
Knowledge and Performance of Critical Care Nurses Toward...
14
Med. J. Cairo Univ., Vol. 81, No. 2, September: 81-94, 2013 www.medicaljournalofcairouniversity.net Knowledge and Performance of Critical Care Nurses Toward Nebulizer Therapy in the Intensive Care Unit at Assiut University Hospital FARES A.A. KHODISH, B.Sc.N*; MONA A. MOHAMMED, D.N.Sc.*; MERVAT ANWAR ABD EL-AZIZ, D.N.Sc.* and HANY AHMED IBRAHEM, M.D.** The Departments of Critical Nursing* and Anesthesiology**, Faculties of Nursing* and Medicine**, Assiut University Abstract Background: A nebulizer is an important device used to inhalant the drugs to treat some pulmonary diseases. The examination of nurse's knowledge and performance regarding the nebulizer therapy has not been conducted before at Assiut University Hospital. Aim of Study: Asses critical care nurse's knowledge and performance related to nebulizer therapy. Methods: Descriptive design was adapted for this study. The sample of this study consisted of 80 nurses working in three intensive care units (38 nurses in traumatic ICU, 20 nurses in postoperative ICU and 22 in general ICU). Two tools were used to collect the required data; nurses' knowledge assessment questionnaire and skills observation checklist related to nebulizer therapy. Results: The findings revealed that (56.2%) of nurses have knowledge about nebulizer therapy at unsatisfactory level (Mean±SD=27.44±12.09) also the findings revealed that (88.8%) of nurses had performance about nebulizer therapy at unsatisfactory level (Mean±SD=29.25±15.97). There was a positive strong relationship between knowledge and perfor- mance regarding nebulizer therapy (r=0.277, p=0.013). Conclusions: Nurse's knowledge and performance about nebulizer therapy were unsatisfactory so that the nurses should be trained enough to give effective and safe care to such patients. Key Words: Nursing knowledge — Nursing performance — Nebulizer therapy. Introduction AEROSOLIZED medications can greatly benefit critically ill patients with respiratory disorders. However, for an aerosol to be clinically useful, it must be delivered effectively to the airways as well as produce a desired therapeutic effect once Correspondence to: Dr. Mona A. Mohammed, The Department of Critical Nursing, Faculty of Nursing, Assiut University delivered pi. A nebulizer is an electrically powered machine that turns liquid medication into a mist so that it can be breathed directly into the lungs through a face mask or mouthpiece [21. It is gener- ally believed that nebulizers are superior to MDIs during mechanical ventilation. The delivery of bronchodilators with MDI in mechanically venti- lated patients has received considerable interest in recent years. This is because the use of metered dose inhalation (MDI) has several advantages over the nebulizer, such as reduced cost, ease of admin- istration, less personnel time, reliability of dosing and a lower risk of contamination. The use of nebulizers under certain circumstances may lead to patient/ventilator dyssynchrony. Finally, nebu- lizers may damage the expiratory transducer of some ventilators, rendering the expiratory volume measurement unreliable [31. Bronchodilators are frequently used in ICU patients receiving invasive mechanical ventilation (IMV) and commonly de- livered through the inhalation route [4]. Medication that is inhaled in the form of small droplets is absorbed immediately into the mucosa and blood stream and is available to the body within minutes. This method of medication delivery is one of the fastest, noninvasive methods of medications de- signed to ease respiratory distress symptoms such as those seen with asthma [51. Some studies reflect that, there are advantages of nebulizertreatment including: Patient coordination required, effective with tidal breathing, high dose possible, dose medication possible, can be used with supplemental oxygen, systemic side effects are less frequent and severe with inhalation compared to systemic deliv- ery (injection, oral); e.g., less muscle tremor, tachycardia, Can deliver combination therapies if compatible and Ultrasonic nebulizer is quiet, and has faster delivery are smaller and more portable 81
Transcript of Knowledge and Performance of Critical Care Nurses Toward...

Med. J. Cairo Univ., Vol. 81, No. 2, September: 81-94, 2013 www.medicaljournalofcairouniversity.net
Knowledge and Performance of Critical Care Nurses Toward Nebulizer Therapy in the Intensive Care Unit at Assiut University Hospital
FARES A.A. KHODISH, B.Sc.N*; MONA A. MOHAMMED, D.N.Sc.*; MERVAT ANWAR ABD EL-AZIZ, D.N.Sc.* and HANY AHMED IBRAHEM, M.D.**
The Departments of Critical Nursing* and Anesthesiology**, Faculties of Nursing* and Medicine**, Assiut University
Abstract
Background: A nebulizer is an important device used to inhalant the drugs to treat some pulmonary diseases. The examination of nurse's knowledge and performance regarding the nebulizer therapy has not been conducted before at Assiut University Hospital.
Aim of Study: Asses critical care nurse's knowledge and performance related to nebulizer therapy.
Methods: Descriptive design was adapted for this study. The sample of this study consisted of 80 nurses working in three intensive care units (38 nurses in traumatic ICU, 20 nurses in postoperative ICU and 22 in general ICU). Two tools were used to collect the required data; nurses' knowledge assessment questionnaire and skills observation checklist related to nebulizer therapy.
Results: The findings revealed that (56.2%) of nurses have knowledge about nebulizer therapy at unsatisfactory level (Mean±SD=27.44±12.09) also the findings revealed that (88.8%) of nurses had performance about nebulizer therapy at unsatisfactory level (Mean±SD=29.25±15.97). There was a positive strong relationship between knowledge and perfor-mance regarding nebulizer therapy (r=0.277, p=0.013).
Conclusions: Nurse's knowledge and performance about nebulizer therapy were unsatisfactory so that the nurses should be trained enough to give effective and safe care to such patients.
Key Words: Nursing knowledge — Nursing performance —Nebulizer therapy.
Introduction
AEROSOLIZED medications can greatly benefit critically ill patients with respiratory disorders. However, for an aerosol to be clinically useful, it must be delivered effectively to the airways as well as produce a desired therapeutic effect once
Correspondence to: Dr. Mona A. Mohammed, The Department of Critical Nursing, Faculty of Nursing, Assiut University
delivered pi. A nebulizer is an electrically powered machine that turns liquid medication into a mist so that it can be breathed directly into the lungs through a face mask or mouthpiece [21. It is gener-ally believed that nebulizers are superior to MDIs during mechanical ventilation. The delivery of bronchodilators with MDI in mechanically venti-lated patients has received considerable interest in recent years. This is because the use of metered dose inhalation (MDI) has several advantages over the nebulizer, such as reduced cost, ease of admin-istration, less personnel time, reliability of dosing and a lower risk of contamination. The use of nebulizers under certain circumstances may lead to patient/ventilator dyssynchrony. Finally, nebu-lizers may damage the expiratory transducer of some ventilators, rendering the expiratory volume measurement unreliable [31. Bronchodilators are frequently used in ICU patients receiving invasive mechanical ventilation (IMV) and commonly de-livered through the inhalation route [4]. Medication that is inhaled in the form of small droplets is absorbed immediately into the mucosa and blood stream and is available to the body within minutes. This method of medication delivery is one of the fastest, noninvasive methods of medications de-signed to ease respiratory distress symptoms such as those seen with asthma [51. Some studies reflect that, there are advantages of nebulizertreatment including: Patient coordination required, effective with tidal breathing, high dose possible, dose medication possible, can be used with supplemental oxygen, systemic side effects are less frequent and severe with inhalation compared to systemic deliv-ery (injection, oral); e.g., less muscle tremor, tachycardia, Can deliver combination therapies if compatible and Ultrasonic nebulizer is quiet, and has faster delivery are smaller and more portable
81

82 Knowledge & Performance of Critical Care Nurses
[6]. Aerosolized medication if not performed with appropriate technique, will lead to several conse-quences and perils such as mucosa irritation, bron-chospasm, dyspnea, airway burns (when heating elements are used), headaches, coughing, tachy-cardia, palpitations, nausea and precipitation of bronchoconstriction most common in asthmatic and COPD patients and may result in hypoxemia [7] . Aerosolized medication must be performed according to right standards and codes in order to reduce its side effects [8]. Diggory & Vallone [9], demonstrated in a study that performing aerosolized medication by well-educated nurses and after checking patient's need has better effect and fewer side effects than performing it routinely [10]. Also revealed in a study that performing aerosolisolized medication by themselves according to the codified protocol will minimize its side effects. Despite the existence of several studies, manual on the basis of evidences about aerosolized medication by nebulizer is not available in most units. There for performing aerosolized medication by nebulizer with the observance of such experimental evidences by nurses is on question 1111. Day et al., [12] in two separate studies in intensive and acute care units, realized nurses' lacking knowledge which was reflected in their performance Nurses are one of the major components of manpower in the field of healthcare. The skills and knowledge of nursing personnel may be directed towards health promo-tion, crisis intervention, maintenance, rehabilitation/ restoration or palliation in care of critically ill patient [13] . Nursing rolebefore using Nebulizer; assess the patient's respiratory status. Note if the patient is using accessory muscles for respiration or if there is flaring of the nares. Auscultate the client's chest for wheezes and crackles. Respiratory distress is the primary reason to administer nebu-lized treatment, the nurse must Place the patient in an upright position (40 to 90 degrees), which allows deep ventilation and maximal diaphragmatic movement Put the mouthpiece in the mouth, be-tween teeth, and close the lips (if using a mask, cover mouth and nose with the mask). Assess the breath sound, pulse rate, respiratory status, oxygen saturation; assess the heart rate during the treatment. In pregnant patient, the fetal heart rate should also be assessed, instruct the patients to take slow deep breaths for 10 seconds through the mouth and hold at end inspiration and wash face if using a mask to prevent rash [1 4] . The nurse must follow the following steps when preparing a medication by a nebulizer machine; if you have the multiple dose vial be; Squeeze the dropper to fill it to the line that matches your prescribed dose, squeeze the medicine into the medicine cup, most medicines
that comes in multiple dose vials needs to be diluted with normal saline [5] . The nurse instructs the patient to do breathing exercise for two or three seconds to give the medication time to fully enter the airways of The lungs. After this first breath continue this cycle of exhalation and inhalation until the dose of medication is finished. Typically, treatment will take roughly five to 10 minutes [15]. During the nebulizing; therapy it may be necessary for the nurse to suction the patient's tracheostomy to enable removal of secretions. This should only be carried out if necessary and if the patient is unable to cough the secretions out of the tube themselves. It should be remembered that suction-ing is an invasive procedure, which may be uncom-fortable and frightening for the patient. It should only be carried out following careful assessment of the need for suctioning and should only be undertaken by practitioners who are competent. Patient indications for suctioning may include: Visible or audible secretions that patient are unable to clear, patient distress, clammy skin or sweating, increased heart rate/respiratory rate reduced oxygen saturation [1 6] . The role of the nurse toward the patient with nebulizer therapy for promoting res-piratory care based. The nurse instructs the patient to breathe through the mouth, taking slow, deep breaths, and then to hold the breath for a few seconds at the end of inspiration for increasing the intrapleural pressure and reopen collapsed alveoli, therapy increasing function residual capacity, the nurse encourage the patient to cough and to monitor the effectiveness of the therapy [17]. So, the signif-icance of the study from an organizational perspec-tive, the large and increasing number of noninvasive procedures at intensive care unit may result in capacity problems such as respiratory infection. A possible solution for these problems might be a reduction in length hospital stay. The number of nebulizer therapy performed at Assiut University ICU units in 2010-2011 more than 450 intervention procedures Observation of nebulizer therapy at ICU showed that most patient who performed nebulizer therapy. Therefore the aim of this study is to investigate Knowledge and practices levels of nurses in ICU at Assiut University Hospital. This study could be beneficial in many ways; first, it will provide data-base that can be utilized by health team members to raise nurse's awareness, and initiate more active nurse's roles at intensive care unit. Second, Health professionals can utilize such information in the care plan for such group of nurses in the future. Third, proper nursing as-sessment and monitoring can improve patient's outcome.

Fares A.A. Khodish, et al. 83
Subjects and Methods
Research design: Descriptive design was adapt-ed for this study.
Studyaim: Investigate critical care nurses' knowledge and performance related to nebulizer therapy.
Research questions: What are nurses' knowledge and performance of toward nebulizer therapy in the intensive care unit at Assiut University Hospital.
Material: Setting:
This study was conducted in three intensive care units (general intensive care units, postoper-ative intensive care units & traumatic intensive care units) at Assiut University Hospital.
Subjects: A sample of convenience included all the avail-
able nursing staff working at the general intensive care units (22 nurses), postoperative intensive care units (20 nurses) & traumatic intensive care units I.C.0 (38 nurses) at Assiut University Hospital (Total 80 nurses).
Tools: Two tools were used to collect the required
data; nurses' knowledge assessment questionnaire and skills observation checklist related to nebulizer therapy.
Tool (1): Nurses' knowledge assessment Question-naire:
Arabic interview questionnaire sheet was con-structed after reviewing the relevant literature to assess nurses' knowledge about a nebulizer ma-chine. It was developed and translated into Arabic language. Thequestionnaire was included three parts. Part (1): Is for nurses' characteristics such asage, marital status, years of experience, depart-ment, qualifications and their attendance of related course training about a nebulizer machine. Part (2): Thispartassesses nurses' knowledge related to nebulizer machine in general such as type, indica-tions for applications, and complications of nebu-lizer machine. Part (3): Assess nurses' knowledge concerning nebulizer therapy related practices including knowledge regarding assessment, prep-aration, application, post nursing care, and docu-mentation of nebulizer therapy.
The total score for this questioner tool was 24 points, the correct response answer was scored as "1" and incorrect response or do not know as "o". The Satisfactory level of knowledge equal or more
than 60% of the maximum score. Unsatisfactory level of knowledge less than 60% of the maximum
Tool (2): Skills observation checklist tool: This tool was adapted from Potter et al., it was
used to assess nursing performance while applying and providing maintenance care of nebulizer ther-apy. The check list items included 71 items. It consists of three parts. Part (1): Includes type of the ICU and the shift (morning, evening or night) when the observation checklist was taken. Part (2): Involves patients' characteristics, such as; age, medical diagnosis and past history. Part (3): Was used to observe nurses' practices while applying and maintaining the nebulizer therapy. It contains five main section covering the main steps of neb-ulizer use and care; assessment, preparation, post-care, maintenance and documentation. First section was for assessment which involves items to be assessed before the application of nebulizer therapy, such as indication of nebulizertherapy, physician's order and medications which used by nebulizer therapy. Second section was concerned with the preparation of equipment and patient. Third section was for the application of the nebulizer therapy including practices such as, breathexercises, vital-singes, suction, mechanical ventilation, pulse oxim-etry, oxygen therapy and arterial blood gas. Section four involves post care practices such as; washing hands and regular care while the nebulizer therapy was maintained. Finally, section five was; docu-mentation of the type of nebulizer, medications, time, indications and unexpected outcomes for nebulizer therapy. Satisfactory levelof performance equal or more than 60% of the maximum score. Unsatisfactory level of performance less than 60% of the maximum score.
Methods: Permission was obtained from the hospital
administrative authority to collect the necessary data. Validation of the study tools was assessed by presenting them to five experts from the critical care nursing field. A pilot study was carried out in march-July 2012 to test the tool. A pilot study was conducted for purpose of testing clarity, complete-ness, and validity, practicability of the study tools of (5) nurses to determine the time involvement. Also it was done to show the possibility and effec-tiveness of using the observation checklist. Neces-sary modification was done. Testing the questions ware done to see if they are relevant and if they elicit the type of information, which are thought according to the answers and comments made by nurse. Some details not required were omitted, either to advance or reduce the tool lengthy test. Also to show the possibility and the effectiveness

84 Knowledge & Performance of Critical Care Nurses
of using the observation checklist regarding the policy of hospital performance
The observation checklist was carried out while the nurses were working during their shifts in these units. Each observation lasted for 20 minutes by using the direct observation technique. At initial interview the researcher explain the nature & purpose of the study, prior to answering the ques-tions to gain their oral consent & cooperation, and fill out the questionnaire sheet by nurses were on duty during morning,afternoon and night shifts. Nurses were observed two hours for each nurse, while they were performance nursing intervention for their patient during this period. The whole period for implementation of study was morning shift.
Statistical analysis:
Data entry was done using compatible personal computer by the investigator. The statistical analysis was done using SPSS-16 statistical software pack-age. The content of each tool was analyzed, cate-gorized and then coded by the investigator. Data were presented using descriptive statistics in the form of frequencies and percentages for qualitative variables, Quantitative continuous data were com-pared using student t-test in case of comparisons between three groups. Pearson correlation analysis was used for assessment of the inter-relationships among quantitative variables. Statistical signifi-cance was considered at p-value<0.05.
Results
Table (1): Presentation of study group at three units in intensive care units.
I.C.0 trauma Postoperative I.C.0 (n=38) (n=20)
No. % No.
10 26.3 6 21 55.2 9 7 18.4 5
10 26.3 4 7 18.42 5 21 55.2 11
4 10.5 7 25 65.7 5 9 23.6 8
0 00.0 0 38 10.0 20
General I.C.0 (n=22) DF=2
No. % X2 p-value
9 7
40.9 31.8
3.187
6 27.2 0.527
2 9.0 6 27.2 2.825 0.588 14 63.6
4 18.1 7 31.8 13.219 0.010* 11 50.0
0 00.0 22 10.0
Characteristics
Age in years: <25 years 25-30 years >30 years
Qualification: Nursing Bachelor Nursing Technical Institute Nursing Diploma
Years of experience: <5 years 5-10 years 10 years and more
Training course: Attended Not attended.
%
30.0 45.0 25.0
20.0 25.0 55.0
35.0 25.5 40.0
00.0 10.0
(*) Statistical significant difference (p<0.05).
Table (1) showed that the total number of nurses are (80) nurses from different of intensive care units, (38) nurses from trauma intensive care unit, (20) from post operative & (22) from general intensive care unit. The majority of nurses (55.2%) were between 25-30 years old in traumatic ICU, The majority of the nurses were nursing diploma (63.6%) in general ICU, and all nurses had no previous training courseabout nebulizer (100%).
There was statistical significant difference related to years of experience (p-value=0.010) and the majority of nurses (65.7%) were between 5-10 years in trauma ICU.
IN;Ll Unsatisfactory
56.2%
Fig. (1): Illustrate nurses' knowledge about nebulizer.
This figure shows that (56.2%) of nurses at unsatisfactory level of knowledge.

Fares A.A. Khodish, et al. 85
Table (2): Description of nurses' knowledge related to nebulizer therapy at three units.
Nurses' knowledge
Units
p-value I.C.0 Postoperativ General
Unsatisf. Satisfact. Unsatisf. Satisfact. Unsatisf. Satisfact.
No. % No. % No. % No. % No. % No. %
Define the nebulizer 20 52.6 18 47.4 10 50.0 10 50.0 17 77.3 5 22.7 0.115 Indications of nebulizer 3 7.9 35 92.1 1 5.0 19 95.0 2 9.1 20 90.9 0.874
Assessment: Sings of hypoxemia 12 31.6 26 68.4 8 40.0 12 60.0 16 72.7 6 27.3 0.007* The lung sound. 16 42.1 22 57.9 9 45.0 11 55.0 16 72.7 6 27.3 0.059 Chest secretions 34 89.4 4 10.5 18 90.0 2 10.0 21 95.4 1 4.5 0.542 The arterial blood gases 12 31.5 28 73.6 5 25.0 15 75.0 10 45.4 12 54.5 0.214 Pulse oximetry 7 18.4 31 81.6 5 25.0 15 75.0 12 54.5 10 45.5 0.011* Pulmonary function test 7 18.4 31 81.6 3 15.0 17 85.0 10 45.5 12 54.5 0.033*
Prepare: The equipment 12 31.5 26 68.4 9 45.0 11 55.0 17 77.2 5 22.7 0.003* The medication 4 10.5 34 89.5 1 5.0 19 95.0 4 18.2 18 81.8 0.394 Checkthe connections 14 36.8 24 63.1 14 70.0 6 30.0 13 59.0 9 40.9 0.039*
Explain breathing exercises 22 57.9 16 42.1 10 50.0 10 50.0 17 77.3 5 22.7 0.163
Complications of nebulizer 28 73.6 10 26.3 16 80.0 4 20.0 19 86.3 3 13.6 0.048*
(*) Statistical significant difference (p<0.05).
Table (2) shows that there were significant difference in nurses' knowledge about Sings of hypoxemia patient (p-value=0.007), and the ma-jority of nurses in General I.C.0 were at unsatis-factory level (72.7%). Also, there was significant difference in nurses' knowledge about pulse oxime-tery (p-value=0.011) and the majority of nurses in I.C.0 trauma were at satisfactory level (81.6%).
Shows there were significant difference in nurses' knowledge aboutpulmonary function test (p-value=0.033) and the majority of nurses in postoperative I.C.0 were at satisfactory level (85.0%). There was significant difference in nurses'
knowledge about prepare theequipment (p-value= 0.003) and the majority of nurses in general ICU were at Unsatisfactory level (77.2%).
There was significant difference in nurses' knowledge about Check all connections of nebulizer (p-value=0.039) and the majority of nurses in postoperative I.C.0 were at Unsatisfactory level (70%).
There was significant difference in nurses' knowledge about complications of nebulizer (p-value=0.048) and the majority of nurses in general I.C.0 were at unsatisfactory level (86.3%).
Table (3):Difference between nurses' knowledge related to nebulizer therapy according to qualification.
Nurses' knowledge
Qualification
p-value Nursing Bachelor
(n=16) Technical Institute
(n=18) Nursing Diploma
(n=46) Unsatis- factory
Satis- factory
Unsatis- factory
Satis- factory
Unsatis- Satis- factory factory
No. % No. % No. % No. % No. % No. % Define of nebulizer 3 18.8 13 81.3 12 66.7 6 33.3 36 78.3 10 21.7 0.000* Indications nebulizer 2 12.5 14 87.5 4 22.2 14 77.8 4 8.7 42 91.3 0.194
Assessment: Signs of hypoxemia 7 43.8 9 56.3 4 22.2 14 77.8 25 54.3 21 45.7 0.067 The lung sound. 13 81.2 3 18.7 16 88.8 2 11.1 46 100.0 0 0.00 0.026* Thechest secretions. 16 100.0 0 0.0 16 88.9 2 11.1 44 95.7 2 4.3 0.317 Arterial blood gases 5 31.3 11 68.8 9 50.0 9 50.0 14 30.4 32 69.6 0.317 Pulse oximetry 4 25.0 12 75.0 4 22.2 14 77.8 16 34.8 30 65.2 0.546 Pulmonary function test 4 25.0 12 75.0 3 16.7 15 83.3 13 28.3 33 71.7 0.629
Prepare medication 2 12.5 14 87.5 1 5.6 17 94.4 6 13.0 40 87.0 0.685
Cleans the equipments 12 31.5 26 68.4 9 45.0 11 55.0 17 77.2 5 22.7 0.003*
Explain: Breathing exercises. 3 81.8 13 18.2 2 11.1 16 88.9 4 8.7 42 91.3 0.548 Procedures of neubilizer 5 31.2 11 68.7 6 33.3 12 66.6 29 63.0 17 37.0 0.024*.
Complications of nebulizer 12 75.0 3 25.0 14 77.7 4 22.2 42 91.3 4 8.7 0.872
(*) Statistical significant difference (p<0.05).
86 Knowledge & Performance of Critical Care Nurses
Table (3) shows there were significant difference in nurses' knowledge aboutdefine of nebulizer (p- value=0 .000) and the majority of nurses in Nursing Bachelorwere at satisfactory level (81.3%), there were significant difference in nurses' knowledge aboutdefine of lung sound (p-value=0.026) and the majority of nurses in Nursing Bachelorwere at unsatisfactory level (81.2%), there were significant
Table (4): Differences nurses' knowledge and nurses' charac-teristics according to department, education, and experience.
Level of Knowledge Nurses'
characteristics
Unsatisfactory Satisfactory p-value
No. % No. % Department:
I.C.0 trauma 20 52.6 18 47.4 47.4 I.C.0 postoperative 10 50.0 10 50.0 50.0 General I.C.0 15 68.2 7 31.8 31.8
Education: Nursing Bachelor 4 25.0 12 75.0 75.0 Nursing Diploma 32 69.6 14 30.4 30.4 Nursing Technical 9 50.0 9 50.0 50.0
Institute
Experience: <5 years 12 80.0 3 20.0 20.0 5-10 years 22 59.5 15 40.5 40.5
10 years 11 39.3 17 60.7 60.7
(*) Statistical significant difference (p<0.05).
Table (4) shows that there was significant dif-ferences regarding to education (p-value=0.07) and experiences (p-value=0.32).
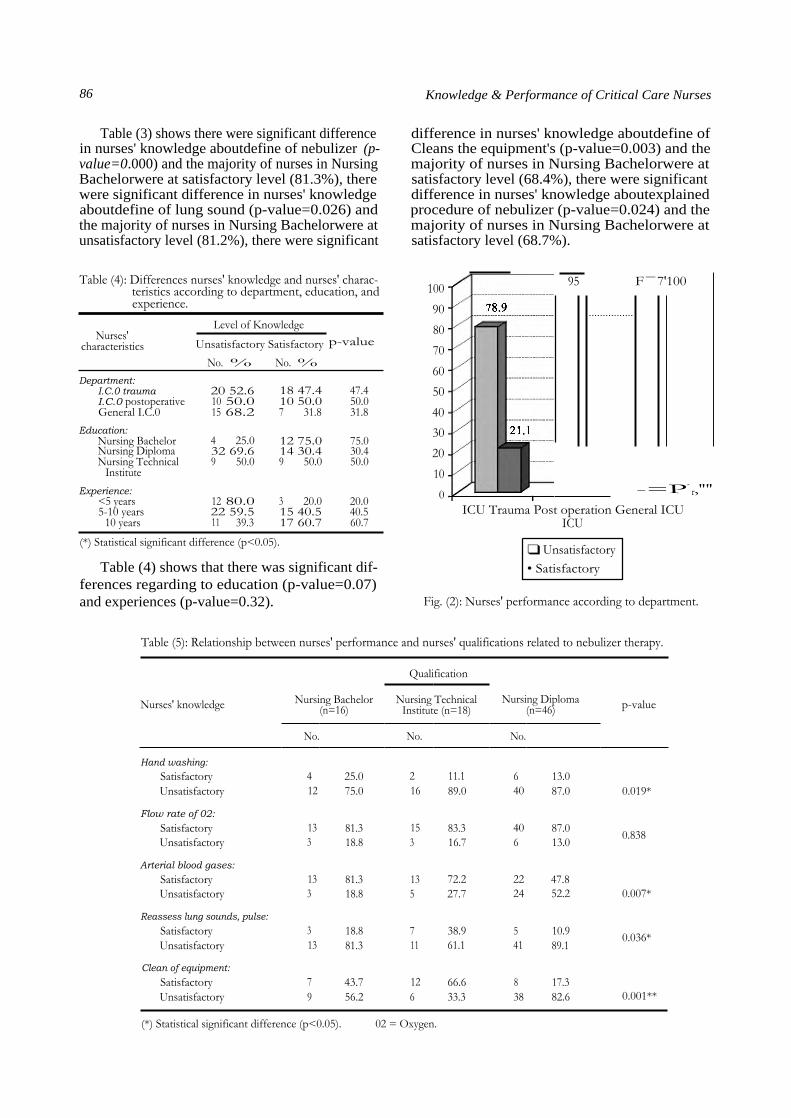
difference in nurses' knowledge aboutdefine of Cleans the equipment's (p-value=0.003) and the majority of nurses in Nursing Bachelorwere at satisfactory level (68.4%), there were significant difference in nurses' knowledge aboutexplained procedure of nebulizer (p-value=0.024) and the majority of nurses in Nursing Bachelorwere at satisfactory level (68.7%).
95 F-7'100
-=P-r,""
ICU Trauma Post operation General ICU ICU
❑ Unsatisfactory • Satisfactory
Fig. (2): Nurses' performance according to department.
100
90
80
70
60
50
40
30
20
10
0
Table (5): Relationship between nurses' performance and nurses' qualifications related to nebulizer therapy.
Nurses' knowledge Nursing Bachelor (n=16)
Qualification
Nursing Diploma (n=46) p-value Nursing Technical
Institute (n=18)
No. No. No.
Hand washing: Satisfactory 4 25.0 2 11.1 6 13.0 Unsatisfactory 12 75.0 16 89.0 40 87.0 0.019*
Flow rate of 02: Satisfactory 13 81.3 15 83.3 40 87.0 0.838 Unsatisfactory 3 18.8 3 16.7 6 13.0
Arterial blood gases: Satisfactory 13 81.3 13 72.2 22 47.8 Unsatisfactory 3 18.8 5 27.7 24 52.2 0.007*
Reassess lung sounds, pulse: Satisfactory 3 18.8 7 38.9 5 10.9 0.036* Unsatisfactory 13 81.3 11 61.1 41 89.1
Clean of equipment: Satisfactory 7 43.7 12 66.6 8 17.3 Unsatisfactory 9 56.2 6 33.3 38 82.6 0.001**
(*) Statistical significant difference (p<0.05). 02 = Oxygen.

Fares A.A. Khodish, et al. 87
Table (5) shows significant difference in nurs-es' performance about washing hands (p-value =0.019) and the majority of nurses innursing Technical Institute were at unsatisfactory level (89.0%).
There was significant difference in nurses' performance about Arterial blood gases (p-value= 0.007) and the majority of nurses in nursing bach-elor were at satisfactory level (81.3%).
There was significant difference in nurses' performance aboutreassessing breath sounds, pulse, oxygen saturation, respiratory rate, (p-value=0.036) and the majority of nurses in nursing diploma were at unsatisfactory level (89.1%).
There was significant difference in nurses' per-formance aboutwashing all parts of the nebulizer (p-value=0.001) and the majority of nurses in nurs-ing diploma were at unsatisfactory level (82.6%).
Table (6): Nurses performance related to nebulizer of MV (mechanical ventilation) according to qualifications.
Qualification
Nurses' knowledge Nursing Bachelor Nursing Technical Nursing Diploma (n=16) Institute (n=18) (n=46) p-value
No. No. No.
Prepare suction equipment:
Satisfactory 14 87.5 14 77.77 33 71.73 Unsatisfactory 2 12.5 4 22.22 13 28.26 0.436
Reassess vital signs: Satisfactory 11 68.7 11 61.11 22 47.82
0.035* Unsatisfactory 5 31.25 7 38.88 24 52.17
Cleans the equipment:
Satisfactory 4 25.0 6 33.33 11 23.39 0.950 Unsatisfactory 12 75.0 12 66.66 35 76.08
Attach MV to endotracheal tube/tracheostomy tube:
Satisfactory 14 87.5 15 83.33 17 00.0 0.010* Unsatisfactory 2 12.5 3 16.66 29 100.0
Secure ventilator tabling:
Satisfactory 12 75.0 11 61.11 0 00.0 0.010* Unsatisfactory 4 25.5 7 38.88 46 100,0
Setup nebulizer which attached with MV:
Satisfactory 12 75.0 13 72.22 32 69.56 0.913 Unsatisfactory 4 25.0 5 27.77 14 30.43
Document all finding before & after therapy: Satisfactory 12 75.0 15 83.33 34 73.91 0.817 Unsatisfactory 4 25.0 3 16.66 12 26.08
(*) Statistical significant difference (p<0.05).
Table (6) shows there were significant difference in nurses' performance about Reassess vital signs (p-value=0.035) and the majority of nurses in Nursing Technical Institute were at satisfactory level (77.7%).
There was significant difference in nurses' performance about Attach mechanical ventilator
to endotracheal tube or tracheostomy tube (p-value =0.10) and the majority of nurses in Nursing Bach-elor were at satisfactory level (87.5%).
There was significant difference in nurses' performance aboutsecure ventilator tabling (p-value=0.010) and the majority of nurses in Nursing Bachelor were at satisfactory level (75%).

Nurses' performance
Units
p-value I.C.0 trauma (n=38)
Postoperative I.C.0 (n=20)
General I.C.0 (n=22)
No. % No. % No. % Prepared suction equipment:
Satisfactory 30 78.9 14 70.0 15 68.2 Unsatisfactory 8 21.1 6 30.0 7 31.8 0.598
Lung sound: Satisfactory 3 7.9 2 10.0 1 4.5 Unsatisfactory 35 92.1 18 90.0 21 95.5 0.792
Reassess vital signs: Satisfactory 8 21.1 3 15.0 1 4.5 Unsatisfactory 30 78.9 17 85.0 21 95.5 0.226
Cleans the equipment at least once daily: Satisfactory 11 28.9 6 30.0 4 18.1 Unsatisfactory 27 71.1 14 70.0 18 81.8 0.012*
Attach MV to endotracheal tube or tracheostomy tube:
Satisfactory 33 86.8 16 30.0 0 0.0 Unsatisfactory 5 13.2 4 70.0 22 100.0 0.000*
Secure ventilator tabling: Satisfactory 28 73.7 17 85.0 0 0.0 Unsatisfactory 10 26.3 3 15.0 22 100.0 0.000*
Documentation: Satisfactory 33 86.8 17 85.0 18 81.8 Unsatisfactory 5 13.2 3 15.0 4 18.2 0.871
Table (7) shows that there was significant dif-ference in nurses' performance about Cleans the equipment at least once daily (p-value=0.012) and the nurses of the majority in general I.C.0 were at unsatisfactory level (81.8%).
There was significant difference in nurses' performance about Attach mechanical ventilator to endotracheal tube or tracheostomy tube (p-value
=0.000) and the majority of the nurses in general I.C.0 were at unsatisfactory level (0.100%).
There was significant difference in nurses' performance about Secure ventilator tabling to reduce pull on tracheostomy or endotracheal tube (p-value = 0.000) and the majority of nurses in general I.C.0 were at unsatisfactory level (100%).
Table (8): Nurses performance related to nebulizer of mechanical ventilation (MV) according to experiences.
88 Knowledge & Performance of Critical Care Nurses
Table (7): Nurses' performance related to nebulizer of mechanical ventilation according to units.
Nurses' performance
Year of experiences
p-value <5 years (n=15)
5-10 years (n=37)
>10 years (n=28)
No. % No. % No. % Prepared suction equipment readily available:
Satisfactory 12 80 28 75.67 18 64.28 Unsatisfactory 3 20 9 24.32 10 35.71 0.314
Reassess vital signs, breathing and lung sound: Satisfactory 4 26.6 10 27.0 11 39.28 Unsatisfactory 11 73.3 27 73.0 17 60.71 0.048*
Cleans the equipment: Satisfactory 5 33.33 10 27.0 16 57.14 Unsatisfactory 10 66.66 27 73.0 12 42.85 0.042*
Attach MV to endotracheal /tracheostomy tube: Satisfactory 13 86.66 33 89.18 27 96.42 Unsatisfactory 2 13.33 4 10.81 1 3.57 0.465
Secure MV tabling: Satisfactory 7 46.66 29 78.37 20 71.42 Unsatisfactory 8 53.33 8 21.62 8 28.57 0.076
Setup nebulizer which attached with MV: Satisfactory 9 60.0 30 81.08 22 78.57 Unsatisfactory 6 40.0 7 18.91 6 13.04 0.253
Documentation: Satisfactory 13 86.6 29 78.37 19 67.85 Unsatisfactory 2 13.33 8 21.62 9 3.57 0.353
(*) Statistical significant difference (p<0.05).

r=0.277 - - - - p=0.013* 0
0
0 00 0 0 0
o 0 000 0 0 0 0
0 0 0 0 0 0 0 0 0
- - - - - - - -0 - - - - -00- - - -a 0 0 00 0
0 00 0 0 0 0 0
0 0 0 0 -o 0- 0-0- 0 00
0 0 0 0
30.00
25.00
20.00
15.00
10.00 -
Fares A.A. Khodish, et al. 89
Table (8) shows there were significant difference in nurses' performance about Reassess vital signs (p-value=0.048) and the majority of the nurses at the age less than 5 years old were at satisfactory level (73.3%).
There was significant difference in nurses' performance about Cleans the equipments at least once daily (p-value=0.042) and the majority of the nurses at the age between 5 to 10 years old (30.0%).
5.00 10.00 15.00 20.00 25.00 30.00 35.00 (*) Statistical significant difference (p<0.05). Fig. (3): Correlation between nurses'
knowledge and performance.
There was a significant positive correlation between score of knowledge and score of perfor-mances (p-value=0.013).
Table (9): Relationship between nurses' performance and nurses' characteristicsaccording to department, education, and experience
Nurses' characteristics
Nurses' performance
p-value Unsatis- factory
Satis- factory
No. % No. %
Department: I.C.0 trauma 30 78.9 8 21.1 Postoperative I.C.0 19 95.0 1 5.0 General I.C.0 22 100.0 0 0.0 0.027*
Education: Nursing Bachelor 10 62.5 6 37.5 Nursing Diploma 45 97.8 1 2.2 Nursing Technical 16 88.9 2 11.1 0.001*
Institute
Experience: <5 years 13 86.7 2 13.3 5-10 years 32 86.5 5 13.5
10 years 26 92.9 2 7.1 0.695
(*) Statistical significant difference (p<0.05).
Table (9) shows that significant differences in nursing performance regarding to department (p-v alue=0 .027) and education (p-value=0.001).
Discussion
Nebulisers are commonly used in the manage-ment of acute exacerbation airways disease. A study was therefore conducted to ascertain what nurses knew about this form of therapy. Several areas of deficient knowledge were revealed, in-cluding how to clean the equipment properly, what the flow rate of gas should be and what type of gas to use. And nursing care for nebuliser therapy is included [17] .
The results of the present study showed that the majority of nurses (55.2%) were between 25 -30 years old in traumatic ICU. the majority of nurses were having nursing diploma (63.6%) in general ICU, and all nurses had no previous training about nebulizer (100%).
This study indicated that there was statistical a significant difference related to years of experi-ence and the majority of nurses were between 5-10 years in trauma ICU. These findings are con-gruent with those of who [18] reported that; years of experience in the hospital significantly correlated to increased knowledge, attitudes and practices among the various categories of staff but this did not translate into good clinical practice in the ward and stated that the education and training are two components of staff development that occur after employee indoctrination (which refers to planned, guided adjustment of employees' organization and work environment). The staff knowledge level and capabilities are a major factor in determining the number of staff required to carry out unit goals. The better trained and more competent the staff, the fewer staff required, which in turn saves the organization money and rise reproductively.
The findings revealed that total knowledge was at an unsatisfactory level. The reasons might be due to education and training of the nurses, all nurses (100%) had not attended training courses about nebulizer. The majority of the nurses in the three units (intensive care unit of trauma, postop-erative intensive care unit and general intensive care unit) had gained a diploma in nursing), There-fore, these factors may affect the unsatisfactory level of knowledge of nurses [19] . Stated that many medical personnel responsible for monitoring and instructing patients in optimal inhaler use. Nurses seldom receive formal training in the use of inhaling devices, and newer inhaling devices designed to obviate problems of technique are at present less likely to be used well by medical personnel soon after their introduction [20] . In another study also discovered that knowledge is acquired primarily

90 Knowledge & Performance of Critical Care Nurses
through experience, usually observation of and working withmentors and continuing education. Tacit knowledge may also be described as practical that is, derived from experience or practice [21]. Recommended that lack of knowledgeable nurses leads to increased risks to patients and may influ-ence patient's outcomes. Nursing shortage also leads to increased workload as the nurse: Patient ratio decreases and one nurse has to provide care for more than one critically ill patient. Shift leaders in both public and private sectors are working under great pressure and a large number of them are also not trained, but simply have the experience of working in an ICU for a number of years.
The current study revealed that the majority of the study sample (81.6%) werehaving satisfactory in nurses' knowledge about pulse oximetery. These finding is in accordance with the results of the study conducted by [22] whomentioned that a pulse oximetry (Sp02) knowledge survey was conducted with 551 experienced critical care nurses at the 2002 American Association of Critical Care Two hundred and seven questionnaires were completed (a response rate of 74.5%). Mean pulse oximetry knowledge, with ICU nurses having significantly higher scores than anesthesia department nurses and those with more than 10 years of experience having significantly higher scores. Correct respons-es did not exceed 50% for six questionnaire items, five of which covered principles of pulse oximetry function. ICU nurses had significantly more correct responses in five items compared to nurses, and in two of them compared to anesthesia department nurses.
It was found in the present study that there was significant difference in nurses' knowledge about cleaning the equipments at least once daily These results are in agreement with the study of Canadian Committee on Antibiotic Resistance, [23], they found that reusable medical equipment must be thoroughly cleaned before disinfection or steriliza-tion, factors that affect the ability to effectively clean medical equipment must be considered prior to cleaning, instruments should be cleaned as soon as possible after use to prevent organic material drying on instruments, place the instrument in a pre-soak of water or an enzymatic solution, this will prevent drying of organic material, organic material must be removed before disinfection or sterilization procedures are initiated and the process for cleaning should include written protocols for disassembly, sorting and soaking, physical removal of organic material, rinsing, drying physical in-spection and wrapping. In this regard Labrague, et al., [24] found that age, gender, length of clinical
experience, and number of trainings attended are not determinants of the knowledge on the principles of sterile technique. This implies that nurses re-gardless of their age, gender, length of clinical experience, and numbers of trainings attended do not differ in knowledge on sterile technique.
The present study of revealed that nurses' knowledge about checking all connections of neb-ulizer and the majority of nurses in postoperative I.C.0 were at unsatisfactory level. McNeal, [25] presented that There are lots of models of nebulizer out there, and each one is a little different from the others. This general guide to nebulizer parts will give a basic idea of what makes a nebulizer system function.
The current study revealed that of nurses' knowl-edge about pulmonary function test were at satis-factory level (85%). In this respect, (Encyclopedia of Nursing) [26], reported that when the results of pulmonary function testing are accurate, the most frequent reason is adequate patient education and/or technician training. It is recommended that person-nel conducting pulmonary function testing have one of the following credentials: Certified respira-tory therapy technician (CRTT); registered respi-ratory therapist (RRT); certified pulmonary function technologist (CPFT); or registered pulmonary function technologist (RPFT).
The results of the present study showed that the majority of studied sample were having unsat-isfactory level of knowledge about complications of the nebulizer. according to (Hoyle, 2012) [27] stated that nurses should have knowledge about any complications that may occur during nebulizer therapy, the patient may become dizzy,complainse of headache or may become disoriented during the course of treatment. If this happens, have patient take off his or her mask or remove his mouthpiece and take a break for a few minutes. Once his head is clear, have him continue the treatment and focus on breathing more slowly than before. In some cases, slower breathing may not resolve dizziness or disorientation. Kulas, [28] who also found that the act of inhaling the medication through a nebu-lizer can cause dry mouth, sore throat, a bad taste in the mouth or hoarseness? Sometimes, nebulizers can cause thrush, which is a yeast infection in the mouth. Symptoms of thrush include white spots in the mouth, bleeding and pain.
The current study results denoted that the ma-jority of the studied nurse's were having a satisfac-tory level of knowledge about the definition of the nebulizer. The present study also showed that there

Fares A.A. Khodish, et al. 91
was significant difference in nurses' knowledge about explaining procedures and the majority of nurses in nursing Bachelor were at satisfactory level of knowledge (68.7%). According to Ethan, [29]the patient should be in a comfortable position throughout the procedure. Once the patient puts the face mask on, he or she can start taking slow, deep breaths. He or she should continue to breathe slowly and deeply until there is no medication left in the Nebulizer cup. This generally takes anywhere from ten to thirty minutes, depending on the pre-scribed quantity of medication.
The current study revealed the majority of nurses in nursing diploma were unsatisfactory knowledge regarding hearing the lung sound (0.00%). This result agrees with Layman, et al., [30]who emphasized that the assessment of the breath sound, pulse rate, respiratory status, oxygen saturation and assess the heart rate during the treatment. In pregnant patient, the fetal heart rate should also be assessed, instruct the patient to take slow deep breaths for 10 seconds through the mouth and hold at end inspiration and wash face if using a mask to prevent rash.
For performance regarding nebulizer, the find-ings showed that total practice was at an unsatis-factory level. The reasons may be due to lack of equipments, ignorance and the activities not in the duties of nurses Plaza, et al., [31] found that a shortage of equipment was identified as obstacle to the facilitation of the nurses' performance in clinical areas.
The present study showed that There was a significant positive correlation between score of knowledge and score of performances (p-value =0.013). This result agreed with Whyte, [32] who have reported that selection of a group of nurses participants was classified as either novice or experienced nurses on the basis of their years of experience. There were 12 experienced nurses and 10 novice nurses. Using an experimental research design based on the expert performance approach, a simulated task environment was developed for the study using a patient simulator and a fully equipped true-to-life intensive care unit suite. Nurses were required to control the physiologic deterioration of the patient with respiratory com-promise in 4 scenarios and were also tested on their knowledge of the constructs present in the scenarios.
The present study revealed significant differ-ences in nursing knowledge regarding to department (p-value=0.027) and education (p-value=0.001) &
there was no significant differences regarding to experiences. Hassan & Aboulazm, [32] stated that the highest mean scores of knowledge was found among nurses' who have bachelor of Science in nursing, and also found there were improvement of nurses' knowledge related to nebulizer.
In the present study we found significant dif-ference in nurses' performance of arterial blood gases (p-value=0.007). Nurses having Bachelor of Sciences in nursing had significantly higher scores than those having technical institute of nursing and those having nursing diploma. Coombs, [33] found that the ABG analysis provides useful mon-itoring, especially for carbon dioxide. In most wards, taking arterial samples has traditionally been a medical role, but some specialist nurses are now taking samples and so need to be able to interpret measurements. Nurses who are not taking samples may be able to initiate earlier intervention if they are able to interpret results. Understanding results can help nurses to understand treatments and interventions, so making nursing more inter-esting.
The present study revealed a significant differ-ence in nurses' performance about reassessing breath sounds, pulse rate, oxygen saturation, res-piratory rate, and peak (p-value=0.036) and the majority of nurses in nursing diploma were at unsatisfactory level (89.1%).
A report by Creed & Spiers, [34] entailed that professional nurse must perform by assessing patient status from breath sounds, respiratory status, pulse rate and other significant respiratory functions needed. Compare, record significant changes and improvement. Refer if necessary and perform other significant respiratory functions. The current study revealed a great lack of performance as regarding of hands washing as all nurses were having an unsatisfactory performance score level and had statistical significant (p-value=0.019). Hand hy-giene is the most important single infection control measure used in nursing [35] .
Pratt, et al., [36] presented that hand contami-nation is one of the main contributing factors in the current infection threat; contaminated hands are responsible for transmitting infection. Effective hand cleaning can significantly reduce infection rates in high risk area. Unfortunately, the result of the present study revealed that the majority of nurses didn't carry out certain procedures in relation to infection control precautions such as hands washing, wearing gloves and cleaning equipments. Lam, et al., [37] presented that hand hygiene has

92 Knowledge & Performance of Critical Care Nurses
been singled out as the most important measures in preventing hospital acquired infection Ahmed, [38] has found lack of knowledge related universal precautions and infection control among nurses.
The current study revealed a great lack of per-formance as regards to washing all parts of the nebulizer. Scores of nurses' performance (p-value =0.001) and the majority of nurses in nursing diploma were at unsatisfactory level (82.6%). According to Ahmed, [39] who found that the ma-jority of nurses practices related to cleaning instru-ments mechanical ventilation inadequately per-formed by nurses having diploma of Science. Robert, et al., [40] mentioned that ineffectual dis-infection of inhalation equipment between therapy sessions of different patients has been reported to produce serious outbreaks of infection. The role of properly disinfected equipment that becomes colonized during use was assessed. In the Vancou-ver General Hospital gram-negative bacilli in the nebulizer water were demonstrated in 10.5% of nebulizers being used for periods of 24 to 72 hours. In at least 15% of patients exposed to contaminate nebulizers the organism was recovered from the respiratory tract 48 hours after removal of the equipment. Only one out of 85 patients exposed to contaminated nebulizers developed pneumonia, and in this instance a clear history of aspiration of vomitus was present. The low incidence of pneu-monia may be related to the high percentage of nebulizers contaminated by organisms of low vir-ulence and might be much greater in hospitals where more highly pathogenic organisms are com-monly found as nebulizer contaminants.
The present study revealed that there was sig-nificant difference in nurses' performance about reassessing vital signs (p-value=0.035) and the majority of nurses in Nursing Bachelor Were at satisfactory level (68.7%). in this regard, Quino, [41] reported that vital signs are necessary reassess-ing patients status; breath sounds, respiratory status, pulse rate and other significant respiratory functions needed. Compare and record significant changes and improvement. Refer if necessary after inhala-tion therapy. Gamal, [42] found that highest mean scores of knowledge and performance among younger nurses' those who have least experience and who have Bachelor of Science in nursing.
The current study revealed a great highof per-formance as regards toattach mechanical ventilator to endotracheal tube or tracheostomy tube (p-value =0.10).
British Thoracic Society, [43] found that nebu-lizers should not be connected directly to a cuffed endotracheal or tracheostomy tube. This could result in a pneumothorax, which occurs when there is no expiratory route for exhaled gases When nebulizing with endotracheal or tracheostomy tubes check compatibility with the nebulizer machine.
In thepresent there was significant difference in nurses' performance about flow rate of 02 de-termined by the patient's condition (p-value=0.021) this result agreed with Nationallnstitute for Health & Clinical Excellence, [44] who reported that driv-ing gas, either an air compressor or piped/cylinder oxygen at 6-8Lt/min flow rate for most efficient nebulization. And the patients with chronic obstruc-tive pulmonary disease (COPD) should not rou-tinely use oxygen driven nebulizers due to the risk of carbon dioxide retention.
The current study showed that there was signif-icant differences nurses' knowledge regarding to education (p-value=0.07) and experiences (p-value =0.32). The findings of the present study are in accordance with Abolwafa, [45] who found that the majority of score of nurses' knowledge who have bachelor of Science in nursing had significant higher score than those who have technical institute and nursing diploma, scores of nurses' who have work experience ranged from 5 to 10 years were higher than those who have work experience less than 5 years.
Conclusion:
Nurses' knowledge and performance about neb-ulizer therapy were unsatisfactory with slightly higher level of knowledge and this could explain that the nurses acquired experience during their nebulizer therapy.
Recommendations:
The nursingstaff in critical careunits are respon-sible for giving care to the patients connected to nebulizer machine should be trained enough to give effective and safe care to such patients.
References 1- HOWARD L.: Current trends in the management of
critically Ill patients: Drug delivery via nebulization, mediscape, available at http://www.medscape.org/ viewar-ticle/413053_4, 2011.
2- PRISCILL, TASHKIN D. and ZIEVE D.: The science of nebulized drug delivery available from http://kidshealth. org/parent/asthma_center/words_ know/nebulizer.html, 2011.
3- GEORGOPOULOS D., MAULOUDI E. and KONDILI 0.: Bronchodilator delivery with metered-dose inhaler
Fares A.A. Khodish, et al. 93
during mechanical ventilation. Journal of Respiratory Critical Care, 4 (4): 227-234, 2002.
4- GUERIN C., et al.: Inhaled bronchodilator administration during mechanical ventilation: Journal of Aerosol. Med-icine Pulmonary Drug, pp. 85-95, 2008.
5- ALTMAN G.B., KERESTZES P. and WCISEL M.: Fun-damental & advanced. Nursing skills, administration nebulizer medications. Skills 5-7, Austrlia. Brasil. Japan, Delmarcengage, p. 584-85, 2010.
6- MAN L.S. and GRACE: What are the advantages and disadvantages of each aerosol delivery device? Is there any benefit of one over another? Journal of Chest, 127: 335-371, 2008.
7- PINNOCK C. and JONES R: Fundamentals of anaesthesia, anaesthesiaequipments, (4th edition), London, Gmm., p. 904-05, 2011.
8- BRAND C.: Nebulizer therapy complications available at https: //www.healthtap.com/#topics/nebulizer_therapy -complications, 2012.
9- DIGGORY P., BAILEY R. and VALLONE A.: Efective-ness of inhaled bronchodilator delivery systems for pa-tients; Journal of Chest, 26: 412-586, Aging, 2007.
10-KELLY C. and LYNES D.: Nebulizer therapy, best practice in the provision of nebulizer therapy. Journal of Nursing Standard. Apr., p. 25 (31): 50-56, 2011.
11- BOE J., DDNNIS J.H., DRISCOLL B.R., BAUER T.T. and HESLOP K.: European respiratory society guidelines on the use of nebulizers. European Respiratory Journal, 28 (3): 278-263, 2011.
12- DAY T., FARNELL S., HAYNES S., WIANWRINGHT S. and WILSON-BARNETTS: Tracheal suctioning: An exploration of nurses knowledge and competence in acute and high dependency ward areas. S. Adv. Nurs., 39 (1): 35-45, 2002.
13- SACHDEVA, 2010.
14- LAYMAN M.E. and PROEHL J.A.: Nebulizer therapy, procedures steps, (4th edition ), p. 171-72, 2009.
15- HOYLE G.M.: How should you instruct a patient to breathe for a nebulizer treatment? available from http:// www.ehow. Com/ way_5678698_should-patient-breathe-nebulizer-treatment_.html, 2012.
16- WOODROW P.: Intensive care nursing, a framework for practice, airway management, (3rd edition), London & New York. Routledge, p. 55, 2011.
17- SMELTZER S. and BARE B.: Textbook of medical-surgical nursing, gas exchange and respiratory function, Philadelphia. New York. London. Lippincott, p. 730-31, 2008.
18- MARQUIS L.B. and HAUSTON J.C.: Leader ship role & practice foundations founctions in nursing, (6th ed), Lippincott, Hong Kong, p. 371, 2009.
19- HANANIA, et al.: Medical personnel's knowledge of and ability to use inhaling devices. Metered-dose inhalers, spacing chambers, and breath-actuated dry powder inhalers Journal of Chest, 105 (1): 111-6, 2009.
20- EVENS J.R. and DONNELLY G.W.: Amodel to describe the relationship between knowledge, skill, and judgment
in nursing practice, Journal Nursing Forum, 1744-6198, 2006.
21- DANIEL R., GRENDELL R.N. and WILKINS F.R.: Nursing fundamentals, caring & clinical decision making, medication administration, (2nd edition), Australia. Brasil. Japan. Spain, Delmercengage, p. 903-04, 2010.
22- GIULIANO and LIU L.M.: Knowledge of Pulse oxime-tryamong critical care nurses; Journal of Dimensions Critical Care Nursing, Jan.-Feb., 25 (1): 44-9, 2006.
23- Canadian Committee on Antibiotic Resistance: Infection prevention and control best practices for Long Term Care, home and community care including health care offices and ambulatory clinics. Available at on line at: http:// www.cpsa.ab.ca/college programs/attachments_ipac/IPAC-Best_Practices_general.pdf, 2007.
24- LABRAGUE L.J., DOLORES L. and LEDRORO J.: Operating room nurses' knowledge and practice of sterile technique. Journal of Nurse Care, 1: 113.Doi.:10. 4172/ 2167-1168.1000113, 2012.
25- DAUTZENBERG B. and CARONE M.: European respi-ratory society guidelines on the use of nebulizers, Journal of Anaesth., 109: 655P-668P, 2012.
26- Encyclopedia of Nursing: Pulmonary function test, avail-able from http://www.enotes.com/pulmonary-function-test--172341.3, 2006.
27- HOYLE G.M.: How should you instruct a patient to breathe for a nebulizer treatment? available from http:// www.ehow.Com/way_5678698_should-patient-breathe-nebulizer-treatment_.html, 2012.
28- KULAS M.: Side effects of nebulizer use available from http : //www. live strong. com/article/23178-side effects-nebulizer-use, 2011.
29- ETHAN P.: Nebulization Procedure, available at http:// www.reference.com/motif/health/nebulzer, 2012.
30- LAYMAN M.E. and PROEHL J.A.: Nebulizer therapy, procedures steps, (4th edition), p. 171-72, 2009.
31- PLAZA V., GINER J. and GOMEZ J.: Knowledge and skills regarding the use of the turbuhaler inhaler, Journal of Archivos De Bronconeumologia, 33 (3): 113-117, 2009.
32- LEWIS S., HEITKEMPER M.M., DIRKSEN S.R. and BUCHER L.: Medical surgical nursing, obstructive pul-monary diseases, (7th edition), Mosby El Sliver, p. 643-44, 2009.
33- WHYTE J.: The relationship between knowledge and clinical performance in Novice and experienced critical care nurses,available at http://www.medscape.com /viewar-ticle/714090, 2009.
34- HASSAN H.E. and ABOULAZM S.F.: Infection control education. The New Egyptian Journal of Medicine, 36 (1): pp. 67-73, 2007.
35- COOMBS M.: Making sense of arterial blood gases, Journal of Nursing Times, 97 (27): 36-38, 2001.
36- CREED F. and SPIERS C.: Care of the acutely ill adult -an essential guide for nurses, humhdifition; (6th edition), Oxford University Press, p: 459, 2011.
37- COBEN B., SAIMAN L. and CIMIOTTI J.: Factors associated with hand hygienepractices in two neonatal intensive care units. Pediatric Infection Control, 2008.

94 Knowledge & Performance of Critical Care Nurses
38-PRATT RJ., PELLOWE C.M. and WILSON J.A.: National evidence-based NHS hospital in England. Journal of Hospital Infection 65.wwwe epicivu-Acuk, 2007.
39- LAM B.C., LEE J. and LAU Y.L.: Hand hygiene practices in neonatal intensive care unit: A multimodal intervention and impact on nasocomial infection. Departement of pediatric and adolescent medicine, queen Mary Hospital, Hong kong, china, lamccb @ha. org.hk.114 (5): pp. 565-571. 2; 6, 2007.
40- AHMED N.F.: Assessment of nurses' knowledge and performance about universal precautions during cesarean section, master degree, Faculty of Nursing, Assiut Uni-versity, 2010.
41- ROBERT: Infant nebulizer treatment, available at http:// www.livestrong.c om/article/269008_infant-nebulizer-treatments, 2011.
42- QUINO F.: Nebulization therapy, available at http://
nursingcrib.com/demo-checklist/nebulization-therapy, 2011.
43- GAMAL L.M.: Establishing standards for prevention of Nosocomial infection in the recovery rooms and surgical ward at El meniauniversity hospital. Doctorate thesis, Faculty of Nursing, Assiut University, 2006.
44- British Thoracic Society: British guideline on the man-agement of asthma. Available at www.brit-thoracic.org.uk , 2008.
45- National Institute for Clinical Excellence: Management of chronic obstructive pulmonary disease in adults and primary and secondary care. NICE. July, Clinical Guide-line, 101, 2010.
46- ABOLWAFA N.F.: In assessment of nurse's knowledge and performances units at El-Menia City Hospitals. Master degree, Faculty of Nursing, Assiut of Hospital, 2009.


![Demo: Uncovering Device Whispers in Smart Homes · 2018. 11. 19. · fortable indoor temperature level [5]. Such highly connected environments exhibit two major challenges, which,](https://static.fdocuments.us/doc/165x107/5fe9f0e712216e691d58b6d2/demo-uncovering-device-whispers-in-smart-homes-2018-11-19-fortable-indoor.jpg)















