
Kinder.1 - Indiana Speech-Language-Hearing Association · Indiana Speech Language Hearing...
21
4/1/2016 1 MEETING THE MEDICARE MARK Renee Kinder MS CCC‐SLP RAC‐CT Indiana Speech Language Hearing Association Saturday April 16 th 9:30‐11:30 COURSE DESCRIPTION Providing high quality documentation of skilled services to Medicare beneficiaries begins with an adequate understanding of regulations set forth via the Medicare Benefit Policy Manual and Local Coverage Determinations (LCDs) in regards to key areas including: skilled versus non‐skilled procedures; traditional interventions versus maintenance based plans of care establishing interventions to promote return from baseline to prior level of function initiating caregiver training to promote carryover of skilled interventions upon discharge from care and documenting outcomes of reasonable and necessary services via goal targets which are functional and measureable. OBJECTIVES: 1. Participant will be able to create functional goal targets to promote reimbursement of services and evidence outcomes. 2. Participant will be able to identify key areas for documenting reasonable and necessary services. 3. Participant will be able to describe procedures which support skilled care. CODING: YOUR FIRST DEFENSE CODING‐KEEPING CONTROL YOUR ST CLAIM EMR BOM PAYER CPT: Evaluation Codes
Transcript of Kinder.1 - Indiana Speech-Language-Hearing Association · Indiana Speech Language Hearing...

4/1/2016
1
MEETING THE MEDICARE MARK
ReneeKinderMSCCC‐SLPRAC‐CTIndianaSpeechLanguageHearingAssociationSaturdayApril16th 9:30‐11:30
COURSE DESCRIPTIONProvidinghighqualitydocumentationofskilledservicestoMedicarebeneficiariesbeginswithanadequateunderstandingofregulationssetforthviatheMedicareBenefitPolicyManualandLocalCoverageDeterminations(LCDs)inregardstokeyareasincluding:
skilledversusnon‐skilledprocedures;
traditionalinterventionsversusmaintenancebasedplansofcare
establishinginterventionstopromotereturnfrombaselinetopriorleveloffunction
initiatingcaregivertrainingtopromotecarryoverofskilledinterventionsupondischargefromcare
anddocumentingoutcomesofreasonableandnecessaryservicesviagoaltargetswhicharefunctionalandmeasureable.
OBJECTIVES:
1.Participantwillbeabletocreatefunctionalgoaltargetstopromotereimbursementofservicesandevidenceoutcomes.
2.Participantwillbeabletoidentifykeyareasfordocumentingreasonableandnecessaryservices.
3.Participantwillbeabletodescribeprocedureswhichsupportskilledcare.
CODING:YOUR FIRSTDEFENSE
CODING‐ KEEPING CONTROL
YOURSTCLAIM
EMRBOMPAYER
CPT:EvaluationCodes
4/1/2016
2
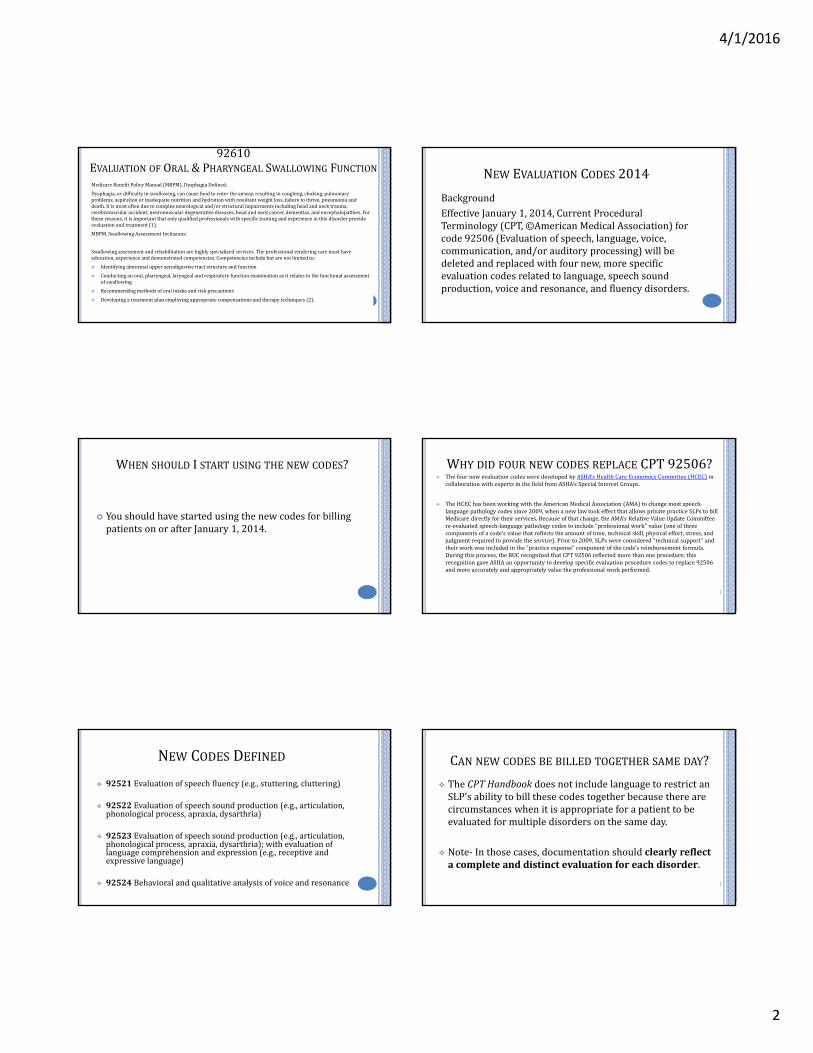
92610EVALUATION OF ORAL &PHARYNGEAL SWALLOWING FUNCTIONMedicareBenefitPolicyManual(MBPM),DysphagiaDefined:
Dysphagia,ordifficultyinswallowing,cancausefoodtoentertheairway,resultingincoughing,choking,pulmonaryproblems,aspirationorinadequatenutritionandhydrationwithresultantweightloss,failuretothrive,pneumoniaanddeath.Itismostoftenduetocomplexneurologicaland/orstructuralimpairmentsincludingheadandnecktrauma,cerebrovascularaccident,neuromusculardegenerativediseases,headandneckcancer,dementias,andencephalopathies.Forthesereasons,itisimportantthatonlyqualifiedprofessionalswithspecifictrainingandexperienceinthisdisorderprovideevaluationandtreatment(1).
MBPM,SwallowingAssessmentInclusions:
Swallowingassessmentandrehabilitationarehighlyspecializedservices.Theprofessionalrenderingcaremusthaveeducation,experienceanddemonstratedcompetencies.Competenciesincludebutarenotlimitedto:
Identifyingabnormalupperaerodigestive tractstructureandfunction
Conductinganoral,pharyngeal,laryngealandrespiratoryfunctionexaminationasitrelatestothefunctionalassessmentofswallowing
Recommendingmethodsoforalintakeandriskprecautions
Developingatreatmentplanemployingappropriatecompensationsandtherapytechniques(2).
NEW EVALUATION CODES 2014
BackgroundEffectiveJanuary1,2014,CurrentProceduralTerminology(CPT,©AmericanMedicalAssociation)forcode92506(Evaluationofspeech,language,voice,communication,and/orauditoryprocessing)willbedeletedandreplacedwithfournew,morespecificevaluationcodesrelatedtolanguage,speechsoundproduction,voiceandresonance,andfluencydisorders.
WHEN SHOULD ISTART USING THE NEW CODES?
YoushouldhavestartedusingthenewcodesforbillingpatientsonorafterJanuary1,2014.
WHY DID FOUR NEW CODES REPLACE CPT92506? ThefournewevaluationcodesweredevelopedbyASHA'sHealthCareEconomicsCommittee(HCEC) in
collaborationwithexpertsinthefieldfromASHA'sSpecialInterestGroups.
TheHCEChasbeenworkingwiththeAmericanMedicalAssociation(AMA)tochangemostspeech‐languagepathologycodessince2009,whenanewlawtookeffectthatallowsprivatepracticeSLPstobillMedicaredirectlyfortheirservices.Becauseofthatchange,theAMA'sRelativeValueUpdateCommitteere‐evaluatedspeech‐languagepathologycodestoinclude"professionalwork"value(oneofthreecomponentsofacode'svaluethatreflectstheamountoftime,technicalskill,physicaleffort,stress,andjudgmentrequiredtoprovidetheservice).Priorto2009,SLPswereconsidered"technicalsupport"andtheirworkwasincludedinthe"practiceexpense"componentofthecode'sreimbursementformula.Duringthisprocess,theRUCrecognizedthatCPT92506reflectedmorethanoneprocedure;thisrecognitiongaveASHAanopportunitytodevelopspecificevaluationprocedurecodestoreplace92506andmoreaccuratelyandappropriatelyvaluetheprofessionalworkperformed.
NEW CODES DEFINED
92521 Evaluationofspeechfluency(e.g.,stuttering,cluttering)
92522 Evaluationofspeechsoundproduction(e.g.,articulation,phonologicalprocess,apraxia,dysarthria)
92523 Evaluationofspeechsoundproduction(e.g.,articulation,phonologicalprocess,apraxia,dysarthria);withevaluationoflanguagecomprehensionandexpression(e.g.,receptiveandexpressivelanguage)
92524 Behavioralandqualitativeanalysisofvoiceandresonance
CAN NEW CODES BE BILLED TOGETHER SAME DAY?
TheCPTHandbook doesnotincludelanguagetorestrictanSLP'sabilitytobillthesecodestogetherbecausetherearecircumstanceswhenitisappropriateforapatienttobeevaluatedformultipledisordersonthesameday.
Note‐ Inthosecases,documentationshouldclearlyreflectacompleteanddistinctevaluationforeachdisorder.

4/1/2016
3
92521‐ EVALUATION OF SPEECH FLUENCY
Inclusions‐ EvaluationofStutteringandCluttering Thefollowingdisordersaretypicallynon‐coveredforthegeriatricMedicarebeneficiary: Fluencydisorder Dysprosody Stutteringandcluttering(exceptneurogenicstutteringcausedbyacquiredbraindamage)
92522‐EVALUATION OF SPEECH SOUNDPRODUCTION
Inclusions‐ Articulation,PhonologicalProcess,Apraxia,Dysarthria
92523EVAL OF SPEECH SOUND PRODUCTIONWITH EVAL OF
LANGUAGE COMPREHENSION AND EXPRESSION
Inclusions‐ Articulation,PhonologicalProcesses,Apraxia,Dysarthria;ReceptiveandExpressiveLanguage
92523IS COMBINED SPEECH SOUND PRODUCTION AND
LANGUAGE ?WHAT IF IONLY EVALUATE LANGUAGE?
Iftwoormoreproceduresarebilledtogetheratleast51%ofthetime,itisstandardtodevelopabundledCPTcodeforthatsetofservices.
ASHAsurveyedpracticesandclinicsandconfirmedthatevaluationsforlanguageareaccompaniedbyevaluationsforspeechsoundproduction80%ofthetime.However,thereverseisnottrue.Itiscommonforspeechsoundproductionabilitiestobeevaluatedindependentofalanguageevaluation,whichiswhythereisastand‐alonecodeforspeechsoundproductionevaluation.
Ifapatientisevaluatedonlyforlanguage,SLPsshouldbill92523withthe‐52modifier,whichisusedwhentheservicesprovided arereducedincomparisonwiththefulldescriptionoftheservice.
CAN IBILL 92522AND 92523SAME DAY?
No,youmayonlybilloneortheother.Aspeechsoundproductionevaluation(CPT92522)isalreadyincludedasapartofCPT92523(speechsoundproductionevaluationwithlanguageevaluation).
92524BEHAVIORAL &QUALITATIVE ANALYSIS OF VOICE &RESONANCE
Q‐ DoesCPT92524(behavioralandqualitativeanalysisofvoiceandresonance)includeinstrumentalassessments?
A‐ No.Thereareseparatecodesforinstrumentalassessments,suchasCPT92520forlaryngealfunctionstudies.
4/1/2016
4
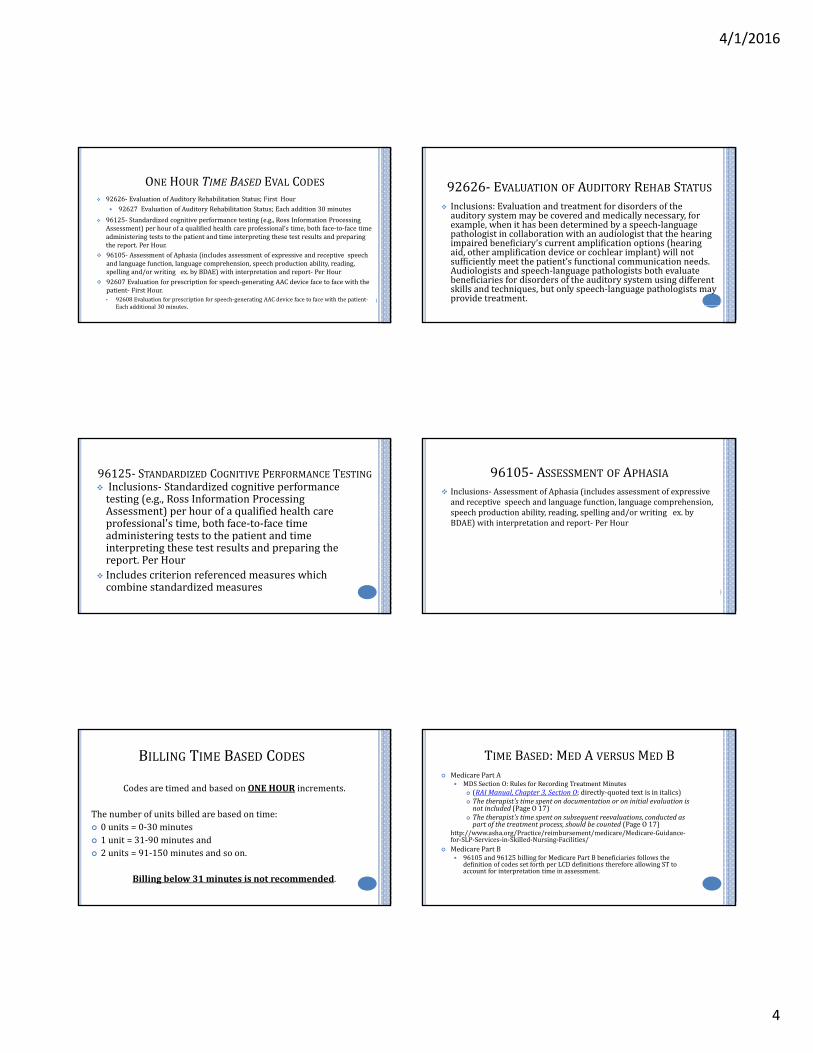
ONE HOUR TIME BASED EVAL CODES 92626‐ EvaluationofAuditoryRehabilitationStatus;FirstHour
92627 EvaluationofAuditoryRehabilitationStatus;Eachaddition30minutes
96125‐ Standardizedcognitiveperformancetesting(e.g.,RossInformationProcessingAssessment)perhourofaqualifiedhealthcareprofessional'stime,bothface‐to‐facetimeadministeringteststothepatientandtimeinterpretingthesetestresultsandpreparingthereport.PerHour.
96105‐ AssessmentofAphasia(includesassessmentofexpressiveandreceptivespeechandlanguagefunction,languagecomprehension,speechproductionability,reading,spellingand/orwritingex.byBDAE)withinterpretationandreport‐ PerHour
92607Evaluationforprescriptionforspeech‐generatingAACdevicefacetofacewiththepatient‐ FirstHour.• 92608Evaluationforprescriptionforspeech‐generatingAACdevicefacetofacewiththepatient‐
Eachadditional30minutes.
92626‐ EVALUATION OF AUDITORY REHAB STATUS Inclusions:Evaluationandtreatmentfordisordersoftheauditorysystemmaybecoveredandmedicallynecessary,forexample,whenithasbeendeterminedbyaspeech‐languagepathologistincollaborationwithanaudiologistthatthehearingimpairedbeneficiary’scurrentamplificationoptions(hearingaid,otheramplificationdeviceorcochlearimplant)willnotsufficientlymeetthepatient’sfunctionalcommunicationneeds.Audiologistsandspeech‐languagepathologistsbothevaluatebeneficiariesfordisordersoftheauditorysystemusingdifferentskillsandtechniques,butonlyspeech‐languagepathologistsmayprovidetreatment.
96125‐ STANDARDIZED COGNITIVE PERFORMANCE TESTING Inclusions‐ Standardizedcognitiveperformancetesting(e.g.,RossInformationProcessingAssessment)perhourofaqualifiedhealthcareprofessional'stime,bothface‐to‐facetimeadministeringteststothepatientandtimeinterpretingthesetestresultsandpreparingthereport.PerHour
Includescriterionreferencedmeasureswhichcombinestandardizedmeasures
96105‐ ASSESSMENT OF APHASIA Inclusions‐ AssessmentofAphasia(includesassessmentofexpressiveandreceptivespeechandlanguagefunction,languagecomprehension,speechproductionability,reading,spellingand/orwritingex.byBDAE)withinterpretationandreport‐ PerHour
BILLING TIME BASED CODES
CodesaretimedandbasedonONEHOUR increments.
Thenumberofunitsbilledarebasedontime: 0units=0‐30minutes 1unit=31‐90minutesand 2units=91‐150minutesandsoon.
Billingbelow31minutesisnotrecommended.
TIME BASED:MED AVERSUS MED B MedicarePartA
MDSSectionO:RulesforRecordingTreatmentMinutes (RAIManual,Chapter3,SectionO;directly‐quotedtextisinitalics) Thetherapist'stimespentondocumentationoroninitialevaluationisnotincluded (PageO17)
Thetherapist'stimespentonsubsequentreevaluations,conductedaspartofthetreatmentprocess,shouldbecounted (PageO17)
http://www.asha.org/Practice/reimbursement/medicare/Medicare‐Guidance‐for‐SLP‐Services‐in‐Skilled‐Nursing‐Facilities/
MedicarePartB 96105and96125billingforMedicarePartBbeneficiariesfollowsthe
definitionofcodessetforthperLCDdefinitionsthereforeallowingSTtoaccountforinterpretationtimeinassessment.
4/1/2016
5
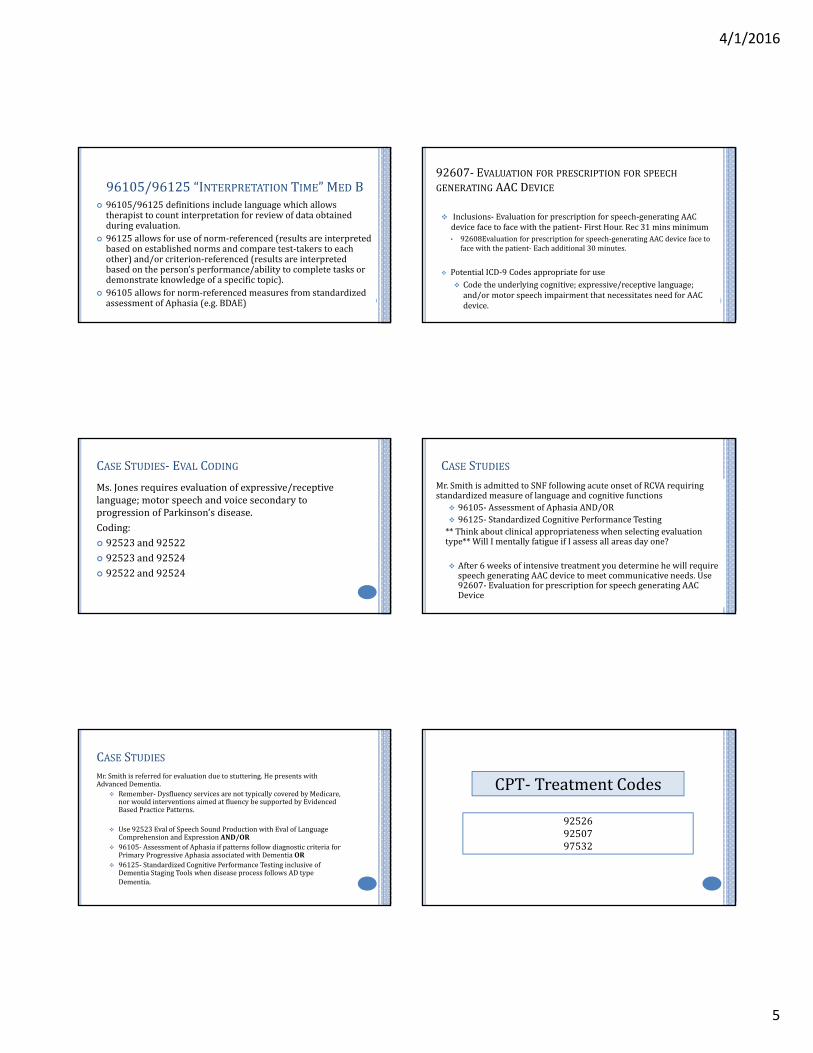
96105/96125“INTERPRETATION TIME”MED B 96105/96125definitionsincludelanguagewhichallowstherapisttocountinterpretationforreviewofdataobtainedduringevaluation.
96125allowsforuseofnorm‐referenced(resultsareinterpretedbasedonestablishednormsandcomparetest‐takerstoeachother)and/orcriterion‐referenced(resultsareinterpretedbasedontheperson’sperformance/abilitytocompletetasksordemonstrateknowledgeofaspecifictopic).
96105allowsfornorm‐referencedmeasuresfromstandardizedassessmentofAphasia(e.g.BDAE)
92607‐ EVALUATION FOR PRESCRIPTION FOR SPEECH
GENERATING AACDEVICE
Inclusions‐ Evaluationforprescriptionforspeech‐generatingAACdevicefacetofacewiththepatient‐ FirstHour.Rec31mins minimum• 92608Evaluationforprescriptionforspeech‐generatingAACdevicefaceto
facewiththepatient‐ Eachadditional30minutes.
PotentialICD‐9Codesappropriateforuse Codetheunderlyingcognitive;expressive/receptivelanguage;and/ormotorspeechimpairmentthatnecessitatesneedforAACdevice.
CASE STUDIES‐ EVAL CODING
Ms.Jonesrequiresevaluationofexpressive/receptivelanguage;motorspeechandvoicesecondarytoprogressionofParkinson’sdisease.Coding: 92523and92522 92523and92524 92522and92524
CASE STUDIESMr.SmithisadmittedtoSNFfollowingacuteonsetofRCVArequiringstandardizedmeasureoflanguageandcognitivefunctions 96105‐ AssessmentofAphasiaAND/OR 96125‐ StandardizedCognitivePerformanceTesting**Thinkaboutclinicalappropriatenesswhenselectingevaluationtype**WillImentallyfatigueifIassessallareasdayone?
After6weeksofintensivetreatmentyoudeterminehewillrequirespeechgeneratingAACdevicetomeetcommunicativeneeds. Use92607‐ EvaluationforprescriptionforspeechgeneratingAACDevice
CASE STUDIESMr.Smithisreferredforevaluationduetostuttering.HepresentswithAdvancedDementia.
Remember‐ DysfluencyservicesarenottypicallycoveredbyMedicare,norwouldinterventionsaimedatfluencybesupportedbyEvidencedBasedPracticePatterns.
Use92523Eval ofSpeechSoundProductionwithEval ofLanguageComprehensionandExpressionAND/OR
96105‐ AssessmentofAphasiaifpatternsfollowdiagnosticcriteriaforPrimaryProgressiveAphasiaassociatedwithDementiaOR
96125‐ StandardizedCognitivePerformanceTestinginclusiveofDementiaStagingToolswhendiseaseprocessfollowsADtypeDementia.
CPT‐ TreatmentCodes
925269250797532

4/1/2016
6
92526‐ DYSPHAGIA THERAPYPatient/caregivertraininginfeeding/swallowingtechniquesProperheadandbodypositioningAmountofintakeperswallowAppropriatediet(determining)textureandviscosityMeansoffacilitatingtheswallowFeedingtechniquesandneedforselfhelpeating/feedingdevicesFacilitationofmorenormaltoneororalfacilitationtechniquesLaryngealelevationtrainingCompensatorySwallowtechniquesOralsensitivitytrainingTechniquestoreduceshortnessofbreathoffatigueduringdurationofmeal.
DYSPHAGIA PER MEDICARE MANUAL
Dysphagia,ordifficultyinswallowing,cancausefoodtoentertheairway,resultingincoughing,choking,pulmonaryproblems,aspirationorinadequatenutritionandhydrationwithresultantweightloss,failuretothrive,pneumoniaanddeath.
Mostoftenduetocomplexneurologicaland/orstructuralimpairmentsincludingheadandnecktrauma,cerebrovascularaccident,neuromusculardegenerativediseases,headandneckcancer,dementias,andencephalopathies.Forthesereasons,itisimportantthatonlyqualifiedprofessionalswithspecifictrainingandexperienceinthisdisorderprovideevaluationandtreatment.(MBPM,2016)
SPECIALIZED DYSPHAGIA CAREPer the Medicare Benefit Policy Manual definition of SLP Scope:Swallowing assessment and rehabilitation are highly specialized services. The professional rendering care must have education, experience and demonstrated competencies. Competencies include but are not limited to: identifying abnormal upper aerodigestive tract structure and function; conducting an oral, pharyngeal, laryngeal and respiratory function examination as it relates to the functional assessment of swallowing; recommending methods of oral intake and risk precautions; and developing a treatment plan employing appropriate compensations and therapy techniques (MBPM, 2016).
THINK…WHAT MAKES MY SERVICES UNIQUE?HowdoyoueducatePatient/caregivertraininginfeeding/swallowingtechniques?Whatchangesaremadetohead&bodypositioningAmountofintakeperswallow(specific)Appropriatediet(determining)textureandviscosityMeansoffacilitatingtheswallowFeedingtechniquesandneedforselfhelpeating/feedingdevicesFacilitationofmorenormaltoneororalfacilitationtechniquesLaryngealelevationtrainingCompensatorySwallowtechniquesOralsensitivitytrainingTechniquestoreduceshortnessofbreathoffatigueduringdurationofmeal
VerbalUnderstanding/ReturnDemo
SPECIFIC‐ tsp;tbsp;#oftrials;goalsrelatedtoPOdiet/therapeuticportion
RelationtoInstrumental
MEASURES:BORG,PulseOx,amountoftimepriorto,signsafter.
NOW…HOW AM IDOCUMENTING THIS?DailyNoteSample1:PatientseenwithnoonmealforskilledST,likesmechanicalmeats,nursingfed100%ofthetime,verbalcuetositupstraight
DailyNoteSample2:PatientreceivedtherapeuticPOtrialsofmechanicalsoftmeatsatnoonmeal,notedincreasedbolusformationwhenpresentedin1tbsp sizebolusasevidencedbyreducedoralstasisthroughoutoralcavitys/pswallow,educationprovidedtoCNAstaffwithnotedverbalunderstandingandreturndemonstrationoftechniqueon7/10trials
92507TREATMENT OF SPEECH,LANGUAGE,VOICE,COMMUNICATION,AUDITORY PROCESSING
Skilledinterventionsaimedat:
Increasingexpressivelanguageskillsincludingabilitytocommunicatewantsandneedsandtreatmentstoaddressappropriatesyntaxandmorphology.Increasereceptivelanguageskillsforcomprehensionofspokenandwrittenlanguageimpactingabilitytorespondtoquestions,followdirections,andcomprehendstructuredandspontaneousinteractionswithothers.Increasingspeechintelligibilityskillsincludinginterventionsaimedatimprovingarticulatorypatternsandaddressingmotorspeechimpairmentssuchasapraxiaofspeechanddysarthria.Improvingpragmaticlanguageskillsrelatedtosocialaspectsofcommunicationincludingadequateknowledgeanduseofrulesforconversationandstory‐tellingandappropriateadaptationsoflanguagebasedonsettingandconversationalpartner.Increasevocalfunctionrelatedtorespiration,phonation,resonance,andpitch.Auralrehabilitationincludingprovisionofspeechreading.Traininganduseofnon‐speechgeneratingaugmentativeandalternativecommunication(AAC).Trainingandmodificationintheuseofavoiceprosthetic.

4/1/2016
7
97532‐ DEVELOPMENT OF COGNITIVE SKILLS
97532isatimebasedcodeusedfordevelopmentofcognitiveskillstoimproveattention,memory,problemsolving(includescompensatorytraining),direct(one‐on‐one)patientcontactbytheprovider,each15minutes
1unit:8minutesto<23minutes 2units:23minutesto<38minutes 3units:38minutesto<53minutes 4units:53minutesto<68minutes 5units:68minutesto<83minutes 6units:83minutesto<98minutes
97532‐ CONSIDERATIONS FOR USE ProvidersshouldbillCPT97532onlywhencognitivetreatmentistrulyadistinct,
separateactivity.Whenappropriatediagnosticassessmentisconducted,shouldcorrespondwithnewonsetforjustificationofdecline.
Differsfromservicesprovidedfor92507‐ Treatmentofspeech,language,voice,communication,and/orauditoryprocessingdisorder;individual.
Canbeusedinconjunctionwith92526,howevershouldnotbeusedsimplyduetothefactdysphagiaservicesarebeingprovidedtoanindividualwithcognitiveimpairment.
Canonlybeusedwhenappropriatedifferentialdiagnosisiscompletedtoruleoutthefollowingasrootcause: AMSassociatedwithperiodofdeliriumincludingthoseassociatedwithinfection(UTI) Underlyinglanguageand/orauditoryimpairmentasprimarycauseofcommunication
breakdowns;
92507AND 97532CorrectCodingInitiative(CCI)Edits 92507and97532CANNOTbebilledsameday.Determiningappropriatecodinguse: DifferentialdiagnosisintorootcauseoffunctionalimpairmentsbeginsatSOC.
Examples: Residentpresentswithdecreasedabilitytofollowcommands.Rootcausecouldbe‐ Decreasedimmediatememoryfordirectives(cog);decreasedattentiontotask(cog);decreasedauditorycomprehensionofdirectives(language);decreaseauditoryacuity(AR‐ 92507perMedicareRegulations)
97532AND 92526 SLPsshouldnotbillcognitivetreatmentwhentheyprovideonlyswallowingorlanguagetreatmenttoapatientwhoalsohascognitivedisorders.
However,itmaybeappropriatetobill97532onthesamedayiftherearedistinctplansofcareandspecificgoalsandtreatmentactivitiesforcognitiveimpairmentandforswallowing
TakeHomePoint‐ Cognitiveimpairmentalonedoesnotnecessitateuseof97532.
CASE STUDIES:97532;92526 Ms.SmithpresentswithasevereoropharyngealdysphagiafollowingTBIwithresultingincreasedoralprocessingofbolus,anteriorspillage,pocketing/stasisaftertheswallow,delayedinitiationofpharyngealswallowandoverts/saspirationwithintake.Deficitsarecompoundedbycognitiveimpairmentsincludingimpulsivitywithintake.
Anticipatedinterventioncoding: 92526forSwallowingTherapy 97532forCognitiveinterventionsr/timpulsivityanddecreasedattentiontotask.

4/1/2016
8
CASE STUDIES:92526;92507 Mr.Jonespresentswithprogressionofdementiawithresultingdecreasedoralcoordination,anteriorloss,increasedprocessinganddecreasedabilitytofollowbasiccommandsatmealsinordertoincreaseabilitytofollowswallowstrategies.
Anticipatedinterventioncoding: 92526forincreasingswallowfunctions 92507forincreasingsuccesswithabilitytofollowcommands.NotelanguagePOCmaybemaintenancebasedinnatureinthatinterventionswillbeshortterminordertoestablish/traincaregiverregardingtechniques.
COMPETENCY CHECK‐WHAT WOULD YOU DO?
MRS.RAY‐ FREQUENT FALLSMrs.RaywasreferredforSpeechTherapyservicessecondarytoincreasedfallsinherroom. DuringinitialpatientinterviewyounotethatMrs.RaypresentswithdecreasedabilitytoverballysequencestepsforADLtasksshepreferstocompleteinherroom(I)including:transferringfromherbedtothewalker;completingdenturecare;andcompletingUBdressingtasks.Youdeterminetherootcauseofherimpairmentsisbasedondeclinesinherreceptivelanguageabilitiesinadditiontodeclinesinexpressivelanguagelimitingherabilitytoformulatethoughtsandrequestassistancefromcaregivers. Anticipatedinterventioncoding:92507languagebasedinterventionsappeartobemostappropriatetomeethercurrentneeds.
MR.SMITH‐ FREQUENT FALLSMr.SmithwasreferredforSpeechTherapyservicessecondarytofrequentfallswhichoccurinhisroom.Hewasadmittedtoyourfacility~1weekagos/pTBIwhichoccurredinthehomeenvironment.BaselinemeasuresduringSTevaluationrevealintactlanguageabilities,howeverhepresentswithsignificantdeclinesincause‐effectproblemsolvingandshorttermmemorytasks.FallsappeartobesubsequenttooveralldecreasedabilitytonegotiateobstaclesinroomenvironmentwhenperformingADLtasks. Anticipatedinterventioncoding‐ 97532toaddresscognitiveimpairmentsrelatedtomemoryandproblemsolving.
MEDICARE BENEFIT POLICY MANUAL
CHAPTER15“REASONABLE AND NECESSARY”
INDICATIONS FOR SPEECH THERAPY SERVICES Speech‐languagepathologyservicesarethoseservicesprovidedwithinthescopeofpracticeofspeech‐languagepathologists
Necessaryforthediagnosisandtreatmentofspeechandlanguagedisorders,whichresultincommunicationdisabilitiesandforthediagnosisandtreatmentofswallowingdisorders(dysphagia)
Regardlessofthepresenceofacommunicationdisability.
(SeeCMSPublication100‐03,MedicareNationalCoverageDeterminations(NCD)Manual,Part3,Section170.3)(CMSPublication100‐02,MedicareBenefitPolicyManual,Chapter15,Section230.3(A))

4/1/2016
9
“REASONABLE AND NECESSARY”EVIDENCED BASED PRACTICE
Theservicesshallbeconsideredunderacceptedstandardsofmedicalpractice tobeaspecificandeffectivetreatmentforthepatient'scondition.Acceptablepracticesfortherapyservicesarefoundin: Medicaremanuals(suchasthismanualandPublications100‐03and100‐04), ContractorsLocalCoverageDeterminations(LCDsandNCDsareavailable
ontheMedicareCoverageDatabase:http://www.cms.hhs.gov/mcdand Guidelinesandliteratureoftheprofessionsofphysicaltherapy,occupational
therapyandspeech‐languagepathology.
Tobeconsideredreasonableandnecessary,thefollowingconditionsmustbemet:(CMSPublication100‐02,MedicareBenefitPolicyManual,Chapter15,Section220.2(B))
“REASONABLE AND NECESSARY”COMPLEXITY AND SOPHISTICATION
Theservicesshallbeofsuchalevelofcomplexityandsophistication ortheconditionofthepatientshallbesuchthattheservicesrequiredcanbesafelyandeffectivelyperformedonlybyaqualifiedtherapist
Servicesthatdonotrequiretheperformanceorsupervisionofatherapistarenotskilledandarenotconsideredreasonableornecessarytherapyservices,eveniftheyareperformedorsupervisedbyaqualifiedprofessional.
Ifthecontractordeterminestheservicesfurnishedwereofatypethatcouldhavebeensafelyandeffectivelyperformedonlybyorunderthesupervisionofsuchaqualifiedprofessional,itshallpresumethatsuchserviceswereproperlysupervisedwhenrequired.However,thispresumptionisrebuttable,and,ifinthecourseofprocessingclaimsitfindsthatservicesarenotbeingfurnishedunderpropersupervision,itshalldenytheclaimandbringthismattertotheattentionoftheDivisionofSurveyandCertificationoftheRegionalOffice.
Tobeconsideredreasonableandnecessary,thefollowingconditionsmustbemet:(CMSPublication100‐02,MedicareBenefitPolicyManual,Chapter15,Section220.2(B))
“REASONABLE AND NECESSARY”MEDICAL DIAGNOSES
Whileabeneficiary'sparticularmedicalconditionisavalidfactorindecidingifskilledtherapyservicesareneeded,abeneficiary'sdiagnosisorprognosisshouldneverbethesolefactorindecidingthataserviceisorisnotskilled.Thekeyissueiswhethertheskillsofaqualifiedtherapistareneededtotreattheillnessorinjury,orwhethertheservicescanbecarriedoutbynonskilled personnel.SeeitemCfordescriptionsofskilled(rehabilitative)services.
Tobeconsideredreasonableandnecessary,thefollowingconditionsmustbemet:(CMSPublication100‐02,MedicareBenefitPolicyManual,Chapter15,Section220.2(B))
“REASONABLE AND NECESSARY”DETERMINING APPROPRIATE FREQUENCY AND DURATION
Theremustbeanexpectationthatthepatient'sconditionwillimprovesignificantlyinareasonable(andgenerallypredictable)periodoftime,ortheservicesmustbenecessaryfortheestablishmentofasafeandeffectivemaintenanceprogramrequiredinconnectionwithaspecificdiseasestate.Inthecaseofaprogressivedegenerativedisease,servicemaybeintermittentlynecessarytodeterminetheneedforassistiveequipmentand/orestablishaprogramtomaximizefunction(seeitemDfordescriptionsofmaintenanceservices);and
Theamount,frequency,anddurationoftheservicesmustbereasonableunderacceptedstandardsofpractice.Thecontractorshallconsultlocalprofessionalsorthestateornationaltherapyassociationsinthedevelopmentofanyutilizationguidelines.
PLAN OF CARE REQUIREMENTS
STEPS
Step1:OrderReceivedStep2:ScreenStep3:EvaluateandDetermineifSkilledInterventionisNecessaryStep4:EstablishPOCStep5:WriteClarificationOrderStep6:GetPOCCertifiedStep7:ReEval asappropriateStep8:Recertifywhennecessary

4/1/2016
10
OVERVIEW:PLAN OF CARE (POC)REQUIREMENTS
OrderorReferral CleardistinctionforEvaluation/Re‐evaluationorScreening Beneficiary'sHistory andtheOnsetorExacerbationDateofthecurrentdisorder. Historyinconjunctioncurrentsymptomsmustestablishsupportforadditional
treatment. PriorLevelofFunctioningshouldbedocumented Baselineabilitiesshouldbedocumented PLOF+Baselineestablishthebasisforthetherapeuticinterventions. Plan,Goals(realistic,long‐term,functionalgoals) Duration oftherapy,Frequency oftherapy,anddefinitionoftheTypeofService. Diagnosticandassessmenttestingservicestoascertainthetype,causalfactor(s)
shouldbeidentifiedduringtheevaluation. Clarifyifplanisanticipatedtoberehabilitative/restorativeormaintenancebased
STEP1:ORDER/REFERRAL Neededforinitialevaluation MDsignatureonPOCactsascertification/clarificationofservicesafterevaluation
Newsignature/certificationneededfor: AnysignificantupdatestoPOCaffectingLTG(willrequirere‐eval orrecertification)
Additionofnewinterventionsnotincludedoninitialplan. Example‐STbeginsservicesfordysphagiaalone,asresidentprogresseswithlaryngealfunctionfurthereval iswarrantedforvoiceandmotorspeech
PTcompletesinitialPOCforwoundcareandprogressespatienttopointwherestandardPTeval isreasonableandnecessary
RecertificationofPOC
STEP2:“SCREENING” Screeningassessmentsarenon‐coveredandshouldnotbebilled.
Theinitialscreeningassessmentsofpatientsorregularroutinereassessmentsofpatientsarenotcovered.
Think…..ScreeningTellsyouEval orNotEvalNoClinicalJudgmentsorSkilledRecommendationsShouldbeMadefromScreenAlone
STEP3:EVALUATION Theorderorreferralfortheevaluationandanyspecifictestinginareasofconcernshouldbedesignatedbythereferringphysicianinconsultationwiththetherapist.
Thedocumentationoftheevaluationorre‐evaluationbythetherapistshoulddemonstratethatanactualhands‐onassessmentoccurredtosupportthemedicalnecessityforreimbursementoftheevaluationorre‐evaluation.
DETERMINESNEEDFORSKILL
EVALUATION DEFINEDEVALUATIONisaseparatelypayablecomprehensiveserviceprovidedbyaclinician,asdefinedabove,thatrequiresprofessionalskillstomakeclinicaljudgmentsaboutconditionsforwhichservicesareindicatedbasedonobjectivemeasurementsandsubjectiveevaluationsofpatientperformanceandfunctionalabilities(BASELINES).
Evaluationiswarrantede.g.,foranewdiagnosis(changefromplof).
Theseevaluativejudgmentsareessentialtodevelopmentoftheplanofcare,includinggoalsandtheselectionofinterventions.
MEDICAL HISTORY
OnsetorExacerbationDate
Onset/ExacerbationDate:thedateofthefunctionalchangewhichasaresultofdxindicatedtheneedforskilledcare
ChronicConditions:Maynotbethedateofdxforcondition,howeverrelatedtoexacerbationofdxprocess
NewConditions:CVA/TBIwillbedateofnewinsult
Inconjunctioncurrentsymptoms
Providecorrelationofwhynewonsethasresultedinsymptomsrequiringyouruniqueskilledservices.

4/1/2016
11
DETERMINE NEED FOR SKILL
EvidencedBasedPractice
ComplexityandSophistication
MedicalDiagnoses
IndividualizedFrequencyandDuration
“REASONABLE AND NECESSARY”EVIDENCED BASED PRACTICE
Theservicesshallbeconsideredunderacceptedstandardsofmedicalpractice tobeaspecificandeffectivetreatmentforthepatient'scondition.Acceptablepracticesfortherapyservicesarefoundin: Medicaremanuals(suchasthismanualandPublications100‐03and100‐04), ContractorsLocalCoverageDeterminations(LCDsandNCDsareavailable
ontheMedicareCoverageDatabase:http://www.cms.hhs.gov/mcdand Guidelinesandliteratureoftheprofessionsofphysicaltherapy,occupational
therapyandspeech‐languagepathology.
Tobeconsideredreasonableandnecessary,thefollowingconditionsmustbemet:(CMSPublication100‐02,MedicareBenefitPolicyManual,Chapter15,Section220.2(B))
“REASONABLE AND NECESSARY”COMPLEXITY AND SOPHISTICATION
Theservicesshallbeofsuchalevelofcomplexityandsophistication ortheconditionofthepatientshallbesuchthattheservicesrequiredcanbesafelyandeffectivelyperformedonlybyaqualifiedtherapist
Servicesthatdonotrequiretheperformanceorsupervisionofatherapistarenotskilledandarenotconsideredreasonableornecessarytherapyservices,eveniftheyareperformedorsupervisedbyaqualifiedprofessional.
Ifthecontractordeterminestheservicesfurnishedwereofatypethatcouldhavebeensafelyandeffectivelyperformedonlybyorunderthesupervisionofsuchaqualifiedprofessional,itshallpresumethatsuchserviceswereproperlysupervisedwhenrequired.However,thispresumptionisrebuttable,and,ifinthecourseofprocessingclaimsitfindsthatservicesarenotbeingfurnishedunderpropersupervision,itshalldenytheclaimandbringthismattertotheattentionoftheDivisionofSurveyandCertificationoftheRegionalOffice.
Tobeconsideredreasonableandnecessary,thefollowingconditionsmustbemet:(CMSPublication100‐02,MedicareBenefitPolicyManual,Chapter15,Section220.2(B))
“REASONABLE AND NECESSARY”MEDICAL DIAGNOSES
Whileabeneficiary'sparticularmedicalconditionisavalidfactorindecidingifskilledtherapyservicesareneeded,abeneficiary'sdiagnosisorprognosisshouldneverbethesolefactorindecidingthataserviceisorisnotskilled.Thekeyissueiswhethertheskillsofaqualifiedtherapistareneededtotreattheillnessorinjury,orwhethertheservicescanbecarriedoutbynonskilled personnel.SeeitemCfordescriptionsofskilled(rehabilitative)services.
Tobeconsideredreasonableandnecessary,thefollowingconditionsmustbemet:(CMSPublication100‐02,MedicareBenefitPolicyManual,Chapter15,Section220.2(B))
“REASONABLE AND NECESSARY”DETERMINING APPROPRIATE FREQUENCY AND DURATION
Theremustbeanexpectationthatthepatient'sconditionwillimprovesignificantlyinareasonable(andgenerallypredictable)periodoftime,ortheservicesmustbenecessaryfortheestablishmentofasafeandeffectivemaintenanceprogramrequiredinconnectionwithaspecificdiseasestate.Inthecaseofaprogressivedegenerativedisease,servicemaybeintermittentlynecessarytodeterminetheneedforassistiveequipmentand/orestablishaprogramtomaximizefunction(seeitemDfordescriptionsofmaintenanceservices);and
Theamount,frequency,anddurationoftheservicesmustbereasonableunderacceptedstandardsofpractice.Thecontractorshallconsultlocalprofessionalsorthestateornationaltherapyassociationsinthedevelopmentofanyutilizationguidelines.
TREATMENT:“SKILLED PROCEDURES” Analysisofactualprogresstowardgoals.
Establishmentoftreatmentgoalsspecifictodysfunctionanddesignedtospecificallyaddresseachproblemidentifiedininitialassessment.
Theselectionandinitialtrainingofadeviceforaugmentativeoralternativecommunicationsystems.
Patientandfamilytrainingtoaugmentrestorativetreatmentortoestablishamaintenanceprogram.Educationofstaffandfamilymustbeginatthetimeofevaluation.
4/1/2016
12
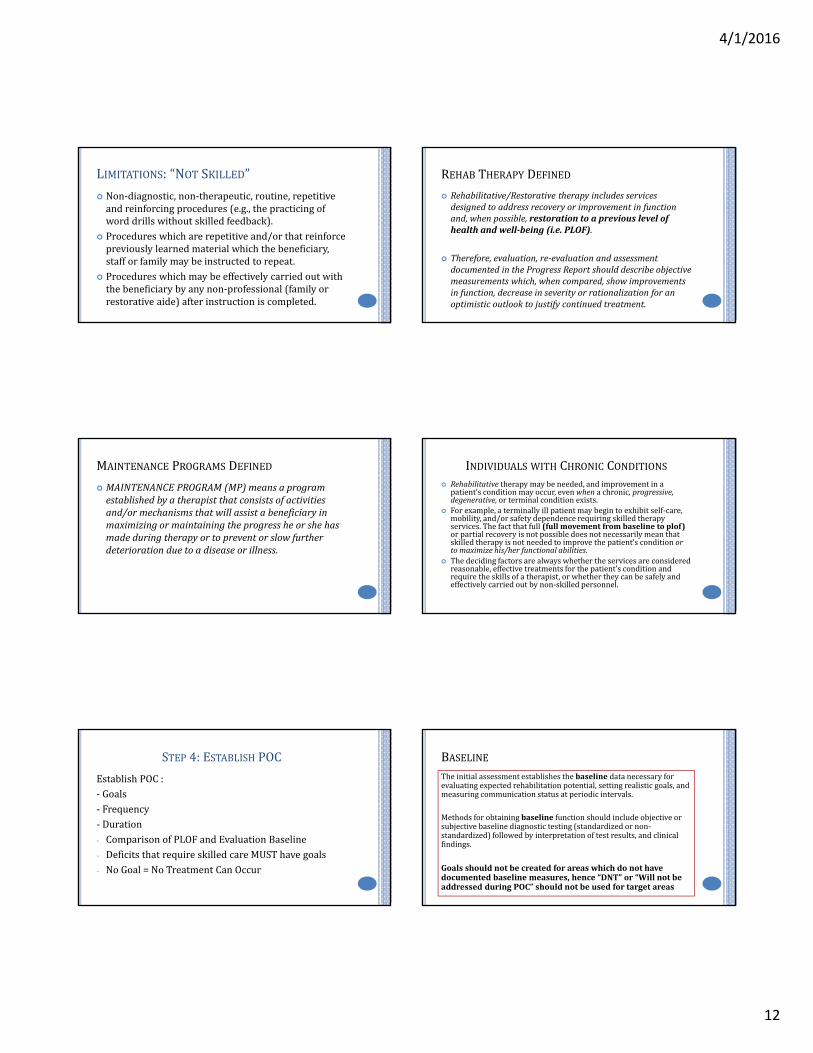
LIMITATIONS:“NOT SKILLED”
Non‐diagnostic,non‐therapeutic,routine,repetitiveandreinforcingprocedures(e.g.,thepracticingofworddrillswithoutskilledfeedback).
Procedureswhicharerepetitiveand/orthatreinforcepreviouslylearnedmaterialwhichthebeneficiary,stafforfamilymaybeinstructedtorepeat.
Procedureswhichmaybeeffectivelycarriedoutwiththebeneficiarybyanynon‐professional(familyorrestorativeaide)afterinstructioniscompleted.
REHAB THERAPY DEFINED
Rehabilitative/Restorativetherapyincludesservicesdesignedtoaddressrecoveryorimprovementinfunctionand,whenpossible,restorationtoapreviouslevelofhealthandwell‐being(i.e.PLOF).
Therefore,evaluation,re‐evaluationandassessmentdocumentedintheProgressReportshoulddescribeobjectivemeasurementswhich,whencompared,showimprovementsinfunction,decreaseinseverityorrationalizationforanoptimisticoutlooktojustifycontinuedtreatment.
MAINTENANCE PROGRAMS DEFINED
MAINTENANCEPROGRAM(MP)meansaprogramestablishedbyatherapistthatconsistsofactivitiesand/ormechanismsthatwillassistabeneficiaryinmaximizingormaintainingtheprogressheorshehasmadeduringtherapyortopreventorslowfurtherdeteriorationduetoadiseaseorillness.
INDIVIDUALS WITH CHRONIC CONDITIONS Rehabilitativetherapymaybeneeded,andimprovementinapatient’sconditionmayoccur,evenwhenachronic,progressive,degenerative,orterminalconditionexists.
Forexample,aterminallyillpatientmaybegintoexhibitself‐care,mobility,and/orsafetydependencerequiringskilledtherapyservices.Thefactthatfull(fullmovementfrombaselinetoplof)orpartialrecoveryisnotpossibledoesnotnecessarilymeanthatskilledtherapyisnotneededtoimprovethepatient’sconditionortomaximizehis/herfunctionalabilities.
Thedecidingfactorsarealwayswhethertheservicesareconsideredreasonable,effectivetreatmentsforthepatient’sconditionandrequiretheskillsofatherapist,orwhethertheycanbesafelyandeffectivelycarriedoutbynon‐skilledpersonnel.
STEP 4:ESTABLISH POC
EstablishPOC:‐ Goals‐ Frequency‐ Duration‐ ComparisonofPLOFandEvaluationBaseline‐ DeficitsthatrequireskilledcareMUSThavegoals‐ NoGoal=NoTreatmentCanOccur
BASELINETheinitialassessmentestablishesthebaseline datanecessaryforevaluatingexpectedrehabilitationpotential,settingrealisticgoals,andmeasuringcommunicationstatusatperiodicintervals.
Methodsforobtainingbaseline functionshouldincludeobjectiveorsubjectivebaselinediagnostictesting(standardizedornon‐standardized)followedbyinterpretationoftestresults,andclinicalfindings.
Goalsshouldnotbecreatedforareaswhichdonothavedocumentedbaselinemeasures,hence“DNT”or“WillnotbeaddressedduringPOC”shouldnotbeusedfortargetareas
4/1/2016
13
DIAGNOSTIC TESTING Diagnosticandassessmenttestingservicestoascertainthetype,causalfactor(s)shouldbeidentifiedduringtheevaluation.
Includesstandardizedandnon‐standardizedfunctionalassessmenttools.
WherecanIfindtheseresources??
PRIOR LEVEL OF FUNCTION
Theresidents’priorleveloffunctionreferstothefunctionallevelofindependencepriortoonsetofdeclinewhichnecessitatedneedforskilledtherapyscreening,andifdeemednecessary,furtherevaluationandskilledintervention.
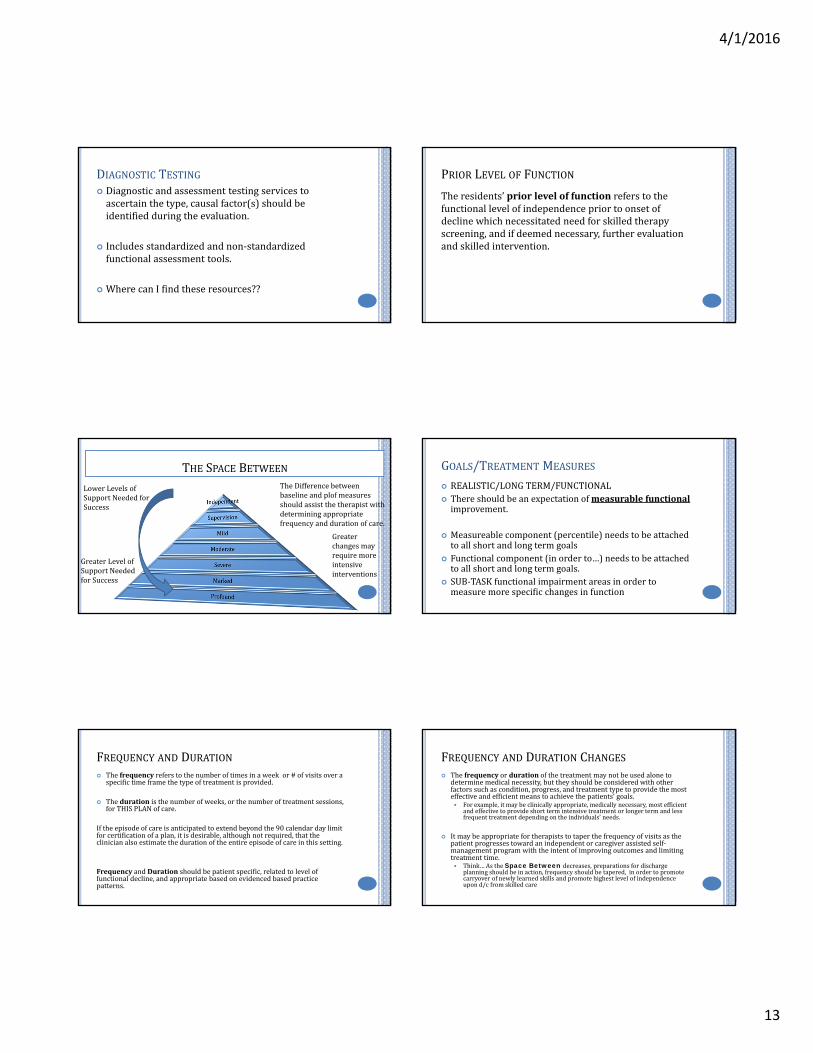
THE SPACE BETWEEN
GreaterLevelofSupportNeededforSuccess
LowerLevelsofSupportNeededforSuccess
TheDifferencebetweenbaselineandplof measuresshouldassistthetherapistwithdeterminingappropriatefrequencyanddurationofcare.
Greaterchangesmayrequiremoreintensiveinterventions
GOALS/TREATMENT MEASURES
REALISTIC/LONGTERM/FUNCTIONAL Thereshouldbeanexpectationofmeasurablefunctionalimprovement.
Measureablecomponent(percentile)needstobeattachedtoallshortandlongtermgoals
Functionalcomponent(inorderto…)needstobeattachedtoallshortandlongtermgoals.
SUB‐TASKfunctionalimpairmentareasinordertomeasuremorespecificchangesinfunction
FREQUENCY AND DURATION Thefrequencyreferstothenumberoftimesinaweek or#ofvisitsovera
specifictimeframethetypeoftreatmentisprovided.
Theduration isthenumberofweeks,orthenumberoftreatmentsessions,forTHISPLANofcare.
Iftheepisodeofcareisanticipatedtoextendbeyondthe90calendardaylimitforcertificationofaplan,itisdesirable,althoughnotrequired,thattheclinicianalsoestimatethedurationoftheentireepisodeofcareinthissetting.
FrequencyandDurationshouldbepatientspecific,relatedtoleveloffunctionaldecline,andappropriatebasedonevidencedbasedpracticepatterns.
FREQUENCY AND DURATION CHANGES Thefrequency orduration ofthetreatmentmaynotbeusedaloneto
determinemedicalnecessity,buttheyshouldbeconsideredwithotherfactorssuchascondition,progress,andtreatmenttypetoprovidethemosteffectiveandefficientmeanstoachievethepatients’goals. Forexample,itmaybeclinicallyappropriate,medicallynecessary,mostefficient
andeffectivetoprovideshorttermintensivetreatmentorlongertermandlessfrequenttreatmentdependingontheindividuals’needs.
Itmaybeappropriatefortherapiststotaperthefrequencyofvisitsasthepatientprogressestowardanindependentorcaregiverassistedself‐managementprogramwiththeintentofimprovingoutcomesandlimitingtreatmenttime. Think…AstheSpace Between decreases,preparationsfordischarge
planningshouldbeinaction,frequencyshouldbetapered,inordertopromotecarryoverofnewlylearnedskillsandpromotehighestlevelofindependenceupond/cfromskilledcare

4/1/2016
14
STEP 5:WRITE CLARIFICATION ORDER
Patienttoreceiveskilled(insertdiscipline)(insertfrequency)(insertduration)inorderto(insertreason)
STEP 6:CERTIFICATION OF EVAL/POC CERTIFICATIONisthePhysician’s/NonPhysicianPractitioner’s(NPP)approvaloftheplanofcare(evaluation).
Certificationrequires SignaturemustbefromthephysicianorNPP Timelycertificationoccurswithin30days Adatedsignatureontheplanofcareorsomeotherdocumentthatindicatesapprovaloftheplanofcare
Wheninitialcertexpires,arecert mustthenbecompletedcertifiedwithin30days(needsMDsignatureanddatewhichcanbeaddedasreceiptdate).
STEP 7:RE‐EVAL AS NEEDED Re‐evaluationmaybecoveredifnecessarybecauseofachangeinthebeneficiary'scondition.
(CMSPublication100‐02,MedicareBenefitPolicyManual,Chapter15,Section220.3.C)
Coveredonlyifthedocumentationsupportstheneedforfurthertestsandmeasurementsaftertheinitialevaluation.
Indicationsforare‐evaluationincludenewclinicalfindings,asignificantchangeinthepatient'scondition,orfailuretorespondtothetherapeuticinterventionsoutlinedintheplanofcare.
Maybeappropriatepriortoplanneddischargeforthepurposesofdeterminingwhethergoalshavebeenmet,orfortheuseofthephysicianorthetreatmentsettingatwhichtreatmentwillbecontinued.
Continuousassessmentofthepatient'sprogressisacomponentofongoingtherapyservicesandisnotpayableasare‐evaluation.
Are‐evaluationisnotaroutine,recurringservicebutisfocusedonevaluationofprogresstowardcurrentgoals,makingaprofessionaljudgmentaboutcontinuedcare,modifyinggoalsand/ortreatmentorterminatingservices.
RE‐ EVALUATIONS ARE NOT
STEP 8:RECERT WHEN NECESSARY
Requirescompletionofrecert documentwithinOptima
RequiresMDsignatureobtainedintimelymanner(30days)
Additionalclarificationorders
REAL WORLD APPLICATION
ASHAPRACTICEPORTALShttp://www.asha.org/practice‐portal/Contain:EvidencedBasedMaps;ClinicalToolsAphasia;Dementia;HearingLoss;TBIinAdults
ASHAPREFERREDPRACTICEPATTERNShttp://www.asha.org/policy/PP2004‐00191/

4/1/2016
15
MAINTENANCE PROGRAMS
Theservicesofamaintenanceprogramthemselvesarenotcovered.However,thedevelopmentofafunctionaltreatmentplanforpatientmaintenanceincludingevaluation,planoftreatment,andstaffandfamilytraining,iscovered,butitmustrequiretheskillsofanSLP,andbeadistinctandseparateservicewhichcanonlybedonesafelybyaSLP
DOCUMENTING “ABILITY TO LEARN” Documentationisexpectedtosupporttheabilityofthebeneficiarytolearnandretaininstruction.
Absenceofsuchdocumentationmayresultinadenialofservices.
Ifthepatienthasquestionablecognitiveskills,abriefcognitive‐communicationassessmentshouldbeperformedinordertoestablishthepatient'slearningability.Thebriefcognitiveassessmentmayalsodeterminetheneedformorecomprehensivecognitiveperformancetesting.
TREATMENT MEASURES
Thereshouldbeanexpectationofmeasurablefunctional improvement.
Think…. Measureablecomponent(percentile)needstobeattachedtoallshortandlongtermgoals
Functionalcomponent(inorderto…)needstobeattachedtoallshortandlongtermgoals.
TREATMENT:“SKILLED PROCEDURES” Designofatreatmentprogramaddressingthebeneficiary'sdisorder.Continuedassessmentandanalysisduringtheimplementationoftheservicesisexpectedatregularintervals.
Establishmentofcompensatoryskillsforcommunication(e.g.,airinjectiontechniquesorwordfindingstrategies).
Establishmentofahierarchyofspeech‐languagetasksandcueinghatdirectsabeneficiarytowardcommunicationgoals.
TREATMENT:“SKILLED PROCEDURES” Analysisofactualprogresstowardgoals.
Establishmentoftreatmentgoalsspecifictospeechdysfunctionanddesignedtospecificallyaddresseachproblemidentifiedininitialassessment.
Theselectionandinitialtrainingofadeviceforaugmentativeoralternativecommunicationsystems.
Patientandfamilytrainingtoaugmentrestorativetreatmentortoestablishamaintenanceprogram.Educationofstaffandfamilymustbeginatthetimeofevaluation.
LIMITATIONS:“NOT SKILLED”
ServicesrenderedbyaSLPassistantoraide. Provisionofpracticeforuseofaugmentativeoralternativecommunicationsystemsafterbeingtaughttheiruse.
Althoughspeech‐languagepathologistsmayperformlaryngoscopyfortheassessmentofvoiceproductionandvocalfunction,laryngoscopyformedicaldiagnosticpurposesmustbeperformedbyaphysician.

4/1/2016
16
LIMITATIONS:“NOT SKILLED”
Non‐diagnostic,non‐therapeutic,routine,repetitiveandreinforcingprocedures(e.g.,thepracticingofworddrillswithoutskilledfeedback).
Procedureswhicharerepetitiveand/orthatreinforcepreviouslylearnedmaterialwhichthebeneficiary,stafforfamilymaybeinstructedtorepeat.
Procedureswhichmaybeeffectivelycarriedoutwiththebeneficiarybyanynon‐professional(familyorrestorativeaide)afterinstructioniscompleted.
AURAL REHAB Theterms,auralrehabilitation,auditoryrehabilitation,auditoryprocessing,lipreadingandspeechreadingareamongthetermsusedtodescribecoveredservicesrelatedtoperceptionandcomprehensionofsoundthroughtheauditorysystem. (CMSPublication100‐02,MedicareBenefitPolicyManual,Chapter15,Section230.3.D.3)
Coverageforspeechreadingisonlyallowedwithdocumentationthatsupportsalossofhearingsensitivitythatcannotbecorrectedwithahearingaidoramplification.Documentationshouldalsosupportvisualacuityofthebeneficiarysufficienttoparticipateinauralrehabilitation.
AURAL REHAB:“MEDICAL NECESSITY” Speechreadingisconsideredmedicallynecessarywhendeterminedbyalicensedaudiologistthattheuseofahearingaidorotheramplificationwouldnotsignificantlyimprovethebeneficiary'sunderstandingofspeech.
Speechreadingtrainingisnotmedicallynecessaryforbeneficiarieswhorefusetowearahearingaid.Routinescreeningforhearingacuityorevaluationsaimedattheuseofhearingaidsisnotacoveredservice.
DETERMINATION OF THE MEDICAL NECESSITY FOR THE SPEECH
READING WILL BE BASED ON THE FOLLOWING CRITERIA: Documentationofbasichearingevaluationandaudiogram; Documentationidentifyingtypeandextentofhearingloss; Documentationofadequatecognitiveandmemoryskills; Documentationthatvisualacuity,withglassesifapplicable,issufficienttoallowthebeneficiarytoparticipateinthetherapy;
Documentationofthebeneficiary'smotivationtoparticipateintherapyinordertoimproveunderstandingofspeech.
SeeCMSPublication100‐02,MedicareBenefitPolicyManual,Chapter15,Section230.3.D.3formoreinformationonauralrehabilitation.
COGNITIVE IMPAIRMENTS :“MEMORY AIDES” Speech‐languagepathologyservicesprovidedforchronicdisordersofmemoryandorientationarecoveredserviceswhensignificantfunctionalprogressisdemonstratedatearlystagesofthedisorder.Whenfunctionalprogressplateaus,thedevelopmentofamaintenanceprogram,includingtrainingofcaregiversandfamilymembersiscovered
Preparationofmemoryaidssuchasmemorybooks,memoryboards,orcommunicationbooksmaybecovered.Supervisionoftheuseofsuchaidsisnotcoveredastheseservicesdonotrequiretheskillsofaqualifiedtherapist.
MEDICAL DIAGNOSES “NOT COVERED” Thefollowingdisordersaretypicallynon‐coveredforthegeriatricMedicarebeneficiary: Fluencydisorder Conceptualhandicap Dysprosody Stutteringandcluttering(exceptneurogenicstutteringcausedbyacquiredbraindamage)
Myofunctional disorders,e.g.,tonguethrust
4/1/2016
17
ENGLISH AS A SECOND LANGUAGE
SpeechtherapyinterventionstoinstructthebeneficiaryinEnglishphrases,whohasaprimarylanguageotherthanEnglish,arenotcovered.
However,whentheprimarylanguageofthebeneficiaryisotherthanEnglish,speechtherapyinterventionsinthepatient'sprimarylanguagewillbecoveredwithintheparametersofthisLCD.
CAN ISKILL FOR THAT?? Nursingrefersaresidentfordietchangeduetoloosingtheirdentures FamilyrefersanewresidentforARservicesafterreceivingacochlear
implant Daughterofaresidentwithadvanceddementiawantstreatmentbecause
hermom“stutters” AnewadmissioncurrentlyonABTforUTIisreferredforcognitivetherapy
dueto“behaviors” YourfacilityMDSCoordinatorrefersaresidentwhopresentswith
decreasedBIMSscoresinSectionCoftheMDS YourRehabDirectorrefersaresidentforspeechclaritybecause“his
denturesmovearoundwhenhetalks” ThefacilityAdministratorwantsyouandOTtobothtreatapatientfor
problemsolvingbecause“ifyoubothtreat,theywillgetbettersooner”
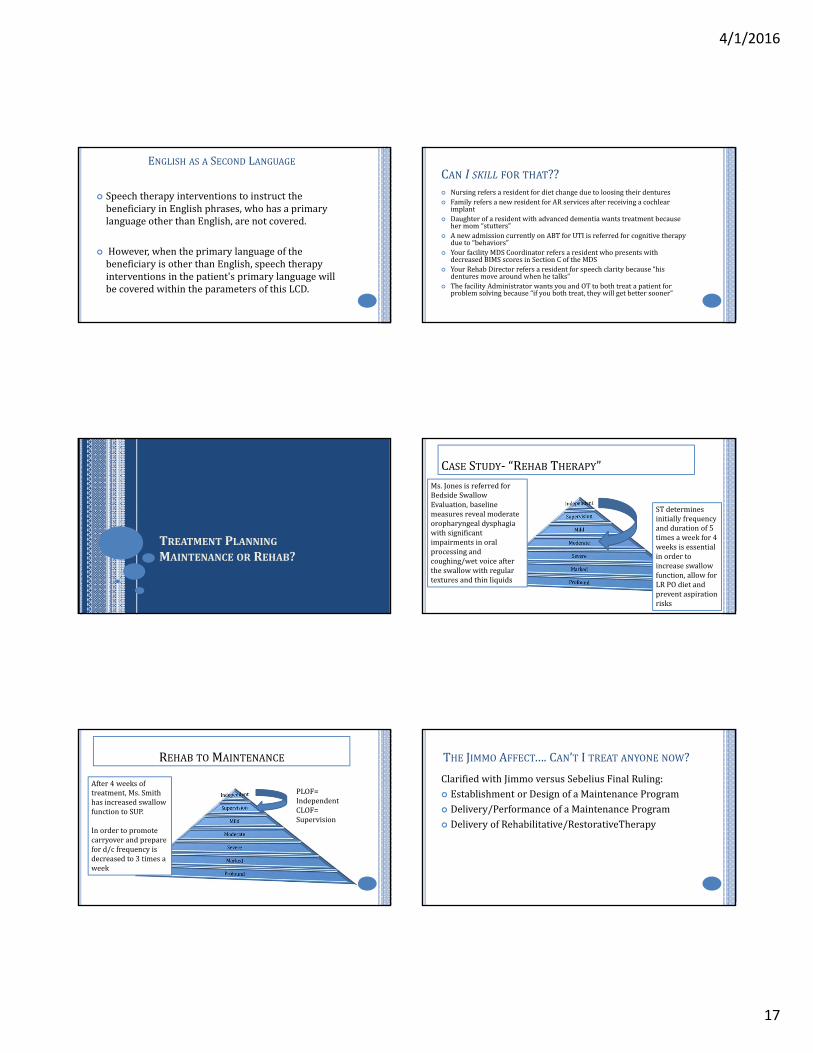
TREATMENT PLANNINGMAINTENANCE OR REHAB?
CASE STUDY‐ “REHAB THERAPY”Ms.JonesisreferredforBedsideSwallowEvaluation,baselinemeasuresrevealmoderateoropharyngealdysphagiawithsignificantimpairmentsinoralprocessingandcoughing/wetvoiceaftertheswallowwithregulartexturesandthinliquids
STdeterminesinitiallyfrequencyanddurationof5timesaweekfor4weeksisessentialinordertoincreaseswallowfunction,allowforLRPOdietandpreventaspirationrisks
REHAB TO MAINTENANCE
After4weeksoftreatment,Ms.SmithhasincreasedswallowfunctiontoSUP.
Inordertopromotecarryoverandprepareford/cfrequencyisdecreasedto3timesaweek
PLOF=IndependentCLOF=Supervision
THE JIMMO AFFECT….CAN’T ITREAT ANYONE NOW?
ClarifiedwithJimmo versusSebelius FinalRuling: EstablishmentorDesignofaMaintenanceProgram Delivery/PerformanceofaMaintenanceProgram DeliveryofRehabilitative/RestorativeTherapy

4/1/2016
18
MAINTENANCE SAMPLE:VOICEMotorSpeech/Voice:SkilledSTservicesmaybedeemedreasonableandnecessaryinordertomaintainvocalclarityandintensityforanindividualwithParkinson’sDiseaseinordertocontinuetrainingviauseofLeeSilvermanVoiceTherapy(LSVT)techniquesformaintenance.Note:transitionfromtherapyservicesaimedatincreasingfunctiontomaintenancetherapyshouldoccurfollowingtherapist/residentdeterminationthatmaxbenefithasbeenachievedataparticularcommunicationlevel(word,phase,sentence,structuredconversation,orspontaneousconversation)withmaintenanceinterventionsbeingaimedatcontinuedcommunicationsuccess(pendingmodificationswhichmaybewarrantedsecondarytotypicaldeclineswithdiseaseprogression)atthislevelatadecreasedintensityfrompriorservices.
Whycantheseservicesnotbetransitionedtoanon‐skilledprofessionalsuchasaCNAorNurseforrestorative/maintenance?Duetotheprogressivenatureofvocalandmotorspeechsystemchanges,theskilledeyeofanSLPisneededtodevelopandcontinuevocalfunctionprotocolandconductdifferentialdiagnosiswhenchangesoccuracrossvarioussystemsofcommunicationwithdiseaseprogression.
MAINTENANCE SAMPLE:COG‐LANGUAGEAuditoryComprehension/Cognition:SkilledSTservicesmaybedeemedreasonableandnecessaryinordertomaintainauditorycomprehensionskillsinthefollowinginstances:Anindividuals/pnewneurologicalinsultfollowingaperiodofintensiveskilledSTinterventionsaimedatincreasingabilitiestocomprehendlanguageandperformcognitivetasks(sequencing,problemsolving)atthehighestlevelpossiblecontinuedservicesformaintenancemaybewarrantedtocontinueskilledtherapeutictasksforhighleveltasksinordertopreventfunctionaldeclinesinpreparationford/ctopriorlivingenvironmentwhilecontinuedservicesarebeingprovidedbyPT/OT.Interventionsprovidedasmaintenanceversusrehabilitationinnaturearetobeprovidedatadecreasedintensityfrominitialservices.
Whycantheseservicesnotbetransitionedtoanon‐skilledprofessional?Skilledinterventionsforhighlevelauditorycomprehensiontasksincludingabilitytofollowmulti‐stepADL/IADLcommands;comprehendconversationalinteractions;sequenceduringtasksandcompletefunctionalproblemsolvingwithothersrequiresadministrationoftaskswhichcannotbeperformedorconductedbyanon‐skilledprofessional.Inaddition,tasksintheaboveinstancewillrequireperiodicmodificationsecondarytoanticipatedincreasedsuccesswithPT/OTsessionswhichwillchangetasksegmentationandprogressionofADLsandIADLs.Remember‐ casessuchasdescribedmayalsomovefromrehabilitativeinnaturetomaintenancetoreturntorehabilitativeinnaturesecondarytoincreasedphysicalabilitiesnecessitatingtheneedforhigherlevelcognitiveandlanguagelearning.
MAINTENANCE SAMPLE:DYSPHAGIASkilledtherapyservicesmaybedeemedreasonableandnecessaryinordertomaintainadequateswallowfunctionsforpleasurefeedingregimentwhichisclearlydefinedandagreeduponbymembersoftheinterdisciplinaryteaminconjunctionwiththeresidentandfamilymembers.
Whycantheseservicesnotbetransitionedtoanon‐skilledprofessional?
PertheMedicareBenefitPolicyManual(2014):
Swallowingassessmentandrehabilitationarehighlyspecializedservices.Theprofessionalrenderingcaremusthaveeducation,experienceanddemonstratedcompetencies.Competenciesincludebutarenotlimitedto:identifyingabnormalupperaerodigestive tractstructureandfunction;conductinganoral,pharyngeal,laryngealandrespiratoryfunctionexaminationasitrelatestothefunctionalassessmentofswallowing;recommendingmethodsoforalintakeandriskprecautions;anddevelopingatreatmentplanemployingappropriatecompensationsandtherapytechniques.
Abovecompetenciescannotbeperformedbyanon‐skilledprofessionalinanindividualpresentingwithdysphagiaseveritywhichwouldwarrantpleasurefeedings.
Note‐ needforpleasurefeedingsmustbenecessitatedbyadysphagiasecondarytooral,pharyngeal,and/orupper1/3rdoftheesophagealphase.Servicesformaintenanceinendstageofdementiasecondarytopresenceoftonguethrustasrootcauseoresophagealimpairments/strictures/blockagesinthelower2/3rdoftheesophaguswouldnotwarrantservicesastheyarenotcoveredfortheMedicareBeneficiary.
GOAL BUILDING
CONSIDERATIONS PRIOR TO CREATING GOALSStepOne:Whatisthegapbetweencurrentbaselineandtheindividualspriorleveloffunction?WhatintensityofservicesareneededtoreturnindividualtoPLOF?StepTwo:Whatistheindividualsdesiredlongtermoutcome?StepThree:Willtheplanberestorativeormaintenancebasedinnature?
CAN IUSE CUESIN MY GOALS? PROS
CanAssistattheStartofCarewithDocumentingstimulability fortasksandabilitytolearn
CanbebeneficialforSHORTTERMmaintenancebasedplanstoreflectlevelofassistneededfromcaregiversatendofskilledcare
Canbebeneficialforshowingincreased“I”forpatientswhenweareabletoweaninconjunctionwithreflectingincreasedfunctionalabilities
CONS IfyouuseingoalyouMUSTmeasureconsistentlyatallPRsandRECERTS
Oncedeemedrepetitiveinnaturedifficulttoshowskilledneed
Clinicianmustshowuniqueskilledneedviaincreasedoverallfunctioninconjunctionwithreductionofcues
MedicarewillNOTALLOWcontinuedskilledneedforcuesalone
4/1/2016
19
GOALS/TREATMENT MEASURES
REALISTIC/LONGTERM/FUNCTIONAL Thereshouldbeanexpectationofmeasurablefunctionalimprovement.
Measureablecomponent(percentile)needstobeattachedtoallshortandlongtermgoals
Functionalcomponent(inorderto…)needstobeattachedtoallshortandlongtermgoals.
SUB‐TASKfunctionalimpairmentareasinordertomeasuremorespecificchangesinfunction
LONG TERM VERSUS SHORT TERM GOALS LONGTERMGOALSshouldreflectthehighestlevelofdesiredfunctionanticipatedupondischarge.Inmostcaseswillbereflectiveofpatient’spriorleveloffunction(PLOF)
SHORTTERMOBJECTIVESarethesteppingstones,targetedspecificareasthatareusedtoincreaseoverallfunctioninordertoachieveLTGs
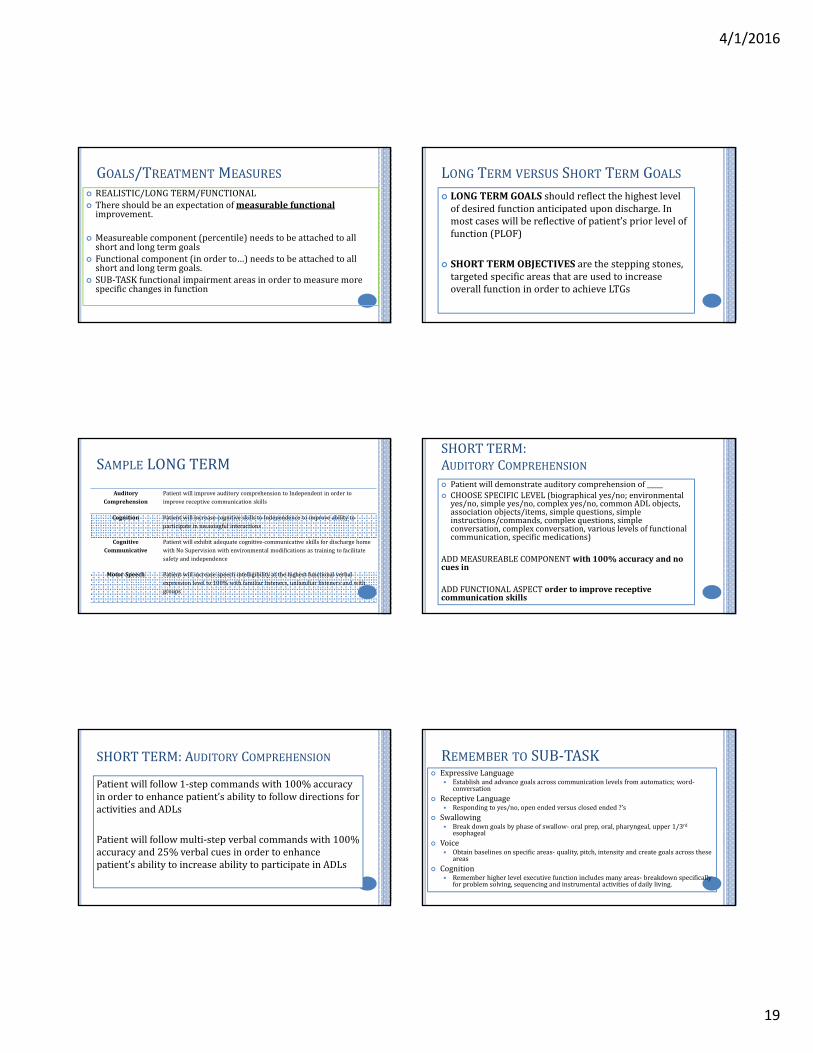
SAMPLE LONGTERM
AuditoryComprehension
PatientwillimproveauditorycomprehensiontoIndependentinordertoimprovereceptivecommunicationskills
Cognition PatientwillincreasecognitiveskillstoIndependencetoimproveabilitytoparticipateinmeaningfulinteractions
CognitiveCommunicative
Patientwillexhibitadequatecognitive‐communicativeskillsfordischargehomewithNoSupervisionwithenvironmentalmodificationsastrainingtofacilitatesafetyandindependence
MotorSpeech Patientwillincreasespeechintelligibilityatthehighestfunctionalverbalexpressionlevelto100%withfamiliarlisteners,unfamiliarlistenersandwithgroups
SHORTTERM:AUDITORY COMPREHENSION Patientwilldemonstrateauditorycomprehensionof_____ CHOOSESPECIFICLEVEL(biographicalyes/no;environmentalyes/no,simpleyes/no,complexyes/no,commonADLobjects,associationobjects/items,simplequestions,simpleinstructions/commands,complexquestions,simpleconversation,complexconversation,variouslevelsoffunctionalcommunication,specificmedications)
ADDMEASUREABLECOMPONENTwith100%accuracyandnocuesin
ADDFUNCTIONALASPECTordertoimprovereceptivecommunicationskills
SHORTTERM:AUDITORY COMPREHENSION
Patientwillfollow1‐stepcommandswith100%accuracyinordertoenhancepatient’sabilitytofollowdirectionsforactivitiesandADLs
Patientwillfollowmulti‐stepverbalcommandswith100%accuracyand25%verbalcuesinordertoenhancepatient’sabilitytoincreaseabilitytoparticipateinADLs
ExpressiveLanguage Establishandadvancegoalsacrosscommunicationlevelsfromautomatics;word‐
conversation
ReceptiveLanguage Respondingtoyes/no,openendedversusclosedended?’s
Swallowing Breakdowngoalsbyphaseofswallow‐ oralprep,oral,pharyngeal,upper1/3rd
esophageal
Voice Obtainbaselinesonspecificareas‐ quality,pitch,intensityandcreategoalsacrossthese
areas
Cognition Rememberhigherlevelexecutivefunctionincludesmanyareas‐ breakdownspecifically
forproblemsolving,sequencingandinstrumentalactivitiesofdailyliving.
REMEMBER TO SUB‐TASK

4/1/2016
20
PARTII:PUTTINGTHEPIECESTOGETHER
DOCUMENTATION& GOALBUILDING
Regulations Incorporatinginto DocumentationThepatient'smedicalrecordmustcontaindocumentationthatfullysupportsthemedicalnecessityforservicesincludedwithinthisLCD.(See"IndicationsandLimitationsofCoverage.")
ProperlydocumentdeclinesfromPLOFwhenmeasuringbaselines;utilize“summary”sectionofevaluationtoindividualizePOCandpaintofclearpictureofhowdeclineshaveaffectedqualityoflife;properlycode“diagnosesthatindicatemedicalnecessity”
Documentationincludes,butisnotlimitedto,relevantmedicalhistory,physicalexamination, resultsofpertinentdiagnostictestsorprocedures.
Utilize“Reasonfor Referral”,“PMH”sectionofevaluationtodocument“relevantmedicalhistory”(e.g.documentingpresenceofParkinson’sDiseasewhenprovidingtreatmentforhypokineticdysarthria)
Notonlyshoulddocumentationdescribetheconditionofthepatientthatnecessitatestheskilledinterventionofthespeech‐languagepathologist,butshouldalsoreportclinicaljudgmentanddescribetheskillednature ofthetreatment.
Clinicianshoulduseskillsettoanalyze patient’sresponsetointerventionsonadailybasisadjustingPOCtomeetpatient’sneedsutilizingtheirbest“clinicaljudgment”(e.g.“Basedonpatient’sdecreasedattentionspanfortaskcompletioningroupsettingswithotherresidents,STwillinitiatetargetstoaddressimpairmentsinordertopromotefollowthroughofnewlylearnedskillsintosettingsoutsideofST”)Rememberdefinitionof“skilled”servicesrequiretheuniqueskillsetofatherapist
Regulations Incorporatinginto Documentation
Documentingtheskilledcomponentsofactivitieswillassistinsupportingthattheservicesaremedicallynecessary.
Includes, treatmentplandevelopment,strategies, hierarchyoftasks,cueinghat,analysisofprogress,establishmentofspecificgoals,selectionandinitialtrainingofAAC,patientandfamilytraining
Documentationofspeechlanguageservices,likeothertherapyservices,mustbeobjective,clear,concise,andmustshowevidenceofthebeneficiary'sprogress inmeetingtreatmentgoals.
Utilize builderstoappropriatelycreatetargetsforareasofimpairmentonevaluation
Documentation intheclinicalrecordmustbedescriptive,clearlyrelatedtofunctionality,andcomplementandcorrelatewithotherdisciplines.
Descriptive‐ DocumentallskilledinterventionsinTENS,PR,utilizeAddendumasneeded.
Clearlyrelated toFunctionality‐ tie “inorderto”portiontogoals
Regulations IncorporatingintoDocumentation
Medicalnecessitymaynotbeestablishedifthereisconflictingdocumentationbetweendisciplinesorwidelyfluctuatingabilitiesindicatinganunstablecondition.
Keepopen linesofcommunicationbetweeninterdisciplinarystaff
Priorleveloffunctioningmustbedocumentedandconsideredinthepatient'streatmentplan,toestablishreasonablegoalsforthepatient'spresentcondition.
Always documentpriorleveloffunctionforareasthatwillbetargetedduringplanofcare;thismayrequirecontactingPOA,familymembersinordertoensureaccuratemeasure
Statementssuchas"mildlyimpairedtomoderatelyimpaired"or"fairplustogoodminus"donotoffersufficientobjectiveandmeasurableinformationtosupportprogressandmayresultindenialofservicesasnotmedicallynecessary.
Effectivelyutilizegoalbuilderssystemtomeasureshorttermtargetsviauseofpercentilestiedtofunction.USE
1. Patientwillexhibitfunctionalcause/effectproblemsolvingskills100%ofattemptsand25%verbalcuesinordertofacilitatedecisionmakingskillscare/needs.VERSUS
2. PatientwillperformfunctionalproblemsolvingtaskswithIndependence
4/1/2016
21
Regulations Incorporatinginto Documentation
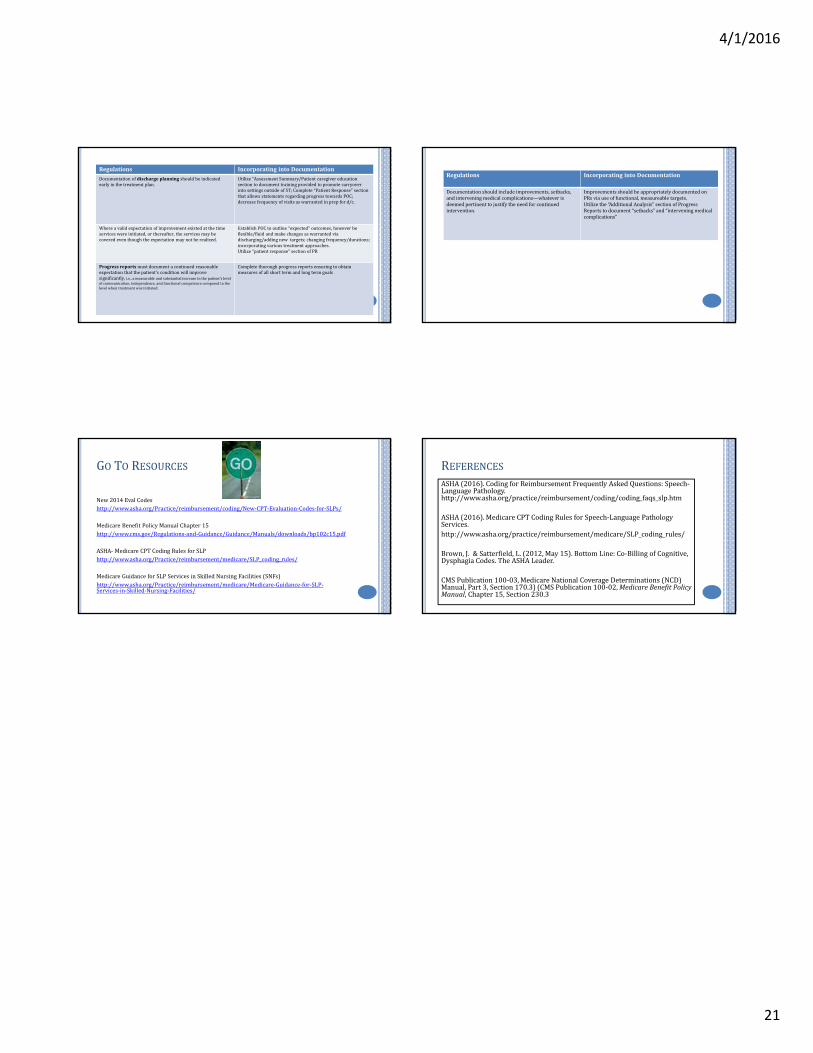
Documentationofdischargeplanningshouldbeindicatedearlyinthetreatmentplan.
Utilize“AssessmentSummary/PatientcaregivereducationsectiontodocumenttrainingprovidedtopromotecarryoverintosettingsoutsideofST;Complete“PatientResponse”sectionthat allowsstatementsregardingprogresstowardsPOC;decreasefrequencyofvisitsaswarrantedinprepford/c.
Whereavalidexpectationofimprovementexistedatthetimeserviceswereinitiated,orthereafter,theservicesmaybecoveredeventhoughtheexpectationmaynotberealized.
EstablishPOCto outline“expected”outcomes,howeverbeflexible/fluidandmakechangesaswarrantedviadischarging/addingnewtargets;changingfrequency/durations;incorporatingvarioustreatmentapproaches.Utilize“patientresponse”sectionofPR
Progressreportsmustdocumentacontinuedreasonableexpectationthatthepatient'sconditionwillimprovesignificantly,i.e.,ameasurableandsubstantialincreaseinthepatient'slevelofcommunication,independence,andfunctionalcompetencecomparedtothelevelwhentreatmentwasinitiated.
Completethorough progressreportsensuringtoobtainmeasuresofallshorttermandlongtermgoals
Regulations IncorporatingintoDocumentation
Documentationshouldincludeimprovements,setbacks,andinterveningmedicalcomplications—whateverisdeemedpertinenttojustifytheneedforcontinuedintervention.
Improvementsshouldbeappropriately documentedonPRsviauseoffunctional,measureabletargets.Utilize the“AdditionalAnalysis”sectionofProgressReportstodocument“setbacks”and“interveningmedicalcomplications”
GO TO RESOURCES
New2014Eval Codeshttp://www.asha.org/Practice/reimbursement/coding/New‐CPT‐Evaluation‐Codes‐for‐SLPs/
MedicareBenefitPolicyManualChapter15http://www.cms.gov/Regulations‐and‐Guidance/Guidance/Manuals/downloads/bp102c15.pdf
ASHA‐ MedicareCPTCodingRulesforSLPhttp://www.asha.org/Practice/reimbursement/medicare/SLP_coding_rules/
MedicareGuidanceforSLPServicesinSkilledNursingFacilities(SNFs)http://www.asha.org/Practice/reimbursement/medicare/Medicare‐Guidance‐for‐SLP‐Services‐in‐Skilled‐Nursing‐Facilities/
REFERENCESASHA(2016).CodingforReimbursementFrequentlyAskedQuestions:Speech‐LanguagePathology.http://www.asha.org/practice/reimbursement/coding/coding_faqs_slp.htm
ASHA(2016).MedicareCPTCodingRulesforSpeech‐LanguagePathologyServices.http://www.asha.org/practice/reimbursement/medicare/SLP_coding_rules/
Brown,J. & Satterfield,L.(2012,May15).BottomLine:Co‐BillingofCognitive,DysphagiaCodes.TheASHALeader.
CMSPublication100‐03,MedicareNationalCoverageDeterminations(NCD)Manual,Part3,Section170.3)(CMSPublication100‐02,MedicareBenefitPolicyManual,Chapter15,Section230.3


















