July/August 2010, Vol 3, No 4
64
REGULATORY Accountable Care Organizations in the Era of Healthcare Reform Interview with Mark B. McClellan, MD, PhD BUSINESS Expect the Unexpected: A Role for Behavioral Economics in Understanding the Impact of Cost-Sharing on Emergency Department Utilization Albert Tzeel, MD, MHSA; Jack Brown, BA Stakeholder Perspective by Alberto M. Colombi, MD, MPH Comparing Medical Cost of Care for Patients with Metastatic Breast Cancer Receiving Taxane Therapy: Claims Analysis Rex W. Force, PharmD; Brooke A. Pugmire, PharmD; Vaughn L. Culbertson, PharmD Stakeholder Perspective by Atheer A. Kaddis, PharmD CLINICAL Effectiveness of Anti-Tumor Necrosis Factor Agents in the Treatment of Rheumatoid Arthritis: Observational Study Anna D’Souza, PhD; Brian L. Meissner, PharmD, PhD; Boxiong Tang, MD, PhD; R. Scott McKenzie, MD; Catherine T. Piech, MBA Stakeholder Perspective by Matthew Mitchell, PharmD, MBA HEALTHCARE REFORM The New Accountable Care Organizations and Medicare Gain-Sharing Program Kip Piper, MA, FACHE The Impact of Healthcare Reform on Payers’ Products, Provider Reimbursement, and Member Engagement Sam Muppalla; Robert Capoblanco ◆ Generic Drug Trends ◆ Industry Trends ™ ©2010 Engage Healthcare Communications, LLC www.AHDBonline.com JULY/AUGUST 2010 VOLUME 3, NUMBER 4 THE PEER-REVIEWED FORUM FOR EVIDENCE IN BENEFIT DESIGN ™ FOR PAYERS, PURCHASERS, POLICYMAKERS, AND OTHER HEALTHCARE STAKEHOLDERS
-
Upload
dalia-buffery -
Category
Documents
-
view
229 -
download
0
description
American Health & Drug Benefits
Transcript of July/August 2010, Vol 3, No 4

©2009 Engage Healthcare Communications, LLCwww.AHDBonline.com
REGULATORY
Accountable Care Organizations in the Era of Healthcare ReformInterview with Mark B. McClellan, MD, PhD
BUSINESS
Expect the Unexpected: A Role for Behavioral Economics in Understanding theImpact of Cost-Sharing on Emergency Department UtilizationAlbert Tzeel, MD, MHSA; Jack Brown, BA
Stakeholder Perspective by Alberto M. Colombi, MD, MPH
Comparing Medical Cost of Care for Patients with Metastatic Breast CancerReceiving Taxane Therapy: Claims AnalysisRex W. Force, PharmD; Brooke A. Pugmire, PharmD; Vaughn L. Culbertson, PharmD
Stakeholder Perspective by Atheer A. Kaddis, PharmD
CLINICAL
Effectiveness of Anti-Tumor Necrosis Factor Agents in the Treatment ofRheumatoid Arthritis: Observational StudyAnna D’Souza, PhD; Brian L. Meissner, PharmD, PhD; Boxiong Tang, MD, PhD; R. Scott McKenzie,MD; Catherine T. Piech, MBA
Stakeholder Perspective by Matthew Mitchell, PharmD, MBA
HEALTHCARE REFORM
The New Accountable Care Organizations and Medicare Gain-Sharing ProgramKip Piper, MA, FACHE
The Impact of Healthcare Reform on Payers’ Products, Provider Reimbursement,and Member EngagementSam Muppalla; Robert Capoblanco
◆ Generic Drug Trends
◆ Industry Trends
™
©2010 Engage Healthcare Communications, LLCwww.AHDBonline.com
JULY/AUGUST 2010 VOLUME 3, NUMBER 4
THE PEER-REVIEWED FORUM FOR EVIDENCE IN BENEFIT DESIGN™
FOR PAYERS, PURCHASERS, POLICYMAKERS, AND OTHER HEALTHCARE STAKEHOLDERS

Image: Colored scanning electron micrograph (SEM) of a pancreatic cancer cell.
goal

©2010 Millennium Pharmaceuticals, Inc. All rights reserved.
To learn more, visit us at millennium.com.
One goal: discovering and delivering breakthrough medicines to combat cancer.
Now the innovative science of a leading American biopharmaceutical company joins
the global assets of Takeda, Japan’s largest pharmaceutical company, for a global
commitment to oncology.
Millennium: The Takeda Oncology Company is developing an extensive pipeline —
among the top in oncology worldwide — with more than 17 compounds in
development for a broad range of solid and hematological cancers.
Our pipeline — rich in novel compounds — includes multiple candidates that target
seven disease pathways: protein homeostasis, anti-angiogenesis, growth-signaling
inhibition, cell-cycle inhibition, apoptosis, immunomodulators and hormone regulation.
We are dedicated to a strong partnership with the oncology community. Together
we can make a dramatic impact on cancer therapeutics over the next decade.

236 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
EDITORIAL BOARD
CLINICAL EDITOR Thomas G. McCarter, MD, FACPChief Clinical OfficerExecutive Health Resources, PA
GOVERNMENT EDITORKevin B. “Kip” Piper, MA, FACHEPresident, Health Results GroupSr. Counselor, Fleishman-Hillard Washington, DC
ACTUARY David WilliamsMilliman Health ConsultantWindsor, CT
CANCER RESEARCHAl B. Benson, III, MD, FACPProfessor of MedicineAssociate Director for ClinicalInvestigationsRobert H. Lurie Comprehensive CancerCenter, Northwestern UniversityPresident, ACCCPast Chair, Board of Directors, NCCN
Samuel M. Silver, MD, PhD, FACPProfessor, Internal MedicineDirector, Cancer Center NetworkDivision of Hematology/OncologyAssistant Dean for ResearchUniversity of Michigan Health Systems
CARDIOLOGY RESEARCH Michael A. Weber, MDProfessor of MedicineDepartment of Medicine (Cardiology)State University of New York
ENDOCRINOLOGY RESEARCHJames V. Felicetta, MD Chairman, Dept. of Medicine Carl T. Hayden Veterans AffairsMedical Center, Phoenix, AZ
EMPLOYERSAlberto M. Colombi, MD, MPHCorporate Medical DirectorPPG Industries, Pittsburgh, PA
Wayne M. Lednar, MD, PhDGlobal Chief Medical OfficerDirector, Integrated Health ServicesDuPont, Wilmington, DE
Arthur F. Shinn, PharmD, FASCPPresident, Managed Pharmacy Consultants, Lake Worth, FL
F. Randy Vogenberg, RPh, PhDPrincipal, Institute of Integrated HealthcareSharon, MASenior Fellow, Jefferson School ofPopulation Health
EPIDEMIOLOGY RESEARCHJoshua N. Liberman, PhD Vice President, Strategic Research CVS Caremark, Hunt Valley, MD
Nirav R. Shah, MD, MPHAssistant Professor of MedicineNYU School of Medicine, NYCSenior Investigator, Geisinger HealthSystem, Danville, PA
HEALTH INFORMATION TECHNOLOGY J. B. Jones, PhD, MBAResearch Associate, Geisinger Health System, Danville, PA
Victor J. Strecher, PhD, MPHProfessor and Director, Center for HealthCommunications ResearchUniversity of Michigan Schools of PublicHealth and Medicine, Ann ArborFounder and Chief Visionary OfficerHealthMedia, Johnson & Johnson Co.
HEALTH OUTCOMES RESEARCH Gordon M. Cummins, MSDirector, IntegriChain
Kavita V. Nair, PhDAssociate Professor, School of PharmacyUniversity of Colorado at Denver
Gary M. Owens, MDPresident, Gary Owens AssociatesGlen Mills, PA
Timothy S. Regan, BPharm, RPhExecutive Director, XcendaPalm Harbor, FL
MANAGED CARE & GOVERNMENT AFFAIRSSharad Mansukani, MDChief Strategic Officer, Nations HealthSenior Advisor, Texas Pacific Group, FL
MANAGED MARKETS Jeffrey A. Bourret, MS, RPh, FASHPSenior Director, Customer Marketing & Innovation, US Specialty CustomersPfizer Specialty Business Unit, PA
Charles E. Collins, Jr, MS, MBAAssociate Director, Managed Markets Marketing, Boehringer-Ingelheim, CT
PATIENT ADVOCACY William E. Fassett, BSPharm, MBA, PhDProfessor of Pharmacy Law & EthicsVice Chair, Dept. of PharmacotherapyCollege of Pharmacy, Washington StateUniversity, Spokane, WA
PERSONALIZED MEDICINE Wayne A. Rosenkrans, Jr, PhDChairman and President, Personalized Medicine Coalition, Distinguished Fellow,MIT Center for Biomedical Innovation
PHARMACOECONOMICSJeff Jianfei Guo, BPharm, MS, PhDAssociate Professor of Pharmacoeconomics& Pharmacoepidemiology, College of Pharmacy, University of Cincinnati Medical Center, OH
PHARMACY BENEFIT DESIGN Joel V. Brill, MDChief Medical Officer, Predictive Health, Phoenix, AZ
William J. Cardarelli, PharmDDirector of PharmacyAtrius HealthHarvard Vanguard Medical Associates
Leslie S. Fish, PharmDSr. Director of Pharmacy ServicesFallon Community Health Plan, MA
Michael S. Jacobs, RPhNational Clinical Practice LeaderBuck Consultants, Atlanta
Paul Anthony Polansky, BSPharm, MBAFormer Executive VP and Chief PharmacyOfficer, Sanovia Corp., Philadelphia, PA
Scott R. Taylor, RPh, MBAAssociate Director, Industry RelationsGeisinger Health System, Danville, PA
POLICY & PUBLIC HEALTH Joseph R. Antos, PhDWilson H. Taylor Scholar in Health CareRetirement PolicyAmerican Enterprise Institute
Jack E. Fincham, PhD, RPh Professor of Pharmacy, School of PharmacyUniversity of Missouri, Kansas City
Alex Hathaway, MD, MPH, FACPMPresident & Founder, J.D. BioEdgeHealth quality and biomedical research consultancy
J. Warren Salmon, PhDProfessor of Health Policy & AdministrationSchool of Public HealthUniversity of Illinois at Chicago
REIMBURSEMENT POLICYGrant D. Lawless, BSPharm, MD, FACPExecutive Director for Payor RelationsCorporate Account, Amgen, CA
RESEARCH & DEVELOPMENT Michael F. Murphy, MD, PhDChief Medical Officer and Scientific Officer Worldwide Clinical TrialsFaculty, Center for Experimental Pharmacology and Therapeutics, Harvard-MIT Division of Health Sciences andTechnology, Cambridge, MA
SPECIALTY PHARMACYAtheer A. Kaddis, PharmDVice President, Managed MarketsDiplomat Specialty PharmacySwartz Creek, MI
James T. Kenney, RPh, MBAPharmacy Operations Manager Harvard Pilgrim Health Care, Wellesley, MA


238 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
PublisherNicholas [email protected]
Associate PublisherMaurice [email protected]
Editorial DirectorDalia [email protected]
Associate EditorLara J. [email protected]
Editorial AssistantJessica A. Smith
Senior Production ManagerLynn Hamilton
Business ManagerBlanche Marchitto
Editor-in-ChiefRobert E. [email protected]
American Health & Drug Benefits is foundedon the concept that health and drug benefitshave undergone a transformation: the econo -metric value of a drug is of equal importanceto clinical outcomes as it is to serving as thebasis for securing coverage in formularies andbenefit designs. Because benefit designs aregreatly affected by clinical, business, and pol-icy conditions, this journal offers a forum forstakeholder integration and collaborationtoward the improvement of healthcare.
This publication further provides benefitdesign de cision makers the integrated industryinformation they require to devise formulariesand benefit designs that stand up to today’sspecial healthcare delivery and business needs.
Contact Information:For reprints, subscription information, andeditorial queries, please contact:[email protected]
T: 732-992-1892F: 732-992-1881
Mission Statement
REGULATORY
242 Accountable Care Organizations in the Era of Healthcare ReformInterview with Mark B. McClellan, MD, PhD
BUSINESS
248 Expect the Unexpected: A Role for Behavioral Economics in Understanding theImpact of Cost-Sharing on Emergency Department UtilizationAlbert Tzeel, MD, MHSA; Jack Brown, BA
255 Stakeholder Perspective by Alberto M. Colombi, MD, MPH
276 Comparing Medical Cost of Care for Patients with Metastatic Breast CancerReceiving Taxane Therapy: Claims AnalysisRex W. Force, PharmD; Brooke A. Pugmire, PharmD; Vaughn L. Culbertson, PharmD
284 Stakeholder Perspective by Atheer A. Kaddis, PharmD
CLINICAL
266 Effectiveness of Anti-Tumor Necrosis Factor Agents in the Treatment ofRheumatoid Arthritis: Observational StudyAnna D’Souza, PhD; Brian L. Meissner, PharmD, PhD; Boxiong Tang, MD, PhD; R. ScottMcKenzie, MD; Catherine T. Piech, MBA
273 Stakeholder Perspective by Matthew Mitchell, PharmD, MBA
TABLE OF CONTENTS
Continued on page 240
American Health & Drug Benefits is included in the following indexing and database services:EMBASE/ElsevierCumulative Index to Nursing and Allied Health Literature (CINAHL)EBSCO research databasesStandard Periodical Directory
JULY/AUGUST 2010 VOLUME 3, NUMBER 4
™ ™
THE PEER-REVIEWED FORUM FOR EVIDENCE IN BENEFIT DESIGN™
FOR PAYERS, PURCHASERS, POLICYMAKERS, AND OTHER HEALTHCARE STAKEHOLDERS

We focus on the humanin human health care
© 2009 Eisai Inc. CO-0100-0905
At Eisai (a•zi), caring for people is our work
Satisfying unmet medical needs and increasing benefits to patients, their families,
and caregivers is Eisai’s human health care (hhc) mission.
This includes the development of innovative medicines–notably the discovery
of the world’s most widely used treatment for Alzheimer’s disease.
Eisai is recognized for our business and patient advocacy partnerships,
as well as our commitment to working with healthcare professionals
to achieve improved patient care worldwide.
That is our quest. That is our promise. That is what makes us Eisai.
Ingenuity that Drives Innovationin Neurology, GI Disorders,
and Oncology/Critical Care
Visit us at www.eisai.com, or 1-888-274-2378

240 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
JULY/AUGUST 2010 VOLUME 3, NUMBER 4
American Health & Drug Benefits, ISSN 1942-2962 (print); ISSN 1942-2970 (online), ispublished 6 times a year by Engage HealthcareCommunications, LLC, 241 Forsgate Drive,Suite 205A, Monroe Township, NJ 08831.Copyright © 2010 by Engage Healthcare Communications, LLC. All rights reserved.American Health & Drug Benefits and The Peer-Reviewed Forum for Evidence in BenefitDesign are trademarks of Engage HealthcareCommunications, LLC. No part of this publication may be reproduced or transmittedin any form or by any means now or hereafterknown, electronic or mechanical, includingphotocopy, recording, or any informationalstorage and retrieval system, without writtenpermission from the Publisher. Printed in theUnited States of America.
Address all editorial correspondence to: [email protected]. Telephone: 732-992-1892. Fax: 732-992-1881.American Health & Drug Benefits, 241 ForsgateDrive, Suite 205A, Monroe Township, NJ 08831.
Permission requests to reprint all or part of anyarticle published in this journal should be addressed to PERMISSIONS DEPARTMENT.Fax: 732-992-1881.
The ideas and opinions expressed in AmericanHealth & Drug Benefits do not necessarily reflect those of the Editorial Board, the Editors,or the Publisher. Publication of an advertise-ment or other product mentioned in American Health & Drug Benefits should not beconstrued as an endorsement of the product orthe manufacturer’s claims. Readers are encour-aged to contact the manufacturers about anyfeatures or limitations of products mentioned.Neither the Editors nor the Publisher assumeany responsibility for any injury and/or damageto persons or property arising out of or related to any use of the material mentionedin this publication.
POSTMASTER: CORRESPONDENCE REGARDING SUBSCRIPTIONS ORCHANGE OF ADDRESS should be directedto CIRCULATION DIRECTOR, AmericanHealth & Drug Benefits, 241 Forsgate Drive,Suite 205A, Monroe Township, NJ 08831.Fax: 732-992-1881. YEARLY SUBSCRIPTIONRATES: One year: $99.00 USD; Two years:$149.00 USD; Three years: $199.00 USD.
™ ™
HEALTHCARE REFORM
261 The New Accountable Care Organizations and Medicare Gain-Sharing ProgramKip Piper, MA, FACHE
289 The Impact of Healthcare Reform on Payers’ Products, Provider Reimbursement,and Member EngagementSam Muppalla; Robert Capoblanco
DEPARTMENTS
274 GENERIC DRUG TRENDSEnhanced Generic Utilization Saved US Healthcare $139.6 Billion in 2009Dalia Buffery, MA, ABD
292 INDUSTRY TRENDS
The Current State of Bundled PaymentsJim Evans CAPTION CONTEST
TABLE OF CONTENTS (Continued)
THE PEER-REVIEWED FORUM FOR EVIDENCE IN BENEFIT DESIGN™
FOR PAYERS, PURCHASERS, POLICYMAKERS, AND OTHER HEALTHCARE STAKEHOLDERS
WEB EXCLUSIVE www.AHDBonline.com
GI Drugs in Late Development: DDW 2010By Alice Goodman

Copyright ©2010, Boehringer Ingelheim Pharmaceuticals, Inc. All rights reserved. (06/10) DI77201MHC-A
exploring DIABETES
inspired to make a
DIFFERENCE

REGULATORY
242 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
Kip Piper, MA, FACHE: You and your colleagueswere influential in developing the ACO concept1 and suc-cessfully persuading Congress to make ACOs an option inMedicare. Are you surprised by the tremendous interest inACOs since enactment of the PPACA this year?
Mark B. McClellan, MD, PhD: There has been areal expansion of interest in ACOs recently, and someof that is not surprising. The key ideas behind account-able care have been around for a while. CMS hasimplemented some Medicare demonstration programspreviously that potentially use ACO concepts, and anumber of private payers and providers have beenworking on ACO implementation as well. I have beena bit surprised by the breadth of interest. It is a reflec-tion of how seriously providers and payers are takingthe healthcare reform law. However, unlike many of the other provisions on
payment reform, ACOs will be a real part of Medicareas of 2012, if not earlier; not a pilot, not a demo, but apart of the Medicare program. That may be contribut-ing to the interest too. And finally, there is growinginterest in making sure that payment policies fit togeth-
er to add up to getting better value, getting higher qual-ity, and avoiding unnecessary costs. That’s contributingto the interest in ACOs. It is a confluence of factors,and in retrospect I should not be so surprised by theintense interest in the ACO model.
Piper: What are some of the factors critical to success-fully implementing an ACO?
McClellan: One is a critical mass of providers whoare willing and able to meaningfully take accountabili-ty for the well-being of a population of patients. Thisincludes a primary care network and other types ofhealthcare providers, maybe even some providers whoare involved in things that are not traditionallythought of as healthcare, such as wellness programs andpopulation health management. But the key thing isthat there is a critical mass of providers who are willingto work together and are able to take meaningful stepsto get to better health for those beneficiaries.Second, there also is a need for a critical mass of pay-
ers. There needs to be enough reform in the way pay-ments work so that steps that traditionally do not makemuch financial sense—such as promoting better coordi-nation of care, taking steps to reduce complications andreadmissions, and exchanging information effectively—make more financial sense. And that takes enough of thepayer community to get behind the effort as well. Having both providers and payers simultaneously
jump together is a challenge, but there is certainly agrowing number of examples of ways to do it successful-
Dr McClellan directs the Engelberg Center for Health CareReform at the Brookings Institution, Washington, DC (www.brookings.edu/health). He is former Commissioner of the USFood and Drug Administration and Administrator of the Centersfor Medicare & Medicaid Services. Mr Piper is a Senior Advisorto TogoRun, Sellers Dorsey, and Fleishman-Hillard, and isHealth Policy Editor of American Health & Drug Benefits.
Accountable Care Organizations in theEra of Healthcare ReformInterview with Mark B. McClellan, MD, PhD
See also Primer on ACOs, page 261
Under the Patient Protection and Affordable Care Act (PPACA) of 2010,Medicare providers, including physician groups and hospitals, will soon have theoption to form accountable care organizations (ACOs) to improve quality andefficiency. ACO participants may share financial gains generated from improvedclinical and economic performance, provided that quality goals and patient safe-guards are met. Through future regulations, the Centers for Medicare & MedicaidServices (CMS) must implement the ACO option no later than January 1, 2012.In this interview, Dr Mark B. McClellan, former CMS Administrator and USFood and Drug Administration Commissioner, discusses the extraordinaryimplications of the new ACO option for improving patient care and reducingunnecessary costs.

ACOs in the Era of Healthcare Reform
243www.AHDBonline.com l American Health & Drug BenefitsVol 3, No 4 l July/August 2010
ly. In the end, the success of ACOs is going to depend onactually reforming care so that costs are lower and resultsare better. It’s not just a matter of getting the criticalmass (of providers and payers), but actually havingmeaningful steps that can be taken. These steps can takea little time, and certainly some effort, to reform the wayhealthcare works, which requires a commitment of time,effort, and expertise to meaningfully redesign care.
Piper: How does the ACO model fit in context with othermajor reforms, most notably bundled payment, global andepisode-based payment reforms, and the medical home model?
McClellan: There is a tendency now to look at whatis in the healthcare reform legislation and what is beingtried in the private sector and states around the coun-try as basically throwing a lot of spaghetti against thewall and seeing what sticks. That is the wrong way tolook at these reforms. They all have a common goal ofimproving care delivery, making it better so thatpatients are healthier, and making it more efficient sothat costs are lower. The best strategy for an organiza-tion is to view these as part of an overall approach togetting that result. So, for example, it can actually beeasier to implement an ACO successfully by pairing itwith a medical home reform. We are seeing many examples of this around the
country, where the providers get the support they needfor coordinating care and spending more time on patientmanagement by the upfront investment needed to sup-port a meaningful medical home. Payers get someaccountability that, by taking these steps (or as they takethese steps upfront to support reforms and care delivery),they are going to be able to see what the ultimate conse-quences are for health and for costs on the back end.That is what an ACO provides. So these reforms cantruly reinforce each other. The best way to approachpayment reform is as pieces that add up to a more com-prehensive and effective whole.
Piper: Long-term, which form of payment do youexpect will work most effectively with the ACO model—shared fee-for-service savings, partial capitation, or someother form of global payment?
McClellan: What we have seen in some earlyadopters is movement toward having less paymentdepend on fee for service. But that is not necessarilygoing to be the outcome. I can imagine some longer-term arrangements where ACOs are operating at aregional level or across a diverse range of providers,where fee-for-service reimbursement may remain a sub-stantial part of payment. The main thing is that ACOs
involve setting up a different kind of tracking system forpayments than you get with fee for service. In the most basic form of ACOs, with shared savings,
in addition to tracking the volume and intensity of serv-ices for traditional fee-for-service payments, the organi-zation and its payers will also track some meaningfulresults for the population of patients being served andper-capita spending. If there are any savings comparedwith fee-for-service costs, those provide an additionalsource of reimbursement for the providers. As people get more used to thinking about things that
they can do to improve care and to work on improvingthose patient-focused performance measures rather thanjust the fee-for-service billing, you can imagine moreweight going to this patient-focused payment approach,and it can be gradual. In some examples, it may start outwith shared savings. Then, as the providers get moreused to working together in this kind of explicit goal-ori-ented way, as they identify some further steps that theycan take together to improve performance, and as theyget more comfortable with an explicit patient-levelfocus, you can imagine putting more weight on the ACOpayment model as opposed to fee for service.So maybe reducing the fee-for-service payment by
20% across the board or for primary care services andputting that money into a partial capitation fund wouldenable the organization to do more to reform care thanit can with the resources from shared savings alone.Different organizations may come out in various places.The whole point is to try to support incremental stepsthat are not too disruptive in the short-term, but thatover time could lead to more fundamental improve-ments and care.
Piper: A few skeptics question the readiness of providerorganizations in areas such as governance, physician relation-ships, coordination, health information technology (HIT),and performance measurement. How do you respond?
McClellan: Yes, this is hard, especially in the statusquo, where it is very difficult for many healthcareproviders and provider organizations. Their paymentrates are being squeezed. They are facing new reimburse-ment and regulatory pressures because of rising health-care costs. Unfortunately, I do not see the status quo get-ting better. So although this is a real challenge, there aresome unique opportunities to support the move toward adifferent kind of payment, in which providers get bettersupport for delivering better care, not just more squeezes.It makes now a really good time to consider moving for-ward on addressing these very hard challenges. For example, there is the federal HIT initiative, with
Medicare and Medicaid incentive payments for adop-

REGULATORY
244 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
tion of electronic health record (EHR) systems andmeaningful use of EHRs. The objectives of the mean-ingful use standards are tied directly to improvingpatient care. This sounds a lot like the goal of account-able care. There are some payments now and over thenext few years in Medicare for physicians and otherhealthcare providers for reporting on performance.That is easier to do if you have an information systemin place and if you are actually developing and usinginformation systems to improve care.CMS now has 2 tracks for performance reporting.
One is the traditional “fill out another claim form”approach, which is burdensome on providers and doesnot help improve quality. The other is to submit infor-mation from systems used to improve care at the patientlevel as a registry-based submission to CMS. An increas-ing number of provider organizations are doing that. There are also other opportunities in terms of medical
homes and other payment reforms that can collectivelyadd up to a significant amount of support for addressingthings such as governance, effective information tech-nology (IT) use, and improving physician relationshipsand coordination. But those opportunities are not goingto be around forever. I think the next few years are prob-ably the best time to take advantage of all of this supportfor building up systems that help providers do what theywant to do, which is get better results for their patientsat a lower cost.
Piper: ACOs have been discussed mostly in terms of hos-pitals and physicians. Does the ACO model hold promise forother combinations of healthcare providers?
McClellan: Yes, it does. It is essential to have a net-work of primary care physicians within an ACO. Butthere are certainly a lot of opportunities to expandbroadly beyond specialist hospitals and other types oftraditional healthcare providers. For example, we haveheard from a number of communities that already havepublic health initiatives in place. They want to expandthese initiatives to use wellness programs and school-based programs to support ACO goals.State Medicaid programs are finding that if they can
expand the support from ACOs and Medicaid to areaslike community-based mental health services, they candocument some significant reductions in medical costsrelated to mental illnesses. There are issues that couldbe addressed through support of care in the communitybut that are not part of traditional healthcare delivery.I think ACOs actually make it easier to move towardless-traditional forms of delivering care and toward pre-venting complications and keeping people well. That’sbecause all these steps in the absence of an ACO run the
risk of payer concerns that they may just lead to highercosts and more expenditures. Therefore, some reluc-tance. With the accountability of the ACO model, itbecomes easier to bring in other types of providers, othertypes of services that may not even be traditional health-care to get the better results and lower costs.
Piper: The Engelberg Center for Health Care Reform, atthe Brookings Institution, provides practical solutions toachieve high-quality, innovative, affordable healthcare. Whatelse is the Engelberg Center working on?
McClellan: Well, this is sort of high noon for health-care reform implementation. A lot of people think thatthe big issues are not coming until 2014, but implemen-tation of reform is under way now. And so we are notonly trying to help with effective implementationaround accountable care, quality and value, and health-care payments, but also on other issues, such as evaluat-ing other types of payment reform and other things thatmay not be viewed as within the traditional reform butprobably should be.For example, we are doing work with a network of
health plans and EHR systems on developing a bettersurveillance capability in this country for monitoring thesafety of medical products. We have got an IT infra-structure now, incomplete as it is, that could providemuch more timely information on potential safety prob-lems. So we need to take steps to use that. Of course, healthcare reform is never done. So we are
following up on some of our earlier work on bending thecurve in healthcare, with ideas that may be consideredin the next round of healthcare reform. The Presidenthas a commission on deficit reduction that will reportlater this year. In 2011, unquestionably there will bemore healthcare legislation related to implementation ofthe new law, funding it, and perhaps building on it. Sowe are trying to provide some useful guidance for all ofthat too. What a lot of these projects have in common is a
recognition that private sector leadership is needed forreal reform in healthcare, and for making our public-private system work better, but that this needs to bealigned with effective federal, state, and local govern-ment policies to support shared goals. And one of thethings we have tried to do here at the EngelbergCenter—as a neutral, expert-oriented think tank—isto help bring together these different perspectives inpractical ways to make progress on the big challenges ofreform in all of these areas. �
Reference1. McClellan MB, McKethan AN, Lewis JL, et al. A national strategy to putaccountable care into practice. Health Aff (Millwood). 2010;29:982-990.

FORMERLYKAPIDEX™
(dexlansoprazole)
1200
1000
800
600
400
200
00 6 12 18 24
Time (h)
Mean plasma concentration (in healthy subjects; day 5; ng/mL)1
DEXILANT 60 mgDEXILANT 30 mgDEXILANT 60 mgDEXILANT 60 mgDEXILANT 30 mgDEXILANT 30 mgDEXILANT 30 mg
DEXILANT 30 mg provided full 24-hour heartburn relief in a majority of symptomatic non-erosive gastroesophageal reflux disease patients at week 41
Conclusions of comparative effi cacy cannot be drawn from this information.
IndicationsDEXILANT is indicated for healing all grades of erosive esophagitis (EE) for up to 8 weeks, maintaining healing of EE for up to 6 months, and treating heartburn associated with symptomatic non-erosive gastroesophageal reflux disease (GERD) for 4 weeks.
Important Safety Information DEXILANT is contraindicated in patients with known hypersensitivity to any component of the formulation. Hypersensitivity and anaphylaxis have been reported with DEXILANT use. Symptomatic response with DEXILANT does not preclude the presence of gastric malignancy. Most commonly reported treatment-emergent adverse reactions: diarrhea (4.8%), abdominal pain (4.0%), nausea (2.9%), upper respiratory tract infection (1.9%), vomiting (1.6%), and flatulence (1.6%). Do not co-administer atazanavir with DEXILANT because atazanavir systemic concentrations may be substantially decreased. DEXILANT may interfere with absorption of drugs for which gastric pH is important for bioavailability (e.g., ampicillin esters, digoxin, iron salts, ketoconazole). Patients taking concomitant warfarin may require monitoring for increases in international normalized ratio (INR) and prothrombin time. Increases in INR and prothrombin time may lead to abnormal bleeding and even death. Concomitant tacrolimus use may increase tacrolimus whole blood concentrations.
Please see adjacent brief summary of prescribing information for DEXILANT.
DEXILANT WORKS ASECOND SHIFT TO HELP SHUT DOWN ACID PUMPS
DEXILANT is the fi rst and only PPI with a Dual Delayed Release™ (DDR) formulation, which provides a second release of drug
11:00:12 AM

BRIEF SUMMARY OF FULL PRESCRIBING INFORMATIONDEXILANT (dexlansoprazole) delayed release capsulesINDICATIONS AND USAGEDEXILANT is indicated for:
CONTRAINDICATIONS
[see Adverse Reactions].WARNINGS AND PRECAUTIONSGastric Malignancy
ADVERSE REACTIONS Clinical Trials Experience
Table 2: Incidence of Treatment-Emergent Adverse Reactionsin Controlled Studies
Adverse Reaction
Placebo
(N=896)%
DEXILANT30 mg
(N=455)%
DEXILANT60 mg
(N=2218)%
DEXILANTTotal
(N=2621)%
Lansoprazole30 mg
(N=1363)%
Tract Infection
Blood and Lymphatic System Disorders: Cardiac Disorders:
Ear and Labyrinth Disorders: Endocrine Disorders: Eye Disorders: Gastrointestinal Disorders:
General Disorders and Administration Site Conditions:
Hepatobiliary Disorders: Immune System Disorders: Infections and
Infestations: Injury, Poisoning
and Procedural Complications:
Laboratory Investigations:
Metabolism and Nutrition Disorders: Musculoskeletal and Connective
Tissue Disorders: Nervous System Disorders:
Psychiatric Disorders: Renal and Urinary
Disorders: Reproductive System and Breast Disorders: ; Respiratory, Thoracic and Mediastinal Disorders:
Skin and Subcutaneous Tissue Disorders: Vascular Disorders:
Postmarketing Experience
Eye Disorders: Gastrointestinal Disorders: General Disorders and Administration Site Conditions: Immune System Disorders:
Respiratory, Thoracic and Mediastinal Disorders:
Skin and Subcutaneous Tissue Disorders:
DRUG INTERACTIONSDrugs with pH-Dependent Absorption Pharmacokinetics
Warfarin
Tacrolimus
USE IN SPECIFIC POPULATIONSPregnancyTeratogenic Effects
6/10 Printed in U.S.A.

A reproduction study conducted in rabbits at oral dexlansoprazole doses up to 30 mg per kg per day (approximately 9-fold the maximum recommended human dexlansoprazole dose (60 mg) revealed no evidence of harm to the fetus due to dexlansoprazole. In addition, reproduction studies performed in pregnant rats with oral lansoprazole at doses up to 40 times the recommended human dose and in pregnant rabbits at oral lansoprazole doses up to 16 times the recommended human dose revealed no evidence of impaired fertility or harm to the fetus due to lansoprazole.Nursing MothersIt is not known whether dexlansoprazole is excreted in human milk. However, lansoprazole and its metabolites are present in rat milk following the administration of lansoprazole. As many drugs are excreted in human milk,and because of the potential for tumorigenicity shown for lansoprazole in rat carcinogenicity studies [see Carcinogenesis, Mutagenesis, Impairment of Fertility],a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.Pediatric Use Safety and effectiveness of DEXILANT in pediatric patients (less than 18 years of age) have not been established.Geriatric UseIn clinical studies of DEXILANT, 11% of patients were aged 65 years and over. No overall differences in safety or effectiveness were observed between these patients and younger patients, and other reported clinical experience has not identified significant differences in responses between geriatric and younger patients, but greater sensitivity of some older individuals cannot be ruled out.Renal ImpairmentNo dosage adjustment of DEXILANT is necessary in patients with renal impairment. The pharmacokinetics of dexlansoprazole in patients with renal impairment are not expected to be altered since dexlansoprazole is extensively metabolized in the liver to inactive metabolites, and no parent drug is recovered in the urine following an oral dose of dexlansoprazole.
Hepatic ImpairmentNo dosage adjustment for DEXILANT is necessary for patients with mild hepatic impairment (Child-Pugh Class A). DEXILANT 30 mg should be considered for patients with moderate hepatic impairment (Child-Pugh Class B). No studies have been conducted in patients with severe hepatic impairment (Child-Pugh Class C).OVERDOSAGEThere have been no reports of significant overdose of DEXILANT. Multiple doses of DEXILANT 120 mg and a single dose of DEXILANT 300 mg did not result in death or other severe adverse events. Dexlansoprazole is not expected to be removed from the circulation by hemodialysis. If an overdose occurs, treatment should be symptomatic and supportive.CLINICAL PHARMACOLOGYPharmacodynamicsAntisecretory ActivityThe effects of DEXILANT 60 mg (n=20) or lansoprazole 30 mg (n=23) once daily for five days on 24-hour intragastric pH were assessed in healthy subjects in a multiple-dose crossover study. Serum Gastrin EffectsThe effect of DEXILANT on serum gastrin concentrations was evaluated in approximately 3460 patients in clinical trials up to 8 weeks and in 1023 patients for up to 6 to 12 months. The mean fasting gastrin concentrations increased from baseline during treatment with DEXILANT 30 mg and 60 mg doses. In patients treated for more than 6 months, mean serum gastrin levels increased during approximately the first 3 months of treatment and were stable for the remainder of treatment. Mean serum gastrin levels returned to pre-treatment levels within one month of discontinuation of treatment.Enterochromaffin-Like Cell (ECL) EffectsThere were no reports of ECL cell hyperplasia in gastric biopsy specimens obtained from 653 patients treated with DEXILANT 30 mg, 60 mg or 90 mg for up to 12 months. During lifetime exposure of rats dosed daily with up to 150 mg per kg per day of lansoprazole, marked hypergastrinemia was observed followed by ECL cell proliferation and formation of carcinoid tumors, especially in female rats [see Nonclinical Toxicology].Effect on Cardiac RepolarizationA study was conducted to assess the potential of DEXILANT to prolong the QT/QTc interval in healthy adult subjects. DEXILANT doses of 90 mg or 300 mg did not delay cardiac repolarization compared to placebo. The positive control (moxifloxacin) produced statistically significantly greater mean maximum and time-averaged QT/QTc intervals compared to placebo.
NONCLINICAL TOXICOLOGYCarcinogenesis, Mutagenesis, Impairment of FertilityThe carcinogenic potential of dexlansoprazole was assessed using lansoprazole studies. In two 24-month carcinogenicity studies, Sprague-Dawley rats were treated orally with lansoprazole at doses of 5 to 150 mg per kg per day, about 1 to 40 times the exposure on a body surface (mg/m2) basis of a 50 kg person of average height [1.46 m2 body surface area (BSA)] given the recommended human dose of lansoprazole 30 mg per day. Lansoprazole produced dose-related gastric ECL cell hyperplasia and ECL cell carcinoids in both male and female rats [see Clinical Pharmacology].In rats, lansoprazole also increased the incidence of intestinal metaplasia of the gastric epithelium in both sexes. In male rats, lansoprazole produced a dose-related increase of testicular interstitial cell adenomas. The incidence of these adenomas in rats receiving doses of 15 to 150 mg per kg per day (4 to 40 times the recommended lansoprazole human dose based on BSA) exceeded the low background incidence (range = 1.4 to 10%) for this strain of rat. In a 24-month carcinogenicity study, CD-1 mice were treated orally with lansoprazole doses of 15 mg to 600 mg per kg per day, 2 to 80 times the recommended human dose based on BSA. Lansoprazole produced a dose-related increased incidence of gastric ECL cell hyperplasia. It also produced an increased incidence of liver tumors (hepatocellular adenoma plus carcinoma). The tumor incidences in male mice treated with 300 mg and 600 mg lansoprazole per kg per day (40 to 80 times the recommended lansoprazole human dose based on BSA) and female mice treated with 150 mg to 600 mg lansoprazole per kg per day (20 to 80 times the recommended human dose based on BSA) exceeded the ranges of background incidences in historical controls for this strain of mice. Lansoprazole treatment produced adenoma of rete testis in male mice receiving 75 to 600 mg per kg per day (10 to 80 times the recommended lansoprazole human dose based on BSA).The potential effects of dexlansoprazole on fertility and reproductive performance were assessed using lansoprazole studies. Lansoprazole at oral doses up to 150 mg per kg per day (40 times the recommended lansoprazole human dose based on BSA) was found to have no effect on fertility and reproductive performance of male and female rats.PATIENT COUNSELING INFORMATION[see FDA-Approved Patient Labeling in the full prescribing information]Information for PatientsTell your patients to watch for signs of an allergic reaction as these could be serious and may require that DEXILANT be discontinued.To ensure the safe and effective use of DEXILANT, this information and instructions provided in the FDA-approved patient labeling should be discussed with the patient. Inform patients of the following:DEXILANT is available as a delayed release capsule.DEXILANT may be taken without regard to food.DEXILANT should be swallowed whole.
follows: - Open capsule; - Sprinkle intact granules on one tablespoon of applesauce; - Swallow immediately.Distributed byTakeda Pharmaceuticals America, Inc.Deerfield, IL 60015U.S. Patent Nos. - 5,045,321; 5,093,132; 5,433,959; 6,462,058; 6,664,276; 6,939,971; and 7,285,668.DEXILANT is a trademark of Takeda Pharmaceuticals North America, Inc. and used under license by Takeda Pharmaceuticals America, Inc.All other trademark names are the property of their respective owners.©2009, 2010 Takeda Pharmaceuticals America, Inc.For more detailed information, see the full prescribing information for DEXILANT or contact Takeda Pharmaceuticals America, Inc. at 1-877-825-3327.KAP0110 R6-Brf; March 2010L-LPD-0310-2
Reference: 1. DEXILANT (dexlansoprazole) package insert, Takeda Pharmaceuticals America, Inc.
DEXILANT™, KAPIDEX™ (dexlansoprazole), and Dual Delayed Release™ are trademarks of Takeda Pharmaceuticals North America, Inc., and are used under license by Takeda Pharmaceuticals America, Inc.
©2010 Takeda Pharmaceuticals North America, Inc. LPD-01139 6/10 Printed in U.S.A.
11:00:13 AM

BUSINESS
248 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
Dr Tzeel is Market Medical Officer, and Mr Brown is FinancialAnalyst, Humana, Inc, Great Lakes Region, Milwaukee, WI.
Expect the Unexpected: A Role for BehavioralEconomics in Understanding the Impact of Cost-Sharing on Emergency Department UtilizationAlbert Tzeel, MD, MHSA; Jack Brown, BA
Background: As employers and payers address increasing healthcare costs, they resortto the tenets of classical economics: if one increases the price for a service (defined as anindividual’s cost-sharing), then that individual’s demand for services should decrease. This,however, may not necessarily be true, and raises the question of whether increased cost-sharing for emergency department services will lead to decreased utilization of those serv-ices as would be expected in classical economics. Objective: To assess the effect of emergency department cost-sharing on patient utiliza-tion of emergency department services.Method: In 2002, we retrospectively reviewed 2001 claims and identified 797 memberswho have had at least 2 nonemergent visits to the emergency department. This cohort wascomprised of members with high emergency department utilization patterns who also hadpotentially differing emergency department copayment changes from one health insuranceplan year to the next. Participants had to be covered by Humana for a minimum of 12 con-secutive months. Of the original cohort, 415 remained covered by Humana after the end ofthe first year, 322 remained covered after the second year, and 194 after the end of thethird year. After completions of three 12-month blocks of time with appropriate claims runout, we assessed changes in the cohort’s emergency department encounters from the pre-vious year to the current year relative to emergency department copayment changes, usingmatched pairs t-test. Results: Surprisingly, in the first 12 months, reductions in emergency department copay-ments resulted in decreases in patient utilization (–58.3% change, P <.007), and increasesin emergency department copayment resulted in an increased utilization (1096.0% change,P <.001). This unexpected trend continued in the second and third periods. Overall, in ourcohort, increases in emergency department copayments were significantly associated withincreased emergency department encounters by different individuals in each of the 3 studyperiods. In contrast, in the 2 groups with no increases in emergency department copay-ments, utilization of these services decreased or remained flat. Conclusion: When assessing the need for emergency department services, many factorsbesides cost play a role in choosing to obtain emergency department care, including indi-vidual assessments of the probability of a given illness and the financial or temporal impli-cations for the care sought in terms of “gains” or “losses” relative to a reference point.Behavioral economics can therefore play a role in understanding why healthcare con-sumers behave as they do. The implications of behavioral economics need to be factoredin when considering a healthcare benefit design.
Am Health Drug Benefits.2010;3(4):248-256.www.AHDBonline.comDisclosures are at end of text
Albert Tzeel
Stakeholder Perspective, page 255

Expect the Unexpected
249www.AHDBonline.com l American Health & Drug BenefitsVol 3, No 4 l July/August 2010
Expect the unexpected, or you won’t find it.”2 Thisadmonition, offered by the Greek Heraclitus morethan 2500 years ago, still rings true today.
Employer-sponsored healthcare coverage continues tosubscribe to classical economics with respect to demandand price. Many employers providing insurance cover-age believe that if they shift costs to those employeeswho consume medical care by increasing copayments orcoinsurance, then those individuals will respond to anew price point for medical services by curbing theirown demand for healthcare.3-7Choices on whether to utilize healthcare can be made
in a rational context when one does not have the pres-sure of a limited time horizon in which to make the deci-sion. In an emergency situation, however, seconds countin the choice to seek care: whether a true emergencyexists lies within the discretion and perception of theconsumer making that decision.O’Grady and colleagues showed that cost-shifting has
an impact on emergency department (ED) use.8 Selbyand colleagues showed that after introducing a copay-ment ranging from $25 to $35 for using the ED, utiliza-tion decreased significantly, with the largest decreases inlesser severity of illness.9 Yet, even with such cost-shift-ing, ED utilization continues to increase.10-12 If cost-shift-ing by itself cannot control increasing ED utilization,what else could be playing a role? Do people behave dif-ferently from what is predicted under classical econom-ics? And, if so, why? Are people irrational when seekingED services? Given the premise that people are irrationaldecision makers when it comes to ED utilization, and aspart of a broader educational initiative to decrease EDutilization in southeastern Wisconsin, we at Humanawanted to confirm that increased cost-sharing (ie, EDcopayment increases) for ED services indeed resulted indecreases in ED utilization.
MethodsData Patterns Early in 2002, we reviewed 2001 data for Humana
Milwaukee HMO ED utilization. Through this reviewwe identified a cohort of 797 unique members for a self-care promotion. Each of these individuals had at least 2
nonemergent ED visits that were amenable to self-care,according to informational books we provided to all ofthem,13,14 as part of our study. Many in the cohort had EDcopayment adjustments for a given benefit year throughtheir employer-sponsored health insurance instituted tomitigate premium cost increases.We followed this cohort for 3 consecutive 12-month
blocks. At the end of each 12-month period, in additionto assorted demographic data, we collected informationon ED utilization and on benefit changes (including ED
KEY POINTS
➤ In designing health insurance coverage, manyemployers believe that shifting some of the cost ofmedical care to employees will reduce demand forsuch care and lower utilization.
➤ However, some studies have suggested thatemergency department utilization continues torise, regardless of any copayment considerations.
➤ This raises the question about any potentialassociation between cost-shifting and emergencydepartment utilization.
➤ An analysis of the association between cost-sharing and emergency care utilizationunexpectedly showed that increasing emergencydepartment copayments was significantlyassociated with increased, rather than decreased,emergency department utilization.
➤ In contrast, among employees with no increase inemergency department copayments, utilizationdecreased or remained flat.
➤ The authors suggest that there is a distinct role forbehavioral economics when attempting to controlhealthcare costs. Contrary to classical economictheory, people often do not make rationaldecisions when it comes to their health.
➤ To affect behavior change in covered populations,employers and payers must understand how peopleview medical risk, especially potentially emergencyrisk, unlike other risks, and incorporate behavioraleconomics in their benefit design decisions.
“
We economists always think that waving money under people’s noses will make thembehave according to some theoretical script. But we’ve tried that with healthcare fordecades and it hasn’t worked. Healthcare isn’t just about financial incentives; it’s alsoabout anxiety, fear, habit, guan-xi—a Chinese word that, loosely translated, means“family or business ties”—and professional pride. We’ve neglected to study the impactthat human behavior has on the system, and I don’t think we can do much to improve itunless we address the noneconomic dimensions of healthcare issues.1
—Uwe Reinhardt, PhD

BUSINESS
250 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
copayments) for members who remained with Humanathroughout that entire 12-month period. Collecting thisinformation for consecutive years allowed for directcomparison with each preceding period. Data analysis at the conclusion of each time period
showed that of the original 797 participants, 415 (52.1%)remained covered by Humana after the first year, 322(40.4%) remained covered after the second year, and194 (24.3%) remained Humana members when datawere collected after the third year.
Statistical AnalysisWe realize that observational analysis could not sub-
stitute for a well-designed study, but we were compelledto examine the findings statistically to see if the datashowed something of potential interest and, if it did, toproffer a possible explanation.Statistical analyses were performed using Microsoft
Excel 97 for Windows and XLSTAT, a Microsoft Exceladd-in package.15 We assessed changes in the cohort’sED encounters from the previous year to the currentone relative to ED copayment changes, using matchedpairs t-test.
ResultsDemographicsAs noted, study participants had to remain active
Humana members for an entire 12-month block of time.Because the study period overlapped calendar years, welost some members at the time of their employer group’srenewal (especially on January 1). Table 1 outlines thedemographic data for 322 members who were activethrough the first 2 years, categorized by age and by sex.
Changes in ED Utilization Associated withCopayment AdjustmentsIn reviewing the data, we found a specific pattern in
each year: the groups who had an ED copayment increasehad an increased number of ED visits (Table 2). Asshown in Table 2, in the first year, if the ED copaymentincreased in a given period (relative to the 12-monthperiod before it), ED utilization actually increased by afactor of nearly 12. Given the low rate of ED utilization
in the group with the increasing ED copayment in thepreceding period, this finding might have simply been acase of regression to the mean. But what if we find simi-lar patterns during the following 2 years? In the second year, a similar pattern emerged. For
the 2 groups whose ED copayment did not increase dur-ing this period, decreases in ED utilization occurred.However, in the third group, whose ED copaymentincreased during the period, we observed a significant(P = .022) and rather large increase in ED utilization—that is, an average increase of nearly 1 full ED visit foreach person in that group, for a total of 46 ED visits.A comparable pattern continued during the third
year. In the groups whose ED copayment did notincrease, we found either a small, nonsignificantincrease or a significant decrease in ED utilization. Theremaining group continued to show that when the EDcopayment increased in a given period, a noteworthy,albeit not significant (� = .05, P = .09) increase in EDutilization occurred. All 3 time frames showed the same counterintuitive
pattern: ED copayment increases were associated withincreased ED utilization. Although there were no indi-viduals who had ED copayment increases in 2 consec-utive periods during any of the 3 intervals, we observedconsistency among unique individuals’ responses to EDcopayment increases.
DiscussionSignificant Implications for EmployersOur original presumption was that individuals
respond to having their ED copayment increased bydecreasing their ED utilization, according to classicaleconomics. But that is not what our data revealed to usyear after year. Why? This inconsistency has tremendous implications for
employer groups that provide health benefits to theiremployees. A given employer may choose to rely onthe tenets of classical economics (ie, increasing EDcopayments to promote decreased ED utilization). Yet,without a general understanding of key ideas frombehavioral economics, that employer may not neces-sarily achieve the desired results.
Table 1 General Demographic Data for Available Cohort after Second Year
CharacteristicTotal
(N = 322)Children (N = 50)
Adults (N = 272)
Male (N = 113)
Female (N = 209)
Average age, yr (SD) 32.6 (18.1) 5.0 (3.7) 37.7 (14.9) 31.7 (20.0) 33.1 (17.1)
Males, N (%) 113 (35.1) 21 (42.0) 92 (33.8) 113 (100) 0 (0.0)
SD indicates standard deviation.

Expect the Unexpected
251www.AHDBonline.com l American Health & Drug BenefitsVol 3, No 4 l July/August 2010
Several behavioral concepts may influence this find-ing and promote the association that our results show forED utilization.
Prospect Theory: Behavioral Economics ExplainsEmergency Care Utilization A review of our results showed an association in
which, on average, if the ED copayment increased, thenED utilization increased as well. We speculate that thereis a legitimate reason for this finding, and we defer onthis to behavioral economics, specifically to “prospecttheory.” This theory arose from experimental proof thatpeople repeatedly violate the principles of expected util-ity theory when making particular decisions. Prospect theory was first proposed by Kahneman and
Tversky in 1979.16 Although a formal discussion ofprospect theory is beyond the scope of this article, 2 ofits key elements are pertinent to this discussion.First, according to prospect theory, a person multi-
plies his or her distinct expected utility by a subjectiveprobability. However, individuals tend to distort thoseprobabilities by overweighting low-probability eventsand underweighting high-probability events (eg, if achild only has the symptoms of fever, neck pain, anddifficulty swallowing, the more likely probability of
streptococcal pharyngitis may be underweighted,whereas the less likely probability of bacterial meningi-tis may be overweighted). This finding would imply that the probability of a
particular healthcare event (eg, vomiting in gastroen-teritis, generalized fever, ear pain) being extremely seri-ous or even life-threatening would most likely be exag-gerated by the individual or the caregiver. Burns andcolleagues corroborate that the overweighting of thehigh-risk, low-probability event tends to promote a uti-lization profile of increased consumption.17Second, individuals view these expected utilities as
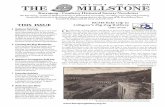
changes from a reference point.18 With respect to“changes from a reference point,” Kahneman andTversky propose that individuals make decisions as ifthey had a “value” function for gains and losses(Figure).16 The horizontal axis in the Figure reflectseither monetary gain (to the right) or monetary loss (tothe left) relative to one’s reference point (ie, the origin).The value function shows that individuals perceive loss-es as more significant than equivalent gains: the valuefunction increases the slope as one moves to the right,until the origin, and decreases the slope as one moves tothe right, away from the origin. Baron describes this Figure as meaning “that, for sim-
Table 2 Changes in Average ED Visits in 3 Years, by ED Copayment Changes
Year (period)Patients,
N
ED visits per person at onset
of period
ED visits per person at end of period
Change in ED visits per person
Change, % P
First 12 mo
Group 2: No copay changes 304 0.80 2.41 1.61 201.3 <.001
Group 2: Copay decreased 8 3.00 1.25 –1.75 –58.3 <.007
Group 3: Copay increased 103 0.23 2.75 2.52 1096.0 <.001
All participants, period 1 415 0.70 2.47 1.77 252.9 <.001
Second 12 mo
Group 1: No copay changes 226 0.98 0.91 –0.07 –7.9 NS
Group 2: Copay decreased 47 1.77 0.81 –0.96 –54.2 <.001
Group 3: Copay increased 49 0.92 1.86 0.94 102.2 .022
All participants, period 2 322 1.08 1.04 –0.04 –3.7 NS
Third 12 mo
Group 1: No copay changes 176 0.85 0.97 0.12 14.1 NS
Group 2: Copay decreased 11 2.09 0.36 1.73 –82.8 <.003
Group 3: Copay increased 7 0.57 1.29 0.72 126.3 NS
All participants, period 3 194 0.91 0.94 0.03 3.3 NS
ED indicates emergency department; NS, not significant (� = .05).

BUSINESS
252 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
ple gambles, subjects tend to avoid risks in the domain ofgains and tend to seek risks in the domain of losses wheregains and losses are defined in terms of expected mone-tary change from their reference point.”18 An increasedED copayment, relative to the previous copayment,would in theory tend to make an individual “risk-seek-ing,” because a potential loss, coupled with an exagger-ated probability for a potentially adverse event, drivesED utilization.
Perceived value versus cost. In other words, there ismore perceived value (because of the higher ED copay-ment/“loss”) for that ED visit than existed before thecopayment change. In addition, from a cognitive stand-point, the individual can rationalize perceived value inthe decision to seek services despite a greater personalfinancial cost. As early as 1969, Doob and colleaguesnoted that according to cognitive dissonance theory, themore something costs, the more people find value in it,and the more they can feel internal pressure to buy it.19Prospect theory’s role may perhaps be better viewed
through the following example. Two families each havea young child who complains of a nonspecific sore throaton a Sunday afternoon. Each family is concerned thatthe child has strep throat, which may develop into rheu-matic fever or worse. For family A, the most recentinsurance changes resulted in a $50 decrease in EDcopayment (from $100 to $50). For family B, the mostrecent insurance changes have resulted in a $50 increasein ED copayment (from $50 to $100). Family A may view this event as a choice between 2
alternatives—going to the ED removes a certain mone-tary gain (compared with last year) for diagnosing apotentially low-probability event—estimated in the pastas a probability of 11% for strep throat for all ED visits inwhich the chief complaint is sore throat, and as 15% to36% in the pediatric population.20,21 Family B may alsoview this event as a choice between 2 alternatives—going to the ED may yield a greater monetary loss (com-pared with last year), but the cost of not going may beeven higher—the financial cost and/or disability
Adapted from Kahneman D, et al. Econometrica. 1979;47:263-292.
Figure Prospect Theory Value Function
Change in utility/value
Change from the reference point
Risk-averse profile
Value: “gains” vs “losses”
Risk-seeking profile
–10 –8 –6 –4 –2 0 2 4 6 8 10
4
2
0
–2
–4
–6
–8
–10

Expect the Unexpected
253www.AHDBonline.com l American Health & Drug BenefitsVol 3, No 4 l July/August 2010
incurred by the child whose strep throat develops intosomething worse, such as acute rheumatic fever in0.01% of all childhood throat infections.20,21For this example, we use a cost of approximately
$25,000 for each case of acute rheumatic fever (adaptedfrom Webb and others).22 From an expected value stand-point, family A now views the decision as a choicebetween a certain “gain” of $50 versus only a possible“gain” of $2.50 (0.0001 � $25,000). The $2.50 is con-sidered the expected financial value for diagnosing 1case of acute rheumatic fever; it represents the “cost” ofremoving uncertainty in diagnosis.
Certain versus possible gain. This value in informa-tion gain does not include additional potential costs ofthe disability or of the financial impact as a result ofmissed time off from work. Family A is risk-averse andwould wait to see if the symptoms worsen before seekingED care, because a sure gain of $50 is preferable to a pos-sible gain of only $2.50. Family B, however, views thechoice as one of a sure loss of $50 compared with only arisk of a loss of $2.50. For them, this choice is easy—tak-ing a chance on losing only $2.50 is significantly betterthan losing $50 for sure. Studies also show that anything constraining one’s
sense of an unlimited future shifts motivations and pri-orities away from a future orientation toward a presentorientation.23 Family B, then, is “risk-seeking” andtherefore seeks ED care for their child. If urgent carewere substituted for ED care, neither family in ourexample would change its decision unless the urgentcare copay/personal cost was less than $2.50. Evenrapid-care clinics found in most national drugstorechains charge more than that for a typical visit. In fact,our data showed that the greater the dollar differentialbetween ED visit copays and copays at alternate sites ofcare (eg, office visits or urgent care), the more likelythe member was to go to the ED.
The Psychology of Time: Behavioral EconomicsExplains Non–Emergency Care UtilizationAnother way of looking at ED-seeking behavior that
would be consistent with our data is to apply the “psy-chology of time.” For the purposes of explaining the pat-terns we saw earlier, the economic curves of demand ver-sus price perform adequately for most conditions inwhich the majority of the “cost” to the individual istime, because the reference value for the ED copaymentdid not change. Tucker and Davison suggest that, “When monetary
costs to consumers are minimal or nonexistent, timecosts function to reduce and regulate demand….Oncetime is ‘spent,’ it cannot be recovered as one mightrecover a monetary loss or replace a tangible good.”24
Time, then, becomes the “currency of choice” whenmoney is not a factor. This may explain why, when an ED copayment
change was not the key issue (ie, it either had notchanged or had decreased), individuals tended to con-sider time their “currency” and might have chosen to useself-care strategies over seeking ED care. In fact, probably because of time’s lack of fungibility,
studies show that in hypothetical choice situations, indi-viduals tend to be either more risk-averse or risk-neutralabout potential time losses, but they tend to be morerisk-seeking with respect to monetary losses.25 AlthoughLeclerc and colleagues based their conclusions on hypo-thetical choices,25 these findings have tremendous impli-cations for employer groups who provide health benefits. A given employer may choose to rely on the tenets of
classical economics (ie, increasing ED copayments topromote decreased ED utilization, or promotion of awider gap between ED copayments and office visitcopayments to drive utilization toward the physician’soffice as an ED substitute). Yet, without a general under-standing of, as well as an incorporation of, some basicideas from behavioral economics, those employer groupsmay not necessarily achieve the results they desire. Phelps once asked if anybody behaved as a “rational
economic actor” in the healthcare market.26 Theanswer comes from Heraclitus’ quote at the beginningof this present article, “expect the unexpected, or youwon’t find it.”2
Limitations As with any study, there are potential limitations to
interpreting our findings. First, we did not collect dataon certain specific characteristics of the cohort.Oftentimes, these traits may influence patient behaviorand may help to explain why ED encounter rates variedat the onset of our review period and in response tochanging ED copayments. It is known, for example, thatpatient characteristics, such as socioeconomic status andchronicity of illness, can impact ED utilization.27,28However, all the individuals for whom we reviewed datawere insured and therefore relatively insulated from theactual cost of the ED visit (outside of an expected copay-ment). We would therefore expect that the results wouldtend to be biased toward an increased ED copaymentyielding decreased ED utilization and not the other wayaround (assuming the effect of classical economics). Second, a selection bias may also be noted, because
the cohort from which all members were drawn camefrom an initial pool of “nonemergent ED utilizers.” Sucha cohort may prejudice the results.29 However, just as wesee a potential association in our data between ED uti-lization and increasing ED copayments, the door now

opens for assessing other areas of potential individual-driven overutilization with increased cost-sharing (eg,specialist office visits). Third, we cannot state with complete certainty that
we did not observe a simple regression to the mean.Regression to the mean effects, however, can take sever-al years to manifest, and it is therefore possible that thiscohort could see a return to baseline ED utilization overthe next several years.30
ConclusionAnalyzing how individuals reconcile their cost for
emergency care relative to obtaining emergent servicescan lead to the discovery of pertinent facts that can havesome bearing on the control of healthcare costs. Firstand foremost, there is a distinct role for behavioral eco-nomics within the sphere of controlling healthcare costs.To achieve behavior changes in their covered popula-tions, employers and payers must understand how peopleview medical risk, how they make decisions regardingfinancial tradeoffs, and how information alters these per-ceptions. Attempting to influence one area, such as per-sonal financial responsibility, without fully understand-ing the systemic implications, can be shortsighted. Second, although classical economic theory still
exerts the most influence in health economics, to affectbehavior change one must realize that people do nottend to be rational actors when it comes to their health. After taking account of the potential impact of
behavioral economics in ED or other medical care uti-lization, further evaluation and analysis are certainlywarranted to better understand how individuals chooseto respond to increasing financial responsibility in thecontext of overall medical care. If employers and payerswant to contain increasing ED (or potentially othermedical care) utilization, they will need to consider theimplications of behavioral economics in their benefitdesign and programmatic decisions. �
AcknowledgmentFinancial support for this article was provided by
Humana Insurance Corporation, a subsidiary ofHumana Inc, Louisville, Kentucky (doing business inWisconsin). The funding agreement insured theauthors’ independence in designing our pilot study,interpreting the data, and writing the article.
Disclosure StatementDr Tzeel and Mr Brown did not report any potential
conflict of interest.
References1.McCue MT. Whither sociology? Princeton economist Uwe Reinhardt says health-care needs to account for human behavior, not just dollar signs. Managed HealthcareExecutive. September 1, 2009. http://managedhealthcareexecutive.modernmedicine.com/mhe/Executive+Profile/Whither-sociology/ArticleStandard/Article/detail/121923?searchString=whither%20sociology. Accessed May 1, 2010. 2. Von Oech R. Expect the Unexpected (Or You Won’t Find It). San Francisco, CA:Berrett-Koehler; 2002. 3.Huskamp HA, Deverka PA, Epstein AM, et al. The effect of incentive-based formu-laries on prescription-drug utilization and spending. N Engl J Med. 2003;349:2224-2232. 4. Piette JD, Heisler M, Wagner TH. Problems paying out-of-pocket medicationcosts among older adults with diabetes. Diabetes Care. 2004;27:384-391.5. Lohr KN, Brook RH, Kamberg CJ, et al. Use of medical care in the Rand HealthInsurance Experiment: diagnosis- and service-specific analyses in a randomized con-trolled trial. Med Care. 1986;24(suppl 9):S1-S87.6. Cherkin DC, Grothaus L, Wagner EH. The effect of office visit copayments onpreventive care services in an HMO. Inquiry. 1990;27:24-38.7. Simon GE, VonKorff M, Durham ML. Predictors of outpatient mental health uti-lization by primary care patients in a health maintenance organization. Am JPsychiatry. 1994;151:908-913.8. O’Grady KF, Manning WG, Newhouse JP, Brook RH. The impact of cost sharingon emergency department use. N Engl J Med. 1985;313:484-490.9. Selby JV, Fireman BH, Swain BE. Effect of a copayment on use of the emergencydepartment in a health maintenance organization. N Engl J Med. 1996;334:635-641.10. Young GP, Wagner MB, Kellerman AL, et al. Ambulatory visits to hospital emer-gency departments. Patterns and reasons for use. 24 hours in the ED study group.JAMA. 1996;276:460-465.11. Tufts Managed Care Institute. Emergency department utilization: trends andmanagement. November-December 2001. www.thci.org/downloads/topic1112_01.pdf.Accessed July 7, 2010.12.US Government Accountability Office. Report to the Chairman, Committee onFinance, US Senate. Hospital emergency departments: crowding continues to occur,and some patients wait longer than recommended time frames. GAO 09-347. April2009. www.gao.gov/new.items/d09347.pdf. Accessed June 28, 2010.13. Pantell RH, Fries JF, Vickery DM. Taking Care of Your Child: A Parent’s Guide toComplete Medical Care. Reading, MA: Perseus Books; 1999.14. Vickery DM, Fries JF. Take Care of Yourself. Cambridge, MA: Perseus Books; 2001.15. XLSTAT Statistical Software. Paris, France: Addinsoft, 1995-2004.16. Kahneman D, Tversky A. Prospect theory: an analysis of choice under risk.Econometrica. 1979;47:263-292.17. Burns Z, Chiu A, Wu G. Overweighting of small probabilities. Prepared forWiley Encyclopedia of Operations Research and Management Science. March 15,2010. http://faculty.chicagobooth.edu/george.wu/research/papers/burns%20chiu%20wu%202010%20Overweighting%20of%20Small%20Probabilities.pdf. AccessedJuly 7, 2010.18. Baron J. Thinking and Deciding. New York, NY: Cambridge University Press;2000:268. 19.Doob AN, Carlsmith JM, Freedman JL, et al. Effect of initial selling price on sub-sequent sales. J Pers Soc Psychol. 1969;11:345-350.20. Kaufman A, Murray D, Starita L, Brickner PW. Streptococcal sore throat follow-up program in a hospital clinic, New York City. Public Health Rep. 1975;90:369-372.21. Linder JA, Bates DW, Lee GM, Finkelstein JA. Antibiotic treatment of childrenwith sore throat. JAMA. 2005;294:2315-2322. 22.Webb KH. Does culture confirmation of high-sensitivity rapid streptococcal testsmake sense? A medical decision analysis. Pediatrics. 1998;101:E2.23. Zimbardo P, Boyd J. The Time Paradox. New York, NY: Free Press; 2008.24. Tucker JA, Davison JW. Waiting to see the doctor: the role of time constraintsin the utilization of health and behavioral health services. In: Bickel WK, VuchinichRE, eds. Reframing Health Behavior Change with Behavioral Economics. Mahwah, NJ:Lawrence Erlbaum; 2000:219-264.25. Leclerc F, Schmitt BH, Dube L. Waiting time and decision making: is time likemoney? J Consumer Res. 1995;22:110-119. 26. Phelps CE. Health Economics. NewYork, NY: HarperCollins; 1992.27. Sun BC, Burstin HR, Brennan TA. Predictors and outcomes of frequent emer-gency department users. Acad Emerg Med. 2003;10:320-328.28. Wong MD, Andersen R, Sherbourne CD, et al. Effects of cost sharing on careseeking and health status: results from the Medical Outcomes Study. Am J PublicHealth. 2001;91:1889-1894.29. Zenner PA, Parke R, Mirkin DP, for Milliman. Insight into two analyticalchallenges for disease management. Milliman Research Report. April 2004.http://publications.milliman.com/research/health-rr/archive/pdfs/Two-Analytical-Challenges-Disease-Management-RR04-01-04.pdf. Accessed August 11, 2004. 30. Johnson A. Measuring DM’s net effect is harder than you might think. ManagCare. 2003;12:28-32.
BUSINESS
254 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4

Expect the Unexpected
255www.AHDBonline.com l American Health & Drug BenefitsVol 3, No 4 l July/August 2010
EMPLOYERS/PAYERS: The implications ofbehavioral economics may differ by medical conditionand by geography. At PPG Industries, we wanted toverify the status of hospital admissions for acute coro-nary artery disease (CAD), in which the “concern”factor is self-evident in 29 of our geographicallydiverse, active working populations. We wanted to seethe effect of copayment, coinsurance, or patient out-of-pocket (OOP) contribution, and the availability ofprimary care inside and outside the worksite. This mayhave scientific and philosophical implications.We calculated the variance of acute CAD hospital
admissions and emergency department (ED) visit ratesper 1000 active employees, based on the presence orabsence of (1) worksite wellness programs (high/lowrank), (2) worksite occupational health professionals(ie, nurse) on staff, and (3) the availability of primarycare physicians (PCPs) in the county where the work-site is located, according to the County HealthRankings.1In our data set, PCP availability rate at the county
level is significantly associated with a reduction inCAD and in ED visit (P <.05) and CAD acute admis-sions rates per 1000 active employees (P <.05). Havingworksite wellness programs (high rank) is associatedwith 2.8-fold fewer acute CAD admissions but has noeffect on CAD-related ED visit rates. Having a work-site occupational health nurse on staff is associatedwith 2.1-fold fewer acute CAD admissions but has noeffect on ED visit rates.What is the role of patient copayment and coinsur-
ance, namely, patient OOP contribution? As much as48% of the variance in acute hospital admissions forCAD in 29 worksites is explained by 3 factors—work-site wellness (P <.01), worksite nurse (P <.05), andOOP cost (P <.05). These interactions are shown inthe prediction profiler (Figure, Panel A, page 256).The practical implications vary by factor. CAD
admissions could be halved from 8/1000 to 4/1000employees by increasing the OOP from 10% to 30%,or by having a worksite nurse or high-rank wellnessprograms on site. If a nurse and such programs arecombined, the hospital admission rate is practicallyreduced to zero.The implications of this are serious. Acting on the
behavioral economic ramifications would require a30% penalty to “scare” half of the admissions away—an ethically questionable, and not plausible, solution.Instead, providing education and frontline profession-al assistance does provide a win-win situation, wherepatients seemingly are healthier and more informeddecision makers.What if we enter in the model the PCP availability
at the county level? This overrides the significance ofhaving a worksite nurse, confirms the relevance ofworksite wellness programs, while OOP costs lose sta-tistical significance (Figure, Panel B, page 256). Thisleads us to hypothesize that health education and pri-mary care do matter, and that occupational nurse sup-port to some extent compensates for the lack of “out-side” primary care by providing some medical homefunction, where that is faltering.These results lead us to the philosophical argument.
In the present study by Dr Tzeel and Mr Brown, it isunclear whether reducing the ED copayment was asso-ciated with discretionary spending on primary careand/or health promotion and, therefore, shifted pur-chasing from ED visits to primary care and/or wellness.But even if that were not the case, establishing a med-ical home would have tangible and intangible effectson many factors and behaviors.In a fair system, a better incentive to counteract the
overuse of ED rather than copayments would be toprovide education and primary care. In sound bites,this may translate to, “If you want health benefits, findyourself a PCP first.” But the game is not neutral. If wecould for a moment make room for evidence-based dis-cussion instead of falling into our preferred prejudices,we would see that the system is such that primary careis penalized, because the provider requires time—goodinformation is hard to organize, and there is no reim-bursement for “medical intelligence” oversight. Medical homelessness is attracting increasing atten-
tion.2 Medical homelessness has been defined in a blogby Dr Bob as, “Not having access to a consistent famil-iar medical setting. Not having a care location whereone is known, or where the medical information isaccurate.”2 In a recent article on medical homelessnesspublished in Health Affairs, Jack Colwill, MD,describes what happens to educated and willing people
Medical Homelessness and Emergency Department Utilization:Economic and Moral Implications
STAKEHOLDER PERSPECTIVE
Continued

BUSINESS
256 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
when they are left without primary care coordinationin spite of a wealth of disjointed specialty care offer-ings.3 One can imagine what would happen to less edu-cated people whose suffering may be needlessly magni-fied by their medical homelessness, despite theirinsurance access.Health insurance companies pretending to become
the medical home may introduce an additional moralhazard, where what is best for the patient is not neces-sarily what is best for their shareholders, because doc-tors are paid by procedures, not by outcomes, and areincluded in networks based on price and not onpatient needs.Dr Colwill describes how medical homes are dis-
couraged by the payment system for physicians and bythe nation’s shortage of PCPs. Given the current UShealthcare system, many patients end up being theirown medical home and the prime healthcare decisionmakers, albeit without appropriate information,knowledge, or assistance. Patients are reduced to con-sumers vulnerable to sales pitches rather thaninformed citizens. In many instances, rather thanpatient empowerment, this becomes a case of patient
abandonment in a confusing, complex, fragmentedand “dis”-integrated, when not adversarial, system.With primary care becoming increasingly scarce,notable primary care “deserts” are becoming evident insemirural areas.So, we welcome behavioral economics rather than
just “deterministic” economics; however, we shouldwonder if people “buy” not only based on their emo-tions but also based on what is available in their terri-tory. In primary care “deserts,” perhaps they acceptwhat is for what is best, not knowing better, and endup “buying” emergency care because there is no othermedical safe haven to fall back on. In that case, EDoveruse is a symptom of medical homelessness, a deep-er problem than mere access to health insurance.1. County Health Rankings. 2010. http://www.countyhealthrankings.org/.Accessed July 26, 2010.2. Dr Rob. The Problem of Medical Homelessness. Better Health Network.Opinion. Published September 2, 2009. http://getbetterhealth.com/the-prob-lem-of-medical-homelessness/ 2009.09.29. Accessed July 27, 2010.3. Colwill JM. Narrative matters. A case of ‘medical homelessness.’ Health Aff(Millwood). 2010;29:1067-1070.
Alberto M. Colombi, MD, MPHCorporate Medical Director
PPG Industries, Pittsburgh, PA
CAD indicates coronary artery disease; PCP, primary care physician.
Figure Acute CAD Admission Rate per 1000 Active Employees (a multifactorial analysis)
0.0833Nurse High/low rank (1-0) Coinsurance + copay
No Yes 0 1 0 0.1 0.2 0.3 0.4
15
10
5
0
Admissions/1000 acute CAD
8.26
5651
±2.82
9813
Panel A (r 2 = 0.48; P <.001)
Panel B (r 2 = 0.45; P <.002)
50 100 150 200 0 1 0 0.1 0.2 0.3 0.4
15
10
5
0
Admissions/1000 acute CAD
6.78
9074
±2.44
13
130.93 0.06185PCP rate High/low rank (1-0) Coinsurance + copay
STAKEHOLDER PERSPECTIVE (Continued)

Partnership. People. Programs. Passion. The Flexibility You Need. The Integrity You Deserve.
| M A N A G E D M A R K E T S Leaders in Business. Partners in Care.
Visit Takeda on the Web at www.tpna.com.

258 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
American Health & Drug Benefits offers an open forum for all healthcare stakeholders toexchange ideas and present their data, innovations, and initiatives to facilitate patient-centered healthcareand benefit design models that meet the needs of all stakeholders—Distributors, Employers, Evaluators,Manufacturers, Patients, Payers, Providers, Purchasers, Regulators, and Researchers.
Readers are invited to submit articles that aim at improving the quality of patient care and the US healthcaredelivery system in general and of benefit design strategies in particular. All articles will undergo a blind peerreview, and acceptance is based on that review.
AGING/DEMENTIA—With the aging of the USpopulation, there is a growing need for early imple-mentation of outcome-based preventive and therapeu-tic strategies for older people.
ALLERGIES—Allergies, such as allergic or seasonalrhinitis, affect millions of Americans daily, resultingin a significant economic burden and human cost.Under treatment and lack of adherence are commonobstacles to patient management.
ARTHRITIS—Musculoskeletal conditions, such asrheumatoid arthritis or osteoporosis, are on the increase,yet many patients are undiagnosed and untreated.Comparing new and available therapies is a key targetfor improving patient outcomes and reducing costs.
CANCER CARE—The growing focus on biologicagents dictates an enhanced study of these therapeu-tic options, including reimbursement policies, cost-management, industry trends, and the biologicpipeline updates.
CARDIOVASCULAR DISEASE—Still a leadingcause of morbidity and mortality among men andwomen. Original, outcome-based research on appro-priate therapies, cost-comparisons, emerging preven-tion strategies, and comparative effectiveness of bestpractices will enhance readers’ decision-making.
DIABETES, OBESITY—The increasing comorbidepidemics of these twin conditions mandates a thor-ough examination of best therapies, adherence issues,access, and prevention strategies. We invite articlesthat will address how to improve patient outcomesand best individualized patient care.
GASTROINTESTINAL CONDITIONS—Recognizing GI conditions, such as hepatitis C,Crohn’s disease, or inflammatory bowel disorder,remains a challenge.
INFECTIOUS DISEASES—The spread of commonand emerging pathogens within the hospital and inthe community remains a major concern requiringincreased vigilance.
MENTAL DISORDERS—Depression, bipolar disor-der, and schizophrenia exert a huge financial andhuman burden on individuals, employers, and payers.Topics of interest include comparative effectivenessanalyses, best practices, and reimbursement.
PAIN MANAGEMENT—Chronic pain is associatedwith a slew of complicated medical disorders and anenormous economic burden, yet pain medications arestill underused. Appropriate topics include best thera-pies, diagnosis, and clinicians’ anxiety about addictionissues and potential misuse.
Manuscripts should follow the Guidelines for Authors, available at www.AHDBonline.com For more information, call 732-992-1892
CALL FOR PAPERS
Areas of high interest include:
Clinical topics of interest include:
• Adherence Issues
• Benefit Design
• Comparative Effectiveness Analyses
• Cost-Effectiveness Analyses
• Decision-Making Tools
• Healthcare Trends
• Health Economics
• Health Plan Initiatives/Innovation
• Health Information Technology
• Innovation in Patient Care
• Off-label Use/Misuse
• Original Research
• Pharmacoeconomics
• Reimbursement Strategies
• Wellness Programs



261www.AHDBonline.com l American Health & Drug BenefitsVol 3, No 4 l July/August 2010
HEALTHCARE REFORM
The accountable care organization (ACO) modelis a new Medicare option for physicians, hospi-tals, and other providers to share in cost-savings.
ACOs represent a dramatic change in Medicare policyand an opportunity to transform care delivery andprovider alignment.
The Medicare Gain-Sharing Program, part of thenewly enacted healthcare reform law, creates the optionfor healthcare providers to form ACOs. Through anACO, providers will take responsibility for quality andoverall care of their Medicare patients. Medicare willthen share with ACO providers the savings fromimproved quality, fewer hospitalizations, and the elimi-nation of unnecessary costs.1,2
Starting in 2012, the ACO model will be a nation-wide option in Medicare fee-for-service (FFS). In addi-tion to shared savings, the ACO option includes free-dom of choice for Medicare beneficiaries, nationalquality measures, evidence-based medicine, patient-cen-tered care delivery, advanced care coordination, andinformation sharing.
Because the ACO model is designed to break down oldbarriers for providers to work together to improve care andreduce medical costs, state Medicaid programs and privatehealth insurers will likely join Medicare in supporting theACO model. Medicare may give preference to ACOs thatare participating in similar arrangements with Medicaid,private payers, and other third parties.
Specifically, Section 1899 of the Social Security Actgoverns the new Medicare Shared Savings Program andthe option for providers to form ACOs. The law was cre-ated by Section 3022 of the Patient Protection andAffordable Care Act of 2010 (PPACA). The Centers forMedicare & Medicaid Services (CMS) must implementthe ACO option no later than January 1, 2012.
Option for Physicians, Hospitals, and Other ProvidersA variety of providers will be able to form an ACO:
• Physicians and other professionals in group practicesor a network of practices, such as a large medicalgroup, an independent provider association, a network
of solo and small group physician practices, and, pre-sumably, a community health center
• Hospitals, physicians, physician groups, and otherhealthcare professionals via a joint venture or partner-ship arrangement
• Hospitals that employ physicians and other health-care professionals, such as an integrated hospital–physician system. Although the ACO is of keen interest to many hos-
pital systems, an ACO need not include a hospital.Physician participation, however, is mandatory.
CMS may permit other combinations or types ofproviders to form an ACO. Therefore, other possibilitiesinclude hospitals, physicians, and postacute providers,such as skilled nursing facilities and home health agencies.
Providers are ineligible to participate in an ACO ifthey participate in a Medicare shared-savings demon-stration, such as the Physician Group Practice Demon -stration project or the new Independence at Homemedical practice pilot.3
Medicare Beneficiary AssignmentAssignment of Medicare beneficiaries to ACOs will
be invisible to the beneficiary. Receiving services froman ACO will not affect Medicare coverage, benefitdesign, or a beneficiary’s freedom to choose physiciansand other providers. Beneficiaries in Medicare Part Aor Part B FFS programs may receive covered servicesfrom any Medicare provider, regardless of whether theprovider is part of an ACO. Medicare beneficiaries whoelect a Medicare Advantage plan are excluded fromthe ACO program.
Minimum Requirements for ACOsAn ACO must have a patient base of at least 5000
Medicare FFS beneficiaries, with participating providersagreeing to accept responsibility for overall patient careand quality for at least 3 years. In addition, to gainMedicare recognition as an ACO, the provider organi-zation, partnership, or joint venture forming the ACOmust meet the following minimum requirements:• A sufficient number of primary care physicians toserve the ACO’s patient population
• A formal legal structure to receive and distributeshared savings
Kip Piper is a Senior Advisor to TogoRun, Sellers Dorsey, andFleishman-Hillard. He is Health Policy Editor of AmericanHealth & Drug Benefits.
The New Accountable Care Organizationsand Medicare Gain-Sharing ProgramKip Piper, MA, FACHE See also Interview with Dr McClellan, page 242

• A leadership and management structure that includesclinical and administrative systems
• Provide sufficient information on participatingproviders and their services to support beneficiarytracking and the determination of payments forshared savings
• Defined processes and systems to:• Promote the practice of evidence-based medicine• Meet federal criteria for patient-centered care• Coordinate care• Report the necessary data for CMS to monitorand assess the ACO’s performance compared withfederally defined clinical performance measuresand cost benchmarks
• Meet federal requirements for electronic prescribingand electronic health records
• Participate in the existing Medicare PhysicianQuality Reporting Initiative, which is expandingunder PPACA.4
Medicare Payment and Shared SavingsSeveral payment methods are possible for ACOs.
Under the primary method, ACO providers will beincentivized to improve clinical performance while con-trolling Medicare spending through, for example, reduc-ing hospitalizations and eliminating unnecessary costs.Specifically, the ACO will receive additional paymentsfrom Medicare if (1) the ACO meets federal expecta-tions for clinical performance, and (2) the ACO’sMedicare per-capita FFS costs are a certain percentagebelow a benchmark.
CMS will set the clinical performance measuresand the proportion of Medicare cost-savings that willbe shared with ACOs. The law sets a methodology forsetting a benchmark for predicted per-capita Part Aand Part B costs. The law allows CMS to create otherpayment methods for ACOs, such as partial capita-tion or global fees. Risk-based payments may be limit-ed to highly integrated health systems and ACOscapable of bearing risk.
Learning from Other Gain-Sharing ProjectsProviders planning to form Medicare ACOs in 2012
may learn from the Brookings-Dartmouth ACOCollaborative, which currently has 5 private sector pilotACOs operating in Arizona, California, Kentucky, andVirginia.5-7 Many of the requirements for MedicareACOs are modeled on recommendations from theBrookings-Dartmouth ACO Collaborative.5-7
Meanwhile, PPACA extended the existing Medicaregain-sharing demonstration through September 2011and created the Medicare Independence at Home pro-gram, a gain-sharing demonstration to test in-home
primary care services for Medicare patients with multiplechronic conditions.8
ObstaclesThe ACO option and the accompanying shared-
savings model raise some potential legal obstacles thatmust be resolved before 2012. In the rules setting up theACO option, the Secretary of the Department of Healthand Human Services (HHS) will have to waive certainlaws and rules that conflict with the gain sharing andprovider alignment in ACOs. Specifically, aspects oflongstanding federal antikickback and physician self-referral laws must be waived for ACO-participatingproviders. HHS will need to waive the laws enough forthe ACO model to work well but not to create unin-tended loopholes. The new law provides the HHS secre-tary with the necessary waiver authority.
In addition, the ACO model may run afoul of federalor state antitrust laws. The Federal Trade Commission(FTC), which oversees and enforces antitrust lawsregarding healthcare providers, will have to offer specif-ic guidance. Like the FTC, state attorneys general willhave to adapt their traditional antitrust thinking to thenew business relationships contemplated under theACO model.
Next Steps ACOs offer the potential for a genuine win-win sit-
uation for physicians, hospitals, beneficiaries, and tax-payers. The precise details for forming and operating anACO will be laid out in federal regulations. CMS isexpected to release a proposed rule on ACOs in late2010, with a final rule likely by mid-2011. Developingrules governing ACOs is one of many tasks facing thenew CMS Administrator, Donald Berwick, MD. �
References1. US Social Security Administration. Compilation of the Social Security laws:shared savings program. www.ssa.gov/OP_Home/ssact/title18/1899.htm. AccessedJune 15, 2010.2. Centers for Medicare & Medicaid Services, Office of Legislation. Medicare“accountable care organizations” Shared Savings Program—New Section 1899 ofTitle XVIII: Preliminary Questions and Answers. June 2010. www.cms.gov/OfficeofLegislation/Downloads/AccountableCareOrganization.pdf. Accessed June 15, 2010.3. Centers for Medicare & Medicaid Services, Office of Research, Development, andInformation. Medicare Physician Group Practice Demonstration. August 2009. www.cms.gov/DemoProjectsEvalRpts/downloads/PGP_Fact_Sheet.pdf. Accessed June 15, 2010.4. Centers for Medicare & Medicaid Services Medicare Physician Quality ReportingInitiative (PQRI). www.cms.gov/pqri/. Accessed June 15, 2010.5. McClellan M, McKethan AN, Lewis JL, et al. A national strategy to put account-able care into practice. Health Aff (Millwood). 2010;29:982-990. 6. Fisher ES, Staiger DO, Bynum JP, Gottlieb DJ. Creating accountable care organi-zations: the extended hospital medical staff. Health Aff (Millwood). 2007;26:44-57.Epub 2006 Dec 5. 7. Engelberg Center for Health Care Reform at Brookings, Brookings Institution, andthe Dartmouth Institute for Health Policy & Clinical Practice. Brookings-DartmouthACO Learning Network. 2010. www.acolearningnetwork.org. Accessed June 15, 2010.8. The Patient Protection and Affordable Care Act, 42 USC 18001, §1866D offederal Social Security Act, as enacted under §3024 (Pub L No. 111-148), March23, 2010. www.gpo.gov/fdsys/pkg/PLAW-111publ148/pdf/PLAW-111publ148.pdf.Accessed June 15, 2010.
HEALTHCARE REFORM
262 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4

In the largest phase 3 study (6 months): • 45% of patients who received ULORIC 40 mg achieved serum uric acid level <6 mg/dL (N=757)
compared to 42% of patients who received allopurinol 300 mg (N=755; p=0.233)1
• 67% of patients who received ULORIC 80 mg achieved serum uric acid level <6 mg/dL (N=756) compared to 42% of patients who received allopurinol 300 mg (N=755; p<0.001)1
ULORIC powerfully lowers serum uric acid levels for long-term control of gout.
ULORIC® is a registered trademark of Teijin Pharma Limited and used under license by Takeda Pharmaceuticals America, Inc.©2009 Takeda Pharmaceuticals North America, Inc. TXF-00321 08/09
infarctions, and non-fatal strokes) in patients treated with ULORIC [0.74 per 100 P-Y (95% CI 0.36-1.37)] than allopurinol [0.60 per 100 P-Y (95% CI 0.16-1.53)]. A causal relationship with ULORIC has not been established. Monitor for signs and symptoms of MI and stroke.
• Liver Enzyme Elevations: In randomized controlled studies, transaminase elevations greater than 3 times the upper limit of normal (ULN) were observed (AST: 2%, 2%, and ALT: 3%, 2% in ULORIC and allopurinol-treated patients, respectively). No dose-effect relationship for these transaminase elevations was noted. Laboratory assessment of liver function is recommended at, for example, 2 and 4 months following initiation of ULORIC and periodically thereafter.
• Adverse reactions occurring in at least 1% of ULORIC-treated patients, and, at least 0.5% greater than placebo, are liver function abnormalities, nausea, arthralgia, and rash.
Individual results may vary based on factors such as baseline serum uric acid levels. Please see brief summary of complete Prescribing Information on adjacent pages.Reference: 1. ULORIC® (febuxostat) full prescribing information, February 2009.
For more information, please visit www.ULORIC.com
IndicationULORIC is a xanthine oxidase (XO) inhibitor indicated for the chronic management of hyperuricemia in patients with gout. ULORIC is not recommended for the treatment of asymptomatic hyperuricemia.
Important Safety Information• ULORIC is contraindicated in patients being treated
with azathioprine, mercaptopurine, or theophylline.
• An increase in gout fl ares is frequently observed during initiation of anti-hyperuricemic agents, including ULORIC. If a gout fl are occurs during treatment, ULORIC need not be discontinued. Prophylactic therapy (i.e. - NSAIDs or colchicine) upon initiation of treatment may be benefi cial for up to six months.
• Cardiovascular Events: In randomized controlled studies, there was a higher rate of cardiovascular thromboembolic events (cardiovascular deaths, non-fatal myocardial

BRIEF SUMMARY OF FULL PRESCRIBING INFORMATION for ULORIC® (febuxostat) tabletsINDICATIONS AND USAGEULORIC® is a xanthine oxidase (XO) inhibitor indicated for the chronic management of hyperuricemia in patients with gout.
ULORIC is not recommended for the treatment of asymptomatic hyperuricemia.
CONTRAINDICATIONSULORIC is contraindicated in patients being treated with azathioprine, mercapto-purine, or theophylline [see Drug Interactions]. WARNINGS AND PRECAUTIONSGout FlareAfter initiation of ULORIC, an increase in gout flares is frequently observed. This increase is due to reduction in serum uric acid levels resulting in mobilization of urate from tissue deposits.
In order to prevent gout flares when ULORIC is initiated, concurrent prophylactic treatment with an NSAID or colchicine is recommended.
Cardiovascular Events In the randomized controlled studies, there was a higher rate of cardiovascular thrombo embolic events (cardiovascular deaths, non-fatal myocardial infarctions, and non-fatal strokes) in patients treated with ULORIC [0.74 per 100 P-Y (95% CI 0.36-1.37)] than allopurinol [0.60 per 100 P-Y (95% CI 0.16-1.53)] [see Adverse Reactions]. A causal relationship with ULORIC has not been established. Monitor for signs and symptoms of myocardial infarction (MI) and stroke.
Liver Enzyme Elevations During randomized controlled studies, transaminase elevations greater than 3 times the upper limit of normal (ULN) were observed (AST: 2%, 2%, and ALT: 3%, 2% in ULORIC and allopurinol-treated patients, respectively). No dose-effect relationship for these transaminase elevations was noted. Laboratory assessment of liver function is recommended at, for example, 2 and 4 months following initiation of ULORIC and periodically thereafter.
ADVERSE REACTIONSClinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
A total of 2757 subjects with hyperuricemia and gout were treated with ULORIC 40 mg or 80 mg daily in clinical studies. For ULORIC 40 mg, 559 patients were treated for 6 months. For ULORIC 80 mg, 1377 subjects were treated for
6 months, 674 patients were treated for 1 year and 515 patients were treated for 2 years.
Most Common Adverse ReactionsIn three randomized, controlled clinical studies (Studies 1, 2 and 3), which were 6 to 12 months in duration, the following adverse reactions were reported by the treating physician as related to study drug. Table 1 summarizes adverse reactions reported at a rate of at least 1% in ULORIC treatment groups and at least 0.5% greater than placebo.
Table 1: Adverse Reactions Occurring in 1% of ULORIC-Treated Patients and at Least 0.5% Greater than Seen in Patients
Receiving Placebo in Controlled Studies
Adverse Reactions
Placebo ULORIC allopurinol*
(N=134)
40 mg daily
(N=757)
80 mg daily
(N=1279) (N=1277)Liver Function Abnormalities 0.7% 6.6% 4.6% 4.2%
Nausea 0.7% 1.1% 1.3% 0.8%
Arthralgia 0% 1.1% 0.7% 0.7%
Rash 0.7% 0.5% 1.6% 1.6%
* Of the subjects who received allopurinol, 10 received 100 mg, 145 received 200 mg, and 1122 received 300 mg, based on level of renal impairment.
The most common adverse reaction leading to discontinuation from therapy was liver function abnormalities in 1.8% of ULORIC 40 mg, 1.2% of ULORIC 80 mg, and in 0.9% of allopurinol-treated subjects.
In addition to the adverse reactions presented in Table 1, dizziness was reported in more than 1% of ULORIC-treated subjects although not at a rate more than 0.5% greater than placebo.
Less Common Adverse ReactionsIn phase 2 and 3 clinical studies the following adverse reactions occurred in less than 1% of subjects and in more than one subject treated with doses ranging from 40 mg to 240 mg of ULORIC. This list also includes adverse reactions (less than 1% of subjects) associated with organ systems from Warnings and Precautions.
Blood and Lymphatic System Disorders: anemia, idiopathic thrombocytopenic purpura, leukocytosis/leukopenia, neutropenia, pancytopenia, splenomegaly, throm bo cytopenia; Cardiac Disorders: angina pectoris, atrial fibrillation/flutter, cardiac murmur, ECG abnormal, palpitations, sinus bradycardia, tachycardia; Ear and Labyrinth Disorders: deafness, tinnitus, vertigo; Eye Disorders: vision blurred; Gastrointestinal Disorders: abdominal distention, abdominal pain, constipation, dry mouth, dyspepsia, flatulence, frequent stools, gastritis, gastro esophageal reflux disease, gastrointestinal discomfort, gingival pain, haematemesis, hyperchlorhydria, hematochezia, mouth ulceration, pancreatitis, peptic ulcer, vomiting; General Disorders and Administration Site Conditions: asthenia, chest pain/discomfort, edema, fatigue, feeling abnormal, gait disturbance, influenza-like symptoms, mass, pain, thirst; Hepatobiliary Disorders: cholelithiasis/cholecystitis, hepatic steatosis, hepatitis, hepatomegaly; Immune System Disorder: hypersensitivity; Infections and Infestations: herpes zoster; Procedural Complications: contusion; Metabolism and Nutrition Disorders: anorexia, appetite decreased/increased, dehydration, diabetes mellitus, hyper-cholesterolemia, hyperglycemia, hyperlipidemia, hypertriglyceridemia, hypokalemia, weight decreased/increased; Musculoskeletal and Connective Tissue Disorders: arthritis, joint stiffness, joint swelling, muscle spasms/twitching/tightness/weakness, musculoskeletal pain/stiffness, myalgia; Nervous System Disorders: altered taste, balance disorder, cerebrovascular accident, Guillain-Barré syndrome, headache, hemiparesis, hypoesthesia, hyposmia, lacunar infarction, lethargy, mental impairment, migraine, paresthesia, somnolence, transient ischemic attack, tremor; Psychiatric Disorders: agitation, anxiety, depression, insomnia, irritability, libido decreased, nervousness, panic attack, personality change; Renal and Urinary Disorders: hematuria, nephrolithiasis, pollakiuria, proteinuria, renal failure, renal insufficiency, urgency, incontinence; Reproductive System and Breast Changes: breast pain, erectile dysfunction, gynecomastia; Respiratory, Thoracic and Mediastinal Disorders: bronchitis, cough, dyspnea, epistaxis, nasal dryness, paranasal sinus hypersecretion, pharyngeal edema, respiratory tract congestion, sneezing, throat irritation, upper respiratory tract infection; Skin and Subcutaneous Tissue Disorders: alopecia, angio edema, dermatitis, dermographism, ecchymosis, eczema, hair color changes, hair growth abnormal, hyperhidrosis, peeling skin, petechiae, photosensitivity, pruritus, purpura, skin discoloration/altered pigmentation, skin lesion, skin odor abnormal, urticaria; Vascular Disorders: flushing, hot flush, hypertension, hypotension; Laboratory Parameters: activated partial thromboplastin time prolonged, creatine increased, bicarbonate decreased, sodium increased, EEG abnormal, glucose increased, cholesterol increased, triglycerides increased, amylase increased, potassium increased, TSH increased, platelet count decreased, hematocrit decreased, hemoglobin decreased, MCV increased, RBC decreased, creatinine increased, blood urea increased, BUN/creatinine ratio increased, creatine phosphokinase (CPK) increased, alkaline phosphatase increased, LDH increased, PSA increased, urine output increased/decreased, lymphocyte count decreased, neutrophil count decreased, WBC increased/decreased, coagulation test abnormal, low density lipoprotein (LDL) increased, prothrombin time prolonged, urinary casts, urine positive for white blood cells and protein.
Cardiovascular SafetyCardiovascular events and deaths were adjudicated to one of the pre-defined endpoints from the Anti-Platelet Trialists’ Collaborations (APTC) (cardiovascular death, non-fatal myocardial infarction, and non-fatal stroke) in the randomized controlled and long-term extension studies. In the Phase 3 randomized controlled studies, the incidences of adjudicated APTC events per 100 patient-years of exposure were: Placebo 0 (95% CI 0.00-6.16), ULORIC 40 mg 0 (95% CI 0.00-1.08), ULORIC 80 mg 1.09 (95% CI 0.44-2.24), and allopurinol 0.60 (95% CI 0.16-1.53).
In the long-term extension studies, the incidences of adjudicated APTC events were: ULORIC 80 mg 0.97 (95% CI 0.57-1.56), and allopurinol 0.58 (95% CI 0.02-3.24).
Overall, a higher rate of APTC events was observed in ULORIC than in allopurinol-treated patients. A causal relationship with ULORIC has not been established. Monitor for signs and symptoms of MI and stroke.
DRUG INTERACTIONSXanthine Oxidase Substrate DrugsULORIC is an XO inhibitor. Drug interaction studies of ULORIC with drugs that are metabolized by XO (e.g., theophylline, mercaptopurine, azathioprine) have not been conducted. Inhibition of XO by ULORIC may cause increased plasma concentrations of these drugs leading to toxicity [see Clinical Pharmacology]. ULORIC is contraindicated in patients being treated with azathioprine, mercaptopurine, or theophylline [see Contraindications]. Cytotoxic Chemotherapy DrugsDrug interaction studies of ULORIC with cytotoxic chemotherapy have not been conducted. No data are available regarding the safety of ULORIC during cytotoxic chemotherapy.
In Vivo Drug Interaction StudiesBased on drug interaction studies in healthy subjects, ULORIC does not have clinically significant interactions with colchicine, naproxen, indomethacin, hydrochlorothiazide, warfarin or desipramine. Therefore, ULORIC may be used concomitantly with these medications.

USE IN SPECIFIC POPULATIONS PregnancyPregnancy Category C: There are no adequate and well-controlled studies in pregnant women. ULORIC should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Febuxostat was not teratogenic in rats and rabbits at oral doses up to 48 mg per kg (40 and 51 times the human plasma exposure at 80 mg per day for equal body surface area, respectively) during organogenesis. However, increased neonatal mortality and a reduction in the neonatal body weight gain were observed when pregnant rats were treated with oral doses up to 48 mg per kg (40 times the human plasma exposure at 80 mg per day) during organogenesis and through lactation period.
Nursing MothersFebuxostat is excreted in the milk of rats. It is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when ULORIC is administered to a nursing woman.
Pediatric UseSafety and effectiveness in pediatric patients under 18 years of age have not been established.
Geriatric UseNo dose adjustment is necessary in elderly patients. Of the total number of subjects in clinical studies of ULORIC, 16 percent were 65 and over, while 4 percent were 75 and over. Comparing subjects in different age groups, no clinically significant differences in safety or effectiveness were observed but greater sensitivity of some older individuals cannot be ruled out. The Cmax and AUC24 of febuxostat following multiple oral doses of ULORIC in geriatric subjects ( 65 years) were similar to those in younger subjects (18-40 years).
Renal ImpairmentNo dose adjustment is necessary in patients with mild or moderate renal impairment (Clcr 30-89 mL per min). The recommended starting dose of ULORIC is 40 mg once daily. For patients who do not achieve a sUA less than 6 mg per dL after 2 weeks with 40 mg, ULORIC 80 mg is recommended.
There are insufficient data in patients with severe renal impairment (Clcr less than 30 mL per min); therefore, caution should be exercised in these patients.
Hepatic ImpairmentNo dose adjustment is necessary in patients with mild or moderate hepatic impairment (Child-Pugh Class A or B). No studies have been conducted in patients with severe hepatic impairment (Child-Pugh Class C); therefore, caution should be exercised in these patients.
Secondary HyperuricemiaNo studies have been conducted in patients with secondary hyperuricemia (including organ transplant recipients); ULORIC is not recommended for use in patients whom the rate of urate formation is greatly increased (e.g., malignant disease and its treatment, Lesch-Nyhan syndrome). The concentration of xanthine in urine could, in rare cases, rise sufficiently to allow deposition in the urinary tract.
OVERDOSAGEULORIC was studied in healthy subjects in doses up to 300 mg daily for seven days without evidence of dose-limiting toxicities. No overdose of ULORIC was reported in clinical studies. Patients should be managed by symptomatic and supportive care should there be an overdose.
CLINICAL PHARMACOLOGY PharmacodynamicsEffect on Uric Acid and Xanthine Concentrations: In healthy subjects, ULORIC resulted in a dose dependent decrease in 24-hour mean serum uric acid concentrations, and an increase in 24-hour mean serum xanthine concentrations. In addition, there was a decrease in the total daily urinary uric acid excretion. Also, there was an increase in total daily urinary xanthine excretion. Percent reduction in 24-hour mean serum uric acid concentrations was between 40% to 55% at the exposure levels of 40 mg and 80 mg daily doses.
Effect on Cardiac Repolarization: The effect of ULORIC on cardiac repolarization as assessed by the QTc interval was evaluated in normal healthy subjects and in patients with gout. ULORIC in doses up to 300 mg daily, at steady state, did not demonstrate an effect on the QTc interval.
Special PopulationsRenal Impairment: Following multiple 80 mg doses of ULORIC in healthy subjects with mild (Clcr 50-80 mL per min), moderate (Clcr 30-49 mL per min) or severe renal impairment (Clcr 10-29 mL per min), the Cmax of febuxostat did not change relative to subjects with normal renal function (Clcr greater than 80 mL per min). AUC and half-life of febuxostat increased in subjects with renal impairment in comparison to subjects with normal renal function, but values were similar among three renal impairment groups. Mean febuxostat AUC values were up to 1.8 times higher in subjects with renal impairment compared to those with normal renal function. Mean Cmax and AUC values for 3 active metabolites increased up to 2- and 4-fold, respectively. However, the percent decrease in serum uric acid concentration for subjects with renal impairment was comparable to those with normal renal function (58% in normal renal function group and 55% in the severe renal function group).
No dose adjustment is necessary in patients with mild to moderate renal impairment [see Dosage and Administration and Use in Specific Populations]. The recommended starting dose of ULORIC is 40 mg once daily. For patients who do not achieve a sUA less than 6 mg per dL after 2 weeks with 40 mg, ULORIC 80 mg is recommended. There is insufficient data in patients with severe renal impairment; caution should be exercised in those patients [see Use in Specific Populations. ULORIC has not been studied in end stage renal impairment patients who are on dialysis. Hepatic Impairment: Following multiple 80 mg doses of ULORIC in patients with mild (Child-Pugh Class A) or moderate (Child-Pugh Class B) hepatic impairment, an average of 20-30% increase was observed for both Cmax and AUC24 (total and unbound) in hepatic impairment groups compared to subjects with normal hepatic function. In addition, the percent decrease in serum uric acid concentration was comparable between different hepatic groups (62% in healthy group, 49% in mild hepatic impairment group, and 48% in moderate hepatic impairment group). No dose adjustment is necessary in patients with mild or moderate hepatic impairment. No studies have been conducted in subjects with severe hepatic impairment (Child-Pugh Class C); caution should be exercised in those patients [see Use in Specific Populations. NONCLINICAL TOXICOLOGY Carcinogenesis, Mutagenesis, Impairment of FertilityCarcinogenesis: Two-year carcinogenicity studies were conducted in F344 rats and B6C3F1 mice. Increased transitional cell papilloma and carcinoma of urinary bladder was observed at 24 mg per kg (25 times the human plasma exposure at maximum recommended human dose of 80 mg per day) and 18.75 mg per kg (12.5 times the human plasma exposure at 80 mg per day) in male rats and female mice, respectively. The urinary bladder neoplasms were secondary to calculus formation in the kidney and urinary bladder.Mutagenesis: Febuxostat showed a positive mutagenic response in a chromosomal aberration assay in a Chinese hamster lung fibroblast cell line with and without metabolic activation in vitro. Febuxostat was negative in the in vitro Ames assay and chromosomal aberration test in human peripheral lymphocytes, and L5178Y mouse lymphoma cell line, and in vivo tests in mouse micronucleus, rat unscheduled DNA synthesis and rat bone marrow cells.Impairment of Fertility: Febuxostat at oral doses up to 48 mg per kg per day (approximately 35 times the human plasma exposure at 80 mg per day) had no effect on fertility and reproductive performance of male and female rats. Animal ToxicologyA 12-month toxicity study in beagle dogs showed deposition of xanthine crystals and calculi in kidneys at 15 mg per kg (approximately 4 times the human plasma exposure at 80 mg per day). A similar effect of calculus formation was noted in rats in a six-month study due to deposition of xanthine crystals at 48 mg per kg (approximately 35 times the human plasma exposure at 80 mg per day).PATIENT COUNSELING INFORMATION[see FDA-Approved Patient Labeling in the full prescribing information]General InformationPatients should be advised of the potential benefits and risks of ULORIC. Patients should be informed about the potential for gout flares, elevated liver enzymes and adverse cardiovascular events after initiation of ULORIC therapy. Concomitant prophylaxis with an NSAID or colchicine for gout flares should be considered.Patients should be instructed to inform their healthcare professional if they develop a rash, chest pain, shortness of breath or neurologic symptoms suggesting a stroke. Patients should be instructed to inform their healthcare professional of any other medications they are currently taking with ULORIC, including over-the-counter medications.Distributed byTakeda Pharmaceuticals America, Inc.Deerfield, IL 60015U.S. Patent Nos. - 6,225,474; 7,361,676; 5,614,520. ULORIC® is a registered trademark of Teijin Pharma Limited and used under license by Takeda Pharmaceuticals America, Inc.All other trademark names are the property of their respective owners©2009 Takeda Pharmaceuticals America, Inc.February 2009For more detailed information, see the full prescribing information for ULORIC (febuxostat) tablets (PI1114 R1; February 2009) or contact Takeda Pharmaceuticals America, Inc. at 1.877.825.3327.PI1114 R1-Brf; February 2009L-TXF-0209-3

CLINICAL
266 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
Anti-tumor necrosis factor (TNF) therapy hasemerged as a major advancement in the man-agement of rheumatoid arthritis (RA). The
anti-TNF agents adalimumab, etanercept, and inflix-imab are often used with conventional disease-modify-ing antirheumatic drugs (DMARDs), such as methotrex-ate, and have been shown in clinical trials to be effectivein reducing the signs and symptoms of RA and in pre-venting the progression of joint damage.1-6
Significant limitations have been noted in the litera-ture as to outcomes of clinical trials and observationalstudies of anti-TNF therapy.7,8 Clinical trial inclusionand exclusion criteria specify select patient populations,which may not necessarily reflect the diversity of patientand disease characteristics in real-world clinical scenar-ios.8 Therefore, real-world studies can offer uniqueinsights over controlled clinical trials.9Although there is greater diversity of patient and dis-
ease characteristics in real-world studies, there may bebias, because patients receive various treatments.Nevertheless, healthcare decision makers are increasing-ly relying on studies of real-world outcomes for decisionsrelated to coverage and reimbursement.10 Many studieshave evaluated the effectiveness of anti-TNF therapiesin patients with RA,1-6 but few real-world studies have
Dr D’Souza is a Manager, and Dr Meissner was a Director(when this research was conducted), Xcenda, Palm Harbor,FL; Dr Tang was Director of Outcomes Research, MedicalAffairs Operations, Dr McKenzie is Regional Director, ClinicalAffairs, and Ms Piech is Vice President, Outcomes Researchand Biometrics, Centocor Ortho Biotech, Horsham, PA.
Effectiveness of Anti-Tumor NecrosisFactor Agents in the Treatment ofRheumatoid Arthritis: Observational StudyAnna D’Souza, PhD; Brian L. Meissner, PharmD, PhD; Boxiong Tang, MD, PhD; R. Scott McKenzie, MD; Catherine T. Piech, MBA
Objective: The efficacy of anti-tumor necrosis factor therapies in rheumatoid arthritis hasbeen demonstrated in randomized clinical trials. The purpose of the present study was toevaluate the effectiveness of these agents for the treatment of rheumatoid arthritis in a real-world setting.Method: This retrospective chart review included patients from 6 clinics in the UnitedStates. Eligibility criteria included age ≥18 years, diagnosis of rheumatoid arthritis, and hav-ing been initiated with anti-tumor necrosis factor therapy (ie, adalimumab, etanercept, orinfliximab) between January 1, 2002, and November 30, 2004. Patients were assessed forup to 2 years after therapy initiation. Primary outcomes of interest were improvements in 4effectiveness measures—joint pain, joint swelling, joint stiffness, and fatigue. A total of 496patients met the study’s inclusion criteria: 84 (16.9%) in the adalimumab group, 146(29.4%) in the etanercept group, and 266 (53.6%) in the infliximab group.Results: Improvement in 1 of the 4 effectiveness measures was documented in 36.8%(n = 25) who received adalimumab, in 47.7% (n = 62) of those who received etanercept, andin 48.7% (n = 115) of patients who received infliximab. The infliximab group was the onlycohort to demonstrate significant improvements from baseline in joint pain, joint swelling,and joint stiffness. The adalimumab group had significant improvement in joint pain (P = .004). No significant change in fatigue scores was reached with any of these agents.Conclusion: In the real-world setting of patients with rheumatoid arthritis, anti-tumornecrosis factor therapy shows significant improvements in joint pain, joint swelling, and jointstiffness, although there are differences in effectiveness in the 4 measures among the 3agents assessed in this study.
Am Health Drug Benefits.2010;3(4): 266-273.www.AHDBonline.comDisclosures are at end of text
Stakeholder Perspective, page 273

Effectiveness of Anti-TNF Agents in Rheumatoid Arthritis
267www.AHDBonline.com l American Health & Drug BenefitsVol 3, No 4 l July/August 2010
evaluated the clinical effectiveness of adalimumab, etan-ercept, and infliximab. The objective of this analysis wasto assess the effectiveness of these agents in improvingjoint pain, joint swelling, joint stiffness, and fatigueamong patients with RA.
MethodsWe conducted a retrospective, observational chart
review using data from 6 rheumatology clinics acrossthe United States, and evaluated treatment effective-ness among a sample of patients with RA who weretreated with anti-TNF therapy (ie, adalimumab, etan-ercept, or infliximab). The study period was fromJanuary 1, 2001, to November 30, 2006. For eachpatient, the observation period included a 1-year peri-od before the index date, which was the date of the firstanti-TNF prescription or administration, and a 2-yearfollow-up period after the index date (Figure). Baselinestatus was assessed during the year before the indexdate. Data were collected for a maximum of 2 yearsafter the index date, or until discontinuation of anti-TNF therapy, whichever occurred first. Patient selection was based on the following inclu-
sion criteria: age ≥18 years; diagnosis of RA; and thera-py initiated with adalimumab, etanercept, or infliximabbetween January 1, 2002, and November 30, 2004, withno documentation of previous anti-TNF therapy.Patients were required to be under the care of the par-ticipating physician or physician group, or have com-plete documentation (related to RA) from anotherprovider for a minimum of 12 months before the indexdate and up to 24 months after the index date (no min-imum follow-up period was required). Patients with a diagnosis of psoriasis, ulcerative coli-
tis, Crohn’s disease, or ankylosing spondylitis wereexcluded from the study, because of the differences inanti-TNF dosage recommendations. In addition,patients were excluded if they had a history of anti-TNFtherapy or any of the following diagnoses any time beforethe index date—malignancy (eg, lymphoma, solid organmalignancy), infection (eg, tuberculosis, bacterial pneu-monia), seizures, demyelinating disorders (eg, multiplesclerosis), heart failure, or drug-induced lupus. Participating clinics identified and provided charts for
all patients meeting the study inclusion criteria. Patientprivacy was maintained through the use of unique alpha-numeric values for each patient in compliance with theHealth Insurance Portability and Accountability Act(HIPAA). The study protocol was approved by the NewEngland Institutional Review Board.Data were collected using a standardized chart
review form with a graphical user interface developedin Microsoft Access. Patient demographics and con-
comitant DMARD use were collected. For this study,concomitant DMARD therapy included hydroxychlo -r oquine, leflunomide, sulfasalazine, azathioprine, peni-cillamine, and auranofin. Response to therapy was evaluated for joint pain,
joint swelling, joint stiffness, and fatigue. Because ofintra- and intervariability in documentation amongphysicians, a data abstraction form was used so that thechart reviewer could document both qualitative andquantitative data.
KEY POINTS
➤ Previous evidence from clinical trials has shownthat anti-TNF agents are effective for the treatment of arthritis.
➤ The goal of this study was to evaluate theeffectiveness of these agents (ie, adalimumab,etanercept, and infliximab) in reducing joint pain,swelling, and stiffness, and fatigue for patients withrheumatoid arthritis in the real-world setting.
➤ Approximately 76% of patients were usingconcomitant DMARD therapy; this was morecommon in patients taking infliximab thanetanercept or adalimumab.
➤ Nearly half of the patients reported animprovement in all 4 measures, but not allimprovements reached significant difference in the2-year follow-up.
➤ The only group with significant improvements in 3measures (all but fatigue) was the infliximab cohort.
➤ The adalimumab cohort had significantimprovements from baseline in joint pain.
➤ The etanercept cohort had the highest percentageof patients who had improvement in joint stiffness.
➤ None of the cohorts had significant improvementsin fatigue.
Figure Study Design
Outcomes assessment
Pretreatmentassessment
1 year beforeindex date
Index date(treatment
initiated withadalimumab,etanercept, or
infliximab)
1 year afterindex date
2 years afterindex date

CLINICAL
268 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
An algorithm was developed to translate qualitativedata into quantitative values. Because there were norelevant studies available to guide the development ofthe algorithm, a clinical and psychometric rationalewas applied to develop an algorithm that could beconsistently applied to the varying levels of physiciandocumentation.A visual analog scale (VAS; 0-10 cm) was the pre-
ferred method for evaluating all 3 joint assessments (ie,pain, swelling, stiffness) and fatigue. If documented VASwas not available, the following algorithm was used: A.Categorical documentation was converted to anumerical value using midpoints of a 0-to-10 scale(median [range]: mild = 1.65 [1-3.3], moderate = 4.95[3.4-6.6], severe = 8.25 [6.7-9.9])
B.Dichotomous documentation was converted to anumerical scale using the midpoints of a 1-to-10 scale(yes = 5, no = 0).If more than 1 form of documentation was present for
a patient visit, the VAS was the preferred type of docu-mentation, followed by categorical and dichotomousdocumentation.Baseline scores were determined through available
documentation on the index date or, if not available,documentation from the closest encounter before theindex dates. The mean scores for joint pain, swelling,and stiffness, and fatigue were determined for the 2-yearfollow-up period. If a patient had multiple assessments,an average was derived. The following criteria were used to define improve-
ment from baseline: A.Decrease in VAS of at least 1 pointB. Change in categorical documentation from “severe”to “moderate/mild” or from “moderate” to “mild”
C.Change in dichotomous documentation from yes to no. Improvement was defined as any improvement during
the 2-year follow-up period among any of the 3 docu-mentation types. Overall improvement was based onimprovement in any of the 4 effectiveness measures.Mean scores were based only on patients with docu-mented information for each joint assessment at thegiven time point (baseline or follow-up period).Basic descriptive statistics and univariate statistical
testing were applied to this analysis. Analysis of vari-ance or Kruskal-Wallis tests (as applicable) wereapplied to continuous variables to determine if differ-ences existed among the 3 cohorts. If differences didexist (ie, P <.05), post-hoc multiple comparison tests(Tukey or Mann-Whitney) that controlled for the fam-ily-wise type 1 error rate were conducted. For the mul-tiple comparison tests, P <.017 (Bonferroni correction)was considered statistically significant. Paired t-testswere conducted to determine if differences existed
among the VAS scores at baseline and during the 2-year follow-up period within each cohort. Chi-squaretests were conducted to assess differences between the3 cohorts on categorical variables. All analyses wereconducted using SAS version 9.1 (Cary, NC).
ResultsThis study enrolled 496 patients, including 84
patients (16.9%) in the adalimumab group, 146(29.4%) in the etanercept group, and 266 (53.6%) inthe infliximab group (Table 1). Overall, 74.0% of thepatients were female, and the mean age (standard devi-ation [SD]) was 56.1 (14.8) years. The mean age was52.6 years in the etanercept group and 57.6 years in theinfliximab group (P <.017). Of patients with documented ethnicity (n = 217),
whites comprised 80.2% of the overall population. Themean (SD) length of disease duration before initiationof anti-TNF therapy was 3.9 (3.5) years, and the mean(SD) length of follow-up after the index date was 614.8(156.0) days. Approximately 76% of patients receivedconcomitant DMARD therapy, which was more com-mon (79.7%) in the infliximab cohort than in theetanercept (68.5%) or adalimumab (75.0%) cohorts(P <.040). The average time that patients remained onanti-TNF therapy ranged from 367 days to 423 days(etanercept, 423 days; adalimumab, 371 days; inflix-imab, 367 days; P = .126).
Overall Clinical Improvement There was wide variation in the type of documenta-
tion used to indicate patient improvement (Table 2).For example, 99% of the patients had documentation forjoint pain, using a dichotomous approach (yes, painexists; no, pain does not exist), and 29% had VAS doc-umentation for this assessment. In total, 12.5% (n = 62) of all patients did not have
joint assessment data to evaluate clinical improvementduring the follow-up period. Of the 434 patients whohad documented information for at least 1 of the 4 effec-tiveness measures, 46.5% (n = 202) reported a clinicalbenefit, including 48.7% (n = 115/236) in the inflix-imab group, 47.7% (n = 62/130) in the etanercept group,and 36.8% (n = 25/68) in the adalimumab group.
Joint PainOverall, 150 of the 429 patients (35.0%) had an
improvement from baseline in joint pain scores duringthe 2-year follow-up (Table 3). The adalimumab andinfliximab groups reported significant improvementsfrom baseline in joint pain scores (P = .004 and P <.001,respectively). The infliximab group had the highest per-centage of patients with documented improvement in

Effectiveness of Anti-TNF Agents in Rheumatoid Arthritis
269www.AHDBonline.com l American Health & Drug BenefitsVol 3, No 4 l July/August 2010
joint pain (36.9%) compared with the etanercept group(36.4%) and the adalimumab group (25.3%), althoughthe difference was not significant.
Joint SwellingApproximately 35% (122 of 348) of patients had an
improvement from baseline in joint swelling scores.Among all patients, mean (SD) joint swelling scores sig-nificantly improved from baseline during the 2-year fol-low-up period (3.2 [1.9] vs 3.0 [1.8], P = .004). In theinfliximab group, the mean (SD) score decreased from3.2 (1.9) at baseline to 3.0 (1.8) during the follow-up
period (P <.001). There were no significant differencesbetween the mean scores at baseline and during the fol-low-up period in the adalimumab or the etanerceptgroups. The percentage of patients with improvement injoint swelling was highest in the infliximab group(38.0%), followed by the etanercept group (33.7%), andthe adalimumab group (26.8%); however, these differ-ences were not significant.
Joint StiffnessAmong all patients, 107 of 380 patients (28.2%) had
an improvement in joint stiffness score, and a significant
Table 2 Patients with Available Documentation of RA Improvement
Outcome
Any type of documentation
N (%)Dichotomous
N (%)Categorical N (%)
Comparison N (%)
VASaN (%)
Joints N (%)
Joint pain 492 (99) 492 (99) 214 (43) 379 (76) 145 (29) 194 (39)
Joint swelling 442 (89) 442 (89) 221 (45) 312 (63) 37 (7) 112 (23)
Joint stiffness 473 (95) 473 (95) 183 (37) 332 (67) 83 (17) 71 (14)
Fatigue 305 (61) 305 (61) 62 (12) 148 (30) 72 (14) —aVAS, 0-10 cm. RA indicates rheumatoid arthritis; VAS, visual analog scale.
Table 1 Patient Demographics, Baseline Characteristics, and DMARD Therapy
Adalimumab (N = 84, 16.9%)
Etanercept (N = 146, 29.4%)
Infliximab (N = 266, 53.6%)
Total (N = 496) P
Mean age, yrsa (SD) 57.1 (12.0) 52.6 (13.8) 57.6 (15.8) 56.1 (14.8) .003
Female, n (%) 65 (77.4) 108 (74.0) 194 (72.9) 367 (74.0) .720
Ethnicity,b n (%) .241
White 29 (70.7) 50 (79.4) 95 (84.1) 174 (80.2)
Black 3 (7.3) 1 (1.6) 2 (1.8) 6 (2.8)
Asian 0 (0.0) 2 (3.2) 3 (2.7) 5 (2.3)
Hispanic 9 (22.0) 10 (15.9) 13 (11.5) 32 (14.8)
Unknown 43 (51.2) 83 (56.9) 153 (57.5) 279 (56.3)
Mean disease duration, yrs (SD) 3.9 (2.8) 4.1 (4.0) 3.8 (3.4) 3.9 (3.5) .719
Mean length of follow-up, days (SD) 606.9 (151.0) 617.8 (153.7) 615.7 (159.3) 614.8 (156.0) .870
Concomitant DMARD therapy,c n (%) 63 (75.0) 100 (68.5)d 212 (79.7)d 375 (75.6) .040aCalculated from 2006.bPercentages computed based on total in each group, not including unknown.cDefined as overlap between anti-TNF therapy and DMARD therapy.dIndicates difference between etanercept and infliximab is significant. The difference in the mean age between these groups was also signifi-cant (P <.017).DMARD indicates disease-modifying antirheumatic drug; SD, standard deviation; TNF, tumor necrosis factor.

CLINICAL
270 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
Table 3 Improvement in Clinical Effectiveness Measures
Clinical measure Adalimumab Etanercept Infliximab Total PJoint pain BaselinePatients, na 68 132 233 433
Mean (SD) score 4.2 (2.5) 4.4 (2.2) 4.3 (2.2) 4.3 (2.2) .867
Follow-up periodPatients, na 67 129 233 429
Mean (SD) score 4.0 (2.4) 4.2 (2.3) 4.0 (2.1) 4.1 (2.2) .730
P (vs baseline) .004 .208 <.001 <.001
Patients with improvement, n (%) 17 (25.3) 47 (36.4) 86 (36.9) 150 (35.0) .200
Joint swellingBaselinePatients, na 57 98 205 360
Mean (SD) score 3.3 (1.7) 3.2 (1.9) 3.2 (1.9) 3.2 (1.9) .880
Follow-up periodPatients, na 56 92 200 348
Mean (SD) score 3.3 (1.8) 3.0 (1.9) 3.0 (1.8) 3.0 (1.8) .456
P (vs baseline) .795 .523 <.001 .004
Patients with improvement, n (%) 15 (26.8) 31 (33.7) 76 (38.0) 122 (35.1) .284
Joint stiffnessBaselinePatients, na 63 115 214 392
Mean (SD) score 3.8 (2.0) 3.8 (1.8) 3.8 (1.8) 3.8 (1.9) .986
Follow-up periodPatients, na 60 111 209 380
Mean (SD) score 3.6 (2.2) 3.9 (2.0) 3.6 (1.8) 3.7 (1.9) .351
P (vs baseline) .124 .520 .001 .022
Patients with improvement, n (%) 15 (25.0) 33 (29.7) 59 (28.2) 107 (28.2) .806
FatigueBaselinePatients, na 29 63 111 203
Mean (SD) score 5.0 (1.9) 5.1 (1.8)b 4.4 (2.0)b 4.7 (1.9) .031
Follow-up periodPatients, na 19 55 95 169
Mean (SD) score 4.8 (2.1) 5.2 (1.7)b 4.2 (2.0)b 4.6 (2.0) .009
P (vs baseline) .631 .153 .296 .290
Patients with improvement, n (%) 5 (26.3) 21 (38.2) 26 (27.4) 52 (30.8) .348
aValues in this row indicate the number of patients with data during period of assessment.bIndicates that the pairwise difference between etanercept and infliximab is significant (P <.017). NOTE: Scores in each of the outcomes measures (joint pain, swelling, and stiffness, and fatigue) ranged from 0 (no symptoms) to 10 (severe symptoms).SD indicates standard deviation.

Effectiveness of Anti-TNF Agents in Rheumatoid Arthritis
271www.AHDBonline.com l American Health & Drug BenefitsVol 3, No 4 l July/August 2010
decrease from baseline was observed in mean scores (P =.022). There were no significant differences between themean scores at baseline and during the follow-up periodwithin the adalimumab group and the etanercept group(Table 3). In the infliximab group, the mean (SD) scoredecreased significantly from 3.8 (1.8) at baseline to 3.6(1.8) during the follow-up period (P = .001).However, the etanercept group had the highest per-
centage of patients who had an improvement in jointstiffness score (29.7%), followed by the infliximab group(28.2%), and the adalimumab group (25.0%); however,these differences were not significant.
FatigueMean fatigue scores decreased from baseline for all
patients and within each therapy group; however, thesedecreases were not significant. The percentage ofpatients with improvement in fatigue was greatest in theetanercept cohort (38.2%), followed by the infliximabgroup (27.4%), and the adalimumab group (26.3%);however, these differences were not significant.When pairwise comparisons were conducted, the
mean (SD) fatigue score for the infliximab group wassignificantly lower (4.2 [2.0]) than in the etanercept(5.2 [1.7]) cohort during follow-up (P <.017). How -ever, the scores at baseline were also lowest in theinfliximab group.
DiscussionThe introduction of anti-TNF therapy is a valuable
addition to the armamentarium of RA treatmentoptions. The efficacy and safety of adalimumab, etaner-cept, and infliximab have been demonstrated in multi-ple randomized controlled trials with favorableresults.3-5,11-13Anti-TNF therapy can improve symptoms,increase physical function, and slow or prevent radio -graphic joint damage in many patients with RA.2,14Overall, the findings of this real-world analysis from 6
US rheumatology clinics support the benefit of anti-TNF therapy in patients with RA as reported in clinicaltrials.1,2,11 In general, the age and sex of the populationswere similar to those typically reported in RA clinicaltrials with anti-TNF agents. Disease duration beforeanti-TNF agent intervention was shorter (ie, about 4years) than that of patients who participated in previousclinical trials (ie, 9-11 years),1,2,11 which may be the resultof recent evidence supporting earlier interventions ormay reflect referral patterns within the participatingrheumatology clinics. Many patients in this analysis were treated with an
anti-TNF therapy and concomitant DMARD therapy(75.6%). The data indicate that concomitant DMARDuse was more common with infliximab treatment than
with the other anti-TNF agents. This combination ther-apy is supported by clinical trials showing that anti-TNFtherapy concomitant with methotrexate has improvedbenefit over methotrexate monotherapy.2,4,13
Nearly half of the patients included in this studyreported an improvement in joint pain, joint swelling,joint stiffness, or fatigue during the 2-year follow-up peri-od. The infliximab group was the only cohort to demon-strate significant improvements from baseline in 3 (jointpain, joint swelling, and joint stiffness) of the 4 clinicaleffectiveness measures. None of the cohorts demonstrat-ed a significant change from baseline in the fatigue score,although numerical improvements were noted.There is no standardized measure to assess outcomes
in routine clinical practice; therefore, physicians typical-ly utilize several measures, including laboratory tests,radiographic scores, joint counts, measures of functionalstatus, global measures, and patient self-reported ques-tionnaires.15-17 Indeed, wide variability has been demon-strated regarding the frequency with which different out-come measures are documented by providers.17The present analysis assessed variable outcome meas-
ures with the development of an algorithm to integrateintra- and intervariability among providers reportingclinical status in patients with RA. A number of toolsare currently available (eg, Simplified Disease ActivityIndex; Clinical Disease Activity Index; Disease ActivityScore, including 28 joints).18,19 However, further explo-ration of a validated practical tool that could be adoptedfor widespread use to monitor RA treatment response iswarranted, followed by exploration of the incentivesneeded to improve such data collection. An advantage of this study is that it provides real-
world outcomes associated with anti-TNF therapy fordrugs that have already demonstrated efficacy and safetyin controlled clinical trials. The 2-year follow-up periodallowed for the assessment of long-term outcomes.However, because this analysis was designed to evaluateanti-TNF agents, other biologic therapies used for RA—including anakinra (Kineret),20 abatacept (Orencia),21and rituximab (Rituxan)22—were not assessed. Randomized clinical trials and observational studies
in routine clinical practice are important for the evalua-tion of therapies and have unique advantages and limi-tations. Although not as scientifically rigorous, real-
There is no standardized measure to assessoutcomes in routine clinical practice;therefore, physicians typically utilizeseveral measures.

CLINICAL
272 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
world studies can complement the information gainedfrom clinical trials. Specifically, one observationalcohort study of the effectiveness of anti-TNF therapy inpatients who would have been ineligible for a clinicaltrial demonstrated that the majority of such patientswould benefit from these treatments.23 Well-designedobservational studies can be invaluable in gaining fur-ther understanding of response to therapy.
LimitationsConsistent with observational research, the limita-
tions of this study include missing data and inconsisten-cies with documentation. Lack of standardized outcomemeasures in clinical practice was confirmed by the resultsand limited the quantitative and qualitative nature ofthis study, thereby requiring the development of an algo-rithm to capture variability in assessment of clinical out-comes among providers. As such, this approach has notbeen validated. Although the study was designed toevaluate patients who were newly initiated with anti-TNF therapy, it is possible that patients might havereceived anti-TNF treatments before the pre-indexassessment period.
Notable limitations of the study are inherent in thenature of observational studies. There exists the possibil-ity of confounding by indication associated with lack ofrandomization, because other unmeasured factors mighthave influenced the selection of one anti-TNF agentover another, and variable reasons for changes in thera-py may influence the outcomes. Also, the retrospectivenature of the analysis prevented the collection ofpatient-reported outcomes. In addition, quantificationof tender or swollen joints and radiographs to assess jointdamage were not available. These factors may have also contributed to the lack of
significant improvements among patients who receivedetanercept in this analysis. Although these patients didnot show significant improvements in the clinicalresponse measures used in this study, etanercept has beenshown to be effective for treating RA in randomized,placebo-controlled clinical trials.4,6 This discrepancy mayalso be a result of the different methods used in measur-ing treatment response.
ConclusionData from this analysis demonstrate the 2-year clin-
ical effectiveness of anti-TNF therapy in patients with
RA. This real-world study shows improvements in jointpain, joint swelling, joint stiffness, and fatigue. Overallclinical improvement was reported in 36.8% of theadalimumab group, 47.7% of the etanercept group, and48.7% of the infliximab group over the 2-year follow-up period. These results are beneficial in that they pro-vide confirmation that benefits seen in clinical trialsare being translated into actual practice. Future obser-vational research, with more uniform patient andprovider assessments during the course of anti-TNFtherapy, is warranted. ■
AcknowledgmentsThe authors thank Rebecca E. Clemente, PhD, and
Robert Achenbach of Centocor Ortho Biotech, Inc, foreditorial support.
Disclosure StatementThis study was supported by funding from Centocor
Ortho Biotech, Inc.
References1. Weinblatt ME, Keystone EC, Furst DE, et al. Adalimumab, a fully human anti-tumor necrosis factor alpha monoclonal antibody, for the treatment of rheumatoidarthritis in patients taking concomitant methotrexate: the ARMADA trial. ArthritisRheum. 2003;48:35-45.2. Lipsky PE, van der Heijde DM, St. Clair EW, et al, for the Anti-Tumor NecrosisFactor Trial in Rheumatoid Arthritis with Concomitant Therapy Study Group.Infliximab and methotrexate in the treatment of rheumatoid arthritis. N Engl J Med.2000;343:1594-1602.3. Keystone EC, Kavanaugh AF, Sharp JT, et al. Radiographic, clinical, and func-tional outcomes of treatment with adalimumab (a human anti-tumor necrosis factormonoclonal antibody) in patients with active rheumatoid arthritis receiving con-comitant methotrexate therapy: a randomized, placebo-controlled, 52-week trial.Arthritis Rheum. 2004;50:1400-1411.4. van der Heijde D, Klareskog L, Rodriquez-Valverde V, et al. Comparison of etan-ercept and methotrexate, alone and combined, in the treatment of rheumatoidarthritis: two-year clinical and radiographic results from the TEMPO study, a double-blind, randomized trial. Arthritis Rheum. 2006;54:1063-1074. 5.Maini RN, Breedveld FC, Kalden JR, et al. Sustained improvement over two yearsin physical function, structural damage, and signs and symptoms among patients withrheumatoid arthritis treated with infliximab and methotrexate. Arthritis Rheum.2004;50:1051-1065.6. Bathon JM, Martin RW, Fleischmann RM, et al. A comparison of etanercept andmethotrexate in patients with early rheumatoid arthritis. N Engl J Med. 2000;343:1586-1593.7.Wolfe F, Michaud K, DeWitt EM. Why results of clinical trials and observationalstudies of anti-tumour necrosis factor (anti-TNF) therapy differ: methodological andinterpretive issues. Ann Rheum Dis. 2004;63(suppl 2):ii13-ii17. 8. Pincus T, Sokka T. Should contemporary rheumatoid arthritis clinical trials be morelike standard patient care and vice versa? Ann Rheum Dis. 2004;63(suppl 2):ii32-ii39. 9. Hawley DJ, Wolfe F. Are the results of controlled clinical trials and observationalstudies of second line therapy in rheumatoid arthritis valid and generalizable as meas-ures of rheumatoid arthritis outcome: analysis of 122 studies. J Rheumatol. 1991;18:1008-1014. 10. Garrison LP Jr, Neumann PJ, Marshall D, Mullins CD. Using real-world data forcoverage and payment decisions: the ISPOR real-world data task force report. ValueHealth. 2007;10:326-335.11. Maini R, St Clair EW, Breedveld F, et al, for the ATTRACT Study Group.Infliximab (chimeric anti-tumour necrosis factor alpha monoclonal antibody) versusplacebo in rheumatoid arthritis patients receiving concomitant methotrexate: a ran-domised phase III trial. ATTRACT study group. Lancet. 1999;354:1932-1939.12.Moreland LW, Schiff MH, Baumgartner SW, et al. Etanercept therapy in rheuma-toid arthritis. A randomized, controlled trial. Ann Intern Med. 1999;130:478-486.13. Breedveld FC, Weisman MH, Kavanaugh AF, et al, for the PREMIERInvestigators. A multicenter, randomized, double-blind clinical trial of combinationtherapy with adalimumab plus methotrexate versus methotrexate alone or adali-
Well-designed observational studies can beinvaluable in gaining further understandingof response to therapy.

Effectiveness of Anti-TNF Agents in Rheumatoid Arthritis
273www.AHDBonline.com l American Health & Drug BenefitsVol 3, No 4 l July/August 2010
mumab alone in patients with early, aggressive rheumatoid arthritis who had not hadprevious methotrexate treatment. Arthritis Rheum. 2006;54:26-37. 14. Taylor PC. Anti-TNF alpha therapy for rheumatoid arthritis: an update. InternMed. 2003;42:15-20.15. American College of Rheumatology Subcommittee on Rheumatoid ArthritisGuidelines. Guidelines for the management of rheumatoid arthritis: 2002 update.Arthritis Rheum. 2002;46:328-346.16. Pincus T, Sokka T. Quantitative measures for assessing rheumatoid arthritis inclinical trials and clinical care. Best Pract Res Clin Rheumatol. 2003;17:753-781. 17. Furst DE, Halbert RJ, Bingham CO, et al. Evaluating the adequacy of diseasecontrol in patients with rheumatoid arthritis: a RAND appropriateness panel.Rheumatology (Oxford). 2008;47:194-199. Epub 2008 Jan 4.18. Leeb BF, Andel I, Sautner J, et al. Disease activity measurement of rheumatoidarthritis: comparison of the simplified disease activity index (SDAI) and the dis-
ease activity score including 28 joints (DAS28) in daily routine. Arthritis Rheum.2005;53:56-60.19.Aletaha D, Smolen J. The simplified disease activity index (SDAI) and the clin-ical disease activity index (CDAI): a review of their usefulness and validity inrheumatoid arthritis. Clin Exp Rheumatol. 2005;23(5 suppl 39):S100-S108.20.Kineret (anakinra). Prescribing information. Thousand Oaks, CA: Amgen Inc; 2001.21. Orencia (abatacept). Prescribing information. Princeton, NJ: Bristol-MyersSquibb; 2008.22. Rituxan (rituximab). South San Francisco, CA: Biogen, Idec Inc, andGenentech, Inc; 2008.23. Zink A, Strangfeld A, Schneider M, et al. Effectiveness of tumor necrosis factorinhibitors in rheumatoid arthritis in an observational cohort study: comparison ofpatients according to their eligibility for major randomized clinical trials. ArthritisRheum. 2006;54:3399-3407.
Effectiveness of Anti-TNFs in Patients with RA, and Coverage Considerations
PAYERS: Over the past several years, rheumatoidarthritis (RA) has become a difficult condition tomanage from a managed care standpoint. Drugs for thetreatment of RA are among the few medication class-es to keep a double-digit trend year after year and havebecome some of the largest cost contributors on a per-centage of per-member per-month basis.Anti-tumor necrosis factor (TNF) agents discussed
in this article were the first medications for RA thatbroke $20,000 for 1 year of treatment. Recently, sever-al anti-TNF biologics have been introduced to themarket that have different modes of action but similarefficacy and similar cost. For these reasons, RA drugshave become a prominent concern for payers, includ-ing health insurance companies and employer groups.However, very little comparative data are available forthese agents. Until such data become available, cover-age decisions will need to be based solely on placebo-controlled trials, postmarketing claims-based or chart-based retrospective analysis, and cost.In 2008, the American College of Rheumatology
(ACR) released its recommendations for the use ofboth nonbiologic disease-modifying antirheumaticdrugs (DMARDs) and biologics.1 The recommenda-tions emphasize the importance of starting therapywith traditional DMARDs, which may be much morecost-effective than starting immediately with a biolog-ic. Another ACR recommendation is using a con-comitant DMARD when a biologic is needed. Themajority of clinical trials show a better response withbiologics when used in combination with a DMARDsuch as methotrexate. However, several retrospective claims analyses
have shown the combination use rate to be lower
than might be expected (based on efficacy resultsfrom pivotal clinical trials). Another challenge hasbeen the need to encourage providers to prescribecombination therapy in support of available evi-dence-based recommendations. Drug manufacturers will likely hesitate to conduct
comparative trials for their products. This meansmore reliance on retrospective analysis or “real-world” data to determine if enough data are availableto recommend coverage of one biologic over anotherfor first-line treatment, after failure of a different bio-logic, as well as the extent or length of coverage forthese products.
PATIENTS: The past decade has given patientswith RA several novel biologic options for the treat-ment of this painful, progressing condition. The varietyof options also gives patients the opportunity to receivetherapy at their provider’s office on a regular basis, orthe option to receive a self-injectable therapy fromtheir pharmacy or specialty pharmacy. Besides the difficult decision of determining the
most appropriate therapy based on efficacy and safe-ty, is the necessity of cost-sharing. Patients need to beinsurance-savvy to realize not only which productsmay be covered but also the type and amount of cost-sharing that is required. Medical versus pharmacybenefit differences may also create challenges tounderstanding optimal coverage opportunities.1. Saag KG, Teng GG, Patkar NM, et al. American College of Rheumatology2008 recommendations for the use of nonbiologic and biologic disease-modifyingantirheumatic drugs in rheumatoid arthritis. Arthritis Rheum. 2008;59:762-784.
Matthew Mitchell, PharmD, MBAManager, Pharmacy Services
SelectHealth, Salt Lake City, UT
STAKEHOLDER PERSPECTIVE

GENERIC DRUG TRENDS
274 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
Areport prepared by IMS Health for the GenericPharmaceutical Association (GPhA) andreleased in July 2010 shows that the utilization
of generics substituted for brand-name products hasbeen making great leaps since 2006.1 The report spansthe decade from 2000 through 2009, comparing therate of generic utilization in each of the past 10 years,and highlighting the exponential rate increase in thepast 4 years (Table 1).1
This uptake in utilization has resulted in savings of$139.6 billion in 2009 alone, representing a 15%growth from the previous year. Not only does this meana significant cost-reduction to the US healthcare sys-tem, it also represents a substantial share—inchingtoward 50%—of the net US sales of all prescriptiondrugs, which amounted to $300.3 billion in 2009,according to IMS.2
Some of the key findings of the new report are1: • In the past decade, generic drugs have saved the US
healthcare system $824 billion • Much of the increase in cost-savings in the past 3 years
has been driven by new generic versions of blockbusterdrugs, such as Norvasc, Zocor, and Zoloft
• Substantial savings from generics are expected to con-tinue in the next 5 years, when $89 billion in brand-name drug sales will lose their patent protection
• Every 2% increase in Medicaid generic drug utilization
translates to an additional $1-billion savings annually,but generics utilization by Medicaid beneficiaries is10% lower than among non-Medicaid plan members
• Utilization of generic central nervous system (CNS)drugs topped the list from 2008 ($41 billion) to 2009($49 billion), a 20% savings
• The 3 therapeutic categories with the highest savingsfrom generics in 2009 were CNS conditions, cardio-vascular diseases, and metabolic disorders, totalingalmost three fourths of the savings.
This growth trend can be expected to continue atleast through 2014, as sales of top-selling brand-nameagents will be losing their patent protection (Table 2),including 5 of the 10 best-selling pharmaceuticals—Lipitor, Plavix, Aricept, Singulair, and Zyprexa.1
Thus makers of generic drugs have their work cut outfor the next 5 years, and payers can begin to design newstrategies to capitalize on this enhanced cost-savingstrategy. And those in charge of Medicaid state planshave room to implement new strategies to garner signif-icant savings from improved generic utilization. �
References1. Generic Pharmaceutical Association. Savings achieved through the use of gener-ic pharmaceuticals 2000-2009. July 2010. http://gphaonline.org/sites/default/files/GPhA%20Savings%20Study%20Book%20Updated%20Web%20FINAL%20Jul23%2010_0.pdf. Accessed August 2, 2010.2. IMS Health. IMS Health reports US prescription sales grew 5.1 percent in 2009,to $300.3 billion. April 1, 2010. www.imshealth.com/portal/site/imshealth/menuitem.a46c6d4df3db4b3d88f611019418c22a/?vgnextoid=d690a27e9d5b7210VgnVCM100000ed152ca2RCRD&vgnextchannel=41a67900b55a5110VgnVCM10000071812ca2RCRD&vgnextfmt=default. Accessed August 2, 2010.
Enhanced Generic Utilization Saved USHealthcare $139.6 Billion in 2009By Dalia Buffery, MA, ABD
140
120
100
80
60
40
20
0
Used with permission from GPhA. Savings achieved through theuse of generic pharmaceuticals 2000-2009. July 2010. Copyright © 2010 GPhA.
Table 1 Generic Drug Savings in 2000-2009 (in $ billions)
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
$51
$139
$121
$101
$55$60 $65 $69
$78$86
Sales, $
2010 2011 2012 2013 2014
40
35
3025
20 15
10
50
$13
$20
$5
$18
$32
Used with permission from GPhA. Savings achieved through theuse of generic pharmaceuticals 2000-2009. July 2010. Copyright © 2010 GPhA.
Table 2 Expected Brand-Name Sales to Expire by 2014(in $ billions)
Sales, $

©2010 Mylan Pharmaceuticals Inc. MYNMKT393A
We Live And Breathe Generics.
800.RX.MYLAN • www.mylanpharms.com
Throughout every department in every facility within our domesticand global network, there is a singular commitment to genericsthat guides and drives every individual at Mylan. That commitmentembodies everything we do and ensures that patients will have theaffordable medicine that they need.
It’s why our research and development team is constantly searching for innovative technologies; why our manufacturingteam is always looking for more efficient ways to produce and distribute the generics in our ever-expanding line; and why ourquality assurance team is continually monitoring our products to be sure they meet our standards.
Our singular commitment has continued to earn us the trust ofpharmacists who rank our products highest in quality* … and it’swhy the Mylan name is synonymous with quality generics.
*U.S. Pharmacist Generic Company Surveys. 2006-2009
Page 1

BUSINESS
276 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
Dr Force is Professor and Director of Research, Family Medicine and Pharmacy Practice, Idaho StateUniversity, and Partner, improveRX, LLC; Dr Pugmire is Clinical Assistant Professor, PharmacyPractice, Idaho State University, and Clinical Project Manager, improveRX; Dr Culbertson isProfessor, Pharmacy Practice, Idaho State University, and Partner, improveRX; all at Pocatello, ID.
Comparing Medical Cost of Care for Patientswith Metastatic Breast Cancer ReceivingTaxane Therapy: Claims Analysis Rex W. Force, PharmD; Brooke A. Pugmire, PharmD; Vaughn L. Culbertson, PharmD
Background: It has been estimated that more than $8 billion is spent annually on the man-agement of breast cancer in the United States. The taxane chemotherapeutic agents are cor-nerstones in the treatment of breast cancer, yet no study has assessed whether the choiceof a taxane affects the economic outcomes of metastatic breast cancer treatment.Objective: To determine if differences exist in the medical cost of care in patients receivingtaxane-based chemotherapy for metastatic breast cancer, and to compare the use of ancil-lary medications (for neutropenia, anemia, and nausea and vomiting) and their associatedcosts among taxanes.Method: We identified women with metastatic breast cancer based on diagnosis codes andthe women’s previous adjuvant chemotherapeutic regimens. Paid medical insurance claimswere captured for the 24-month study period, from January 1, 2006, through December 31,2007. The groups were determined according to the specific taxane administered. Total med-ical costs were captured from the date of first taxane administration to the end of data avail-ability. Outpatient pharmacy costs were not available. A multivariate analysis was used toevaluate the total medical costs in each group. Median total medical costs per patient permonth during the study period were adjusted using a multiple regression analysis. Utilizationand cost of medications administered in the office or hospital for chemotherapy-inducedadverse effects were captured and adjusted with Tobit models.Results: Of the 2245 study participants, 1035 received docetaxel, 997 received genericpaclitaxel, and 213 received nab-paclitaxel. On average, patients in the nab-paclitaxel groupreceived more doses (9.6) than those in the generic paclitaxel (6.0) or docetaxel (4.8) groups.The multivariate analysis was robust, explaining 72% of the variability in total medical costsacross the 3 taxane groups. Median per-patient per-month total medical costs for study par-ticipants were within approximately $800 of each other among the groups. Generic paclitax-el had the lowest total medical costs. The total costs for docetaxel and nab-paclitaxel werenot significantly different. Nab-paclitaxel had the lowest utilization and lowest costs associat-ed with colony-stimulating factors. The proportion of patients receiving erythropoiesis-stimu-lating agents was not significantly different among the 3 drugs, but the costs for these agentswere significantly lower in patients receiving nab-paclitaxel than in those receiving docetaxel.Antiemetic use was highest in the docetaxel group, but the costs for antiemetics were not dif-ferent among the 3 taxane groups.Conclusion: The differences in total medical costs among the 3 taxanes were modest. Totalmedical costs were lowest for patients receiving generic paclitaxel and comparable betweenthe docetaxel and nab-paclitaxel groups. Patients taking nab-paclitaxel received more dosesthan patients taking the other taxanes. Nab-paclitaxel was associated with lower utilizationand costs for colony-stimulating factors compared with generic paclitaxel and docetaxel.
Am Health Drug Benefits.2010;3(4):276-284.www.AHDBonline.comDisclosures are at end of text
Rex W. Force
Stakeholder Perspective, page 284

Comparing Medical Cost of Care for MBC
277www.AHDBonline.com l American Health & Drug BenefitsVol 3, No 4 l July/August 2010
Breast cancer is the most frequently diagnosed can-cer in US women, and ranks second among can-cer-related deaths in women, after lung cancer.1 It
is estimated that $8.1 billion (in 2004 $US) in totalhealthcare costs are spent annually on breast cancerdiagnosis and treatment in the United States.2Chemotherapeutic agents represent a significant portionof the cost of breast cancer treatment, and health plansare managing these costs with care pathways and otherutilization management strategies.
The Taxanes Taxanes are among the most frequently used forms of
systemic therapy for the treatment of breast cancer.3These chemotherapeutic agents can be prescribed aloneor in combination with other systemic therapies or withlocal treatment, such as surgery and/or radiation.Taxanes are mitotic inhibitors originally isolated fromthe bark of the Pacific yew tree, Taxus brevifolia. Threetaxanes are currently available in the United States,although this is an area of active drug development.
The first of these agents to be marketed in the UnitedStates, paclitaxel injection (Taxol), was approved by theUS Food and Drug Administration (FDA) in 1992 as aninjectable formulation dissolved in a proprietary versionof polyethoxylated castor oil called Cremophor EL andethanol as a delivery agent.4 The second agent—doce -taxel (Taxotere)—received FDA approval in 1996;docetaxel is a semisynthetic taxane dissolved in polysor-bate 80 and 13% ethanol and water for injection.5
The toxicity of these 2 solvent-based taxanes includesbone marrow suppression (principally neutropenia),alopecia, and hypersensitivity reactions.6
Irizarry and colleagues reviewed 171 reported cases ofanaphylaxis associated with the Cremophor EL–basedpaclitaxel. A total of 34% were fatal reactions, althoughthe authors suggested that this adverse event (AE) isunderreported.7 Although neurotoxicity and myalgias/arthralgias have been cited as potential AEs with pacli-taxel and docetaxel, these events are of greater clinicalconcern with paclitaxel—again, likely because of theCremophor EL solvent.6 However, docetaxel has beenassociated with the development of significant fluidretention (eg, edema, ascites, pleural effusions), the inci-dence and severity of which appear to be reduced by pre-medication with corticosteroids.6 These toxicities mayresult in dose reductions, delays in continuation of treat-ment, or even discontinuation of chemotherapy.
In an attempt to reduce the significant toxicity asso-ciated with the solvent-based taxanes, a new formula-tion of paclitaxel was developed—nab-paclitaxel(Abraxane)—in which the active drug is bound to albu-min.8 Nab-paclitaxel received FDA approval in 2005.
This albumin-bound paclitaxel has demonstrated superi-or efficacy over the solvent-based paclitaxel in the treat-ment of metastatic breast cancer (MBC), as well as amore favorable AE profile.9,10
Although the solvent-based taxanes—paclitaxel anddocetaxel—have lower drug acquisition costs than nab-paclitaxel, nab-paclitaxel offers potential clinical advan-tages, such as better tumor responses with lower rates ofsevere neutropenia and infusion-related reactions.9,10
Systematic reviews have indicated that taxanes areamong the most active regimens in MBC.11 However,differences in the toxicity and efficacy of the taxanesexist. Gradishar and colleagues found that nab-paclitax-el was associated with better response rates comparedwith the solvent-based generic paclitaxel in MBC (33%vs 19%, respectively; P = .001), with a longer time totumor progression (23.0 weeks vs 16.9 weeks, respective-ly; P = .006).10 In addition, the rates of severe neutrope-nia were significantly lower in the nab-paclitaxel group(9% vs 22%, respectively; P <.001).10
Similarly, in another study, nab-paclitaxel was associ-ated with a significantly longer progression-free survival(12.9 months vs 7.5 months, respectively; P = .0065)compared with docetaxel in women with MBC.12
KEY POINTS
➤ Medication costs for oncology continue to increasedramatically. The treatment of metastatic breastcancer consists of several treatment modalities,including a taxane.
➤ Taxane use in metastatic breast cancer should beevaluated with cost of care analyses to account fordifferences in ancillary medication use, costs ofcomplications, and other chemotherapeuticstrategies. These factors contribute to total medicalcost, which may be used as the primary outcomemeasure in a pharmacoeconomic evaluation ratherthan simply drug acquisition cost alone.
➤ This is the first study to evaluate the total cost of care for metastatic breast cancer from theperspective of taxane choice among the 3 availabletaxanes—generic paclitaxel, docetaxel, and nab-paclitaxel.
➤ Per-patient per-month medical costs for womenreceiving 1 of the 3 taxanes were within $800 ofeach other. As can be expected, generic paclitaxelwas the least expensive.
➤ The overall costs of breast cancer management arerelated to the entire chemotherapeutic regimen,potential side effects, and costs of hospitalization. Inthis study, women receiving nab-paclitaxel had thelowest expenditures for colony-stimulating factors.

BUSINESS
278 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
Grade-3 or -4 neutropenia occurred in 94% of thepatients receiving docetaxel and in 38% of patientsreceiving nab-paclitaxel.12
To evaluate the economic implications of these dif-ferences in efficacy and toxicity, Dranitsaris and col-leagues performed a pharmacoeconomic analysis of nab-paclitaxel in MBC.13 Nab-paclitaxel was less expensivethan docetaxel per quality-adjusted life-year in the cost-utility model, but more expensive than generic paclitax-el.13 The disadvantages of this type of analysis include avariety of model assumptions that render the real-worldimplications of the results difficult to interpret by phar-macy and medical directors at health plans.
In 2008, Barron and colleagues evaluated all-causecosts in women treated for breast cancer using claimsfrom 5 US health plans.14 The authors reported meanunadjusted per-patient per-month (PPPM) all-causecosts of $4421 in women receiving treatment for breastcancer compared with PPPM costs of $3352 for age-matched controls without breast cancer.14 The top 3 costcategories included hospitalizations, drug therapy, andsurgical intervention.14 The components of total cost areof interest to payers, because they manage increasingcosts associated with breast cancer treatment. PPPMcost calculations provide plan managers with an esti-mate of the cost of treating patients with a specific con-dition. These costs are quite different and generallymuch higher than typical actuarial estimates of per-member per-month dollar amounts.
The benefits and costs with any new treatment optionneed to be fully evaluated. At a December 2009 ICOREHealthcare Managed Care Advisory Board meeting inBethesda, MD, payers questioned the value of nab-pacli-taxel because of its higher acquisition cost. However, acomparison between nab-paclitaxel and solvent-basedtaxanes should include the costs associated with toxicity,drug utilization, and ancillary medication use rather thandrug acquisition costs alone. These factors contribute tototal medical cost, which may be used as the primaryoutcome measure in a pharmacoeconomic evaluation.
To clarify these issues surrounding the use of the tax-anes, we performed a pragmatic, retrospective evaluationof paid medical claims, with the intent of determiningthe impact of taxane choice on total medical costs in thetreatment of MBC.
MethodsThis study was a cost comparison using paid medical
claims from all locations of service from national com-mercial payer sources. Medical claims include all officevisits, hospital charges, procedures (eg, laboratory tests,x-rays), and medications administered in the physicianoffice, infusion center, or hospital. Total medical costs
were derived from these data elements. Outpatient phar-macy claims and costs were not available and thereforewere not included.
Data were handled in compliance with the HealthInsurance Portability and Accountability Act of 1996.Because the data analysis did not involve any patientintervention and used a limited data set with blindedpatient identification, a certificate of exemption wasobtained from our Institutional Review Board. Thesponsor had no role in the study design, analysis, or writ-ing of the paper. Investigators had exclusive access to thedata and independently developed the research designand wrote the manuscript.
Study Population and Case DefinitionsThe data set was derived from a total of 95,530,675
procedure claims from 6,130,088 unique patients(Ingenix Consulting, Eden Prairie, MN). Claims datawere analyzed for 24 months, from January 1, 2006, toDecember 31, 2007. Only allowed charges from patientscoded with a diagnosis of breast cancer were included inthe final analysis. Patients receiving taxane therapy wereidentified using stepwise computerized algorithms todefine a subset of taxane use in MBC (Figure 1).
Initially, all patients with breast cancer with anInternational Classification of Diseases, Ninth Revision,Clinical Modification (ICD-9-CM) diagnosis code of174.X were identified. Patients with a single taxaneadministration were then removed from the analysis.Next, patients who may have developed breast cancer asa secondary site were excluded (1) if any other cancerdiagnosis (ICD-9-CM codes 140.XX-173.XX; 175.XX-195.XX; and 200.XX-208.XX) occurred in the 6 monthspreceding the initial breast cancer diagnosis, or (2) ifthey received any chemotherapy other than office- orhospital-administered adriamycin-cyclophosphamide inthe 6 months before their first breast cancer diagnosis.
Taxane use within this subgroup was subject to thefollowing criteria to define taxane use in MBC: • Taxane administration occurring more than 30 daysafter an established doxorubicin-cyclophosphamide-taxane adjuvant regimen
• Concurrent (±3 days) taxane administration witheither doxorubicin or cyclophosphamide in whichdoxorubicin-cyclophosphamide use did not conformto established adjuvant treatment regimens
• Taxane administration occurring after a secondary(metastatic) cancer diagnosis (ICD-9-CM codes140.XX-173.XX and 175.XX-199.XX)
• Taxane use not described by these rules was eliminatedfrom further analysis, because this subgroup of patientstended to have incomplete data and therefore an accu-rate assessment of chemotherapy use could not be done.

Comparing Medical Cost of Care for MBC
279www.AHDBonline.com l American Health & Drug BenefitsVol 3, No 4 l July/August 2010
Drug use was identified by the following J codes:• J9170 indicating docetaxel 20 mg• J9265 indicating generic paclitaxel 30 mg• J9264 indicating nab-paclitaxel 1 mg.
For analytical purposes, the index date was defined asthe date of a patient’s first dose of taxane; from this pointonward, total paid charges were captured. Patients wereplaced in generic paclitaxel, docetaxel, and nab-paclitax-el groups according to their first taxane use. Patients werenot required to be continuously enrolled over the study
period, because multiple regression analysis was used toadjust for individual patient enrollment period variabili-ty (eg, total months with a claim was a control variable).
Analytical Outcomes and Cost AnalysisMean age was determined for each of the 3 groups
based on the patients’ date of birth and date of first tax-ane use (index date). The number of taxane dosesreceived was determined. In addition, the mean dosinginterval for each taxane was calculated; however, inter-
Breast cancera in 2006-2007with ≥1 taxaneb dose
(n = 6986)
Breast cancer with ≥2 taxane doses (n = 5286)
Exclude patients with only 1 taxane dose (n = 1700)
Breast cancer only (n = 2669)
Second cancer sitec afterbreast cancer diagnosis
(n = 1676)
Exclude other primary canceroccurring before breast or second cancerc (n = 941)
Excluded taxane adjuvant or other regimens
(n = 2100)
Final metastatic group (n = 2245)
➤
➤➤
➤
➤ ➤
➤
➤
Metastatic taxane useTaxane administration occurring:• After a new cancer diagnosis (n = 1152)• Where no established A-C adjuvant regimen could be identified after
breast cancer diagnosis (n = 618)• After a breast cancer diagnosis where A-C were not administered on
the same day (n = 475).
aICD-9-CM diagnosis codes 174.0 to 174.9.bTaxanes include J codes J9170, J9264, and J9265.cSecondary cancer, defined as any other primary cancer (ICD-9-CM codes 140.XX-195.XX or ICD-9-CM codes 196.XX-199.XX).A-C indicates adriamycin-cyclophosphamide; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification.
Figure 1 Study Flow Diagram
➤

BUSINESS
280 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
vals longer than 60 days were excluded from the inter-val calculations. Duration of months in the databasewas measured from the date of first taxane administra-tion (index date) to the time of last claim, because ofdisenrollment, end of the data period, or death.
Chemotherapy and biologic agent utilization—specifically bevacizumab (Avastin), trastuzumab(Herceptin), gemcitabine (Gemzar), and vinorelbine(Navelbine)—was determined before, concurrent with,and post-taxane utilization; each was included as a con-trol variable in the multivariate analysis (SAS, SASInstitute, Inc, Cary, NC). The total medical cost statis-tical model also adjusted for age; number of procedures(ie, office visits, hospitalizations, laboratory tests) afterindex date; number of unique diagnoses after indexdate; number of months with claims in the data setafter index date; number of taxane doses; and the pres-ence of a taxane claim in the first month. Proceduresand diagnoses were included in the multivariate analy-sis and served as surrogates for severity of illness.Medical costs are reported in actual US dollars, from2006 and 2007, without discounting.
While adjusting for these variables, total medicalcost comparisons were calculated, as well as PPPMtotal medical costs for managing patients with MBCfor the 3 taxane groups. All medical costs were cap-tured from the index date through the end of the datacollection period, while controlling for the durationof available data and duration of enrollment for eachpatient.
Utilization of ancillary medications was defined as aclaim for colony-stimulating factors (CSFs) or erythro-poiesis-stimulating agents (ESAs) between days 0 and+21, or antiemetics between days 0 and +5 after eachtaxane administration. Cost comparisons of CSFs orESAs between days 0 and +21 after taxane administra-tion, or antiemetics between days 0 and +5 after taxaneadministration, were made using Tobit models.
Tobit models are utilized when the entire study popu-lation does not undergo the same interventions. Forexample, not all patients received CSFs; Tobit modelscan control for unbalanced utilization and allow for an
appropriately adjusted evaluation of cost. For the pur-poses of this analysis, all the variables included in themultivariate analysis were also included in the Tobitanalyses. Throughout the study, all comparisons wereconsidered significantly different at P <.05.
ResultsTaxane Utilization
A total of 2245 women with a mean (± standard devi-ation [SD]) age of 53 years (± 10 years) receiving a tax-ane for MBC were included in the study. The docetaxelgroup included 1035 patients, the generic paclitaxelgroup included 997 patients, and the nab-paclitaxelgroup included 213 patients. Mean (± SD) residence inthe database was longer for patients receiving nab-pacli-taxel (16.5 ± 6.6 months) compared with docetaxel(12.6 ± 6.3 months) and generic paclitaxel (13.5 ± 6.4months). Nab-paclitaxel had a significantly higher meannumber of doses per patient (9.4; 95% confidence inter-val [CI], 8.5-10.2), followed by generic paclitaxel (7.0;95% CI, 6.6-7.3) and docetaxel (5.9; 95% CI, 5.5-6.3),which was adjusted for residence in the database by pair-wise comparisons using the Bonferroni method. Themean (± SD) dosing intervals for patients receivingdocetaxel, generic paclitaxel, and nab-paclitaxel were20.5 ± 6.2 days, 16.2 ± 8.8 days, and 15.8 ± 8.9 days,respectively (Table 1).
Other Chemotherapy UtilizationA higher proportion of patients received chemother-
apy before the initiation of nab-paclitaxel than beforeinitiating either generic paclitaxel or docetaxel (P <.05for both); a greater proportion of patients taking genericpaclitaxel than patients taking docetaxel (P <.05)received previous chemotherapy (Table 2). The rate ofconcurrent chemotherapy use was greater in patientstaking docetaxel compared with those taking genericpaclitaxel or nab-paclitaxel (P <.05 for both); the use forthe latter 2 drugs was not significantly different. Post-taxane chemotherapy utilization was not significantlydifferent among the 3 groups (P >.05).
Analyses of the concurrent use of bevacizumab
Table 1 Sample Characteristics
DrugPatients,
NTotal doses,
NMean/patient (95%
CI)aMean interval, day (SD)
Mean database residence, mo (SD)
Docetaxel 1035 5009 5.9 (5.5-6.3) 20.5 (6.2) 12.6 (6.3)
Generic paclitaxel 997 6078 7.0 (6.6-7.3) 16.2 (8.8) 13.5 (6.4)
Nab-paclitaxel 213 2088 9.4 (8.5-10.2) 15.8 (8.9) 16.5 (6.6)aAdjusted for months of database residence. CI indicates confidence interval; SD, standard deviation.

Comparing Medical Cost of Care for MBC
281www.AHDBonline.com l American Health & Drug BenefitsVol 3, No 4 l July/August 2010
revealed that a greater proportion of patients in the nab-paclitaxel group received bevacizumab concurrentlycompared with patients receiving generic paclitaxel anddocetaxel, and the rate of patients using generic pacli-taxel who received concurrent bevacizumab was greater(P <.05 for all) than patients taking docetaxel (Table 3).A higher proportion of patients receiving nab-paclitaxelalso received bevacizumab after the taxane; the rate ofbevacizumab use was greater after generic paclitaxel thanafter docetaxel (P <.05 for both), but the difference wasnot significant (P >.05) between patients receiving nab-paclitaxel and generic paclitaxel (Table 2). The propor-tion of patients receiving concurrent or post-taxanetrastuzumab was not significantly different (P >.05)among the 3 groups (Table 3).
The rate of patients using nab-paclitaxel whoreceived concurrent and post-taxane gemcitabine wasgreater than in the generic paclitaxel and the docetaxelgroups (P <.05 for both), which were not significantlydifferent (P >.05) from each other in either setting.
The proportion of patients taking nab-paclitaxel whoreceived vinorelbine concurrently was greater thanpatients taking generic paclitaxel or docetaxel (P <.05for both), and the proportion of generic paclitaxelpatients who received concurrent vinorelbine was morethan those taking docetaxel (P <.05). The proportion ofpatients receiving post-taxane vinorelbine was not sig-nificantly different among the 3 groups (P >.05).
Total Medical Cost AnalysisThe total medical cost model was robust (r2 = 0.72).
Increased total medical cost was attributable to a num-ber of factors, whereas decreased total medical cost wasattributable to advancing age and previous chemothera-py (see Appendix at www.AHDBonline.com).
Over the 24-month study period, adjusted medianPPPM total medical costs were higher in patients receiv-ing nab-paclitaxel ($3997; 95% CI, $3634-$4396) anddocetaxel ($4042; 95% CI, $3844-$4251) (P <.05 forboth comparisons) than in patients receiving genericpaclitaxel ($3203; 95% CI, $3029-$3388). However,these costs were not significantly different between thenab-paclitaxel and docetaxel groups (Table 4).
When nab-paclitaxel was used as the initial treat-ment, the adjusted total medical costs were 25% (95%CI, 15%-36%) higher than when generic paclitaxel wasused first, holding other factors constant. Similarly,when docetaxel was used as the initial treatment, theadjusted total medical costs were 26% (95% CI, 20%-33%) higher than when treatment was initiated withgeneric paclitaxel. There was no significant difference inadjusted total medical costs of care between docetaxeland nab-paclitaxel.
Ancillary Medication Utilization and Cost AnalysisIn the analysis of ancillary medication use, rates of
CSF use were significantly higher for docetaxel than forgeneric paclitaxel and nab-paclitaxel (P <.05 for both);the latter 2 agents were not significantly different(P >.05) from each other (Table 5). Rates of ESA usewere not significantly different among the 3 groups(P >.05). Antiemetic use was significantly greater fordocetaxel than for generic paclitaxel (P <.05) but notsignificantly different between nab-paclitaxel andgeneric paclitaxel or nab-paclitaxel and docetaxel (P>.05 for both; Table 5). Figure 2 outlines the differences in ancillary medica-
Table 2 Before, Concurrent, and Post-Taxane Chemotherapy Use
Chemotherapy and taxane use
Docetaxel (N = 1035)
Generic paclitaxel (N = 997)
Nab-paclitaxel(N = 213)
Pre-taxanechemotherapy, % 34.4 43.0a 56.3b
Concurrent taxane-chemotherapy use, % 73.8c 65.2 62.0
Post-taxanechemotherapy, % 40.0 44.5 47.0
aP <.05 compared with docetaxel. bP <.05 compared with docetaxel and generic paclitaxel. cP <.05 compared with generic paclitaxel and nab-paclitaxel.
Table 3 Concurrent and Post-Taxane Bevacizumab,Trastuzumab, Gemcitabine, and Vinorelbine Use
Chemotherapyconcurrent/post-taxane use
Docetaxel (N = 1035), %
Generic paclitaxel
(N = 997), %Nab-paclitaxel(N = 213), %
Concurrentbevacizumab
4.9 13.1a 36.6b
Post-taxanebevacizumab
4.7 7.6a 12.2a
Concurrenttrastuzumab
23.6 25.3 27.2
Post-taxanetrastuzumab
18.5 19.6 15.5
Concurrentgemcitabine
4.8 5.4 18.3b
Post-taxanegemcitabine
6.8 8.2 14.6b
Concurrentvinorelbine
1.8 3.9a 11.7b
Post-taxanevinorelbine
3.6 4.0 7.0
aP <.05 compared with docetaxel.bP <.05 compared with docetaxel and generic paclitaxel.

BUSINESS
282 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
tion costs associated with generic paclitaxel and nab-paclitaxel compared with docetaxel. Per-patient CSFcosts were significantly lower with generic paclitaxel(–$7933) and with nab-paclitaxel (–$12,410) comparedwith docetaxel (P <.05); patients in the generic paclitax-el group had greater expenditures for CSFs comparedwith nab-paclitaxel (P <.05). Per-patient ESA costs weresignificantly lower with nab-paclitaxel (–$552) com-
pared with docetaxel (P <.05). There were no differencesin the costs of antiemetics between the groups (Figure 2).
DiscussionIn this retrospective claims analysis, we were able to
identify patients with MBC and effectively control foran array of variables, while evaluating total medical costsin this population. This type of analysis reflects theexpenditures incurred by a health plan and underscoresthe importance of a comprehensive analysis that con-trols for patient and treatment variability; this is pre-ferred to a simple comparison of drug acquisition costs orof mean (or median) total medical costs.
The median adjusted PPPM total medical costs forpatients receiving taxanes for MBC were within about$800 of each other (Table 4). Median PPPM total med-ical costs for docetaxel and nab-paclitaxel were not sta-tistically different, although total medical costs associat-ed with generic paclitaxel treatment were about 25%lower than docetaxel and nab-paclitaxel when analyzedwith multiple regression. The cost model explained 72%of the variability in total medical costs.
To evaluate the total medical costs associated withthe use of nab-paclitaxel instead of generic paclitaxel,we performed a post-hoc analysis of a hypotheticalhealth plan covering 1 million lives. If the annual inci-dence of breast cancer is 122.9 per 100,000 patients andapproximately 33% have MBC, then 406 patients([1,000,000 � 0.001229] � 0.33 = 406) from the hypo-thetical cohort would have MBC.15
The median total PPPM medical cost differencebetween nab-paclitaxel and generic paclitaxel is $794(Table 4). If this cost were distributed across the entireinsured population, each 10% increase in the proportionof patients receiving nab-paclitaxel instead of genericpaclitaxel would represent a $0.032 incremental increasein total medical expenditures per member per month.The patients receiving nab-paclitaxel would be expectedto realize a reduction in neutropenia and related costs.
In the present study, patients received more doses ofnab-paclitaxel than either docetaxel or generic paclitax-el; this may be attributed to a number of factors, includ-ing stage of treatment, tolerability, and efficacy. Becausenab-paclitaxel is often used in late-stage MBC,8 patientsobserved receiving this taxane might have required moreaggressive treatment. This was confirmed in our study,because nab-paclitaxel was administered more frequent-ly in combination with bevacizumab, gemcitabine, andvinorelbine, which were used more often by patientswith advanced MBC.
Other studies have underscored the impact of costelements in addition to drug acquisition cost in deter-mining total costs.3,14 An analysis by Barron and col-
Table 5 Ancillary Medication Utilization among Patients Receiving a Taxane
Ancillary drug use
Docetaxel (N = 1035), %
Generic paclitaxel(N = 997), %
Nab-paclitaxel(N = 213), %
CSFs 61.6a 43.4 38.0
ESAs 44.5 49.5 53.1
Antiemetics 92.6b 87.5 88.3aP <.05 compared with generic paclitaxel and nab-paclitaxel. bP <.05 compared with generic paclitaxel with the Marascuillo procedure. CSFs indicates colony-stimulating factors; ESAs, erythropoiesis-stimulating agents.
Table 4 Per-Patient Per-Month Total Medical Costs of Care forthe Taxanes in Metastatic Breast Cancer
Adjusted median PPPM (95% CI), $
Generic paclitaxel 3203 (3029-3388)
Docetaxel 4042 (3844-4251)
Nab-paclitaxel 3997 (3634-4396)CI indicates confidence interval; PPPM, per patient per month.
aP <.05.CSFs indicates colony-stimulating factors; ESAs, erythropoiesis-stimulating agents.
2000
0101
–552a –136 –235
–2000
–4000
–6000
–8000 –7933a
–10,000
–12,000–12,410a
–14,000
Generic paclitaxelNab-paclitaxel
CSFs ESAs Antiemetics
Figure 2 Mean Ancillary Medication Costs per Member during24 Months Compared with Docetaxel

Comparing Medical Cost of Care for MBC
283www.AHDBonline.com l American Health & Drug BenefitsVol 3, No 4 l July/August 2010
leagues demonstrated that the significant economicburden of breast cancer is driven mainly by hospitaliza-tions, which contribute to the total cost at a rate morethan twice that of chemotherapy.14 However, the costsof chemotherapy were significant, and the analysis wasperformed before the availability of several expensiveagents used by patients with MBC.14 More recently,Kruse and colleagues found that chemotherapeuticagents accounted for nearly 60% of costs associatedwith breast cancer.3
In the present analysis, chemotherapy expenses (tax-ane plus all other chemotherapy) represented between44% and 62% of unadjusted mean total medical costs,exclusive of outpatient pharmacy chemotherapy, in the3 taxane groups. The sum of hospital, office visit, andother charges (eg, laboratory tests, x-rays) representedless than 41% of unadjusted mean total medical costs inthe 3 taxane groups. In the analyses by Barron and col-leagues and Kruse and colleagues, the mean PPPM totalmedical costs were $4996 and $4421, respectively,3,14compared with our median values, which ranged from$3203 to $4042.
In our analysis, patients receiving nab-paclitaxel hadsignificantly lower expenditures for CSFs compared withdocetaxel or generic paclitaxel. This may be explainedby the improved tolerability and lower rates of neu-tropenia observed with the albumin-bound formulation.In a study based on a database of patients hospitalized forfebrile neutropenia, Kuderer and colleagues concludedthat a number of patient-specific factors, such as severi-ty of disease, type of malignancy, and comorbidities con-tribute to increased mortality, length of stay, and hospi-talization costs.16 Such factors should be taken intoconsideration, and appropriate therapies should be uti-lized, to address these concerns as a means of improvingoutcomes and controlling costs.
LimitationsThe most obvious limitation of this analysis is the ret-
rospective nature of the study, which does not control fordrug selection biases related to the stage of therapy. Wewent to considerable effort to identify patients withMBC; however, it is difficult to identify second- andthird-line therapies in a relatively short period of follow-up. Continuous enrollment was not an inclusion criteri-on for patient selection, but duration of residence in thedata set was used as a control variable. Requiring con-tinuous enrollment of our population of patients withMBC would have significantly limited our sample sizes.
Furthermore, in this type of analysis it is difficult tocontrol for patient severity of illness, because the clini-cal status of the patient is not available. We did, howev-er, control for the number of procedures and the number
of unique diagnoses for the patients included in thisanalysis. Both of these variables were associated with sig-nificant increases in total costs.
In addition, this analysis did not specifically identifyAE rates, such as infusion-related AEs; however, thecosts associated with AEs are included in the total med-ical cost calculations.
These data represent a snapshot in time rather than acomprehensive view of disease progression from early- tolate-stage illness.
Tobit analyses have been criticized in healthcareclaims analyses, because of highly variable costs overtime. Although outpatient drug therapy costs were notcaptured, any bias should be equally applied across all 3taxane groups.
Finally, the clinical efficacy of the taxanes was notassessed in this study.
ConclusionsAnalysis of the myriad factors besides drug acquisition
cost is necessary to make a determination of the costs ofa particular therapy. The efficacy and tolerability of var-ious treatments are reflected in total costs, where reduc-tions in AEs and the use of ancillary medications offsethigher drug acquisition costs. In the case of the taxanes,the overall costs of breast cancer management are relat-ed to the entire chemotherapeutic regimen, as well as tothe costs of hospitalization. These factors contribute tototal medical cost, which may be used as the primaryoutcome measure in a pharmacoeconomic evaluationrather than simply drug acquisition cost. In this analysisof total medical costs, generic paclitaxel was the leastexpensive, whereas nab-paclitaxel and docetaxel result-ed in similar overall medical expenditures. ■
AcknowledgmentThe authors thank Teri Peterson, MS, for her assis-
tance with the statistical analyses.
Disclosure StatementsThis project was sponsored by Abraxis Oncology, manu-
facturer of Abraxane (nab-paclitaxel). The sponsor had norole in the study design, analysis, or writing of the manuscript.The investigators had exclusive access to the data and inde-pendently developed the research design and wrote this report.Dr Force, Dr Pugmire, and Dr Culbertson have received
research/grant support from Abraxis and ICORE Health -care. Dr Force is also a Consultant to Abraxis and ICOREHealthcare.
References1. American Cancer Society. Cancer Facts & Figures 2008. Atlanta, GA: AmericanCancer Society; 2008. 2. Brown ML, Riley GF, Schussler N, Etzioni R. Estimating health care costs relat-ed to cancer treatment from SEER-Medicare data. Med Care. 2002;40(suppl 8):IV-104-IV-117.3. Kruse GB, Amonkar MM, Smith G, et al. Analysis of costs associated with admin-

BUSINESS
284 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
istration of intravenous single-drug therapies in metastatic breast cancer in a U.S.population. J Manag Care Pharm. 2008;14:844-857. 4. Taxol (paclitaxel) injection prescribing information. New York, NY: Bristol-MyersSquibb; July 2007.5.Taxotere (docetaxel) prescribing information. Bridgewater, NJ: sanofi-aventis; 2007.6.Markman M. Managing taxane toxicities. Support Care Cancer. 2003;11:144-147.Epub 2002 Oct 15.7. Irizarry LD, Luu TH, McKoy JM, et al. Cremophor EL-containing paclitaxel-induced anaphylaxis: a call to action. Community Oncol. 2009;6:132-134.8. Abraxane (paclitaxel) prescribing information. Los Angeles, CA: AbraxisBioScience; 2007. 9. Desai, N, Trieu V, Yao Z, et al. Increased antitumor activity, intratumor paclitaxelconcentrations, and endothelial cell transport of cremophor-free, albumin-boundpaclitaxel, ABI-007, compared with cremophor-based paclitaxel. Clin Cancer Res.2006;12:1317-1324.10. Gradishar WJ, Tjulandin S, Davidson N, et al. Phase III trial of nanoparticlealbumin-bound paclitaxel compared with polyethylated castor oil-based paclitaxel in
women with breast cancer. J Clin Oncol. 2005;23:7794-7803. Epub 2005 Sep 19.11. Ghersi D, Wilcken N, Simes J, Donoghue E. Taxane containing regimens formetastatic breast cancer. Cochrane Database Syst Rev. 2005;2:CD003366. 12.Gradishar WJ, Krasnojon D, Cheporov S, et al. Significantly longer progression-free survival with nab-paclitaxel compared with docetaxel as first-line therapy formetastatic breast cancer. J Clin Oncol. 2009;27:3611-3619. Epub 2009 May 26.13. Dranitsaris G, Cottrell W, Spirovski B, Hopkins S. Economic analysis of albu-min-bound paclitaxel for the treatment of metastatic breast cancer. J Oncol PharmPract. 2009;15:67-78. Epub 2008 Nov 26.14. Barron JJ, Quimbo R, Nikam PT, Amonkar MM. Assessing the economic bur-den of breast cancer in a US managed care population. Breast Cancer Res Treat.2008;109:367-377. Epub 2007 Aug 3.15. Horner MJ, Ries LAG, Krapcho M, et al (eds). SEER Cancer Statistics Review,1975-2006. National Cancer Institute. Bethesda, MD. http://seer.cancer.gov/statfacts/html/breast.html. Accessed June 10, 2010. 16. Kuderer NM, Dale DC, Crawford J, et al. Mortality, morbidity, and cost associ-ated with febrile neutropenia in adult cancer patients. Cancer. 2006;106:2258-2266.
PAYERS: The beauty of this article by Force andcolleagues is that it makes the reader think. In this dayand age when we are all focused on cost of care, drugacquisition costs, cost-sharing, and the like, we tendto forget about clinical outcomes, and what is best forthe patient. Although it is ideal to find therapieswithin a therapeutic class that are lowest in cost andprovide equal or better clinical outcomes than com-parator therapies, this is rarely the case. Have wefound our answer based on the published results of thisret rospective analysis?
Metastatic breast cancer is a serious, life-threateningcondition. Metastatic breast cancer treatment is veryexpensive. This is fact. The use of a generic product,paclitaxel, as the preferred taxane for treating metasta-tic breast cancer as the means to keep cost of care incheck based on this article may be non sequitur.
The National Comprehensive Cancer NetworkClinical Practice Guidelines for breast cancer list all3 marketed taxanes (paclitaxel, docetaxel, and nab-paclitaxel) as preferred agents for the treatment ofmetastatic breast cancer.1 The product labeling fornab-paclitaxel cites a clinical trial that comparednab-paclitaxel with paclitaxel and demonstrated sig-nificantly better overall response rate with nab-pacli-taxel.2 In addition, several clinical trials cited in thisarticle demonstrated advantages for using nab-pacli-taxel compared with paclitaxel and docetaxel interms of progression-free survival and lower rates ofadverse events. Note, however, that nab-paclitaxelhas not demonstrated better overall survival com-pared with paclitaxel.
Force and colleagues found that the per-patient per-month medical cost of care was approximately $800lower with paclitaxel compared with nab-paclitaxel or
docetaxel. When comparing nab-paclitaxel and doc-etaxel, there was no significant difference in cost ofcare. Patients receiving nab-paclitaxel received moredoses than patients receiving the other taxanes, andthese patients also had the lowest utilization and costsassociated with colony-stimulating factors.
The limitations of this study were few but signifi-cant. This is a retrospective study that does not con-trol for drug selection based on the stage of therapy.It is also difficult to control for severity of illness in aret rospective study. Finally, the clinical efficacy ofthe taxanes was not assessed in this study.
Many payers have already implemented strategiesmaking paclitaxel the preferred taxane for theirmembership, based on its generic availability and itsacquisition costs that are lower than for the othertaxanes. These payers can demonstrate significantsavings related to drug cost trends and spending. Itwould be interesting to evaluate the impact of taxaneproduct preferencing on clinical outcomes in addi-tion to drug cost trends and spending.
I am confident that payers put more importanceon improved clinical outcomes than on cost trends.When implementing product preferencing strategies,proactively developing analyses that demonstrateimproved clinical outcomes while resulting in cost-savings is what the industry needs.
1. National Comprehensive Cancer Network. NCCN clinical practice guide-lines in oncology: breast cancer V.2.2010. www.nccn.org/professionals/physician_gls/PDF/breast.pdf. Accessed July 23, 2010.2. Abraxane (paclitaxel protein-bound particles for injectable suspension).Prescribing information. Bridgewater, NJ: Abraxis Bioscience; March 2010.
Atheer A. Kaddis, PharmDVice President, Managed Markets
Diplomat Specialty Pharmacy
Can We Afford Improved Clinical Outcomes?
STAKEHOLDER PERSPECTIVE

For your members with moderate to severe plaque psoriasis
Please see Important Safety Information and Brief Summary of Prescribing Information for STELARA™on the following pages.
www.STELARAinfo.com
IndicationSTELARA™ is indicated for the treatment of adult patients (18 years or older)with moderate to severe plaque psoriasis who are candidates for phototherapy orsystemic therapy.
DosingSTELARA™ is administered by subcutaneous injection.
• For patients weighing ≤100 kg (220 lbs), the recommended dose is 45 mg initiallyand 4 weeks later, followed by 45 mg every 12 weeks
• For patients weighing >100 kg (220 lbs), the recommended dose is 90 mg initiallyand 4 weeks later, followed by 90 mg every 12 weeks
In patients weighing >100 kg, 45 mg was also shown to be efficacious. However,90 mg resulted in greater efficacy in these patients.
The safety and efficacy of STELARA™ have not been evaluated beyond two years.
Dosage forms and strengthsSTELARA™ contains 90 mg of ustekinumab per mL.
• 45 mg/0.5 mL in a single-use, prefilled syringe, with an NDC number of 57894-060-03
• 90 mg/1 mL in a single-use, prefilled syringe, with an NDC number of 57894-061-03

IMPORTANT SAFETY INFORMATIONInfectionsSTELARA™ may increase the risk of infections and reactivation of latent infections. Serious bacterial, fungal, andviral infections were reported. Infections requiring hospitalization included cellulitis, diverticulitis, osteomyelitis,gastroenteritis, pneumonia, and urinary tract infections. STELARA™ should not be given to patients with a clinicallyimportant active infection and should not be administered until the infection resolves or is adequately treated.Instruct patients to seek medical advice if signs or symptoms suggestive of an infection occur. Exercise cautionwhen considering use of STELARA™ in patients with a chronic infection or a history of recurrent infection.
Theoretical Risk for Vulnerability to Particular InfectionsIndividuals genetically deficient in IL-12/IL-23 are particularly vulnerable to disseminated infections frommycobacterium, Salmonella, and Bacillus Calmette-Guerin (BCG) vaccinations. Serious infections and fataloutcomes have been reported in such patients. It is not known whether patients with pharmacologic blockadeof IL-12/IL-23 from treatment with STELARA™ will be susceptible to these types of infections. Considerappropriate diagnostic testing as dictated by clinical circumstances.
Pre-Treatment Evaluation of Tuberculosis (TB)Evaluate patients for TB prior to initiating treatment with STELARA™. STELARA™ should not be given to patientswith active TB. Initiate treatment of latent TB before administering STELARA™. Patients should be monitoredclosely for signs and symptoms of active TB during and after treatment with STELARA™.
MalignanciesSTELARA™ is an immunosuppressant and may increase the risk of malignancy. Malignancies were reportedamong patients who received STELARA™ in clinical studies. The safety of STELARA™ has not been evaluatedin patients who have a history of malignancy or who have a known malignancy.
Reversible Posterior Leukoencephalopathy Syndrome (RPLS)One case of RPLS has been reported in a STELARA™-treated patient. If RPLS is suspected, discontinueSTELARA™ and administer appropriate treatment.RPLS is a neurological disorder, which is not caused by an infection or demyelination. RPLS can present withheadache, seizures, confusion, and visual disturbances. RPLS has been associated with fatal outcomes.
ImmunizationsPrior to initiating therapy with STELARA™, patients should receive all immunizations recommended by currentguidelines. Patients being treated with STELARA™ should not receive live vaccines. BCG vaccines should not begiven during treatment or within one year of initiating or discontinuing STELARA™. Exercise caution whenadministering live vaccines to household contacts of STELARA™ patients, as shedding and subsequenttransmission to STELARA™ patients may occur. Non-live vaccinations received during a course of STELARA™may not elicit an immune response sufficient to prevent disease.
Concomitant TherapiesThe safety of STELARA™ in combination with other immunosuppressive agents or phototherapy has not beenevaluated. Ultraviolet-induced skin cancers developed earlier and more frequently in mice genetically manipulatedto be deficient in both IL-12 and IL-23 or IL-12 alone. The relevance of these findings in mouse models formalignancy risk in humans is unknown.
Most Common Adverse ReactionsThe most common adverse reactions (≥3% and higher than that with placebo) in clinical trials for STELARA™45 mg, STELARA™ 90 mg, or placebo were: nasopharyngitis (8%, 7%, 8%), upper respiratory tract infection(5%, 4%, 5%), headache (5%, 5%, 3%), and fatigue (3%, 3%, 2%), respectively.
Please see Brief Summary of Prescribing Information for STELARA™ on the following page.
Reference: STELARA™ Prescribing Information 12/2009. Horsham, PA: Centocor Ortho Biotech Inc.
representing the products of
www.STELARAinfo.com ©2010 Centocor Ortho Biotech Services, LLC 4/10 25STPMC10012
25US10030

Brief Summary of Prescribing Information for STELARA™ (ustekinumab) STELARA™ Injection, for subcutaneous useSee package insert for Full Prescribing InformationINDICATIONS AND USAGE: STELARA™ is indicated for the treatment of adult patients (18 yearsor older) with moderate to severe plaque psoriasis who are candidates for phototherapy or systemictherapy. CONTRAINDICATIONS: None. WARNINGS AND PRECAUTIONS: InfectionsSTELARA™ may increase the risk of infections and reactivation of latent infections. Seriousbacterial, fungal, and viral infections were observed in subjects receiving STELARA™ (see AdverseReactions). STELARA™ should not be given to patients with any clinically important activeinfection. STELARA™ should not be administered until the infection resolves or is adequatelytreated. Instruct patients to seek medical advice if signs or symptoms suggestive of an infectionoccur. Exercise caution when considering the use of STELARA™ in patients with a chronicinfection or a history of recurrent infection. Serious infections requiring hospitalization occurredin the psoriasis development program. These serious infections included cellulitis, diverticulitis,osteomyelitis, viral infections, gastroenteritis, pneumonia, and urinary tract infections. TheoreticalRisk for Vulnerability to Particular Infections Individuals genetically deficient in IL-12/IL-23are particularly vulnerable to disseminated infections from mycobacteria (including nontuberculous,environmental mycobacteria), salmonella (including nontyphi strains), and Bacillus Calmette-Guerin(BCG) vaccinations. Serious infections and fatal outcomes have been reported in such patients. Itis not known whether patients with pharmacologic blockade of IL-12/IL-23 from treatment withSTELARA™ will be susceptible to these types of infections. Appropriate diagnostic testing shouldbe considered, e.g., tissue culture, stool culture, as dictated by clinical circumstances.Pre-treatment Evaluation for Tuberculosis Evaluate patients for tuberculosis infection priorto initiating treatment with STELARA™. Do not administer STELARA™ to patients with activetuberculosis. Initiate treatment of latent tuberculosis prior to administering STELARA™. Consideranti-tuberculosis therapy prior to initiation of STELARA™ in patients with a past history of latentor active tuberculosis in whom an adequate course of treatment cannot be confirmed. Patientsreceiving STELARA™ should be monitored closely for signs and symptoms of active tuberculosisduring and after treatment. Malignancies STELARA™ is an immunosuppressant and mayincrease the risk of malignancy. Malignancies were reported among subjects who receivedSTELARA™ in clinical studies (see Adverse Reactions). In rodent models, inhibition ofIL-12/IL-23p40 increased the risk of malignancy (see Nonclinical Toxicology). The safety ofSTELARA™ has not been evaluated in patients who have a history of malignancy or who have aknown malignancy. Reversible Posterior Leukoencephalopathy Syndrome One case ofreversible posterior leukoencephalopathy syndrome (RPLS) was observed during the clinicaldevelopment program which included 3523 STELARA™-treated subjects. The subject, who hadreceived 12 doses of STELARA™ over approximately two years, presented with headache,seizures and confusion. No additional STELARA™ injections were administered and the subjectfully recovered with appropriate treatment. RPLS is a neurological disorder, which is not causedby demyelination or a known infectious agent. RPLS can present with headache, seizures,confusion and visual disturbances. Conditions with which it has been associated includepreeclampsia, eclampsia, acute hypertension, cytotoxic agents and immunosuppressive therapy.Fatal outcomes have been reported. If RPLS is suspected, STELARA™ should be discontinuedand appropriate treatment administered. Immunizations Prior to initiating therapy withSTELARA™, patients should receive all immunizations appropriate for age as recommended bycurrent immunization guidelines. Patients being treated with STELARA™ should not receive livevaccines. BCG vaccines should not be given during treatment with STELARA™ or for one yearprior to initiating treatment or one year following discontinuation of treatment. Caution is advisedwhen administering live vaccines to household contacts of patients receiving STELARA™ becauseof the potential risk for shedding from the household contact and transmission to patient. Non-livevaccinations received during a course of STELARA™ may not elicit an immune response sufficientto prevent disease. Concomitant Therapies The safety of STELARA™ in combination with otherimmunosuppressive agents or phototherapy has not been evaluated. Ultraviolet-induced skincancers developed earlier and more frequently in mice genetically manipulated to be deficient inboth IL-12 and IL-23 or IL-12 alone (see Nonclinical Toxicology). ADVERSE REACTIONS: Thefollowing serious adverse reactions are discussed elsewhere in the label: Infections (see Warningsand Precautions); Malignancies (see Warnings and Precautions); and RPLS (see Warnings andPrecautions). Clinical Studies Experience The safety data reflect exposure to STELARA™ in2266 psoriasis subjects, including 1970 exposed for at least 6 months, 1285 exposed for at leastone year, and 373 exposed for at least 18 months. Because clinical trials are conducted underwidely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannotbe directly compared to rates in the clinical trials of another drug and may not reflect the ratesobserved in practice. Adverse reactions listed below are those that occurred at a rate of at least1% and at a higher rate in the STELARA™ groups than the placebo group during theplacebo-controlled period of STUDY 1 and STUDY 2. The numbers (percentages) of adversereactions reported for placebo-treated patients (n=665), patients treated with 45 mg STELARA™(n=664), and patients treated with 90 mg STELARA™ (n=666), respectively, were:Nasopharyngitis: 51 (8%), 56 (8%), 49 (7%); Upper respiratory tract infection: 30 (5%), 36 (5%),28 (4%); Headache: 23 (3%), 33 (5%), 32 (5%); Fatigue: 14 (2%), 18 (3%), 17 (3%); Diarrhea:12 (2%), 13 (2%), 13 (2%); Back pain: 8 (1%), 9 (1%), 14 (2%); Dizziness: 8 (1%), 8 (1%), 14(2%); Pharyngolaryngeal pain: 7 (1%), 9 (1%), 12 (2%); Pruritus: 9 (1%), 10 (2%), 9 (1%); Injectionsite erythema: 3 (<1%), 6 (1%), 13 (2%); Myalgia: 4 (1%), 7 (1%), 8 (1%); Depression: 3 (<1%),8 (1%), 4 (1%). Adverse drug reactions that occurred at rates less than 1% included: cellulitisand certain injection site reactions (pain, swelling, pruritus, induration, hemorrhage, bruising, andirritation). One case of RPLS occurred during clinical trials (see Warnings and Precautions).Infections In the placebo-controlled period of clinical studies of psoriasis subjects (averagefollow-up of 12.6 weeks for placebo-treated subjects and 13.4 weeks for STELARA™-treatedsubjects), 27% of STELARA™-treated subjects reported infections (1.39 per subject-year offollow-up) compared with 24% of placebo-treated subjects (1.21 per subject-year of follow-up).Serious infections occurred in 0.3% of STELARA™-treated subjects (0.01 per subject-year offollow-up) and in 0.4% of placebo-treated subjects (0.02 per subject-year of follow-up) (seeWarnings and Precautions). In the controlled and non-controlled portions of psoriasis clinical trials,61% of STELARA™-treated subjects reported infections (1.24 per subject-year of follow-up).
Serious infections were reported in 0.9% of subjects (0.01 per subject-year of follow-up).Malignancies In the controlled and non-controlled portions of psoriasis clinical trials, 0.4% ofSTELARA™-treated subjects reported malignancies excluding non-melanoma skin cancers (0.36per 100 subject-years of follow-up). Non-melanoma skin cancer was reported in 0.8% ofSTELARA™-treated subjects (0.80 per 100 subject-years of follow-up) (see Warnings andPrecautions). Serious malignancies included breast, colon, head and neck, kidney, prostate, andthyroid cancers. Immunogenicity The presence of ustekinumab in the serum can interfere withthe detection of anti-ustekinumab antibodies resulting in inconclusive results due to assayinterference. In STUDIES 1 and 2, antibody testing was done at time points when ustekinumabmay have been present in the serum. In STUDY 1 the last ustekinumab injection was betweenWeeks 28 and 48 and the last test for anti-ustekinumab antibodies was at Week 52. In STUDY 2the last ustekinumab injection was at Week 16 and the last test for anti-ustekinumab antibodieswas at Week 24. In STUDY 1 (N=743), antibody results were found to be positive, negative, andinconclusive in 38 (5%), 351 (47%), and 354 (48%) patients, respectively. In STUDY 2 (N=1198),antibody results were found to be positive, negative, and inconclusive in 33 (3%), 90 (8%), and1075 (90%) patients, respectively. The data reflect the percentage of subjects whose test resultswere positive for antibodies to ustekinumab in a bridging immunoassay, and are highly dependenton the sensitivity and specificity of the assay. Additionally, the observed incidence of antibodypositivity in an assay may be influenced by several factors, including sample handling, timing ofsample collection, concomitant medications and underlying disease. For these reasons,comparison of the incidence of antibodies to ustekinumab with the incidence of antibodies toother products may be misleading. DRUG INTERACTIONS: Drug interaction studies have notbeen conducted with STELARA™. Live Vaccines Live vaccines should not be given concurrentlywith STELARA™ (see Warnings and Precautions). Concomitant Therapies The safety ofSTELARA™ in combination with immunosuppressive agents or phototherapy has not beenevaluated (see Warnings and Precautions). CYP450 Substrates The formation of CYP450enzymes can be altered by increased levels of certain cytokines (e.g., IL-1, IL-6, IL-10, TNF�, IFN)during chronic inflammation. Thus, ustekinumab could normalize the formation of CYP450enzymes. A role for IL-12 or IL-23 in the regulation of CYP450 enzymes has not been reported.However, upon initiation of ustekinumab in patients who are receiving concomitant CYP450substrates, particularly those with a narrow therapeutic index, monitoring for therapeutic effect(e.g., for warfarin) or drug concentration (e.g., for cyclosporine) should be considered and theindividual dose of the drug adjusted as needed (see Clinical Pharmacology). USE IN SPECIFICPOPULATIONS: Pregnancy Pregnancy Category B There are no studies of STELARA™ inpregnant women. STELARA™ should be used during pregnancy only if the potential benefitjustifies the potential risk to the fetus. No teratogenic effects were observed in the developmentaland reproductive toxicology studies performed in cynomolgus monkeys at doses up to 45 mg/kgustekinumab, which is 45 times (based on mg/kg) the highest intended clinical dose in psoriasispatients (approximately 1 mg/kg based on administration of a 90 mg dose to a 90 kg psoriasispatient). Ustekinumab was tested in two embryo-fetal development toxicity studies. Pregnantcynomolgus monkeys were administered ustekinumab at doses up to 45 mg/kg during the periodof organogenesis either twice weekly via subcutaneous injections or weekly by intravenousinjections. No significant adverse developmental effects were noted in either study. In anembryo-fetal development and pre- and post-natal development toxicity study, three groups of20 pregnant cynomolgus monkeys were administered subcutaneous doses of 0, 22.5, or 45 mg/kg ustekinumab twice weekly from the beginning of organogenesis in cynomolgus monkeysto Day 33 after delivery. There were no treatment-related effects on mortality, clinical signs, bodyweight, food consumption, hematology, or serum biochemistry in dams. Fetal losses occurred insix control monkeys, six 22.5 mg/kg-treated monkeys, and five 45 mg/kg-treated monkeys.Neonatal deaths occurred in one 22.5 mg/kg-treated monkey and in one 45 mg/kg-treatedmonkey. No ustekinumab-related abnormalities were observed in the neonates from birth throughsix months of age in clinical signs, body weight, hematology, or serum biochemistry. There wereno treatment-related effects on functional development until weaning, functional developmentafter weaning, morphological development, immunological development, and gross andhistopathological examinations of offsprings by the age of 6 months. Nursing Mothers Cautionshould be exercised when STELARA™ is administered to a nursing woman. The unknown risksto the infant from gastrointestinal or systemic exposure to ustekinumab should be weighed againstthe known benefits of breast-feeding. Ustekinumab is excreted in the milk of lactating monkeysadministered ustekinumab. IgG is excreted in human milk, so it is expected that STELARA™ willbe present in human milk. It is not known if ustekinumab is absorbed systemically after ingestion;however, published data suggest that antibodies in breast milk do not enter the neonatal andinfant circulation in substantial amounts. Pediatric Use Safety and effectiveness of STELARA™in pediatric patients have not been evaluated. Geriatric Use Of the 2266 psoriasis subjectsexposed to STELARA™, a total of 131 were 65 years or older, and 14 subjects were 75 years orolder. Although no differences in safety or efficacy were observed between older and youngersubjects, the number of subjects aged 65 and over is not sufficient to determine whether theyrespond differently from younger subjects. OVERDOSAGE: Single doses up to 4.5 mg/kgintravenously have been administered in clinical studies without dose-limiting toxicity. In case ofoverdosage, it is recommended that the patient be monitored for any signs or symptoms of adversereactions or effects and appropriate symptomatic treatment be instituted immediately. PATIENTCOUNSELING INFORMATION: Instruct patients to read the Medication Guide before startingSTELARA™ therapy and to reread the Medication Guide each time the prescription is renewed.Infections Inform patients that STELARA™ may lower the ability of their immune system to fightinfections. Instruct patients of the importance of communicating any history of infections to thedoctor, and contacting their doctor if they develop any symptoms of infection. Malignancies Patientsshould be counseled about the risk of malignancies while receiving STELARA™.Prefilled Syringe Manufactured by: Vial Manufactured by:Centocor Ortho Biotech Inc., Centocor Ortho Biotech Inc.,Horsham, PA 19044, Horsham, PA 19044,License No. 1821 at License No. 1821 atBaxter Pharmaceutical Solutions, Cilag AG,Bloomington, IN 47403 Schaffhausen, Switzerland1-800-457-6399 25US10041© Centocor Ortho Biotech Inc. 2009 December 2009

JOIN AHDB PEER REVIEW
Articles fall into 3 main areas related to healthcare:Regulatory, Business, and Clinical. These main categoriesare represented from the different vantage points of allstakeholders in healthcare and are divided into manysubcategories, including (but not limited to):
• Administration/Management• Benefit design• Disease management/state (eg, asthma,infectious diseases, pain management, schizophrenia)
• Drug therapy (including biologics, generics)• Drug utilization• Employer benefits• Finance/economics• Health information technology• Health policy/reform• Patient education/initiatives/quality-of-life issues• Pharmacoeconomics: cost-benefit analysis,cost-effectiveness
• Pharmacy management: pharmacology,specialty pharmacy, pharmacy benefits
• Reimbursement: Medicare/Medicaid,health insurance, prior authorization
• Research: methods, study design,data collection/analysis
American Health & Drug Benefits(AHDB) is looking for medical
and pharmacy directors,P & T Committee members, and
other experts in benefit designwho are interested in joining our
peer reviewers and assist inmaintaining the high quality ofarticles published in the journal.
You will be asked to reviewat least 1 or 2 articles per year inyour area of expertise. Reviewers’
names will be published inAHDB at the end of the year.
Reviewers should have at least 1area of expertise in a health-relatedfield for which they feel qualified
to assess the content and quality ofmanuscripts submitted for
publication in AHDB.
To become a peer reviewer, please complete the form below and fax to: 732-992-1881or e-mail to [email protected]
Reviewer Information
_______________________________________________________________________________________First Name Last Name Credentials
_______________________________________________________________________________________Title Company
_______________________________________________________________________________________Address
_______________________________________________________________________________________E-mail Phone

289www.AHDBonline.com l American Health & Drug BenefitsVol 3, No 4 l July/August 2010
HEALTHCARE REFORM
The Healthcare Reform Act—officially called thePatient Protection and Affordable Care Act(PPACA)—institutes sweeping changes across
all healthcare stakeholders, including payers, providers,and plan members. In fact, the amount of changerequired by the PPACA is so extensive, distilling allthe changes down and accounting for their impact is aserious challenge for the industry as a whole. However,if we focus on the apparent macro changes that affectpayers—an increase in competition for the group mar-ket, an increase in overall access, and new regulationson expense caps for medical costs—a rational set ofassumptions becomes apparent for predicting the directimpact on stakeholders. The implementation of thesechanges will cause payers to: 1.Develop new products and provider networks that arealigned based on the benefit structure and the needs ofthe covered population; these tailored, personalizedproducts and provider networks will enable payers tomore effectively serve their customers’ needs
2.Design new provider-reimbursement models that shiftmethodology from paying for individual services toreimbursing for improved member health and well-ness, the latter being driven by provider performance,quality measurement, and member outcomes
3.Create new provider- and member-engagementstrategies that enable greater information sharingand transparency for improved decision support
4. Implement/redesign internal payer processes to fur-ther drive down administrative costs. Although some reform requirements have enact-
ment dates as far as 2018, we consider reform a com-plete overhaul of the healthcare system, necessitating aphased approach to ensure success. Payers, providers,and plan members need to begin preparing for thesechanges, because the changes will affect the traditionalstakeholder relationships we take part in today.
Greater Differentiation for Payer Products The needs of plan members vary across the spectrum
of benefit designs—some need only preventive healthbenefits, whereas others require preventive and cata-strophic coverage levels. The PPACA will driveapproximately 32 million more members into thehealthcare system.1 Some of these new members willfall into traditional lines of business for a payer; how-ever, estimates by the Congressional Budget Office andPriceWaterhouseCoopers predict that these memberswill drive expansion in the individual market.2The government-mandated healthcare exchanges,
stipulated by the PPACA, are poised to be the principalavenue for competition within the individual market.The benefit structures will be defined by the government,so the area for differentiation from the payer’s perspectivewill be on price, the member’s experience, and compati-bility of the network with the plan member’s needs. In addition, as the individual insurance market
increases, the group insurance market is estimated todecrease by 3 million members.2 This potential decreasein the member population, coupled with increasedpayer dependence on the profitability experience in thegroup market, will cause increased competition for thevalued group customer. Continued emphasis on differ-entiation by product and network, furthered by benefitdesigns that align with a group’s individual healthcareneeds, will drive success in this area of the payer market.
Redefining Provider-Reimbursement ModelsAlong with membership population changes, the
regulatory change that excludes payers from denyingcoverage, combined with the change that institutesnew spending caps on medical costs, is already begin-ning to drive innovation in provider-reimbursementmethodologies. Traditional fee-for-service (FFS) reimbursement me -
thodologies do not enable payers to optimally managenew member populations with fluctuating/nonpre-dictable risk profiles, and they do not account forphysician/provider performance and quality programs.
Mr Muppalla is Executive Vice President and Chief Strategyand Marketing Officer, and Mr Capobianco is Director ofMarketing, Portico Systems, Blue Bell, PA.
The Impact of Healthcare Reform on Payers’ Products, ProviderReimbursement, and MemberEngagement Sam Muppalla and Robert Capobianco Sam Muppalla

HEALTHCARE REFORM
290 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
The Massachusetts Attorney General’s 2010 report,Examination of Health Care Cost Trends and Cost Drivers,3provides evidence supporting the need for changes inthe reimbursement model. The report relates substantialevidence that nonstandard and non–quality-basedprovider contracts are a major contributor to risinghealthcare costs.3 The emergence of provider reimburse-ment models based on episodic and global payments islikely in reaction to these developments. These reim-bursement models will not completely eliminate the FFSmodel, but they enable hybrid pricing models that com-bine FFS payments with reimbursement payments forthe delivery of reliable evidence-based care.
Changing Payer-to-Provider-to-MemberEngagement ModelsAlthough these reimbursement and product changes
are derivative in nature, stemming from changes inmultiple parts of the PPACA, the anticipated payer-to-provider-to-member engagement changes are primarilydriven by the PPACA’s call for improved collaborationand information-sharing among all stakeholders. ThePPACA reignites the focus on how to increase the clin-ical collaboration between payers and providers andhow to better engage members to improve their health-care decisions.The healthcare marketplace has shown movement
in this direction via patient-centered medical homepilot projects and other team-based delivery programs.Such programs intend to facilitate evidence-basedmedicine and coordination between the care-deliveryteam and the particular member’s care program. These types of collaborative care environments, in
conjunction with the American Reinvestment andRecovery Act, are fueling a new round of payer invest-
ment in point-of-service tools, such as electronic med-ical records, e-prescribing, and e-laboratory order entrysystems. These assets between payers and providers areneeded to facilitate the exchange and analysis of clini-cal information by all parties to better serve membersand improve their overall health status. The member’s interactions with their providers and
payers will also take on a new dynamic. With the riseof an individual market and a likely acceleration ofpayer products like health savings accounts, memberswill share a greater amount of financial responsibilityfor the care services provided. In line with this greaterfinancial responsibility, payers and providers will needto be able to provide quality and cost information tomembers in a more seamless and transparent fashion toimprove member decision-making capability.
ConclusionAs a result of increased competition, expanded
access, and amplified cost-containment pressurescaused by the Reform Act, payers will need to changetheir operational DNA to achieve product differentia-tion, administrative and medical cost-containment,and quality-based relationships with their provider net-works. Changes in the payer industry will have a rippleeffect, driving all stakeholders toward taking the evolu-tionary steps necessary for successful operation in theoverhauled healthcare delivery system of tomorrow. �
References1. Congressional Budget Office. Letter to Nancy Pelosi. March 20, 2010. www.cbo.gov/ftpdocs/113xx/doc11379/AmendReconProp.pdf. Accessed June 30, 2010.2. PriceWaterhouseCoopers’ Health Research Institute. Health Reform: Prosperingin a Post-reform World. May 2010. http://pwchealth.com/cgi-local/hcregister.cgi?link=reg/prospering-in-a-post-reform-world.pdf. Accessed June 30, 2010.3. Office of Attorney General Martha Coakley, Examination of Health Care CostTrends and Cost Drivers. March 16, 2010. www.mass.gov/Cago/docs/healthcare/final_report_w_cover_appendices_glossary.pdf. Accessed June 30, 2010.
Request your FREE SUBSCRIPTION toAme Ric An He Al t H & DRu g Be n e f it s ®
Please provide all information indicated, including date and signature. INCOMPLETE CARDS WILL NOT BE PROCESSED.
❑ YES! I would like to receive American Health & Drug Benefits® as well as related educational supplements FREE!❑ NO. Please discontinue my subscription.
Signature (Required) Specialty
Date (Required) Address
Name City/State/ZIP
Company E-mail
Title Phone
Fax to: 732.992.1881


INDUSTRY TRENDS
292 American Health & Drug Benefits l www.AHDBonline.com July/August 2010 l Vol 3, No 4
Much attention is now focused on bundled pay-ment as a promising mechanism of healthcarereform. Early signs point to the potential of this
initiative to reduce fragmentation in healthcare delivery,while improving quality and addressing spiraling costs.Bundled payment requires the involved parties to agreeon a defined package of care and services for a particularcondition; this treatment episode is then paid in a singlepayment that is apportioned among multiple providers(both professionals and facilities) across many settings.This bundled payment—or “episode-based payment”—is currently the subject of ongoing pilot projects acrossthe United States.
Payer and provider organizations can learn from theseexperiments as they shape their own programs and thenbring them to scale.
Successful Experiments One of the earliest experiments in bundled payment
began with a Medicare pilot program in the early 1990sfor a handful of surgical procedures. Within the nextdecade, global payments became more widely used forcertain procedures; obstetrics may be the best-known,with a single payment for prenatal and postdelivery pro-fessional services and often a separate diagnosis-relatedgroup payment to the hospital for facility services.
Episode-based payment expands the scope of globalpayment into a single payment shared by multipleproviders as a means to encourage care coordination.Several successful experiments have been seen primarilyin staff models or integrated healthcare settings.
Geisinger’s ProvenCare. The most notable exampleis the ProvenCare program at Geisinger Health Systemin Pennsylvania, which accepts a single payment forseveral procedures, including elective coronary arterybypass graft (CABG), percutaneous transluminal coro-nary angioplasty, total hip replacement, cataract surgery,and low back pain treatment.1 Using evidence-basedmedicine and other input from professional associa-tions, Geisinger defined critical patient care steps thatmust be accomplished in each clearly defined bundle.1,2To ensure quality, physician payment may be tied, inpart, to adherence to process-of-care performance meas-ures.3 Results at Geisinger have included reduced
lengths of stay, lower readmission rates, and outcomesthat exceed national averages.1
Medicare. Recently, the Centers for Medicare &Medicaid Services launched the Acute Care EpisodeDemonstration project at 5 sites in 4 states to test bun-dled payments for Medicare Part A (for inpatient hospi-tal care, skilled nursing care, and hospice care) andMedicare Part B (includes doctors’ fees and outpatienthospital visits) for 9 orthopedic and 28 cardiac inpatientsurgical services and procedures. A portion of the cost-savings is designated to be shared with Medicare benefi-ciaries. Results are expected after 2013.4
Prometheus. The Prometheus Payment model, spon-sored largely by the Robert Wood Johnson Foundation,is the subject of ongoing pilot projects. The model takesinto account 3 components in determining payment5:• Evidence-informed base payment• Patient-specific severity adjustment• Allowance for “potentially avoidable complications.”
This last element is essential in most current bundledpayment scenarios. If complications are avoided, theproviders may be paid more than they would havereceived under conventional fee-for-service, with theultimate aim of reducing complications and overall cost.Although this retrospective approach limits the oppor-tunity to influence provider behavior, the Prometheusmodel continues to provide an important example asexperiments in bundled payment move forward.
Lessons from Early Initiatives: Payer-ProviderCollaboration, and Transparency
A key lesson learned from these early initiatives isthat clinicians must play a leading role in decision-mak-ing—physicians need to be involved in defining thebundle, in managing care, and in defining the responsi-bility of each provider involved.
Transparency is also critical. This requires a funda-mental cultural shift away from adversarial relationshipsbetween payers and providers. Bundled payments shouldrepresent a true alignment of incentives among thepayer, provider, and the patient. All providers andpatients must have access to what they can expect witha bundled payment, what the bundle includes andexcludes, who the participants are, and how it all works.
The Current State of BundledPaymentsJim EvansVice President, McKesson Health Solutions

INDUSTRY TRENDS
293www.AHDBonline.com l American Health & Drug BenefitsVol 3, No 4 l July/August 2010
Everyone needs to know what they stand to gainthrough better coordination and quality of care.
To recruit members, plans may need to remind themthat providers involved in any bundled payment initia-tive typically are those who meet quality standards andare committed to working collaboratively to achieve thebest patient outcomes. Patients also may be expected toplay a role, as they do in the Geisinger program, by sign-ing a “patient compact” that they will comply with carerecommendations.
Tools and Processes Require Automation Most experiments in bundled payments thus far have
occurred in staff model organizations (in which thephysicians work for the organization), prompting thequestions of how and whether these successes can beadapted in more open networks. The answer lies inautomation, which can create a virtual system to achievesimilar results. Automation will be essential to bring toscale the experiments that now rely on manual process-es during their pilot phases.
Contract management, claim processing, and wasteand abuse functions must be integrated to support newpayment frameworks. This requires:• Episodes of care that are defined in such a way that
logic can be built and applied in an automated fashion• Dynamic contracting that incorporates episodes of
care terms and definitions• Systems that automatically convert contract terms to
terms in the payment system• Claims processing technology that can look across
facility and professional claims, and across time, toassociate all services that should be included orexcluded as part of an episode of care; slow responsemay result in inappropriate payment, which couldjeopardize payer confidence
• Autoadjudication of complex contracts with multiplepayment arrangements
• The ability to apply clinical knowledge to claim pay-ment decisions so that payments will be defensible toproviders
• Waste and abuse systems that can detect new means ofinappropriate optimization of payment that mayspring up in response to a new payment model
• Interoperability between payment and quality data• Systems with the flexibility to adapt as new payment
mechanisms evolve• Transparency among all stakeholders.
Time Is Ripe to Start a Pilot Project A good starting point for organizations that wish to
design a bundled payment project is to focus on whatyou, or your providers, do best, and to create partner-ships with those providers. Hospitals are probably inthe best position to spearhead quality improvementsaround bundled payments by creating incentives forcare coordination.
The areas that are well-suited for initial ventures intobundled payment are high-complexity procedures thatare common, well-defined, and have a clear standard ofcare, such as joint replacement, CABG, and therapeuticcardiac catheterization. Measurable quality goals, such asshorter hospital stays or length of time to ambulation,should be in place from the outset. The ultimate focusshould always be on the delivery of quality care. Anadditional, intriguing way to look at success would bewhether claim appeals decrease.
Although government programs are investigatinghow to integrate bundled payment into Medicare, theindustry does not need to stand by and wait for thoseresults. Collaboration among payers, providers, andpatients will bring them closer to their shared goals ofreducing cost and improving quality. Organizations thatwork collaboratively to innovate, and have the tools todo so, will lead the way. ■
References1. Geisinger Health System. About ProvenCare. www.geisinger.org/provencare/.Accessed July 8, 2010.2. Agency for Healthcare Research and Quality. Innovation profile: use of clinical“bundles,” fixed pricing, and patient compact enhances adherence with guidelinesand improves outcomes in bypass surgery, diabetes, and other areas. May 25, 2009.www.innovations.ahrq.gov/content.aspx?id=2373. Accessed July 8, 2010.3. Casale AS, Paulus RA, Selna MJ, et al. “ProvenCareSM”: a provider-driven pay-for-performance program for acute episodic cardiac surgical care. Ann Surg. 2007;246:613-621.4. Centers for Medicare & Medicaid Services. Medicare news: CMS announcessites for a demonstration to encourage greater collaboration and improve qualityusing bundled hospital payments. January 6, 2009. www.cms.gov/DemoProjectsEvalRpts/downloads/ACEPressRelease.pdf. Accessed July 8, 2010.5. de Brantes F, Rosenthal MB, Painter M. Building a bridge from fragmentation toaccountability—the Prometheus Payment model. N Engl J Med. 2009;361:1033-1036. Epub 2009 Aug 19.
Check out our updated user-friendly websiteEnhanced search capabilities • Full text & PDFs for all articles • Weekly web exclusives
www.AHDBonline.com

Victoza® (liraglutide [rDNA origin] injection)Rx onlyBRIEF SUMMARY. Please consult package insert for full prescribing information.
WARNING: RISK OF THYROID C-CELL TUMORS: Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice. It is unknown whether Victoza® causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans, as human relevance could not be ruled out by clinical or nonclinical studies. Victoza® is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Based on the findings in rodents, monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials, but this may have increased the number of unnecessary thyroid surgeries. It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors. Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions].
INDICATIONS AND USAGE: Victoza® is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus. Important Limitations of Use: Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans, pre-scribe Victoza® only to patients for whom the potential benefits are considered to outweigh the potential risk. Victoza® is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise. In clinical trials of Victoza®, there were more cases of pancreatitis with Victoza® than with comparators. Victoza® has not been studied sufficiently in patients with a history of pancreatitis to determine whether these patients are at increased risk for pancreatitis while using Victoza®. Use with caution in patients with a history of pancreatitis. Victoza® is not a substitute for insulin. Victoza® should not be used in patients with type 1 dia-betes mellitus or for the treatment of diabetic ketoacidosis, as it would not be effective in these settings. The concurrent use of Victoza® and insulin has not been studied.CONTRAINDICATIONS: Victoza® is contraindicated in patients with a personal or family history of medullary thyroid carcinoma (MTC) or in patients with Multiple Endocrine Neoplasia syn-drome type 2 (MEN 2).WARNINGS AND PRECAUTIONS: Risk of Thyroid C-cell Tumors: Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas and/or carcinomas) at clinically relevant exposures in both genders of rats and mice. Malignant thyroid C-cell carcinomas were detected in rats and mice. A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls. It is unknown whether Victoza® will cause thyroid C-cell tumors, including medullary thyroid car-cinoma (MTC), in humans, as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies [see Boxed Warning, Contra-indications]. In the clinical trials, there have been 4 reported cases of thyroid C-cell hyperplasia among Victoza®-treated patients and 1 case in a comparator-treated patient (1.3 vs. 0.6 cases per 1000 patient-years). One additional case of thyroid C-cell hyperplasia in a Victoza®-treated patient and 1 case of MTC in a comparator-treated patient have subsequently been reported. This comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations >1000 ng/L suggesting pre-existing disease. All of these cases were diagnosed after thyroidectomy, which was prompted by abnormal results on routine, protocol-specified measurements of serum calcitonin. Four of the five liraglutide-treated patients had elevated calcitonin concentrations at baseline and throughout the trial. One liraglutide and one non-liraglutide-treated patient devel-oped elevated calcitonin concentrations while on treatment. Calcitonin, a biological marker of MTC, was measured throughout the clinical development program. The serum calcitonin assay used in the Victoza® clinical trials had a lower limit of quantification (LLOQ) of 0.7 ng/L and the upper limit of the reference range was 5.0 ng/L for women and 8.4 ng/L for men. At Weeks 26 and 52 in the clinical trials, adjusted mean serum calcitonin concentrations were higher in Victoza®-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator. At these timepoints, the adjusted mean serum calcitonin values (~ 1.0 ng/L) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 0.1 ng/L or less. Among patients with pre-treatment serum calcitonin below the upper limit of the reference range, shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victoza® 1.8 mg/day. In trials with on-treatment serum calcitonin measurements out to 5-6 months, 1.9% of patients treated with Victoza® 1.8 mg/day developed new and persistent calci-tonin elevations above the upper limit of the reference range compared to 0.8-1.1% of patients treated with control medication or the 0.6 and 1.2 mg doses of Victoza®. In trials with on-treat-ment serum calcitonin measurements out to 12 months, 1.3% of patients treated with Victoza® 1.8 mg/day had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range, compared to 0.6%, 0% and 1.0% of patients treated with Victoza® 1.2 mg, placebo and active control, respectively. Otherwise, Victoza® did not produce consistent dose-dependent or time-dependent increases in serum calcitonin. Patients with MTC usually have calcitonin values >50 ng/L. In Victoza® clinical trials, among patients with pre-treatment serum calcitonin <50 ng/L, one Victoza®-treated patient and no comparator-treated patients developed serum calcitonin >50 ng/L. The Victoza®-treated patient who developed serum calcitonin >50 ng/L had an elevated pre-treatment serum calcitonin of 10.7 ng/L that increased to 30.7 ng/L at Week 12 and 53.5 ng/L at the end of the 6-month trial. Follow-up serum calci-tonin was 22.3 ng/L more than 2.5 years after the last dose of Victoza®. The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 19.3 ng/L at baseline to 44.8 ng/L at Week 65 and 38.1 ng/L at Week 104. Among patients who began with serum calcitonin <20 ng/L, calcitonin elevations to >20 ng/L occurred in 0.7% of Victoza®-treated patients, 0.3% of placebo-treated patients, and 0.5% of active-comparator-treated patients, with an incidence of 1.1% among patients treated with 1.8 mg/day of Victoza®. The clinical significance of these findings is unknown. Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (e.g. a mass in the neck, dysphagia, dyspnea or persistent hoarseness). It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC, and such monitoring may increase the risk of unnecessary procedures, due to low test specificity for serum calcitonin and a high background incidence of thyroid disease. Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinolo-gist for further evaluation. Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victoza®, if serum calcitonin is measured and found to be elevated, the patient should be referred to an endocrinologist for further evaluation. Pancreatitis: In clinical
trials of Victoza®, there were 7 cases of pancreatitis among Victoza®-treated patients and 1 case among comparator-treated patients (2.2 vs. 0.6 cases per 1000 patient-years). Five cases with Victoza® were reported as acute pancreatitis and two cases with Victoza® were reported as chronic pancreatitis. In one case in a Victoza®-treated patient, pancreatitis, with necrosis, was observed and led to death; however clinical causality could not be established. One additional case of pan-creatitis has subsequently been reported in a Victoza®-treated patient. Some patients had other risk factors for pancreatitis, such as a history of cholelithiasis or alcohol abuse. There are no con-clusive data establishing a risk of pancreatitis with Victoza® treatment. After initiation of Victoza®, and after dose increases, observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain, sometimes radiating to the back and which may or may not be accompanied by vomiting). If pancreatitis is suspected, Victoza® and other potentially suspect medications should be discontinued promptly, confirmatory tests should be performed and appropriate management should be initiated. If pancreatitis is confirmed, Victoza® should not be restarted. Use with caution in patients with a history of pancreatitis. Use with Medications Known to Cause Hypoglycemia: Patients receiving Victoza® in combination with an insulin secretagogue (e.g., sulfonylurea) may have an increased risk of hypoglycemia. In the clinical trials of at least 26 weeks duration, hypoglycemia requiring the assistance of another person for treat-ment occurred in 7 Victoza®-treated patients and in no comparator-treated patients. Six of these 7 patients treated with Victoza® were also taking a sulfonylurea. The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea or other insulin secretagogues [see Adverse Reactions]. Macrovascular Outcomes: There have been no clinical studies establishing con-clusive evidence of macrovascular risk reduction with Victoza® or any other antidiabetic drug.ADVERSE REACTIONS: Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. The safety of Victoza® was evaluated in a 52-week monotherapy trial and in four 26-week, add-on combination therapy trials. In the monotherapy trial, patients were treated with Victoza® 1.2 mg daily, Victoza® 1.8 mg daily, or glimepiride 8 mg daily. In the add-on to metformin trial, patients were treated with Victoza® 0.6 mg, Victoza® 1.2 mg, Victoza® 1.8 mg, placebo, or glimepiride 4 mg. In the add-on to glimepiride trial, patients were treated with Victoza® 0.6 mg, Victoza® 1.2 mg, Victoza® 1.8 mg, placebo, or rosiglitazone 4 mg. In the add-on to metformin + glimepiride trial, patients were treated with Victoza® 1.8 mg, placebo, or insulin glargine. In the add-on to metformin + rosiglitazone trial, patients were treated with Victoza® 1.2 mg, Victoza® 1.8 mg or placebo. Withdrawals: The incidence of withdrawal due to adverse events was 7.8% for Victoza®-treated patients and 3.4% for comparator-treated patients in the five controlled trials of 26 weeks duration or longer. This difference was driven by withdrawals due to gastrointestinal adverse reactions, which occurred in 5.0% of Victoza®-treated patients and 0.5% of comparator-treated patients. The most common adverse reactions leading to withdrawal for Victoza®-treated patients were nausea (2.8% versus 0% for comparator) and vomiting (1.5% versus 0.1% for comparator). Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials. Tables 1 and 2 summarize the adverse events reported in ≥5% of Victoza®-treated patients in the five controlled trials of 26 weeks duration or longer.Table 1: Adverse events reported in ≥ 5% of Victoza®-treated patients or ≥5% of glimepiride-treated patients: 52-week monotherapy trial
All Victoza® N = 497 Glimepiride N = 248Adverse Event Term (%) (%)Nausea 28.4 8.5Diarrhea 17.1 8.9Vomiting 10.9 3.6Constipation 9.9 4.8Upper Respiratory Tract Infection 9.5 5.6Headache 9.1 9.3Influenza 7.4 3.6Urinary Tract Infection 6.0 4.0Dizziness 5.8 5.2Sinusitis 5.6 6.0Nasopharyngitis 5.2 5.2Back Pain 5.0 4.4Hypertension 3.0 6.0
Table 2: Adverse events reported in ≥ 5% of Victoza®-treated patients and occur-ring more frequently with Victoza® compared to placebo: 26-week combination therapy trials
Add-on to Metformin TrialAll Victoza® +
Metformin N = 724
Placebo + Metformin N = 121
Glimepiride + Metformin N = 242
Adverse Event Term (%) (%) (%)Nausea 15.2 4.1 3.3Diarrhea 10.9 4.1 3.7Headache 9.0 6.6 9.5Vomiting 6.5 0.8 0.4
Add-on to Glimepiride TrialAll Victoza® +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Event Term (%) (%) (%)Nausea 7.5 1.8 2.6Diarrhea 7.2 1.8 2.2Constipation 5.3 0.9 1.7Dyspepsia 5.2 0.9 2.6

Add-on to Metformin + GlimepirideVictoza® 1.8 + Metformin + Glimepiride
N =230
Placebo + Metformin + Glimepiride
N =114
Glargine + Metformin + Glimepiride
N =232
Adverse Event Term (%) (%) (%)Nausea 13.9 3.5 1.3Diarrhea 10.0 5.3 1.3Headache 9.6 7.9 5.6Dyspepsia 6.5 0.9 1.7Vomiting 6.5 3.5 0.4
Add-on to Metformin + RosiglitazoneAll Victoza® + Metformin +
Rosiglitazone N = 355Placebo + Metformin
+ Rosiglitazone N = 175Adverse Event Term (%) (%)Nausea 34.6 8.6Diarrhea 14.1 6.3Vomiting 12.4 2.9Decreased Appetite 9.3 1.1Anorexia 9.0 0.0Headache 8.2 4.6Constipation 5.1 1.1Fatigue 5.1 1.7
Gastrointestinal adverse events: In the five clinical trials of 26 weeks duration or longer, gastroin-testinal adverse events were reported in 41% of Victoza®-treated patients and were dose-related. Gastrointestinal adverse events occurred in 17% of comparator-treated patients. Events that occurred more commonly among Victoza®-treated patients included nausea, vomiting, diar-rhea, dyspepsia and constipation. In clinical trials of 26 weeks duration or longer, the percentage of patients who reported nausea declined over time. Approximately 13% of Victoza®-treated patients and 2% of comparator-treated patients reported nausea during the first 2 weeks of treat-ment. Immunogenicity: Consistent with the potentially immunogenic properties of protein and peptide pharmaceuticals, patients treated with Victoza® may develop anti-liraglutide antibodies. Approximately 50-70% of Victoza®-treated patients in the five clinical trials of 26 weeks dura-tion or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment. Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 8.6% of these Victoza®-treated patients. Sampling was not performed uniformly across all patients in the clinical trials, and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies. Cross-reacting anti-liraglutide antibod-ies to native glucagon-like peptide-1 (GLP-1) occurred in 6.9% of the Victoza®-treated patients in the 52-week monotherapy trial and in 4.8% of the Victoza®-treated patients in the 26-week add-on combination therapy trials. These cross-reacting antibodies were not tested for neutral-izing effect against native GLP-1, and thus the potential for clinically significant neutralization of native GLP-1 was not assessed. Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 2.3% of the Victoza®-treated patients in the 52-week monotherapy trial and in 1.0% of the Victoza®-treated patients in the 26-week add-on combination therapy trials. Among Victoza®-treated patients who developed anti-liraglutide antibodies, the most common category of adverse events was that of infections, which occurred among 40% of these patients compared to 36%, 34% and 35% of antibody-negative Victoza®-treated, placebo-treated and active-control-treated patients, respectively. The specific infections which occurred with greater frequency among Victoza®-treated antibody-positive patients were primarily nonserious upper respiratory tract infections, which occurred among 11% of Victoza®-treated antibody-positive patients; and among 7%, 7% and 5% of antibody-negative Victoza®-treated, placebo-treated and active-control-treated patients, respectively. Among Victoza®-treated antibody-negative patients, the most common category of adverse events was that of gastrointestinal events, which occurred in 43%, 18% and 19% of antibody-negative Victoza®-treated, placebo-treated and active-con-trol-treated patients, respectively. Antibody formation was not associated with reduced efficacy of Victoza® when comparing mean HbA1c of all antibody-positive and all antibody-negative patients. However, the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victoza® treatment. In clinical trials of Victoza®, events from a composite of adverse events potentially related to immunogenicity (e.g. urticaria, angioedema) occurred among 0.8% of Victoza®-treated patients and among 0.4% of comparator-treated patients. Urticaria accounted for approximately one-half of the events in this composite for Victoza®-treated patients. Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immu-nogenicity events composite than were patients who did not develop anti-liraglutide antibodies. Injection site reactions: Injection site reactions (e.g., injection site rash, erythema) were reported in approximately 2% of Victoza®-treated patients in the five clinical trials of at least 26 weeks duration. Less than 0.2% of Victoza®-treated patients discontinued due to injection site reactions. Papillary thyroid carcinoma: In clinical trials of Victoza®, there were 6 reported cases of papillary thyroid carcinoma in patients treated with Victoza® and 1 case in a comparator-treated patient (1.9 vs. 0.6 cases per 1000 patient-years). Most of these papillary thyroid carcinomas were <1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultra-sound. Hypoglycemia: In the clinical trials of at least 26 weeks duration, hypoglycemia requiring the assistance of another person for treatment occurred in 7 Victoza®-treated patients (2.6 cases per 1000 patient-years) and in no comparator-treated patients. Six of these 7 patients treated
with Victoza® were also taking a sulfonylurea. One other patient was taking Victoza® in combina-tion with metformin but had another likely explanation for the hypoglycemia (this event occurred during hospitalization and after insulin infusion) (Table 3). Two additional cases of hypoglyce-mia requiring the assistance of another person for treatment have subsequently been reported in patients who were not taking a concomitant sulfonylurea. Both patients were receiving Victoza®, one as monotherapy and the other in combination with metformin. Both patients had another likely explanation for the hypoglycemia (one received insulin during a frequently-sampled intra-venous glucose tolerance test, and the other had intracranial hemorrhage and uncertain food intake).Table 3: Incidence (%) and Rate (episodes/patient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victoza® Treatment
Active Comparator
Placebo Comparator
Monotherapy Victoza®
(N = 497)Glimepiride
(N = 248)None
Patient not able to self−treat 0 0 —Patient able to self−treat 9.7 (0.24) 25.0 (1.66) —Not classified 1.2 (0.03) 2.4 (0.04) —Add-on to Metformin
Victoza® + Metformin (N = 724)
Glimepiride + Metformin (N = 242)
Placebo + Metformin (N = 121)
Patient not able to self−treat 0.1 (0.001) 0 0Patient able to self−treat 3.6 (0.05) 22.3 (0.87) 2.5 (0.06)Add-on to Glimepiride Victoza® +
Glimepiride (N = 695)
Rosiglitazone + Glimepiride
(N = 231)
Placebo + Glimepiride
(N = 114)Patient not able to self−treat 0.1 (0.003) 0 0Patient able to self−treat 7.5 (0.38) 4.3 (0.12) 2.6 (0.17)Not classified 0.9 (0.05) 0.9 (0.02) 0Add-on to Metformin + Rosiglitazone
Victoza® + Metformin +
Rosiglitazone (N = 355)
None
Placebo + Metformin +
Rosiglitazone (N = 175)
Patient not able to self−treat 0 — 0Patient able to self−treat 7.9 (0.49) — 4.6 (0.15)Not classified 0.6 (0.01) — 1.1 (0.03)Add-on to Metformin + Glimepiride
Victoza® + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin + Glimepiride
(N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self−treat 2.2 (0.06) 0 0Patient able to self−treat 27.4 (1.16) 28.9 (1.29) 16.7 (0.95)Not classified 0 1.7 (0.04) 0
In a pooled analysis of clinical trials, the incidence rate (per 1,000 patient-years) for malig-nant neoplasms (based on investigator-reported events, medical history, pathology reports, and surgical reports from both blinded and open-label study periods) was 10.9 for Victoza®, 6.3 for placebo, and 7.2 for active comparator. After excluding papillary thyroid carcinoma events [see Adverse Reactions], no particular cancer cell type predominated. Seven malignant neoplasm events were reported beyond 1 year of exposure to study medication, six events among Victoza®-treated patients (4 colon, 1 prostate and 1 nasopharyngeal), no events with placebo and one event with active comparator (colon). Causality has not been established. Laboratory Tests: In the five clinical trials of at least 26 weeks duration, mildly elevated serum bilirubin concentra-tions (elevations to no more than twice the upper limit of the reference range) occurred in 4.0% of Victoza®-treated patients, 2.1% of placebo-treated patients and 3.5% of active-comparator-treated patients. This finding was not accompanied by abnormalities in other liver tests. The significance of this isolated finding is unknown.OVERDOSAGE: In a clinical trial, one patient with type 2 diabetes experienced a single overdose of Victoza® 17.4 mg subcutaneous (10 times the maximum recommended dose). Effects of the overdose included severe nausea and vomiting requiring hospitalization. No hypoglycemia was reported. The patient recovered without complications. In the event of overdosage, appropriate supportive treatment should be initiated according to the patient’s clinical signs and symptoms.More detailed information is available on request. For information about Victoza® contact: Novo Nordisk Inc., 100 College Road West, Princeton, New Jersey 08540, 1−877-484-2869Date of Issue: January 2010 Version: 1Manufactured by: Novo Nordisk A/S, DK-2880 Bagsvaerd, DenmarkVictoza® is a registered trademark of Novo Nordisk A/S. Victoza® is covered by US Patent Nos. 6,268,343; 6,458,924; and 7,235,627 and other patents pending. Victoza® Pen is covered by US Patent Nos. 6,004,297; 6,235,004; 6,582,404 and other patents pending.© 2010 Novo Nordisk A/S 140586-R1 4/2010

© 2010 Novo Nordisk A/S 141395 May 2010
Victoza® is a registered trademark of Novo Nordisk A/S.
Visit VictozaPro.com to learn more.
Targets beta cells
Provides powerful andsustained reductions in A1C*
Can provide the additional benefi t of weight loss
Safety and tolerability were studied in clinical trials that included nearly 4000 patients
Victoza® is not indicated for the management of obesity, and weight change was a secondary end point in clinical trials.
Once-daily Victoza®:
Indications and usageVictoza® is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus. Because of the uncertain relevance of the rodent thyroid C-cell tumor fi ndings to humans, prescribe Victoza® only to patients for whom the potential benefi ts are considered to outweigh the potential risk. Victoza® is not recommended as fi rst-line therapy for patients who have inadequate glycemic control on diet and exercise. In clinical trials of Victoza®, there were more cases of pancreatitis with Victoza® than with comparators. Victoza® has not been studied suffi ciently in patients with a history of pancreatitis to determine whether these patients are at increased risk for pancreatitis while using Victoza®. Use with caution in patients with a history of pancreatitis. Victoza® is not a substitute for insulin. Victoza® should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis, as it would not be effective in these settings. The concurrent use of Victoza® and insulin has not been studied.
Important safety informationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice. It is unknown whether Victoza® causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans, as human relevance could not be ruled out by clinical or nonclinical studies. Victoza® is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Based on the fi ndings in rodents, monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials, but this may have increased the number of unnecessary thyroid surgeries. It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors. Patients should be counseled regarding the risk and symptoms of thyroid tumors.
If pancreatitis is suspected, Victoza® should be discontinued. Victoza® should not be re-initiated if pancreatitis is confi rmed. When Victoza® is used with an insulin secretagogue (e.g. a sulfonylurea) serious hypoglycemia can occur. Consider lowering the dose of the insulin secretagogue to reduce the risk of hypoglycemia. There have been no studies establishing conclusive evidence of macrovascular risk reduction with Victoza® or any other antidiabetic drug. The most common adverse reactions, reported in ≥5% of patients treated with Victoza® and more commonly than in patients treated with placebo, are headache, nausea, diarrhea, and anti-liraglutide antibody formation. Immunogenicity-related events, including urticaria, were more common among Victoza®-treated patients (0.8%) than among comparator-treated patients (0.4%) in clinical trials. Victoza® has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patients. Victoza® should be used with caution in patients with renal impairment and in patients with hepatic impairment.
Please see brief summary of Prescribing Information on adjacent page.
* Victoza® was evaluated in a 52-week monotherapy trial and in four 26-week, add-on combination trials.
11:24 AM