
June 2012, Vol 3, No 3
28
© 2012 Green Hill Healthcare Communications, LLC NAVIGATING PATIENTS ACROSS THE CONTINUUM OF CANCER CARE TM JUNE 2012 www.AONNonline.org VOL 3, NO 3 SURVIVORSHIP RESEARCH Problems and Process in a Study Design—Lessons Learned ORIGINAL RESEARCH Implementation of a Theory- Based, Nonclinical Patient Navigator Program to Address Barriers in an Urban Cancer Center Setting WEB SITE REVIEW www.PatientAdvocate.org PAF – Patient Advocate Foundation: Solving insurance and healthcare access problems since 1996
-
Upload
the-oncology-nurse -
Category
Documents
-
view
215 -
download
1
description
June 2012 issue of the Journal of Oncology Navigation & Survivorship
Transcript of June 2012, Vol 3, No 3
© 2012 Green Hill Healthcare Communications, LLC
NAVIGATING PATIENTS ACROSS THE CONTINUUM OF CANCER CARETM
JUNE 2012 www.AONNonline.org VOL 3, NO 3
SURVIVORSHIP RESEARCHProblems and Process in a StudyDesign—Lessons Learned
ORIGINAL RESEARCHImplementation of a Theory-Based, Nonclinical PatientNavigator Program to Address Barriers in an Urban Cancer Center Setting
WEB SITE REVIEWwww.PatientAdvocate.orgPAF – Patient AdvocateFoundation: Solving insurance and healthcare access problemssince 1996

The median age of patients treated in the VISTA§ trial was 71 years (range: 48-91).
N

Living Proof
INDICATION
CONTRAINDICATIONS
WARNINGS, PRECAUTIONS AND DRUG INTERACTIONS�
�
�
�
�
�
�
�
�
ADVERSE REACTIONS
Survival never gets old
VELCADE (bortezomib) Indication and Important Safety Information
VELCADE® (bortezomib) delivered >13-month overall survival advantage in combination with MP† vs MP alone for previously untreated multiple myeloma (median 56.4 vs 43.1 months‡; 60.1-month median follow-up§)
NOW APPROVED FOR SUBCUTANEOUS ADMINISTRATION*
SUBCUTANEOUS ADMINISTRATION*
NOW APPROVED FOR
SUBCUTANEOUS ADMINISTRATION*
NOW APPROVED FOR
SUBCUTANEOUS ADMINISTRATION*
Living Proof
Living Proof

Brief Summary
INDICATIONS:VELCADE® (bortezomib) for Injection is indicated for the treatment of patients with multiple myeloma. VELCADE is indicated for the treatment of patients with mantle cell lymphoma who have received at least 1 prior therapy.CONTRAINDICATIONS: VELCADE is contraindicated in patients with hypersensitivity to bortezomib, boron, or mannitol. VELCADE is contraindicated for intrathecal administration. WARNINGS AND PRECAUTIONS: VELCADE should be administered under the supervision of a physician experienced in the use of antineoplastic therapy. Complete blood counts (CBC) should be monitored frequently during treatment with VELCADE.Peripheral Neuropathy: VELCADE treatment causes a peripheral neuropathy that is predominantly sensory. However, cases of severe sensory and motor peripheral neuropathy have been reported. Patients with pre-existing symptoms (numbness, pain or a burning feeling in the feet or hands) and/or signs of peripheral neuropathy may experience worsening peripheral neuropathy (including ≥ Grade 3) during treatment with VELCADE. Patients should be monitored for symptoms of neuropathy, such as a burning sensation, hyperesthesia, hypoesthesia, paresthesia, discomfort, neuropathic pain or weakness. In the Phase 3 relapsed multiple myeloma trial comparing VELCADE subcutaneous vs. intravenous the incidence of Grade ≥ 2 peripheral neuropathy events was 24% for subcutaneous and 41% for intravenous. Grade ≥ 3 peripheral neuropathy occurred in 6% of patients in the subcutaneous treatment group, compared with 16% in the intravenous treatment group. Starting VELCADE subcutaneously may be considered for patients with pre-existing or at high risk of peripheral neuropathy.Patients experiencing new or worsening peripheral neuropathy during VELCADE therapy may benefit from a decrease in the dose and/or a less dose-intense schedule. In the single agent phase 3 relapsed multiple myeloma study of VELCADE vs. Dexamethasone following dose adjustments, improvement in or resolution of peripheral neuropathy was reported in 51% of patients with ≥ Grade 2 peripheral neuropathy in the relapsed multiple myeloma study. Improvement in or resolution of peripheral neuropathy was reported in 73% of patients who discontinued due to Grade 2 neuropathy or who had ≥ Grade 3 peripheral neuropathy in the phase 2 multiple myeloma studies. The long-term outcome of peripheral neuropathy has not been studied in mantle cell lymphoma.Hypotension: The incidence of hypotension (postural, orthostatic, and hypotension NOS) was 13%. These events are observed throughout therapy. Caution should be used when treating patients with a history of syncope, patients receiving medications known to be associated with hypotension, and patients who are dehydrated. Management of orthostatic/postural hypotension may include adjustment of antihypertensive medications, hydration, and administration of mineralocorticoids and/or sympathomimetics.Cardiac Disorders: Acute development or exacerbation of congestive heart failure and new onset of decreased left ventricular ejection fraction have been reported, including reports in patients with no risk factors for decreased left ventricular ejection fraction. Patients with risk factors for, or existing heart disease should be closely monitored. In the relapsed multiple myeloma study of VELCADE vs. dexamethasone, the incidence of any treatment-emergent cardiac disorder was 15% and 13% in the VELCADE and dexamethasone groups, respectively. The incidence of heart failure events (acute pulmonary edema, cardiac failure, congestive cardiac failure, cardiogenic shock, pulmonary edema) was similar in the VELCADE and dexamethasone groups, 5% and 4%, respectively. There have been isolated cases of QT-interval prolongation in clinical studies; causality has not been established.Pulmonary Disorders: There have been reports of acute diffuse infiltrative pulmonary disease of unknown etiology such as pneumonitis, interstitial pneumonia, lung infiltration and Acute Respiratory Distress Syndrome (ARDS) in patients receiving VELCADE. Some of these events have been fatal. In a clinical trial, the first two patients given high-dose cytarabine (2 g/m2 per day) by continuous infusion with daunorubicin and VELCADE for relapsed acute myelogenous leukemia died of ARDS early in the course of therapy. There have been reports of pulmonary hypertension associated with VELCADE administration in the absence of left heart failure or significant pulmonary disease. In the event of new or worsening cardiopulmonary symptoms, a prompt comprehensive diagnostic evaluation should be conducted.Reversible Posterior Leukoencephalopathy Syndrome (RPLS): There have been reports of RPLS in patients receiving VELCADE. RPLS is a rare, reversible, neurological disorder which can present with seizure, hypertension, headache, lethargy, confusion, blindness, and other visual and neurological disturbances. Brain imaging, preferably MRI (Magnetic Resonance Imaging), is used to confirm the diagnosis. In patients developing RPLS, discontinue VELCADE. The safety of reinitiating VELCADE therapy in patients previously experiencing RPLS is not known.Gastrointestinal Adverse Events: VELCADE treatment can cause nausea, diarrhea, constipation, and vomiting sometimes requiring use of antiemetic and antidiarrheal medications. Ileus can occur. Fluid and electrolyte replacement should be administered to prevent dehydration.Thrombocytopenia/Neutropenia: VELCADE is associated with thrombocytopenia and neutropenia that follow a cyclical pattern with nadirs occurring following the last dose of each cycle and typically recovering prior to initiation of the subsequent cycle. The cyclical pattern of platelet and neutrophil decreases and recovery remained consistent over the 8 cycles of twice weekly dosing, and there was no evidence of cumulative thrombocytopenia or neutropenia. The mean platelet count nadir measured was approximately 40% of baseline. The severity of thrombocytopenia was related to pretreatment platelet count. In the relapsed multiple myeloma study of VELCADE vs. dexamethasone, the incidence of significant bleeding events (≥Grade 3) was similar on both the VELCADE (4%) and dexamethasone (5%) arms. Platelet counts should be monitored prior to each dose of VELCADE. Patients experiencing thrombocytopenia may require change in the dose and schedule of VELCADE. There have been reports of gastrointestinal and intracerebral hemorrhage in association with VELCADE. Transfusions may be considered. The incidence of febrile neutropenia was <1%.Tumor Lysis Syndrome: Because VELCADE is a cytotoxic agent and can rapidly kill malignant cells, the complications of tumor lysis syndrome may occur. Patients at risk of tumor lysis syndrome are those with high tumor burden prior to treatment. These patients should be monitored closely and appropriate precautions taken.Hepatic Events: Cases of acute liver failure have been reported in patients receiving multiple concomitant medications and with serious underlying medical conditions. Other reported hepatic events include increases in liver enzymes, hyperbilirubinemia, and hepatitis. Such changes may be reversible upon discontinuation of VELCADE. There is limited re-challenge information in these patients.Hepatic Impairment: Bortezomib is metabolized by liver enzymes. Bortezomib exposure is increased in patients with moderate or severe hepatic impairment; these patients should be treated with VELCADE at reduced starting doses and closely monitored for toxicities.Use in Pregnancy: Pregnancy Category D. Women of childbearing potential should avoid becoming pregnant while being treated with VELCADE. Bortezomib administered to rabbits during organogenesis at a dose approximately 0.5 times the clinical dose of 1.3 mg/m2 based on body surface area caused post-implantation loss and a decreased number of live fetuses.
ADVERSE EVENT DATA: Safety data from phase 2 and 3 studies of single-agent VELCADE (bortezomib) 1.3 mg/m2/dose administered intravenously twice weekly for 2 weeks followed by a 10-day rest period in 1163 patients with previously treated multiple myeloma (N=1008, not including the phase 3, VELCADE plus DOXIL® [doxorubicin HCI liposome injection] study) and previously treated mantle cell lymphoma (N=155) were integrated and tabulated. In these studies, the safety profile of VELCADE was similar in patients with multiple myeloma and mantle cell lymphoma.In the integrated analysis, the most commonly reported adverse events were asthenic conditions (including fatigue, malaise, and weakness); (64%), nausea (55%), diarrhea (52%), constipation (41%), peripheral neuropathy NEC (including peripheral sensory neuropathy and peripheral neuropathy aggravated); (39%), thrombocytopenia and appetite decreased (including anorexia); (each 36%), pyrexia (34%), vomiting (33%), anemia (29%), edema (23%), headache, paresthesia and dysesthesia (each 22%), dyspnea (21%), cough and insomnia (each 20%), rash (18%), arthralgia (17%), neutropenia and dizziness (excluding vertigo); (each 17%), pain in limb and abdominal pain (each 15%), bone pain (14%), back pain and hypotension (each 13%), herpes zoster, nasopharyngitis, upper respiratory tract infection, myalgia and pneumonia (each 12%), muscle cramps (11%), and dehydration and anxiety (each 10%). Twenty percent (20%) of patients experienced at least 1 episode of ≥Grade 4 toxicity, most commonly thrombocytopenia (5%) and neutropenia (3%). A total of 50% of patients experienced serious adverse events (SAEs) during the studies. The most commonly reported SAEs included pneumonia (7%), pyrexia (6%), diarrhea (5%), vomiting (4%), and nausea, dehydration, dyspnea and thrombocytopenia (each 3%).In the phase 3 VELCADE + melphalan and prednisone study in previously untreated multiple myeloma, the safety profile of VELCADE administered intravenously in combination with melphalan/prednisone is consistent with the known safety profiles of both VELCADE and melphalan/prednisone. The most commonly reported adverse events in this study (VELCADE+melphalan/prednisone vs melphalan/prednisone) were thrombocytopenia (52% vs 47%), neutropenia (49% vs 46%), nausea (48% vs 28%), peripheral neuropathy (47% vs 5%), diarrhea (46% vs 17%), anemia (43% vs 55%), constipation (37% vs 16%), neuralgia (36% vs 1%), leukopenia (33% vs 30%), vomiting (33% vs 16%), pyrexia (29% vs 19%), fatigue (29% vs 26%), lymphopenia (24% vs 17%), anorexia (23% vs 10%), asthenia (21% vs 18%), cough (21% vs 13%), insomnia (20% vs 13%), edema peripheral (20% vs 10%), rash (19% vs 7%), back pain (17% vs 18%), pneumonia (16% vs 11%), dizziness (16% vs 11%), dyspnea (15% vs 13%), headache (14% vs 10%), pain in extremity (14% vs 9%), abdominal pain (14% vs 7%), paresthesia (13% vs 4%), herpes zoster (13% vs 4%), bronchitis (13% vs 8%), hypokalemia (13% vs 7%), hypertension (13% vs 7%), abdominal pain upper (12% vs 9%), hypotension (12% vs 3%), dyspepsia (11% vs 7%), nasopharyngitis (11% vs 8%), bone pain (11% vs 10%), arthralgia (11% vs 15%) and pruritus (10% vs 5%).In the phase 3 VELCADE subcutaneous vs. intravenous study in relapsed multiple myeloma, safety data were similar between the two treatment groups. The most commonly reported adverse events in this study were peripheral neuropathy NEC (38% vs 53%), anemia (36% vs 35%), thrombocytopenia (35% vs 36%), neutropenia (29% vs 27%), diarrhea (24% vs 36%), neuralgia (24% vs 23%), leukopenia (20% vs 22%), pyrexia (19% vs 16%), nausea (18% vs 19%), asthenia (16% vs 19%), weight decreased (15% vs 3%), constipation (14% vs 15%), back pain (14% vs 11%), fatigue (12% vs 20%), vomiting (12% vs 16%), insomnia (12% vs 11%), herpes zoster (11% vs 9%), decreased appetite (10% vs 9%), hypertension (10% vs 4%), dyspnea (7% vs 12%), pain in extremities (5% vs 11%), abdominal pain and headache (each 3% vs 11%), abdominal pain upper (2% vs 11%). The incidence of serious adverse events was similar for the subcutaneous treatment group (36%) and the intravenous treatment group (35%). The most commonly reported SAEs were pneumonia (6%) and pyrexia (3%) in the subcutaneous treatment group and pneumonia (7%), diarrhea (4%), peripheral sensory neuropathy (3%) and renal failure (3%) in the intravenous treatment group.DRUG INTERACTIONS: Bortezomib is a substrate of cytochrome P450 enzyme 3A4, 2C19 and 1A2. Co-administration of ketoconazole, a strong CYP3A4 inhibitor, increased the exposure of bortezomib by 35% in 12 patients. Therefore, patients should be closely monitored when given bortezomib in combination with strong CYP3A4 inhibitors (e.g. ketoconazole, ritonavir). Co-administration of omeprazole, a strong inhibitor of CYP2C19, had no effect on the exposure of bortezomib in 17 patients. Co-administration of rifampin, a strong CYP3A4 inducer, is expected to decrease the exposure of bortezomib by at least 45%. Because the drug interaction study (n=6) was not designed to exert the maximum effect of rifampin on bortezomib PK, decreases greater than 45% may occur. Efficacy may be reduced when VELCADE is used in combination with strong CYP3A4 inducers; therefore, concomitant use of strong CYP3A4 inducers is not recommended in patients receiving VELCADE. St. John’s Wort (Hypericum perforatum) may decrease bortezomib exposure unpredictably and should be avoided. Co-administration of dexamethasone, a weak CYP3A4 inducer, had no effect on the exposure of bortezomib in 7 patients. Co-administration of melphalan-prednisone increased the exposure of bortezomib by 17% in 21 patients. However, this increase is unlikely to be clinically relevant.USE IN SPECIFIC POPULATIONS:Nursing Mothers: It is not known whether bortezomib is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from VELCADE, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.Pediatric Use: The safety and effectiveness of VELCADE in children has not been established.Geriatric Use: No overall differences in safety or effectiveness were observed between patients ≥age 65 and younger patients receiving VELCADE; but greater sensitivity of some older individuals cannot be ruled out.Patients with Renal Impairment: The pharmacokinetics of VELCADE are not influenced by the degree of renal impairment. Therefore, dosing adjustments of VELCADE are not necessary for patients with renal insufficiency. Since dialysis may reduce VELCADE concentrations, VELCADE should be administered after the dialysis procedure. For information concerning dosing of melphalan in patients with renal impairment, see manufacturer’s prescribing information.Patients with Hepatic Impairment: The exposure of bortezomib is increased in patients with moderate and severe hepatic impairment. Starting dose should be reduced in those patients.Patients with Diabetes: During clinical trials, hypoglycemia and hyperglycemia were reported in diabetic patients receiving oral hypoglycemics. Patients on oral antidiabetic agents receiving VELCADE treatment may require close monitoring of their blood glucose levels and adjustment of the dose of their antidiabetic medication.Please see full Prescribing Information for VELCADE at VELCADEHCP.com.
VELCADE, MILLENNIUM and are registered trademarks of Millennium Pharmaceuticals, Inc. Other trademarks are property of their respective owners.
Millennium Pharmaceuticals, Inc., Cambridge, MA 02139 Copyright © 2012, Millennium Pharmaceuticals, Inc.All rights reserved. Printed in USA V-12-0151 4/12
10:21 AM

PUBLISHING STAFFSENIOR VICE PRESIDENT, SALES & MARKETING
Philip [email protected]
PUBLISHERJohn W. Hennessy
DIRECTOR CLIENT SERVICESJack Iannaccone
EDITORIAL DIRECTORKristin Siyahian
MANAGING EDITORJim Scelfo
EDITORIAL ASSISTANTJennifer Brandt
SENIOR COPY EDITORRosemary Hansen
PRODUCTION MANAGERStephanie Laudien
QUALITY CONTROL DIRECTORBarbara Marino
BUSINESS MANAGERBlanche Marchitto
CIRCULATION [email protected]
Journal of Oncology Navigation & Survivorship, ISSN 2166-0999 (print); ISSN 2166-0980 (online), is published 6 timesa year by Green Hill Healthcare Communications, LLC,241 Forsgate Drive, Suite 205C, Monroe Twp, NJ 08831.Telephone: 732.656.7935. Fax: 732.656.7938. Copy right©2012 by Green Hill Health care Com muni cations, LLC.All rights reserved. Journal of Oncology Navigation &Survivorship logo is a registered trademark of Green HillHealthcare Communications, LLC. No part of this publica-tion may be reproduced or transmitted in any form or by anymeans now or hereafter known, electronic or mechanical,including photocopy, recording, or any informational stor-age and retrieval system, without written permission fromthe publisher. Printed in the United States of America.
EDITORIAL CORRESPONDENCE should be ad dressed to MANAGING EDITOR, Journal of OncologyNavigation & Survivorship (JONS), 241 Forsgate Drive, Suite205C, Monroe Twp, NJ 08831. E-mail: [email protected] SUBSCRIPTION RATES: United States and pos-sessions: individuals, $50.00; institutions, $90.00; single issues,$5.00. Orders will be billed at individual rate until proof of sta-tus is confirmed. Prices are subject to change without notice.Correspondence regarding permission to reprint all or part ofany article published in this journal should be addressed toREPRINT PERMISSIONS DEPART MENT, Green HillHealthcare Communications, LLC, 241 Forsgate Drive, Suite205C, Monroe Twp, NJ 08831. The ideas and opinionsexpressed in JONS do not necessarily reflect those of the edito-rial board, the editorial director, or the publisher. Publication ofan advertisement or other product mention in JONS should notbe construed as an endorsement of the product or the manufac-turer’s claims. Readers are encouraged to contact the manufac-turer with questions about the features or limitations of theproducts mentioned. Neither the editorial board nor the pub-lisher assumes any responsibility for any injury and/or damageto persons or property arising out of or related to any use of thematerial contained in this periodical. The reader is advised tocheck the appropriate medical literature and the product infor-mation currently provided by the manufacturer of each drug tobe administered to verify the dosage, the method and durationof administration, or contraindications. It is the responsibility ofthe treating physician or other healthcare professional, relyingon independent experience and knowledge of the patient, todetermine drug dosages and the best treatment for the patient.Every effort has been made to check generic and trade names,and to verify dosages. The ultimate responsibility, however, lieswith the prescribing physician. Please convey any errors to theeditorial director.
ABOUT THE COVERPurgatoryOil by a Healthcare ProfessionalTexas
Artwork from the Lilly Oncology On Canvas: Expressions of a Cancer JourneyArt Competition (www.LillyOncologyOnCanvas.com).
JUNE 2012 • VOL 3, NO 3TABLE OF CONTENTS
SURVIVORSHIP RESEARCH
8 Problems and Process in a Study Design—Lessons LearnedBy Carol Guarnieri, RN, MSN, FNP-C, AOCNS; Patrice Welsh Benjamin, RN, MA, OCN; Melanie O’Hara, RN, MSN, OCN; Marlene Miller, RN, MSN, CORLN; Lindsay Thomas, RN, MSN, OCN;Maria Bautista, MS, ANP, CGRN; Sally Kazilek, RN, MSN, OCN; Melanie Brewer, DNSc, RN, FNP-BC
ORIGINAL RESEARCH
14 Implementation of a Theory-Based, NonclinicalPatient Navigator Program to Address Barriers in anUrban Cancer Center SettingBy Linda Fleisher, PhD, MPH; Suzanne M. Miller, PhD; Danielle Crookes, MPH; Venk Kandadai, MPH; Kuang Yi Wen, PhD;Rachel E. Slamon, BS; Jeanne Chaivous, MSW
WEB SITE REVIEW
26 www.PatientAdvocate.orgPAF – Patient Advocate Foundation: Solving insurance and healthcare access problems since 1996By Lillie D. Shockney, RN, BS, MAS
AONNONLINE.ORG JOURNAL OF ONCOLOGY NAVIGATION & SURVIVORSHIP 5

Editor-in-ChiefLillie D. Shockney, RN, BS, MASUniversity Distinguished Service AssociateProfessor of Breast CancerDepts of Surgery and OncologyAdministrative Director, Johns HopkinsBreast Clinical ProgramsAdministrative Director, Johns HopkinsCancer Survivorship ProgramsAssociate Professor, JHU School ofMedicine, Depts of Surgery &Gynecology and ObstetricsAssociate Professor, JHU School of [email protected]
Section EditorsBreast CancerSharon Gentry, RN, MSN, AOCN, CBCNBreast Health NavigatorDerrick L. Davis Forsyth Regional Cancer Center
Prostate CancerFrank delaRama, RN, MS, AOCNSClinical Nurse SpecialistOncology/GenomicsCancer Care ClinicPalo Alto Medical Foundation
Healthcare Disparities Linda Fleisher, PhD, MPHAssistant Vice PresidentOffice of Health Communications & Health DisparitiesAssistant ProfessorCancer Prevention & ControlFox Chase Cancer Center
Health Promotion and OutreachIyaad Majed Hasan, MSN, FNPDirector and Nurse PractitionerSurvivorship Clinic and ProgramCleveland ClinicTaussig Cancer Center
AONN Research CommitteeMarcy Poletti, RN, MSN Program Administrator, Oncology ServicesWake Forest University Baptist Medical Center
Elaine Sein, RN, BSN, OCN, CBCNSenior Project ManagerFox Chase Cancer Center Partners
Penny Widmaier, RN, MSNNurse NavigatorBotsford Cancer Center
MISSION STATEMENTThe Journal of Oncology Navi gation &Survivorship (JONS) promotes reliance on evi-dence-based practices in navigating patients withcancer and their caregivers through diagnosis,treatment, and survivorship. JONS also seeks tostrengthen the role of nurse and patient navigatorsin cancer care by serving as a platform for theseprofessionals to disseminate original research find-ings, exchange best practices, and find support fortheir growing community.
Dear Colleague,
T he summer months are often a period of time when there is less happening inthe “cancer awareness” arena. For this reason, I want to challenge everyone toget the creative juices flowing and think about some new and innovative ways
to raise awareness and truly inspire consumers to take better care of themselves bygetting the cancer screening tests they need. This might mean changing the way outreach is traditionally done. Is there a way to
reach the right populations of people at risk other than setting up a booth at a healthfair? Recently, I thought about this regarding colorectal cancer screenings. (Let’s faceit, no one wants to walk over to a colorectal cancer education booth!) So rather thanexpecting people to come to us, I recommended that we go to them—beginning withour own Hopkins employees. Two wonderful willing people here got into costumes—a polyp costume (a modified tomato costume available online will do) and a police-woman’s uniform—and went into various departments as the “polyp police”!!Handcuffed together, the policewoman showed employees seated at their desk thatshe had “caught this one, but it had already gone bad” and recommended that theyread the criteria for who needs colonoscopy screening done and call the (new)Hopkins employee scheduling number to get scheduled. It was fun, engaging, andcaused lots of employees to talk about colon cancer!!And the polyp police will be making the rounds every month to a different department
here to spread the word. We don’t want to do this just during national colorectal cancerawareness month, right? People sure need to be aware during months other than March.So write to us and let us know some of your innovative ideas you have already
implemented that others, including me, can learn from. Also share with us newprograms that you will be launching soon. I’m working next on breast cancerawareness and lung cancer awareness and have some hopefully clever ways toinspire people to get screening mammograms as well as give up the cancer sticks. Got any ideas yet? Let me know! g
With best regards,
Lillie D. Shockney, RN, BS, MASEditor-in-Chief
INSPIRE AWARENESSTHROUGH INNOVATIVEIDEAS
6 JUNE 2012 • VOLUME 3, ISSUE 3 AONNONLINE.ORG
LETTERS FROM LILLIE

Journal of Oncology
The Official Journal of the Academy of Oncology Nurse NavigatorsNAVIGATION & SURVIVORSHIP
®
®
�"�2)/�$�0!��(2�+/!-.%)(-���)/.�.$!�Journal of Oncology Navigation & Survivorship��
*'!�-!� )(.� .��,%-.%(��%2�$%�(��.�[email protected]
www.AONNonline.org/manuscripts The ONLY journal focused on patient navigation
and survivorship care in oncology patients
aSubmitManuscript!
JONSAsize71311
� �� �� � �� �

It is estimated that nearly 12 million individualsin the United States are living with cancer.1Cancer survivorship is defined as the experience
of living with, through, and beyond cancer forboth patients and the people in their lives whoare impacted by the diagnosis. Survivorshipencompasses the physical, psychological, emo-tional, social, spiritual, and economic aspects oflife.2 Psychological distress, impaired organ func-tion, sexual dysfunction, cosmetic changes, limi-tations in mobility, communication issues, anddecreased cognition are among some of the prob-lems faced by many cancer survivors. The eco-
nomic impact of a cancer diagnosis can be anadditional burden to cancer survivors throughincreased out-of-pocket medical expenses,changes in employment status, and decreasedaccess to affordable health insurance.3In addition to the physical and psychological
effects of the disease and its treatment, living withcancer presents substantial life challenges to sur-vivors and their families. Long-term adverse out-comes for cancer survivors may cause distress andnegatively impact quality of life (QOL). TheNational Comprehensive Cancer Network(NCCN) has challenged healthcare providers to
Problems and Process in a Study Design—Lessons LearnedBy Carol Guarnieri, RN, MSN, FNP-C, AOCNSOncology Nurse Practitioner, Scottsdale Healthcare, Scottsdale, Arizona
Patrice Welsh Benjamin, RN, MA, OCNOncology Nurse Clinician, Scottsdale Healthcare, Scottsdale, Arizona
Melanie O’Hara, RN, MSN, OCNCancer Care Coordinator, Scottsdale Healthcare, Scottsdale, Arizona
Marlene Miller, RN, MSN, CORLNCancer Care Coordinator, Scottsdale Healthcare, Scottsdale, Arizona
Lindsay Thomas, RN, MSN, OCNDirector of Oncology Services, Scottsdale Healthcare, Scottsdale, Arizona
Maria Bautista, MS, ANP, CGRNRadiation Oncology Nurse Practitioner, Scottsdale Healthcare, Scottsdale, Arizona
Sally Kazilek, RN, MSN, OCNRadiation Therapy Nurse, Banner Desert Medical Center, Mesa, Arizona
Melanie Brewer, DNSc, RN, FNP-BCDirector of Nursing Research, Scottsdale Healthcare, Scottsdale, Arizona
Abstract: Healthcare professionals want to ensure that every patient receives quality care throughout thecontinuum of their cancer illness. In addition, many national organizations have challenged healthcareproviders to provide comprehensive services to cancer survivors. Research indicates that long-term adverseoutcomes for cancer survivors are more prevalent, serious, and persistent than previously known. As a result,survivorship care presents many new avenues for nursing research. In developing our survivorship program,an interdisciplinary team at our hospital developed an exploratory pilot research study to evaluate theimpact of assessment, education, support, and guidance on patients’ quality of life and distress. The goalof the pilot study was to evaluate our interventions and make recommendations to expand our survivorshipservices to all cancer patients in our hospital system. We encountered several problems with implementingour study. This paper describes our research process and the problems we encountered with our studydesign and the revisions that were made in order to accrue patients and achieve our goals. A descriptionof these challenges and the changes we made may assist others with their research endeavors.
8 JUNE 2012 • VOLUME 3, ISSUE 3 AONNONLINE.ORG
SURVIVORSHIPRESEARCH

SURVIVORSHIPRESEARCH
provide comprehensive services to cancer sur-vivors and has provided evidence-based guide-lines and tools to assist in improving outcomesand enhancing QOL.4 In the report from theInstitute of Medicine, From Cancer Patient toCancer Survivor: Lost in Transition, 10 recom-mendations were made to improve the QOL ofcancer survivors. The first recommendation isthat healthcare providers, patient advocates,and other stakeholders should work together toraise awareness of the needs of cancer survivors,establish cancer survivorship as a distinct phaseof cancer care, and act to ensure the delivery ofappropriate survivorship care.3 Since care forsurvivors is a key component of a quality cancerprogram, leaders at Scottsdale Healthcare(SHC) wanted to develop a cancer survivorshipprogram in response to these recommendations.SHC is a large community-based hospital systemlocated adjacent to the Phoenix metropolitanarea. An interdisciplinary team from theVirginia G. Piper Cancer Center (VGPCC) atSHC developed an exploratory research study toevaluate the impact of assessment, education, sup-port, and guidance on the QOL and distress inhead and neck cancer and lung cancer patientswho had completed a minimum of 4 weeks of radi-ation therapy. Evaluating the effects of this pro-gram on patient distress and QOL was needed todetermine whether program modifications, revi-sions, and/or additional services were indicated inorder to minimize distress and enhance QOL for allcancer survivors. After an evaluation of outcomes,modifications would be made as needed to improveimplementation processes, identify gaps in avail-able services, and estimate the financial resourcesand personnel necessary to expand and sustain acommunity-based survivorship program. The pro-gram would then be offered to all adult cancer sur-vivors who contact the VGPCC for care.
REVIEW OF THE LITERATUREDistressDistress is defined by the NCCN as a multifacto-rial unpleasant emotional experience of a psy-chological (cognitive, behavioral, emotional),social, and/or spiritual nature that may interferewith the ability to cope effectively with cancer,its physical symptoms, and its treatment. Distressextends along a continuum, ranging from normalfeelings of vulnerability, sadness, and fear toproblems that can become disabling, such as
depression, anxiety, panic, social isolation, andexistential and spiritual crisis.4Psychological distress in patients with cancer
can negatively impact their QOL. According toVachon, approximately one-third of cancer sur-vivors report distressing symptoms that may rangefrom sadness to debilitating depression.5 Accordingto the National Cancer Institute, 44% of cancersurvivors report some anxiety, with 23% reportingsignificant anxiety.6 The most common fear amongcancer survivors is the fear of recurrence, rangingfrom 5% to 89%, depending on the type of cancerdiagnosis, stage of cancer, and other factors.7
Quality of LifeQOL is defined by the conceptual frameworkbased on research by Ferrell and colleagues andincludes an individual’s perception of physical,psychological, social, and spiritual well-being.8 Asthe treatment of cancer has become more success-ful, the number of cancer survivors has risen.Long-term survival from cancer has brought QOLto the forefront as an issue in cancer survivorship.QOL is defined as an individual’s assessment ofhis or her own general well-being. A core conceptof measuring QOL is obtaining self-assessment bythe patient across multiple “domains,” or areas, ofwell-being. In order to assess QOL in cancer sur-vivors, standardized, self-administered question-naires are generally used. It is recommended thatassessments be repeated at regular intervals over aperiod of time, focusing on function in physical,psychological, social, and spiritual domains.3
SURVIVORSHIP BY DISEASE SITEHead and Neck CancerHead and neck cancers can have a profound
The first recommendation is thathealthcare providers, patient advocates,and other stakeholders should worktogether to raise awareness of the needsof cancer survivors, establish cancer sur-vivorship as a distinct phase of cancercare, and act to ensure the delivery ofappropriate survivorship care.
AONNONLINE.ORG JOURNAL OF ONCOLOGY NAVIGATION & SURVIVORSHIP 9
SURVIVORSHIPRESEARCH
impact on a survivor’s QOL. The head and neckregion is important for the functions of eating andspeech. Head and neck cancer survivors oftenundergo a combination of surgery, chemotherapy,and radiation. The combination of cancer and itstreatment can leave a significant alteration in thisarea cosmetically, functionally, and socially. Thetreatment results in a variety of long-term effectssuch as xerostomia, loss of taste, dental decay/loss,and tissue loss resulting in disfigurement.9 Patientswith head and neck cancer experience a variety ofpsychological symptoms and disorders of anxietyand depression, possibly at rates greater thanthose seen in patients with other types of cancer.10
According to a review by Goldstein and col-leagues, QOL in head and neck cancer patientsworsens during and shortly after treatment andthen gradually improves, approaching baselinelevels 12 months after diagnosis.11 This is consis-tent with the time frame of our intervention. Anawareness of the type of issues experienced byhead and neck cancer patients is vital for accurateassessment and effective intervention. By identify-ing needs early on, we can better understand thesurvivor’s concerns, provide education, and makeappropriate referrals. A review of the head andneck cancer studies by Pandey et al and Karnell etal identified that anxiety, depression, family dis-tress, social distress, and impact on activities ofdaily living all resulted from a cancer diagnosis.12,13
Lung CancerLung cancer patients have been identifiedthrough multiple studies as having high levels ofdistress.14-16 Symptoms that increase distress thathave repeatedly been identified for lung cancerpatients include fatigue, pain, cough, dyspnea,sleep disruptions, decreased appetite, anxiety,depression, and problems with family relation-ships and physical and cognitive functioning. The2 most reported symptoms are fatigue andpain.17,18 The lung cancer research clearly demon-strates the serious nature of distress and the
impact on QOL. In their study of 333 patients ina multidisciplinary lung cancer clinic, Graves andcolleagues utilized the distress tool and identifiedclinically significant distress in 61.6% of thepatients.14 Sarna and colleagues describe seriousdisruptions in the psychological and social aspectsof QOL in 217 women with non–small cell lungcancer who were between 6 months and 5 yearsout from diagnosis.18
CONCEPTUAL FRAMEWORKThe conceptual framework used in this study wasthe QOL model for cancer survivors developed byFerrell and Grant at the City of Hope (COH)Medical Center.19 QOL is defined as a multidi-mensional concept consisting of 4 domains thatinclude physical, psychological, social, and spiri-tual well-being. The concept is based on thebelief that each domain contributes to an individ-ual’s perception of overall QOL.3 Results from theCOH QOL questionnaire were going to providethe foundation for patient-directed goal settingfocusing on the 4 domains of QOL.
STUDY DESIGNObjectiveThis study evaluated the impact of assessment,education, support, and guidance on QOL anddistress in head and neck cancer and lung cancerpatients who had completed a minimum of 4 weeks of radiation therapy at SHC.
MethodThis study employed a nonexperimental, ex -ploratory, descriptive design. The study was con-ducted in an outpatient radiation center in a largeSouthwestern community-based hospital. Thesample for the study consisted of adult oncologypatients with a lung cancer or head and neck can-cer diagnosis receiving radiation therapy for atleast 4 weeks. An anticipated enrollment in thestudy was 90 participants, based on the number ofhead and neck cancer and lung cancer patientstreated at the hospital.Inclusion criteria included those older than
18 years, who were able to speak, read, write, andunderstand English, had a primary diagnosis oflung cancer or head and neck cancer, and wereable to complete a minimum of 4 weeks of radia-tion therapy. Patients were identified by the nurs-ing staff in radiation oncology.Patients who met the inclusion criteria were
By identifying needs early on, we can better understand the survivor’s
concerns, provide education, and make appropriate referrals.
10 JUNE 2012 • VOLUME 3, ISSUE 3 AONNONLINE.ORG

SURVIVORSHIPRESEARCH
asked to consider participation in the study. If thepatient agreed, he or she was enrolled into thestudy. The COH QOL for Cancer Survivors andNCCN Distress surveys with an attached cover let-ter were distributed by mail 1 month after the com-pletion of radiation therapy. Patients were contact-ed by phone to schedule the first meeting with thecase management team and to answer any ques-tions concerning completion of the questionnaires.Each participant was assigned a survivorship
advanced practice team. Program team memberswere master’s-prepared certified oncology nursesand/or master’s-prepared licensed medical socialworkers and were investigators in this study. Aftercompletion of the assessment tools described, par-ticipants met with a team member to review theresults of the assessment tools and work togetherto define patient-specific goals. Survivors were towork with their primary team member to developan action plan to help address their concerns andgoals. Referrals to the appropriate services andproviders would be initiated as needed.Additional didactic information addressing
common issues facing cancer survivors was to beprovided at each patient contact. Topics includedmaintaining personal health records, the medicaltreatment summary and follow-up plan, commonphysical and emotional concerns, and practicalmatters. Patients also received a LIVE-STRONG™ Survivorship Notebook and othereducational materials as determined by partici-pant needs.Participant contact with a primary team mem-
ber would occur on a monthly basis, and more or less frequently as indicated through ongoingassessment of patient needs. The additional con-tacts were conducted in person or via phone calls.In addition to individualized case managementservices, participants were offered personalizededucation, psychosocial support and referrals, andcommunity education seminars.Collection of demographic information and
QOL and Distress surveys were to be completed 1 month posttreatment, and they were to berepeated at 3 and 6 months after completion ofradiation therapy. Surveys were to be either mailedto patients for completion or completed in person.Data collected in the study were to be reported
in the aggregate without patient-identifyinginformation to protect anonymity. The study wasapproved by the Institutional Review Board atSHC, where the investigators were employed.
DATA ANALYSIS PLANData were to be entered using a double entry intoa customized Excel spreadsheet. Discrepancieswere to be checked and corrected. All data col-lected in this study were going to be documentedusing summary tables. Descriptive statistics wereto be provided for each variable measured, bygroup and measurement period. Statistics were toinclude sample size, arithmetic mean, median,standard deviation, and minimum and maximumfor continuous variables. Categorical variableswere going to be summarized using frequenciesand percentages. Geometric means were to becalculated for variables that are non-normally dis-tributed. Statistical analyses were to be performedusing SPSS version 16.0.The primary analysis was to compare Distress
Thermometer and QOL scores at 6 months acrossgroups. Preliminary analysis was to be conductedto assess the degree of intercorrelation among thedomain scores on the QOL instrument and thesingle score on the Distress Thermometer.
LESSONS LEARNEDParticipant RecruitmentA major problem encountered was that ourpatient accrual was very slow. Patients chose notto participate for a variety of reasons. Our refusalrate was over 60%. Even for the patients whoconsented, not 1 patient was able to complete thestudy requirements. We chose this population oflung and head and neck cancer patients becausewe thought that these patients could benefit fromextra assistance and education. However, ourpatients stated they did not have the energy tocomplete the forms or attend the meetings. Bothwere too burdensome and taxing. In our initialstudy, we also attempted to study a patient popu-lation with whom we did not have an establishedprofessional relationship. In the redesign, wechose patients according to our subspecialties
In addition to individualized case management services, participantswere offered personalized education,psychosocial support and referrals, andcommunity education seminars.
AONNONLINE.ORG JOURNAL OF ONCOLOGY NAVIGATION & SURVIVORSHIP 11

SURVIVORSHIPRESEARCH
area. This allowed the advanced practice nurse(APN) to develop a rapport with the patientbefore inviting him/her to participate in thestudy. We felt that developing a trusting relation-ship prior to an invitation to participate in thestudy also enhanced our recruitment process.
Need for Study RevisionThe study has since been through several revi-sions. Through this process we have learned sev-eral lessons. First, the burden of a new diagnosisand treatment for severely ill patients, along withthe burden of completing study questionnaires,was overwhelming. We needed to simplify thestudy. To facilitate recruitment, we broadened thestudy to include all newly diagnosed patients. Allpatients who agree to participate are given theNCCN Distress tool and the COH QOL tool.Upon completion of the questionnaires, the APNmeets with the patient and significant other(s) toidentify areas of concern and establish goals. TheAPN continues to meet with the patient as nec-essary. After 3 months of interventions, thepatient is given an evaluation form to complete,assessing whether the APN’s interventions andeducation were helpful. Implementing this simpleand less- complicated design, we are continuingto recruit and maintain patients.
CONCLUSIONCancer survivorship care represents a major areaof research opportunities. In developing a sur-vivorship program that encompasses the needs ofour patients, this was our first attempt to conducta research study. We learned that a simplifiedresearch design and less strict recruitment criteriawere beneficial. With our current simplifieddesign, we are recruiting and maintainingpatients. One of our most important lessons wasthat research happens by persevering throughobstacles and multiple revisions. Most important-ly, through our persistent efforts, our goal remains
to assist our patients in meeting their needs byproviding individualized care to help minimizedistress and improve their QOL. g
REFERENCES1. American Cancer Society. Learn about cancer. www.cancer.org/Cancer/news/News/numberofuscancersurvivorsgrowing.Accessed January 5, 2012.2. Clark EJ, Stovall EL, Leigh L, et al. Imperatives for qualitycancer care: access, advocacy, action, and accountability. In:Scherr SL, ed. Self-Advocacy: A Cancer Survivor’s Handbook.Silver Spring, MD: National Coalition for Cancer Survivor -ship; 1996.3. Hewitt M, Greenfield S, Stovall, E, eds. From Cancer Patientto Cancer Survivor: Lost in Transition. Washington, DC: TheNational Academies Press; 2005.4. National Comprehensive Cancer Network. NCCN ClinicalPractice Guidelines in Oncology: Distress Management.http://nccn.org/professionals/physician_gls/PDF/distress.pdf.Accessed January 7, 2012.5. Vachon M. Psychosocial distress and coping after cancertreatment. Cancer Nurs. 2006;29(2 suppl):26-31.6. National Cancer Institute. Anxiety disorder PDQ. www.can-cer.gov/cancertopics/pdq/supportivecare/anxiety/healthprofessional. 2008. Accessed February 5, 2009.7. Alfano CM, Rowland JH. Recovery issues in cancer survivor-ship: a new challenge for supportive care. Cancer J.2006;12:432-443.8. Ferrell BR, Grant M, Dow KH. Quality of life model appliedto cancer survivors. http://prc.coh.org/pdf/cancer_survivor_QOL.pdf. 2004. Accessed February 5, 2009.9. Rogers SN, Ahad SA, Murphy AP. A structured review andtheme analysis of papers published on ‘quality of life’ in headand neck cancer: 2000-2005. Oral Oncol. 2007;43:843-868.10. Haman KL. Psychologic distress and head and neck cancer:part 1—review of the literature. J Support Oncol. 2008;6:155-163.11. Goldstein DP, Hynds Karnell L, Christensen AJ, et al.Health-related quality of life profiles based on survivorship sta-tus for head and neck cancer patients. Head Neck. 2007;29:221-229.12. Pandey M, Devi N, Thomas B, et al. Distress overlaps withanxiety and depression in patients with head and neck cancer.Psychooncology. 2007;16:582-586.13. Karnell L, Christensen AJ, Rosenthal EL, et al. Influence ofsocial support on health-related quality of life outcomes in headand neck cancer survivors. Head Neck. 2007;29:143-146.14. Graves KD, Arnold SM, Love CL, et al. Distress screeningin a multidisciplinary lung cancer clinic: prevalence and predic-tors of clinically significant distress. Lung Cancer. 2007;55:215-224.15. Logue AE, Gawiak CT, Houlihan N, et al. Development ofa non-small cell lung cancer (NSCLC) survivorship program:baseline clinical characteristics and quality of life (QOL): PD5-3-8. J Thoracic Oncol. 2007;2:S481.16. Zabora J, BrintzenhofeSzoc K, Curbow B, et al. The preva-lence of psychological distress by cancer site. Psychooncology.2001;10:19-28.17. Cooley ME, Short TH, Moriarty HJ. Symptom prevalence,distress, and change over time in adults receiving treatment forlung cancer. Psychooncology. 2003;12:694-708.18. Sarna L, Brown JK, Cooley ME, et al. Quality of life andmeaning of illness of women with lung cancer. Oncol NursForum. 2005;32:E9-E19.19. Ferrell BR, Grant M. Quality of life Patient/CancerSurvivor version. http://prc.coh.org/QOL-CS.pdf. AccessedFebruary 12, 2009.
12 JUNE 2012 • VOLUME 3, ISSUE 3 AONNONLINE.ORG
Developing a trusting relationship prior to an invitation to participate
in the study also enhanced our recruitment process.

VELCADE and Millennium are registered trademarks of Millennium Pharmaceuticals, Inc. Other trademarks are property of their respective owners.
Millennium Pharmaceuticals, Inc., Cambridge, MA 02139
Copyright © 2010, Millennium Pharmaceuticals, Inc. All rights reserved. Printed in USA V-10-0196 11/10
*The VELCADE Reimbursement Assistance Program does not file claims
or appeal claims for callers, nor can it guarantee that you will be successful
in obtaining reimbursement

ORIGINAL RESEARCH
Cancer patients from all backgrounds face amyriad of psychosocial and practical issuesthat impact their cancer diagnosis, treat-
ment, and survivorship experience.1-3 The timefrom an initial diagnosis to the onset of treatmentcan be overwhelming for patients as they need tomanage multiple providers and healthcare sys-tems, understand their insurance coverage andthe specifics of their diagnosis and treatmentoptions, as well as deal with the emotional chal-lenges of facing an often unexpected diagnosis. Patient navigation programs and strategies
have emerged as an important approach toaddressing the range of psychosocial issues; accessto care; and utilization of cancer screening, diag-nostic, and treatment services.4 The role ofpatient navigation in cancer screening and carewas initiated in the Harlem Cancer Educationand Demonstration Project in the early 1990s,
when patient navigation served as a means toimprove timely movement along the cancer carecontinuum in medically underserved popula-tions.5 Since that time, federally funded researchhas been implemented to evaluate the impact ofpatient navigation services, various governmentand voluntary agencies have developed patientnavigation models and services, professional asso-ciations have emerged, and the evidence basesupporting the positive effects of patient naviga-tion has grown.6Within the emerging field of patient naviga-
tion,4 numerous models and approaches havebeen described, including clinical (often nursenavigators) and nonclinical (other health profes-sionals and/or community health workers) navi-gation and mixed models that include bothapproaches.7-9 Often these different models areimplemented based on where along the cancer
Implementation of a Theory-Based, Nonclinical PatientNavigator Program to Address Barriers in an UrbanCancer Center SettingBy Linda Fleisher, PhD, MPH; Suzanne M. Miller, PhD; Danielle Crookes, MPH; Venk Kandadai, MPH; Kuang Yi Wen, PhD; Rachel E. Slamon, BSFox Chase Cancer Center, Philadelphia, Pennsylvania
Jeanne Chaivous, MSWTemple University, Philadelphia, Pennsylvania
14 JUNE 2012 • VOLUME 3, ISSUE 3 AONNONLINE.ORG
Abstract: Cancer patients face a myriad of psychosocial and practical issues. Especially challenging isthe time from an initial diagnosis to the onset of treatment, and patient navigation services are impor-tant to guide patients, especially underserved populations, through this maze of uncertainty. Here wereport on the Pennsylvania Patient Navigator Demonstration Project (PaPND) designed to evaluate theacceptability, feasibility, and impact of a culturally and linguistically appropriate nonclinical navigatorprogram. The development of the project, based on behavioral theory and community-based participa-tory research principles, is described. Forty-four cancer patients from diverse backgrounds participatedin the study, which included a baseline assessment, navigation services, and a 4-week and 12-weekfollow-up assessment. On average, participants experienced 1.8 barriers, with transportation and insur-ance issues the most common barriers. The majority (56%) of the barriers required more than an hour ofthe navigator’s time to address, with insurance, transportation, and caregiver/support issues requiringthe most time. Overall, patients were fairly satisfied with the navigation services. After patient naviga-tion, the findings showed improvement in patients’ worry, their understanding of their disease, and theirbeliefs in the importance of treatment, as well as their own self-efficacy in managing cancer-relatedissues. Results also suggest issues that need to be addressed include providing and connecting cancerpatients to appropriate information to improve their understanding of their diagnosis and their recom-mended treatments and areas in which the integration of nonclinical and clinical navigation is essential.In addition, more attention to the assessment of psycho social issues, such as the patients’ emotional wor-ries, and more comprehensive training in these areas would enhance navigation programs.

ORIGINAL RESEARCH
continuum the patient navigation services arefocused. Although current randomized controltrials are expected to provide more definitiveconclusions about impact and cost-effectivenessof patient navigation, there are lessons to belearned from ongoing program evaluations anddemonstration projects focused on establishingand implementing patient navigation in real-world settings.10,11Toward that end, we conducted a demonstra-
tion project, called the Pennsylvania PatientNavigator Demonstration Project (PaPND) fund-ed by the Pennsylvania Department of Health.The aims of the PaPND were to evaluate theacceptability, feasibility, and impact of a cultural-ly and linguistically appropriate navigator pro-gram relying on a nonclinical patient navigationmodel. Specifically, the role of the nonclinicalnavigators was to address psychosocial and accessbarriers for patients during the period betweendiagnosis and initiation of treatment. The pro-gram was guided by the Cognitive-Social HealthInformation Processing (C-SHIP) theoreticalframework,2,3 which focuses on the cognitive andemotional factors as well as the practical skillsthat impact health behaviors. Our goal was toinfuse these concepts into the navigator trainingand baseline assessment and evaluate the impactof navigation on these factors. Our previous experience in service-related
research12 supported our approach to the designand implementation of the program using com-munity-based participatory research (CBPR)13,14concepts by involving the sites in the grant appli-cation and project development process, fundinga dedicated onsite navigator, jointly supervisingthe navigator, and participating in the evaluation.Navigation services were offered to all patientswho had just been diagnosed with breast, cervical,prostate, colorectal, or lung cancer and were pro-vided in both English and Spanish. The evalua-tion included data on barriers faced by partici-pants, navigator’s time to address the barriers,impact on psychosocial needs, and satisfactionwith the navigation services.
METHODSStudy SiteThis nonrandomized, longitudinal 3-year demon-stration project was developed and conducted atTemple University Hospital in Philadelphia,Pennsylvania. At the time that this project was
initially planned, there were few patient naviga-tion programs and even fewer best practice train-ing and implementation tools. Therefore, wedeveloped a patient navigator training programand institution-specific implementation proce-dures and processes; we also designed and con-ducted a program evaluation. Temple University Health System (TUH) is an
urban 514-bed tertiary medical center, which pro-vides care to over 20,000 inpatients and 150,000outpatients annually. The hospital serves a pre-dominantly low-income population, and thepatient population is 47% African American and14% Hispanic. This site was chosen to address theneeds of historically medically underserved popu-lations. This study was approved by theInstitutional Review Board at Fox Chase CancerCenter and Temple Medical System.
Inclusion/Exclusion Criteria of ParticipantsEligible participants were at least 18 years of age,with a diagnosis of breast, cervical, colorectal,prostate, or lung cancer. Participants were ineligi-ble for the study if they could not speak English orSpanish, were unable to give proper informedconsent, or had already begun treatment for theircancer diagnosis. Participants were referred to theprogram by physicians, radiologists, and patholo-gists or were identified directly by the navigator aseligible for the program.
Development of Program and TrainingBuilding on the emerging literature on patientnavigation and CBPR principles, procedures andprocesses were developed in collaboration withthe implementation-site investigator and keyhospital staff. The key goals were to develop thenavigator job description, determine the organi-zational reporting structure, install the navigationtracking software, study procedures and processes,and oversee ongoing project management. FoxChase Cancer Center research staff focused most
Specifically, the role of the nonclinicalnavigators was to address psychosocialand access barriers for patients duringthe period between diagnosis and initiation of treatment.
AONNONLINE.ORG JOURNAL OF ONCOLOGY NAVIGATION & SURVIVORSHIP 15

ORIGINAL RESEARCH
on the research study implementation while thecommunity-based cancer center focused on casemanagement of patient care and treatment. Theintegration of research and service was overseenby project managers at both sites through weeklycontact to coordinate, review, and discuss theresearch study, implementation, research issues,and data collection. Management and adminis-tration of the patient navigation program alsorequired considerable logistical coordination,involving numerous planning meetings, partici-pation in various cancer program meetings toaddress potential concerns, and development ofan implementation process that was congruentwith hospital operations and policies. The teamaddressed program planning with collaborativeand creative coordination, including the develop-ment of a customized contact-management soft-ware package (SugarCRM Enterprise), whichprovided a system to keep notes on each contactwith participants and any follow-up with otherentities (eg, insurance company, transportation,primary care, etc).
A comprehensive, 2-week navigation training,modeled on the National Cancer Institute’s(NCI) Cancer Information Service training andthe Pfizer Patient Navigation in Cancer CareToolkit, included face-to-face sessions with a stafftrainer, self-directed learning modules, and 2online sessions. Topics covered included basic can-cer concepts, the cancer continuum, resources, andbarriers to treatment. Training was also providedon key navigator skills such as assessment andproblem identification, the navigator’s role andresponsibilities, and communication skills. The C-SHIP framework was integrated throughout thetraining to ensure that the patient navigatorunderstood the importance of both cognitive and
affective issues as well as how to address these issueswhen providing navigation services. The trainingalso included a component on the value of researchas well as Health Insurance Portability andAccountability Act (HIPAA) and HumanSubjects Protection certification.
Navigator Qualification and TrainingThe patient navigator was recruited and hiredby TUH, with the assistance and consultationof Fox Chase Cancer Center. The navigatorpossessed a bachelor’s degree in social work,was bilingual (English/Spanish), and was fromthe community in which participants wererecruited, giving her an intimate knowledge ofthe community’s population and resources. Shehad no previous experience with formalizedpatient navigation or behavioral research.Once hired, Fox Chase provided the navigatorwith in-depth training on patient navigation.The implementation site provided its owninstitutional orientation.
Study ImplementationPatients were identified by the registration listor by direct referral from providers. The patientnavigator first contacted eligible individuals byphone to obtain provisional informed consentand then secured final, written informed con-sent and HIPAA authorization at the first face-to-face clinic appointment. In addition, thenavigator administered a baseline psychosocialsurvey and identified barriers to obtainingtreatment and care. Two follow-up telephoneassessments were administered by studyresearch assistants at 4- and 12-weeks after thebaseline assessment to determine the impact ofthe navigator intervention. Self-reportedpatient satisfaction was included in both the 4and 12-week assessments. All study measuresand follow-up interviews were conducted ineither English or Spanish, as appropriate. Totrack barriers and the services provided to eachparticipant, the navigator used the trackingsoftware. Data recorded in this log includedparticipant demographics, participant eligibili-ty, barriers experienced, services provided, andthe time period to address the recorded barriers.A section was available to record more detailednarrative. Individuals who were in need of nav-igator services but did not want to participatein the study were provided with these services.
The navigator possessed a bachelor’sdegree in social work, was bilingual(English/Spanish), and was from the
community in which participants wererecruited, giving her an intimateknowledge of the community’s
population and resources.
16 JUNE 2012 • VOLUME 3, ISSUE 3 AONNONLINE.ORG

ORIGINAL RESEARCH
Figure 1 depicts the overall study design andimplementation.
Study Measures and AnalysisThe baseline survey was used to provide the ini-tial patient needs assessment as well as to collectdata for the study evaluation. The baselinemeasures included demographics, health status,cancer diagnosis, and perceived barriers to care.The barriers were categorized using the C-SHIPframework into (1) practical barriers (ie, healthinsurance copays), (2) negative cognitions (eg,lack of understanding of treatment procedures),(3) negative expectancies and beliefs (eg, fatal-ism), and (4) affective barriers (eg, worry aboutdiagnosis). These measures were assessed notonly at baseline but also at 4 weeks and 12 weekspost initial consult. A face-valid 9-item ques-tionnaire on patient satisfaction, designed bythe study team, was administered at both the 4-week and 12-week follow-up assessments. Thesequestions evaluated participants’ satisfactionwith the navigator services, such as receivingcancer-related information, assistance withinsurance-related problems, and getting commu-nity services. Participants were asked to indicatetheir agreement with each statement on a 5-point scale (0 = “Not at all” to 4 = “Verymuch”), and then scores were summed for anoverall satisfaction score. After the initial consult and completion of
the baseline survey, the navigator provided nav-igation services and tracked specific barriers thatwere addressed in the case management soft-ware. The navigator contacted the patients asneeded during the treatment process. The barri-ers were tracked across the array of barriers (eg,transportation, scheduling, insurance, physical/emotional support, housing/living issues, care-giver support, referral issues, other systemsissues, and other financial issues). A barrier wasdefined as an issue described by the participantand subsequently addressed by the patient navi-gator. The navigator also recorded the timerequired to address each barrier.Descriptive statistics were generated for all
variables and barrier data. A 2-sided, nonpara-metric, Wilcoxon signed-rank test was used toascertain the difference in satisfaction scores at 4and 12 weeks. Significance was determined atthe 0.05 level, and data analysis was done usingSAS version 9.2.
RESULTSBackground CharacteristicsParticipants enrolled in the study (N = 44) pro-vided written consent and completed the baselineassessment. Table 1 shows the baseline character-istics of the study population. All participantswere followed up after 4 weeks, and about 80%were followed up after 12 weeks. The mean age of the enrolled participants was
56.7 years (SD = 11.7; median = 55). The major-ity were African American (64%), were women(82%), earned less than $15,000 annually (63%),were unemployed (91%), and had a high schooleducation or less (80%). Breast and prostate can-cers represented over 70% of the case load. Justunder one-third of participants reported beingHispanic/Latino.
Addressing Identified BarriersOn average, participants experienced 1.8 barriers(SD = 1.1; min = 1; max = 4). Figure 2 describesthe types of barriers addressed by the navigators.
Overall Study Design of the Pennsylvania Patient Navigator Demonstration Project
Figure 1
Patient referred to navigator(Physician, radiology, pathology)
Navigator serviceContinues providing ongoing service
Navigator calls patient• Determines eligibility• Obtains verbal consent
Navigator follow-upExtracts information from chart
2 months
Navigator meets patient• Obtains written consent• Conducts baseline survey• Completes assessment usingonline management log
Telephone follow-up4 weeks
Telephone follow-up12 weeks
Research Assistant
p p
p
p
AONNONLINE.ORG JOURNAL OF ONCOLOGY NAVIGATION & SURVIVORSHIP 17
p

ORIGINAL RESEARCH
Transportation and insurance issues (practicalbarriers) were the most common, representingnearly 60% of all the barriers addressed. Supportissues (physical, emotional, caregiver) represent-ed nearly 20% of the barriers addressed. We also reviewed the time required to address
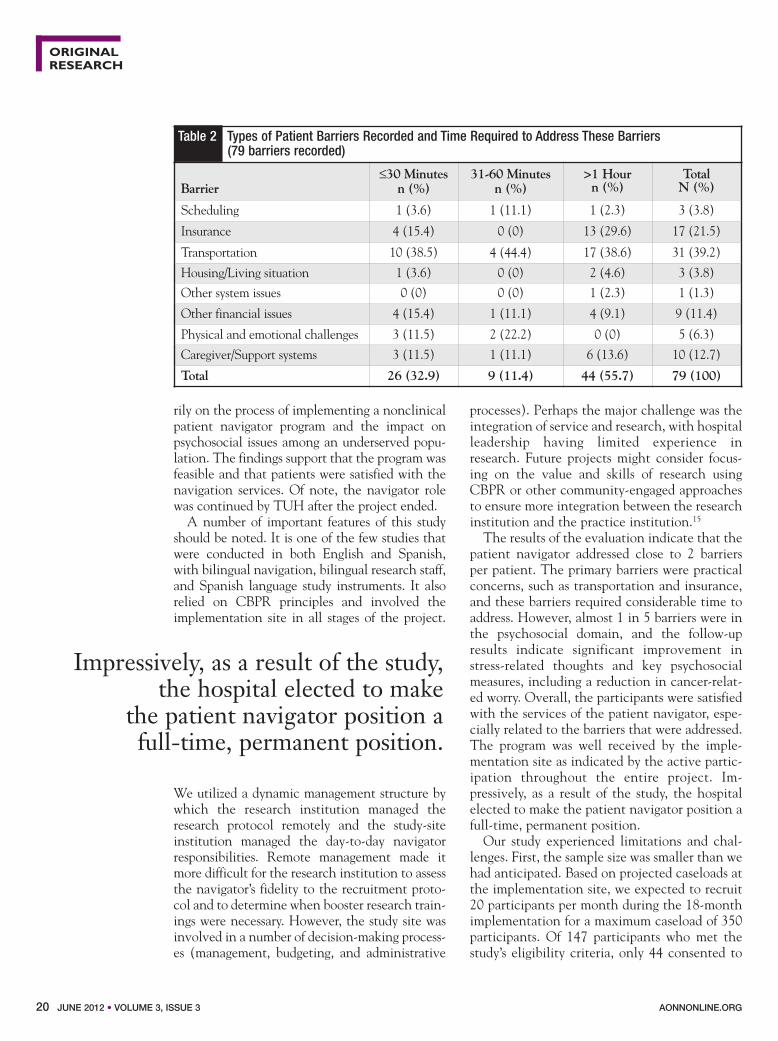
these barriers and created 3 categories: 30 minutesor less; 30 to 60 minutes, and greater than anhour. The majority (56%) of the barriers requiredmore than an hour of the navigator’s time toaddress, with insurance, transportation, and care-giver/support issues requiring the most time(Table 2).
Patient SatisfactionSatisfaction was assessed through telephone fol-low-ups, and satisfaction items addressed how thenavigator helped with cancer-related informa-tion, provided help with insurance and variousmedical services, was culturally sensitive, andhelped with family and other responsibilities.
Higher scores indicated higher levels of satis-faction. The highest-rated items included seek-ing cancer-related information, access to careand community services, and being culturallysensitive (Table 3). There was improvement,although not significant, in specific measuresover time. The overall satisfaction score signif-icantly increased from 4 weeks (2.7) to 12weeks (3.5). Table 3 depicts the mean scores ofeach of the 9 satisfaction items.
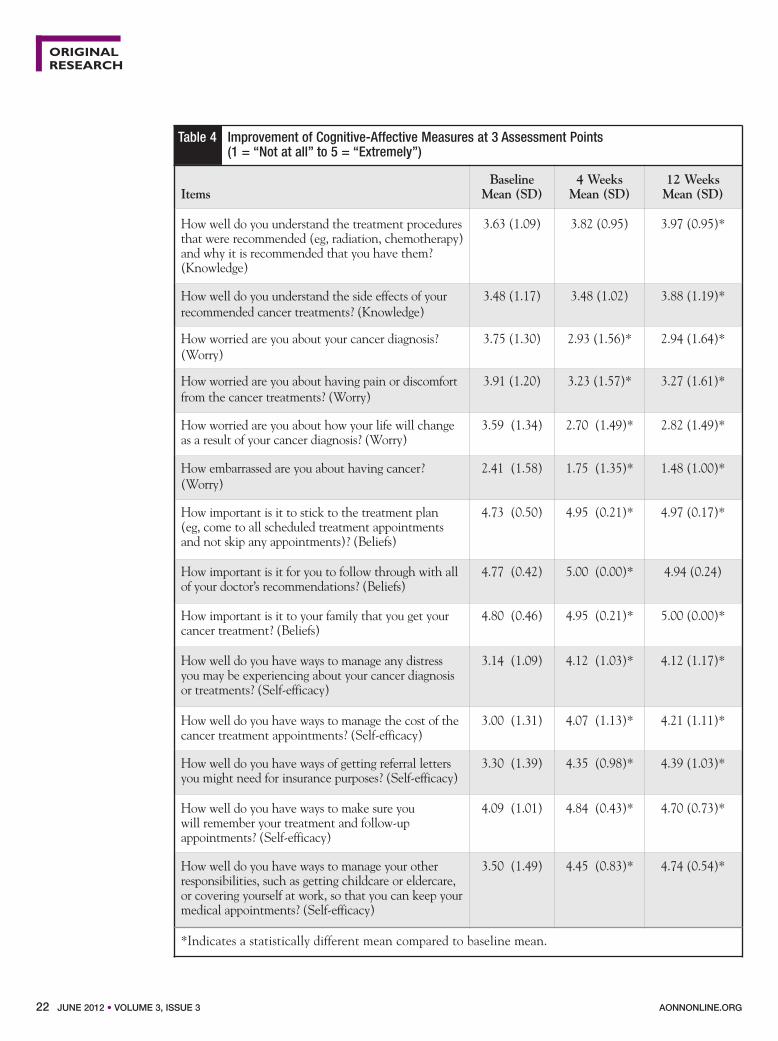
Impact of the Navigator Interventions onChanges in Cognitive-Affective MeasuresDescriptive and exploratory analyses were con-ducted for the cognitive-affective measures thatwere evaluated through self-reported assess-ment at baseline, 4 weeks, and 12 weeks. Themeasures were assessed on a 5-point scale (1 =“Strongly disagree” to 5 = “Strongly agree”).These measures included cancer worry, knowl-edge about treatment, beliefs about following
the treatment regimen, and ability to cope withself–management related issues. Table 4 showsthe mean and standard deviation of the items thatshowed significant changes on the post naviga-tion assessment. Higher scores reflect more posi-tive self-perceptions, except for worry measures.Two of the knowledge-related measures showedsignificant improvement at 12 weeks. Reductionsin worry about the cancer diagnosis, pain, lifechanges, and embarrassment were seen at 4 and 12weeks. Expectancies and beliefs or values/goalsmeasures also showed improvement. Patientsreported higher scores on the importance ofadhering to the treatment plan, following throughwith physician recommendations, and the impor-tance of family support. In regard to self-regulato-ry skills, patients reported improvements in man-agement of distress, ways to cope with financialrelated issues, remembering appointments, andmanaging other responsibilities.
DISCUSSION The Pennsylvania Navigating Cancer Patients(PaPND) demonstration project evaluated theacceptability, feasibility, and impact of a cultural-ly and linguistically appropriate patient navigatormodel in an urban hospital. Findings from thisstudy contribute to the emerging literature basethat investigates the use of navigation during theperiod from cancer diagnosis to treatment. ThePaPND had a modest budget and focused prima-
Frequency of the Different Types of Patient Barriers Recorded by the Patient Navigator
Figure 2
35
30
25
20
15
10
5
0
Frequency
ReferralIssues
1
OtherSystemIssues
Scheduling Housing/Living
Situation
Physicaland
EmotionalChallenges
OtherFinancialIssues
Caregiver/SupportSystems
Insurance Transpor -tation
Barrier Type
3 3 5
9 10
17
31
The majority (56%) of the barriersrequired more than an hour of the nav-igator’s time to address, with insurance,transportation, and caregiver/support
issues requiring the most time.
18 JUNE 2012 • VOLUME 3, ISSUE 3 AONNONLINE.ORG

ORIGINAL RESEARCH
Table 1 Background Characteristics of Study Participants (N = 44)
Age N (%)55 years or younger 22 (50)
Older than 55 years 22 (50)RaceAmerican Indian/Alaskan Native 1 (2.3)Asian 1 (2.3)
African American 28 (63.6)
Pacific Islander 0 (0) Caucasian 14 (31.8)
EthnicityHispanic/Latino 14 (31.8)Non–Hispanic/Latino 30 (68.2)
GenderMale 8 (18.2)Female 36 (81.8)
Marital statusSingle/Never married 15 (34.1)Single/Living with other 2 (4.5)Married 9 (20.5)Separated, divorced, or widow(er) 18 (40.9)
Annual incomeLess than $15,000 28 (63.6)$15,000 or more 16 (36.4)
Education level
High school or less 35 (79.5)
College or more 9 (20.5)Employment
Unemployed 40 (90.9)Employed 4 (9.1)
Current smoker?
Yes 16 (36.4)No 28 (63.6)
Have some type of private or government insurance?
Yes 38 (86.4)No 6 (13.6)
Cancer diagnosis
Breast 23 (52.3)Cervical 3 (6.8)Colorectal 6 (13.6)Lung 3 (6.8)Prostate 9 (20.5)
AONNONLINE.ORG JOURNAL OF ONCOLOGY NAVIGATION & SURVIVORSHIP 19
ORIGINAL RESEARCH
rily on the process of implementing a nonclinicalpatient navigator program and the impact on psychosocial issues among an underserved popu-lation. The findings support that the program wasfeasible and that patients were satisfied with thenavigation services. Of note, the navigator rolewas continued by TUH after the project ended.A number of important features of this study
should be noted. It is one of the few studies thatwere conducted in both English and Spanish,with bilingual navigation, bilingual research staff,and Spanish language study instruments. It alsorelied on CBPR principles and involved theimplementation site in all stages of the project.
We utilized a dynamic management structure bywhich the research institution managed theresearch protocol remotely and the study-siteinstitution managed the day-to-day navigatorresponsibilities. Remote management made itmore difficult for the research institution to assessthe navigator’s fidelity to the recruitment proto-col and to determine when booster research train-ings were necessary. However, the study site wasinvolved in a number of decision-making process-es (management, budgeting, and administrative
processes). Perhaps the major challenge was theintegration of service and research, with hospitalleadership having limited experience inresearch. Future projects might consider focus-ing on the value and skills of research usingCBPR or other community-engaged approachesto ensure more integration between the researchinstitution and the practice institution.15 The results of the evaluation indicate that the
patient navigator addressed close to 2 barriersper patient. The primary barriers were practicalconcerns, such as transportation and insurance,and these barriers required considerable time toaddress. However, almost 1 in 5 barriers were inthe psychosocial domain, and the follow-upresults indicate significant improvement instress-related thoughts and key psychosocialmeasures, including a reduction in cancer-relat-ed worry. Overall, the participants were satisfiedwith the services of the patient navigator, espe-cially related to the barriers that were addressed.The program was well received by the imple-mentation site as indicated by the active partic-ipation throughout the entire project. Im -pressively, as a result of the study, the hospitalelected to make the patient navigator position afull-time, permanent position.Our study experienced limitations and chal-
lenges. First, the sample size was smaller than wehad anticipated. Based on projected caseloads atthe implementation site, we expected to recruit20 participants per month during the 18-monthimplementation for a maximum caseload of 350participants. Of 147 participants who met thestudy’s eligibility criteria, only 44 consented to
Table 2 Types of Patient Barriers Recorded and Time Required to Address These Barriers (79 barriers recorded)
Barrier≤30 Minutes n (%)
31-60 Minutes n (%)
>1 Hourn (%)
TotalN (%)
Scheduling 1 (3.6) 1 (11.1) 1 (2.3) 3 (3.8)
Insurance 4 (15.4) 0 (0) 13 (29.6) 17 (21.5)
Transportation 10 (38.5) 4 (44.4) 17 (38.6) 31 (39.2)
Housing/Living situation 1 (3.6) 0 (0) 2 (4.6) 3 (3.8)Other system issues 0 (0) 0 (0) 1 (2.3) 1 (1.3)
Other financial issues 4 (15.4) 1 (11.1) 4 (9.1) 9 (11.4)
Physical and emotional challenges 3 (11.5) 2 (22.2) 0 (0) 5 (6.3)
Caregiver/Support systems 3 (11.5) 1 (11.1) 6 (13.6) 10 (12.7)
Total 26 (32.9) 9 (11.4) 44 (55.7) 79 (100)
Impressively, as a result of the study,the hospital elected to make
the patient navigator position a full-time, permanent position.
20 JUNE 2012 • VOLUME 3, ISSUE 3 AONNONLINE.ORG

ORIGINAL RESEARCH
participate in the study. This low accrual ratemight be attributed to patient skepticismregarding participation in research, the timerequired to complete the baseline assessment,and limited training of the navigator in thenature and value of research and the researchprocess. More training in study recruitmentmight have been helpful since the patient nav-igator did not have previous experience inbehavioral research. In scenarios in which thereis limited or no experience in behavioralresearch, patient navigator training shouldinclude modules discussing the understandingof research, the value of conducting research,the role of research protocols, and the impor-tance of accrual and program fidelity. Although patients were satisfied, and the nav-
igator addressed some of the critical issuesregarding access to care, the evaluation resultssuggest that issues need to be addressed, includ-ing providing and connecting cancer patients toappropriate information to improve their under-standing of their diagnosis and recommendedtreatments and identifying where the integra-tion of clinical navigation is essential. In addi-tion, more attention to the assessment of psy-chosocial issues, such as the patients’ emotionalworries, and more comprehensive training inthese areas would enhance navigation programs. As patient navigation in cancer care becomes
a standard component of patient-centered care,it is important to explore the various models ofnavigation and evaluate the adaptation ofpatient navigation functions across the cancer
continuum. The large, NCI-funded PatientNavigation Research Program studies willundoubtedly fill existing empirical gaps on theimpact, cost-effectiveness, and sustainability ofnavigator programs.11,16,17 In addition, there is aneed to evaluate the feasibility of implementingpatient navigation programs at the communitylevel18-20 as this is still where much cancer careis delivered. This study and others will provide
valuable information to determine the re -sources, both in personnel and infrastructure,that are necessary to promote sustainability inthe real-world, community setting.11 As patientnavigation is emerging as a viable interventionto reduce patient, provider, and systems barri-ers,11 it is important to explore how to expandthese programs to systematically assess andaddress the broad array of psychosocial issuesthat face patients along their journey from diag-nosis to survivorship. g
Table 3 Mean (SD) Patient Satisfaction Scores of Navigator Services Provided( (0 = "Not at all satisfied" to 4 = "Highly satisfied")
Satisfaction Measure Items 4 Weeks 12 Weeks
Seeking cancer-related information 3.3 (1.3) 3.5 (1.2)
Getting medical services 3.1 (1.5) 3.6 (1.8)
Taking care of insurance-related problem 2.5 (1.9) 3.6 (1.8)
Scheduling recommended appointments 2.5 (1.8) 3.4 (1.3)Getting community services 2.7 (1.8) 3.6 (1.3)
Being sensitive to cultural needs 2.8 (1.8) 3.7 (1.6)
Handling family needs at home 2.2 (1.9) 3.1 (1.3)
Answering any concerns 3.1 (1.6) 3.6 (1.7)
Dealing with other responsibilities 2.3 (1.9) 3.4 (1.8)
Overall mean across items 2.7 (1.7) 3.5 (1.6)
As patient navigation in cancer carebecomes a standard component ofpatient-centered care, it is important toexplore the various models of navigationand evaluate the adaptation of patientnavigation functions across the cancercontinuum.
AONNONLINE.ORG JOURNAL OF ONCOLOGY NAVIGATION & SURVIVORSHIP 21
ORIGINAL RESEARCH
Table 4 Improvement of Cognitive-Affective Measures at 3 Assessment Points (1 = “Not at all” to 5 = “Extremely”)
ItemsBaselineMean (SD)
4 WeeksMean (SD)
12 WeeksMean (SD)
How well do you understand the treatment proceduresthat were recommended (eg, radiation, chemotherapy)and why it is recommended that you have them?(Knowledge)
3.63 (1.09) 3.82 (0.95) 3.97 (0.95)*
How well do you understand the side effects of your recommended cancer treatments? (Knowledge)
3.48 (1.17) 3.48 (1.02) 3.88 (1.19)*
How worried are you about your cancer diagnosis?(Worry)
3.75 (1.30) 2.93 (1.56)* 2.94 (1.64)*
How worried are you about having pain or discomfortfrom the cancer treatments? (Worry)
3.91 (1.20) 3.23 (1.57)* 3.27 (1.61)*
How worried are you about how your life will change as a result of your cancer diagnosis? (Worry)
3.59 (1.34) 2.70 (1.49)* 2.82 (1.49)*
How embarrassed are you about having cancer?(Worry)
2.41 (1.58) 1.75 (1.35)* 1.48 (1.00)*
How important is it to stick to the treatment plan (eg, come to all scheduled treatment appointments and not skip any appointments)? (Beliefs)
4.73 (0.50) 4.95 (0.21)* 4.97 (0.17)*
How important is it for you to follow through with allof your doctor’s recommendations? (Beliefs)
4.77 (0.42) 5.00 (0.00)* 4.94 (0.24)
How important is it to your family that you get yourcancer treatment? (Beliefs)
4.80 (0.46) 4.95 (0.21)* 5.00 (0.00)*
How well do you have ways to manage any distress you may be experiencing about your cancer diagnosis or treatments? (Self-efficacy)
3.14 (1.09) 4.12 (1.03)* 4.12 (1.17)*
How well do you have ways to manage the cost of thecancer treatment appointments? (Self-efficacy)
3.00 (1.31) 4.07 (1.13)* 4.21 (1.11)*
How well do you have ways of getting referral lettersyou might need for insurance purposes? (Self-efficacy)
3.30 (1.39) 4.35 (0.98)* 4.39 (1.03)*
How well do you have ways to make sure you will remember your treatment and follow-up appointments? (Self-efficacy)
4.09 (1.01) 4.84 (0.43)* 4.70 (0.73)*
How well do you have ways to manage your otherresponsibilities, such as getting childcare or eldercare, or covering yourself at work, so that you can keep yourmedical appointments? (Self-efficacy)
3.50 (1.49) 4.45 (0.83)* 4.74 (0.54)*
*Indicates a statistically different mean compared to baseline mean.
22 JUNE 2012 • VOLUME 3, ISSUE 3 AONNONLINE.ORG
ORIGINAL RESEARCH
CORRESPONDING AUTHORSuzanne Miller, PhDSenior Member and ProfessorDirector, Psychosocial and BiobehavioralMedicine ProgramFox Chase Cancer CenterRobert C. Young Pavilion333 Cottman Ave. - 4th FloorPhiladelphia, PA 19111Tel: 215-728-4069Fax: 215-214-1651Email: [email protected]
DISCLOSURE OF FUNDINGThis work was supported by a grant from thePennsylvania Department of Health (SAP
ACKNOWLEDGMENTSThe authors want to acknowledge the efforts ofeach implementation site, especially project coor-dinators and patient navigators. In addition, weacknowledge the support of Fox Chase CancerCenter’s Behavioral Core Facility and the Officeof Health Communications & Health Disparities.
REFERENCES1. Miller SM, Bowen DJ, Croyle RT, et al, eds. Handbook ofCancer Control and Behavioral Science: A Resource forResearchers, Practitioners, and Policy Makers. Washington, DC:American Psychological Association; 2009.2. Miller SM, Diefenbach MA. C-ship: a cognitive-socialhealth information processing approach to cancer. In: Krantz D,ed. Perspectives in Behavioral Medicine. Mahwah, NJ: LawrenceErlbaum; 1998.3. Miller SM, Shoda Y, Hurley K. Applying cognitive-socialtheory to health-protective behavior: breast self-examination incancer screening. Psychol Bull. 1996;119:70-94.4. Thompson FE, Midthune D, Subar AF, et al. Developmentand evaluation of a short instrument to estimate usual dietaryintake of percentage energy from fat. J Am Diet Assoc.2007;107:760-767.
5. Freeman HP, Muth BJ, Kerner JF. Expanding access to cancerscreening and clinical follow-up among the medically under-served. Cancer Pract. 1995;3:19-30.6. Esparza A, Calhoun E. Measuring the impact and potentialof patient navigation: proposed common metrics and beyond.Cancer. 2011;117(suppl 15):3535-3536.7. Burstein HJ Jr. What is a patient navigator, and should wehave them in major cancer centers? J Natl Compr Canc Netw.2009;7:905.8. Dohan D, Schrag D. Using navigators to improve care ofunderserved patients: current practices and approaches. Cancer.2005;104:848-855.9. Wells KJ, Battaglia TA, Dudley DJ, et al. Patient navigation:state of the art or is it science? Cancer. 2008;113:1999-2010.10. Cancer Prevention and Treatment Demonstration forEthnic and Racial Minorities. Centers for Medicare &Medicaid Services Web site. URL Published February 8, 2011.Accessed May 31, 2012.11. Freund KM, Battaglia TA, Calhoun E, et al. NationalCancer Institute Patient Navigation Research Program: meth-ods, protocol, and measures. Cancer. 2008;113:3391-3399.12. Fleisher L, Kornfeld J, Davis S, et al. The NCI’s CancerInformation Service’s Research Continuum Framework: inte-grating research into cancer education practice (1999-2004). J Cancer Educ. 2007;22(suppl 1):S41-S48.13. Israel BA, Eng E, Schulz A, et al, eds. Methods inCommunity-Based Participatory Research for Health. SanFrancisco, CA: Jossey-Bass; 2005.14. Minkler M, Wallerstein N, eds. Community-BasedParticipatory Research for Health. San Francisco, CA: Jossey-Bass; 2003.15. Steinberg ML, Fremont A, Khan DC, et al. Lay patientnavigator program implementation for equal access to cancercare and clinical trials: essential steps and initial challenges.Cancer. 2006;107:2669-2677.16. Ferrante JM, Chen PH, Kim S. The effect of patient navi-gation on time to diagnosis, anxiety, and satisfaction in urbanminority women with abnormal mammograms: a randomizedcontrolled trial. J Urban Health. 2008;85:114-124.17. Ramsey S, Whitley E, Mears VW, et al. Evaluating the cost-effectiveness of cancer patient navigation programs: conceptualand practical issues. Cancer. 2009;115:5394-5403.18. Freeman HP. Patient navigation: a community based strategyto reduce cancer disparities. J Urban Health. 2006;83:139-141.19. Freeman HP. Patient navigation: a community centeredapproach to reducing cancer mortality. J Cancer Educ.2006;21(suppl 1):S11-S14.20. Nguyen TT, McPhee SJ, Bui-Tong N, et al. Community-based participatory research increases cervical cancer screeningamong Vietnamese-Americans. J Health Care Poor Underserved.2006;17(suppl 2):31-54.
AONNONLINE.ORG JOURNAL OF ONCOLOGY NAVIGATION & SURVIVORSHIP 23
Visit our user-friendly Web site
www.AONNonline.orgIn addition to Web-only exclusives, news coverage, journal articles,
contests, and polling questions, you’ll have the opportunity to participate in a number of activities offered!

Third Annual Navigation andSurvivorship Conference
Friday, September 1412:45 – 1:00pm Welcome
Conference Co-Chairs:Sharon Gentry, RN, MSN, AOCN, CBCNLillie D. Shockney, RN, BS, MAS
1:00 – 2:00pm Pre-Conference Workshops& Beginners Track
2:15 – 3:15pm • Core Principles of NavigationNicole Messier, RN, BSN Pamela J. Vlahakis, RN, MSN, CBCNMembers• Getting Excited about Research – Case Examples Linda Fleisher, PhD, MPH Elaine Sein, RN, BSN, OCN, CBCN
• Panel Discussion: Building Optimal Community Outreach – Lay and Community Jean B. Sellers, RN, MSN (Moderator)Leah Leilani Beck, BSJessica Denton, MSW
• Implementing a Survivorship Program/ClinicCynthia Waddington, RN, MSN, AOCN
3:15 – 3:30pm Break3:30 – 5:00pm Administrators Track
• Administering a Navigation Program Bonnie J. Miller, RN, BSN, OCN, FAAMAElizabeth Whitley, PhD, RN Navigators Track• How Do Case Managers and Navigators Interface?Nancy Skinner, RN-BC, CCM
5:00 – 6:00pm FREE TIME6:00 – 8:00pm Welcome Reception/Posters in the Exhibit Hall
Saturday, September 157:30 – 8:30am Breakfast Symposium/Product Theater8:30 – 8:45am Welcome & Introductions
Conference Co-Chairs8:45 – 9:45am General Session 1: Navigation Update: 2012
Current Regulations – Navigation & Survivorship Care Plan Linda Ferris, PhD
9:45 – 10:00am Break10:00 – 11:30am Disease-Site–Specific Breakouts
Stand-Alone Sessions• Breast Cancer NavigationMary Rooney, RN, BSN, OCN
• Thoracic Oncology NavigationPamela Matten, RN, BSN, OCN
• GI Cancer NavigationCoralyn Martinez, MSN, RN, OCN
• Colorectal Cancer NavigationMaura Kadan, RN, MSN, OCN
• GYN Cancer NavigationRobin A. Atkinson, RN, BSN, OCN
PRELIMINARY AGENDA* • Prostate Cancer NavigationJuli Aistars, RN, MS, APN, AOCNRapid Fire Sessions with Panel• Head, Neck, & Neuro NavigationHeather Stern, RN, BSN, CNOR, OCNAnd
• Hematology/OncologyTina Scherer, RN, MSN, OCNAdministrators Session • The Role of the AdministratorLisa Shalkowski, RN, BSN, MSM
11:45 – 1:00pm Lunch in the Exhibit Hall1:15 – 2:15pm Advocacy Keynote
TBD2:15 – 3:15pm General Session 2: Best Practices in
Survivorship Care RehabilitationJulie Silver, MD
3:15 – 4:15pm General Session 3: Plenary SessionFinancial and Legal Issues for Our Cancer PatientsDavid S. Landay, JD
4:15 – 5:00pm The Art of Exceptional Professional Performance– Making a Difference in Your Patients’ LivesSelinza Mitchell, RN
5:00 – 7:00pm Poster Award Reception in the Exhibit HallPamela Matten, RN, BSN, OCN
7:00pm Conclusion of Day – Networking FREE TIME
Sunday, September 167:30 – 8:30am Breakfast Symposium/Product Theater8:30 – 9:30am General Session 4: Navigation in the Age of
Personalized Cancer CareSharon Gentry, RN, MSN, AOCN, CBCNLillie D. Shockney, RN, BS, MAS
9:30 – 10:30am General Session 5: Best Practices in AddressingHealth InequitiesLauren Kelley, MSW, MPA Adrienne Lofton, RN, MSN
10:30 – 10:45am Break10:45 – 12:15pm Practice Setting – Panel Discussion with
Moderator• Office-Based
Roxanne Parker, RN, MSN, CPN (Moderator)• AcademicBonnie J. Miller, RN, BSN, OCN, FAAMA
• Community Hospital–BasedKaryl Blaseg, RN, MSN, OCN
12:15 – 1:15pm Lunch in the Exhibit Hall1:30 – 2:30pm Clinical Survivorship Guidance
Mandi Pratt-Chapman, MAKatherine Sharpe, MTS
2:30 – 2:45pm Conclusion/Final RemarksConference Co-Chairs
*Preliminary agenda, subject to change.
s c
� � �� �� � �� �

Register online: www.regonline.com/aonn2012CONFERENCE REGISTRATIONSeptember 14-16, 2012
Phoenix, Arizona Arizona Grand
E
B
Breast Health NavigatorDerrick L. Davis ForsythRegional Cancer CenterWinston-Salem, NC
University Distinguished Associate Professor of Breast CancerAdm Director, Johns Hopkins Clinical Breast ProgramsAdm Director, Johns Hopkins Cancer Survivorship ProgramsDepts of Surgery and OncologyAssociate Professor, JHU School of Medicine,Depts of Surgery, Oncology and GynecologyAssociate Professor, JHU School of NursingJohns Hopkins Avon Foundation Breast CenterBaltimore, MD
Sharon Gentry, RN, MSN, AOCN,CBCN
Lillie D. Shockney, RN, BS, MAS
CONFERENCE CO-CHAIRS
Juli Aistars, RN, MS, APN, AOCN
Robin A. Atkinson, RN, BSN, OCN
Leah Leilani Beck, BS
Karyl Blaseg, RN, MSN, OCN
Jessica Denton, MSW
Linda Ferris, PhD
Linda Fleisher, PhD, MPH
Maura Kadan, RN, MSN, OCN
Lauren Kelley, MSW, MPA
David S. Landay, JD
Adrienne Lofton, RN, MSN
Coralyn Martinez, MSN, RN, OCN
Pamela Matten, RN, BSN, OCN
Nicole Messier, RN, BSN
Bonnie J. Miller, RN, BSN, OCN,FAAMA
Roxanne Parker, RN, MSN, CPN
Mandi Pratt-Chapman, MA
Mary Rooney, RN, BSN, OCN
Tina Scherer, RN, MSN, OCN
Elaine Sein, RN, BSN, OCN, CBCN
Jean B. Sellers, RN, MSN
Lisa Shalkowski, RN, BSN, MSM
Katherine Sharpe, MTS
Julie Silver, MD
Nancy Skinner, RN-BC, CCM
Heather Stern, RN, BSN, CNOR, OCN
Pamela J. Vlahakis, RN, MSN, CBCN
Cynthia Waddington, RN, MSN, AOCN
Elizabeth Whitley, PhD, RN
FACULTY*
*For full information visit www.aonnonline.org
AONN’s Third Annual Conference will continue to advance the nav-igation profession by expanding the scope of educational sessions, net-working opportunities, and poster presentations. In addition, this year’sconference will address the evolving challenges of program improve-ment, the role of personalized medicine, and implementing best prac-tices in navigation, survivorship, and psychosocial care.
CONFERENCE OVERVIEW
AONN’s Third Annual Conference is the only meeting that gives youaccess to decision-makers and key practitioners involved in oncologynavigation and survivorship. If your company provides any of the fol-lowing services/products for the oncology healthcare community, thisis the meeting for you.
• Pharmaceutical/Biotech• Genetic Laboratory Services• Navigation Software• Patient Advocacy• Training
TARGET AUDIENCE
• Patient Access• Reimbursement• Publishers• Education• Certification
This educational initiative is directed toward oncology nurse nav-igators, patient navigators, and social workers.
GoalAONN’s Third Annual Navigation and Survivorship Conferencewill advance the role of navigation and survivorship in cancer careto ultimately improve the quality of patient care.
Objectives• Discuss the evolution of the role of navigation in healthcare
• Assess strategies for navigating diverse patient populations by cancer type and environmental factors
• Define methods for providing patient support and guidance in the age of personalized cancer care
• Evaluate best practices regarding survivorship and psychosocial care
CONTINUING EDUCATION INFORMATION
This is an opportunity to share research, programs, and results withyour colleagues. Submit your abstract via e-mail to [email protected] Deadline: August 1, 2012
CALL FOR ABSTRACTS
Medical Learning Institute, Inc.Provider approved by the California Board of Registered Nursing,Provider Number 15106, for up to 12.25 contact hours.
REGISTERED NURSE DESIGNATION
This activity is pending approval from the National Association of SocialWorkers. Contact hours for this continuing social worker education activ-ity have been submitted to the National Association of Social Workers.
SOCIAL WORK DESIGNATION
This activity is jointly sponsored by AONN Foundation for Learning, Inc.,Center of Excellence Media, LLC, and Medical Learning Institute, Inc.
SPONSORS
*Early Bird Rate: $295Includes Membership through September 30, 2013.
Conference Registration: $345Includes Membership through September 30, 2013.
*Early bird expires August 1, 2012.
� � �� �� � �� �

WEB SITEREVIEW
AONNONLINE.ORG JOURNAL OF ONCOLOGY NAVIGATION & SURVIVORSHIP 26
T he Patient Advocate Foundation (PAF)states that their mission is to provide effec-tive mediation and arbitration services to
patients to remove obstacles to healthcare, includ-ing medical debt crisis, insurance access issues, andemployment issues for patients with chronic,debilitating, and life-threatening illnesses. There are many services and programs offered
to patients via PAF, and today we highlight oneof particular pertinence to oncology nurse navi-gators: case management.
PAF’s professional case managers and attor-neys specialize in mediation, negotiation, andarbitration to advocate on behalf of patients fac-ing specific issues with their insurer, employer,and/or creditor regarding access to care, insur-ance, job retention, and/or debt crisis matters rel-ative to their diagnosis of life-threatening ordebilitating disease. In addition to direct case management assis-
tance, PAF provides the programs and partnershipslisted below:
VIRGINIA CARES UNINSURED Program—read more for those of you in the state of VirginiaVirginia Cares Uninsured Program (VCUP) is acollaborative effort between PAF and theCommonwealth of Virginia to provide dedicatedcase management services to individuals through-out the state of Virginia who are diagnosed with achronic, life-threatening, and/or debilitating ill-ness and who are experiencing access-to-health-care issues. VCUP case managers provide assis-tance to Virginians requiring access to care,medications, and transportation for treatment, aswell as issues involving insurance appeals, benefitexclusions, and copays. Case managers assist patients with applying
for, expediting, and appealing Social Security
Disability Insurance (SSDI), SupplementalSecurity Income (SSI), Long-Term Disability(LTD) and/or Short-Term Disability (STD). Theynegotiate funding and/or insurance coverage toaccess medical devices, surgical procedures, andmedications. They also arbitrate with facilities toobtain medical discounts and/or write-offs for serv-ices. Case managers also mediate access to free orreduced medication, nutrition, housing, utilities,and free or reduced transportation and lodging forpatients who must travel for treatment. They also address COBRA, Medicaid, Medicare, andHIPAA plan issues relating to a patient’s diagnosis.
PAF/AMERICAN CANCER SOCIETYPARTNERSHIPPAF has partnered with the American CancerSociety to provide case management services topatients nationwide who have been diagnosedwith cancer or are being screened for symptoms ofcancer. PAF provides extended services topatients experiencing healthcare issues to includeinsurance, debt crisis, employment, and/or out-
www.PatientAdvocate.orgPAF – PATIENT ADVOCATEFOUNDATION: Solving insurance and healthcare access problems since 1996By Lillie D. Shockney, RN, BS, MAS
PAF’s professional case managers andattorneys specialize in mediation, nego-tiation, and arbitration to advocate onbehalf of patients facing specific issueswith their insurer, employer, and/orcreditor regarding access to care, insur-ance, job retention, and/or debt crisismatters relative to their diagnosis oflife-threatening or debilitating disease.
WEB SITEREVIEW
27 JUNE 2012 • VOLUME 3, ISSUE 3 AONNONLINE.ORG
of-pocket expenses related to cancer diagnosisand treatment. The dedicated PAF case managers assist
patients with insurance appeals, copays forchemotherapy treatment and medications, trans-portation to and from treatment, debt crisis inrelation to the patient’s diagnosis, preauthoriza-tions, enrollment and/or eligibility for state- andfederal-funded programs (Medicare or Medicaid),billing/coding errors, and unpaid medical debt.
PAF/LIVESTRONG PARTNERSHIPPAF has partnered with LIVESTRONG to pro-vide direct case management services to patientsnationwide who have been diagnosed with can-cer or are in need of cancer screening. PAF pro-vides extended services to patients experiencinghealthcare issues to include insurance, debt crisis,employment, and/or out-of-pocket expensesrelated to cancer diagnosis and treatment. The dedicated PAF case managers assist
patients nationwide with insurance appeals,preauthorizations, billing/coding errors, and assis-tance with unpaid medical debt to include co-pays for chemotherapy treatment and medications.
PAF assists the uninsured and under insured withaccessing care and debt crisis situations due to apatient’s diagnosis. Case managers are availableto assist patients with eligibility for state- andfederal-funded programs such as Medicare,Medicaid, and Social Security DisabilityInsurance.
SURVIVORSHIP OF CANCERS INUNDERSERVED POPULATIONSPAF was awarded a grant by the Centers forDisease Control and Prevention for educationand outreach to underserved populations. Thediseases that fall under this grant are breast, cer-vical, ovarian, prostate, and colorectal cancers,along with melanoma (skin cancer).The dedicated PAF case managers assist patients
nationwide with insurance appeals, preauthoriza-tions, billing/coding errors, and assistance withunpaid medical debt to include co-pays forchemotherapy treatment and medications. PAFassists the uninsured and underinsured with access-ing care and debt crisis situations due to a patient’sdiagnosis. Case managers are available to assistpatients with eligibility for state- and federal-fund-ed programs such as Medicare, Medicaid, andSocial Security Disability Insurance. g
Please take the time to visit this website andsee the wealth of information and resources avail-able to you and your cancer patients or reachthem at the following address or phone number:
Patient Advocate [email protected] Butler Farm RoadHampton, VA 23666Tel: 800-532-5274Fax: 757-873-8999
The dedicated PAF case managersassist patients nationwide with
insurance appeals, preauthorizations,billing/coding errors, and assistancewith unpaid medical debt to include co-pays for chemotherapy treatment
and medications.
Visit our user-friendly Web site
www.AONNonline.orgIn addition to Web-only exclusives, news coverage, journal articles,
contests, and polling questions, you’ll have the opportunity to participate in a number of activities offered!

PriorityConsult®
Oncology Patient Navigation & Clinical Tracking Software
Priority Consult Oncology Your Solution for Patient NavigationPriority Consult Oncology Navigation assists navigators, clinicians and staff in directing & tracking a patient through the entire care continuum - designed for ease of use in a complicated field.
Interface with other applications to save t ime
Easily report cancer center quality indicators
Support tumor board with custom patient summaries
Navigate any cancer type
Design custom reports
Generate treatment summary documents & survivorship plans
Create referring physician communication documents
www.priorityconsult .comSchedule a software demonstration today. Visit www.priorityconsult.com or call 1.866.396.1445.
Don’t have a systematic approach to patient navigation?Need a way to easily view the status and next step of every patient within your program?
Priority Consult Oncology
Priority Consult Oncology
Priority Consult Oncology
Priority Consult Oncology
Priority Consult Oncology Navigation assists navigators,
Navigationo YYour Solution for Patient
Priority Consult Oncology
Priority Consult Oncology Navigation assists navigators,
Navigationour Solution for Patient
Priority Consult Oncology
Priority Consult Oncology Navigation assists navigators,
our Solution for Patient Priority Consult Oncology
Priority Consult Oncology Navigation assists navigators,
our Solution for Patient logy
patient within your program?status and next step of every Need a way to easily view the navigation?approach to patient Don’t have a systematic
complicated field.the entire care continuum - designed for ease of use in a
Priority Consult Oncology Navigation assists navigators,
patient within your program?status and next step of every Need a way to easily view the
approach to patient Don’t have a systematic
complicated field.the entire care continuum - designed for ease of use in a
Priority Consult Oncology Navigation assists navigators,
snoitacilppatiwecafretnI
the entire care continuum - designed for ease of use in a
Priority Consult Oncology Navigation assists navigators,
emitevasotrehtoh
the entire care continuum - designed for ease of use in a
Priority Consult Oncology Navigation assists navigators,
patient within your program?
patient within your program?
eitapmotppsuc
omuttropt
pt
uS
cidp
niyty
ilauqtrop
dery
tlisaE
seirammustnhtiwdraobro
srotaretnecrecnact
aertetareneG
otsucngiseD
ynaetagivaN
yrammustnemta
stropermo
epytrecnac
y
PriorPPPPPP
C
yritty
®onsultC
®
itacinummocrreferetaerC
&stnemucodaertetareneG
stnemucod
pno
naicisyhpd
gnir
ly
ppihsrovivrus&yl
rammustnemta
snalyyl
C
Schedule a software demonstration today
Oncology P
onsultC
Schedule a software demonstration today
vigation & Clinicatient Nagy P Patient Na
.priorityconsult.com or call 1.866.396.1445.
vigation & Clinicisit www. VSchedule a software demonstration today
.priorityconsult.com or call 1.866.396.1445.
acking Softrracking SoftTTral c cal
oc.tlusnocytiroirp.www
.priorityconsult.com or call 1.866.396.1445.
earrewwaracking Soft
mo


















