
Kenneth E. Thorpe, Ph.D. Emory University The Carter Center Health Care Reform: Challenges And...
21
Kenneth E. Thorpe, Ph.D. Emory University The Carter Center Health Care Reform: Challenges And Opportunities for Behavioral Health November 5, 2009 1
-
Upload
abigayle-lindsay -
Category
Documents
-
view
214 -
download
1
Transcript of Kenneth E. Thorpe, Ph.D. Emory University The Carter Center Health Care Reform: Challenges And...

Kenneth E. Thorpe, Ph.D.Emory University
The Carter CenterHealth Care Reform: Challenges And Opportunities for Behavioral HealthNovember 5, 2009
1

• Intertwined issues—Value for health spending—Cost containment—Health security
• Policy options—Care coordination inside and outside the
traditional health system—Prevention—Payment reforms
• Evidence• Reform prospects
2

No care coordination in FFS Medicare 95% of spending in Medicare linked to
chronically ill patients Six chronic conditions (diabetes,
others) account for 40% of rise in Medicare spending—mainly conditions requiring drug and ambulatory care
High rates of preventable hospital admissions and readmissions
A third of the rise in spending traced to the doubling of obesity
3

Long-term savings Lifetime health spending for obese
seniors is 15%-40% than for normal-weight peers with no chronic disease
Near-term savings RCTs show savings potential of
>$10 billion/year in Medicare with existing care management protocols
4

Siloed care that does not integrate mental health, acute care, and chronic disease prevention, treatment, and management
Fragmentation 40% primary care docs in groups <4 More than ½ of people with serious chronic
conditions see >3 different physicians yearly Separation of prevention and treatment Outdated payment and delivery system
designed largely for acutely ill not chronically ill patients.
5

Prevention Health risk appraisal and personalized
care plan added to Medicare No cost sharing for USPSTF “disease
detection” screenings Care management-system reform
ACOs – accountable care organizations Medical home pilots
Payment reforms
6

Prevention and care management Identify key functions in successful models
that improve quality and reduce costs, such as: Coordinated care across providers and settings Transitional care Patient support, especially for medication
adherence Community-based care and support
Key: scaling and replication Federal investment ($30B)
7

8
Community Prevention
Hospital
HEALTH INFORMATION TECHNOLOGY
Outcome Metrics, Evaluation
Bundled Payments
Specialists
Specialists
Specialists

Targeting the right patients Medication and testing adherence Transitional care programs Close integration with the coordinating
provider practice Ability to link with and refer to effective
community-based interventions Real-time evaluation and information on
clinical markers with feedback
9

Medicare demos Integrated practices achieve better outcomes
and savings Savings up to 5% possible in current system
Penn transitional care RCTs 56% reduction in readmissions; 65% fewer
hospital days Average costs $4,845 lower
YMCA-DPP 11 lbs (~5%) weight loss; 58% diabetes Improved control of other CVD risk factors
10

Trust for America’s Health community-based interventions Short-term ROI 1:1 Longer-term ROI ~6:1
Value of HIT Improved care coordination and administrative
processes Properly implemented and widely adopted,
annual savings from efficiency alone could be $77 billion or more
Health and safety benefits could double savings
11

Medication adherence Adherence generally low: 50%-65% for common
chronic conditions such as hypertension and diabetes
Nonadherence is costly: ~$100 billion/year for hospitalizations alone
Proven strategies: patient education; improved dosing schedules; additional open clinic hours; improved communication between providers and patients
Adherence ROI: 7:1 for diabetes, 5.1:1 for hyperlipidemia, 3.98:1 for hypertension; overall healthcare spending 15% lower for CHF
12

Community-based prevention $10/person/year could yield more than $16
billion in medical cost savings annually within 5 years
Coordinated care Meta-analysis of chronic disease
management studies showed 36%-45% drop in readmissions; 35%-45% drop in total hospital costs; ROIs from 1.4 to 32.7; Medicare savings from reduced CHF readmissions of $424 million per year
13

Coordinated care Interventions for diabetes resulted
in $685-$950 drop in per patient per year costs; 9% drop in all-cause hospitalizations; 71% drop in ER/hospital utilization; 21% fewer total claims
Transitional care $25 billion investment in CHTs over
10 years could produce savings of $100 billion over the same period
14

Prevention is not a single intervention Interventions must be evidence-based
Growing body of research shows what works
Integrated prevention is based in both the community and the health system Primary, secondary, and tertiary prevention are all
essential
Payment reform is critical Incent prevention through payment revisions
15

State-level efforts pave the way Private sector is also innovating Senate bill released October 26 House bill introduced October 29
16

Expand the capacity of two independent, advisory task forces — the U.S. Preventive Services Task Force (USPSTF) and the Task Force on Community Preventive Services (TFCPS) — to undertake rigorous, systematic reviews of existing science
Invest in prevention research to expand the evidence base
Eliminate cost‐sharing on recommended preventive services delivered by Medicare, Medicaid, and public option insurance (or Health Insurance Exchange)
Deliver community preventive services Invest in state, territorial, and local public health
infrastructure Provide grants to implement TFCPS‐recommended services
17

Establish Prevention and Wellness Trust funded at $2.4 Billion in FY2010 and rising to $3.5 Billion in FY2014: $30 million in each of FY 2010-2014 to fund the activities
of the Clinical and Community Preventive Services Task Force.
$100 million in FY 2010 for prevention and wellness research and rising to $300 million in FY2014.
$1.1 billion in FY 2010 for community-based prevention and wellness services and rising to $1.6 billion in FY2014.
$800 million in FY2010 for core public health infrastructure and activities for state and local health departments rising to $1.3 Billion in FY2014.
$350 million in each of FY2010-2014 for core public health infrastructure and activities for CDC.
18

Mandates national public-private partnership for a prevention and health promotion outreach and education campaign
“Community Transformation” grants for implementation, evaluation, and dissemination of proven evidence-based community preventive health activities to reduce chronic disease rates, address health disparities, and develop a stronger evidence base of effective prevention
“Healthy Aging, Living Well” program to improve the health of the pre-Medicare-eligible population to help control chronic disease and reduce Medicare costs. Pilot programs would evaluate chronic disease risk factors,
conduct evidence-based public health interventions, and ensure that individuals identified with or at risk for chronic disease receive clinical treatment to reduce risk
Community Health Teams
19

Medicare pilots to test bundled payments
Value-based purchasing in Medicare to pay hospitals based on performance – focus on preventable readmissions
Care coordination – especially for “duals” – patients eligible for both Medicare and Medicaid
Comparative effectiveness research: focus on clinical services
20
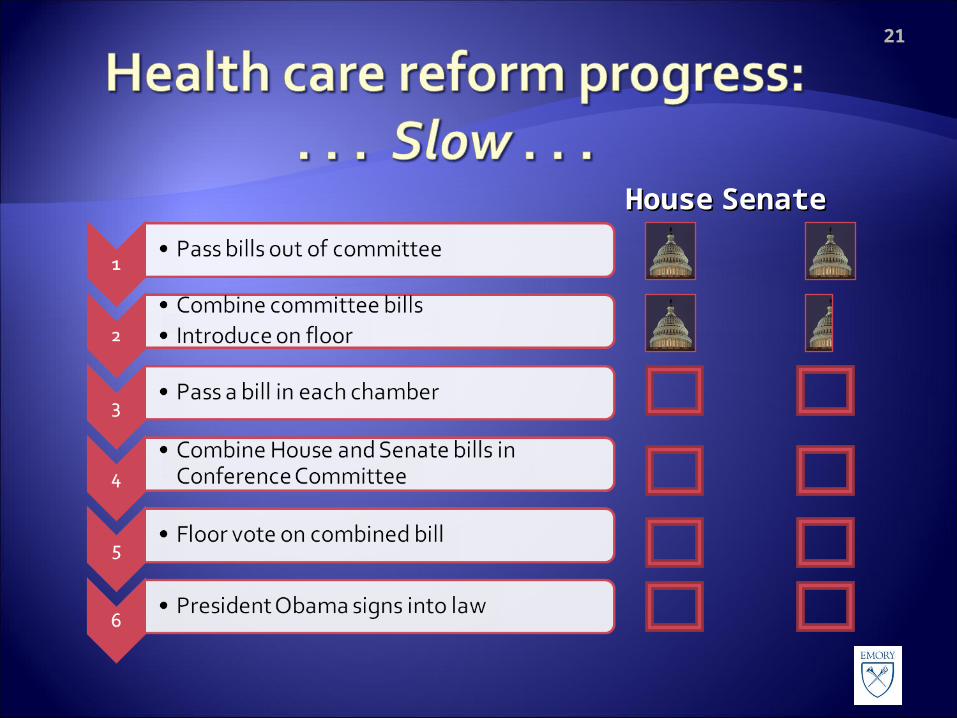
HouseHouse SenateSenate
21


















