Nutritional status and its effect on treatment outcome among HIV ...
Upload
saskatchewan-health-care-quality-summitCategory
view
1.609download
0description

Know Your Status Project: HIV Case Management as a Model of Improvement of Quality of Care Leslie Ann Smith and Jocelyn Andrews
This Session is sponsored by:

Presenters:
Jocelyn Andrews, Regional Director of Primary Health Care and Population Health
Leslie-Ann Smith, Nurse in Charge
First Nations and Inuit Health Branch - Saskatchewan (FNIHB-SK)
April 2013
Know Your Status Project: HIV Case Management
as Model of Improvement of Quality of Care


Introduction
• HIV/AIDS remains an issue of concern for Canada.
• In Canada, the number of new infections in 2011 was estimated
at 3,175 (PHAC).
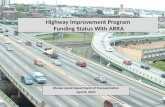
• Saskatchewan has the highest incidence of HIV in Canada, with
the highest burden among First Nations/Métis people
(Figures 1 & 2).

2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
SK 2.5 3.9 5.4 7.6 10.2 12.6 16.7 19.3 16.2 17.2
Canada 7.9 7.8 7.9 7.7 7.8 7.5 7.9 7.2 6.8 6.4
0
5
10
15
20
25
Cru
de
ra
te p
er
10
0,0
00
Year of diagnosis
Figure 1: Rate of HIV cases by year, Saskatchewan and Canada, 2002 to 2011 (sources: SK Ministry of Health, PHAC)

0
30
60
90
120
150
180
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Nu
mb
er
of
ca
se
s
Year of diagnosis
Figure 2: HIV Cases by self-reported ethnicity, Saskatchewan, 2002 to 2011 (source: SK Ministry of Health)
Aboriginal Non-Aboriginal/Unspecified

Background and Context First Nations and Inuit Health Quality Improvement Framework
• Articulate First Nations and Inuit Health Branch’s commitment to
improving continuously the quality of First Nations and Inuit
(FNI) health services
• Provide common vision, language and understanding of Quality
Improvement for First Nations and Inuit Health Services
• Prepare a foundation for quality improvement action planning
BUILD PEOPLE CAPABILITIES
BUILD SYSTEM CAPACITY

Background and Context
• High rates of Chlamydia and Gonorrhea
• Increase Hepatitis C
• Sporadic cases of HIV
• IDU population identified and growing
• Initial testing in for the Know Your Status (KYS) project began in
January 2011.
• Mobile Infectious Diseases clinic with physician services held
quarterly since July 2011.

This is a first of its kind client focused,
mobile, community-based, multi-disciplinary
HIV /STI project delivered in First Nations
community.

Objectives
Key objectives are:
1. Decrease the number of new cases of HIV and STIs in
community;
2. Decrease stigma and increase understanding of HIV and
STIs; and
3. Develop community and professional capacity to manage
HIV and STIs.

Method
Approach for case management: Client Focused Care
Culturally competent care is provided by a multi-disciplinary
team with ID specialist, pharmacist, mental health worker and
community health nurses in the health clinic or directly in
patients’ homes.
• Client focused culturally sensitive care is being provided one-to-
one care by community health nurses, including assisting in the
delivery of ARV and other supportive care.

Health Indicators
Maximum Time to Care:
• Maximum time to care, from testing to treatment, is three
months. The time varies depending on the blood work. In many
cases the time to care is less than three months.
Access to appropriate care:
• Clinics are provided by Infectious Diseases Doctor quarterly, on
regular basis.
Cultural Safety:
• Case management occurs within the community. The specific
needs of each client are respected (e.g. meeting times and
locations).

Approach
• Access to testing to clients and contacts by CHNs
working in rural First Nation settings
• If positive for Chlamydia and Gonorrhea, expand
testing to all those with risky behavior for:
• Hepatitis
• Syphilis
• HIV
• Pregnancy testing for high risk

Approach
• Referrals to PA Sexual Health - relationship building
for team (nurse to nurse), better understanding of
program.
• Referrals to family physicians/NPs limited.
• Numerous home visits to same client (challenging).
• We needed one nurse to run CDC program.
• Requisition in hand-MHO needed to be on board.

• Approach was not working.
• Most clients would not go to PA-Positive living
program.
• Transportation issue to lab-even with requisition in
hand.
• Poor access to care.

• We needed to develop a community based, but also
culturally responsive program that would meet the
needs of our high risk clients.
• We needed to start testing in the community-Veni-
puncture, POCT, urinalysis.
New Ideas

Action Plan
• We advocated for change to our community health program.
• Involved Nursing Office-RNO, ZNO and NIC and met with the
Chief.
• HPPH-MHO/CDC coordinator was briefed on what we would
like to do to improve service delivery.
• ARNO-was involved in the collaboration with SDCL.
• Lab licensing - Quality Assurance testing for Tests: POCT,
Pregnancy.
• Forms for project

Action Plan
• Community Meetings with Chief and Council and
Health Director.
• Community Information Sessions - Nursing and HIV
Coordinator.

Training
• Pre and post-test counseling
• Veni-puncture training
• SDCL tour
• PA positive living program - Marlene Allen
• PA South Hill Lab

Testing and Referrals
• Testing open to everyone
• High school testing
• Treat positive Chlamydia / Gonorrhea clients
• Refer all clients with Hep C and HIV to PA Positive
Living Program
• Dr. Lanoie for methadone program

Concerns with Testing and Referrals
• Clients would not go to PA for most referrals-stigma
• Many wanting treatment but unable to do follow-up
that was needed
• Poor access to physicians and NPs
• We have an obligation to ensure clients are followed
up
• No relationship

Solutions for Testing and Referral Concerns
• Clients already had relationship with nurses and
trusted them
• Needed to develop relationships with doctors and
other health care professionals
• Very sensitive issue
• ID doctor willing to come into community for client
assessment-VIP-relationship building

Client Case Management
• Appointments
• AV Treatment
• Methadone
• Medication delivery/follow up
• Frequent testing-case management
• Social networking ongoing

Program Concerns
• POCT testing-immediate result
• CD4 & CD8 & VL
• Strict guidelines for quality specimens
• Follow-up blood work and appointments (numerous)
• Workload
• Paper overload
• Confidentiality-protecting client, community concerns

Lessons Learned and Limitations
There are three crucial elements for success of a community-
centered multi-disciplinary care model:
1. Community readiness, ownership and mobilization to ensure the
development of culturally appropriate strategies to deal with HIV
related issues and harm reduction;
2. Continuous alignment of resources, internal and external to meet
the needs of HIV clients; and
3. Creation of effective, on-going partnerships.

Conclusion and Recommendations
• Applied Quality Improvement principles & outcomes: STEEP
(Safe; Timely; Equitable; Effective and Efficient; Patient-Centered)
• The first year evaluation of the project has been finalized in
2012 and recommendations approved and endorsed by the First
Nations community
• Use of available and existing resources and tools
• Continued partnership-building
• Continuum in care and social support to clients
• Evidence-based approach















References
• Public Health Agency of Canada (2012) Estimates of HIV prevalence
and incidence in Canada
• Saskatchewan Ministry of Health (2012): HIV/AIDS Annual Report
Saskatchewan
• Saskatchewan Ministry of Health (2010): The Saskatchewan HIV
Strategy 2010-14
• Health Canada/FNIHB Project Evaluation (2012): Know Your Status. A
Comprehensive Review of HIV testing, Case Management and
Treatment in a Saskatchewan First Nation.
• Reif F, Golon SE, Smith SR (2005): Barriers to accessing HIV/AIDS
care in North Carolina: Rural and urban differences. AIDS Care, 17(5),
558-565.

Acknowledgements
To…
• Chief Morin and all key stakeholders from Big River First Nations for
their engagement in this project
• Community Health Nurses and clients involved in this project
• The Ministry of Health and Regional Health Authorities involved
• All the multidisciplinary team for their dedicated contribution and
participation in this project
…THANK YOU!