Keynote: Proven Strategies to Advance Integrated Care in the Latino Community
27
Sea Mar Community Health Centers Presents 9th Annual Latino Health Forum Proven Strategies to Advance Integrated Care in the Latino Community Anna Ratzliff, MD, PhD Assistant Professor Associate Director for Education, Division of Integrated Care & Public Health Department of Psychiatry & Behavioral Sciences University of Washington
-
Upload
sea-mar-community-health-centers -
Category
Health & Medicine
-
view
41 -
download
1
Transcript of Keynote: Proven Strategies to Advance Integrated Care in the Latino Community

Sea Mar Community Health Centers Presents9th Annual Latino Health Forum
Proven Strategies to Advance Integrated Care in the Latino Community
Anna Ratzliff, MD, PhDAssistant Professor
Associate Director for Education, Division of Integrated Care & Public HealthDepartment of Psychiatry & Behavioral Sciences
University of Washington
Disclosures
• Consulting Psychiatrist Contract, Community Health Plan of Washington
• Supported from contracts and grants to the AIMS Center at the University of Washington

Daniel

Mental health disorders are common – who gets treatment?

The other 9 patients. No Treatment Primary Care Provider
Mental Health Provider
Wang et al 2005

Disparities in Depression Care for Minority
Populations• Worse access to mental health
treatment1
• Less likely to be identified2
• Less likely to receive antidepressant medications 3
• Have worse outcomes 4
1- Miranda et al. Am J Psychiatry. 2008 Sep;165(9):1102-8. 2- Borowsky et al J Gen Intern Med. 2000 Jun;15(6):381-8.3- Miranda J, Cooper L. J Gen Intern Med 2004; 19: 120-6.4- Van Voorhees et al Med Care Res Rev. 2007 Oct;64(5 Suppl):157S-94S.

Why not just refer?
½ do not follow through
2 visit mean
Grembowski, Martin et al. 2002 Simon, Ding et al. 2012

Why not just refer?
Thomas KC et al, 2009
1 in 5: unmet need for non-prescribers96%: unmet need for prescribers

Is there a better way?Yes - Collaborative Care!
http://aims.uw.edu/daniels-story-introduction-collaborative-care

Principle 1: Patient Centered Team Care
PCP
Patient BH CareManager
Psychiatric Consultant
CoreProgram
New Roles
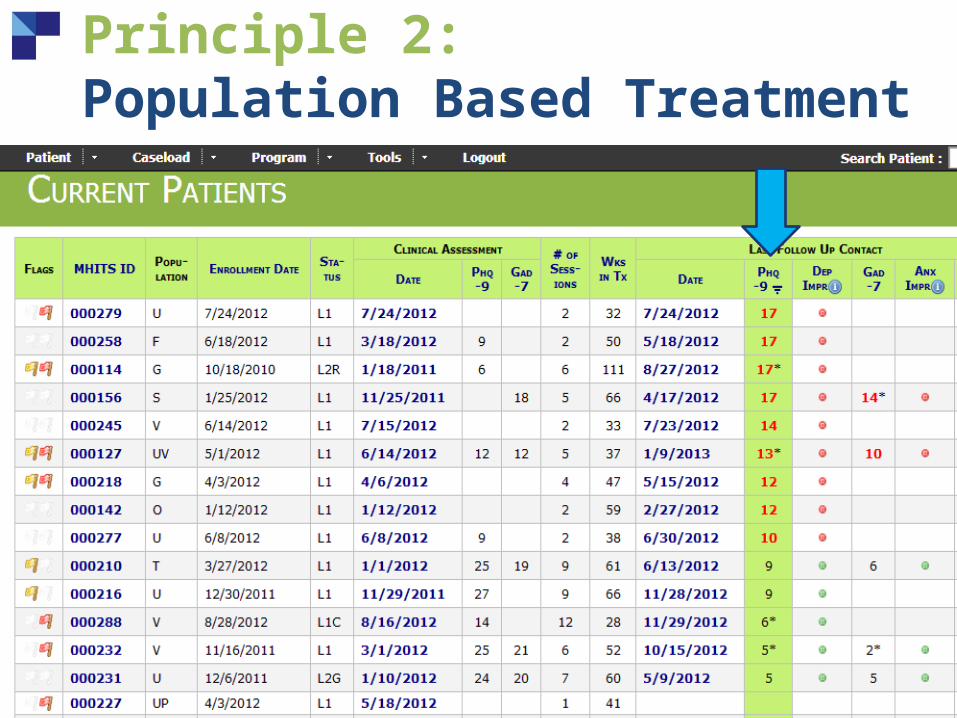
Principle 2: Population Based Treatment

Principle 3: Measurement Based Treatment To Target

Principle 4: Evidence-Based Treatment
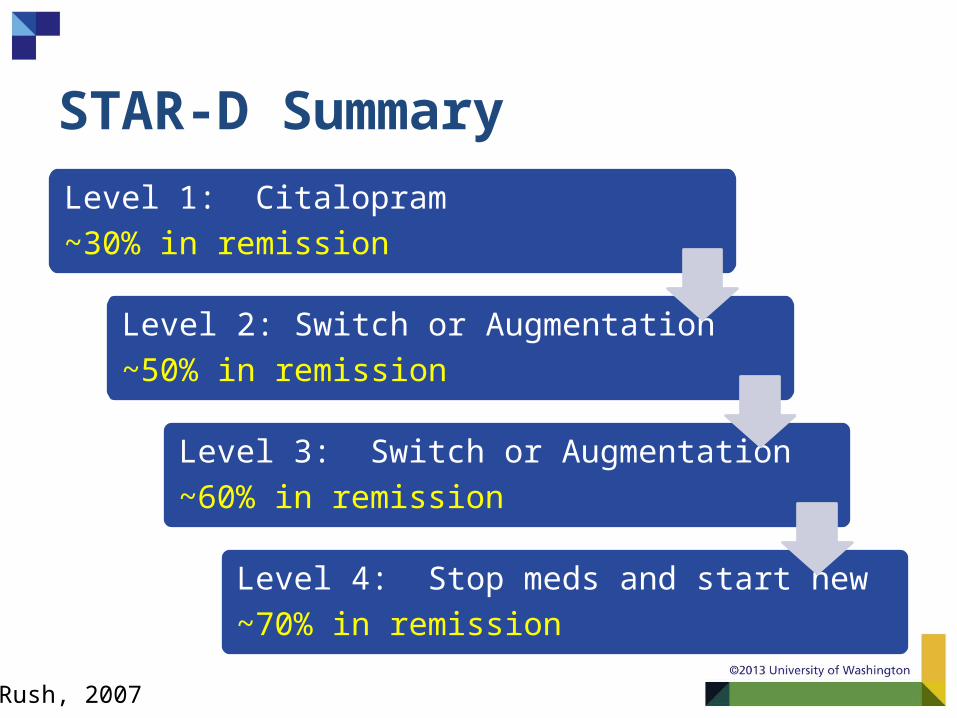
STAR-D Summary
Level 1: Citalopram ~30% in remission
Level 2: Switch or Augmentation ~50% in remission
Level 3: Switch or Augmentation ~60% in remission
Level 4: Stop meds and start new~70% in remission
Rush, 2007

Principle 5: Accountable Care

Pay-for-performance cuts median time to depression treatment response in half.
0.0
00.2
50.5
00.7
51.0
0
Estim
ate
d C
um
ula
tive P
rob
ab
lility
0 8 16 24 32 40 48 56 64 72 80 88 96 104 112 120 128 136
Weeks
Before P4P After P4P
Unützer et al. 2012.

Collaborative Care: The Research Evidence • Now over 80 Randomized Controlled Trials (RCTs)
• Meta analysis of collaborative care (CC) for depression in primary care (US and Europe)
Consistently more effective than usual care
• Since 2006, several additional RCTs in new populations and for other common mental disorders• Including anxiety disorders, PTSD
Archer, J. et al., 2012

Doubles Effectiveness of Care for Depression
%
Participating Organizations
50 % or greater improvement in depression at 12 months
Unützer et al., JAMA 2002; Psych Clin North America 2004
1 2 3 4 5 6 7 80
10
20
30
40
50
60
70 Usual Care IMPACT

White Black Latino0%
10%
20%
30%
40%
50%
60%
43%
54%
42%
19%23%
14%
IMPACT Care
Care as Usual
IMPACT Care BenefitsDisadvantaged
Populations
Arean et al. Medical Care, 2005
50 % or greater improvement in depression at 12 months

IMPACT: Summary1) Improved Outcomes:
• Less depression• Less physical pain• Better functioning• Higher quality of life
2) Greater patient and provider satisfaction
3) More cost-effective
“I got my life back” THE TRIPLE
AIM

MHIP: > 30,000 clients served across Washington State
•Funded by State of Washington and Public Health Seattle & King County (PHSKC)• Administered by Community Health Plan of Washington and PHSKC in partnership with the UW AIMS Center
2008Pilot initiated in King &
Pierce Counties
2009Expanded state-wide to over 100 CHCs and 30
CMHCs

MHIP High-Risk Mothers Program
• Low income women who are pregnant or parenting
• Community health clinics in King County• Identified by primary care provider with
mental health care need• Enrolled in Collaborative Care

MHIP High-Risk Mothers Program Outcomes
All Latina White Black Asian0
10
20
30
40
50
60
70% of Population with Depression
Improvement
Huang et al. Family Practice 2012 20:394-400.
What could you do?

Daniel’s Mom
“I believe it it’s made all the difference for him.”

Menu of Inspiration Options
Patient Centered Team
Population Based Care
Measurement-Based Treatment
to Target
Evidence-Based Treatment
Accountable Care
•Use patient centered goals.•Communication with other providers.
•Track patient outcomes.•Set a practice improvement goal.
•Participate in continuing ed.•Form a learning collaborative.
• Use screeners regularly.•Track patient goals regularly.
•Use a registry.•Lead efforts for implementation.

Acknowledgments:
Daniel and his familyAnnie McGuireAngel MathisRebecca SladekJürgen UnützerAIMS Center Staff
www.aims.uw.edu