Kidney-Bone and Beyond: An Academic Career - UCLA CTSI · Normal Metabolic Pathway. LIVER . KIDNEY...
47
Kidney-Bone and Beyond: An Academic Career Isidro B. Salusky, M.D. Distinguished Professor of Pediatrics Chief, Division of Pediatric Nephrology Director, Clinical Translational Research Center Associate Dean of Clinical Research David Geffen School of Medicine at UCLA
Transcript of Kidney-Bone and Beyond: An Academic Career - UCLA CTSI · Normal Metabolic Pathway. LIVER . KIDNEY...

Kidney-Bone and Beyond: An Academic Career
Isidro B. Salusky, M.D. Distinguished Professor of Pediatrics
Chief, Division of Pediatric Nephrology Director, Clinical Translational Research Center
Associate Dean of Clinical Research David Geffen School of Medicine at UCLA

Holick MF, Lancet 6:357, 2001

With Hectorol® (doxercalciferol) Therapy
HO 25 (OH)D2
OH
HO VITAMIN D2
LIVER KIDNEY
OH
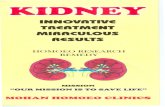
Normal Metabolic Pathway
LIVER KIDNEY FAILURE
In Kidney Failure
No Active Vitamin D Hormone
LIVER
Active Vitamin D Hormone HO 25 (OH)D2
HO 1,25 D2
OH
OH
HO VITAMIN D2
HO HECTOROL
OH
HO
HO
1.24 D2 Minor Active Vitamin D Hormone
OH
HO
OH
1.25 D2 Major Active Vitamin D Hormone
OH

Feedback Loops in SHPT
Ca = calcium; CVD = cardiovascular disease; P = phosphorus. Courtesy of Kevin Martin, MB, BCh.
↑ PTH
Bone Disease Fractures Bone pain
Marrow fibrosis Erythropoietin resistance
↑ Serum P ↓1,25D Calcitriol
Renal Failure
↑ PTH
Systemic Toxicity CVD
Hypertension Inflammation Calcification
Immunological
↓25D
↓ Ca++
Decreased Vitamin D Receptors and Ca-Sensing Receptors

Progression to Renal Failure
Normal Diffuse
Nodular Hyperplasia
Adenomatous Hyperplasia
Early Nodular
Progressive loss of kidney function
VDR Expression
CaSR Expression
Partial 1,25(OH)2D resistance
Progressive loss of 1,25(OH)2D has a profound effect on the structure and function of the parathyroid glands
1α-Hydroxylase
Murayama A, Takeyama K, Kitanaka S, et al. Endocrinology. 1999;140(5):2224-2231; Fukagawa M, Yi H, Fukuda N, et al. Artif Organs. 1995;19(12):1210-1214; Satomura K, Seino Y, Yamaoka K, et al. Kidney Int. 1988; 34:712–716.
Alteration of Parathyroid Gland Function

Spectrum of Renal Osteodystrophy
Normal bone formation Mild
Adynamic
Osteomalacia
PTH
Al+3
Mixed lesion
Osteitis fibrosa
Calcium, Vitamin D
High turnover Low turnover Vascular Calcification Process





Therapeutic Options for the Treatment of Renal Osteodystrophy
Phosphate Binders Active Vitamin D Analogues
Calcimimetic Drugs
Cinacalcet
Oxacalcitrol - Japan Paracalcitol - USA Stage 5 Doxercalciferol - USA Stage 3-5 Aluminum
Ca-Salts

Salusky IB et al NEJM 1990

Change in Plasma Al levels During the Course of the Study
Salusky IB et al NEJM 1990

Change in Plasma Aluminum Levels after DFO

A
Therapeutic Options for the Treatment of Renal Osteodystrophy
Phosphate Binders Active Vitamin D Analogues
Calcimimetic Drugs
Cinacalcet
Oxacalcitrol - Japan Paracalcitol - USA Stage 5 Doxercalciferol - USA Stage 3-5 Sevelamer:
Ca free – Metal Free Lanthanum Ca: Ca free - Metal +

Decreased Vitamin D Receptors
Decreased Ca-Sensing Receptors
Parathyroid Glands
Increased PTH Secretion
Hypocalcemia
Reduced Renal Mass
Decreased Serum 1,25(OH)2D
(Active Vitamin D Calcitriol)
Increased Serum Phosphate
Reduced Kidney Function and SHPT
National Kidney Foundation. Am J Kidney Dis. 2003;42:S1-S201. Cheng S, et al. Ther Clin Risk Manag. 2006;2:297-301.

Progression of CKD and Indices of Bone Metabolism
Martinez I et al. NDT S-11 3:22-28, 1996, Walters et al, D&I, 31: 735, 2002

Clinical Features of Childhood ROD
Height < -2 SD 153 (61.9%) Clinical manifestations of bone disease 91 (36.8%) Deformities 63 (25.5%) Pathological fractures 33 (13.4%) Aseptic bone necrosis 32 (13.0%) Mild disabling bone disease 26 (10.5%) Severe disabling bone disease 18 (7.3%) Invalidating bone disease (all) 44 (17.8%)
Groothoff JW KI 63 (2003) 266–275

STUDY DESIGN
Calcitriol
+
CaCO3
Calcitriol
+
Sevelamer 1-α D2
+
CaCO3
1-α D2
+
Sevelamer

500
3500
2500
1500
Bon
e Fo
rmat
ion
Rat
e (u
m2 /m
m2 /d
ay)
1 α(OH)D2 + CaCO3
1,25(OH)2D3 + CaCO3
1 α(OH)D2 + Sevelamer
1,25(OH)2D3 + Sevelamer
Effects of Therapy on Bone Turnover
6000
Initial
Final
* * *
*
* p<0.001
Wesseling K. et al KI 2010

Bone Gene Expression in Calcified Plaque
Bostrom K et al JCI 1993

Extra-Skeletal Calcification in Chronic Renal Failure
Courtesy of Kevin Martin, M.D.

Lumen
Intimal Atherosclerotic Plaque


(Giachelli et al 2004)
Process of Vascular Calcification

Coronary Artery Calcification in Young Dialysis Patients
0.1
1
10
100
1000
10000
0 5 10 15 20 25 30 35 Age (years)
Cal
cific
atio
n Sc
ore*
N=39
*Determined by EBT. Goodman WG, et al. N Engl J Med. 2000;342:1478-1483.
Calcification scores doubled in patients with positive initial scan when rescanned at 20 months

Risk Factors Associated With Increased Risk for Cardiac Calcification in Young Dialysis Patients
* Modifiable. Serum calcium was not significant. Goodman WG, et al. N Engl J Med. 2000;342:1478-1483.
Coronary No Calcification Calcification Factor (n=14) (n=25) P Value
Ca from 6456 ± 4278 3325 ± 1490 0.02 calcium binders (mg/day)*
Serum P (mg/dL) 6.9 ± 0.9 6.3 ± 1.2 0.06
Ca × P product (mg2/dL2)* 65.0 ± 10.6 56.4 ± 12.7 0.04
Age (years) 26 ± 3 15 ± 5 <0.001
Mean duration of dialysis (years) 14 ± 5 4 ± 4 <0.001

Risk of Cardiovascular Calcification Is Increased in Dialysis Patients
*Determined by EBT. CAD = coronary artery disease; CV = cardiovascular. †Rumberger JA, et al. Mayo Clin Proc. 1999;74:243-252. Braun J, et al. Am J Kidney Dis. 1996;27:394-401.
0
500
1000
1500
2000
2500
28-39 40-49 50-59 60-69 Age (years)
Mea
n C
oron
ary
Arte
ry
Cal
cium
Sco
re*
Nondialysis, No CAD (n = 22) Nondialysis, CAD (n = 80) Dialysis (n = 49)
Very high CV risk†

Coronary Artery Calcification by Presence of CKD and Diabetes: The Dallas Heart Study Population
Kramer et al. J Am Soc Nephrol. 2005;16:507-513.
Total
No CKD (n=2449)
Stage 1-2 CKD (n =170)
Stage 3-5 CKD (n = 41)
Non-Diabetic
No CKD (n = 2182)
Stage 1-2 CKD (n = 108)
Stage 3-5 CKD (n = 28)
Diabetic
No CKD (n = 267)
Stage 1-2 CKD (n = 62)
Stage 3-5 CKD (n = 13)
CAC≤10 CAC 11-100 CAC 101-400 CAC >400
0% 20% 40% 60% 80% 100%

Arterial Media Calcification in ESRD
London GM, et al. Nephrol Dial Transplant. 2003;18:1731-1740

Cardiovascular disease (CVD) mortality general population versus ESRD patients
Foley et al. Am J Kidney Dis. 1998;32:S112-S119
GP=general population
Age (years)
Annu
al C
VD m
orta
lity
(%)
0.001
0.01
0.1
1
10
100
25-34 35-44 45-54 55-64 65-74 75-84 >85
GP male GP female GP black GP white dialysis male dialysis female dialysis black dialysis white

Charles Nolan, MD

Vascular Calcification in Patients With CKD
Patients with Stage 5 CKD are at high risk for vascular calcification Vascular calcifications are present in almost 50% of patients with
stage 4 CKD and new dialysis patients Vascular calcification can be quantified Vascular calcification is associated with modifiable risk factors
– Ca intake from calcium-based binders – S-P, S-Ca and Ca × P product – Therapy with vitamin D
Vascular calcification results in arterial stiffening and increased pulse pressure and adynamic bone disease
Goodman WG, et al. N Engl J Med. 2000;342:1478-1483. Guérin AP, et al. Nephrol Dial Transplant. 2000;15:1014-1021. Ribeiro S, et al. Nephrol Dial Transplant. 1998;13:2037-2040. Raggi P, et al. J Am Coll Cardiol. 2002b;39:695-701.

New Definition of ROD: CKD-MBD
A systemic disorder of mineral and bone metabolism due to CKD manifested by either one or a combination of the following:
–Abnormalities of calcium, phosphorus, PTH, or
vitamin D metabolism
–Abnormalities in bone turnover, mineralization, volume, linear growth, or strength
–Vascular or other soft tissue calcification Moe et al Kidney International June 2006

A
Therapeutic Options for the Treatment of Renal Osteodystrophy
Phosphate Binders Active Vitamin D Analogues
Calcimimetic Drugs
Cinacalcet
Oxacalcitrol - Japan Paracalcitol - USA Stage 5 Doxercalciferol - USA Stage 3-5 Sevelamer:
Ca free – Metal Free Lanthanum Ca: Ca free - Metal +

FGF-23 and Rickets
ADHR (Autosomal Dominant Hypophosphatemic rickets) TIO (Tumor Induced Osteomalacia) XLH (X-linked hypophosphatemia) ARHP (Autosomal Recessive Hypophosphatemia)
Hypophosphatemia Renal phosphate wasting Low (or inappropriately normal) 1,25D Normal serum Ca levels Increased FGF-23 values

FGF-23 is Produced in Osteocytes and Regulates Phosphorus and Vitamin D
Osteoblast Osteocyte
DMP-1
MEPE-ASARM
PHEX
FGF-23
1,25(OH)2D Pi
Dietary animals + humans + CKD
Pituitary Choroid
DCT PCT
Klotho

OB OC
BONE MARROW
OCY
BONE OSTEOID
OCY
Traditional Bone Histomorphometry

Connections between blood vessels and osteocyte-lacunocanaliculi
Feng JQ. et al. Curr Opin.Nephrol.Hypertens. 18:285, 2009
Novel Regulators of Phosphate and Bone Metabolism
MARKER
Phex Early and late osteocytes
Phosphate metabolism
OF45/MEPE Late osteoblast through osteocytes
Inhibitor of bone formation/regulator of phosphate metabolism
DMPI Early and mature osteocytes
Sclerostin Late embedded osteocyte
Inhibitor of bone formation
FGF23 Early and mature osteocytes
Induces hypophosphatemia
Phosphate metabolism and mineralization
EXPRESSION FUNCTION

Increased Serum Pi, PTH and FGF23 by GRF in 447 CKiD Children
GFR (ml/min/1.73 m2)
Perc
enta
ge
Portale A et al CJASN 2013

Bone FGF-23 Expression (50x)
Healthy Control CKD (Stage 2)
Pereira RC et al Bone 2009 in press

Bone DMP1 Expression (200x)
Healthy Control CKD (Stage 2)
Pereira RC et al Bone 2009 in press

FGF23 Associated with LVH in Patients with CKD
(Faul C et al. JCI 2012)

cFGF-23 Quartiles and Mortality in Dialysis Patients (Gutierrez et al. NEJM 2008)

Temporal aspects of disordered mineral metabolism in CKD
Anal
yte
conc
entr
atio
n
>10,000
1000
90 60
30 4 0 >90 75 60 45 30 15 0 3 6 >12
GFR (mL/min/1.73 m2)
Time post-transplant (months)
1,25D (pg/mL)
cFGF-23 (RU/mL)
1 2 3
4
Dialysis
Wolf M. J Am Soc Nephrol 2010;21. [Epub ahead of print] cFGF-23, C-terminal Fibroblast Growth Factor-23
PTH (pg/mL)
Normal PTH range
P (mg/dL)
Normal P range
1. Increased FGF-23 is the earliest alteration in mineral
metabolism in CKD
2. Gradually increasing FGF-23 levels cause early
decline in 1,25D levels 3 .This frees PTH from
feedback inhibition, leading to SHPT
4. All these changes occur long before increases in
serum P levels are evident

Wolf, J Am Soc Nephrol 2010

UCLA Renata Pereira, Ph.D., Pediatrics
Joel Hernandez M.D., Pediatrics
Barbara Gales, R.N., Pediatrics
Jonathan Goldin, M.D.,Ph.D., Radiology
Robert Elashoff, Ph.D, Biomathematics
Katherine Wesseling, M.D., Pediatrics
Collaborators
Immutopics Jeffrey Lavigne Richard Zahranik Loma Linda Med. Ctr. Shobha Sahney, M.D. Mass. General Hospital Harald Jüppner, M.D.
Support: NIDDK, NCRR