Journal, Second-degree Wenckebach type block to block ...The second-degree block in this case can...
10
British Heart Journal, I972, 34, II27-II36. Second-degree Wenckebach type AV block due to block within the atrium' Onkar S. Narula, Manfred Runge2, and Philip Samet From the Division of Cardiology, Department of Internal Medicine, Mount Sinai Hospital of Greater Miami, Miami Beach, Florida, and the University of Miami, School of Medicine, Miami, Florida, U.S.A. Two patients with a history of paroxysmal supraventricular tachycardia were analysed by His bundle and intra-atrial recordings. The electrocardiogram showed sinus bradycardia in I patient and sinus bradycardia with sino-atrial Wenckebach in the other. The conduction times through the A V node and His Purkinje system were normal in both cases. The intra-atrial conduction time was slightly prolonged (55 msec) in one and normal (40 msec) in the other during normal sinus rhythm. In both cases with atrial pacing from high right atrium, the conduction time from the pacing impulse (PI) to atrial activation in the area of the A Vjunction (PI-A) progressively lengthened with increase in atrial pacing rate and finally classical second-degree Wenckebach type of block was manifested at cycle lengths of 460 and 465 msec. The pacing impulse to QRS interval (PI-R) showed a progressive increase before the blocked stimulus. The lengthening of the PI-R interval was due to progressive increase in the intra-atrial (PI-A) conduction time. In the dropped beats, the pacing impulse was notfollowed by an A deflection. This observation indicated Type I block within the atrium. Similarly, during induced premature atrial beats, the PI-A time progressively lengthened as the coupling interval was shortened. These findings were reproducible and were seen despite a fourfold increase in stimulus strength and changes in electrodes and site of stimulation along the lateral right atrial border. This study (I) shows second-degree Wenckebach block within the atrium; (2) supports the existence of sinoatrial Wenckebach; and (3) suggests the atrium as another possible site for re-entry and a cause for supraventricular tachycardia because of the degree of delay and block exhibited within the atrium. It is well known that block during impulse transmission may occur at any site where a difference in functional refractory period is present or where decremental conduction occurs (Hoffman and Cranefield, I960; Cranefield, Hoffnan, and de Carvalho, 1959; Cranefield, Klein, and HofEnan, I971; Singer, Lazzara, and Hoffman, I967). Mobitz (I924) first defined the electrocardiographic criteria for the two types of second-degree atrioventricular (AV) block (Type I and II). The Type II block, commonly known as Mobitz II, has been clinically and experi- mentally localized to the His-Purkinje system (Donoso, Adler, and Friedberg, I964; Kauf- man et al., I96I; Watanabe and Dreifus, Received 28 February I972. 1 This report was presented at the 2Ist Annual Scien- tific Session of the American College of Cardiology, I-5 March I972, Chicago, Illinois. 2 Present address: First Medical Clinic, University of Hamburg, Hamburg 20, West Germany. I967; Narula and Samet, I970). In contrast, Wenckebach type (Mobitz I) of AV block is generally considered to occur in the AV node. Recent reports have also shown that the Wenckebach type of block may be ob- served within the His bundle and bundle- branches (Narula and Samet, I970; Puech et al., 1970). Intra-atrial conduction defects have been known to cause first-degree AV block (Katz and Pick, I956; Narula et al., 197I). Though second-degree block within the atrium has been previously proposed, it has not been documented (Phibbs, I963). The purpose of this study is to present the electrophysiological data in 2 patients who manifested the typical Wenckebach AV block secondary to blocked P waves within the atrium itself, i.e. proximal to the AV node. It is also shown that in these 2 cases, the intra-atrial conduction time was rate-depen- dent and progressively increased with in- crease in rate. The evidence further shows on January 31, 2021 by guest. Protected by copyright. http://heart.bmj.com/ Br Heart J: first published as 10.1136/hrt.34.11.1127 on 1 November 1972. Downloaded from
Transcript of Journal, Second-degree Wenckebach type block to block ...The second-degree block in this case can...

British Heart Journal, I972, 34, II27-II36.
Second-degree Wenckebach type AV block dueto block within the atrium'
Onkar S. Narula, Manfred Runge2, and Philip SametFrom the Division of Cardiology, Department of Internal Medicine,Mount Sinai Hospital of Greater Miami, Miami Beach, Florida, andthe University of Miami, School of Medicine, Miami, Florida, U.S.A.
Two patients with a history of paroxysmal supraventricular tachycardia were analysed by Hisbundle and intra-atrial recordings. The electrocardiogram showed sinus bradycardia in I patientand sinus bradycardia with sino-atrial Wenckebach in the other. The conduction times throughthe AV node and His Purkinje system were normal in both cases. The intra-atrial conductiontime was slightly prolonged (55 msec) in one and normal (40 msec) in the other during normalsinus rhythm. In both cases with atrial pacing from high right atrium, the conduction time fromthe pacing impulse (PI) to atrial activation in the area of the A Vjunction (PI-A) progressivelylengthened with increase in atrial pacing rate and finally classical second-degree Wenckebachtype of block was manifested at cycle lengths of 460 and 465 msec. The pacing impulse toQRS interval (PI-R) showed a progressive increase before the blocked stimulus. The lengtheningof the PI-R interval was due to progressive increase in the intra-atrial (PI-A) conductiontime. In the dropped beats, thepacing impulse was notfollowed by anA deflection. This observationindicated Type I block within the atrium. Similarly, during induced premature atrial beats, thePI-A time progressively lengthened as the coupling interval was shortened. These findings werereproducible and were seen despite a fourfold increase in stimulus strength and changes inelectrodes and site of stimulation along the lateral right atrial border. This study (I) showssecond-degree Wenckebach block within the atrium; (2) supports the existence of sinoatrialWenckebach; and (3) suggests the atrium as another possible site for re-entry and a cause forsupraventricular tachycardia because of the degree of delay and block exhibited within the atrium.
It is well known that block during impulsetransmission may occur at any site where adifference in functional refractory period ispresent or where decremental conductionoccurs (Hoffman and Cranefield, I960;Cranefield, Hoffnan, and de Carvalho, 1959;Cranefield, Klein, and HofEnan, I971;Singer, Lazzara, and Hoffman, I967). Mobitz(I924) first defined the electrocardiographiccriteria for the two types of second-degreeatrioventricular (AV) block (Type I and II).The Type II block, commonly known asMobitz II, has been clinically and experi-mentally localized to the His-Purkinje system(Donoso, Adler, and Friedberg, I964; Kauf-man et al., I96I; Watanabe and Dreifus,
Received 28 February I972.1 This report was presented at the 2Ist Annual Scien-tific Session of the American College of Cardiology,I-5 March I972, Chicago, Illinois.2 Present address: First Medical Clinic, University ofHamburg, Hamburg 20, West Germany.
I967; Narula and Samet, I970). In contrast,Wenckebach type (Mobitz I) of AV block isgenerally considered to occur in the AVnode. Recent reports have also shown thatthe Wenckebach type of block may be ob-served within the His bundle and bundle-branches (Narula and Samet, I970; Puechet al., 1970). Intra-atrial conduction defectshave been known to cause first-degree AVblock (Katz and Pick, I956; Narula et al.,197I). Though second-degree block withinthe atrium has been previously proposed, ithas not been documented (Phibbs, I963).The purpose of this study is to present the
electrophysiological data in 2 patients whomanifested the typical Wenckebach AV blocksecondary to blocked P waves within theatrium itself, i.e. proximal to the AV node.It is also shown that in these 2 cases, theintra-atrial conduction time was rate-depen-dent and progressively increased with in-crease in rate. The evidence further shows
on January 31, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.11.1127 on 1 N
ovember 1972. D
ownloaded from

II28 Narula, Runge, and Samet
some of the potential inherent fallacies ofarrhythmia interpretations based solely onthe duration of the PR interval in the surfaceelectrocardiogram.
Case reportsCase I A 69-year-old white woman was ad-mitted because of tachycardia. At the age of 17,she was told she had a heart murmur. Episodesof palpitations, first noted at age 52, were con-trolled by quinidine administration. Digoxin(0-25 mg daily) was started at 6i because ofexertional dyspnoea. Three weeks before admis-sion, she stopped digitalis and quinidine therapy,whereupon recurrent tachycardias developed.On examination, she exhibited the typical find-ings of mitral insufficiency and stenosis. X-rayexamination revealed cardiomegaly with leftatrial enlargement and calcified mitral valveleaflets. The clinical impression was rheumaticheart disease, cardiomegaly, mitral stenosis andinsufficiency, pulmonary hypertension, and par-oxysmal supraventricular tachycardia, Class II-C.The electrocardiogram on admission (Fig. I,
20 April I971) showed supraventricular tachy-cardia (probably atrial tachycardia with 2: I AVblock) with a ventricular rate of I I5 a minute. TheQRS complex was o0og sec in duration with a
normal axis. The next day, the ventricular ratewas 95 a minute after digitalis therapy. Two daysafter admission, an electrocardiogram revealedsinus bradycardia (45 a minute). The PR inter-val was o-i8 sec and the QRS complex remainedunchanged (Fig. I, 22 April 197I).On the sixth hospital day, a cardiac conduction
study was performed to help guide future drugor possible pacing therapy. His bundle recordingsand sinus node recovery time were obtained asdescribed previously (Narula et al., 1970; Narula,Samet, and Javier, 1972). During the study, thesinus cycle length ranged from I250 to I400msec. The PR interval was I75 msec. The con-trol conduction times through the AV node(A-H) and His Purkinje system were 75 and 45msec, respectively. The conduction time throughthe atrium was slightly prolonged (55 msec) andsuggested intra-atrial conduction delay. This wasfurther confirmed during induced premature atrialbeats and atrial pacing with 2 msec pulse dura-tion. During premature atrial beats, the con-duction time from the pacing impulse in the highright atrium to atrial (A2) activation in the areaof the AV junction progressively lengthened(from go to i6o msec) with increase in prematurityof the premature atrial beats (Fig. 2, Panel A toD). The absolute atrial refractory period, asmeasured by induced premature atrial beats atdouble the diastolic threshold was 425 msec(Fig. 2, Panel E).
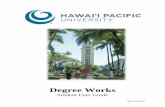
FIG. I Case i. Rhythm strip (20 April 1971) shows supraventricular tachycardia which isfollowed by normal sinus rhythm 2 days later (22 April 197I). The I2 standard electrocardiogramleads are shown below.
4/20/71
-.. ..- lI l..~~~~~~~~~~~...-. l 'L-3 ...lj;lll ll;l B||l;4
_~ ~ ~ ~ ~~ ~. .. ... .. ... .. ....._-.
4/22/711- t1'0 1 1 - ' 1 1 1 1 1 - 1'1 11-~~~~~~~~~~~~~....01'1.11:-'1:'1'1':'1'.'1'11'1'1 1'1: .1''1'''1-1'1.'11''.1.'1.'- 1'1 11.'..1.' ILlblA;~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. ..
.. . s l l l l ! - W : 1
L-3L--Llil~~~~~~~~~~~..4;Xlt lll111 111IWL
L-1~~~~~~~~~~~~~~~~~~~~~~ ~~~ ~~~~~~~~~~~~~~~~~~~~~~~~~L-2L-3:aVR aVL:aV , v
b
on January 31, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.11.1127 on 1 N
ovember 1972. D
ownloaded from

Second-degree Wenckebach type AV block due to block within the atrium 1129
Al ~:..!
A-A 1435 msec 1230 p1A2?.l.l--e
A IV A1410 S;H; 840 tpi
;1 1Al.Pt740 msecPl 0C2I1.ms*c
A.A 1350 msec Al ) 625 t1.
i1 IJAl-Pt 1130 msecPt-A2 100 misc
1460
A3I .1
A31490 .
mAi:t
-*'ri 01Ai.r;Ii465 mselcPt-A2 160 ms.c 1
;' 1Al AlI Al51270 Pi 1260 J /i1505
Al-Pi 425mse l.1I
FI G. 2 Case i. Effect of prematuirity ofpremature atrial beats on the pacing impulse (PI) toatrial (A) activation (PI-A) time. (A-D) Simultaneous bipolar (BE) recordingsfrom the area ofthe AVjunction (BH) with standard electrocardiogram lead I. During induced premature atrialbeats, as the coupling interval (Ai-PI) was shortenedfroM 1220 to 465 msec, the PI topremature atrial activation (A2) in the area of the AVjunction (PI-A2) time progressivelylengthened from 90 msec (Panel A) to i6o msec (Panel D). (E) A more premature stimulus (PI)at a coupling interval (AI-PI) of 425 msec showed absolute refractoriness of the atrium.A = Atrial electrogram during normal sinus rhythm. A2 = Atrial electrogram during inducedpremature atrial beats. BH= Bipolar His bundle electrogram. V= Ventricular activation recordedfrom the area of the AV junction. Time lines in this and subsequent Figures= sec.
During atrial pacing, the PR interval progres-sively lengthened with increase in rate (cyclelength from 1000 to 530 msec) (Fig. 3). The latterPR interval prolongation was caused by alengthening of the pacing impulse-atrial (PI-A)time (from II0 to I8o msec) in addition to the in-crease in AH time. With further increase in atrialpacing rate (cycle length of465 msec), Wenckebachtype second-degree AV block was manifestedwithin the atrium with an increase in pacingimpulse-atrial time until finally the atrial com-
plex was blocked and the pacing impulse (PI) wasnot followed by an A wave (Fig. 4). The lengthen-ing of the pacing impulse-atrial time was not pro-gressive though it increased from I05 to 330msec preceding the dropped beat. The AHinterval also exhibited an incomplete atypicalWenckebach phenomenon at the latter atrialpacing cycle length (465 msec). The Wencke-bach cycle in the AH interval was not complete(with a blocked P wave in the AV node) becausethe simultaneous occurrence of Wenckebach
L-1
B
I
C
D
EfW.tI
%!
n;-rr f
on January 31, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.11.1127 on 1 N
ovember 1972. D
ownloaded from

1130 Narula, Runge, and Samet
BE(BH)
L-1
aVF
VI
AP Cycle Length = 1000 msec
I IL.Al A VI1&'"I
rig AS. i I A.L. ' t L.110 PI.A 110 os c 110 110;
AP Cycle Length = 615 msec
X,\Lo1, *,41, 1 g.1.L I h.^~~~~~~~~~~~~~lo130 1 P1-A 130 ms.cs 1301
1l-~.-J
AP Cycle Length = 530 msec
ti ii IiUL. .-- U
(BH) l I
L-1CaCovf__ I-T-
.A 1 Al Vl I
),.A 180 msec 170
,fyOn A-
A 1 !
1.SC IpI I
i I Al1
F-1"I Ig
FIG . 3 Case i. Effect of increase in atrial pacing rate on PI-A time. The right atrium wasstimulated from the same site (high RA) as in Fig. 2. (A) Simultaneous recordings of BE(BH)with 3 standard electrocardiogram leads (I, aVF, Vi). The PI-A time was 1IO msec. (B-C)With progressive increase in atrial pacing rate (cycle length shortened to 530 msec), the PI-Atime progressively lengthened from IIO msec (Panel A) to I8o msec (Panel C) and contributed tothe lengthening of the PI-R interval. The PI-A time varies slightly in Panel C.
periods within the atrium resulted in a transientincrease in AA interval (slowing of atrial rate),and hence a transient decrease in AH conductiontime. This case shows simultaneously two sitesofWenckebach block, i.e. incomplete Wenckebachin the AV node and complete Wenckebach withinthe atrium. It is of interest that the- surfaceelectrocardiogram does not show obvious droppedbeats but simulates uninterrupted i: i AV con-duction because of these two simultaneous sitesof second-degree Wenckebach type of AV block(Fig. 4, Panel B). The second-degree block inthis case can only be diagnosed on the basis ofthe intracardiac recordings.The sinus node recovery time was measured
as described previously and was conspicuouslyprolonged (22oo msec+sinus cycle length). This
observation suggested a sick sinus node (Narulaet al., I972). During ventricular pacing, retro-grade conduction to the atrium was absent.
Case 2 A 73-year-old white woman was ad-mitted because of a 2-year history of frequentpalpitations despite quinidine administration butwithout digitalis. She was a known diabetic forthe last I3 years and was well controlled with 32units of Lente insulin daily. On examination,slight cardiomegaly and an atrial gallop soundwere noted. She had discontinued quinidine I0days before admission.The electrocardiogram had shown sinus brady-
cardia with rates ranging from 48 to 55 a minutefor the past i8 months. The electrocardiogramrecorded on 28 July I97I (Fig. 5) was compatible
I R.Ie;i I ILA J
(MH) l130
L-1 -BaVF -y'
I, IJl
13_i_
T- 1. --
135 $
O-Ot
r- ~~-'
;I rut W-IA :1__l AIA- -- :%4=1110it',11011FA^ -.-0- --4 U64-moli- -4 ol1rO'VOOw,L; , , ~-7PO-IFT -!-r lRF
vI
RP
on January 31, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.11.1127 on 1 N
ovember 1972. D
ownloaded from

Second-degree Wenckebach type AV block due to block within the atrium II31
BE(BH)
VF
FIG. 4 Case I. During atrial pacing, second-degree Wenckebach type of block was localizedin the atrium. (A) Simultaneous recordings of BE(BH) with 3 standard electrocardiogram leads(I, aVF, VI). First 2 beats with normal sinus rhythm show normal PR (I75 msec), AH (75msec), and HV (45 msec) intervals. The PA time (55 msec) during normal sinus rhythm wasslightly prolonged. Latter half shows onset of atrial pacing at a cycle length of 545 msec. This isaccompanied by an increase in PI-R (230 to 335 msec), PI-A (IOO to 155 msec), and A-H(85 to 135 msec) intervals before stabilization of these periods. (B) With increase in atrial pacingrate (cycle length = 465 msec), Wenckebach type of second-degree intra-atrial block wasmanifested. There was a progressive increase in PI-R from 245 to 645 msec before a beat wasdropped (6th PI). The PI-A progressively lengthened from ro5 to 330 msec before the 6thpacing impulse is not followed by an A wave indicating intra-atrial block. A new cycle againstarts (7th pacing impulse) with a short PI-A (130 msec) time. Simultaneously with an increasein PI-A time, the AH interval also lengthened progressively (95 to 385 msec) in a Wenckebachpattern (Ist to 3rd paced beats). In the subsequent beats, the AH interval unexpectedly decreasedto 270 msec (5th paced beat) without completing the Wenckebach cycle. This resultedfrom asudden decrease in AA intervalfrom 435 msec (in the 4th A) to 6i5 msec (6th A) despite aconstant atrial pacing rate due to an increase in P1-A time or Wenckebach in the atrium. Thiscase represents a complete Wenckebach in the atrium (PI-A interval) and a partial Wenckebach
" in the AV node (AH interval).
with 4: 3 sinoatrial Wenckebach. The PR andQRS intervals were I65 and 8o msec, respec-tively.At the time of cardiac conduction study, the
sinus cycle length ranged from Io6o to 1II40msec. The PR, PA, AH, and HV times wereI65, 40, 80, and 45 msec, respectively. On atrialpacing with increase in rate (cycle length 6oo-480 msec), the pacing impulse-atrial time progres-sively increased from 8o to I25 msec. With furtherincrease in atrial pacing rate (cycle length 460msec), second-degree Wenckebach block wasseen (Fig. 6, Panel B). The PI-R interval pro-
gressively lengthened from 215 to 335 msecuntil the atrial pacing impulse was not followedby a QRS complex because of the intra-atrialblock. The intracardiac recordings revealed aprogressive lengthening of the conduction timefrom the pacing impulse to the atrial activationrecorded from the area ofthe AV junction (PI-A=70 to I50 msec) until the pacing impulse was notfollowed by an A wave indicating second-degreeintra-atrial block. Similarly, during inducedpremature atrial beats, a progressive increase inpacing impulse-atrial time (80-I45 msec) wasobserved as the coupling interval was shortened
on January 31, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.11.1127 on 1 N
ovember 1972. D
ownloaded from

1132 Narula, Runge, and Samet
FIG. 5 Case 2. Twelve-lead standard electrocardiogram is shown above. Rhythm strip (Vi)recorded on 28 July I97I is highly suggestive of SA Wenckebach (4:3).
FIG. 6 Case 2. During atrial pacing, second-degree Wenckebach was localized in the atrium.(A) Simultaneous BE recordings from the area of the AV junction (BH) and 3 standardelectrocardiogram leads (I, aVF, Vi). During normal sinus rhythm, the PR (I65 msec), PA(40 msec), AH (8o msec), and HV (45 msec) intervals are normal. (B) Atrial pacing at a cyclelength of 460 msec shows Wenckebach second-degree block (4:3) localized within the atrium.The PI-R and PI-A progressively lengthen from 2I5 to 335 and 70 to I5o msec before a beatis dropped (4th pacing impulse). In the dropped beat, the pacing impulse is not followed by an Awave, indicating block within the atrium proximal to the area of the AVjunction. After thedropped beat, the Wenckebach cycle repeats itself.
A!
BE100ms fh(BH) isij 7 *: .~~~~~~PP 1080 msoc
PRR 165 msecP-A 40 msecA-H 80 msecH-V 45 msec
A~~~~~~~~~~~~~~~~~~~~AaVF / _
AP Cycle Length 460 msocA! k~~A- Al A
B p pi P8 + .tH Pi IS PI: pI. r(215 310 i3 PI-R 235 mis c 310 325
0'135 | lS0 - Pl A 90m9sc 135 145100 130 140 - A-H 100 msec 130 135B-45 45 45 M45
B -VF
V
on January 31, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.11.1127 on 1 N
ovember 1972. D
ownloaded from

Second-degree Wenckebach type AV block due to block within the atrium 1133
from IOIO to 470 msec (Fig. 7). During normalsinus rhythm the right atrium was absolutelyrefractory to stimulation with induced prematureatrial beats at a coupling interval of 385 msec atdouble the diastolic threshold. During ventri-cular pacing, retrograde conduction to the atriumwas absent. The sinus node recovery time wasnormal (4oo msec+average sinus cycle length).
Discussion
The present study demonstrates a hithertopostulated but unproven site for the exhibi-tion of second-degree Wenckebach block. Ithas been previously indicated that first-degree
AV block may result from intra-atrial con-duction delays; this concept was recentlyconfirmed in a study using intracardiacrecordings (Katz and Pick, I956; Narulaet al., 197I). The latter study suggested thatpatients with abnormal intra-atrial (PA)conduction may exhibit progressive incre-ment in PA (PI-A) time as the PP intervalis shortened either by atrial pacing or bypremature atrial beats. It was also conjecturedthat PA conduction defects, similar to defectsin other segments of the conduction system,may cause higher degrees ofAV block (Narulaet al., 197I). The two cases in this studydeveloped second-degree Wenckebach type
FIG . 7 Case 2. Effect ofpremature atrial beats inducedfrom the high RA, in the region of thesinus node, on the PI-A conduction time. A-C. As the coupling interval (P-PI) was progressivelyshortened from 1O0O msec to 470 msec, there was a progressive lengthening of the PI-A intervalfrom 8o to 145 msec. The vertical broken line shows the simultaneous onset of the P wave in thestandard electrocardiogram leads and atrial activation in the area of the AVjunction((BE)BH). This raises the possibility of preferential conduction to the AVjunction from thestimulation site.
A-VI(BH)' ,0
i
aVF PIA40
X_-_̂,/ _ AIH go AAH 1,
B
BE(BH)
L-1
OVF
VI
BE(BH)
L-lC aVF
vI
on January 31, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.11.1127 on 1 N
ovember 1972. D
ownloaded from

1134 Narula, Runge, and Samet
of AV block within the atrium during atrialpacing. The progressive lengthening of thepacing impulse to QRS (PI-R) interval wasclearly shown to be caused in part by anincrease in conduction time from the pacingsite in the high right atrium to low rightatrium (the area of the AV junction) until,finally, the pacing stimulus was not followedby an A wave (Fig. 6). This indicates blockwithin the atrium. Case I (Fig. 4) is of interestbecause the study showed simultaneouslytwo different sites of block, i.e. within theatrium and the AV node. The Wenckebachcycle in the AV node (AH interval) was par-tial or incomplete because of the delay andblock in intra-atrial conduction before theimpulse arrival at the AV junction. As aresult, the AH interval, which at first pro-gressively lengthened, suddenly shortenedbecause the AA interval increased secondaryto intra-atrial Wenckebach. These observa-tions again indicate the limitations in theuse of the standard electrocardiogram forthe localization of the site of conductiondefects (Narula et al., I97I).
Localization of the precise site of blockwithin the atrium was not attempted and isbeyond the scope of the present study as thiswould require close bipolar recordingsthroughout the atrium. It may be argued thatthe dropped beat is due to a pacing failure,resulting either from poor positioning ormovement of the stimulating electrodes andan inadequate stimulus strength. Thesepossibilities can be excluded for the follow-ing reasons. (i) To rule out the first possi-bility, the pacing electrodes were moved tovarious sites along the entire length of thelateral border of the right atrium; similarphenomena were observed at the variedpacing sites. (2) Catheter movement wasexcluded by constant fluoroscopic viewingduring the sequence of atrial pacing. (3) TheWenckebach phenomenon was seen even atpacing with a stimulus strength of 4 times thethreshold value and stimulus pulses of 2 msecduration. (4) As the atrial pacing rate wasdecreased, I: I atrial excitation and AV con-duction resumed without other changes. TheWenckebach phenomenon was reproducibleat will. With increase in pacing rate, thedegree of block proportionately increasedand eventually 2:I pacer stimulus - atrialdepolarization block was manifested. (5)Finally, the progressive and classic increasein conduction time from the pacing impulseat high right atrium to the atrial depolariza-tion in the area of the AV junction (PI-A)indicates that this phenomenon resulted fromblock within the atrium rather than a fortui-
tous failure in pacing due to any of the abovementioned possibilities.The underlying mechanism responsible
for the development of intra-atrial block isof interest. Various possibilities should bementioned. (i) In the dropped beat, thepacing stimulus occurred during the absoluteatrial refractory period. This is probablynot the case because the absolute atrialrefractory period as evaluated by inducedpremature atrial beats during normal sinusbeat (despite relatively prolonged sinus cyclelengths) was shorter than the interval at whichthe dropped beats occurred during pacing.The atrial refractory period during atrial pac-ing should be less than that during normalsinus rhythm since the pacing cycle lengthduring second-degree block was less than50 per cent of that during normal sinusrhythm. (2) The atrium was depolarizedaround the stimulating electrodes but theexcitation failed to propagate because of con-duction block in the adjacent atrium probablydue to a disease process. This concept is sup-ported by the progressive increase in the iso-electric interval from the pacing impulse to theonset ofthe P wave (Fig. 6). It may be that dur-ing the isoelectric period, the number of atrialfibres depolarized was not sufficient enoughto produce a P wave on the standard electro-cardiogram which requires depolarization ofa large segment of atrial muscle. Normallythe onset of the surface lead P wave precedesthe atrial depolarization recorded from thearea of the AV junction (or low right atrium)by 25-45 msec (Narula et al., I970, Fig. I).However, in Case 2 (Fig. 7) during the in-duced premature atrial beats, the onset ofthe P wave occurred at the same time as theatrial depolarization in the area of the AVjunction. This suggests abnormal impulsetransmission and probably segmented orlocalized atrial depolarization without a Pwave in the electrocardiogram. An alternativeexplanation may be considered in the latterinstance, namely that there is preferentialconduction through specialized tracts from thepoint of stimulation to the AV junction ratherthan conduction through the remainder ofthe atrium usually responsible for the produc-tion of the P wave on the surface electrocardio-gram (Sherf and James, I969; Holsinger,Wallace, and Sealy, I968). In any case, theatrial stimulus did not result in impulsepropagation to the AV junction and theventricles causing second-degree AV block.
Several reports have described the exis-tence of sinoatrial block (Type I and II) butvarious explanations proposed regarding itsmechanism are controversial and lack experi-
on January 31, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.11.1127 on 1 N
ovember 1972. D
ownloaded from

Second-degree Wenckebach type AV block due to block within the atrium 1135
mental verification (Mackenzie, I902; Bar-low, 1927; Eyster and Meek, I917; Scherf,I946, I969; Greenwood, Finkelstein, andMonheit, I96I). Our study is an experimentalmodel, with the atrial pacing stimulus repre-senting the sinus node, which supports theconcept of sinoatrial Wenckebach due toabnormal conduction between the sinusnode and atrium. It is of interest that inCase 2, the sinus node recovery time, whichis an indication of sinus node function as an
impulse generator, was normal (Narula et al.,I972). The bradycardia in this case was prob-ably secondary to sinoatrial block rather thanthe poor sinus node function, especially inview of the evidence of intra-atrial second-degree block. Also at times, electrocardio-graphic findings of sinoatrial Wenckebachwere observed in this patient (Fig. 5) thoughother possibilities may be entertained, i.e. in-creased vagal tone. However, in Case i, thesinus bradycardia was probably the result ofboth mechanisms, i.e. sinoatrial block andpoor sinus node function because the sinusnode recovery time was prolonged.
Previous studies from this laboratory havestressed the role of intra-atrial conduction(PA) delays in the production of first-degreeAV block and have recommended division ofthe measurement of conduction time fromthe onset of the P wave to the onset of Hisbundle deflection into intra-atrial (PA or
PI-A) and AV nodal (AH) intervals as op-
posed to the PH, or PI-H intervals used byothers (Narula et al., 1970, I971; Damatoet al., I969). The latter studies have con-
sidered PH interval as representative of bothatrial and AV nodal conduction times. The
> present study, by showing first-degree andsecond-degree block within the atrium, re-
iterates the importance of dividing PH intoPA and AH intervals so as not to overlookthe role of intra-atrial conduction delays.The data also show that the PR interval maynot provide an accurate measure of total
s atrioventricular conduction time under spe-
cial circumstances. Fig. 6 and 7 show thatthe atrial pacing impulse may be followed bya long isoelectric segment before the inscrip-tion of the P wave. This suggests that an
impulse may develop and propagate in theatrium for significant periods without pro-
s ducing a deflection in the standard electro-cardiogram in specialized circumstances. It isto be emphasized that the PR interval may
be normal despite a first-degree block second-ary to intra-atrial conduction delay, becausethe initial segment of the PR, as measuredon the surface electrocardiogram, may beisoelectric due to intra-atrial conduction
abnormalities. Similar conclusions were madein a recent study during open heart surgeryusing multiple stimulating and recordingsites in the atrium under direct vision (Waldoet al., I970). In the latter study, the maxi-mum isoelectric segments between the pacingimpulse and the onset of the P wave rangedbetween 10-25 msec, depending upon thesite of stimulation and the proximity ofspecialized intra-atrial tracts. In addition, itwas pointed out that the polarity and shapeof the P wave could be altered by a few milli-metres change in the atrial stimulation site(Waldo et al., I970). The present study is inagreement with these latter findings and sug-gests that the shape of the P wave and thePR interval is not a reliable means for local-ization of the site of impulse origin. In ourcases, the prolongation of the PI-A time,despite varying stimulating sites, probablyindicates a conspicuous degree of conductiondefect.
In Case 2, during induced premature atrialbeats, the onset of P wave and atrial depolar-ization in the area of the AV junction occurredsimultaneously with no measurable PA (PI-A)time. This and a previous study (Narula et al.,I97I) suggest the following: (I) A short PAtime, especially during ectopic atrial arrhyth-mias, may not delineate the complete intra-atrial conduction time. Under these circum-stances, atrial pacing in the area of the sinusnode may be needed to evaluate true intra-atrial conduction time. (2) In cases withsinus rhythm, the conduction time duringatrial pacing from the region of the sinusnode to the area of the AV junction maybe an additional, clinically useful, parameterfor the evaluation of the intra-atrial conduc-tion.One of the prerequisites for the mechanism
of re-entry is a local conduction delay of suffi-cient magnitude during impulse transmissionto enable complete recovery of the tissue atthe subsequent time of impulse arrival atthe site of its origin enabling a second pas-sage of the impulse. The state for single ormultiple re-entry beats is thus provided(Cranefield et al., I959; Moe, Cohen, andVick, I963; Schuilenberg and Durrer, I968;Wallace and Daggett, I964; Han, Malozzi,and Moe, I968). A recent study has indicatedthat AV nodal delay is usually a prerequisitefor supraventricular tachycardias due to re-entry. It was stressed that the AV node andnot the atrium or the His Purkinje systemis the essential site for re-entry (Goldreyerand Damato, 197I). However, the studymerely showed that the re-entry site wasproximal to the His bundle. The possibility
on January 31, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.11.1127 on 1 N
ovember 1972. D
ownloaded from

1136 Narula, Runge, and Samet
that the atrium and not the AV node was thesite of re-entry was not excluded by theexperimental data of these investigators.Other experimental studies have, in fact,shown that the sinus node itself may be thesite for re-entry (Wallace and Daggett, I964;Han et al., I968). Both patients in our studyhad a history of palpitations, and in Case i,atrial tachycardia was documented. Further-more, in Case i, it was shown that Wencke-bach type of block occurred in the atriumwithout dropped beats at the AH interval,i.e. in the AV node (Fig. 4). If the supra-ventricular tachycardia in this case wassecondary to re-entry, then the probablesite for re-entry was within the atrium ratherthan the AV node. The supraventriculartachycardias in the second case may also beexplained on the same basis.
ReferencesBarlow, P. (1927). The clinical occurrence of sino-
auricular block. Lancet, I, 65.Cranefield, P. F., Hoffman, B. F., and de Carvalho,
A. P. (1959). Effects of acetylcholine on singlefibers of the atrioventricular node. CirculationResearch, 7, I9.
Cranefield, P. F., Klein, H. O., and Hoffman, B. F.(I97I). Conduction of the cardiac impulse. I.Delay, block, and one way block in depressedPurkinje fibers. Circulation Research, 28, I99.
Damato, A. N., Lau, S. H., Helfant, R. H., Stein, E.,Berkowitz, W. D., and Cohen, S. I. (I969). Studyof atrioventricular conduction in man using elec-trode catheter recordings of His bundle activity.Circulation, 39, 287.
Donoso, E., Adler, L. N., and Friedberg, C. K. (1964).Unusual forms of second degree atrioventricularblock, including Mobitz type II block, associatedwith the Morgagni-Adams-Stokes syndrome.American Heart J'ournal, 67, 150.
Eyster, J. A. E., and Meek, W. J. (19I7). Experimentson the origin and conduction of the cardiac im-pulse. VII. Sinoventricular and sino-auricularheart block. Archives of Internal Medicine, I9, 117.
Goldreyer, B. N., and Damato, A. N. (I97I). Theessential role of atrioventricular conduction delayin the initiation of paroxysmal supraventriculartachycardia. Circulation, 43, 679.
Greenwood, R. J., Finkelstein, D., and Monheit, R.(I96I). Sino-atrial heart block with Wenckebachphenomenon. American Journal of Cardiology, 8,140.
Han, J., Malozzi, A. M., and Moe, G. K. (I968).Sino-atrial reciprocation in the isolated rabbitheart. Circulation Research, 22, 355.
Hoffman, B. F., and Cranefield, P. F. (I960). Electro-physiology of the Heart. McGraw-Hill, New York.
Holsinger, J. W., Jr., Wallace, A. G., and Sealy, W. C.(I968). The identification and surgical signifi-cance of the atrial internodal conduction tracts.Annals of Surgery, I67, 447.
Katz, L. N., and Pick, A. (1956). Clinical Electrocardio-graphy. Part I. The Arrhythmias. Lea and Febiger,Philadelphia.
Kaufman, J. G., Wachtel, F. W., Rothfield, E., andBernstein, A. (I96I). The association of completeheart block and Adams-Stokes syndrome in twocases of Mobitz type of block. Circulation, 23, 253.
Mackenzie, J. (I902). The cause of heart irregularityin influenza. British Medical Journal, 2, I4I.
Mobitz, W. (I924). Uber die Unvollstandige Storungder Erregungsuberleitung Zwischen Vorhof undKammer des menschlichen Herzens. Zeitschriftfuir die gesamte experimenteelle Medizin, 41, i8o.
Moe, G. K., Cohen, W., and Vick, R. L. (I963).Experimentally induced paroxysmal A-V nodaltachycardia in the dog. American Heart Journal,65, 87.
Narula, 0. S., Cohen, L. S., Samet, P., Lister, J. W.,Scherlag, B. J., and Hildner, F. J. (I970). Local-ization ofA-V conduction defects in man by record-ing of His bundle electrogram. American Journalof Cardiology, 25, 228.
Narula, 0. S., and Samet, P. (I970). Wenckebachand Mobitz type II A-V block due to block withinthe His bundle and bundle branches. Circulation,41, 947.
Narula, 0. S., Samet, P., and Javier, R. P. (1972).Significance of the sinus-node recovery time.Circulation, 45, I40.
Narula, 0. S., Scherlag, B. J., Samet, P., and Javier,R. P. (I97i). Atrioventricular block: localizationand classification by His bundle recordings.American Journal of Medicine, 50, 146.
Phibbs, B. (I963). Paroxysmal atrial tachycardia withblock around the ectopic pacemaker. Circulation,28, 949.
Puech, P., Grolleau, R., Latour, H., DuFoix, R.,Cabasson, J., and Robin, J. (I970). L'enregistre-ment de l'activit6 electrique du faisceau de Hisdans les blocs A-V spontanes. Archives des Maladiesdu Coeur et des Vaisseaux, 63, 784.
Scherf, D. (I946). Experimental sino-auricular block.Proceedings of the Society for Experimental Biologyand Medicine, 6I, 286.
Scherf, D. (I969). The mechanism of sino-atrial block.American Journal of Cardiology, 23, 769.
Sherf, L., and James, T. N. (I969). A new electro-cardiographic concept: synchronized sinoventri-cular conduction. Diseases of the Chest, 55, I27.
Schuilenberg, R. M., and Durrer, D. (I968). Atrialecho beats in the human heart elicited by inducedatrial premature beats. Circulation, 37, 68o.
Singer, D. H., Lazzara, R., and Hoffman, B. F. (1967).Interrelationships between automaticity and con-duction in cardiac Purkinje 'fibers. CirculationResearch, 2I, 537.
Waldo, A. L., Vitikainen, K. J., Kaiser, G. A., Malm,J. R., and Hoffman, B. F. (1970). The P wave andP-R interval: effects of the site of origin of atrialdepolarization. Circulation, 42, 653.
Wallace, A. G., and Daggett, W. M. (I964). Re-excitation of the atrium. 'The echo phenomenon'.American HeartJournal, 68, 66i.
Watanabe, Y., and Dreifus, L. S. (I967). Seconddegree atrioventricular block. CardiovascularResearch, I, I50.
Requests for reprints to Dr. Onkar S. Narula,Division of Cardiology, Department of InternalMedicine, Mount Sinai Hospital of GreaterMiami, 4300 Alton Road, Miami Beach, Florida33I40, U.S.A.
on January 31, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.11.1127 on 1 N
ovember 1972. D
ownloaded from