Journal of Idiophatic Scoliosis in Adolescents
16
2013 Massachusetts Medical Society Aut hor : M. Timothy Hresko, M.D. Tutor : dr. Maksum Pandelima Sp.OT Louise Andre 07700217
-
Upload
louiseandre -
Category
Documents
-
view
218 -
download
0
Transcript of Journal of Idiophatic Scoliosis in Adolescents

7/27/2019 Journal of Idiophatic Scoliosis in Adolescents
http://slidepdf.com/reader/full/journal-of-idiophatic-scoliosis-in-adolescents 1/16
2013 Massachusetts Medical Society
Author : M. Timothy Hresko, M.D.
Tutor : dr. Maksum Pandelima Sp.OT
Louise Andre
07700217

7/27/2019 Journal of Idiophatic Scoliosis in Adolescents
http://slidepdf.com/reader/full/journal-of-idiophatic-scoliosis-in-adolescents 2/16
clinical practice A 12-year-old girl presents with her parents after a
positive school screening for scoliosis.
Physical examination reveals shoulder and torsoasymmetry with trunk imbalance (i.e., shift fromthe midline). Neurologic and skin examinationsare normal.
How should the patient be evaluated and treated?

7/27/2019 Journal of Idiophatic Scoliosis in Adolescents
http://slidepdf.com/reader/full/journal-of-idiophatic-scoliosis-in-adolescents 3/16
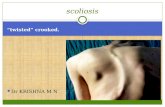
The Clinical Problem Scoliosis is the most common deformity of the spine.
Scoliosis is defined as a lateral curvature of the spine
that is 10 degrees or greater on a coronal radiographicimage while the patient is in a standing position

7/27/2019 Journal of Idiophatic Scoliosis in Adolescents
http://slidepdf.com/reader/full/journal-of-idiophatic-scoliosis-in-adolescents 4/16
Scoliosis is typically categorized according to cause
Congenital
scoliosis
Neuromuscularscoliosis
Idiopathicscoliosis
is an anatomical anomaly due to failure of formation orsegmentation of the vertebral column which, with growth, may
lead to progressive spinal deformity
In most patients with scoliosis, however,the cause is unrecognized
is deformity caused by dysfunction of the centralnervous system

7/27/2019 Journal of Idiophatic Scoliosis in Adolescents
http://slidepdf.com/reader/full/journal-of-idiophatic-scoliosis-in-adolescents 5/16
In the growing child, the primary complication of scoliosis is disfigurement of the torso with shoulder or waist asymmetry, trunk imbalance, or rib rotation.
Adolescent patients with thoracic scoliosis of greaterthan 50 degrees are at increased risk for shortness of
breath later in life
Lung volumes are diminished as compared with norms
when thoracic idiopathic scoliosis reaches 70 degrees,and symptomatic restrictive pulmonary disease iscommon in patients with a curve magnitude thatexceeds 100 degrees

7/27/2019 Journal of Idiophatic Scoliosis in Adolescents
http://slidepdf.com/reader/full/journal-of-idiophatic-scoliosis-in-adolescents 6/16
Evaluation Figure 1. Inclinometer Test.
The patient is bent forward withthe knees in extension and thearms reaching toward the feet withthe palms together.
The inclinometer is placed at theapex of the rib deformity, and the view is of the “horizon” of thespine.

7/27/2019 Journal of Idiophatic Scoliosis in Adolescents
http://slidepdf.com/reader/full/journal-of-idiophatic-scoliosis-in-adolescents 7/16
Axial rotation of the trunk on the Adams test can be
quantified with an inclinometer; rotation of less than
7 degrees is associated with a 95% probability of acurve that is less than 30 degrees on radiography
Skin examination is warranted to rule outmanifestations of neurofibromatosis

7/27/2019 Journal of Idiophatic Scoliosis in Adolescents
http://slidepdf.com/reader/full/journal-of-idiophatic-scoliosis-in-adolescents 8/16
Spinal radiography remains the standard of imagingfor the evaluation of scoliosis.
A posteroanterior radiograph of the spine from C7 tothe iliac crest is recommended, obtained with digital-imaging enhancement with the patient in a standingposition (Fig. 2)

7/27/2019 Journal of Idiophatic Scoliosis in Adolescents
http://slidepdf.com/reader/full/journal-of-idiophatic-scoliosis-in-adolescents 9/16
Figure 2. PosteroanteriorRadiograph of the Spine in a Patient with an
Immature Skeleton.
The radiograph, which was obtained while the patient was in a standing
position, shows a right thoracicscoliosis of 26 degrees from the 4thto the 10th thoracic vertebrae, whichis typical of an idiopathic scoliosis.
A secondary curve of 15 degrees tothe left is shown in the lumbar
spine. The Cobb angle of measurement of scoliosis is definedas the angle between a line parallelto the superior vertebrae and a lineat the inferior vertebrae of thecurve.

7/27/2019 Journal of Idiophatic Scoliosis in Adolescents
http://slidepdf.com/reader/full/journal-of-idiophatic-scoliosis-in-adolescents 10/16
Magnetic resonance imaging (MRI) is useful in theevaluation of an abnormality of the neural axis, but itis not routinely required.

7/27/2019 Journal of Idiophatic Scoliosis in Adolescents
http://slidepdf.com/reader/full/journal-of-idiophatic-scoliosis-in-adolescents 11/16
Treatment
Nonoperative Therapy
Many nonoperative treatment options, such asphysical therapy, surface electrical stimulation,
and chiropractic treatment
Many nonoperative treatment options, such asphysical therapy, surface electrical stimulation, and
chiropractic treatment, have been proposed, butsupporting data are lacking from controlled studies.

7/27/2019 Journal of Idiophatic Scoliosis in Adolescents
http://slidepdf.com/reader/full/journal-of-idiophatic-scoliosis-in-adolescents 12/16
Treatment with the use of a rigid thoracolumbarorthotic brace is currently preferred for children3 yearsof age through adolescence who are at risk forprogressive scoliosis (i.e., patients with a curvemagnitude of 25 to 45 degrees and considerable
growth remaining).

7/27/2019 Journal of Idiophatic Scoliosis in Adolescents
http://slidepdf.com/reader/full/journal-of-idiophatic-scoliosis-in-adolescents 13/16
Operative Treatment Operative treatment is indicated when progressive
scoliosis exceeds 45 degrees in patients with animmature skeleton or when progression or associated
pain occurs after skeletal maturity
Involved a spinal fusion and internal fixation with astainless-steel Harrington rod to maintain the spine in
a straighter position.

7/27/2019 Journal of Idiophatic Scoliosis in Adolescents
http://slidepdf.com/reader/full/journal-of-idiophatic-scoliosis-in-adolescents 14/16
Infection is a major concern
Early postoperative infections (within 3 months)
complicate approximately 1% of operations inotherwise healthy adolescents and are usually due to
Staphylococcus aureus or streptococcus
Late-onset infections (>1 year after the operation),
generally caused by Propionibacterium acnes or S.epidermidis

7/27/2019 Journal of Idiophatic Scoliosis in Adolescents
http://slidepdf.com/reader/full/journal-of-idiophatic-scoliosis-in-adolescents 15/16
Conclusions
and Recommendations The patient in the vignette has findings on a physical
examination that are typical of idiopathic scoliosis(uneven shoulders, rib prominence on the forward-bend Adams test, and no skin, extremity, or neurologicfindings to suggest a secondary cause)
If the patient has a curvature of 20 degrees or greaterand an immature skeleton, referral to an orthopedicsurgeon is appropriate.

7/27/2019 Journal of Idiophatic Scoliosis in Adolescents
http://slidepdf.com/reader/full/journal-of-idiophatic-scoliosis-in-adolescents 16/16
Brace treatment is commonly recommended forpatients with a curve magnitude of 25 to 45 degreesand clinically significant growth remaining, but it
requires adherence to the recommended number of hours of treatment (usually ≥12 hours daily) until theskeleton is mature
In addition, the benefits of brace treatment versus
watchful waiting remain unclear, pending results of anongoing randomized trial. Surgery is indicated inpatients with an immature skeleton if progressivescoliosis exceeds 45 degrees.