medical sonography. Int. J. Ind. Ergon. 40, 306–314.
Carayon, P., 2010. Human factors in patient safety as an innovation. Appl. Ergon. 41,657–665.
Carayon, P., Wetterneck, T.B., Rivera-Rodriguez, A.J., Hundt, A. Schoofs, Hoonakker,P., Holden, R., Gurses, A.P., 2014. Human factors systems approach to healthcarequality and patient safety. Appl. Ergon. 45, 14–25.
Chaffin, D., 1969. A computerized biomechanical model: development and use instudying gross body actions. J. Biomech. 2, 429–441.
Chaffin, D.B., Andersson, G.B.J., Martin, B.J., 2006. Occupational Biomechanics,fourth ed. John Wiley & Sons, New York.
Douglas, A., Wiegmann, D.A., Eggman, A.A., ElBardissi, A.W., Parker, S. Henrickson,Sundt, T.M., 2010. Improving cardiac surgical care: a work systems approach.Appl. Ergon. 41, 701–712.
Dz. U. Nr 237, poz. 1656. Ustawa z dnia 19 grudnia 2008 r. o emeryturachpomostowych (translation in English: The Act of 19 December 2008 on bridgingpensions).
ElBardissi, A.W., Sundt, T.M., 2012. Human factors and operating room safety. Surg.Clin. North Am. 92 (1), 21–35.
Engels, J., Landeweerd, J., Kant, Y., 1994. An OWAS-based analysis of nurses’ workingpostures. Ergonomics 37, 909–919.
Garg, A., Chaffin, D., Herrin, G., 1978. Prediction of metabolic rates for manualmaterials handling jobs. Am. Ind. Hyg. Assoc. J. 39, 661–674.
Groborz, A., Tokarski, T., Roman-Liu, D., 2011. Analysis of postural load during tasksrelated to milking cows – a case study. Int. J. Occup. Saf. Ergon. (JOSE) 17, 423–432.
Hignett, S., 1995. Fitting the work to the physiotherapist. Physiotherapy 81, 549–552.
Hignett, S., 1996. Postural analysis of nursing work. Appl. Ergon. 27, 171–176.Hignett, S., McAtamney, L., 2000. Rapid Entire Body Assessment (REBA). Appl. Ergon.
31, 201–205.Hoy, J., Mubarak, N., Nelson, S., Sweerts de Landas, M., Magnusson, M., Okunribido,
O., Pope, M., 2005. Whole body vibration and posture as risk factors for low backpain among forklift truck drivers. J. Sound Vib. 284, 933–946.
Janowitz, I.L., Gillen, M., Ryan, G., Rempel, D., Trupin, L., Swig, L., Mullen, K.,Rugulies, R., Blanc, P.D., 2006. Measuring the physical demands of work inhospital settings: design and implementation of an ergonomics assessment.Appl. Ergon. 37, 641–658.
Karhu, O., Kansi, P., Kuorinka, I., 1977. Correcting working postures in industry: apractical method for analysis. Appl. Ergon. 8, 199–201.
Karwowski, W., Grobelny, J., Michalski, R., 2008. Workload assessmentpredictability for digital human models. In: Duffy, V.G. (Ed.), Handbook ofDigital Human Modeling Research for Applied Ergonomics and Human FactorsEngineering. CRC Press.
Kee, D., Karwowski, W., 2007. A comparison of three observational techniques forassessing postural loads in industry. Int. J. Occup. Saf. Ergon. (JOSE) 13, 3–14.
Lee, E.C., Rafiq, A., Merrell, R., Ackerman, R., Dennerlein, J.T., 2005. Ergonomics andhuman factors in endoscopic surgery: a comparison of manual vs teleroboticsimulation systems. Surg. Endosc. 19, 1064–1070.
Marcos, P., Seitz, T., Bubb, H., Wichert, A., Feussner, H., 2006. Computer simulationfor ergonomic improvements in laparoscopic surgery. Appl. Ergon. 37, 251–258.
Matern, U., Koneczny, S., 2007. Safety, hazards and ergonomics in the operatingroom. Surg. Endosc. 21, 1965–1969.
McAtamney, L., Corlett, E.N., 1993. RULA: a survey method for the investigation ofwork-related upper limb disorders. Appl. Ergon. 24, 91–99.
Nevala-Puranen, N., 1995. Reduction of farmers’ postural load duringoccupationally oriented medical rehabilitation. Appl. Ergon. 26, 411–415.
Nevala-Puranen, N., Kallionpaa, M., Ojanen, K., 1996. Physical load and strain inparlor milking. Int. J. Ind. Ergon. 18, 277–282.
Nguyen, N.T., Ho, H.S., Smith, W.D., Philipps, C., Lewis, C., De Vera, R.W., Berguer, R.,2001. An ergonomic evaluation of surgeons’ axial skeletal and upper extremitymovements during laparoscopic and open surgery. Am. J. Surg. 182, 720–724.
Perkiö-Mäkelä, M., Hentilä, H., 2005. Physical workstrain of dairy farming in loosehousing barns. Int. J. Ind. Ergon. 35, 57–65.
Pohjonen, T., Punakallio, A., Louhevaara, V., 1998. Participatory ergonomics forreducing load and strain in home care work. Int. J. Ind. Ergon. 21, 345–352.
Porter, J.M., Case, K., Freer, M.T., 1996. SAMMIE: a 3D human modelling computeraided ergonomics design system. Co-design J. 07 (08), 68–75.
de Sá, F.D., do Nascimento, M.A.A., de Melo, A.C.C., da Costa Santos, J., Adissi, P.J.,2006. Comparison of methods RULA and REBA for evaluation of postural stressin odontological services. In: Third International Conference on ProductionResearch – Americas’ Region (ICPR-AM06).
Saurin, T.A., de Macedo Guimarães, L.B., 2008. Ergonomic assessment of suspendedscaffolds. Int. J. Ind. Ergon. 38, 238–246.
Scott, G.B., Lambe, N.R., 1996. Working practices in a perchery system, using OVAKOWorking posture Analysing System (OWAS). Appl. Ergomnics 27, 281–284.
Sheikhzadeh, A., Gore, Ch., Zuckerman, J.D., Nordin, M., 2009. Perioperating nursesand technicians’ perceptions of ergonomic risk factors in the surgicalenvironment. Appl. Ergon. 40, 833–839.

188 J. Bartnicka / Safety Science 71 (2015) 178–188
Soueid, A., Oudit, D., Thiagarajah, S., Laitung, G., 2010. The pain of surgery: painexperienced by surgeons while operating. Int. J. f Surg. 8, 118–120.
Szeto, G.P.Y., Cheng, S.W.K., Poon, J.T.C., Ting, A.C.W., Tsang, R.C.C., Ho, P., 2012.Surgeons’ static posture and movement repetitions in open and laparoscopicsurgery. J. Surg. Res. 172, e19–e31.
Trejoa, A., Jungc, M.-Ch., Oleynikov, D., Hallbeck, M.S., 2007. Effect of handle designand target location on insertion and aim with a laparoscopic surgical tool. Appl.Ergon. 38, 745–753.
Väyrynen, S., Pekkarinen, A., Tornberg, V., 1994. Some links between accidents, posturalload and accessibility in chemical plant maintenance. Saf. Sci. 18, 125–133.
Vedder, J., 1998. Identifying postural hazards with a video-based occurrencesampling method. Int. J. Ind. Ergon. 22, 373–380.
Vincent, Ch., Moorthy, K., Sarker, S.K., Chang, A., Darzi, A.W., 2004. Systemsapproaches to surgical quality and safety. From concept to measurement. Ann.Surg. 239 (4), 475–482.
Waters, T.R., Putz-Anderson, V., Garg, A., Fine, L.J., 1993. Revised NIOSH equation forthe design and evaluation of manual lifting tasks. Ergonomics 36, 749–776.
Whitea, H.A., Kirby, R.L., 2003. Folding and unfolding manual wheelchairs: anergonomic evaluation of health-care workers. Appl. Ergon. 34, 571–579.
Wichert, A., Marcos-Suarez, P., Vereczkei, A., Seitz, T., Bubb, H., Feussner, H., 2004.Improvement of the ergonomic situation in the integrated operating room forlaparoscopic operations. Int. Congr. Ser. 1268, 842–846.
Xiao, D.J., Jakimowicz, J.J., Albayrak, A., Goossens, R.H.M., 2012. Ergonomic factorson task performance in laparoscopic surgery training. Appl. Ergon. 43, 548–553.
Xinhua, L., Youhui, L., Qi, L., 2011. Virtual assembly and simulation of vibration sievebased on a human-interface environment. Proc. Eng. 15, 2988–2992.
Youssef, Y., Lee, G., Godinez, C., Sutton, E., Klein, R.V., George, I.M., Seagull, F.J., Park,A., 2011. Laparoscopic cholecystectomy poses physical injury risk to surgeons:analysis of hand technique and standing position. Surg. Endosc. 25, 2168–2174.


















