Journal of plastic reconstructive & aesthetic surgery JPRAS 2010 di Summa (2).pdf
9
Adipose-derived stem cells enhance peripheral nerve regeneration P.G. di Summa a,b , P.J. Kingham b,c , W. Raffoul a , M. Wiberg c , G. Terenghi b , D.F. Kalbermatten a,c, * a Chirurgie Plastique et Reconstructive CHUV, Universite´de Lausanne, Rue de Bugnon 46, 1005 Lausanne, CH, Switzerland b Blond McIndoe Research Laboratories. The University of Manchester, Manchester, UK c Departments of Surgical and Perioperative Science (Hand surgery) and Integrative Medical Biology (Anatomy), Umea University, Umea, Sweden Received 30 March 2009; accepted 10 September 2009 KEYWORDS Adipose-derived stem cells; Peripheral nerve regeneration; Differentiated cells; Sciatic nerve Summary Traumatic injuries resulting in peripheral nerve lesions often require a graft to bridge the gap. Although autologous nerve auto-graft is still the first-choice strategy in recon- structions, it has the severe disadvantage of the sacrifice of a functional nerve. Cell transplan- tation in a bioartificial conduit is an alternative strategy to create a favourable environment for nerve regeneration. We decided to test new fibrin nerve conduits seeded with various cell types (primary Schwann cells and adult stem cells differentiated to a Schwann cell-like pheno- type) for repair of sciatic nerve injury. Two weeks after implantation, the conduits were removed and examined by immunohisto- chemistry for axonal regeneration (evaluated by PGP 9.5 expression) and Schwann cell pres- ence (detected by S100 expression). The results show a significant increase in axonal regeneration in the group of fibrin seeded with Schwann cells compared with the empty fibrin conduit. Differentiated adipose-derived stem cells also enhanced regeneration distance in a similar manner to differentiated bone marrow mesenchymal stem cells. These observations suggest that adipose-derived stem cells may provide an effective cell population, without the limitations of the donor-site morbidity associated with isolation of Schwann cells, and could be a clinically translatable route towards new methods to enhance peripheral nerve repair. ª 2009 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published by Elsevier Ltd. All rights reserved. Numerous surgical procedures are performed each year for peripheral nerve repair, with a significant amount of lost working days with corresponding economic consequences. 1 Nerve lesions without defect or with a short gap are usually treated by end-to-end coaptation. Traumatic injuries resulting in longer peripheral nerve lesions often require a graft to bridge the gap. Unfortunately, full recovery may never be achieved, particularly with extended lesions. 2 Although autologous nerve autograft is still the first-choice * Corresponding author. Tel.: þ41 21 314 25 06; Fax: þ41 21 314 25 31. E-mail address: [email protected] (D.F. Kalbermatten). ARTICLE IN PRESS 1748-6815/$ - see front matter ª 2009 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.bjps.2009.09.012 Journal of Plastic, Reconstructive & Aesthetic Surgery (2009) xx,1e9 + MODEL Please cite this article in press as: di Summa PG et al., Adipose-derived stem cells enhance peripheral nerve regeneration, J Plast Reconstr Aesthet Surg (2009), doi:10.1016/j.bjps.2009.09.012
Transcript of Journal of plastic reconstructive & aesthetic surgery JPRAS 2010 di Summa (2).pdf

ARTICLE IN PRESS
Journal of Plastic, Reconstructive & Aesthetic Surgery (2009) xx, 1e9
+ MODEL
Adipose-derived stem cells enhance peripheralnerve regeneration
P.G. di Summa a,b, P.J. Kingham b,c, W. Raffoul a, M. Wiberg c,G. Terenghi b, D.F. Kalbermatten a,c,*
a Chirurgie Plastique et Reconstructive CHUV, Universite de Lausanne, Rue de Bugnon 46, 1005 Lausanne, CH, Switzerlandb Blond McIndoe Research Laboratories. The University of Manchester, Manchester, UKc Departments of Surgical and Perioperative Science (Hand surgery) and Integrative Medical Biology (Anatomy), UmeaUniversity, Umea, Sweden
Received 30 March 2009; accepted 10 September 2009
KEYWORDSAdipose-derivedstem cells;Peripheral nerveregeneration;Differentiated cells;Sciatic nerve
* Corresponding author. Tel.: þ41 2125 31.
E-mail address: daniel.kalberKalbermatten).
1748-6815/$-seefrontmatterª2009Britdoi:10.1016/j.bjps.2009.09.012
Please cite this article in press as:Reconstr Aesthet Surg (2009), doi:10
Summary Traumatic injuries resulting in peripheral nerve lesions often require a graft tobridge the gap. Although autologous nerve auto-graft is still the first-choice strategy in recon-structions, it has the severe disadvantage of the sacrifice of a functional nerve. Cell transplan-tation in a bioartificial conduit is an alternative strategy to create a favourable environmentfor nerve regeneration. We decided to test new fibrin nerve conduits seeded with various celltypes (primary Schwann cells and adult stem cells differentiated to a Schwann cell-like pheno-type) for repair of sciatic nerve injury.
Two weeks after implantation, the conduits were removed and examined by immunohisto-chemistry for axonal regeneration (evaluated by PGP 9.5 expression) and Schwann cell pres-ence (detected by S100 expression). The results show a significant increase in axonalregeneration in the group of fibrin seeded with Schwann cells compared with the empty fibrinconduit. Differentiated adipose-derived stem cells also enhanced regeneration distance ina similar manner to differentiated bone marrow mesenchymal stem cells. These observationssuggest that adipose-derived stem cells may provide an effective cell population, without thelimitations of the donor-site morbidity associated with isolation of Schwann cells, and could bea clinically translatable route towards new methods to enhance peripheral nerve repair.ª 2009 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
Numerous surgical procedures are performed each year forperipheral nerve repair, with a significant amount of lost
314 25 06; Fax: þ41 21 314
[email protected] (D.F.
ishAssociationofPlastic,Reconstruc
di Summa PG et al., Adipose-de.1016/j.bjps.2009.09.012
working days with corresponding economic consequences.1
Nerve lesions without defect or with a short gap are usuallytreated by end-to-end coaptation. Traumatic injuriesresulting in longer peripheral nerve lesions often requirea graft to bridge the gap. Unfortunately, full recovery maynever be achieved, particularly with extended lesions.2
Although autologous nerve autograft is still the first-choice
tiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.
rived stem cells enhance peripheral nerve regeneration, J Plast

ARTICLE IN PRESS
2 P.G. di Summa et al.
+ MODEL
strategy in reconstructions, they have several disadvan-tages caused by the limited availability of donor tissue,sacrifice of functional nerve and potential formation ofneuroma.2e4
Nerve autografts have been mimicked by venous andarterial conduit grafts, which show no functional benefitscompared with standard nerve grafts.5 Allografts have alsobeen tested, but they require an undesirable long-termimmunosuppressive therapy.6 Many attempts have beenmade to develop conduits made of biodegradable mate-rials, which could guide the regenerating axons withoutinhibiting the process of growth and maturation.7 Recently,we described a bioresorbable nerve constructed from fibringlue,8 which shows good tissue acceptance and a porousstructure that allows neurotrophic growth factors topenetrate into the lumen of the conduit. Moreover, theresorption of the conduit within 4 weeks avoids compres-sion syndromes and enhances biocompatibility.9
Our aim was to optimise the fibrin conduit, previouslydescribed, by seeding it with regenerative cells. Celltransplantation in a bioartificial conduit is an alternativestrategy to create a favourable environment for nerveregeneration10: in this study, we compared different cellpopulations such as primary Schwann cells (SCs) and stemcells differentiated towards to a Schwann cell phenotype.
SCs offer a highly preferred substrate for axon migrationand release of bioactive factors that further enhancemigration. They synthesise adhesion molecules (CAMs),release growth factors (GFs) and build up basementmembranes for the support and guidance of the sproutingaxons.11,12 Despite showing regeneration enhancement,13
SCs have limited clinical applications. The culture ofa sufficient amount of SC to achieve optimal conditions fortransplantation in nerve conduits is time consuming andrequires particular care for in vitro expansion anda constant input of GFs.14 Moreover, SCs are not easilyaccessible without nerve biopsy and bear the need tosacrifice an autologous nerve, with the related complica-tions of anaesthesia and pain at the harvest site.4,15
Instead, the ideal transplantable cell should be easilyaccessible, should proliferate rapidly in culture and shouldsuccessfully integrate into the host tissue with immunologicaltolerance.16,17 The growing applicability of stem cells hasopened new frontiers to nerve regeneration: the advantageof using these cell lines is that cell differentiation may bestimulated by advancing axons and pluripotency, allowsmultiple differentiation paths, which can create a positiveenvironment for axonal regeneration.1
Bone-marrow-derived mesenchymal stem cells (MSCs)can be induced to differentiate into non-mesenchymal fatesin vitro, such as Schwann cells, improving myelin formationand nerve regeneration in vivo after their transplantationinto different models of peripheral nerve injury.18e20
Adipose tissue is a mesodermally derived complex tissuethat, besides adipocytes and pre-adipocytes, containsa stromal population, which includes microvascular endo-thelial cells, smooth muscle cells, resident monocytes,lymphocytes and stem cells.21,22 These non-adipocyte cellsare known as stromal vascular fraction (SVF) and can beisolated by centrifugation of collagenase-digested adiposetissue.23 In the past few years, it has been shown howcultured SVFs give rise to multipotent precursor cell from
Please cite this article in press as: di Summa PG et al., Adipose-deReconstr Aesthet Surg (2009), doi:10.1016/j.bjps.2009.09.012
adipose tissue stromal cells.24e26 Although literatureterminology can be confusing,27,28 we will use the genericnomenclature of adipose-derived stem cells (ADSCs) todescribe these cells.
As previously cited, stem and progenitor cells from adultstromal tissue retain the capacity to differentiate towardsmesenchymal and non-mesenchymal lineages, similar tobonemarrow stromal cells,24,29 showing pluripotency above mul-tipotency.30 Regarding neural differentiation, several studiesproved trans-differentiation of ADSC.23,24,31e33 This suggeststhat adult stem cells may not be as limited by lineage aspreviously thought and, in fact, manifest profound plasticity.
Recently, we showed how Schwann cell-like differenti-ated ADSC could enhance neurite outgrowth in vitro.4 Inthis current study, we have tested the ability of thedifferentiated ADSC to enhance nerve regeneration in vivo.We compared these cells with SC-differentiated MSCs andprimary adult SCs seeded in fibrin conduits.
Materials and Methods
Fibrin conduit
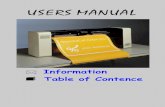
The fibrin conduit was prepared from two-compound fibringlue (Tisseel� Kit VH 1.0, Baxter SA, USA). Tisseel�contains fibrinogen, 70e110 mg ml�1; plasma fibronectin,2e9 mg ml�1; factor XIII, 10e50 U ml�1; plasminogen,40e120 mg ml�1; aprotinin solution 3000 KIU ml�1; thrombin4 IU ml�1; and calcium chloride 40 mmol l�1. Fibrin glue wasdispensed in a mould prepared from silicone arounda stainless steel core and pressed into shape for 5 min(Figure 1). This allows the generation of uniform conduitsmeasuring 14 mm in length, with a 2-mm lumen and 1-mmwall thickness designed to bridge a 10-mm gap in the leftsciatic nerve of 250 g adult Sprague-Dawley rats (Janvier,France).
Cell harvest
Schwann cellsAll cells were obtained from Sprague-Dawley rats (Janvier,France). These were euthanised by CO2 according to thelocal veterinary commission in Lausanne (Switzerland) andstudy was carried out in accordance with the EuropeanCommunity Council directive 86/609/ECC for the care anduse of laboratory animals.
To harvest Schwann cells, sciatic nerves were exposed,removed and kept in Dulbecco’s modified Eagle’s mediumplus glutamax (DMEM, Invitrogen, UK) containing 1% pen-icillinestreptomycin. Nerves were then dissected in trunks,de-sheathed and finally chopped in 1-mm segments. Thesegments were then plated in a Petri dish with SC growthmedium supplemented by 14 mM forskolin and 100 ng ml�1
neuregulin-1 b1 (R&D Systems, UK). The cells were incu-bated for 2 weeks at 37 �C with 5% CO2 with fresh mediumadded approximately every 72 h. After these 2 weeks,medium was aspirated and 0.125% (w/v) collagenase typeIV and 117 U mg�1 dispase were added to the Petri dish.After 24-h incubation, the cell suspension was filteredthrough a 70-mm cell strainer (Falcon; BD BiosciencesDiscovery Labware, Bedford, MA), centrifuged at 900 rpm
rived stem cells enhance peripheral nerve regeneration, J Plast

Figure 1 Preparation of fibrin conduits.A. The fibrin conduit (Tisseel�) with stainless steel wire inserted in the lumen as a spacerwhile the conduit is stored before implantation.B. The fibrin conduit shows an intact lumen after removal of the stainless steelwire.C. The fibrin conduits are stored in DMEM medium before being seeded with regenerative cells.D. A fibrin conduit implantedin vivo to repair a rat sciatic nerve injury.
ARTICLE IN PRESS
Adipose-derived stem cells enhance peripheral nerve regeneration 3
+ MODEL
for 5 min to obtain the cell pellet. Finally, the cell pelletwas re-suspended in SC growth medium, seeded into25-cm2 flask precoated with poly-D-lysine (Sigma, St Louis,MO, USA) and incubated in the same conditions. Thefollowing day, the medium was freshly changed and thecells were left to proliferate. At confluence, the SCs werepurified by an antibody complement method to eradicatethe remaining fibroblasts.13,17,34
Adipose-derived stem cellsAdipose-derived stem cells were harvested as describedpreviously.4 After euthanasia, the inguinal fat pad was care-fully dissected and minced using a sterile razor blade. Thetissue was enzymatically digested for 2 h at 37 �C using 0.15%(w/v) collagenase type I (Invitrogen, UK). The solution waspassed through a 70-mm filter to remove undissociated tissue,neutralised by adding modified Eagle’s medium (a-MEM;Invitrogen, UK) containing 10% (v/v) foetal bovine serum(FBS) and centrifuged at 800� g for 5 min. The stromal cellpellet was re-suspended in MEM containing 10% (v/v) FBS and1% (v/v) penicillin/streptomycin solution. The cultures weremaintained at sub-confluent levels in a 37 �C incubator with5% CO2 and passaged with trypsin/ethylenediaminetetra-acetic acid (EDTA) (Invitrogen, UK) when required.
Bone-marrow-derived mesenchymal stem cellsMSCs were harvested from adult Sprague-Dawley rat femoralbones34: mesenchymal cell growth medium (MEM- a; Invi-trogen; supplemented with 10% FBS (v/v) and 1% penicillinestreptomycin) was injected through each marrow cavity using
Please cite this article in press as: di Summa PG et al., Adipose-deReconstr Aesthet Surg (2009), doi:10.1016/j.bjps.2009.09.012
a 21-guage needle. The resulting cell suspension was tritu-rated, filtered through a 70-mm Falcon filter and centrifugedfor 5 min at 600 g. The supernatant was aspirated, the cellbolus re-suspended in mesenchymal cell growth medium andthe cells plated in 75-cm2 tissue culture flasks and incubatedin 5% CO2 at 37 �C. Haematopoietic cells were eliminated bywashing daily with DMEM until all the non-adherent cells wereremoved. The cells were then allowed to grow to confluence.
Stem cell differentiation
The multi-potent nature of the cell cultures was tested byensuring their ability to differentiate along various lineages,as previously described.4,34 Further, undifferentiated ADSCsand MSCs were differentiated into an SC-like phenotype atearly passages.4,18 Growth medium was removed from sub-confluent cultures and replaced with medium supplementedwith 1 mM b-mercaptoethanol (Sigma-Aldrich, UK) for 24 h.The cells were then washed and fresh medium supplementedwith 35 ng ml�1 all-trans-retinoic acid was added. A further72 h later, the cells were washed and the medium replacedwith differentiation medium; cell growth medium supple-mented with 5 ng mle1 platelet-derived growth factor (PDGF;PeproTech Ltd., UK), 10 ng ml�1 basic fibroblast growth factor(bFGF; PeproTech Ltd., UK), 14 mM forskolin and 200 ng ml�1
neuregulin-1 b1. The cells were incubated for 2 weeks underthese conditions with fresh medium added approximatelyevery 72 h. To confirm the effectiveness of the differentiationof ADSC and their similarity to the Schwann cell population,we performed cell immunostaining for typical Schwann cells
rived stem cells enhance peripheral nerve regeneration, J Plast

ARTICLE IN PRESS
4 P.G. di Summa et al.
+ MODEL
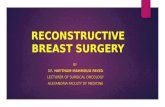
markers S100 and GFAP.4 Cultures of differentiated ADSC(dADSC) and SC were compared by immunostaining: the cellswere incubated with mouse anti-glial fibrillary acidic protein(GFAP; 1:500; LabVision, USA) and rabbit anti-S100 (1:500;Dako, Denmark) overnight at 4 �C. Phosphate-buffered solu-tion (PBS)-washed slides were then treated with goat anti-rabbit FITC (1:100; Vector Labs, UK) and goat anti-mouse CY3(1:200; Amersham, UK) conjugated secondary antibodies.Slides were examined using an Olympus IX51 inverted fluo-rescence microscope. The dADSCs showed similar immuno-cytochemical properties when compared with SCs (Figure 2).Bone-marrow-derived MSCs were differentiated (dMSC) ina similar manner as previously shown.34
Cell seeding and microsurgery
A couple of hours before implantations in rats, the cellswere trypsinised and, after centrifugation, 2� 106 cellswere suspended in 50 ml of differentiation medium andinjected into the fibrin tubes. To avoid cell dispersion duringthe procedure, one side of the fibrin tube was previouslycapped by a fibrin glue clot. Before implantation, the fibrinconduit was easily decapped from the fibrin clots at its ends.The control group in the absence of cells (empty) wassimilarly filled with 50 ml of differentiation medium alone.The sciatic nerve was transected and nerve ends were fixedto the conduit by a single epineural suture (9/0 Prolene,Ethicon): proximal and distal nerve stumps were inserted2 mm into the tube, thus leaving a 10-mm gap. Muscles andfascia layers were closed with single resorbable stitches (4/0 Softcat, Braun) and the skin by a continuous runningsuture (4/0 Prolene, Ethicon). The various groups of fibrinconduits (each one formed by six animals for a total n Z 24)were left in place for 2 weeks and subsequently harvestedtogether with the proximal and distal nerve stumps.
Nerve conduit harvesting andimmunohistochemistry
Animals were sacrificed after 2 weeks by CO2 chambereuthanasia. Harvested conduits were fixed by para-formaldehyde (PFA) for 16 h, then rinsed 24 h at 4 �C in PBScontaining 30% sucrose and 0.1% sodium azide, with PBSchanges after about 12 h to eliminate any PFA remnants.The specimens were then embedded in OCT freezing media(Tissue-tek, Sakura, Japan), and longitudinal cryo-sections(14 mm) were prepared onto slides (Superfrost� plus,Menzel-Glaser, Germany).
After 3� 5 min PBS washes, a casein blocking solutionwas applied for 1 h before incubating slides overnight withprimary antibodies rabbit anti-S100 (1:500, Dako, UK) andrabbit anti-PGP 9.5 (1:500, Dako, UK). The following dayafter 3� 5 min PBS washes, slides were incubated withsecondary antibody (1:500, Alexa Fluor goat anti-rabbit,Invitrogen, USA) at room temperature in the dark for40 min. After 3� 5 min PBS washes, the slides were finallymounted with Vectashield with DAPI (Vector Labs, UK) andexamined under the fluorescence microscope(10�magnification) with the regenerating conus directedtowards the distal end.35 Axonal regeneration distance(PGP 9.5) and S100 positive cell distribution inside the
Please cite this article in press as: di Summa PG et al., Adipose-deReconstr Aesthet Surg (2009), doi:10.1016/j.bjps.2009.09.012
conduit were evaluated using an optical microgrid: thelength was measured from the beginning of the conduit tothe last visible sprout of the regenerating conus.
Statistical analysis
One-way analysis of variance (ANOVA) with Bonferronimultiple comparison test was used to statistically analysedata (GraphPad Prism). Significance was determined as*P< 0.05, **P< 0.01 and ***P< 0.001.
Results
Cell seeding and conduit properties
Prior to in vivo experiments, we tested the fibrin conduit andits capacity to retain cells within. We filled two differentfibrin conduits with ADSC (80� 106 ml�1 cell concentration),then we fixed them at 48 h. By DAPI staining, we found a goodcapacity of fibrin of retaining cells inside the lumen(Figure 3). Fibrin conduits were easy to handle and micro-surgical suture was uneventful. All animals survived; none ofthe animals developed infections or surgical complicationsexcept autotomy, which was present in one case out of 24.After 2 weeks in vivo, fibrin conduits showed an intactstructure, with proximal and distal ends partially resorbed.No signs of haematoma or infection were detected.
Axon regeneration
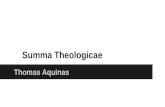
Sciatic nerve axonal regeneration was different depending onthe type of cells which had been seeded in the fibrin conduits.Axonal regeneration distance was assessed proximally by PGP9.5 immunohistochemistry (Figure 4). Conduits filled with SCsshowed the best regeneration distance (5.758� 0.12 mm)followed by fibrin containing dMSC (4.986� 0.19 mm) ordADSC (4.968� 0.22 mm) (Figure 6A). All three groups withcells resulted in better regeneration than the empty fibrinconduit group (4.155� 0.07 mm). PGP 9.5 positive axons wereassociated with S100 positive cells at the proximal regener-ating stumps (Figure 5). The distances of S100 positive cellmigration at the stumps showed a similar pattern to PGP 9.5:the SC group (5.858� 0.13 mm) followed by conduits con-taining dMSC (5.035� 0.21 mm) or dADSC (5.032� 0.20 mm)and empty fibrin conduits (4.108� 0.08 mm) (Figure. 6B).
Statistical analysis showed that fibrin conduits seededwith SC significantly improved axonal regenerationdistance, and proximal SC invasion compared with theempty fibrin conduit (** p< 0.01). Differentiated adult stemcells also showed a positive impact on nerve regenerationwith a significantly enhanced nerve regeneration distance(dADSC vs. empty: p< 0.05 PGP 9.5 and p< 0.01 S100;dMSC vs. empty: p< 0.01 for both PGP 9.5 and S100). Nosignificant difference was noticed between the dADSCgroup and the dMSC group with either staining.
Discussion
In this study, we analysed the behaviour of fibrin conduitsseeded with different cell populations as a nerve guide to
rived stem cells enhance peripheral nerve regeneration, J Plast

Figure 2 Differentiation of stem cells, dADSC and SC immunostained for S100 (green), GFAP (red) and DAPI (blue). Differenti-ation of ADSC resulted in 40% of cells co-expressing the SC markers and with a bipolar elongated morphology. SC cultures wereroutinely >97% positive for both S100 and GFAP indicating the absence of significant quantities of contaminating fibroblast cells.
ARTICLE IN PRESS
Adipose-derived stem cells enhance peripheral nerve regeneration 5
+ MODEL
Please cite this article in press as: di Summa PG et al., Adipose-derived stem cells enhance peripheral nerve regeneration, J PlastReconstr Aesthet Surg (2009), doi:10.1016/j.bjps.2009.09.012

Figure 3 Analysis of cell seeding. A. Haematoxylin staining of a fibrin conduit seeded with cells in vitro and (B) shown at highmagnification.C DAPI staining of a fibrin conduit seeded with cells in vitro and (D) shown at high magnification.
ARTICLE IN PRESS
6 P.G. di Summa et al.
+ MODEL
repair sciatic nerve injury. We compared the regenerationachievable with SC, dADSC, dMSC and with an emptyconduit. First, we found that all conduits seeded with cellssupported axonal regeneration without collapsing andretained a lumen, which provides a permissive environmentfor regeneration.
No signs of haematoma or infection were detected atexplantations, confirming the good tissue acceptance offibrin without altering the tissue environment at theimplantation side. Moreover, first signs of resorption at the
Figure 4 PGP 9.5 staining shows axonal regeneration in thefibrin conduits either empty or seeded with different regenera-tive cells. A. Empty fibrin conduit. B. Fibrin conduitþ dADSC.C. Fibrin conduitþ dMSC. D. Fibrin conduitþ SC.
Please cite this article in press as: di Summa PG et al., Adipose-deReconstr Aesthet Surg (2009), doi:10.1016/j.bjps.2009.09.012
edges were noted after 2 weeks in vivo, displaying biode-gradability of the fibrin conduit. The porous structure ofthe conduit, already noted with in vitro experiments,8
seems to allow passage of neurotrophic factors into thelumen, the surface of fibrin forms a barrier preventingfibrous tissue to invade the lumen.36
Fibrin has been previously used as a matrix for MSC cellsuspension37 and as a new nerve guide8: our results showthat, at least in the short term, the fibrin conduit can be
Figure 5 S100 staining shows the proximal Schwann cellmigration in the fibrin conduits either empty or seededwith different regenerative cells. A. Empty fibrin conduit.B. Fibrin conduitþ dADSC. C. Fibrin conduitþ dMSC. D. Fibrinconduitþ SC.
rived stem cells enhance peripheral nerve regeneration, J Plast

Figure 6 Quantification of regeneration distances measured with (A) PGP 9.5 and (B) S100 cell staining. Graphs showa significant improvement in axon regeneration distance in all groups (dADSC, dMSC, SC), when compared with the empty fibringroup. Values are mean distances (mm)� SEM. (* p< 0.05; ** p< 0.01; *** p< 0.001).
ARTICLE IN PRESS
Adipose-derived stem cells enhance peripheral nerve regeneration 7
+ MODEL
optimised by cell delivery, resulting in higher peripheralnerve regeneration.
The best regenerative values were found combiningfibrin conduits and SC. This should be expected, given thecrucial role covered by SCs in nerve regeneration and increating the adequate environment through which regen-erating axons grow to reach their peripheral targets.12
Indeed, SCs were injected for the first time into a fibrinconduit, giving encouraging results, with a better regen-erating distance when compared statistically with theempty fibrin conduit. These data seem to strengthen theargument that SC can help in enhancing nerve regenerationwhen seeded in a conduit.10,14
Concerning dMSC and dADSC, we also detected a statis-tically significant improvement in nerve regenerationdistance (PGP 9.5 staining, respectively, 4.986 and 4.968for dMSC and dADSC vs. 4.155 in the empty fibrin conduit).From these data, we could argue that, even if these cellsstill not reach the full regenerative potential of SC, theycan play an effective role in nerve regeneration. Interest-ingly, we could find that dADSC promote regeneration in thesame manner as dMSC (difference between the two groupsp> 0.05) as we saw reporting overlapping results when wecompared the axonal regeneration distance (PGP 9.5) andSC invasion (S100) for the two groups.
This seems to confirm the previously reported similari-ties between these two cell populations, concerningmorphology,38 immune phenotype39 and trans-differentia-tion capacity along mesodermal27 and non-mesodermallineages.26,40 This equivalence of dADSC and dMSC in
Please cite this article in press as: di Summa PG et al., Adipose-deReconstr Aesthet Surg (2009), doi:10.1016/j.bjps.2009.09.012
promoting peripheral nerve regeneration can be promising,considering the already successful application of MSCin vivo in the longer-term group.14,34,35 Stem cells could aidregeneration by the release of soluble nerve growth factorssuch as brain-derived neurotrophic factor41 or angiogenicmolecules, including vascular endothelial growth factor.42
Other studies have shown that dMSC can physically engraftand myelineate regenerating axons in vivo20, suggestingthat multiple mechanisms may exist in stem cell therapy.
In terms of future clinical use, humans have abundantsubcutaneous fat deposits, and ADSCs can be isolated inlarge quantities by conventional liposuction procedureunder local anaesthesia, thus overcoming the discomfortand the tissue morbidity associated with bone marrowaspiration and showing potential advantages for tissueengineering application, compared with MSC.40,43,44
Furthermore, the frequency of MSCs in bone marrow rangesbetween 1 in 25 000 to 1 in 100 000,45 whereas ADSCsconstitute a more abundant proportion, approximately 2%of lipoaspirate cells.25,28
The promising results achieved from the combination ofregenerative cells and fibrin conduit are hopeful steps forfuture clinical applications in cases of peripheral nerveinjury. Similarly, the interesting outcomes obtained fromthe dADSCs, which appear comparable to the dMSC,underline the effectiveness of this cell population and theirpromising applications in nerve regeneration. A longer-termgroup will be necessary to confirm the positive effects onfunctional recovery and to see if dADSC will maintain thissimilarity compared with dMSC.
rived stem cells enhance peripheral nerve regeneration, J Plast

ARTICLE IN PRESS
8 P.G. di Summa et al.
+ MODEL
Acknowledgements
We thank Professor Daniel V. Egloff, director of thedepartment for plastic surgery CHUV for his support anduseful comments to this project and Catherine PythoudBSc, Jean Francois Brunet PhD for technical support. Theauthors are grateful to the SwissLife Foundation, the SUVAand the University of Lausanne FBM for their financialsupport.
Conflict of Interest
None.
References
1. Chalfoun CT, Wirth GA, Evans GR. Tissue engineered nerveconstructs: where do we stand? J Cell Mol Med 2006;10:309e17.
2. Hu J, Zhu QT, Liu XL, et al. Repair of extended peripheralnerve lesions in rhesus monkeys using acellular allogenic nervegrafts implanted with autologous mesenchymal stem cells. ExpNeurol 2007;204:658e66.
3. Marchesi C, Pluderi M, Colleoni F, et al. Skin-derived stem cellstransplanted into resorbable guides provide functional nerveregeneration after sciatic nerve resection. Glia 2007;55:425e38.
4. Kingham PJ, Kalbermatten DF, Mahay D, et al. Adipose-derivedstem cells differentiate into a Schwann cell phenotype andpromote neurite outgrowth in vitro. Exp Neurol 2007;207:267e74.
5. Battiston B, Tos P, Conforti LG, et al. Alternative techniquesfor peripheral nerve repair: conduits and end-to-side neuro-rrhaphy. Acta Neurochir Suppl 2007;100:43e50.
6. Bain JR, Mackinnon SE, Hudson AR, et al. The peripheral nerveallograft in the primate immunosuppressed with Cyclosporin A:I. Histologic and electrophysiologic assessment. Plast ReconstrSurg 1992;90:1036e46.
7. Mohanna PN, Terenghi G, Wiberg M. Composite PHB-GGFconduit for long nerve gap repair: a long-term evaluation.Scand J Plast Reconstr Surg Hand Surg 2005;39:129e37.
8. Kalbermatten DF, Pettersson J, Kingham PJ, et al. New fibrinconduit for peripheral nerve repair. J Reconstr Microsurg 2009;25:27e33.
9. Kalbermatten DF, Kingham PJ, Mahay D, et al. Fibrin matrix forsuspension of regenerative cells in an artificial nerve conduit.J Plast Reconstr Aesthet Surg 2008;61:669e75.
10. Stang F, Fansa H, Wolf G, et al. Structural parameters ofcollagen nerve grafts influence peripheral nerve regeneration.Biomaterials 2005;26:3083e91.
11. Terenghi G. Peripheral nerve regeneration and neurotrophicfactors. J Anat 1999;194:1e14.
12. Rodriguez FJ, Verdu E, Ceballos D, et al. Nerve guides seededwith autologous schwann cells improve nerve regeneration.Exp Neurol 2000;161:571e84.
13. Mosahebi A, Woodward B, Wiberg M, et al. Retroviral labelingof Schwann cells: in vitro characterization and in vivo trans-plantation to improve peripheral nerve regeneration. Glia2001;34:8e17.
14. Pereira Lopes FR, Camargo de Moura Campos L, DiasCorrea Jr J, et al. Bone marrow stromal cells and resorbablecollagen guidance tubes enhance sciatic nerve regeneration inmice. Exp Neurol 2006;198:457e68.
15. Kamada T, Koda M, Dezawa M, et al. Transplantation of bonemarrow stromal cell-derived Schwann cells promotes axonal
Please cite this article in press as: di Summa PG et al., Adipose-deReconstr Aesthet Surg (2009), doi:10.1016/j.bjps.2009.09.012
regeneration and functional recovery after complete transec-tion of adult rat spinal cord. J Neuropathol Exp Neurol 2005;64:37e45.
16. Azizi SA, Stokes D, Augelli BJ, et al. Engraftment and migrationof human bone marrow stromal cells implanted in the brains ofalbino ratsesimilarities to astrocyte grafts. Proc Natl Acad SciU S A 1998;95:3908e13.
17. Tohill M, Terenghi G. Stem-cell plasticity and therapy forinjuries of the peripheral nervous system. Biotechnol ApplBiochem 2004;40:17e24.
18. Dezawa M, Takahashi I, Esaki M, et al. Sciatic nerve regenerationin rats induced by transplantation of in vitro differentiatedbone-marrow stromal cells. Eur J Neurosci 2001;14:1771e6.
19. Tohill MP, Mann DJ, Mantovani CM, et al. Green fluorescentprotein is a stable morphological marker for schwann celltransplants in bioengineered nerve conduits. Tissue Eng 2004;10:1359e67.
20. Keilhoff G, Goihl A, Langnase K, et al. Transdifferentiation ofmesenchymal stem cells into Schwann cell-like myelinatingcells. Eur J Cell Biol 2006;85:11e24.
21. Kokai LE, Rubin JP, Marra KG. The potential of adipose-derivedadult stem cells as a source of neuronal progenitor cells. PlastReconstr Surg 2005;116:1453e60.
22. Prunet-Marcassus B, Cousin B, Caton D, et al. From heteroge-neity to plasticity in adipose tissues: site-specific differences.Exp Cell Res 2006;312:727e36.
23. Safford KM, Rice HE. Stem cell therapy for neurologic disor-ders: therapeutic potential of adipose-derived stem cells. CurrDrug Targets 2005;6:57e62.
24. Zuk PA, Zhu M, Mizuno H, et al. Multilineage cells from humanadipose tissue: implications for cell-based therapies. TissueEng 2001;7:211e28.
25. Strem BM, Hicok KC, Zhu M, et al. Multipotential differentiationof adipose tissue-derived stemcells. Keio J Med 2005;54:132e41.
26. Guilak F, Lott KE, Awad HA, et al. Clonal analysis of thedifferentiation potential of human adipose-derived adult stemcells. J Cell Physiol 2006;206:229e37.
27. Schaffler A, Buchler C. Concise review: adipose tissue-derivedstromal cellsebasic and clinical implications for novel cell-based therapies. Stem Cells 2007;25:818e27.
28. Fraser JK, Wulur I, Alfonso Z, et al. Fat tissue: an underap-preciated source of stem cells for biotechnology. TrendsBiotechnol 2006;24:150e4.
29. Sanchez-Ramos J, Song S, Cardozo-Pelaez F, et al. Adult bonemarrow stromal cells differentiate into neural cells in vitro.Exp Neurol 2000;164:247e56.
30. Safford KM, Hicok KC, Safford SD, et al. Neurogenic differen-tiation of murine and human adipose-derived stromal cells.Biochem Biophys Res Commun 2002;294:371e9.
31. Ashjian PH, Elbarbary AS, Edmonds B, et al. In vitro differen-tiation of human processed lipoaspirate cells into early neuralprogenitors. Plast Reconstr Surg 2003;111:1922e31.
32. Safford KM, Safford SD, Gimble JM, et al. Characterization ofneuronal/glial differentiation of murine adipose-derived adultstromal cells. Exp Neurol 2004;187:319e28.
33. Wang B, Han J, Gao Y, et al. The differentiation of ratadipose-derived stem cells into OEC-like cells on collagenscaffolds by co-culturing with OECs. Neurosci Lett 2007;421:191e6.
34. Caddick J, Kingham PJ, Gardiner NJ, et al. Phenotypic andfunctional characteristics of mesenchymal stem cells differ-entiated along a Schwann cell lineage. Glia 2006;54:840e9.
35. Tohill M, Mantovani C, Wiberg M, et al. Rat bone marrowmesenchymal stem cells express glial markers and stimulatenerve regeneration. Neurosci Lett 2004;362:200e3.
36. Takazawa R, Yamato M, Kageyama Y, et al. Mesothelial cellsheets cultured on fibrin gel prevent adhesion formation in anintestinal hernia model. Tissue Eng 2005;11:618e25.
rived stem cells enhance peripheral nerve regeneration, J Plast

ARTICLE IN PRESS
Adipose-derived stem cells enhance peripheral nerve regeneration 9
+ MODEL
37. Bensaid W, Triffitt JT, Blanchat C, et al. A biodegradable fibrinscaffold for mesenchymal stem cell transplantation. Bioma-terials 2003;24:2497e502.
38. Kern S, Eichler H, Stoeve J, et al. Comparative analysis ofmesenchymal stem cells from bone marrow, umbilical cordblood, or adipose tissue. Stem Cells 2006;24:1294e301.
39. Gimble JM, Katz AJ, Bunnell BA. Adipose-derived stem cells forregenerative medicine. Circ Res 2007;100:1249e60.
40. Zuk PA, Zhu M, Ashjian P, et al. Human adipose tissue is a sourceof multipotent stem cells. Mol Biol Cell 2002;13:4279e95.
41. Zhao L, Wei X, Ma Z, et al. Adipose stromal cells-conditionalmedium protected glutamate-induced CGNs neuronal death byBDNF. Neurosci Lett 2009;452:238e40.
Please cite this article in press as: di Summa PG et al., Adipose-deReconstr Aesthet Surg (2009), doi:10.1016/j.bjps.2009.09.012
42. Rehman J, Traktuev D, Li J, et al. Secretion of angiogenic andantiapoptotic factors by human adipose stromal cells. Circu-lation 2004;109:1292e8.
43. Tholpady SS, Katz AJ, Ogle RC. Mesenchymal stem cells fromrat visceral fat exhibit multipotential differentiation in vitro.Anat Rec A Discov Mol Cell Evol Biol 2003;272:398e402.
44. Matsumoto T, Kano K, Kondo D, et al. Mature adipocyte-derived dedifferentiated fat cells exhibit multilineage poten-tial. J Cell Physiol 2008;215:210e22.
45. Banfi A, Bianchi G, Galotto M, et al. Bone marrow stromaldamage after chemo/radiotherapy: occurrence, consequencesand possibilities of treatment. Leuk Lymphoma 2001;42:863e70.
rived stem cells enhance peripheral nerve regeneration, J Plast