Kenneth L. Woods, DO, MPH Disease Update WOODS.pdf · Lyme Disease 11 Spirochete Borrelia...
41
Kenneth L. Woods, DO, MPH Chair, Department of Medicine Medical Director, Infectious Disease Chair, Infection Control/Prevention Committee Chair, Antibiotic Stewardship Subcommittee Trinity Health System Steubenville, Ohio Email: [email protected]
Transcript of Kenneth L. Woods, DO, MPH Disease Update WOODS.pdf · Lyme Disease 11 Spirochete Borrelia...

Kenneth L. Woods, DO, MPH
Chair, Department of Medicine
Medical Director, Infectious Disease
Chair, Infection Control/Prevention Committee
Chair, Antibiotic Stewardship Subcommittee
Trinity Health System
Steubenville, Ohio
Email: [email protected]

Disclosures
Nothing to disclose.

Objectives
Discuss Lyme Disease and practical implications in
Primary Care.
Review diagnostic testing for Lyme Disease.
Discuss the management of Lyme Disease and
prevention/prophylaxis strategies.
Lyme Disease - Background
4
History:
First recognized in 1976, in Lyme, CT.
Recognized as spirochete from tick vector in 1982.
Spirochete bacterium Borrelia burgdorferi.
Ixodies scapularis (Blacklegged or deer tick) vector.
Horizontal vector with white footed mouse, white tailed
deer, chipmunks, squirrels. (humans are end host)
Most common vector borne disease in US.
Most common tick-borne disease in N. America & Europe.
6th most common reportable disease in US.
>40,000 cases / yr in US.
Lyme Disease
5
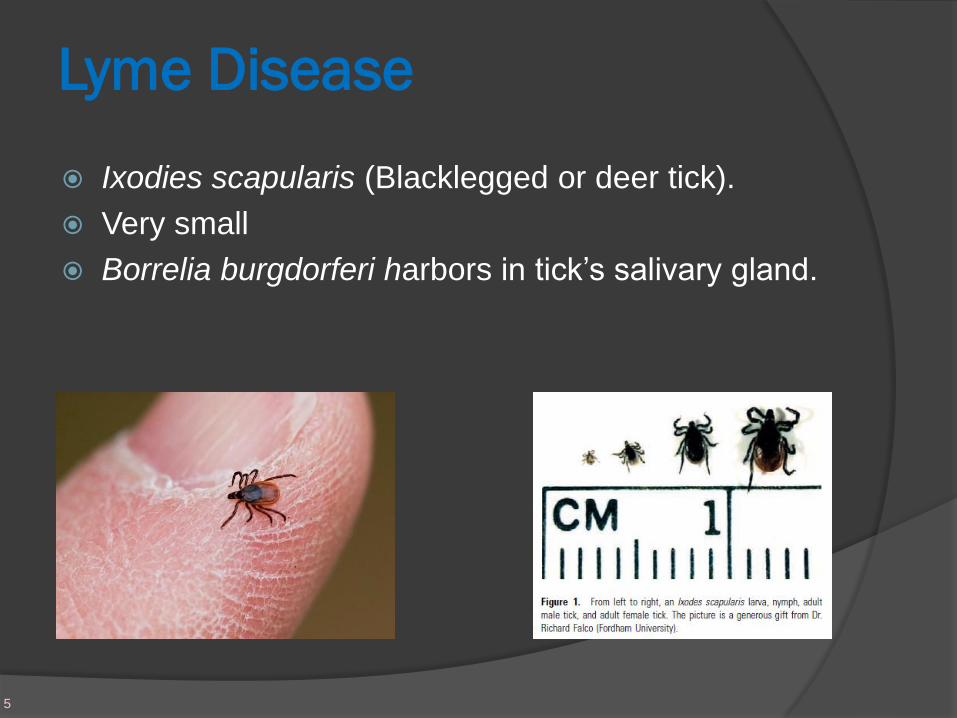
Ixodies scapularis (Blacklegged or deer tick).
Very small
Borrelia burgdorferi harbors in tick’s salivary gland.

Lyme Disease
6
CDC 2016 incidence map

Lyme Disease
7

Lyme Disease - seasonality
8
*CDC through 2016

Lyme Disease
9
Spirochete Borrelia burgdorferi.
Motile, corkscrew-shaped bacterium
Up to 11 flagella
Small linear chromosome
Grows best at 33 C, on Barbour-Stoenner-Kelly medium,
but rarely grown (poor sensitivity).
Giemsa or Wright stain.
Can stain weakly Gram negative.
Larger than most spirochetes.

Lyme Disease
10
Spirochete Borrelia burgdorferi.
Pathogenesis / Virulence factors:
Osp (outer surface protein) A-F.
Helps adapt to and survive different environment
between arthropod to mammal.
Decorin binding proteins that allow to bind to collagen
especially in heart, nervous system, and
joints/synovium.
Depends on host for nutritional requirements.
Incubation period 3-32 days.
Multiplies locally at site of inoculation.

Lyme Disease
11
Spirochete Borrelia burgdorferi
Dissemination takes days to weeks, but has been
recovered from bld, CSF, synovial fluid, myocardium,
retina, muscle, bone, spleen, liver, brain…
Affected tissues often show lymphocyte infiltration,
vasculitis, or hypervascular occlusion.
Can inactivate complement cascade.
Extensive antigenic variation/changes to minimize
immune recognition
IgG can take months to develop.
Increase in mononuclear cells in peripheral blood, IFN-γ
Host defense mostly via B-cell response, complement
fixation, and opsonization.
Lyme Disease
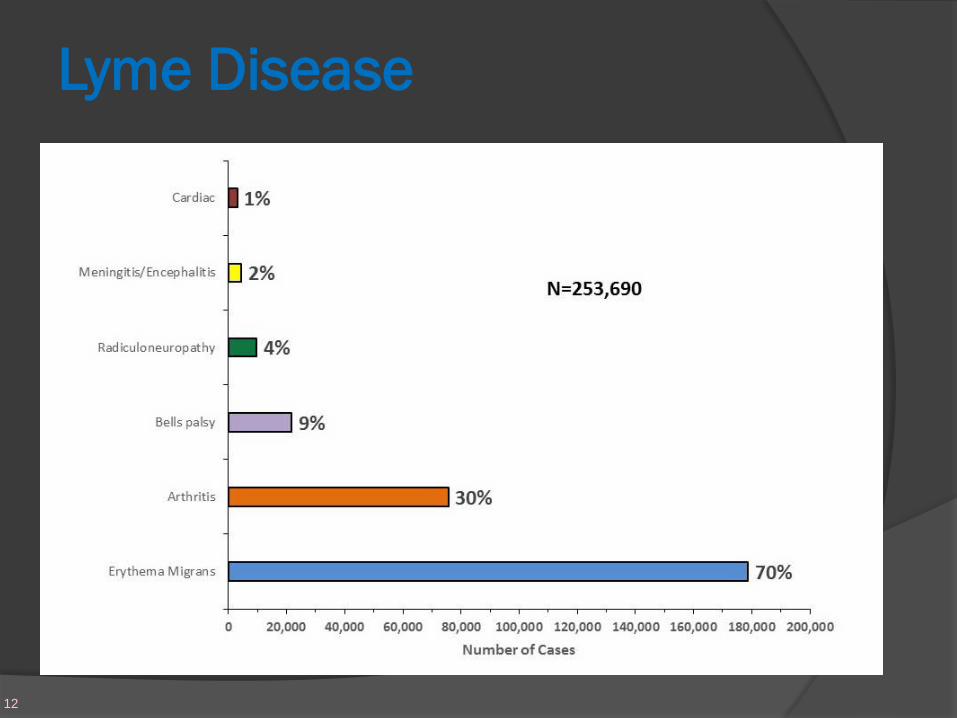
12

Lyme Disease – Stages
13
Three main stages:
1. Early/Localized:
Avg ~7 days after tick bite.
Erythema migrans rash in ~70-80%.
○ Most patients do not recall tick bite.
○ Mostly groin, thigh, axilla.
○ Starts without the center clear ring
○ Rash can be pruritic (rarely) or hot or even painful.
○ Rare to see EM on head/face – more common to be
linear streaking in the head/face region.
○ Can be multiple lesions.
Headache and joint aches common.

Lyme Disease
14
Erythema migrans
• Usually appears 7-14 days after tick attachment
(usually takes attachment >32h).
• Rare to be <5 cm diameter.
• Rare to occur <48 h from tick bite, and more likely
hypersensitivity reaction if occurs rapidly.

Lyme Disease – Stages
15
2. Disseminated/late infection:
Days to weeks after tick bite.
EM rash similar to early disease, but less prominent,
smaller, and lack indurated or clear center, can be
multiple skin lesions, malar rash, or urticaria.
Often this stage is where the malaise, myalgia, fatigue,
fevers, chills, conjunctivitis, lymphadenopathy develop.
Musculoskeletal pain (60%), headache/neck stiffness,
hepatitis, splenomegally, cough, testicular swelling,
hematuria, proteinuria.
Rare to get Lyme arthritis (<<10%) but mostly unilateral
knee.

Lyme Disease – Stages
16
2. Disseminated infection/Neuroborreliosis:
10-15% of untreated pts progress to neurological sx
(meningitis/encephalitis, cranial neuritis (esp CN-VII),
tingling or neuropathies, short term memory fx
CN-VII palsy does not equate to Neuroborreliosis.
Focal neuro sx/sx.
CSF shows lymphocytic pleocytosis.
Lyme Disease - Stages
17
2. Disseminated-Cardiac involvement/myocarditis:
○ 5-10% of untreated pts progress to cardiac sx with
classic finding of varying degree AV block and
myocarditis. (avg time 2 mo.).
○ ~54% have at least intermittent 3rd degree block.
○ 3:1 Male:female dominance.
○ Pathology shows perivascular interstitial infiltration as
well as AV node infiltration.
○ Cardiac MRI associated with epicardial contrast
enhancement (as opposed to subendothelial
enhancement with ACS/ischemic heart dis).

Lyme Disease - Stages
18
3. Late/persistent:
~60% of all patients.
Sx include myalgia/arthralgia/joint swelling, esp large
joints with knee #1.
Intermittent sx that usually resolved by 1-2 yrs.

Lyme Disease – Stages
19
Post Lyme syndrome – controversial.
Also called PTLDS (Post-treatment Lyme Disease
Syndrome).
Previously “chronic Lyme disease”.
Sx’s lasting >6 months.
>25% of patients will have sx’s >3 months after treatment.
Most common sx: HA/joint aches, fatigue, neuro-congnitive
disturbances.
Several studies looking at tissue/DNA/PCR/Culture without
evidence of active infection after abx (all were positive
before Abx treatment).

Lyme Disease
20
Transplacental transmission has been reported although
very rare (2 cases).
Co-infection is not uncommon, Anaplasma
phagocytophilum (Ehrlichiosis), Babesia microti (RBC
parasite).
Possibly as high as 40% in some areas are
coinfected.
Clues to co-infection are high leukocytosis or
leukopenia, thrombocytopenia, anemia, fever >48h
after treatment.

Lyme Disease
21
Diagnosis

Lyme Disease - Diagnosis
22
Early dx largely based on clinical basis.
Serology not recommended if EM rash.
Lyme Disease - Diagnosis
23
2-step lab testing algorithm (most labs automated).
1. EIA (enzyme immunoassay) for Lyme Ab.
○ IgM peaks 2-4 wks, normalizes 6-8 wks (?).
○ IgG peaks 4-6 months.
○ False + with Syphilis, RA, SLE, EBV, SBE reported.
2. +ELISA is followed by Western Blot.
○ WB IgM bands (2 for dx): 23, 39, 41 kDa.
○ WB IgG bands (5 for dx): 18, 23, 28, 30, 39, 41, 45,
58, 66, 93 kDa.
If neg EIA, no WB is needed.
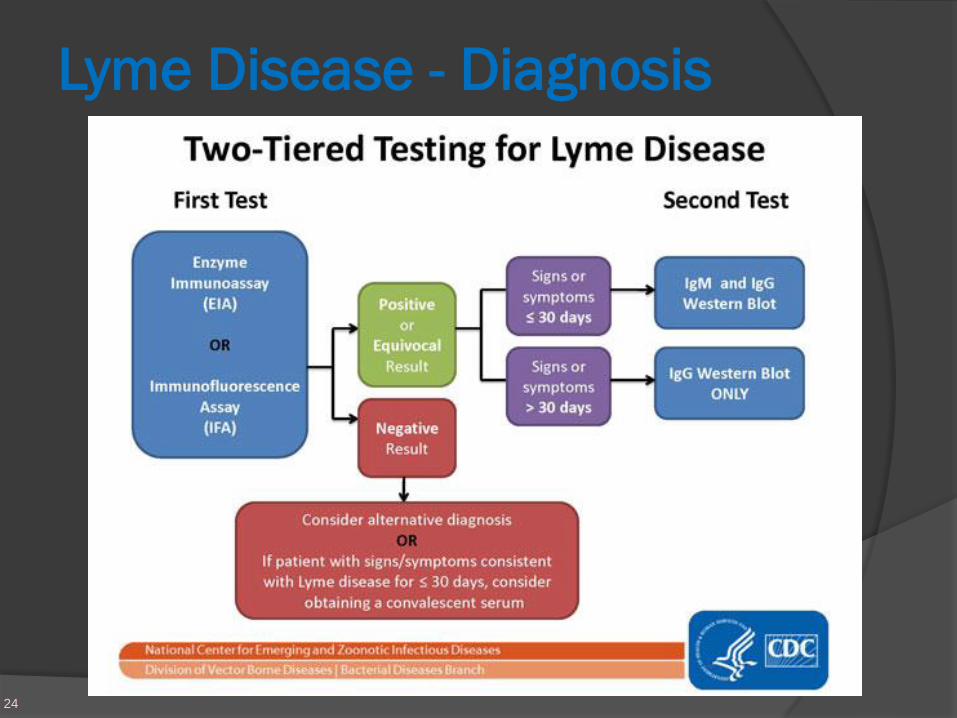
Lyme Disease - Diagnosis
24

Lyme Disease - Diagnosis
25
PCR is available.
○ Poor sensitivity for serum PCR or early/localized
disease.
○ Good sensitivity for organ level/invasive disease.
CSF, myocardial tissue, synovial fluid (superior to
culture).

Lyme Disease – Neuroborreliosis Dx
26
Should not rely on clinical sx/sx alone; guidelines
recommend if clinical suspicion perform CSF analysis
and only consider Neuroborreliosis dx if CSF supports.
Most common indication for LP is severe/prolonged
headache w/ positive Lyme serology/compatible sx.
CN-VII palsy does not equate to Neuroborreliosis.
Lyme CSF DNA by PCR (good sens/spec).
Lyme CSF Ab production (less sensitive unless very late
into course of disease where DNA rarely detected).
CSF: elev protein, >100 WBC, norm glucose.
Almost all CNS Lyme cases have positive serology.

Lyme Disease
27
Treatment

Lyme Disease - Treatment
28
IDSA and CDC Guidelines recommend treating based on
clinical findings if early disease.
Early disease (adults & children >8 y.o.):
Doxycycline 100 mg PO bid x 14d (BEST)
(10-21d acceptable)
Amoxicillin 500 mg PO tid x14-21d
Cefuroxime (Ceftin) 500 mg PO bid x14-21d
Early disease children <8 yo:
Amoxicillin 50 mg/kg/d divided TID x14-21d
Cefuroxime (Ceftin) 30 mg/kg/d divided BID x14-21d

Doxycycline Precautions
29
Given that Lyme disease is mostly seen in summer/sunny
months, MUST caution patients on PHOTOSENSITIVITY.
Relatively contraindicated if pregnant, breast feeding, or
age <8 y.o.
Higher rates of GI upset, minimized by taking with food.
Esophageal irritation reported, minimized with 6-8 oz H20
and remain upright x30 min after dose.

Lyme Disease – Treatment Pearls
30
~15% get Jarisch-Herxheimer-like reaction 1st 24h of Rx.
A lot of data on short courses of Doxycycline are equal
effectiveness so 21d no longer recommended w/o
neuro/cardiac/Lyme arthritis.
Longer durations have no benefit to reduce symptoms
but have increased adverse effects, mortality and other
complications.
Ceftriaxone not superior to PO’s but is effective.
CTX x1, then 10d doxy = 400% inc diarrhea. (IV not
better!)

Lyme Disease – Treatment Pearls
31
Azithromycin/clarithromycin less effective so avoid. Maybe
4th line options.
First generation cephalosporins, FQ’s, bactrim are all
ineffective.
Persistent/severe joint sx “can consider" additional 2 wks
of PO ATB’s, but not exclusively recommended.
No repeat ATB’s recommended if recurrent symptoms.
Recommend no treatment for seropositive patients that
are asymptomatic.
IgM/IgG can remain positive for years.

Lyme Disease – PLEASE trial
32
Persistent Lyme-Empiric Abx Study of Europe 2014.
Randomized, double-blind, placebo-controlled trial.
N=280 patients.
Followed through 26-wk post treatment.
Compared short vs. long duration abx (2 wk vs. 12 wk).
PLEASE trial (Persistent Lyme-Empiric Abx Study of Europe. BMC Infec Dis 2014, 14(543).
Berende A, et.al. Randomized Trial of Longer-Term Therapy for Symptoms Attributed to
Lyme Disease. NEJM. 2016, Vol 374(13): 1209-1220.

Lyme Disease – PLEASE trial
33
No differences in:
Quality of life scores (RAND-36).
Patient reported sx’s.
Neuropsychological assessment.
Objective fatigue measures/activity monitoring.
68% of patients reported at least 1 possible adverse drug
event.
Diarrhea 32.5% (note 1 episode of diarrhea counted).
Nausea 15.7%.
Rash 11%; Photosensitivity 6.8%.
Mucosal yeast infection 7.1%.
PLEASE trial (Persistent Lyme-Empiric Abx Study of Europe. BMC Infec Dis 2014, 14(543).
Berende A, et.al. Randomized Trial of Longer-Term Therapy for Symptoms Attributed to
Lyme Disease. NEJM. 2016, Vol 374(13): 1209-1220.

Lyme Disease – Treatment
34
Neuroborreliosis/CNS Lyme disease:
Ceftriaxone 2 gm IV daily for 14 days (historically)
(*newer evidence* or until clinical improvement, then
can consider complete 21d course with PO doxy).
PCN-G 24M units/day IV x14 days (normal renal fx).
Doxycycline 100-200 mg PO bid may be equivocal to IV
Ceftriaxone. IV Doxy should not be needed.
Steroids do not appear to add any benefit (CNS or CN-
VII palsy related Lyme disease)

Lyme Disease – Treatment
35
Lyme Myocarditis:
Temporary pacer often required, average duration
needed is 3 days – 6 wks.
Ceftriaxone 2gm IV daily or PCN-G 24m units/day IV x
14 days or until clinical improvement in heart block.
(very little data to support; no RCT’s)
Followed by Doxycycline 100 mg PO BID to finish 14-21
days total abx course.
Cardiac involvement usually reverses quickly with
treatment (3-7 days). However, 9+ deaths reported.

Lyme Disease – Treatment
36
Lyme arthritis:
Should be treated for up to 28 days w/ PO’s (same as early).
(Not arthralgia, but septic Lyme arthritis).
IV Abx compared to PO showed no different in outcome
other than increase adverse effects and cost.
Avoid intra-articular steroid injections (worsens
outcome).
NSAIDs recommended.
No recommendation on systemic steroids.
Related joint pain may persist for years (>5 yrs has
been reported)

Lyme Disease
37
Prevention
&
Prophylaxis

Lyme Disease – Prevention
38
Most useful prevention is avoiding exposure.
Decreased tick habitat.
Protective clothing (tight fitting, tucked shirts, pants tucked
into socks, etc.).
DEET based insect repellant.
Daily “tick checks”
Early and complete tick removal. If tick mouth parts not
fully removed from skin, topical disinfectant application
only.
Human Lyme disease vaccine 1999-2002 (not avail).

Lyme Disease – Prophylaxis
39
Routine abx prophylaxis or serology testing in absence of
disease (signs/symptoms) is not recommended.
No universal recommendation for post-tick bite
prophylactic ATB’s.
Can consider if: (must have ALL)
1. High endemic area with tick infection rate >20%,
2. Known I. scapularis tick attachment >36h.
3. Doxycyline not contraindicated, AND
4. Abx started within 72 hrs.
If all 4 of the above Doxycycline 200 mg PO x1 (for
adults/children age >8 y.o 4mg/kg max 200 mg).
No other abx recommended (only doxy).
Testing of ticks is NOT recommended (research only)

Berende A, et.al. Randomized Trial of Longer-Term Therapy for Symptoms
Attributed to Lyme Disease. NEJM. 2016, Vol 374(13): 1209-1220.
CDC Website (Accessed 10/2018): https://www.cdc.gov/lyme/index.html
Mandell’s Principles and Practice of Infectious Diseases. 8th ed. 2015.
Marks C et.al. Antibiotic Treatment for Chronic Lyme Disase-Say No to the
DRESS. JAMA 2016. Dec 1;176(12): 1745-1746
NIH Website (Accessed 10/2018): https://www.niaid.nih.gov/diseases-
conditions/lyme-disease
PLEASE trial (Persistent Lyme-Empiric Abx Study of Europe. BMC Infec Dis
2014, 14(543).
Wormser G, et.al. The Clinical Assessment, Treatment, Prevention of Lyme
Disease, HGA, and Babesiosis: Clinical Practice Guidelines by IDSA. CID
2016:43, 1089-1134.
References:

E-mail: [email protected]