Know Factson Fiber - Kellogg's Nutrition Healthcare ... · by Burkitt, Trowell, and others helps...
19
the Facts of Fiber KNOW
Transcript of Know Factson Fiber - Kellogg's Nutrition Healthcare ... · by Burkitt, Trowell, and others helps...
the Facts of FiberKNOW
05
14
27
Table of Contents
Forward
Properties ofDifferent Fibers
Fiber and Metabolic Syndrome
History
Benefits of Fiber
Fiber and Cancer
Defining Fiber
Fiber and Digestive Health
Fiber and the Immune System
Fiber Sources
Prebiotic Effects
Recommended Amounts
Types of Grains
Fiber and Weight Management
Fiber and GI Disorders
Filling the Fiber Gap
Properties of Fiber
Fiber and Diabetes
Fiber and Cardiovascular Health
References
01
08
23
02
10
24
06
20
16
28
04
12
25
07
21
18
30
It’s been linked to better health for literally thousands of years, but only in recent times have people begun to understand why we need it – and how much we need.
From digestive health to associated reduction of serious health risks like heart attacks, strokes, and certain cancers, scientific studies continue to reveal more reasons everyone should add fiber to their diets. However, a full nine out of ten Americans - both children and adults - still fall below recommended levels, prompting the Dietary Guidelines for Americans to call our inadequate consumption a “significant public health concern.” 1,2
Bridging this gap means educating consumers about what fiber is, where to find it, and which types we need. As a health professional, you can be a key part of meeting this challenge, and this comprehensive resource on fiber can help. From refreshing your knowledge to researching guidelines, sources, and specific quantities, you’ll find answers to “most of” your fiber questions here.
1
Table of Contents
Forward
FIBER
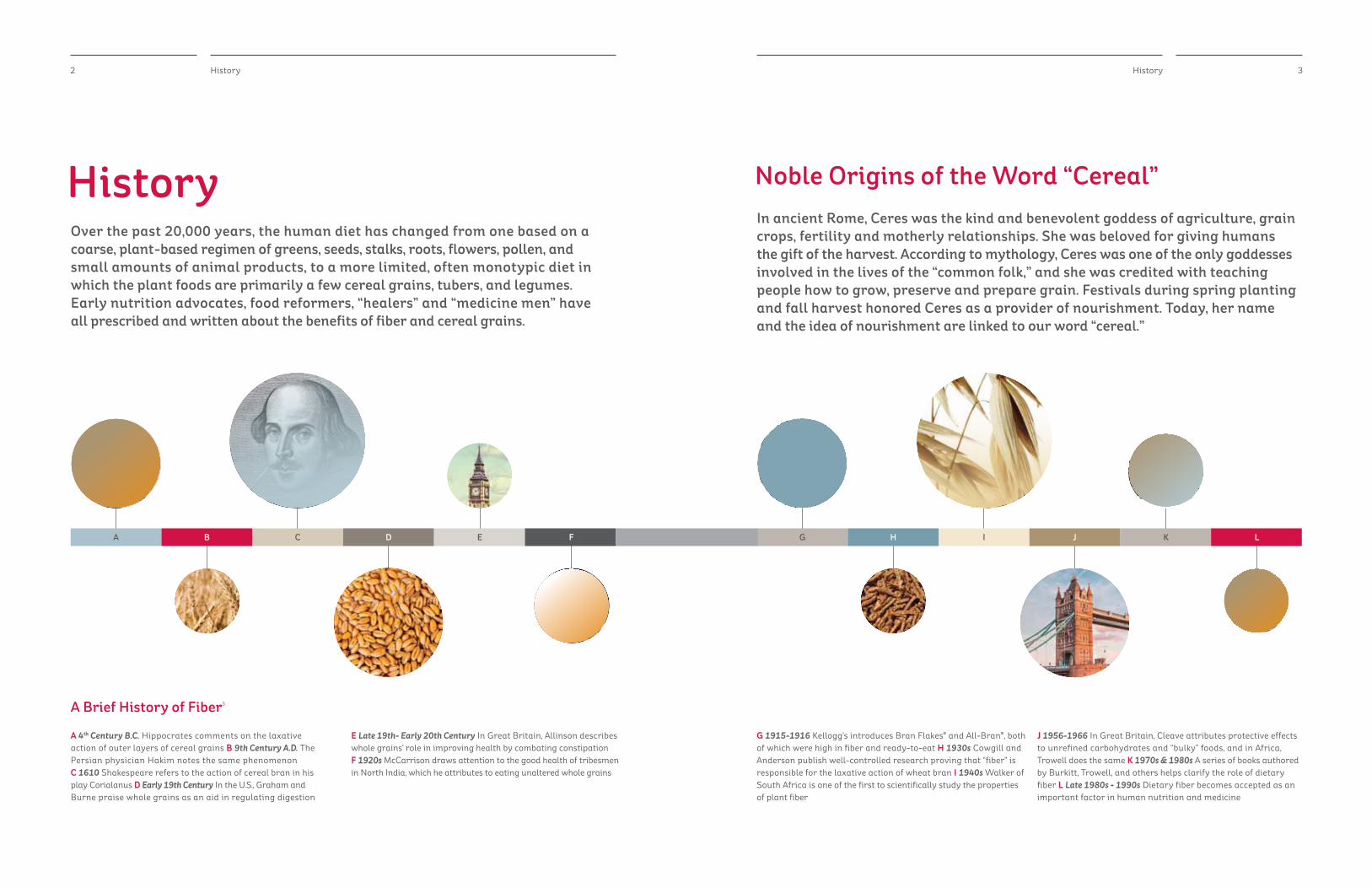
HistoryOver the past 20,000 years, the human diet has changed from one based on a coarse, plant-based regimen of greens, seeds, stalks, roots, flowers, pollen, and small amounts of animal products, to a more limited, often monotypic diet in which the plant foods are primarily a few cereal grains, tubers, and legumes. Early nutrition advocates, food reformers, “healers” and “medicine men” have all prescribed and written about the benefits of fiber and cereal grains.
In ancient Rome, Ceres was the kind and benevolent goddess of agriculture, grain crops, fertility and motherly relationships. She was beloved for giving humans the gift of the harvest. According to mythology, Ceres was one of the only goddesses involved in the lives of the “common folk,” and she was credited with teaching people how to grow, preserve and prepare grain. Festivals during spring planting and fall harvest honored Ceres as a provider of nourishment. Today, her name and the idea of nourishment are linked to our word “cereal.”
A 4th Century B.C. Hippocrates comments on the laxative action of outer layers of cereal grains B 9th Century A.D. The Persian physician Hakim notes the same phenomenon C 1610 Shakespeare refers to the action of cereal bran in his play Corialanus D Early 19th Century In the U.S., Graham and Burne praise whole grains as an aid in regulating digestion
E Late 19th- Early 20th Century In Great Britain, Allinson describes whole grains’ role in improving health by combating constipation F 1920s McCarrison draws attention to the good health of tribesmen in North India, which he attributes to eating unaltered whole grains
G 1915-1916 Kellogg’s introduces Bran Flakes® and All-Bran®, both of which were high in fiber and ready-to-eat H 1930s Cowgill and Anderson publish well-controlled research proving that “fiber” is responsible for the laxative action of wheat bran I 1940s Walker of South Africa is one of the first to scientifically study the properties of plant fiber
J 1956-1966 In Great Britain, Cleave attributes protective effects to unrefined carbohydrates and “bulky” foods, and in Africa, Trowell does the same K 1970s & 1980s A series of books authored by Burkitt, Trowell, and others helps clarify the role of dietary fiber L Late 1980s - 1990s Dietary fiber becomes accepted as an important factor in human nutrition and medicine
Noble Origins of the Word “Cereal”
History
A Brief History of Fiber3
2 3History
A GC IE KB HD JF L
The FDA’s analytical definition is important in terms of food labeling while IOM’s definition references fibers’ role in health and well-being. In this guide, we’ll use “fiber” as the general term for all sources of fiber, both dietary and functional. However, since all fibers have unique characteristics that may confer specific health benefits, we will speak to those individually.
Physiological (IOM)4
Dietary Fiber
Non-digestible carbohydrates and lignins that are intrinsic and intact in plants.
Functional Fiber
Isolated, non-digestible carbohydrates that have beneficial physiological effects in humans.
Total Fiber
Analytical (FDA) (for food labeling purposes)
The measurement of all types of fiber in any food Dietary Fiber
4 Defining Fiber
Defining FiberIn the nutrition science realm, we use two slightly different definitions for fiber: one physiological, and the other analytical. The Institute of Medicine (IOM) and the Food and Drug Administration (FDA) each offer differing definitions to arrive at what is called “total fiber.”
5Fiber Sources
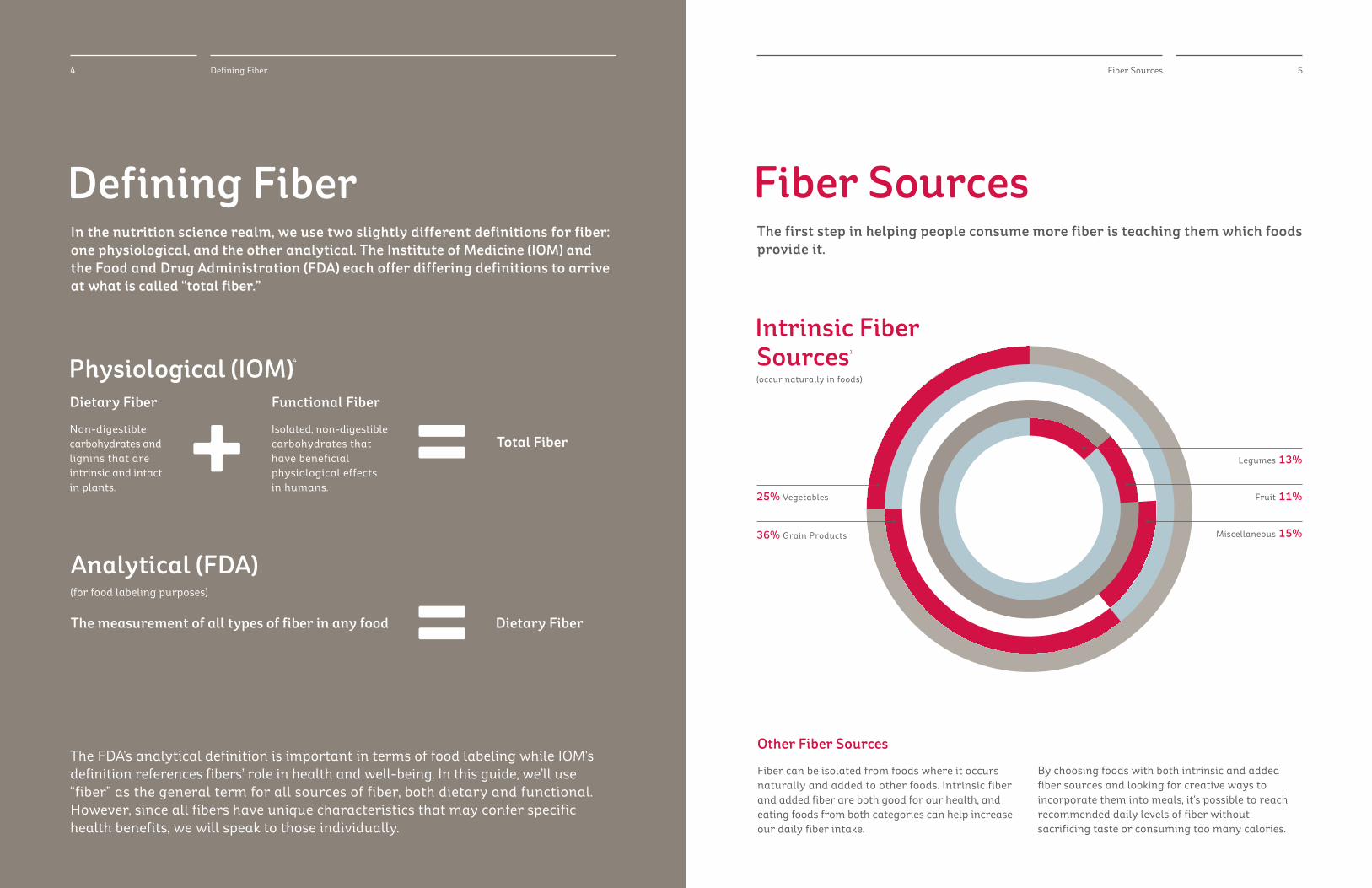
Fiber SourcesThe first step in helping people consume more fiber is teaching them which foods provide it.
Other Fiber Sources
Fiber can be isolated from foods where it occurs naturally and added to other foods. Intrinsic fiber and added fiber are both good for our health, and eating foods from both categories can help increase our daily fiber intake.
By choosing foods with both intrinsic and added fiber sources and looking for creative ways to incorporate them into meals, it’s possible to reach recommended daily levels of fiber without sacrificing taste or consuming too many calories.
Intrinsic Fiber Sources1
(occur naturally in foods)
Fruit 11%
Legumes 13%
25% Vegetables
36% Grain Products Miscellaneous 15%
Rice Wheat Chia Quinoa
7Properties of Fiber
Properties of FiberOne of the ways scientists evaluate fibers is by noting their physical and chemical properties, including solubility, viscosity, fermentability, and water-holding capacity.2
Property Ability Effect on Health
Solubility Ability to dissolve in water.
While it was once thought that solubility could predict physiological function, research has found that this is not the case. Both soluble and insoluble fibers may provide the same type of benefits but to varying degrees.
Viscosity Ability to thicken when mixed with fluids (including intestinal fluids).
Thought to aid certain fibers in modulating blood lipids.
Water-holding Capacity
Ability of the fiber to bind with and hold water in the small and large intestine.
Helps to increase fecal bulk, possibly shortening transit time through the bowels.
Fermentability Ability to be fermented by microflora in the large intestine to produce carbon dioxide, methane, hydrogen and short chain fatty acids (SCFA).
SCFAs serve as the primary energy source for colonic cells to help support a healthy colonic environment.
6 Types of Grains
Types of GrainsGrains are the largest contributor of fiber1 in the American diet. Scientists classify them into two groups: cereal grains and non-cereal grains (sometimes called pseudo-cereal grains). These terms are acknowledged by AACC International (formerly, American Association of Cereal Chemists), the world’s foremost authorities on cereal grains.
Cereal Grains
• Edibleseedsfromplantsinthegrassfamily.
• Containmacronutrients:carbohydrates, including fiber, protein, and fat, as well as vitamins and minerals.
• Containimportantphytonutrientsincluding phenolic compounds, flavonoids, condensed tannins, lignans, and others. These phytonutrients and their human health benefits represent an emerging field of scientific study.
• Examples:wheat,maize,oats,rye,corn,barley, triticale, millet, sorghum, rice.
Pseudo-Cereal Grains
• Ediblefruitsorseedsfromplantsoutsidethe grass family.
• Containmacronutrients:carbohydrates, including fiber, protein, and fat, as well as vitamins and minerals.
• Containimportantphytonutrientsincluding phenolic compounds, flavonoids, condensed tannins, lignans, and others. These phytonutrients and their human health benefits represent an emerging field of scientific study.
• Canbecookedandeatenlikeothergrains.
• Examples:quinoa,amaranth,chia,buckwheat.
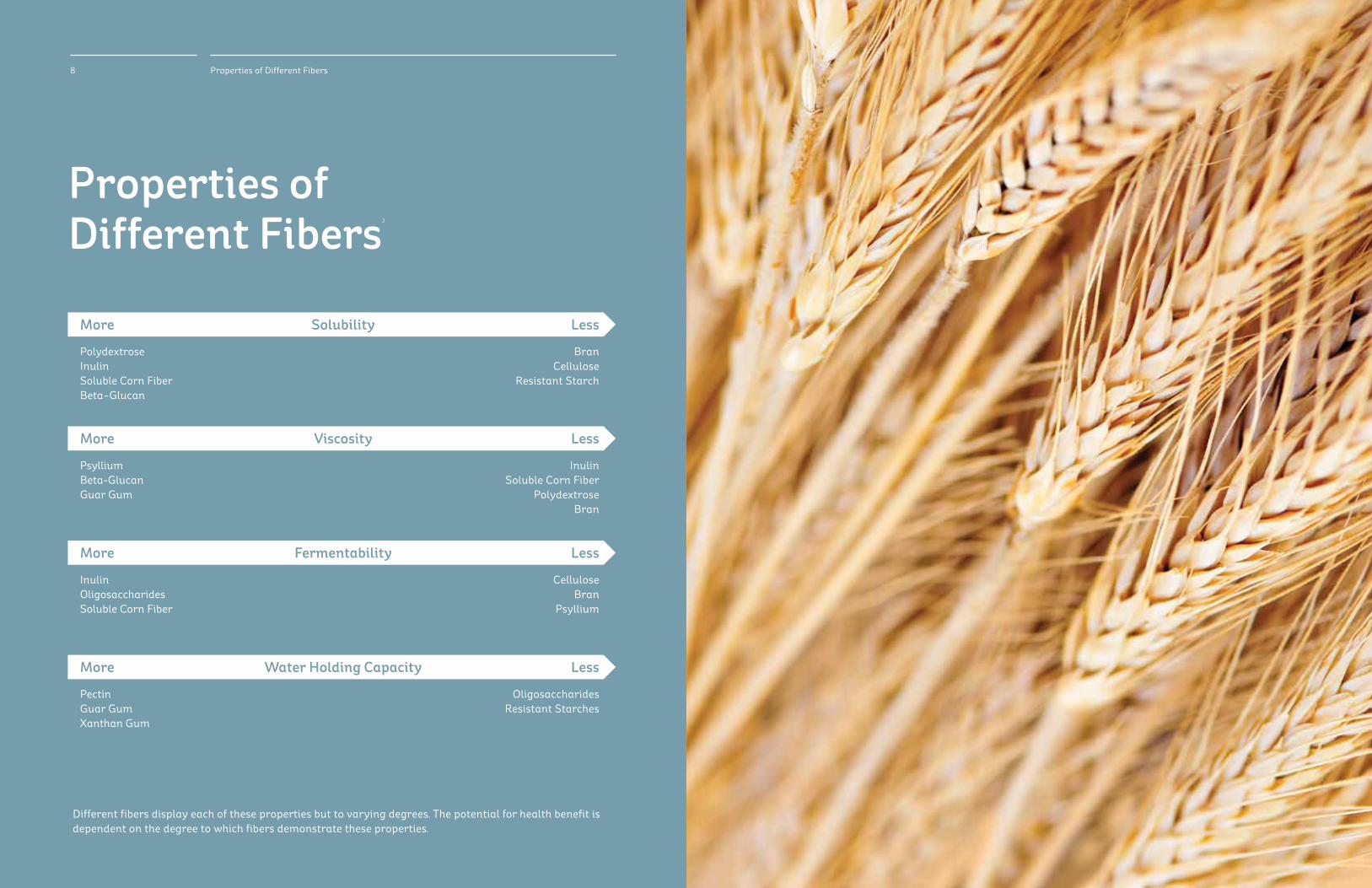
More
PolydextroseInulinSoluble Corn FiberBeta-Glucan
More
Psyllium Beta-GlucanGuar Gum
More
InulinOligosaccharidesSoluble Corn Fiber
More
PectinGuar GumXanthan Gum
Solubility
Viscosity
Fermentability
Water Holding Capacity
8 Properties of Different Fibers
Properties of Different Fibers2
Different fibers display each of these properties but to varying degrees. The potential for health benefit is dependent on the degree to which fibers demonstrate these properties.
Less
BranCellulose
Resistant Starch
Less
InulinSoluble Corn Fiber
PolydextroseBran
Less
CelluloseBran
Psyllium
Less
OligosaccharidesResistant Starches
Benefits of FiberFiber is a unique nutrient. Unlike other nutrients that our bodies need, fiber is not digested and absorbed. This uniqueness confers the health benefits that are associated with fiber. Eating enough fiber has been linked to a positive impact on many important health issues. The following pages feature some of the latest findings on fiber’s relationship to topics including:
•DigestiveHealth•WeightManagement•CardiovascularHealth•Diabetes•MetabolicSyndrome•Cancer•TheImmuneSystem
These findings are from both interventional and observational trials. While observational trials typically study the associations of fiber benefits from all fiber sources, interventional fiber trials may look at singular, isolated fibers in order to study the health benefits.
10 Benefits of Fiber
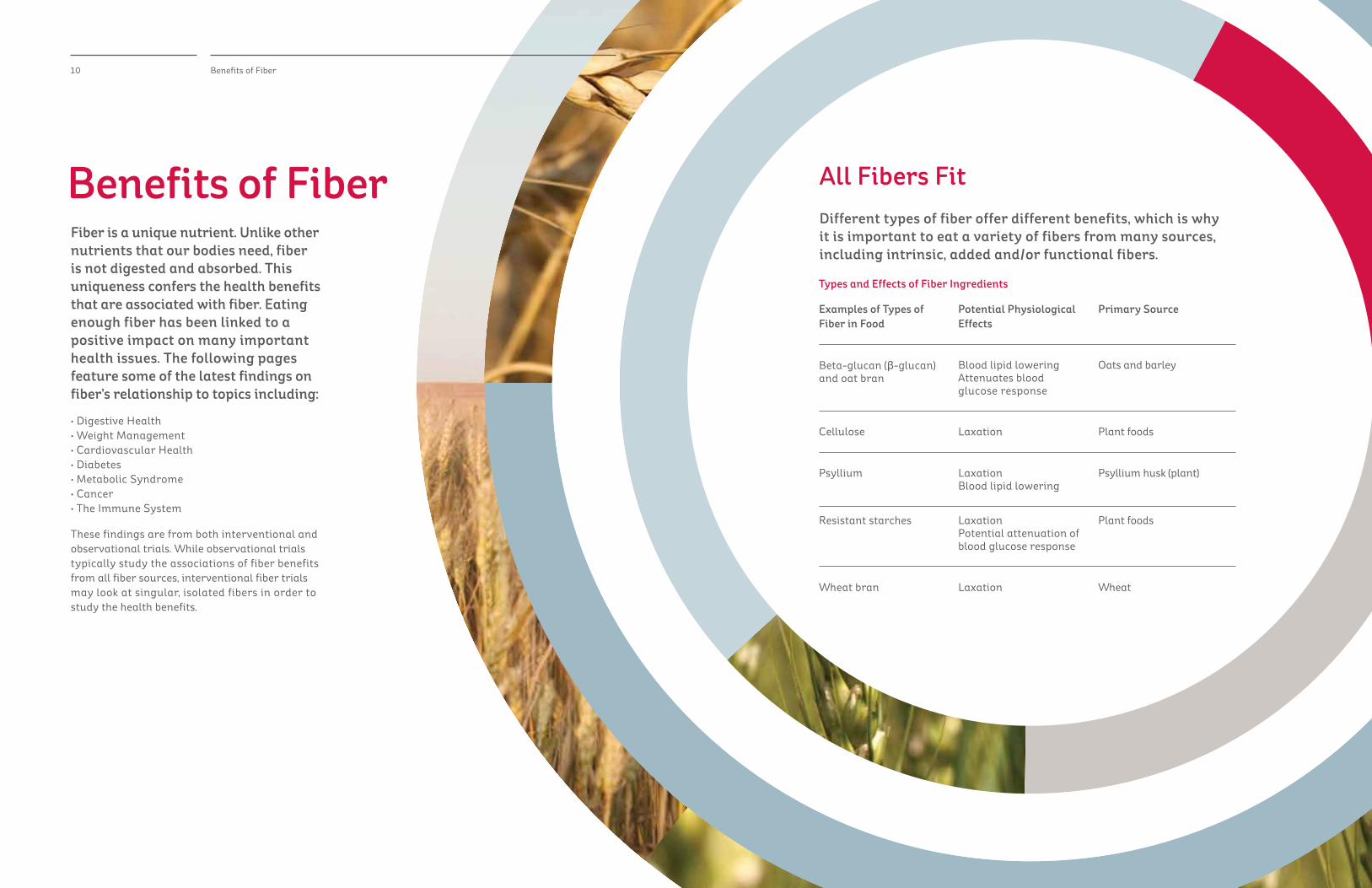
All Fibers FitDifferent types of fiber offer different benefits, which is why it is important to eat a variety of fibers from many sources, including intrinsic, added and/or functional fibers.
Types and Effects of Fiber Ingredients
Examples of Types of Fiber in Food
Potential Physiological Effects
Primary Source
Beta-glucan (β-glucan) and oat bran
Cellulose
Psyllium
Resistant starches
Wheat bran
Blood lipid lowering Attenuates blood glucose response
Laxation
Laxation Blood lipid lowering
Laxation Potential attenuation of blood glucose response
Laxation
Oats and barley
Plant foods
Psyllium husk (plant)
Plant foods
Wheat
13Digestive System12 Fiber and Digestive Health
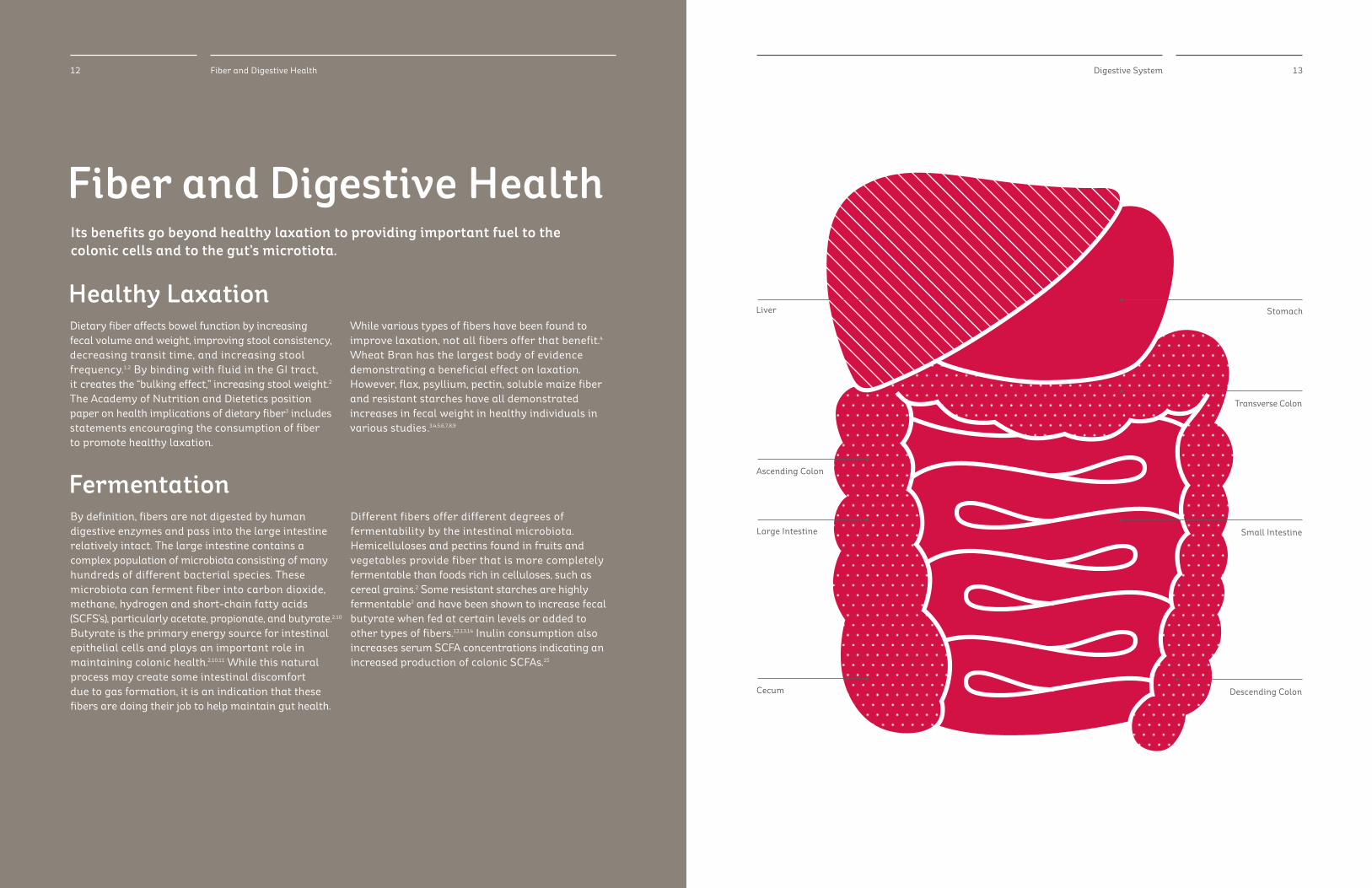
Fiber and Digestive HealthIts benefits go beyond healthy laxation to providing important fuel to the colonic cells and to the gut’s microtiota.
Healthy Laxation
Fermentation
Dietary fiber affects bowel function by increasing fecal volume and weight, improving stool consistency, decreasing transit time, and increasing stool frequency.1,2 By binding with fluid in the GI tract, it creates the “bulking effect,” increasing stool weight.2 The Academy of Nutrition and Dietetics position paper on health implications of dietary fiber3 includes statements encouraging the consumption of fiber to promote healthy laxation.
While various types of fibers have been found to improve laxation, not all fibers offer that benefit.4 Wheat Bran has the largest body of evidence demonstrating a beneficial effect on laxation. However,flax,psyllium,pectin,solublemaizefiberand resistant starches have all demonstrated increases in fecal weight in healthy individuals in various studies.3,4,5,6,7,8,9
By definition, fibers are not digested by human digestiveenzymesandpassintothelargeintestinerelatively intact. The large intestine contains a complex population of microbiota consisting of many hundreds of different bacterial species. These microbiota can ferment fiber into carbon dioxide, methane, hydrogen and short-chain fatty acids (SCFS’s), particularly acetate, propionate, and butyrate.
Butyrate is the primary energy source for intestinal epithelial cells and plays an important role in maintaining colonic health.2,10,11 While this natural process may create some intestinal discomfort due to gas formation, it is an indication that these fibers are doing their job to help maintain gut health.
Different fibers offer different degrees of fermentability by the intestinal microbiota. Hemicelluloses and pectins found in fruits and vegetables provide fiber that is more completely fermentable than foods rich in celluloses, such as cereal grains.2 Some resistant starches are highly fermentable2 and have been shown to increase fecal butyrate when fed at certain levels or added to other types of fibers.12,13,14 Inulin consumption also increases serum SCFA concentrations indicating an increased production of colonic SCFAs.15
Stomach
Small Intestine
Descending Colon
Transverse Colon
Large Intestine
Ascending Colon
Cecum
Liver
2,10
14 Prebiotic Effects 15Prebiotic Effects
Prebiotic EffectsSome fibers are classified as prebiotics, which some scientists have proposed can provide health benefits. While most prebiotics are fiber, not all fibers are prebiotics.
Prebiotics: Are selectively fermented ingredients that result in specific changes in the composition and/or activity of the gastrointestinal microbiota, thus conferring benefit(s) upon host health.1
Understanding PrebioticsCharacteristics
•ResistanttodigestionandabsorptionintheGItract.
•Fermentablebyinterstinalmicrobiota.
•Abletoselectivelystimulatethegrowthand/or activity of intestinal bacteria (namely bifidobacteria andlactobacilli)potentiallyassociatedwithhealth/ well being.2
Types
Confirmed
•Inulin,whichnaturallyoccursinvaryingamounts in foods such as leeks, asparagus, chicory, Jerusalem artichokes, garlic, onions, wheats, oats and soybeans3,4,5 may be extracted to add to foods as a “functional” fiber.2
•Short-chainfructooligosachharides(FOS),soybean oligosaccharides, and galactooligosaccharides (GOS).6,7,8,9 These are also naturally-occurring in foods or extracted to add to foods.2
Potential
•Solublecornfiber.9,10
•Polydextrose.9,10
Proposed Health Benefits2
(based on evidence, consensus, and emerging science)
•Reducedprevalenceanddurationofinfectiousand antibiotic-associated diarrhea.
•Reducedsymptomsassociatedwithinflammatory bowel disease.
•Enhancedbioavailabilityofminerals,including calcium, magnesium and possibly iron.
•Reducedriskfactorsforcardiovasculardisease.
•Promotionofsatietyandweightmanagement.
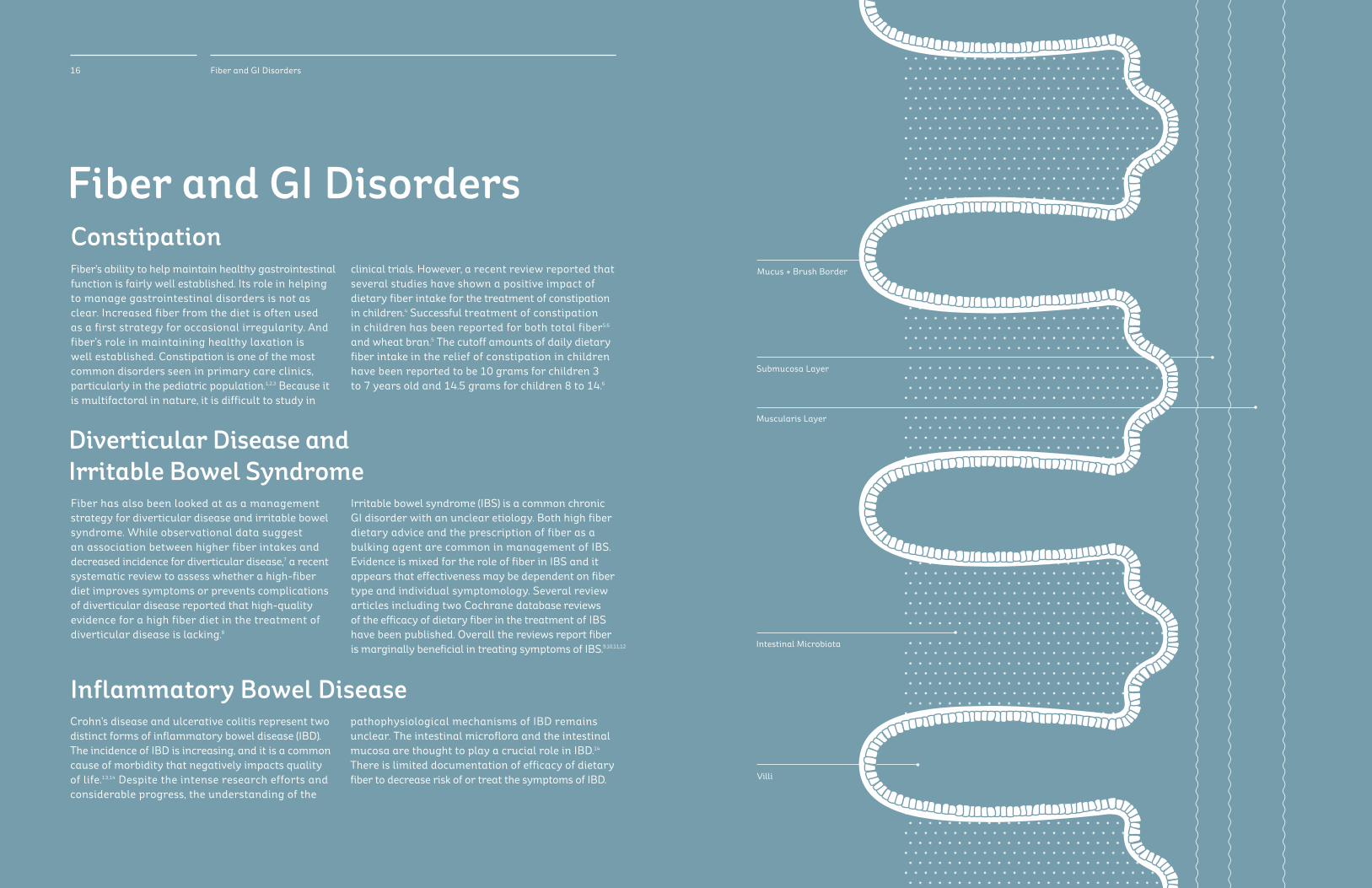
Diverticular Disease and Irritable Bowel SyndromeFiber has also been looked at as a management strategy for diverticular disease and irritable bowel syndrome. While observational data suggest an association between higher fiber intakes and decreased incidence for diverticular disease,7 a recent systematic review to assess whether a high-fiber diet improves symptoms or prevents complications of diverticular disease reported that high-quality evidence for a high fiber diet in the treatment of diverticular disease is lacking.8
Irritable bowel syndrome (IBS) is a common chronic GI disorder with an unclear etiology. Both high fiber dietary advice and the prescription of fiber as a bulking agent are common in management of IBS. Evidence is mixed for the role of fiber in IBS and it appears that effectiveness may be dependent on fiber type and individual symptomology. Several review articles including two Cochrane database reviews of the efficacy of dietary fiber in the treatment of IBS have been published. Overall the reviews report fiber is marginally beneficial in treating symptoms of IBS.
16 Fiber and GI Disorders
Fiber and GI Disorders
Inflammatory Bowel Disease
ConstipationFiber’s ability to help maintain healthy gastrointestinal function is fairly well established. Its role in helping to manage gastrointestinal disorders is not as clear. Increased fiber from the diet is often used as a first strategy for occasional irregularity. And fiber’s role in maintaining healthy laxation is well established. Constipation is one of the most common disorders seen in primary care clinics, particularly in the pediatric population.1,2,3 Because it is multifactoral in nature, it is difficult to study in
clinical trials. However, a recent review reported that several studies have shown a positive impact of dietary fiber intake for the treatment of constipation in children.4 Successful treatment of constipation in children has been reported for both total fiber5,6 and wheat bran.5 The cutoff amounts of daily dietary fiber intake in the relief of constipation in children have been reported to be 10 grams for children 3 to 7 years old and 14.5 grams for children 8 to 14.6
Crohn’s disease and ulcerative colitis represent two distinct forms of inflammatory bowel disease (IBD). The incidence of IBD is increasing, and it is a common cause of morbidity that negatively impacts quality of life.13,14 Despite the intense research efforts and considerable progress, the understanding of the
pathophysiological mechanisms of IBD remains unclear. The intestinal microflora and the intestinal mucosa are thought to play a crucial role in IBD.14 There is limited documentation of efficacy of dietary fiber to decrease risk of or treat the symptoms of IBD. Villi
Mucus + Brush Border
Intestinal Microbiota
Submucosa Layer
Muscularis Layer
9,10,11,12
19Heart Diagram
Aorta
Pulmonary Artery
Pulmonary Vein
Mitral Valve
Left Ventricle
Cardiac Muscle
Superior Vena Cava
Pulmonary Veins
Right Atrium
Inferior Vena Cava
Tricuspid Valve
Right Ventricle
18 Fiber and Cardiovascular Health
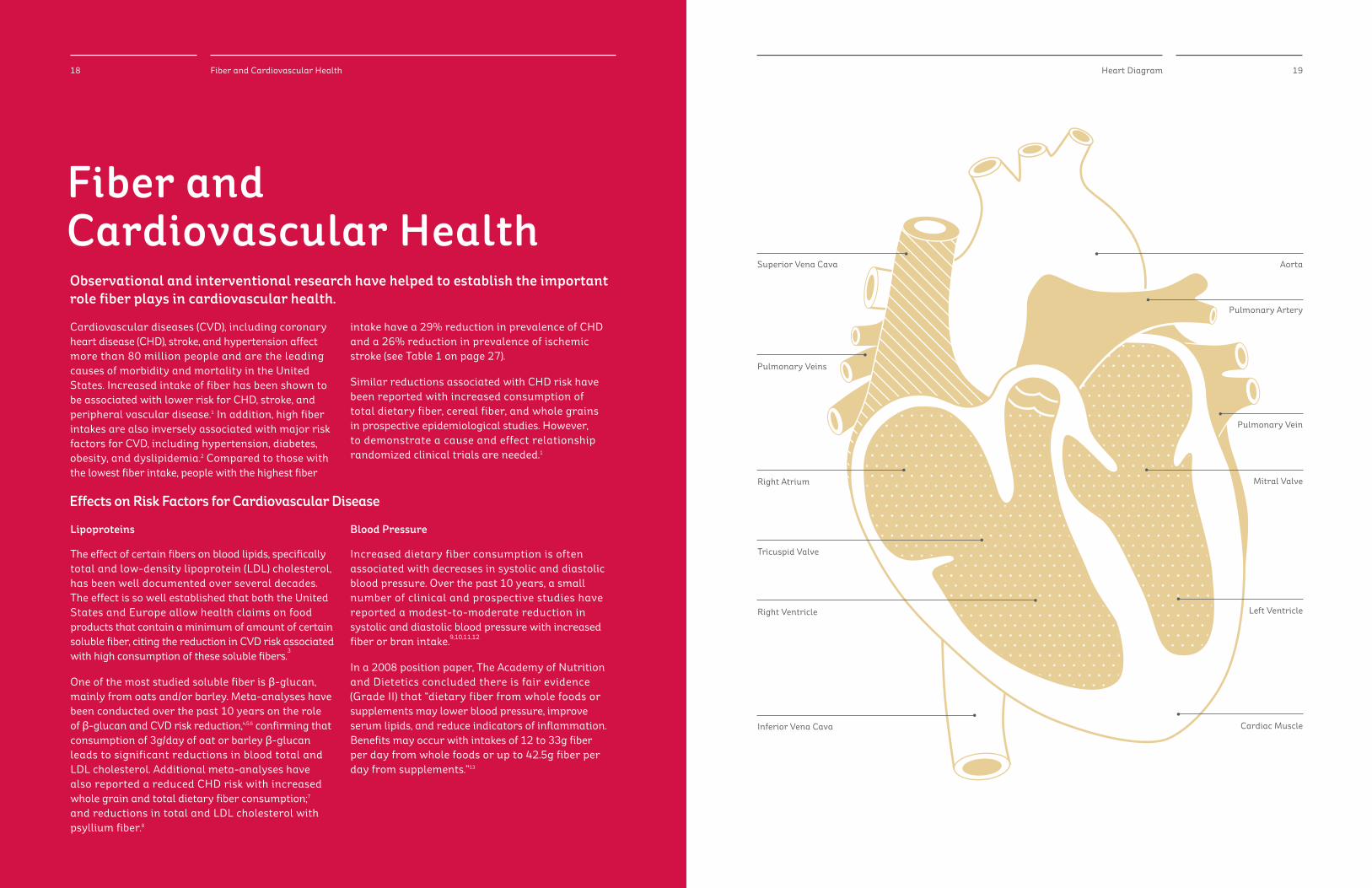
Fiber and Cardiovascular Health
Cardiovascular diseases (CVD), including coronary heart disease (CHD), stroke, and hypertension affect more than 80 million people and are the leading causes of morbidity and mortality in the United States. Increased intake of fiber has been shown to be associated with lower risk for CHD, stroke, and peripheral vascular disease.1 In addition, high fiber intakes are also inversely associated with major risk factors for CVD, including hypertension, diabetes, obesity, and dyslipidemia.2 Compared to those with the lowest fiber intake, people with the highest fiber
intake have a 29% reduction in prevalence of CHD and a 26% reduction in prevalence of ischemic stroke (see Table 1 on page 27). Similar reductions associated with CHD risk have been reported with increased consumption of total dietary fiber, cereal fiber, and whole grains in prospective epidemiological studies. However, to demonstrate a cause and effect relationship randomizedclinicaltrialsareneeded.1
Blood Pressure
Increased dietary fiber consumption is often associated with decreases in systolic and diastolic blood pressure. Over the past 10 years, a small number of clinical and prospective studies have reported a modest-to-moderate reduction in systolic and diastolic blood pressure with increased fiber or bran intake.9,10,11,12
In a 2008 position paper, The Academy of Nutrition and Dietetics concluded there is fair evidence (Grade II) that “dietary fiber from whole foods or supplements may lower blood pressure, improve serum lipids, and reduce indicators of inflammation. Benefits may occur with intakes of 12 to 33g fiber per day from whole foods or up to 42.5g fiber per day from supplements.”13
Lipoproteins
The effect of certain fibers on blood lipids, specifically total and low-density lipoprotein (LDL) cholesterol, has been well documented over several decades. The effect is so well established that both the United States and Europe allow health claims on food products that contain a minimum of amount of certain soluble fiber, citing the reduction in CVD risk associated with high consumption of these soluble fibers.
3
One of the most studied soluble fiber is β-glucan, mainlyfromoatsand/orbarley.Meta-analyseshavebeen conducted over the past 10 years on the role of β-glucan and CVD risk reduction,4,5,6 confirming that consumptionof3g/dayofoatorbarleyβ-glucan leads to significant reductions in blood total and LDL cholesterol. Additional meta-analyses have also reported a reduced CHD risk with increased whole grain and total dietary fiber consumption;7 and reductions in total and LDL cholesterol with psyllium fiber.8
Effects on Risk Factors for Cardiovascular Disease
Observational and interventional research have helped to establish the important role fiber plays in cardiovascular health.

20 Fiber and Weight Management
Fiber and Weight Management
Diets high in fiber, particularly whole grain and cereal fibers, have been associated with lower body weights in both cross-sectional and prospective cohort studies.3 Consequently, people who consume high fiber diets are also less likely to be obese compared to those who consume low fiber diets.4 According to the Academy of Nutrition and Dietetics’ fiber position paper, high-fiber diets help people manage their weight due to the bulking effect of fiber which emerging science indicates may be more satiating.5 Increasing dietary fiber consumption may decrease energy absorption by diluting a diet’s energy availability while maintaining other
important nutrients.3 Several large cohort studies and reviews have been published in the past 10 years examining the role of fiber in body weight management; however, there is a lack of human interventional studies specifically testing the role of fiber in weight management.5-12
Clinical research is needed to determine the specific role of fiber in body weight management, including definingtypeoffiber/combinationsoffibersandoptimal daily intakes. Future clinical research should also examine the role of dietary fiber on weight loss.
Approximately 66% of US adults are overweight or obese, resulting in an increased risk for serious chronic health conditions including diabetes, cardiovascular disease, and certain types of cancer.1,2 Due to the tremendous health burden of these chronic illnesses, researchers are studying ways to help people manage their weight, and thereby help them lower their risk for obesity and chronic illness.
21Fiber and Diabetes
Fiber and Diabetes
With the increasing prevalence of obesity and type 2 diabetes mellitus (T2DM), public health officials and scientists are actively researching dietary factors that may help the public manage their blood glucose and insulin levels. It is thought that healthy dietary and lifestyle practices may help keep blood glucose and insulin levels within normal ranges and decrease risk for developing obesity and type 2 diabetes.
Dietary fiber is one of the key nutrients shown to help manage blood glucose and insulin responses and ultimately decrease risk for T2DM.1 The recommended dietary fiber intake from the American Diabetes Association matches the recommendation from the Institute of Medicine’s DRI Report for US adults,2 primarily based upon reducing risk of heart disease. The IOM also states that there is evidence that total fiber intake reduces the risk of diabetes.2
Of the different fibers investigated for glucose control, β-glucan from oats and barley are among the most researched. The majority of studies suggest a beneficial role for β-glucan in helping to maintain or lower glucose responses.3-22 While the majority of studies have focused on β-glucan, other fibers have been shown to also help manage blood glucose including rye, guar gum, psyllium, and certain modified fibers.23-51 Future studies are needed to determine the optimal dose and timing of these different fibers on their ability to modulate the glucose response.
Investigation into fiber to help manage glucose response is leading health authorities to make recommendations for increased fiber in the diet.
Fiber and Metabolic Syndrome
Individuals with MetS have a two-fold increase in risk for heart attack or stroke and a five-fold increased risk for developing diabetes compared to individuals who do not have metabolic syndrome. MetS is considered a “wake-up call” for people because it can be controlled by maintaining a healthy weight, eating a healthy diet, and getting adequate physical activity which will help reduce a person’s risk for developing CVD and diabetes.1 As part of a healthy diet, both the AHA and American Diabetes Association recommend consuming a diet high in whole grains, fruits and vegetables, lean meats and fish, and low-fat or fat-free dairy products.3
Studies have suggested that dietary fiber intake is inversely associated with MetS. While most research has focused on the effects of dietary fiber in CVD and diabetes risk, a smaller number of studies have highlighted the inverse association between dietary fiber and MetS. These later findings are particularly significant given that changes in diet and lifestyle can help ameliorate risk factors for MetS, and consequently lower risk for CVD and diabetes. More research,includingrandomized,controlledtrials, is warranted to determine the role that fiber plays in the etiology of MetS and consequently CVD and diabetesinbothchildren/adolescentsandadults.4-25
Metabolic Syndrome (MetS) is a cluster of inter-related risk factors that together increase a person’s risk for cardiovascular disease (CVD) and diabetes. According to the American Heart Association (AHA), approximately 34% of adult Americans have clinically defined MetS.1 MetS is defined as the presence of at least three of the following cardio-metabolic risk factors: abdominal obesity, elevated triglycerides, low HDL cholesterol, elevated blood pressure, and impaired fasting glucose.2
22 Fiber and Metabolic Syndrome 23Fiber and Metabolic Syndrome
25Fiber and the Immune System
Fiber and the Immune SystemImmune health is complicated but more information is being uncovered about fiber’s impact on immune markers.
The GI tract is the largest immune organ for humans. The gut-associated lymphoid tissue (GALT) contains about 60% of all lymphocytes in the body. Dietary constituents, including dietary fiber andprebiotics, impact the function of the GI immune system.1 Prebiotic fibers may impact the GI immune system indirectly as a result of fermentation and the growth of certain intestinal microbiota.2 An inverse association between dietary fiber and C-reactive protein (CRP), a marker of inflammation, has been reported in cohort and cross-sectional human studies. A small number of clinical trials have reported lower CRP concentrations with a wide range of fiber intakes. Whole grain and cereal fiber intakes have also been associated with lower concentrations of pro- inflammatory biomarkers. The impact of dietary fibers on measures of inflammation and clinical disease outcomes are an area for future research.
Survey data and observational and prospective data have all reported inverse associations between either total fiber intake or cereal grain fiber intake and inflammatory markers such as CRP, interleukin-6 (IL-6) and tumor necrosis factor-alpha receptor-2. (TNF-alpha-R2).3-14 Emerging science provides conflicting data on reduction of inflammatory markers associated with intake of certain fibers.15
Evidence for the role of prebiotic fibers in infant nutrition is overall insufficient to draw conclusions.16-21 Research with healthy university students supplemented with GOS has shown reduced GI symptoms and duration of cold or flu symptoms.22
24 Fiber and Cancer
Fiber and CancerRisk factors, prevention and treatments for various cancers are multi-factorial. Fiber’s role is but one tool that can help support a dietary approach.
Research has suggested that dietary fiber may decrease the prevalence of several gastrointestinal disorders that may include colorectal cancer.1 These studies have proposed that fiber favorably interacts with the gastrointestinal tract through a variety of mechanisms, thereby decreasing the prevalence of these disorders. While fiber has known mechanisms that exert a positive effect on gastrointestinal health, it is most likely just one component of many that together help lower risk for disease.
With this holisitic approach, the American Cancer Society recommends that people get enough fiber in their diet by filling their plate two-thirds full with plant foods such as fruits, vegetables, whole grains, legumes and nuts. In addition to fiber, the fruits, vegetables, and grains also contain a wealth of micronutrients and phytochemicals that may play an important role in health.2
Research, primarily from prospective studies, has suggested an inverse association between dietary fiber intake and cancer risk, particularly colorectal cancer and other gastrointestinal cancers. More studies are needed to further determine the specific role of fiber in cancer etiology, as well as the role that fiber plays as part of a complex, multi-factorial diet in cancer risk.3-18
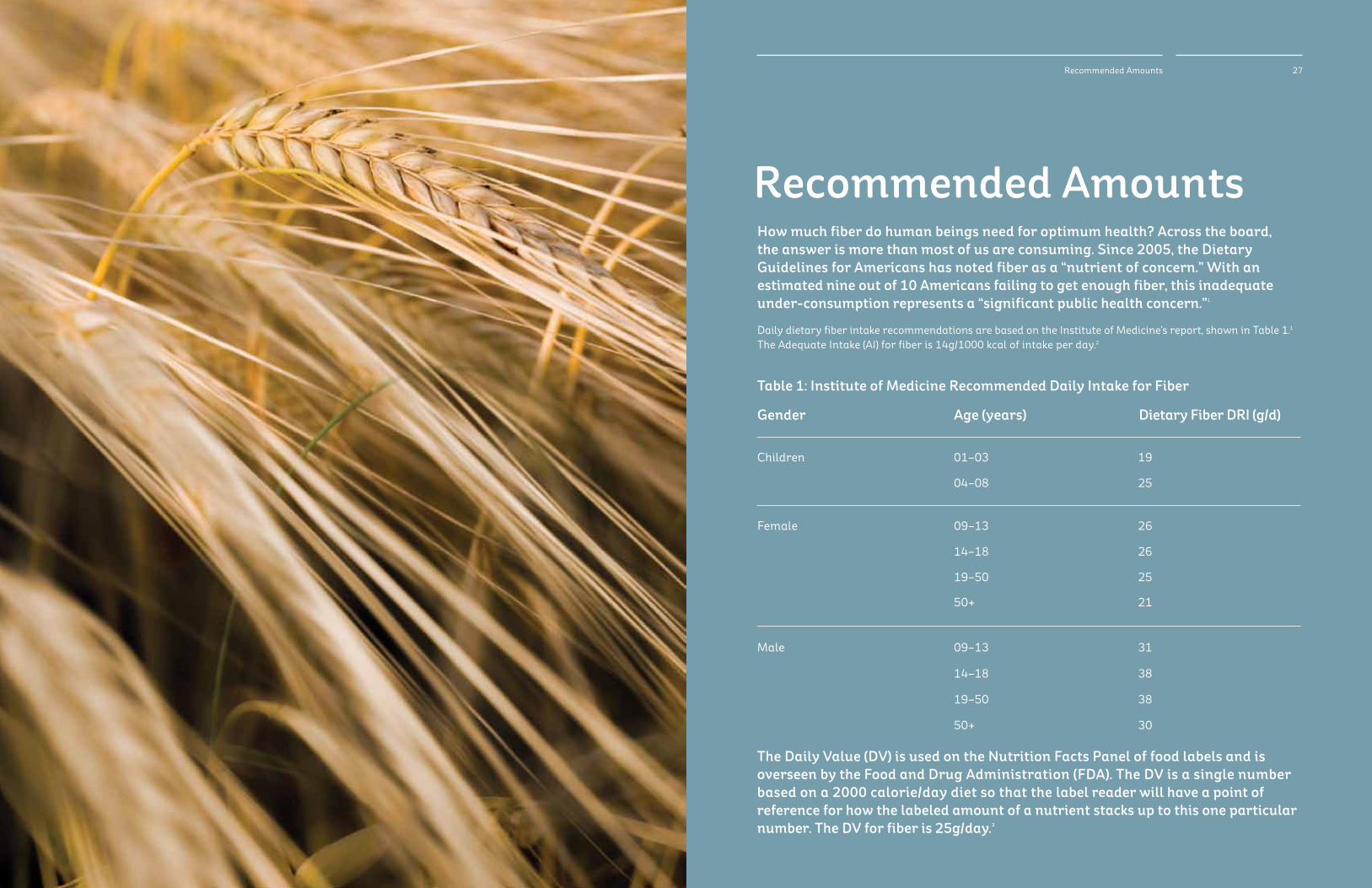
Recommended AmountsHow much fiber do human beings need for optimum health? Across the board, the answer is more than most of us are consuming. Since 2005, the Dietary Guidelines for Americans has noted fiber as a “nutrient of concern.” With an estimated nine out of 10 Americans failing to get enough fiber, this inadequate under-consumption represents a “significant public health concern.”1
Daily dietary fiber intake recommendations are based on the Institute of Medicine’s report, shown in Table 1.1 TheAdequateIntake(AI)forfiberis14g/1000kcalofintakeperday.2
Gender
Children
Age (years)
01–03
09–13
09–13
19–50
19–50
04–08
14–18
14–18
50+
50+
Dietary Fiber DRI (g/d)
19
26
31
25
38
25
26
38
21
30
Table 1: Institute of Medicine Recommended Daily Intake for Fiber
Female
Male
The Daily Value (DV) is used on the Nutrition Facts Panel of food labels and is overseen by the Food and Drug Administration (FDA). The DV is a single number based on a 2000 calorie/day diet so that the label reader will have a point of reference for how the labeled amount of a nutrient stacks up to this one particular number. The DV for fiber is 25g/day.3
27Recommended Amounts

29Filling the Fiber Gap28 Filling the Fiber Gap
Filling the Fiber Gap Simple Steps to Eating More FiberAs a health professional, you can help more people enjoy the benefits of eating enough fiber. The educational tools and recipes on our website will support you in discussing these issues. With the help of nutrition professionals, consuming enough dietary fiber can become much more common throughout the population.
Find sample meal plans, client-friendly handouts and presentations, recent studies on fiber, and more, all at kelloggnutrition.com.
•Thereisalackofconsumerunderstandingabout dietary fiber and why it is important in the diet. One study reported consumers consider fiber an important health “gauge” when making food selections.1
- Still nearly 70% of consumers in International Food Information Council Foundation’s 2013 Food and Health Survey indicate fiber and whole grains are strong considerations for making purchase decisions.2 - Emphasis on whole grains could be confounding consumer’s perceptions of fiber intake as noted in a 2009 consumer survey indicating that 85% of consumers expected whole grain foods to provide a good or excellent source of fiber, which is not always the case.3
• Intakeoffiber-richfruits,vegetablesandwhole grains remain below recommended levels, despite dietary recommendations and nutrition education campaigns.
•MostfoodsintypicalAmericandietsdeliveronlyone to three grams of fiber per serving. While they are eaten often enough to supply some fiber, it is not enough to reach recommended levels.
Why is there such a large gap between actual fiber intake and the recommended amount? There are likely many reasons.
Fiber and Cardiovascular Health
1. Anderson JW et al. Health benefits of dietary fiber. Nutrition Reviews. 2009;67:188-205.2. Lairon D et al., Dietary fiber intake and risk factors for cardiovascular diseaseinFrenchadults.AmJClinNutr.2005;82:1185-1194.3. CastroIAetal.Functionalfoodsforcoronaryheartdiseaseriskreduction: a meta-analysis using a multivariate approach. Am J Clin Nutr. 2005;82:32-40.4. Talati R et al., The effects of barley-derived soluble fiber on serum lipids. AnnFamMed2009;7:157-63.5. Tiwari UT and Cummins E. Meta-analysis of the effect of β-glucan intake onbloodcholesterolandglucoselevels.Nutrition.2011;27:1008-1016.6. Kelly SAM et al. Wholegrain cereals for coronary heart disease (review). Cochrane Library. 2009; 3.7. Anderson JW et al. Whole grain foods and heart disease risk. J Am Coll Nutr.2000;19:291S-299S.8. Wei ZH et al. Time- and dose-dependent effect of psyllium on serum lipids inmild-to-moderatehypercholesterolemia:ameta-analysisofcontrolled clinicaltrials.EurJClinNutr.2009;63:821-827.9. Keenan JM et al. Oat ingestion reduces systolic and diastolic blood pressureinpatientswithmildorborderlinehypertension:apilottrial.J FamPract.2002;51:369-375.10. Pins JJ et al. Do whole-grain oat cereals reduce the need for antihypertensive medication and improve blood pressure control? J Fam Pract.2002;51:353-359.11. Davy BM et al. Oat consumption does not affect resting casual and ambulatory 24-h arterial blood pressure in men with high-normal blood pressuretostage1hypertension.JNutr.2002:132:394-398.12.FlintAJ,HuFB,GlynnRJ,JensenMK,FranzM,SampsonL,RimmEB.Whole grainsandincidenthypertensioninmen.AmJClinNutr.2009;90(3):493-8. Epub 2009 Jul 1.13.SlavinJL.PositionoftheAmericanDieteticAssociation:Health implicationsofdietaryfiber.JAmDietAssoc.2008;108:1716-1731.
Fiber and Weight Management
1. Ogden CL et al. Prevalence of overweight and obesity in the United States, 1999-2004.JAMA.2006,295:1549-1555.2. Li Z et al. Health ramifications of the obesity epidemic. Surg Clin North Am. 2005,85:681-701.3. Lattimer JM and Haub MD. Effects of dietary fiber and its components on metabolichealth.Nutrients.2010,2:1266-1289.4. Anderson JW. Dietary fiber and associated phytochemicals in prevention andreversalofdiabetes.In:Pasupuleti,VK,AndersonJW,eds. Nutraceuticals,GlycemicHealthandType2Diabetes.Ames,Iowa: BlackwellPublishingProfessional;2008:111-142.5. SlavinJL.PositionoftheAmericanDieteticAssociation:Health implicationsofdietaryfiber.JAmDietAssoc.2008;108:1716-1731.6. Anderson JW et al. Health benefits of dietary fiber. Nutrition Reviews. 2009, 67:188-205.7. Du H, et al.. Dietary fiber and subsequent changes in body weight and waist circumference in European men and women. Am J Clin Nutr. 2010;91:329-336.8. Tucker LA, Thomas KS. Increasing total fiber intake reduces risk of weight andfatgainsinwomen.JNutr2009;139:576-581.9. Davis JN et al. Inverse relation between dietary fiber intake and visceral adiposityinoverweightLatinoyouth.AmJClinNutr.2009b;90:1160-1166.10. Harland JI and Garton LE. Whole-grain intake as a marker of healthy body weight and adiposity. Whole-grain intake as a marker of healthy body weightandadiposity.PublicHealthNutrition2008;11(6):554-63.11. Williams PG, Grafenauer SJ, O’Shea JE. Cereal grains, legumes, and weight management:acomprehensivereviewofthescientificevidence.NutrRev. 2008;66(4):171-82.12. Koh-Banerjee P et al. Changes in whole-grain, bran, and cereal fiber consumption in relation to 8-y weight gain among men. Am J Clin Nutr. 2004,80:1237-1245.
Fiber and Diabetes
1. American Diabetes Association, Bantle JP, Wylie-Rosett J, Albright AL, Apovian CM, Clark NG, et al. Nutrition recommendations and interventions fordiabetes:apositionstatementoftheAmericanDiabetesAssociation. DiabetesCare.2008Jan;31Suppl1:S61-78.2. InstituteofMedicine,FoodandNutritionBoard.DietaryReferenceIntakes: Energy, Carbohydrates, Fiber, Fat, Fatty Acids, Cholesterol, Protein and AminoAcids.Washington,DC:NationalAcademiesPress;2005.3. Juntunen KS, Niskanen LK, Kiukkonen KH, Poutanen KS, Holst JJ, Mykkänen HM. Postprandial glucose, insulin, and incretin responses to grain products inhealthysubjects.AmJClinNutr2002;75:254-262.
4. Behall KM, Scholfield DJ, Hallfrisch J. Comparison of hormone and glucose responses of overweight women to barley and oats. J Am Coll Nutr 2005;24:182-188.5. Biörklund M, van Rees A, Mensink RP, Önning G. Changes in serum lipids and postprandial glucose and insulin concentrations after consumption of beverages with β-glucansfromoatsorbarley:arandomizeddose- controlledtrial.EurJClinNutr2005;59:1272-1281.6. Weickert MO, Mohlig M, Koebnick C, Holst JJ, Namsolleck P, Ristow M, OsterhoffM,RochlitzH,RudovichN,SprangerJ,PfeifferAFH.Impactof cereal fibre on glucose-regulating factors. Diabetologia 2005; 48:2343-2353.7. DeAngelisM,RizzelloCG,AlfonsiG,ArnaultP,CappelleS,DiCagnoR, Gobbetti M. Use of sourdough lactobacilli and oat fibre to decrease the glycaemicindexofwhitewheatbread.BrJNutr2007;98:1196-1205.8. HlebowiczJ,WickenbergJ,Fahlström,BjörgellO,AlmérL-O,andDarwich G. Effect of commercial breakfast fiber cereals compared with corn flakes on postprandial blood glucose, gastric emptying and satiety in healthy subjects:arandomizedblindedcrossovertrial.NutrJ.2007;6:22.9. HlebowiczJ,DarwicheG,BjörgellO,AlmérL-O.Effectofmuesliwith4g oat β-glucan on postprandial blood glucose, gastric emptying and satiety inhealthsubjects:arandomizedblindedcrossovertrial.JAmCollNutr 2008;27:470-475.10. Maki KC, Davidson MH, Witchger MS, Dicklin MR, Subbaiah PV. Effects of high-fiber oat and wheat cereals on postprandial glucose and lipid responsesinhealthymen.IntJVitamNutrRes2007a;77:347-356.11. Maki KC, Galant R, Samuel P, Tesser J, Witchger MS, Ribaya-Mercado JD, Blumberg JB, Geohas J. Effects of consuming foods containing oat β-glucan on blood pressure, carbohydrate metabolism and biomarkers of oxidative stress in men and women with elevated blood pressure. Eur J Clin Nutr2007b;61:786-795.12. PanahiS,EzataghaA,TemelliF,VasanthanT,VuksanV.β-glucan from two sources of oat concentrates affect postprandial glycemia in relation to the levelofviscosity.JAmCollNutr2007;26:639-644.13. Tuomasjukka S, Viitanen M, Kallio H. The glycaemic response to rolled oat isnotinfluencedbythefatcontent.BritJNutr2007;97:744-748.14. Mäkeläinen H, Anttila H, Sihvonen J, Hietanen R-M, Tahvonen R, Salemin E, Mikola M, Sontag-Strohm T. The effect of β-glucan on the glycemic and insulinindex.EurJClinNutr2007;61:779-785.15. Alminger M, Eklund-Jonsson C. Whole-grain cereal products based on a high-fibre barley or oat genotype lower post-prandial glucose and insulin responsesinhealthyhumans.EurJNutr2008;47:294-300.16. Granfeldt Y, Nyberg L, Björck I. Muesli with 4 g oat β-glucans lowers glucose and insulin responses after a bread meal in healthy subjects. Eur J ClinNutr2008;62:600-607.17. Nilsson A, Östman E, Preston T, Björck I. Effects of GI vs content of cereal fibre of the evening meal on glucose tolerance at a subsequent standardizedbreakfast.EurJClinNutr2008a;62:712-720.18. Nilsson AC, Östman EM, Granfeldt Y, and Björck IME. Effect of cereal test breakfasts differing in glycemic index and content of indigestible carbohydrates on daylong glucose tolerance in healthy subjects. Am J Clin Nutr.2008b;87:645-654.19. Juvonen KR, Purhonen A-K, Salmenkallio-Marttila M, Lähteenmäki L, LaaksonenKE,HerzigK-H,UusitupaMIJ,PoutanenKS,KarhunenLJ. Viscosity of oat bran-enriched beverages influences gastrointestinal hormonalresponsesinhealthyhumans.JNutr2009;139:461-466.20. Regand A, Tosh SM, Wolever TM, Wood PJ. Physicochemical properties of beta-glucan in differently processed oat foods influence glycemic response. JAgricFoodChem.2009;57:8831-8838.21. Ulmius M, Johannsson A, and Önning G. The influence of dietary fiber source and gender on the postprandial glucose and lipid response in healthysubjects.EurJNutr.2009;48:395-402.22. Granfeldt YE, Björck IM. A bilberry drink with fermented oatmeal decreases postprandial insulin demand in young healthy adults. Nutr J 2011;10:57.23. Keogh GF, Cooper GJS, Mulvey TB, McArdle BH, Coles GD, Monro JA, and PoppinSD.Randomizedcontrolledcrossoverstudyoftheeffectofahighly β-glucan enriched barley on cardiovascular disease risk factors in mildly hypercholesterolemicmen.AmJClinNutr.2003;78:711-8.24. Casiraghi MC, Garsetti M, Testolin G, and Brighenti F. Post-prandial responses to cereal products enriched with barley β-glucan. J Am Coll Nutr.2006;25:313-320.25. Poppitt SD, van Drunen JDE, McGill A-T, Mulvey TB and Leahy FE. Supplementation of a high-carbohydrate breakfast with barley β-glucan improves postprandial glycemic response for meals but not beverages. AsiaPacJClinNutr.2007;16:16-24.26. Kim H, Stote KS, Behall KM, Spears K, Vinyard B, and Conway JM. Glucose and insulin responses to whole grain breakfasts varying in soluble fiber, β-glucan.EurJNutr.2009;48:170-175.27. Thondre PS and Henry CJK. High molecular-weight barley β-glucan in chaptis (unleavened Indian flatbread) lowers glycemic index. Nutr Res. 2009;29:480-486.
Forward, History, and Defining Fiber
1. PositionoftheAmericanDieteticAssociation:Healthimplicationsof dietaryfiber.JAmDietAssoc.2008;108:1716-1731.2. United States Department of Agriculture Center for Nutrition Policy and Promotion.DietaryGuidelinesforAmericans2010.Availableat:http:// www.cnpp.usda.gov/Publications/DietaryGuidelines/2010/PolicyDoc/ PolicyDoc.pdf.3. Spiller, Gene A. CRC Handbook of Dietary Fiber in Human Nutrition, 3rd edition CRC Press, Boca Raton, Fl 2001. 4. Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids. Washington DC:NationalAcademiesPress;2005.
Fiber Sources, Types of Grains, and Properties of Fiber
1. United States Department of Agriculture, Center for Nutrition Policy and Promotion,HomeEcomonicsResearchReportNumber58:Nutrient Content of the US Food Supply, 2005, Washington DC; March 2008.2. Spiller, Gene A. CRC Handbook of Dietary Fiber in Human Nutrition, 3rd edition CRC Press, Boca Raton, Fl 2001.
Fiber and Digestive Health
1. Raninen K, Lappi J, Mykkanen H, Poutanen K. Dietary fiber type reflects physiologicalfunctionality:comparisonofgrainfiber,inulin,and polydextrose.NutritionReviews2011;69:9-21.2. Institute of Medicine, 2005. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients). National Academy Press, Washington, D.C.3. PositionoftheAmericanDieteticAssociation:Healthimplicationsof dietaryfiber.JAmDietAssoc.2008;108:1716-1731.4. Dahl WJ, Lockert EA, Cammer AL, Whiting SJ. Effects of flax fiber on laxation and glycemic response in healthy volunteers. J Med Food 2005;8:508-11.5. Cummings JH. The effect of dietary fiber on fecal weight and composition. In:Spiller,GeneA.CRCHandbookofDietaryFiberinHumanNutrition,3rd edition CRC Press, Boca Raton, Fl 2001.6. Boler BM, Serao MC, Bauer LL, Staeger MA, Boileau TW, Swanson KS, Fahey GC Jr. Digestive physiological outcomes related to polydextrose and solublemaizefibreconsumptionbyhealthyadultmen.BrJNutr 2011;106:1864-71.7. Flood MT, Auerbach MH, Craig SA. A review of the clinical toleration studiesofpolydextroseinfood.FoodChemToxicol2004;432:1531-42.8. Maki KC, Sanders LM, Reeves MS, Kaden VN, Rains TM, Cartwright Y. Beneficial effects of resistant starch on laxation in healthy adults. Int J FoodSciNutr2009;60Suppl4:296-305.9. Jenkins DJ, Kendall CW, Vuksan V, Augustin LS, Li YM, Lee B, Mehling CC, Parker T, Faulkner D, Seyler H, Vidgen E, Fulgoni V. The effect of wheat bran particlesizeonlaxationandcolonicfermentation.JAmCollNutr 1999;18:339-45.10. MacfarlaneGT,MacfarlaneS.Fermentationinthehumanlargeintestine: its physiologic consequences and the potential contribution of prebiotics. J ClinGastroenterol2011;45:S120-7.11. Hamer HM, Jonkers D, Venema K, Vanhoutvin S, Troost FJ, Brummer RJ. Reviewarticle:theroleofbutyrateoncolonicfunction.AlimentPharmacol Ther2008;27:104-19.12. McOrist AL, Miller RB, Bird AR, Keogh JB, Noakes M, Topping DL, Conlon MA. Fecal butyrate levels vary widely among individuals but are usually increasedbyadiethighinresistantstarch.JNutr2011;141:883-9.13. MuirJG,YeowEG,KeoghJ,PizzeyC,BirdAR,SharpeK,O’OeaK,MacraeFA. Combining wheat bran with resistant starch has more beneficial effects on fecalindexesthandoeswheatbranalone.AmJClinNutr2004;79:1020-8.14. Verbeke K, Ferchaud-Roucher V, Preston T, Small AC, Henckaerts L, Krempf M, Wang H, Vonk RJ, Priebe MG. Influence of the type of indigestible carbohydrate on plasma and urine short-chain fatty acid profiles in healthyhumanvolunteers.EurJClinNutr2010;64:678-84.15. Tarini J, Wolever TM. The fermentable fibre inulin increases postprandial serum short-chain fatty acids and reduces free-fatty acids and ghrelin in healthysubjects.ApplPhysiolNutrMetab2012;35:9-16.
Prebiotic Effects
1. Gibson GR, Scott KP, Rastall RA, Tuohy KM, Hotchkiss A, Dubert-Ferrandon A,GareauM,MurphyEF,SaulnierD,LohG,etal.Dietaryprebiotics:current statusandnewdefinition.FoodScienceandTechnologyBulletin: FunctionalFoods.2010;7:1–19.
2. Brownawell AM, Caers W, Gibson GR, Kendall CW, Lewis KD, Ringel Y, SlavinJL.Prebioticsandthehealthbenefitsoffiber:currentregulatory status,futureresearch,andgoals.JNutr2012;142:962-74.3. KleessenB,SchwarzS,BoehmA,FuhrmannH,RichterA,HenleT,Krueger M. Jerusalem artichoke and chicory inulin in bakery products affect faecal microbiotaofhealthyvolunteers.BrJNutr.2007Sep;98(3):540-9.4. Kolida S, Meyer D, Gibson GR. A double-blind placebo-controlled study to establish the bifidogenic dose of inulin in healthy humans. Eur J Clin Nutr 2007;61:1189-95.5. Costabile A, Kolida S, Klinder A, Gietl E, Bäuerlein M, Frohberg C, LandschützeV,GibsonGR.Adouble-blind,placebo-controlled,cross-over study to establish the bifidogenic effect of a very-long-chain inulin extracted from globe artichoke (Cynara scolymus) in healthy human subjects.BrJNutr2010;104:1007-17.6. BouhnikY,RaskineL,SimoneauG,VicautE,NeutC,FlouriéB,BrounsF, Bornet FR. The capacity of nondigestible carbohydrates to stimulate fecal bifidobacteriainhealthyhumans:adouble-blind,randomized,placebo- controlled, parallel-group, dose-response relation study. Am J Clin Nutr 2004;80:1658-64.7. van Loo J, Coussement P, de Leenheer L, Hoebregs H, Smits G. On the presence of inulin and oligofructose as natural ingredients in the western diet.CritRevFoodSciNutr.1995;35:525–52.8. Walton GE, van den Heuvel EG, Kosters MH, Rastall RA, Tuohy KM, Gibson GR. A randomised crossover study investigating the effects of galacto- oligosaccharides on the faecal microbiota in men and women over 50 yearsofage.BrJNutr2012;107:1466-75.9. Boler BM, Serao MC, Bauer LL, Staeger MA, Boileau TW, Swanson KS, Fahey GC Jr. Digestive physiological outcomes related to polydextrose and solublemaizefibreconsumptionbyhealthyadultmen.BrJNutr 2011;106:1864-71.10. Hooda S, Boler BM, Serao MC, Brulc JM, Staeger MA, Boileau TW, Dowd SE, Fahey GC Jr, Swanson KS. 454 pyrosequencing reveals a shift in fecal microbiota of healthy adult men consuming polydextrose or soluble corn fiber.JNutr2012;142:1259-65.
Fiber and GI Disorders
1. Shah ND, Chitkara DK, Locke GR, Meek PD, Talley NJ. Ambulatory care for constipation in the United States, 1993-2004. Am J Gasteroenterol 2008;103:1746-53.2. MugieSM,DiLorenzoC,BenningaMA.Constipationinchildhood.NatRev GastroenterolHepatol2011;8:502-11.3. KranzS,BrauchlaM,SlavinJL,MillerKB.Whatdoweknowaboutdietary fiber intake in children and health? The effects of fiber intake on constipation,obesity,anddiabetesinchildren.AdvNutr.2012Jan;3(1):47-53.4. Maffei HV, Vicentini AP. Prospective evaluation of dietary treatment in childhoodconstipation:highdietaryfiberandwheatbranintakeare associated with constipation amelioration. J Pediatr Gastroenterol Nutr 2011;52:55-9.5. Chao HC, Lai MW, Kong MS, Chen SY, Chen CC, Chiu CH. Cutoff volume of dietaryfibertoameliorateconstipationinchildren.JPediatr2008;153:45-9.6. Sullivan PB, Alder N, Shrestha B, Turton L, Lambert B. Effectiveness of using a behavioural intervention to improve dietary fibre intakes in childrenwithconstipation.JHumNutrDiet2012;25:33-42.7. Crowe FL, Appleby PN, Allen NE, Key TJ. Diet and risk of diverticular disease in Oxford cohort of European Prospective Investigation in Cancer and Nutrition(EPIC):prospectivestudyofBritishvegetarianandnon- vegetarians.BMJ2011;343:d4131.doi:10.1136/bmj.d4131.8. Unlu C, Danieals L, Vrouenraets BC, Boermeester MA. A systematic review of high-fibre dietary therapy in diverticular disease. Int J Colorectal Dis 2012;27:419-27.9. BijkerkCJ,MurisJW,KnottnerusJA,HoesAW,deWitNJ.Systematicreview: the role of different types of fibre in the treatment of irritable bowel syndrome.AlimentPharmacolTher2004;19:245-51.10. Ford AC, Talley NJ, Spiegel BM, Foxx-Orenstein AE, Schiller L, Quigley EM, Moayyedi P. Effect of fibre, antispasmodics, and peppermint oil in the treatmentofirritablebowelsyndrome:systematicreviewandmeta- analysis.BMJ2008;;337:a2313.doi:10.1136/bmj.a2313.11. HeizerWD,SouthernS,McGovernS.Theroleofdietinsymptomsof irritablebowelsyndromeinadults:anarrativereview.JAmDietAssoc 2009;109:1204-7.12. 57. Shen YH, Nahas R. Complementary and alternative medicine for treatmentofirritablebowelsyndrome.CanFamPhysician2009;55:143-8.13. Ioannidis O, Varnalidis I, Paraskevas G, Botsios D. Nutritional modulation oftheinflammatorybowelresponse.Digestion2011;84:89-101.14. 63. Hou JK, Abraham B, El-Serag H. Dietary intake and risk of developing inflammatoryboweldisease:asystematicreviewoftheliterature.AmJ Gastroenterol2011;106:563-73.
References31References
28. Chillo S, Ranawana DV, Pratt M, and Henry JK. Glycemic response and glycemic index of semolina spaghetti enriched with barley β-glucan. Nutrition.2011;27:653-658.29. Jones KL, MacIntosh C, Su Y-C, Wells F, Chapman IM, Tonkin A, and HorowitzM.Guargumreducespostprandialhypotensioninolderpeople. JAmGeriatrSoc.2001;49:162-167.30. SierraM,GarciaJJ,Fernández,DiezMJ,CalleAP,Sahagún,andthe Farmafibra Group. Effects of ispaghula husk and guar gum on postprandial glucose and insulin concentrations in healthy subjects. Eur J ClinNutr.2001;55:235-243.31. Kovacs EMR, Westerterp-Plantenga MS, Saris WHM, Melanson KJ, Goossens I, Geurten P, and Brouns F. The effect of guar gum addition to a semisolid meal on appetite related to blood glucose, in dieting men. Eur J ClinNutr.2002;56:771-778.32. Kovacs EMR, Westerterp-Plantenga MS, Saris WHM, Melanson KJ, Goossens I, Geurten P, and Brouns F. Associations between spontaneous meal initiations and blood glucose dynamics in overweight men in negativeenergybalance.BrJNutr.2002;87:39-45.33. Wolf BW, Wolever TMS, Lai CS, Bolognesi C, Radmard R, Maharry KS, GarlebKA,HertzlerSR,andFirkinsJL.Effectsofabeveragecontainingan enzymaticallyinduced-viscositydietaryfiber,withorwithoutfructose,on the postprandial glycemic response to a high glycemic index food in humans.EurJClinNutr.2003;57:1120-1127.34. Williams JA, Lai C-S, Corwin H, Ma Y, Maki KC, Garleb KA, and Wolf BW. Inclusion of guar gum and alginate into a crispy bar improves postprandialglycemiainhumans.JNutr.2004;134:886-889.35. Adam TCM and Westerterp-Plantenga MS. Glucagon-like peptide-1 release and satiety after a nutrient challenge in normal-weight and obese subjects.BrJNutr.2005;93:845-851.36. Karhunen LJ, Juvonen KR, Flander SM, Liukkonen K-H, Lähteenmäki L, SiloahoM,LaaksonenDE,HerzigK-H,UusitupaMI,andPoutanenKS.A psyllium fiber-enriched meal strongly attenuates postprandial gastrointestinal peptide release in healthy young adults. J Nutr. 2010;140:737-744.37. Frost GS, Brynes AE, Dhillo WS, Bloom SR, and McBurney MI. The effects of fiber enrichment of pasta and fat content on gastric emptying, GLP-1, glucose,andinsulinresponsestoameal.EurJClinNutr.2003;57:293-298.38. Juntunen KS. Laaksonen DE, Autio K et al. Atructural differences between rey and wheat breads but not total fiber content may explain the lower postprandial insulin response to rye bread. Am J Clin Nutr. 2003;78:957-964.39. HlebowiczJ,JönssonJM,LindstedtS,BjörgellO,DarwichG,andAlmérL-O. Effect of commercial rye whole-meal bread on postprandial blood glucose andgastricemptyinginhealthysubjects.NutrJ.2009;8:26.40. RosénLAH,BlancoSilvaLO,AnderssonUK,HolmC,ÖstmanEM,andBjörck IME.Endospermandwholegrainryebreadsarecharacterizedbylow post-prandial insulin response and a beneficial blood glucpse profile. Nutr J.2009;8:42.41. RosénLAH,ÖstmanEM,andBjörckIME.Effectsofcerealbreakfastson postprandial glucose, appetite regulation and voluntary energy intake atasubsequentstandardizedlunch:focusingonryeproducts.NutrJ. 2011;10:7.42. Cani PD, Lecourt E, DeWulk EM, Sohet FM, Pachikian BD, Naslain D, De BakerF,Neyrinck,andDelazenneNM.Gutmicrobiotafermentationof prebiotics increases satietogenic and incretin gut peptide production with consequences for appetite sensation and glucose response after a meal. AmJClinNutr.2009;90:1236-43.43. Tarini J and Wolever TMS. The fermentable fiber inulin increases postprandial serum short-chain fatty acids and reduces free-fatty acids andghrelininhealthysubjects.ApplPhysiolNutrMetab.2010;35:9-16.44. Brand-Miller JC, Atkinson FS, Gahler RJ, Kacinik V, Lyon MR, and Wood S. Effects of PGX, a novel functional fiber, on acute and delayed postprandial glycemia.EurJClinNutr.2010;64:1488-1493.45. Jenkins AL, Kacinik V, Lyon MR, and Wolever TMS. Effect of adding the novel fiber, PGX®, to commonly consumed foods on glycemic response, glycemicindexandGRIP:asimpleandeffectivestrategyforreducing post-prandialbloodglucoselevels-arandomized,controlledtrial.NutrJ. 2010a;9:58.46. Jenkins AL, Kacinik V, Lyon MR, and Wolever TMS. Reduction of postprandial glycemia by the novel viscous polysaccharide PGX, in a dose-dependent manner, independent of food form. J Am Coll Nutr. 2010b;29:92-98.47. Park OJ, Kang NE, Chang MJ, and Kim WK. Resistant starch supplementation influences blood lipid concentrations and glucose control inoverweightsubjects.JNutrSciVitaminol.2004;50:93-9.48. Nilsson AC, Östman EM, Holst JJ, and Björck IME. Including indigestible carbohydrates in the evening meal of healthy subjects improves glucose tolerance, lowers inflammatory markers, and increases satiety after a subsequentstandardizedbreakfast.JNutr.2008c;138:732-739.49. Bodinham CL, Frost GS, and Robertson MD. Acute ingestion of resistant starchreducesfoodintakeinhealthyadults.BrJNutr.2010;103:917-922.
50. Li M, Pio J-H, Tian Y, Li W-D, Li K-J, and Yang X-G. Postprandial glycemic and insulinemic responses to GM-resistant starch-enriched rice and the production of fermentation-related H2 in healthy Chinese adults. Br J Nutr.2010;103:1029-1034.51. Behall KM, Scholfield DJ, Hallfrisch JG, Liljeberg-Elmstahl HG. Consumption of both resistant starch and beta-glucan improves postprandial plasma glucose and insulin in women. Diabetes Care 2996;29:976-81.
Fiber and Metabolic Syndrome
1. AmericanHeartAssociation.http://www.heart.org/HEARTORG/Accessed July 24, 2012.2. GrundySMetal.Definitionofmetabolicsyndrome:reportoftheNational Heart,Lung,andBloodInstitute/AmericanHeartAssociationConference onscientificissuesrelatedtothedefinition.Circulation.2004;109: 433-438.3. AmericanDiabetesAssociation.http://www.diabetes.org/Accessed July 24, 2012.4. Anderson JW et al. Health benefits of dietary fiber. Nutrition Reviews. 2009; 67:188-205.5. Weickert MO et al. Cereal fiber improves whole-body insulin sensitivity in overweightandobesewomen.DiabetesCare.2006;29:775-780.6. McKeown NM et al. Carbohydrate nutrition, insulin resistance and the prevalence of the metabolic syndrome in the Framingham Offspring Cohort.DiabetesCare.2004;27:538-46.7. Ye EQ et al. Greater whole-grain intake is associated with lower risk of type 2diabetes,cardiovasculardisease,andweightgain.JNutr.2012;142: 1304-1313.8. Pal S et al., The effect of a fibre supplement compared to a healthy diet on body composition, lipids, glucose, insuling and other metabolic syndrome risk factors in overweight and obese individuals. Br J Nutr. 2011; 105:90-100.9. Weikert MO et al. Effects of supplemented isoenergetic diets differing in cereal fiber and protein content on insulin sensitivity in overweight humans.AmJClinNutr.2011;94:459-71.10. Johnston KL et al. Resistant starch improves insulin sensitivity in metabolicsyndrome.DiabetMed.2010;27:391-7.11. Ulmius M et al. The influence of dietary fiber source and gender on the postprandial glucose and lipid response in healthy subjects. Eur J Nutr. 2009;48:395-402.12.BoSetal.Dietorexercise:whatismoreeffectiveinpreventingorreducing metabolicalterations?EurJEndocrinol.2008;159:685-91.13. Bo S et al. Effectiveness of a lifestyle intervention on metabolic syndrome. Arandomizedcontrolledtrial.JGenInternMed.2007;22:1695-703.14. Katcher HI et al. The effects of a whole-grain-enriched hypocaloric diet on cardiovascular disease risk factors in men and women with metabolic syndrome.AmJClinNutr.2008;87:79-90.15. Roberts CK et al. Effect of a short-term diet and exercise intervention on inflammatory/anti-inflammatorypropertiesofHDLinoverweight/obese menwithcardiovascularriskfactors.JApplPhysiol.2008;101:1727-32.16. Juntunen KS et al. High-fiber rye bread and insulin secretion and sensitivityinhealthypostmenopausalwomen.AmJClinNutr.2003;77: 385-391.17. Pereira MA et al. Effect of whole grains on insulin sensitivity in overweight hyperinsulinemicadults.AmJClinNutr.2002;75:848-855.18. Pal S and Radavelli-Bagatini. Effects of psyllium on metabolic risk factors. ObesRev.2012doiu:10.1111/j/1467-789X.2012.01020.x.19. Yoo S, Nicklas T, Baranowski T, Zakeri IF, Yang SJ, Srinivasan SR, Berenson GS. Comparison of dietary intakes associated with metabolic syndrome riskfactorsinyoungadults:theBogalusaHeartStudy.AmJClinNutr 2004;80:841-8.20.EsmaillzadehA,KimiagarM,MehrabiY,AzadbakhtL,HuFB,WillettWC. Dietary patterns, insulin resistance, and prevalence of the metabolic syndromeinwomen.AmJClinNutr2007;85:910-8.21. Panagiotakos DB, Pitsavos C, Skoumas Y, Stefanadis C. The association between food patterns and the metabolic syndrome using principal componentsanalysis:TheATTICAStudy.JAmDietAssoc.2007;107:979-87.22.Hosseinpour-NiaziS,MirmiranP,SohrabG,Hosseini-EsfahaniF,AziziF. Inverse association between fruit, legume, and cereal fiber and the risk of metabolicsyndrome:TehranLipidandGlucoseStudy.DiabetesResClin Pract2011;94:276-83.23.DorganJFetal.Adolescentdietandmetabolicsyndromeinyoungwomen: results of the Dietary Intervention Study in Children (DISC) follow-up study.JClinEndocrinolMetab.2011;96:E1999-2008.24. Carlson JJ et al. Dietary fiber and nutrient density are inversely associated with the metabolic syndrome in US adolescents. J Am Diet Assoc. 2011; 111:1688-1695.25.KubenaKS.Metabolicsyndromeinadolescents:issuesandopportunities. JAmDietAssoc.2011;111:1674-1679.
Fiber and Cancer
1. Anderson JW et al. Health benefits of dietary fiber. Nutrition Reviews. 2009;67:188-205.2. American Cancer Association. www.cancer.org.3. Bingham, SA, Day NE, and Luben R. Dietary fibre in food and protection against colorectal cancer in the European Prospective Investigation into CancerandNutrition(EPIC):anobservationalstudy.Lancet.2003;361: 1496-1501.4. MAMetal.Cerealfiberintakemayreduceriskofgastricadenocarcinomas: theEPIC-EURGASTstudy.IntJCancer.2007;121:1618-23.5. DahmCCetal.,Dietaryfiberandcolorectalcancerrisk:anested case-control study using food diaries. J Natl Cancer Inst. 2010; 102:614-626.6. Peters U et al. Dietary fiber and colorectal adenoma in a colorectal cancer earlydetectionprogramme.Lancet.2003;361:1491-5.7. WorldCancerResearchFund/AmericanInstituteforCancerResearch. 2007.Food,nutrition,physicalactivityandthepreventionofcancer: aglobalperspective.Washington,DC:AmericanInstitutefor Cancer Research. 8. AuneDetal.,Dietaryfibre,wholegrains,andriskofcolorectalcancer: systematic review and dose-response meta-analysis of prospective studies. BritishMedicalJournal.2011;343:d6617.doi:10.1136/bmj.d6617.9. ParkYetal.Dietaryfiberintakeandriskofcolorectalcancer:apooled analysisofprospectivecohortstudies.JAMA.2005;294:2849-57.10. Belle FN et al. Dietary fiber, carbohydrates, glycemic index, and glycemic load in relation ro breast cancer prognosis in the HEAL cohort. Cancer EpidemiolBiomarkersPrev.2011;20:890-9.11.DongJYetal.Dietaryfiberintakeandriskofbreastcancer:ameta- analysisofprospectivecohortstudies.AmJClinNutr.2011;94:900-905.12.AuneDetal.Dietaryfiberandbreastcancerrisk:asystematicreviewand meta-analysisofprospectivestudies.AnnOncol2012;23:1394-402.13. Bandera EV et al. Association between dietary fiber and endometrial cancer:adose-responsemeta-analysis.AmJClinNutr.2007;86:1730-7.14.BidoliEetal.Fiberintakeandpancreaticcancerrisk:acase-controlstudy. AnnOncol23:264-268.15.SuzukiRetal.Aprospectiveanalysisoftheassociationbetweendietary fiberintakeandprostatecancerriskinEPIC.IntJCancer.2009;124:245-9.16. Sansbury LB et al. The effect of strict adherence to a high-fiber, high-fruit, and –vegetables ad low-fat eating pattern on adenoma recurrence. Am J Epidemiol.2009;170:576-84.17.LanzaEetal.,Thepolyppreventiontrialcontinuedfollow-upstudy:no effect of a low-fat, high-fiber, high-fruit and –vegetable diet on adenoma recurrenceeightyearsafterrandomization.CancerEpidemiolBiomarkers Prev.2007;16:1745-52.18. Pierce JP et al., Influence of a diet very high in vegetables, fruit, and fiber andlowinfatonprognosisfollowingtreatmentforbreastcancer:the Women’sHealthyEatingandLiving(WHEL)randomizedtrial.JAMA.2007; 298:289-98.
Fiber and the Immune System
1. Anderson JW, Baird P, Davis RH Jr, Ferreri S, Knudtson M, Koraym A, Waters V, Williams CL. Health benefits of dietary fiber. Nut Rev 2009;188-205.2. Roberfroid M, Gibson GR, Hoyles L, McCartney AL, Rastall R, Rowland I, WolversD,WatzlB,SzajewskaH,StahlB,GuarnerF,RespondekF,Whelan K,CoxamV,DaviccoMJ,LéotoingL,WittrantY,DelzenneNM,CaniPD, NeyrinckAM,MeheustA.Prebioticeffects:metabolicandhealthbenefits. BrJNutr2010;104Suppl2:S1-63.3. AjaniUA,FordES,MokdadAH.DietaryfiberandC-reactiveprotein: findings from national health and nutrition examination survey data. J Nutr2004;134:1181-5.4. MaY,GriffithJA,Chasan-TaberL,OlendzkiBC,JacksonE,StanekEJ3rd,Li W, Pagoto SL, Hafner AR, Ockene IS. Association between dietary fiber and serumC-reactiveprotein.AmJClinNutr2006;83:760-6.5. Herder C, Peltonen M, Koenig W, Sütfels K, Lindström J, Martin S, Ilanne-Parikka P, Eriksson JG, Aunola S, Keinänen-Kiukaanniemi S, Valle TT, Uusitupa M, Kolb H, Tuomilehto J; Finnish Diabetes Prevention Study Group. Anti-inflammatory effect of lifestyle changes in the Finnish DiabetesPreventionStudy.Diabetologia2009;52:433-42.6. Wannamethee SG, Whincup PH, Thomas MC, Sattar N. Associations between dietary fiber and inflammation, hepatic function, and risk of type 2diabetesinoldermen:potentialmechanismsforthebenefitsoffiberon diabetesrisk.DiabetesCare2009;32:1823-5.7. King DE, Egan BM, Woolson RF, Mainous AG 3rd, Al-Solaiman Y, Jesri A. Effect of a high-fiber diet vs a fiber-supplemented diet on C-reactive proteinlevel.ArchInternMed2007;167:502-6.
8. MaY,HébertJR,LiW,Bertone-JohnsonER,OlendzkiB,PagotoSL,TinkerL, Rosal MC, Ockene IS, Ockene JK, Griffith JA, Liu S. Association between dietary fiber and markers of systemic inflammation in the Women’s Health InitiativeObservationalStudy.Nutrition2008;24:941-9.9. North CJ, Venter CS, Jerling JC. The effects of dietary fibre on C-reactive protein, an inflammation marker predicting cardiovascular disease. Eur J ClinNutr2009;63:921-33.10. Ford ES, Mokdad AH, Liu S. Healthy Eating Index and C-reactive protein concentration:findingsfromtheNationalHealthandNutrition ExaminationSurveyIII,1988-1994.EurJClinNutr2005;59:278-83.11. de Mello VD, Schwab U, Kolehmainen M, Koenig W, Siloaho M, Poutanen K, Mykkänen H, Uusitupa M. A diet high in fatty fish, bilberries and wholegrain products improves markers of endothelial function and inflammation in individuals with impaired glucose metabolism in a randomisedcontrolledtrial:theSysdimetstudy.Diabetologia 2011;54:2755-67.12. Jacobs DR Jr, Andersen LF, Blomhoff R. Whole-grain consumption is associated with a reduced risk of noncardiovascular, noncancer death attributed to inflammatory diseases in the Iowa Women’s Health Study. AmJClinNutr2007;85:1606-14.13. Chuang SC, Vermeulen R, Sharabiani MT, Sacerdote C, Fatemeh SH, Berrino F, Krogh V, Palli D, Panico S, Tumino R, Athersuch TJ, Vineis P. The intake of grain fibers modulates cytokine levels in blood. Biomarkers 2011;16:504-10.14. Mateo Anson N, Aura AM, Selinheimo E, Mattila I, Poutanen K, van den Berg R, Havenaar R, Bast A, Haenen GR. Bioprocessing of wheat bran in whole wheat bread increases the bioavailability of phenolic acids in men and exertsantiinflammatoryeffectsexvivo.JNure2011;141:137-43.15. King DE, Mainous AG 3rd, Egan BM, Woolson RF, Geesey ME. Effect of psylliumfibersupplementationonC-reactiveprotein:thetrialtoreduce inflammatorymarkers(TRIM).AnnFamMed2008;6:100-6.16. Osborn DA, Sinn JK. Prebiotics in infants for prevention of allergic disease and food hypersensitivity. Cochrane Database Syst Rev 2007;17;(4):CD006474.17. Lomax AR, Calder PC. Prebiotics, immune function, infection and inflammation:areviewoftheevidence.BrJNutr2009;101:633-58.18. Rao S, Srinivasjois R, Patole S. Prebiotic supplementation in full-term neoneates:asystematicreviewofrandomizedcontrolledtrials.Arch PediatrAdolescMed2009;163:755-64.19.SzajewskaH.Probioticsandprebioticsinpreterminfants:wherearewe? Wherearewegoing?EarlyHumDev2010;86Suppl1:81-6.20. Thomas DW, Greer FR; American Academy of Pediatrics Committee on Nutrition; American Academy of Pediatrics Section on Gastroenterology, Hepatology, and Nutrition. Probiotics and prebiotics in pediatrics. Pediatrics2012;126:1217-31.21. Braegger C, Chmielewska A, Decsi T, Kolacek S, Mihatsch W, Moreno L, PieścikM,PuntisJ,ShamirR,SzajewskaH,TurckD,vanGoudoeverJ; ESPGHAN Committee on Nutrition. Supplementation of infant formula withprobioticsand/orprebiotics:asystematicreviewandcommentbythe ESPGHAN committee on nutrition. J Pediatr Gastroenterol Nutr 2011;52:238-50.22. Hughes C, Davoodi-Semiromi Y, Colee JC, Culpepper T, Dahl WJ, Mai V, Christman MC, Langkamp-Henken B. Galactooligosaccharide supplementation reduces stress-induced gastrointestinal dysfunction and daysofcoldorflu:arandomized,double-blind,controlledtrialinhealthy universitystudents.AmJClinNutr2011;93:1305-11.
Recommended Amounts
1. U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2010. 7th Edition, Washington, DC:U.S.GovernmentPrintingOffice,December2010.2. InstituteofMedicine,FoodandNutritionBoard.DietaryReferenceIntakes: Energy, Carbohydrates, Fiber, Fat, Fatty Acids, Cholesterol, Protein and AminoAcids.Washington,DC:NationalAcademiesPress;2005.3. U.S.FoodandDrugAdministration.AppendixF:CalculatethePercent DailyValuefortheAppropriateNutrients.GuidanceforIndustry:AFood Labeling Guide.
Filling the Fiber Gap
1. Hartman Group Compass Eating Database, 2012.2. International Food Information Council Foundation Food and Health Survey, 2013.3. Williams CL, Felt-Gunderson P. Analysis of average daily fiber intake amongready-to-eatcerealconsumers:roleofwhole-graincerealsin closing the fiber gap. American Jl of Lifestyle Medicine published on-line March 6, 2013.
33References32 References

®,™, © 2013 Kellogg NA Co.