Journal Progest journal
10
Progesterone therapy in women with epilepsy Ewa Motta 1 , Anna Golba 1 , Zofia Ostrowska 1 , Arkadiusz Steposz 1 , Maciej Huc 1 , Justyna Kotas-Rusnak 2 , Jarogniew J. £uszczki 3,4 , Stanis³aw J. Czuczwar 3,5 , W³adys³aw Lasoñ 6 Correspondence: Abstract: Background: Progesterone with its anti-seizure effect plays a role in the pathophysiology of catamenial epilepsy which affects 31–60% of epileptic women. In this study, an attempt to treat women suffering from catamenial epilepsy with progesterone, as an adjuvant drug, was made. Methods: Th e tr ea tment wa s gi ve nto36 wo men ag ed20–40 ye ar s (mea n age:30.75 ± 6.0 5) wi th se iz ur esin theen ti resecond ha lfof the menstrual cycle, who were found to have low serum levels of progesterone on days 22, 27, 28 of the cycle in comparison with a control group of healthy women. The patients were administered progesterone in a daily dose of 50 mg on days 16–25 of each cyc le. The ser um lev elsof ant iep ile pti c dru gs we re ass aye d. The per iodof pro ges ter onethe rap y ran ged fro m 3 to 45 mont hs (17 .7 on average). Results: Three patients were free of secondary generaliz ed seizures, and one – of simple partial seizures. A decline in the frequency of primary and secondary generalized seizures by 20–96% (55.9% on average) was accomplished in 18 patients (primary g eneral- ized by 20– 96% – 54.7% on ave rag e, andsecondar ily gen eralized by 38– 85%– 59% on ave rag e).A dec lin e in thefrequ enc y of com- plex partial seizure s by 38–87% (63.1% on average) wa s achieved in 15 women. In 1 patient, the frequency of myoclonic seizures decreased by 46%. There was no improvement in 5 women (3 patients with generalized, 1 with complex partial and 1 with simple partial se izures). A n exacerba tion of s eizure fre quency occurred in 5 patients. Adver se effects were not found in any of the subjects. The average concentrations of antiepileptic drugs during hormonal th erapy were in the therapeutic range. Conclusion: Progesterone combined with antiepileptic therapy was well tolerated and resulted in a significant reduction of seizure frequency in majority of patients with catamenial epilepsy . Key words: catamenial epilepsy, progesterone therapy, menstrual cycle 89
-
Upload
bhara-julyandhika-irdi -
Category
Documents
-
view
235 -
download
0
Transcript of Journal Progest journal

8/12/2019 Journal Progest journal
http://slidepdf.com/reader/full/journal-progest-journal 1/10
Progesterone therapy in women with epilepsy
Ewa Motta1, Anna Golba1, Zofia Ostrowska1, Arkadiusz Steposz1,Maciej Huc1, Justyna Kotas-Rusnak2, Jarogniew J. £uszczki3,4,
Stanis³aw J. Czuczwar3,5, W³adys³aw Lasoñ6
Correspondence:
Abstract:
Background: Progesterone with its anti-seizure effect plays a role in the pathophysiology of catamenial epilepsy which affects31–60% of epileptic women. In this study, an attempt to treat women suffering from catamenial epilepsy with progesterone, asan adjuvant drug, was made.Methods: The treatment was given to 36 women aged 20–40 years (mean age:30.75 ± 6.05) with seizuresin the entiresecond half of the menstrual cycle, who were found to have low serum levels of progesterone on days 22, 27, 28 of the cycle in comparison witha control group of healthy women. The patients were administered progesterone in a daily dose of 50 mg on days 16–25 of eachcycle.Theserum levelsof antiepileptic drugs were assayed. Theperiod of progesterone therapy rangedfrom 3 to 45 months (17.7 onaverage).Results: Three patients were free of secondary generalized seizures, and one – of simple partial seizures. A decline in the frequencyof primary and secondary generalized seizures by 20–96% (55.9% on average) was accomplished in 18 patients (primary general-ized by 20–96% – 54.7% on average, andsecondarilygeneralized by 38–85%– 59%on average).A decline in thefrequency of com- plex partial seizures by 38–87% (63.1% on average) was achieved in 15 women. In 1 patient, the frequency of myoclonic seizuresdecreased by 46%. There was no improvement in 5 women (3 patients with generalized, 1 with complex partial and 1 with simple partial seizures). An exacerbation of seizure frequency occurred in 5 patients. Adverse effects were not found in any of the subjects.The average concentrations of antiepileptic drugs during hormonal therapy were in the therapeutic range.Conclusion: Progesterone combined with antiepileptic therapy was well tolerated and resulted in a significant reduction of seizurefrequency in majority of patients with catamenial epilepsy.
Key words:
catamenial epilepsy, progesterone therapy, menstrual cycle
89

8/12/2019 Journal Progest journal
http://slidepdf.com/reader/full/journal-progest-journal 2/10
Introduction
Both experimental and clinical evidence indicates thatovarian hormones exert a profound effect on neuronalexcitability, though in a complex manner. The effectsof estrogens on brain function are mediated by twodifferent nuclear estradiol receptors: ER and ER [12, 42]. The ER are involved in regulation of repro-ductive neuroendocrine and several behavioral func-tions, whereas the role of ER in the brain is rather modulatory [12]. These receptors are ligand-dependenttranscription factors, however, nonnuclear estrogenreceptors coupled to second messenger systems canalso be found e.g., in dendrites, presynaptic terminalsand glia cells [28].
Estradiol exerts generally proconvulsant activity.Specifically, estrogen per se was documented to pro-duce epileptic foci in the feline sensory motor cortex[23] or to shorten the acquisition of kindled seizures by electric stimulation of the amygdala or pentetra-zole injections in ovariectomized rats [22]. Further,estradiol replacement in ovariectomized rats led toa significant enhancement of postictal events – for in-stance, myoclonic jerks [5]. Estradiol also aggravatesseizures evoked by bicuculline, picrotoxin and kai-
nate, but not those induced by flurothyl [30, 37, 41].On the other hand, in juvenile rats ER was shown tomediate antiseizure effects of testosterone metabolites[8]. In contrast to estrogens, progesterone is recog-nized as an anticonvulsant, however, its mechanism of action in the central nervous system has been only partially unravelled. Progesterone receptor belongs toa family of nuclear transcription factors and consistsof two isoforms, PR-A and PR-B, derived from thesame gene. These isoforms are abundant in brain tis-sue and appear to differentially regulate expression of
neurotransmitter synthesizing enzymes and their re-ceptors [9]. Recent data point to a crucial involvementof progesterone nuclear receptors in the developmentand persistence of experimental epileptogenesis. Tothis end, it has been reported that mice which lack both PR-A and PR-B isoforms were more resistant tohippocampal and amygdalar kindling than the wild-type mice [33]. Progesterone also prevented generali-zation in kindled seizures in rats, this effect being,however, observed in sexually immature rats [21].Other data indicate that the anticonvulsant effects of progesterone may be mainly mediated by its metabo-
lite allopregnanolone, a neurosteroid positive modula-
tor of GABA receptor function [24]. Indeed, proges-terone suppressed the pentetrazole-induced convul-sions in male mice and this effect was reversed by
finasteride, a 5-reductase inhibitor, which preventsconversion of progesterone to allopregnanolone. In-terestingly, a progesterone receptor antagonist, mife- pristone, remained without any significant actionupon the convulsive threshold in female mice againstelectroconvulsions or pentetrazole-induced seizures[4]. Further evidence that antiseizure effects of pro-gesterone result from its conversion to allopreg-nanolone and do not require progesterone receptorswas provided by Reddy et al. [31]. These investiga-tors conducted adequate experiments in progesteronereceptor knockout mice of both sexes using pentetra-zole, maximal electroshock and amygdala-kindlingseizure models. However, subsequent study per-formed by these authors suggested that the kindling-retarding effects of progesterone may partly involvethe progesterone-receptor-dependent mechanism [32].In contrast to convulsive seizure models, progesteroneaggravates spike-wave discharges in a genetic modelof absence epilepsy, and this effect also depends on itsconversion to allopregnanolone [40]. Collectively, theexperimental data suggest that modulation of seizureactivity by ovary hormones engages both genomic
and non-genomic mechanisms and depends on animalmodel of seizures.
The cyclical occurrence of epileptic seizures wasalready observed in antiquity. In 1857, Locock no-ticed that seizures in women were often associatedwith hysteria or menstruation [29]. Their connectionwith the menstrual cycle was described for the firsttime by Gowers in 1885 [29]. The term “catamenialepilepsy” comes from the Greek word “katomenios”,meaning “monthly”. Catamenial epilepsy is a particu-lar disease in which there is a cyclical increase in the
number of seizures during menses or in other phasesof the menstrual cycle. Herzog defined catamenialepilepsy as a greater than average seizure frequencyduring perimenstrual or periovulatory periods in nor-mal ovulatory cycles and during the luteal phase inanovulatory cycles [20]. Cyclical changes in the con-centrations of circulating estrogens and progesteroneare now accepted to play a role in the development of catamenial epilepsy. The fluctuations in concentra-tions of antiepileptic drug and changes in water andelectrolyte balance have been also proposed as causesfor the occurrence of catamenial epilepsy [1, 13, 15,
25, 27, 35, 36, 38, 39]. Progesterone with its antisei-
90
8/12/2019 Journal Progest journal
http://slidepdf.com/reader/full/journal-progest-journal 3/10
zure effect plays a pivotal role in the pathophysiologyof catamenial epilepsy which affects 31–60% epilepticwomen [2, 7, 19]. The enhanced susceptibility to sei-zures in perimenstrual catamenial epilepsy is thoughtto result from the rapid decrease of progesterone and,consequently, its metabolite plasma level at the timeof menstruation. Furthermore, since the neurosteroidwithdrawal leads to opposite changes in the benzodi-azepine- and allopregnanolone-sensitive GABA re-
ceptor subunits, the neurosteroid replacement therapyhas been proposed [34].
Objective
In the present study, an attempt to treat epilepticwomen with progesterone was made. The aim of thisstudy was to find out whether efficacy of progester-one therapy depends on types of seizures (generalizedvs. partial seizures), duration of treatment and co-medication with specific antiepileptic drugs.
Method
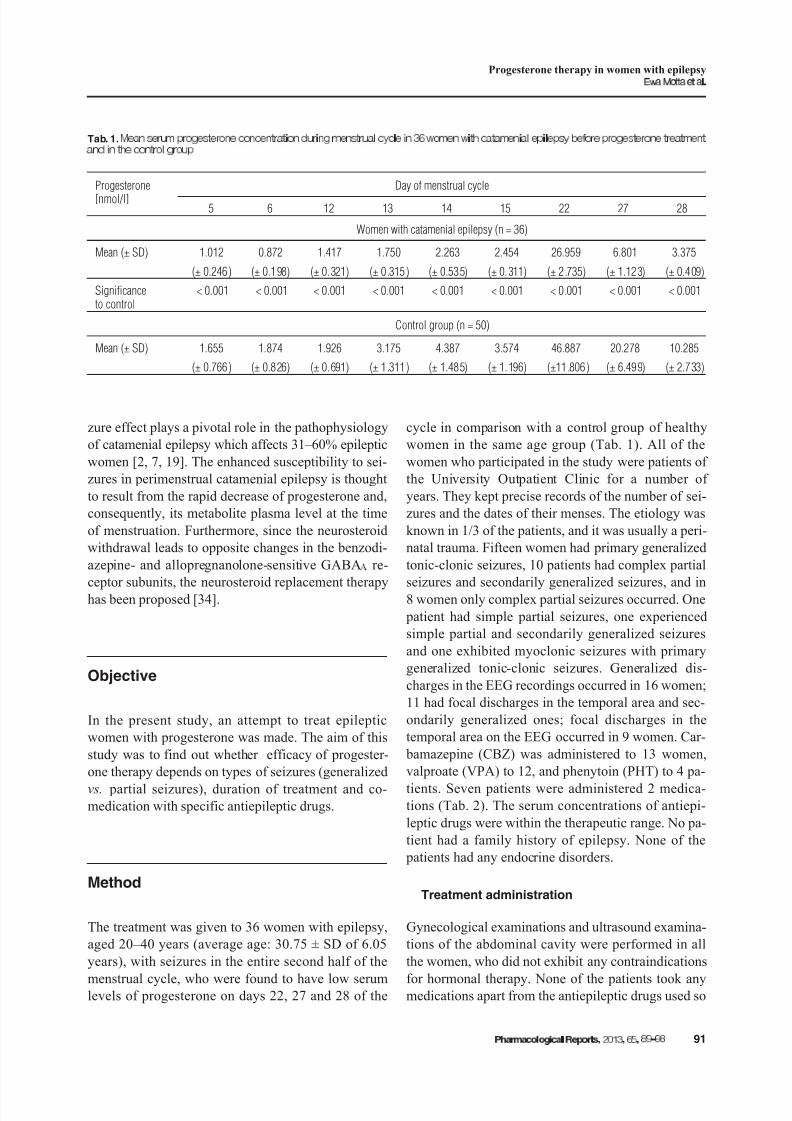
The treatment was given to 36 women with epilepsy,aged 20–40 years (average age: 30.75 ± SD of 6.05years), with seizures in the entire second half of the
menstrual cycle, who were found to have low serumlevels of progesterone on days 22, 27 and 28 of the
cycle in comparison with a control group of healthywomen in the same age group (Tab. 1). All of thewomen who participated in the study were patients of the University Outpatient Clinic for a number of years. They kept precise records of the number of sei-zures and the dates of their menses. The etiology wasknown in 1/3 of the patients, and it was usually a peri-natal trauma. Fifteen women had primary generalizedtonic-clonic seizures, 10 patients had complex partial
seizures and secondarily generalized seizures, and in8 women only complex partial seizures occurred. One patient had simple partial seizures, one experiencedsimple partial and secondarily generalized seizuresand one exhibited myoclonic seizures with primarygeneralized tonic-clonic seizures. Generalized dis-charges in the EEG recordings occurred in 16 women;11 had focal discharges in the temporal area and sec-ondarily generalized ones; focal discharges in thetemporal area on the EEG occurred in 9 women. Car- bamazepine (CBZ) was administered to 13 women,valproate (VPA) to 12, and phenytoin (PHT) to 4 pa-
tients. Seven patients were administered 2 medica-tions (Tab. 2). The serum concentrations of antiepi-leptic drugs were within the therapeutic range. No pa-tient had a family history of epilepsy. None of the patients had any endocrine disorders.
Treatment administration
Gynecological examinations and ultrasound examina-tions of the abdominal cavity were performed in allthe women, who did not exhibit any contraindications
for hormonal therapy. None of the patients took anymedications apart from the antiepileptic drugs used so
91
Progesterone therapy in women with epilepsy
Tab. 1.
Progesterone
[nmol/l]
Day of menstrual cycle
5 6 12 13 14 15 22 27 28
Women with catamenial epilepsy (n = 36)
Mean (± SD) 1.012 0.872 1.417 1.750 2.263 2.454 26.959 6.801 3.375
(± 0.246) (± 0.198) (± 0.321) (± 0.315) (± 0.535) (± 0.311) (± 2.735) (± 1.123) (± 0.409)
Significanceto control
< 0.001 < 0.001 < 0.001 < 0.001 < 0.001 < 0.001 < 0.001 < 0.001 < 0.001
Control group (n = 50)
Mean (± SD) 1.655 1.874 1.926 3.175 4.387 3.574 46.887 20.278 10.285
(± 0.766) (± 0.826) (± 0.691) (± 1.311) (± 1.485) (± 1.196) (±11.806) (± 6.499) (± 2.733)

8/12/2019 Journal Progest journal
http://slidepdf.com/reader/full/journal-progest-journal 4/10
far at fixed doses. Nobody used contraceptive agents.Seizure charts prepared by the patients for severalyears made it possible to compare seizure frequencyduring hormonal therapy with the same period prior tothe therapy. Following consultations with a gynecolo-gist, all the patients were given progesterone in 50 mgsublingual tablets at a 2 × 25 mg dose on days 16–25of each cycle. During hormonal therapy, the serumconcentrations of progesterone were assayed every 6
months on days 22, 27 and 28 of the cycle, but whenthese concentrations exceeded the lower limit of con-centrations in healthy women, the estimations were performed every 3 months. Before and after proges-terone therapy, the serum concentrations of antiepi-leptic drugs (CBZ, VPA and PHT) were also assayed.Hormonal therapy was discontinued if the serum con-centrations of progesterone were close to the averageconcentration of this hormone in the group of healthywomen, or when patient planned a pregnancy. Proges-terone therapy was also intended to be stopped in thecase of any adverse effects.
Ethics
All the women gave written informed approved by thelocal bioethics committee consent to participation inthe study.
Statistical analysis
Microsoft Excel 2003 and StatSoft STATISTICA 7.1PL were used to perform statistical calculations.
The hypothesis of the consistency of the distribu-tion of progesterone levels in each group with the nor-mal distribution was verified with the use of the
Shapiro-Wilk test.The classic Student’s t-test was used for intergroup
comparisons of progesterone levels in the case of con-sistency of the distribution of variables with the nor-mal distribution and after ascertaining homogeneityof variance with the use of the Fisher-Snedecor testfor two variances. If heterogeneity of variance wasfound, Satterwhite’s test was used. If the distributionof progesterone levels in each group was inconsistentwith the normal distribution, the verification of thehypothesis assuming that two samples come from thesame population was carried out with the use of theMann-Whitney U test.
Analysing the qualitative characteristics, the verifi-cation of the hypothesis of independence of two char-acteristics was conducted with the use of the nonpara-metric test.
Results
The periods of progesterone therapy ranged from 3 to45 months (the average period of therapy was 17.7months) (Tab. 3). Only 1 patient was treated for theshortest period of 3 months; the patient discontinuedthe treatment herself, without giving a reason despitea decline in seizure frequency by 25%. In addition, 10more patients in whom the progesterone therapy pe-riod ranged between 4 and 12 months gave up treat-ment. In this group, treatment was discontinued in1 patient due to a lack of improvement, and 2 patientswith rare seizures discontinued treatment because of a slightly higher number of generalized seizures (one
woman had 1 seizure more, and the other had 2 sei-zures more during the whole period of therapy. Threewomen who had 2 types of seizures discontinuedtreatment because the frequency of secondarily gener-alized seizures did not decline in spite of the disap- pearance of simple partial seizures in one of them anda decline in the frequency of complex partial seizures by 56% and 84%, respectively, in the other two pa-tients. The remaining 4 patients, in whom seizure fre-quency decreased by 30–84%, including one with twotypes of seizures in whom generalized seizures
ceased, gave up progesterone therapy for non-medicalreasons. Hormonal therapy was discontinued due to
92
Tab. 2.
Drug n Mean dose (± SD) [mg/d]
CBZ 13 1192.31 (± 256.46)
VPA 12 1483.33 (± 265.72)
PHT 4 375.0 (± 50.0)
CBZ + PHT 5 CBZ 660.0 (± 134.16)
PHT 300.0 (± 70.71)
CBZ + VPA 1 CBZ 900.0 VPA 1200.0
PHT + VPA 1 PHT 300.0 VPA 800.0

8/12/2019 Journal Progest journal
http://slidepdf.com/reader/full/journal-progest-journal 5/10
a planned pregnancy in 2 patients who had two typesof seizures treated for 22 and 23 months, respectively,in whom secondarily generalized seizures subsided,and the frequency of complex partial seizures was re-duced by 45 and 86%, respectively. A planned preg-nancy was also the reason for giving up progesteronetherapy by a patient in whom the frequency of gener-
alized seizures decreased by 67% during 6-monththerapy. Side effects were not found in any of the sub- jects. To sum up the results of progesterone replace-ment therapy in all the women, the disappearance of secondarily generalized seizures was achieved in 3 patients, and of simple partial seizures – in 1 woman.A decline in the frequency of primary and secondarilygeneralized seizures by 20–96% (by 55.9% on aver-age) was found in 18 patients (respectively, primarilygeneralized ones by 20–96% – 54.7% on average; and
secondarily generalized ones by 38–85% – by 59% onaverage). A decline in the frequency of partial com- plex seizures by 38–87% (by 63.1% on average) wasachieved in 15 women. In 1 patient, the frequency of myoclonic seizures decreased by 46% (Tab. 4).
There was no improvement in 5 women (3 of the patients had generalized seizures, 1 patient had com-
plex partial seizures and 1 patient had simple partialseizures). A slight exacerbation of seizure frequencyoccurred in 5 patients. In this group, 3 women (in-cluding 2 with rare seizures) had 1–2 generalized sei-zures more over the 4–24 months of treatment. Two patients with complex partial seizures had, respec-tively, 12 and 7 seizures more, one in the period of 24months, and the other one over 15 months of hormo-nal therapy. In total, prior to progesterone therapy,3407 complex partial seizures were recorded in 18 pa-
93
Progesterone therapy in women with epilepsy
Tab. 4.
n
Seizure activity in patients
After progesterone treatment
Percent of improvment (decrease of seizures)
Mean (± SD) Median Minimum MaximumQuartile
No change Exacerbation Improvement Lower Upper
S E I Z U R E
T Y P E S Complex partial 18 1 2 15 63.07 (± 16.24) 60.00 38.00 87.00 49.00 84.00
Generalized 27 3 3 21 62.19 (± 27.71) 66.00 20.00 100.00 38.00 85.00
Simple partial 2 1 0 1 100.00 100.00 100.00 100.00 100.00 100.00
Myoclonic 1 0 0 1 46.00 46.00 46.00 46.00 46.00 46.00
Tab. 3.
n Mean (± SD) Median Minimum MaximumQuartile
Lower Upper
S E I Z U R E S
Complex partialbefore treatment
18189.28 (±136.84) 120.50 32.00 475.00 92.00 255.00
after treatment 79.94 (± 55.73) 65.50 10.00 190.00 30.00 120.00
Generalizedbefore treatment
2747.33 (± 45.86) 46.00 1.00 198.00 10.00 64.00
after treatment 23.33 (± 27.41) 12.00 0.00 97.00 3.00 38.00
Simple partialbefore treatment
258.00 (± 25.46) 58.00 40.00 76.00 40.00 76.00
after treatment 19.50 (± 27.58) 19.50 0.00 39.00 0.00 39.00
Myoclonicbefore treatment
1460.00 460.00 460.00 460.00 460.00 460.00
after treatment 248.00 248.00 248.00 248.00 248.00 248.00
Duration of treatment [months] 36 17.69 (± 10.71) 16.50 3.00 45.00 7.00 24.00
8/12/2019 Journal Progest journal
http://slidepdf.com/reader/full/journal-progest-journal 6/10
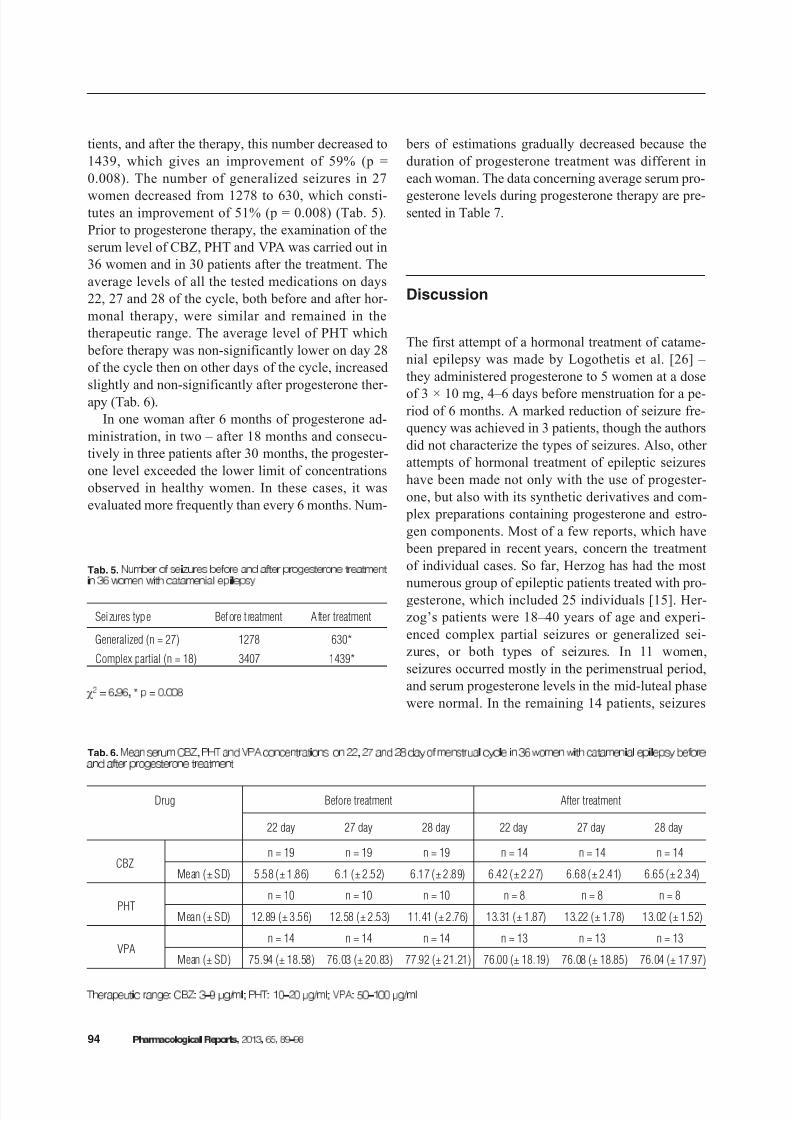
tients, and after the therapy, this number decreased to1439, which gives an improvement of 59% (p =0.008). The number of generalized seizures in 27
women decreased from 1278 to 630, which consti-tutes an improvement of 51% (p = 0.008) (Tab. 5).Prior to progesterone therapy, the examination of theserum level of CBZ, PHT and VPA was carried out in36 women and in 30 patients after the treatment. Theaverage levels of all the tested medications on days22, 27 and 28 of the cycle, both before and after hor-monal therapy, were similar and remained in thetherapeutic range. The average level of PHT which before therapy was non-significantly lower on day 28of the cycle then on other days of the cycle, increasedslightly and non-significantly after progesterone ther-apy (Tab. 6).
In one woman after 6 months of progesterone ad-ministration, in two – after 18 months and consecu-tively in three patients after 30 months, the progester-one level exceeded the lower limit of concentrationsobserved in healthy women. In these cases, it wasevaluated more frequently than every 6 months. Num-
bers of estimations gradually decreased because theduration of progesterone treatment was different ineach woman. The data concerning average serum pro-
gesterone levels during progesterone therapy are pre-sented in Table 7.
Discussion
The first attempt of a hormonal treatment of catame-nial epilepsy was made by Logothetis et al. [26] – they administered progesterone to 5 women at a dose
of 3 × 10 mg, 4–6 days before menstruation for a pe-riod of 6 months. A marked reduction of seizure fre-quency was achieved in 3 patients, though the authorsdid not characterize the types of seizures. Also, other attempts of hormonal treatment of epileptic seizureshave been made not only with the use of progester-one, but also with its synthetic derivatives and com- plex preparations containing progesterone and estro-gen components. Most of a few reports, which have been prepared in recent years, concern the treatmentof individual cases. So far, Herzog has had the most
numerous group of epileptic patients treated with pro-gesterone, which included 25 individuals [15]. Her-zog’s patients were 18–40 years of age and experi-enced complex partial seizures or generalized sei-zures, or both types of seizures. In 11 women,seizures occurred mostly in the perimenstrual period,and serum progesterone levels in the mid-luteal phasewere normal. In the remaining 14 patients, seizures
94
Tab. 6.
Drug Before treatment After treatment
22 day 27 day 28 day 22 day 27 day 28 day
CBZn = 19 n = 19 n = 19 n = 14 n = 14 n = 14
Mean (± SD) 5.58 (± 1.86) 6.1 (± 2.52) 6.17 (± 2.89) 6.42 (± 2.27) 6.68 (± 2.41) 6.65 (± 2.34)
PHTn = 10 n = 10 n = 10 n = 8 n = 8 n = 8
Mean (± SD) 12.89 (± 3.56) 12.58 (± 2.53) 11.41 (± 2.76) 13.31 (± 1.87) 13.22 (± 1.78) 13.02 (± 1.52)
VPAn = 14 n = 14 n = 14 n = 13 n = 13 n = 13
Mean (± SD) 75.94 (± 18.58) 76.03 (± 20.83) 77.92 (± 21.21) 76.00 (± 18.19) 76.08 (± 18.85) 76.04 (± 17.97)
Tab. 5.
Seizures type Before t reatment After treatment
Generalized (n = 27) 1278 630*
Complex partial (n = 18) 3407 1439*

8/12/2019 Journal Progest journal
http://slidepdf.com/reader/full/journal-progest-journal 7/10
occurred in the entire second half of the cycle, and progesterone levels in the mid-luteal phase werelower than 15.9 mmol/l. Progesterone lozenges,200 mg twice a day, were given to all of them. Proges-terone was administered in 11 women with perimen-strual seizures on days 23–25 of the menstrual cycle,
and in 14 patients with seizures in the second half of the cycle on days 15–25. Herzog compared thenumber of seizures during the 3-month hormonaltherapy with the 3-month period prior to the begin-ning of the progesterone therapy. Improvement oc-curred in 18 out of the 25 treated women. A decline inthe frequency of tonic-clonic seizures by 58% and partial seizures by 54% was recorded. Herzog ob-served that the best effects occurred in women inwhom progesterone was administered for longer time.There was no improvement in 5 patients, and treat-
ment was discontinued in 2 women due to progester-one intolerance, though its symptoms (asthenia, de-
pression) were not very intense. The serum levels of antiseizure medications, tested once a month in themid-luteal phase during hormonal therapy, werewithin the normal range, similar to the period beforetreatment with progesterone [15].
Eighteen women, in 15 of whom antiepileptic ther-
apy was not changed, continued hormonal therapyfor 3 years. With unchanged antiepileptic therapy,3 women treated with progesterone did not have sei-zures; seizure frequency declined by 75–99% in4 women, and by 50–74% in 8 women [16].
Several years earlier, Herzog used progesterone totreat 8 women with complex partial seizures with se-rum progesterone levels in the mid-luteal phase below7.95 mmol/l [14]. Two patients were not taking antie- pileptic medication. For 3 months, the patients re-ceived vaginal suppositories with progesterone at
a dose of 50–400 mg every 12 h. Measuring proges-terone levels 2–6 h after suppositories, its doses were
95
Progesterone therapy in women with epilepsy
Tab. 7.
Month Progesterone
[nmol/l]
Day of menstrual cycle Significance to control (p)
22 27 28 22 27 28
0n 36 36 36
< 0.001 < 0.001 < 0.001Mean (± SD) 26.96 ± 2.74 6.8 ± 1.12 3.38 ± 0.41
6n 30 30 30
< 0.001 < 0.001 < 0.001Mean (± SD) 31.22 ± 3.49 9.95 ± 2.48 5.32 ± 1.22
9n 1 1 1
Mean (± SD) 49.11 18.51 8.27
12n 25 25 25 < 0.001 < 0.001 < 0.001
Mean (± SD) 34.36 ± 3.97 12.29 ± 3.33 6.81 ± 1.55
18n 18 18 18 < 0.001 < 0.001 < 0.001
Mean (± SD) 35.67 ± 3.73 13.32 ± 3.1 7.44 ± 1.15
21n 2 2 2
Mean (± SD) 49.58 ± 2.6 22.77 ± 4.31 11 ± 1.16
24n 13 13 13 0.04 0.005 0.03
Mean (± SD) 38.85 ± 4.61 15.17 ± 3.31 8.44 ± 1.82
30n 7 7 7 0.35 0.32 0.56
Mean (± SD) 41.89 ± 5.42 17.89 ± 4.22 9.34 ± 1.65
33n 3 3 3
Mean (± SD) 47.01 ± 1.87 19.51 ± 1.72 11.51 ± 0.47
Control
n 50 50 50
Mean (± SD) 46.89 ± 11.81 20.28 ± 6.5 10.28 ± 2.73

8/12/2019 Journal Progest journal
http://slidepdf.com/reader/full/journal-progest-journal 8/10

8/12/2019 Journal Progest journal
http://slidepdf.com/reader/full/journal-progest-journal 9/10
tween norethisterone and antiseizure medications,which may cause a decrease in the level of the hor-mone necessary “for action”. Mattson et al. [27], ana-
lyzing the results of this study, concluded that the in-effectiveness of norethisterone resulted from intervalsin administration of the hormone. Hall [11], whohad earlier administered norethisterone at a dose of 0.35 mg/day to a 29-year-old woman with tonic-clonic seizures in the perimenstrual period, did notobserve seizures during the 7 months of using the hor-mone. Earlier, this patient had been taking a combinedcontraceptive preparation (ethinylestradiol + norges-trel) because of dysmenorrhoea, not having seizureseither. This preparation, due to strong chest pain, wasreplaced with one that only contained progesterone(norethisterone), with a similar effect.
To sum up, all the previous attempts focused onhormonal treatment of epilepsy, it seems that slightlydifferent results of such therapy may be associatedwith taking preparations from different groups, at dif-ferent doses, in different ways and for different peri-ods of time. Extending attempts of hormonal treat-ment of epilepsy and gaining experience associatedwith the treatment could perhaps help to establish beneficial standards of such therapy in the future. Re-ferring to our results, the anticonvulsant activity of
progesterone in some women and the possibility of using this hormone in some cases of drug resistantcatamenial epilepsy have been confirmed. The last publication of Herzog et al. which appeared only inJune 2012 provides another strong evidence for thistherapy [18].
Disclosure of conflict of interest:
References:
1. Ansell B, Clarke E: Epilepsy and menstruation. The roleof water retention. Lancet, 1956, 15, 1232–1235.
2. Bazan AC, Montenegro MA, Cendes F, Min LL,Guerreiro CA: Menstrual cycle worsening of epilepticseizures in women with symptomatic focal epilepsy.Arg Neuropsiguiatr, 2005, 63, 751–756.
3. Boèan P, Dvorak K, Krejèi P: Hormonal dependenceof some paroxysmal pathological conditions (Czech).Ès Gynek, 1981, 4, 35–38.
4.
Borowicz KK, £uszczki J, Matuszek M, Kleinrok Z,Czuczwar SJ: Effects of tamoxifen, mifepristone, and cy-
proterone on the electroconvulsive threshold and pentetrazole-induced convulsions in mice. Pol J Pharma-col, 2002, 54, 103–109.
5. Buterbaugh GG: Postictal events in amygdala-kindled
female rats with and without estradiol replacement.Exp Neurol, 1987, 95, 697–713.
6. Dana-Haeri J, Richens A: Effect of norethisterone onseizures associated with menstruation. Epilepsia, 1983,24, 377–381.
7. El-Khayat HA, Soliman NA, Tomoum HY, Omran MA,El-Wakad AS, Shatia RH: Reproductive hormonalchanges and catamenial pattern in adolescent femaleswith epilepsy. Epilepsia, 2008, 49, 1619–1626.
8. Frye CA, Ryan A, Rhodes M: Antiseizure effects of 3-androstanediol and/or 17-estradiol may involve ac-tions at estrogen receptor . Epilepsy Behav, 2009, 16,418–422.
9. González-Flores O, Gómora-Arrati P, García-Juárez M,Miranda-Martínez A, Armengual-Villegas A, Camacho-Arroyo I, Guerra-Araiza C: Progesterone receptor iso-forms differentially regulate the expression of tryptophanand tyrosine hydroxylase and glutamic acid decarboxy-lase in the rat hypothalamus. Neurochem Int, 2011, 59,671–676.
10. Grünewald RA, Aliberti V, Panayiotopoulos CP: Exacer- bation of typical absence seizures by progesterone. Sei-zure, 1992, 1, 137–138.
11. Hall S: Treatment of menstrual epilepsy with a progester-one only oral contraceptive. Epilepsia, 1977, 18, 235–236.
12. Handa RJ, Ogawa S, Wang JM, Herbison AE: Roles for estrogen receptor beta in adult brain function. J Neuroen-
docrinol, 2012, 24, 160-173.13. Herkes GK, Eadie M, Sharbrough F, Moyer T: Patterns
of seizure occurrence in catamenial epilepsy. EpilepsyRes, 1993, 15, 47–52.
14. Herzog AG: Intermittent progesterone therapy and fre-quency of complex partial seizures in women with men-strual disorders. Neurology, 1986, 36, 1607–1610.
15. Herzog AG: Progesterone therapy in women with com- plex partial and secondary generalized seizures. Neurol-ogy, 1995, 45, 1660–1662.
16. Herzog AG: Progesterone therapy in women with epilepsy:a 3-year follow-up. Neurology, 1999, 52, 1917–1918.
17. Herzog AG: Reproductive endocrine considerations andhormonal therapy for women with epilepsy. Epilepsia,
1991, 32 Suppl 6, 27–33.18. Herzog AG, Fowler KM, Smithson SD, Kalayjian LA,
Heck CN, Sperling MR, Liporace JD et al.: Progesteronevs placebo therapy for woman with epilepsy: A random-ized clinical trial. Neurology, 2012, 12, 1959–1966.
19. Herzog AG, Harden CL, Liporace J, Pennell P, Schomer DL, Sperling M, Fowler K et al.: Frequency of catame-nial seizure exacerbation in women with localization-related epilepsy. Ann Neurol, 2004, 56, 431–434.
20. Herzog AG, Klein P, Ransil BJ: Three patterns of cata-menial epilepsy. Epilepsia, 1997, 38, 1082–1088.
21. Holmes GL, Weber DA: The effect of progesterone on kin-dling: a developmental study. Brain Res, 1984, 318, 45–53.
22.
Hom AC, Buterbaugh GG: Estrogen alters the acquisi-tion of seizures kindled by repeated amygdale stimula-
97
Progesterone therapy in women with epilepsy

8/12/2019 Journal Progest journal
http://slidepdf.com/reader/full/journal-progest-journal 10/10
tion or pentylenetetrazole administration in ovariecto-mized female rats. Epilepsia, 1986, 27,103–108.
23. Julien RM, Fowler GW, Danielson MG: The effects of antiepileptic drugs on estrogen-induced electrographic
spike wave discharges. J Pharmacol, 1975, 193, 647–656.24. Kokate TG, Banks MK, Magee T, Yamaguchi S,
Rogawski MA: Finasteride, a 5-reductase inhibitor, blocks the anticonvulsant activity of progesterone inmice. J Pharmacol Exp Ther, 1999, 288, 679–684.
25. Kumar N, Behari M, Ahuja GK, Jailkhani BJ: Phenytoinlevels in catamenial epilepsy. Epilepsia, 1988, 29, 155–158.
26. Logothetis J, Harner R, Morrell M, Torres F: The role of estrogens in catamenial exacerbations of epilepsy. Neu-rology, 1959, 9, 352–360.
27. Mattson RH, Cramer JA, Caldwell BV, Siconolfi BC:Treatment of seizures with medroxyprogesterone acetate: preliminary report. Neurology, 1984, 34, 1255–1257.
28. McEwen BS: Invited review: Estrogens effects onthe brain: multiple sites and molecular mechanisms.J Appl Physiol, 2001, 91, 2785–2801.
29. Newmark ME, Penry JK: Catamenial epilepsy: a review.Epilepsia, 1982, 21, 281–300.
30. Nicoletti F, Speciale C, Sortino MA, Summa G, CarusoG, Patti F, Canonico PL: Comparative effects of estradiol benzoate, the antiestrogen clomiphene citrate, and the progestin medroxyprogesterone acetate on kainic acid-induced seizures in male and female rats. Epilepsia,1985, 26, 252–257.
31. Reddy DS, Castaneda DC, O’Malley BW, RogawskiMA: Anticonvulsant activity of progesterone and neu-rosteroids in progesterone receptor knockout mice.
J Pharmacol Exp Ther, 2004, 310, 230–239.32. Reddy DS, Gangisetty O, Briyal S: Disease-modifyingactivity of progesterone in the hippocampus kindlingmodel of epileptogenesis. Neuropharmacology, 2010, 59,573–581.
33. Reddy DS, Mohan A: Development and persistence of limbic epileptogenesis are impaired in mice lacking pro-gesterone receptors. J Neurosci, 2011, 3, 650–658.
34. Reddy DS, Rogawski MA: Neurosteroid replacementtherapy for catamenial epilepsy. Neurotherapeutics,2009, 6, 392–401.
35. Rodriquez-Macias KA: Catamenial epilepsy: gyneco-
logical and hormonal implications. Five case reports.Gynecol Endocrinol, 1996, 10, 139–142.
36. Rosciszewska D, Buntner B., Guz I, Zawisza L: Ovarianhormones, anticonvulsant drugs and seizures during themenstrual cycle in women with epilepsy. J Neurol Neu-rosurg Psychiatry, 1986, 49, 47–51.
37. Schwartz-Giblin S, Korotzer A, Pfaff DW: Steroid hor-mone effects on picrotoxin-induced seizures in femaleand male rats. Brain Res, 1989, 476, 240–247.
38. Shavit G, Lerman P, Korczyn AD, Kivity S, Behar M,Gitter S: Phenytoin pharmacokinetics in catamenial epi-lepsy. Neurology, 1984, 34, 959–961.
39. Tuveri A, Paoletti AM, Orrù M, Melis GB, Marotto MF,Zedda P, Marrosu F et al.: Reduced serum level of THDOC,
an anticonvulsant steroid in women with perimenstrualcatamenial epilepsy. Epilepsia, 2008, 49, 1221–1229.
40. van Luijtelaar G, Budziszewska B, Tetich M, Lasoñ W:Finasteride inhibits the progesterone-induced spike-wavedischarges in a genetic model of absence epilepsy. Phar-macol Biochem Behav, 2003, 75, 889–894.
41. Velísek L, Velísková J, Etgen AM, Stanton PK, MoshéSL: Region-specific modulation of limbic seizure sus-ceptibility by ovarian steroids. Brain Res, 1999, 842,132–138.
42. Weiser MJ, Foradori CD, Handa RJ: Estrogen receptor beta in the brain: from form to function. Brain Res Rev,2008, 57, 309–320
43. Zimmerman EA, Holden KR, Reiter EO, Dekaban AS:Medroxyprogesterone acetate in the treatment of seizuresassociated with menstruation. J Pediatr, 1973, 83, 959–963.
Received: in therevised form:
accepted:
98