Katie Flanagan - Malaria vaccines current status and challenges
22
Malaria vaccines: Current status and challenges A/Prof Katie Flanagan Clinical Associate Professor & Head of Infectious Diseases, Northern Tasmania Director of Systems Vaccinology Trial Centre, Clifford Craig Medical Research Trust, Tasmania Adjunct , Dept of Immunology and Pathology, Monash University, Melbourne
-
Upload
waidid -
Category
Health & Medicine
-
view
42 -
download
2
Transcript of Katie Flanagan - Malaria vaccines current status and challenges

Malaria vaccines: Current status and challenges
A/Prof Katie Flanagan
Clinical Associate Professor & Head of Infectious Diseases, Northern Tasmania
Director of Systems Vaccinology Trial Centre, Clifford Craig Medical Research Trust, Tasmania
Adjunct , Dept of Immunology and Pathology, Monash University, Melbourne

Cases 214 million cases in 2015
Incidence 37% decrease in incidence between 2000 and 2015
Mortality 60% decrease in deaths between 2000 and 2015 (>98% of deaths from P. falciparum)
Malaria elimination is now considered feasible

3.2 billion people at risk per year 200-300 million cases per year world wide ~0.5 million fatalities – mainly in children and pregnant women
Malaria poses a huge economic burden 1-6% of GDP
Control measures such as ITNs, spraying, prophylaxis, early diagnosis & Rx
o are not sufficient alone o failing due to insecticide resistance, drug resistant parasites o expensive (>$2.6 billion spent on malaria control in 2013)
A malaria vaccine would greatly assist in the drive to eradicate malaria from
the world since vaccines are considered the most cost-effective means of control, prevention, elimination, eradication of infectious diseases

0 !C- > F$4) !G' , ' 6&%4!H&94IC</ $4!" ' +<!2 ' , D4%!0 +%&D4+6!
Liver or Pre-erythrocytic
Stage
Blood Stage
Sexual Stage
Complex parasite with multiple life cycle stages making vaccine development challenging

From Barry & Arnott, Front Immunol 2014; 5(359): 4

Immune Response to Malaria Infection
From Crompton et al, Annu Rev Immunol 2014; 32: 157
Successful vaccine probably needs to induce cellular (CD4 and CD8 T cells) and Ab responses
Multi-stage vaccine preferable for inducing sterilising immunity

Crompton et al, Annu Rev Immunol 2014; 32: 157
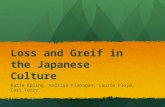
Acquired Natural Immunity Takes Years to Develop

Conway, Trends in Genomics 2015;31(2):97
Barry & Arnott, Front Immunol 2014;5(359):4

UK adults Phase I – safety, dose finding and immunogenicity UK adults Phase IIa – sporozoite challenge study (CHMI)
African adults Phase I – safety and immunogenicity African age de-escalation Phase I – safety, dose finding and
immunogenicity (2-5 years 5-12 months 10 weeks) African adults Phase IIb – efficacy (time to infection by blood film+ fever or
PCR)
African infants Phase I / IIb – efficacy (time to infection) African infants Phase I - EPI immunogenicity African infants Phase III – efficacy
File for license

From Conway, Trends in Genomics 2015;31(2):97

Regulatory requirements
Time
Certification
Testing each adjuvant/antigen to complete product development
Increasing inflexibility along the translational path
Costs
Large investment (RTS,S investment from GSK and BMGF $610 million)
Requires partnerships
Vaccine production costs high
Technological innovation/ QC commitment to a limited number of products
Risk aversion - old technologies (e.g. VLPs) preferred

Ouattara and Laurens, CID 2015;60:930

Consists of a fusion protein of pre-erythrocytic circumsporozoite protein (CS)
antigen repeat region, CS T cell epitopes and HBsAg
Hybrid particle vaccine in AS01B adjuvant produced by GSK
Only malaria vaccine to reach phase III clinical trials
Induces CD4 T cells but not CD8 T cells in humans
Strain/variant specific protection (consists of 1 of 10 natural variants of CS)
Kaslow and Biernaux. Vaccine 2015;33:7425

Efficacy against clinical malaria in phase III trials (to 14m post vaccination) 50.4% (95% CI 45.8-54.6) in 5-17 month old children (n=6,000)
30.1% (95% CI 23.6-36.1) in 6-12 week old infants (n=6,537)
This efficacy is too low for deployment in the field
Efficacy mediated by high titre anti-CS antibody responses
Kaslow & Biernaux. Vaccine 2015;33:7425

To facilitate malaria elimination it is estimated that a vaccine should induce >85% sterile protection for >6 months (Hoffman. Vaccine 2015;33:D13)
Kaslow & Biernaux. Vaccine 2015;33:7425

Potent T cell responses
Adenovirus Prime Modified Vaccinia Ankara (MVA) Boost
Main Ags - CS protein and thromobospondin related adhesion protein (TRAP) Inhibit sporozoite motility and hepatocyte invasion Prime-boost strategies with DNA and viral vector vaccines
US Navy
DNA prime, AdHu5 boost +/- AMA-1 Jenner Centre, Oxford, UK (Prof Adrian Hill)
Fowlpox prime, MVA boost with full-length CS DNA prime, MVA boost with full-length CS Chimp adenovirus prime (ChAd63), MVA boost with TRAP
Highly potent CD8 T cell responses and Abs Being tested in combination with RST,S
Disappointing results in challenge studies

It has long been known that injecting humans with irradiated sprorozoites
confers complete protection against malaria challenge
Hoffman et al. have shown 100% efficacy after 4-6 i.v. doses of 1.35x105 spz
(4 mosquitoes per dose)
Broad ranging immunity induced - Abs, CD4 and CD8 T cells, NK cells, γδ T
cells
Protection lasts >1 year (VE of 55% at 59 weeks)
Early efficacy correlates with antibody and γδ T cell responses
Later efficacy probably requires tissue resident CD8 T cells
Safe, well tolerated, meets regulatory standards
Feasibility concerns –
Large scale manufacture - new sporozoite culture techniques being developed
IV vaccination required
Stored in liquid N2
Attenuated sporozoites may revert to virulent forms or be under-attenuated

3 weeks
3 weeks 21-25 weeks 21-25 weeks 59 weeks
100% sterile protection against controlled human malaria infection at 59
weeks in n=5 subjects (f) (Ishizuka et al. Nat Med 2016;22(6):614)
Recently granted FDA fast track approval
Other whole parasite approaches are being pursued including sporozoites +
chemoprophylaxis, genetic and chemical attenuation

Beeson et al. FEMS Microbiol Rev
2016;40(3):343
Various blood stage vaccines are being tested in human clinical trials Target merozoites to inhibit RBC invasion Infection still occurs but is blocked at the blood stage Merozoites express multiple antigens so identifying the ideal target(s) is
challenging Leading targets include MSP1, MSP2, MSP3, AMA1, EBA175, PfRH5 Significant polymorphism of Ag targets Abs and CMI responses thought to be required for protection Human efficacy trials have been disappointing No in vitro assays or challenge models that provide correlates of protection in
human studies Live attenuated whole blood stage vaccines are being developed

Crompton et al, Ann Rev Immunol 2014;
32: 157
Also called SSM-VIMT – vaccines that target sexual, sporogenic, and /or
mosquito stage antigens to interrupt malaria transmission
Inhibit ookinite development in the mosquito midgut thereby blocking
transmission – do not prevent infection / clinical disease
A handful of antigenic targets currently being developed as vaccines
Humans produce Abs to Ags expressed during the human sexual stage &/or
mosquito life-cycle
Abs are ingested by the mosquito and prevent parasite development
Passive immunisation with monoclonal Abs also being explored
Challenges:
Expressing and purifying appropriately folded
target proteins
Low level Ab titres induced by current candidate
vaccines
Lack of assays for correlating efficacy in the field

TLRs, PRRs, PAMPs, inflammasome activators (Alum) Positive short term effects
Increase immunity; modulate type of immunity
Negative long term effects Pro-inflammatory Tregs
NSEs (sex differential)
Nanoparticle based vaccines: from VLPs to synthetic NPs Positive short and long-term effects Some can increase immunity without inflammation (or Treg) NSEs Beneficial NPs (PS, silver) ↑resistance to asthma and influenza

Despite >30 years of intense efforts we still don’t have an effective malaria
vaccine
The vaccine development pathway is very slow and very expensive
The parasite has multiple stages where it expresses different antigens and a
multistage and multi-antigen vaccine may be preferable
Most major antigenic sites are highly polymorphic (but do have conserved
regions) thus an ideal vaccine needs to be strain transcending
An ideal vaccine would induce Abs, CD4 and CD8 T cells
T cell inducing vaccines need to cover multiple HLA haplotypes to be effective
in different regions of the world
Models for surrogates of protection are lacking for human trials
Results of subunit vaccine studies have been disappointing
The whole sporozoite vaccine approach is highly promising but has several
logistic caveats