Journal of Clinical Dentistry · Colgate ProClinical A1500 electric toothbrush, electronic sensors...
40
SENIOR EDITOR Robert C. Emling, EdD EDITORIAL BOARD Caren M. Barnes, RDH, MS Annerose Borutta, Prof.Dr.med.habil. Robert L. Boyd, DDS, MEd Neil W. Brayton, DDS Kenneth H. Burrell, DDS, MS Mark E. Cohen, PhD David Drake, MS. PhD Heinz Duschner, Prof.Dr. William Michael Edgar, PhD, DDSc, FDSRCS Denise Estafan, DDS, MS Stuart L. Fischman, DMD Rosa Helena Miranda Grande, DDS, PhD John J. Hefferren, PhD Mark E. Jensen, DDS, PhD Carl J. Kleber, MSD, PhD Israel Kleinberg, DDS, PhD, DSc Karl F. Leinfelder, DDS, MS Jonathan Mann, DMD, MSc Kenneth Markowitz, DDS Milton V. Marshall, PhD, DABT Pier Francesco Porciani, MD, MScD Howard M. Proskin, PhD Mark S. Putt, MSD, PhD Bruce R. Schemehorn, MS Warren Scherer, DDS Jon B. Suzuki, DDS, PhD, MBA Jason M. Tanzer, DMD, PhD Norman Tinanoff, DDS, MS Henry O. Trowbridge, DDS, PhD Richard I. Vogel, DMD James S. Wefel, PhD Anthony E. Winston, BSc Wayne T. Wozniak, PhD Stefan Zimmer, Prof. Dr. med dent. PUBLISHER Stephen M. Siegel The Journal of Clinical Dentistry ® THE INTERNATIONAL JOURNAL OF APPLIED DENTAL RESEARCH www.JClinDent.com The Journal of Clinical Dentistry (ISSN 0895-8831) is published by Professional Audience Communications, Inc., P.O. Box 243,Yardley, PA 19067. POSTMASTER; Send address change to P.O. Box 243,Yardley, PA 19067. Copyright © 2012 by the YES Group, Inc. All rights reserved. No part of this publication may be reproduced without written permission from the publisher. Volume XXIII 2012 Special Issue A
Transcript of Journal of Clinical Dentistry · Colgate ProClinical A1500 electric toothbrush, electronic sensors...

SENIOR EDITORRobert C. Emling, EdD
EDITORIAL BOARDCaren M. Barnes, RDH, MSAnnerose Borutta, Prof.Dr.med.habil.Robert L. Boyd, DDS, MEdNeil W. Brayton, DDSKenneth H. Burrell, DDS, MSMark E. Cohen, PhDDavid Drake, MS. PhDHeinz Duschner, Prof.Dr.William Michael Edgar, PhD, DDSc,FDSRCSDenise Estafan, DDS, MSStuart L. Fischman, DMDRosa Helena Miranda Grande, DDS, PhDJohn J. Hefferren, PhDMark E. Jensen, DDS, PhDCarl J. Kleber, MSD, PhDIsrael Kleinberg, DDS, PhD, DScKarl F. Leinfelder, DDS, MSJonathan Mann, DMD, MScKenneth Markowitz, DDSMilton V. Marshall, PhD, DABTPier Francesco Porciani, MD, MScDHoward M. Proskin, PhDMark S. Putt, MSD, PhDBruce R. Schemehorn, MSWarren Scherer, DDSJon B. Suzuki, DDS, PhD, MBAJason M. Tanzer, DMD, PhDNorman Tinanoff, DDS, MSHenry O. Trowbridge, DDS, PhDRichard I. Vogel, DMDJames S. Wefel, PhDAnthony E. Winston, BScWayne T. Wozniak, PhDStefan Zimmer, Prof. Dr. med dent.
PUBLISHERStephen M. Siegel
TheJournal of
Clinical Dentistry®THE INTERNATIONAL JOURNAL OF APPLIED DENTAL RESEARCH
www.JClinDent.com
The Journal of Clinical Dentistry (ISSN 0895-8831) is published by Professional Audience Communications, Inc., P.O. Box 243,Yardley, PA 19067.POSTMASTER; Send address change to P.O. Box 243,Yardley, PA 19067.
Copyright © 2012 by the YES Group, Inc. All rights reserved. No part of this publication may be reproduced without written permission from the publisher.
Volume XXIII 2012 Special Issue A

The Journal of Clinical Dentistry has been accepted for inclusion onMEDLINE, the BIOSIS, SCISEARCH, BIOMED tad EMBASE databases.and the Automatic Subject Citation Alert.
The Journal of Clinical Dentistry is dedicated to the publication of significant clinical and applied dental research and reviews. All scientific studies publishedin this Special Issue have been reviewed and approved by members of theEditorial Board on the basis of clarity, scientific accuracy and the application ofacceptable standards for the research presented. The publication of these articlesin no way implies an endorsement of the products listed therein by The Journalof Clinical Dentistry, its Editors, Editorial Board, or the Publisher.
The Journal of Clinical Dentistry is printed on recycled paper.

ContentsIntelligent Technology for Superior Cleaning of
Teeth and Gums. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A1John Gatzemeyer, Fotinos Panagakos
Comparative Efficacy of a Specially Engineered Sonic PoweredToothbrush with Unique Sensing and Control Technologiesto Two Commercially Available Power Toothbrusheson Established Plaque and Gingivitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A5
Farid Ayad, Dolores M. Petrone, Gerald N. Wachs, Luis R. Mateo,Patricia Chaknis, Fotinos Panagakos
A Clinical Study Comparing the Supragingival Plaqueand Gingivitis Efficacy of a Specially Engineered SonicPowered Toothbrush with Unique Sensing andControl Technologies to a Commercially AvailableManual Flat-Trim Toothbrush . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A11
Salim Nathoo, Suru Mankodi, Luis R. Mateo, Patricia Chaknis, Foti Panagakos
Laboratory Evaluation of Plaque Removal at Interproximal Sitesby a Specially Engineered Powered Toothbrush withUnique Sensing and Control Technologies . . . . . . . . . . . . . . . . . . . . . . . . A17
James H. Kemp, Caren M. Barnes, Christine M. Spirgel, Xiuren Shi, Samuel L. Yankell
Laboratory Evaluation of Extrinsic Stain Removal by aSpecially Engineered Sonic Powered Toothbrush withUnique Sensing and Control Technologies . . . . . . . . . . . . . . . . . . . . . . . . A21
Venda P. Maloney, James Kemp, Fotinos Panagakos, Luis R. Mateo
Ergonomic Audit of a Specially Engineered Sonic PoweredToothbrush with Unique Sensing and Control Technologies,the Sonicare FlexCare, and the Oral-B Smart Series 5000 . . . . . . . . . . . . A26
Gail Hunter, Laurie Burns, Brian Bone, Thomas Mintel, Eduardo Jimenez
Usability Research Study of a Specially Engineered SonicPowered Toothbrush with Unique Sensingand Control Technologies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A31
Gail Hunter, Laurie Burns, Brian Bone,Thomas Mintel, Eduardo Jimenez


Intelligent Technology for Superior Cleaning of Teeth and Gums
John Gatzemeyer, Fotinos Panagakos
Colgate-Palmolive Technology CenterPiscataway, NJ, USA
IntroductionEarly power toothbrushes, introduced commercially in the
1960s, were often designed based on the conventional manualtoothbrush. Movement generally simulated hand motion, back-and-forth or side-to-side, offering little cleaning advantage overmanual toothbrushes.1 These early commercially availablepower toothbrushes maintained a clear lack of superioritycompared with manual toothbrushes, and problems withmechanical breakdowns caused their sales to decreasesignificantly following their initial introduction.2
A new rechargeable electric toothbrush has been developedwhich demonstrates superior plaque removal and provides ahigher level of technology or “intelligence” to help users brushbetter than with similar devices, and reinforce dentalprofessional recommendations for tooth brushing. This wasachieved through a combination of high frequency cleaning,electronic sensors, and ergonomics. By acting in concert, thesefeatures help compensate for less-than-adequate brushingtechnique to achieve superior cleaning without significantretraining of the user.
Research into candidate technologies for oral care deviceswas conducted in a variety of global markets. This resulted in adetailed analysis of multiple technologies in an effort tounderstand the strengths and weaknesses of each, and toidentify a lead candidate for development. During the course ofthis assignment, sonic cleaning and, specifically, productsoffered by Omron Healthcare Company in Japan wereidentified as leads. Omron is a worldwide leader in medicalhome healthcare and wellness products using unique sensingand control technologies.3
Sensing and control refers to smart technologies (as seen incompact, lightweight, easy, efficient, fast, and optimal solutions)that, unlike conventional sensing technologies, are not limitedstrictly to data input function, but rather integrate the areas ofsensing and control to output high-value information forsubsequent human or system processing.
These guiding principles manifest themselves in the Colgate®
ProClinical™ A1500 electric toothbrush, which provides uniquesensing and control technologies that automatically select thebest bristle movement for the position in the mouth of thebrush to effectively remove plaque, while being gentle on thegums. This Special Issue of The Journal of Clinical Dentistrydiscusses the product attributes, and demonstrates how thisspecially engineered sonic powered toothbrush with uniquesensing and control technologies combines these key featuresinto an intelligent technology and design that automatically
adjusts the speed and motion of brush strokes for superiorcleaning of teeth and gums.
High Frequency CleaningTo consumers who have accepted that they need to do more
with their oral health, and to dental professionals who promoteeffective oral hygiene routines, there is understanding andagreement that a powered toothbrush provides more effectivecleaning than a manual toothbrush. The Colgate ProClinicalA1500 electric toothbrush uses high frequency brush strokeswhich are referred to as sonic (cleaning). Sonic is defined ashaving a frequency within the audibility range of the humanear, which is well established as being roughly 20Hz to 20kHz.Since all the modes of the Colgate ProClinical A1500 electrictoothbrush operate at a frequency range between 20,000–32,500strokes per minute, which translates to 334Hz–542Hz, thesemovements are in the frequency of those defined as sonic.
The Colgate ProClinical A1500 electric toothbrush has threesettings or modes: Auto, Optimum, and Deep Cleaning. Bypressing the Mode button on the handle display (Figure 1),these different modes provide high frequency or sonic bristlestrokes, while incorporating unique movements to enhance thecleaning effect for different parts of the mouth. The Auto Modefunction is designed to allow the brush to automatically adjustas the handle is rotated by the user to different orientations in
A1
Figure 1. Model A1500 LED handle display in Auto Mode at 45º angle.

the mouth. These automatic adjustments are signaled to the userby audible speed changes from the toothbrush. The OptimumMode is mid-speed and operates at a frequency of 27,000strokes per minute. The Optimum Mode operates with up-downand side-to-side strokes to clean along the gum line (Figure 2).The Deep Clean Mode has faster speed and operates at afrequency of 32,500 strokes per minute with up-down strokesthat clean deep behind and between teeth (Figure 3).
Auto Mode for Intelligent CleaningPrevious research has indicated that people rarely change
their personal brushing technique irrespective of the design ofthe toothbrush used.4 The challenge has continually been todesign a toothbrush that could help the user overcome poorbrushing techniques. By incorporating an Auto Mode into theColgate ProClinical A1500 electric toothbrush, electronicsensors automatically adjust the speed and motion for the bestcleaning experience without forcing the user to change thesespeeds manually. It also utilizes an LED display that helps toguide the user to the proper 45° brushing angle along thegumline.
The electronic sensors that automatically adjust the speedand motion are accelerometers, which are electromechanicalcomponents used to measure acceleration forces. By measuringthese forces, the accelerometer determines the tilt angle of aparticular device. For example, accelerometers are found insmart phones and other devices to deliver screen orientation(landscape or portrait) among other features. By combiningmultiple accelerometers, the Colgate ProClinical A1500 electrictoothbrush will adjust the speed and action of the head basedon location.
Early qualitative research highlighted the benefits of theAuto Mode. Respondents involved in consumer studies usingthe Colgate ProClinical A1500 electric toothbrush understoodthe automatic speed changes provided additional value to theirbrushing experience. These consumers appreciated that thebrush had different speeds for different parts of the mouth andassociated this with a higher degree of sophistication or a“smarter brush.”5
This intelligence was further supported by researchconducted by Omron with the assistance of the Nippon Schoolof Dentistry in Japan. Their studies indicated that there needsto be a guiding tool for easy implementation and usage of a45° brushing angle for the gumline. As part of the BassMethod, tilting the (front) bristles of the toothbrush to a 45°angle on the tooth axis to allow part of the bristles to makecontact with the gingival sulcus improves plaque removal withlittle tooth abrasion, but can be a difficult position for patientsto achieve. Based on their investigation while using an electrictoothbrush with accelerometers, it was shown that the anglesthat are difficult to achieve in the Bass tooth brushing methodcan be easily reproduced when using the Omron toothbrush.6
Therefore, based on the Auto Mode and display featureilluminating a “45” with a blue light on the handle display, thebrushing angle can be confirmed and is thought to be efficientwith guiding the patient’s brushing angle.
The PapersClinical Evaluations
The Colgate ProClinical A1500 electric toothbrush wasevaluated in two in vivo clinical trials.
1. The Colgate ProClinical A1500 electric toothbrush with the Triple Clean refill brush head was compared to twocommercially available power toothbrushes.7 Plaque andgingivitis were assessed at baseline and after four weeksof use. Plaque was also assessed after a single use. The
Figure 2. Visual of Optimum Mode brush head movement operatingwith up-down and side-to-side strokes.
Figure 3. Visual of Deep Clean Mode brush head movement thatoperates with up-down strokes.
A2 The Journal of Clinical Dentistry Vol. XXIII, Spec. Iss. A
Colgate ProClinical A1500 electric toothbrush provided astatistically significantly greater level of efficacy in theremoval of dental plaque after a single tooth brushing andafter four weeks’ use when compared to twocommercially available power toothbrushes. This newsonic powered toothbrush with sensing and controltechnology also provided a statistically significantlygreater level of efficacy in the reduction of gingivitis andgingival bleeding when compared to one of thecommercially available power toothbrushes.
2. The Colgate ProClinical A1500 electric toothbrush with the Triple Clean refill brush head was compared to aregular manual flat-trim toothbrush.8 Plaque and gingivitiswere assessed at baseline, four weeks, and 12 weeks ofuse. Plaque was also assessed after a single brushing. TheColgate ProClinical A1500 electric toothbrush providedstatistically significantly greater reductions in supra-gingival plaque, gingivitis, and gum bleeding whencompared to the manual flat-trim toothbrush at all post-baseline evaluations.
Laboratory EvaluationsThe Colgate ProClinical A1500 electric toothbrush was
evaluated in two in vitro studies.1. The Colgate ProClinical A1500 electric toothbrush with
the Triple Clean and Sensitive refill heads was comparedto a manual flat-trim toothbrush for interproximal accessefficacy (IAE).9 Overall IAEs for the Colgate ProClinicalA1500 electric toothbrush with the Triple Clean andSensitive refill heads were statistically significantly greaterthan the manual flat-trim toothbrush. The ColgateProClinical A1500 electric toothbrush with the Sensitiverefill head demonstrated increased efficiencies comparedto the Triple Clean refill heads for IAE means.
2. The Colgate ProClinical A1500 electric toothbrush with the Triple Clean and Sensitive refill brush heads wascompared in the laboratory to a manual flat-trimtoothbrush for extrinsic stain removal.10 The ColgateProClinical A1500 electric toothbrush effectively removedextrinsic stains from the surfaces of teeth with both theTriple Clean and the Sensitive refill brush heads, and thisremoval was statistically significantly greater than thepercentage of stain removed by the manual flat-trimtoothbrush.
Ergonomics and Usability EvaluationsThe handle design of the Colgate ProClinical A1500 electric
toothbrush is more than simply an interface between theworking head of the toothbrush and the person using it. Thedesign of the brush combines both ergonomics and style toachieve a better intuitive brushing experience. The angle of thetoothbrush handle is different than other power toothbrushesand is perceived to make reaching and cleaning back teetheasier. The lightweight design of the device and the diameterof the handle also contribute to its function by making it moremaneuverable. The handle function is further enhanced byspecial thumb indents to help the user orient the brush
correctly. These thumb indents help the user position the brushat 45° which is the recommended angle to clean along thegumline. This is confirmed to the user when the 45° angleblue light in the handle display is illuminated, signaling to theconsumer that they have achieved the proper brushing angle.These ergonomic features, along with the high frequencycleaning and sensor technology, all contribute to improvedbrushing during clinical trials. Two studies were conductedevaluating the ergonomics of the new power toothbrush alongwith its consumer usability.
1. A complete ergonomic evaluation of the Colgate ProClinical A1500 electric toothbrush was performed comparing it to two commercially available power toothbrushes.11 All three toothbrushes have adequate grip zones, provide grip security, and provide easy access to the on/off button. The handle of the Colgate ProClinical A1500 electric toothbrush angles downward and provides additional advantages through improved grip security and visibility. It is also relatively easy to use with its changes in speeds, brush movements, and resulting changes in audible feedback.
2. A longitudinal usability evaluation of the Colgate ProClinical A1500 electric toothbrush was conducted among users of manual toothbrushes.12 Users commented that this toothbrush was easier to maneuver within the mouth, which resulted in a cleaner feeling. Additionally,consumers spent more time brushing their teeth and more time on individual sections of the teeth in comparison to the time spent with a manual toothbrush.
ConclusionsThe Colgate ProClinical A1500 electric toothbrush provides
a combination of features that contribute to the brushingexperience and efficacy for users. By utilizing high frequencybrushing with electronic sensors and ergonomics, these featuresautomatically adjust to achieve superior cleaning withoutsignificant retraining of the user. The following articles in thisSpecial Issue will further emphasize this by assessing bothclinical and ergonomic performance to support this new electrictoothbrush. These studies demonstrate how the ColgateProClinical A1500 electric toothbrush combines these keyfeatures into an intelligent technology and design thatautomatically adjusts the speed and motion of brush strokes forsuperior cleaning of teeth and gums.
References1. Walters PA, Cugini M, Biesbrock AR, Warren PR. A novel oscillating-
rotating power toothbrush with SmartGuide: designed for enhanced performance and compliance. J Contemp Dent Pract 2007;8:1-9.
2. Penick C. Power toothbrushes: a critical review. Int J Dent Hyg 2004;2:40-4.
3. http://finance.yahoo.com/news/colgate-palmolive-company-omron-healthcare-145600240.
4. Hohlbein DJ, Williams MI, Mintel TE. Driving toothbrush innovation through a cross-functional development team. Compend Contin Educ Dent 2004;25(Suppl 2):7-11.
5. Data on file, Colgate-Palmolive Company. 6. Morozumi Y, Iwahori T, Yamashita A, Tada K, Sugawara A, Nakamura T,
Takashio T, Sato S. Study on tooth brushing angle by introducing
A3The Journal of Clinical DentistryVol. XXIII, Spec. Iss. A

accelerometer in powered toothbrush, Japanese Society of Periodontology, 52nd Spring Scientific Meeting, May 2009, Okayama,Japan, Presentation P-45
7. Ayad F, Petrone DM, Wachs GN, Mateo LR, Chaknis P, Panagakos F. Comparative efficacy of a specially engineered sonic powered toothbrush with unique sensing and control technologies to two commercially available power toothbrushes on established plaque and gingivitis. J Clin Dent 2012;23(Spec Iss A):A5-10.
8. Nathoo S, Mankodi S, Mateo LR, Chaknis P, Panagakos F. A clinical study comparing the supragingival plaque and gingivitis efficacy of a specially engineered sonic powered toothbrush with unique sensing and control technologies to a commercially available manual flat-trim toothbrush. J Clin Dent 2012;23(Spec Iss A):A11-6.
9. Kemp JH, Barnes CM, Spirgel CM, Shi X, Yankell SL. Laboratory
evaluation of plaque removal at interproximal sites by a specially engineered powered toothbrush with unique sensing and control technologies. J Clin Dent 2012;23(Spec Iss A):A17-20.
10. Maloney VP, Kemp J, Mateo LR, Panagakos F. Laboratory evaluation of extrinsic stain removal by a specially engineered sonic powered toothbrush with unique sensing and control technologies. J Clin Dent2012;23(Spec Iss A):A21-5.
11. Hunter G, Burns L, Bone B, Mintel T, Jimenez E. Ergonomic audit of a specially engineered sonic powered toothbrush with unique sensing and control technologies, the Sonicare FlexCare, and the Oral-B Smart Series 5000. J Clin Dent 2012;23(Spec Iss A):A26-30.
12. Hunter G, Burns L, Bone B, Mintel T, Jimenez E. Usability research study of a specially engineered sonic powered toothbrush with unique sensing and control technologies. J Clin Dent 2012;23(Spec Iss A):A31-4
A4 The Journal of Clinical Dentistry Vol. XXIII, Spec. Iss. A

Comparative Efficacy of a Specially Engineered Sonic PoweredToothbrush with Unique Sensing and Control Technologies
to Two Commercially Available Power Toothbrushes on Established Plaque and Gingivitis
Farid Ayad
Far Management, Inc.Mississauga, Ontario, Canada
Dolores M. Petrone, Gerald N. Wachs
Concordia Clinical Research, Inc.Cedar Knolls, NJ, USA
Luis R. Mateo
LRM Statistical ConsultingHoboken, NJ, USA
Patricia Chaknis, Fotinos Panagakos
Colgate-Palmolive Technology CenterPiscataway, NJ, USA
Abstract• Objective: To evaluate the efficacy on plaque and established gingivitis of a new specially engineered sonic powered toothbrush
with unique sensing and control technologies as compared to two commercially available power toothbrushes.• Methods: This examiner-blind, three-treatment, parallel clinical study assessed plaque reduction via the comparison of pre- to
postbrushing after a single use, and following four weeks’ use measured by the Rustogi Modification of the Modified Navy Plaque Index. This study also assessed gingivitis using the Löe and Silness Gingival Index after four weeks’ use. Qualifying adult male and female subjects from the northern New Jersey area reported to the study site after refraining from all oral hygiene procedures for 24 hours, and from eating, drinking, or smoking for four hours. Following an examination for gingivitis and plaque (pre-brushing), they were randomized into three balanced groups, each group using one of the three study toothbrushes in the order specified by a pre-determined randomization plan. Subjects were instructed to brush their teeth for two minutes under supervision with their assigned toothbrush according to the manufacturers’ instructions and a commercially available toothpaste (Colgate® Cavity Protection), after which they were once again evaluated for plaque (post-brushing). Subjects were then dismissed from the study site with the toothpaste and their assigned toothbrush to use at home twice daily for the next four weeks. They again reported to the study site at which time they were evaluated for plaque and gingivitis.
• Results: One-hundred eighty-four subjects complied with the protocol and completed the clinical study. Relative to the two commercially available toothbrushes, the new specially engineered sonic powered toothbrush with unique sensing and control technologies provided statistically significantly (p < 0.05) greater reductions in whole mouth plaque index scores (21.9 and 25.8%,respectively), gingival margin plaque index scores (14.5% and 18.9%, respectively), interproximal plaque index scores (160.0% and 136.4%, respectively), facial plaque index scores (17.9% for both), lingual plaque index scores (29.2% for both), and interproximal lingual plaque index scores (200.0% and 350.0%, respectively) after a single tooth brushing. Relative to the two commercially available toothbrushes, the new sonic powered toothbrush also provided statistically significantly (p < 0.05) greater reductions in whole mouth plaque index scores (47.4% and 40.0%, respectively), gingival margin plaque index scores (46.2% and 40.7%,respectively), interproximal plaque index scores (650% and 1400%, respectively), facial plaque index scores (47.6% and 40.9%,respectively), lingual plaque index scores (47.1% and 31.6%, respectively), and interproximal lingual plaque index scores (350.0% and 500.0%, respectively) after four weeks. There was no statistically significant (p > 0.05) difference between the two commercially available toothbrushes for any plaque index score comparison. Relative to one of the commercially available toothbrushes, the new sonic powered toothbrush provided statistically significant reductions (p < 0.05) in gingival index scores (25.0%) and gingivitis severity scores (33.3%) after four weeks of product use. There were no statistically significant (p > 0.05) differences in gingivitis or gingivitis severity index scores between the new sonic powered toothbrush and the other commercially available toothbrush.
A5

IntroductionThe control of bacterial biofilm, also known as dental plaque,
is essential for the maintenance of oral health. Plaque acts as areservoir for bacteria and left alone will eventually inflame thegingiva, resulting in periodontal diseases such as gingivitis andperiodontitis.1 Even though the marketplace in the past twentyyears has been flooded with new products containingchemotherapeutic agents claiming to help control plaque,effective tooth brushing continues to be the best to disrupt andcontrol plaque biofilm.2
Tooth brushing is the most widely used form of oral hygiene,but is often far from satisfactory in removing and controllingplaque.3 The clinical effectiveness of tooth brushing is dependenton a number of factors, including toothbrush design and toothbrushing methods, time, and frequency. Mechanical removal ofplaque by tooth brushing is greatly dependent on the skills,perseverance, and motivation of the individual and is, therefore,highly variable and inconsistent in the general population. It hasbeen reported that, on average, the plaque removal of users ofmanual toothbrushes after a single brushing is 43%.4
Power toothbrushes were introduced in the 1960s and haveevolved from those which simulated back-and-forth or side-to-side hand motion to the sonic and oscillating-rotatingtechnologies that are found in the most recently marketed powertoothbrushes. A new specially engineered sonic poweredtoothbrush with unique sensing and control technologies hasbeen introduced by the Colgate-Palmolive Company (New York,NY, USA). This examiner-blind, three-treatment, parallel clinicalstudy evaluated the efficacy of this new toothbrush compared totwo commercially available power toothbrushes, the Oral-B®
Smart Series 5000 Power Toothbrush (Procter & Gamble Co.,Cincinnati, OH, USA) and the Sonicare™ Flexcare PowerToothbrush (Philips Sonicare, Stamford, CT, USA), for theremoval of plaque and reduction in gingivitis over a four-weekperiod. This study assessed whole mouth, gumline (gingivalmargin), interproximal, facial, lingual and interproximal lingualplaque removal by comparing pre and post-brushing plaquelevels using the Rustogi Modification of the Modified NavyPlaque Index,5 after one use and again after four-weeks’ use.Additionally, a comparison of gingivitis scores using the Löe andSilness Gingival Index6 prior to the pre-brushing plaqueexamination and again after four weeks was evaluated. Thestudy protocol was submitted to and approved by an InstitutionalReview Board.
Materials and MethodsThis independent clinical study employed an examiner-blind,
three-treatment, parallel design. Adult male and female subjectsfrom the northern New Jersey, USA area were enrolled into thestudy based upon the following criteria:
1. Subjects had to be between the ages of 18 and 70 years inclusive, in generally good health, and possess a minimum of 20 uncrowned permanent natural teeth (excluding third molars). They needed to be available for the duration of the study and to sign an informed consent form.
2. Subjects were required to present a mean Rustogi Modification of the Modified Navy Plaque Index score of 0.6 or greater and a Löe and Silness Gingival Index score of at least 1.0 at their screening examination.
3. Subjects were excluded from the study if they had orthodontic appliances, removable prostheses or partial dentures, tumors of the soft or hard tissues of the oral cavity, advanced periodontal disease, or five or more carious lesions requiring restorative treatment.
4. Subjects were also excluded if they had received a dental prophylaxis within one month prior to entry into the study,or if they had received antibiotic therapy or steroids any time during the month prior to entry into the study. Pregnant or lactating women were also excluded.
5. Subjects were excluded if they had a history of allergies to oral care products, personal care consumer products or their ingredients, or if they had any medical condition that would preclude them from not eating and drinking for four hours prior to their examination.
Subjects reported to the study site after refraining from anyoral hygiene procedures for 24 hours and from eating, drinking,and smoking for four hours. Following an examination forgingivitis (baseline) and supragingival plaque (pre-brushing),qualified subjects were randomized based on their plaque scoresinto three balanced groups. Groups were assigned to one of thethree study toothbrushes in the order specified by a predeter-mined randomization plan. The three toothbrushes were:
1. TC: Colgate® ProClinical™ A1500 Power Toothbrush with the Triple Clean brush head (Colgate-Palmolive Company,New York, NY, USA) used in the Auto Mode;
2. PG: Oral-B Smart Series 5000 Power Toothbrush (Procter & Gamble Co, Cincinnati, OH, USA) used in the Daily Clean Mode with Flossaction brush head; and
3. PH: Sonicare Flexcare Power Toothbrush (Philips-Sonicare Co., Stamford, CT, USA) used in the Clean Mode with Contoured brush head.
Subjects were provided with their assigned toothbrush andcommercially available fluoride toothpaste (Colgate® CavityProtection) and were instructed to brush their teeth for twominutes under supervision and according to the manufacturer’sinstructions, after which time they were once again evaluatedfor plaque (post-brushing). Subjects were then given theirassigned toothbrush and toothpaste for use at home for the nextfour weeks. At the end of four weeks, subjects reported to thestudy site after refraining from any oral hygiene procedures for
• Conclusion: A new specially engineered sonic powered toothbrush with unique sensing and control technologies provides significantly greater levels of efficacy on the removal of dental plaque after a single tooth brushing and after four weeks’ use when compared to two commercially available power toothbrushes. The new sonic powered toothbrush also provides significantly greater levels of efficacy on the reduction of gingivitis and gingival bleeding when compared to one of the commercially available power toothbrushes.
(J Clin Dent 2012;23[Spec Iss A]:A5-A10)
Vol. XXIII, Spec. Iss. AThe Journal of Clinical DentistryA6
24 hours and from eating, drinking, and smoking for four hours.Clinical Scoring Procedures
Gingivitis. Gingivitis was scored according to the Löe-Silness Gingival Index as modified by Talbott, et al.7 Each toothwas scored in six areas: mesiofacial, midfacial, distofacial,mesiolingual, midlingual, and distolingual as follows:0 = Absence of inflammation1 = Mild inflammation: slight change in color and little changein texture2 = Moderate inflammation: moderate glazing, redness, edema,hypertrophy; tendency to bleed on probing3 = Severe inflammation: marked redness and hypertrophy;tendency to bleed spontaneouslyThird molars and teeth with cervical restorations or prostheticcrowns were excluded from the scoring procedure. Wholemouth mean scores were obtained by averaging the valuesrecorded from all scoreable tooth surfaces.
Gingivitis Severity Index. In addition to calculating a meanLöe-Silness Gingival Index score for each subject, a meanGingivitis Severity Index was also calculated for each subject.8
This index allows for a comparison of the gingival sites thatreceived the Löe-Silness Gingival Index scores of 2 and 3 (i.e.,bleeding sites). The mean Gingivitis Severity Index wascalculated for each subject by dividing the total number ofgingival sites scored 2 or 3 by the total number of teeth scoredin the mouth.
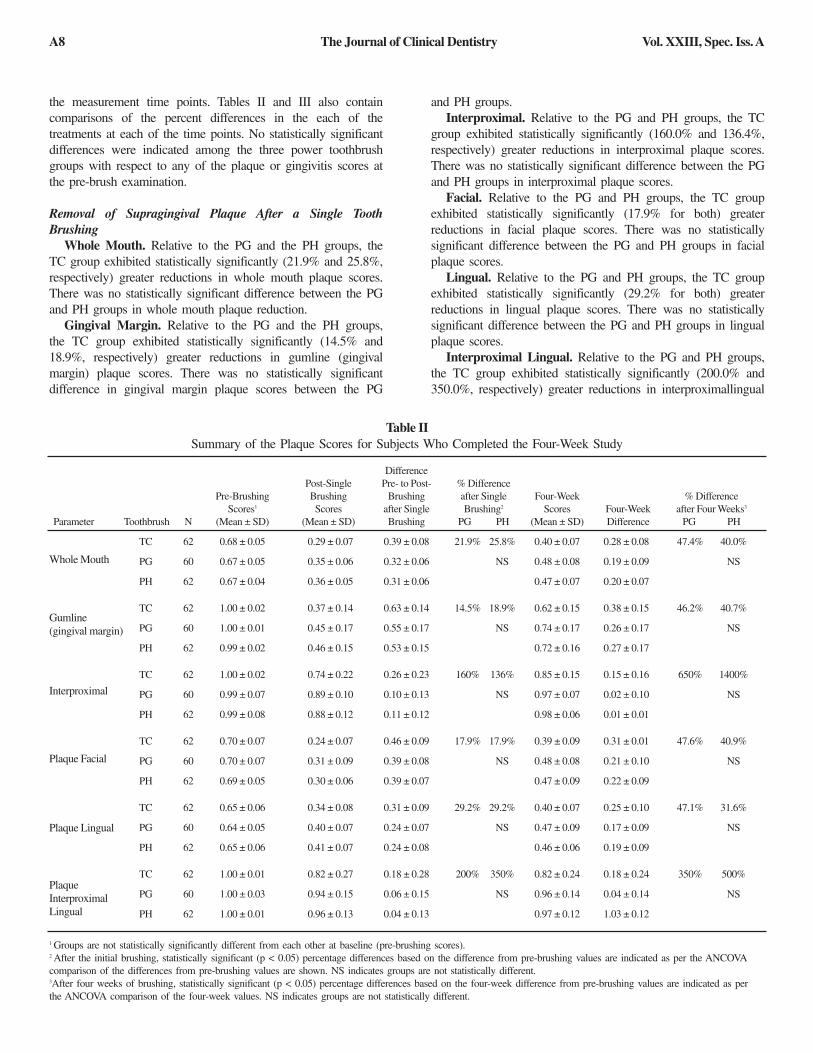
Dental Plaque. Plaque was scored according to the RustogiModification of the Modified Navy Plaque Index. Supragingivalplaque on the facial and lingual surfaces of each tooth wasdisclosed and recorded as present or absent on nine discreteareas of the tooth (Figure 1). Third molars were excluded fromthe scoring procedure. From these site-wise scores, a plaquescore was determined for each subject by calculating theproportion of sites in the mouth at which plaque was present.Six parameters were evaluated as follows:
Whole Mouth scores – A, B, C, D, E, F, G, H, I for bothfacial and lingual surfacesGumline (Gingival Margin) scores – A, B, CInterproximal scores – D, FFacial scores – A, B, C, D, E, F, G, H, ILingual scores – A, B, C, D, E, F, G, H, IInterproximal lingual scores – D, F
The same dental examiner conducted all of the dentalexaminations performed in the study. The examiner had beentrained, calibrated, and was highly experienced as to theclinical scoring procedures used in this study.
Oral Soft Tissue AssessmentThe dental examiner visually examined the oral cavity and
peri-oral area at each visit. These examinations includedevaluation of the soft and hard palate, gingival mucosa, buccalmucosa, mucogingival fold areas, tongue, sublingual andsubmandibular areas, salivary glands, and the tonsilar andpharyngeal areas.
Adverse EventsAdverse events were obtained from subjects and from dental
examinations by the examining dentist.
Statistical MethodsStatistical analyses were performed separately for the
gingivitis assessments and dental plaque assessments.Comparisons of the treatment groups with respect to baselinegingival index scores and plaque index scores were performedusing an analysis of variance (ANOVA). Comparisons of thetreatment groups with respect to baseline-adjusted gingival andplaque scores at the follow-up examinations were performedusing analyses of covariance (ANCOVAs). After the initialbrushing, the response used for the between-product analysiswas the difference between the pre- and post-brushing meanvalues. After four weeks, the response used for the betweenproduct analysis was the four-week endpoint. Post-ANCOVApair-wise comparisons of the study treatments were performedusing Tukey’s test for multiple comparisons. All statistical testsof hypotheses were two-sided, and employed a level ofsignificance of α = 0.05.
ResultsOne-hundred eighty-four (184) subjects entered, complied withthe protocol, and completed the clinical study. The gender andage for the subjects who completed the study are presented inTable I. Throughout the study, no adverse effects of the oralhard or soft tissues were observed by the dental examiner orreported by the participants.
Table II presents a summary of the mean plaque scores foreach of the six site-wise plaque indices taken at each of themeasurement time points. Table III presents a summary of themean gingivitis and mean gingivitis severity scores at each ofFigure 1. The Rustogi Modification of the Navy Plaque Index.
Table ISummary of Age and Sex Characteristics for Subjects
Who Completed the Clinical Study
Toothbrush Male Female Total Mean Range
TC 18 44 62 46 19-69
PG 12 48 60 46 18-69
PH 16 46 62 44 20-67
Number of Subjects Age
Vol. XXIII, Spec. Iss. A The Journal of Clinical Dentistry A7
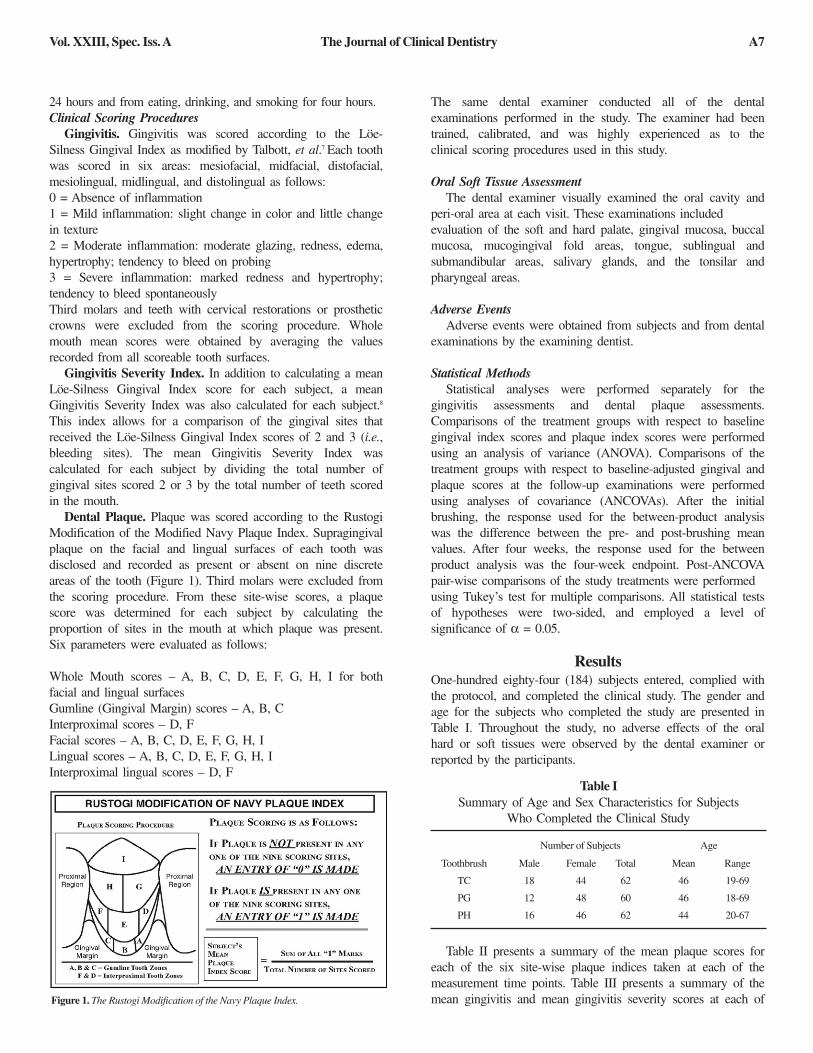
the measurement time points. Tables II and III also containcomparisons of the percent differences in the each of thetreatments at each of the time points. No statistically significantdifferences were indicated among the three power toothbrushgroups with respect to any of the plaque or gingivitis scores atthe pre-brush examination.
Removal of Supragingival Plaque After a Single ToothBrushing
Whole Mouth. Relative to the PG and the PH groups, theTC group exhibited statistically significantly (21.9% and 25.8%,respectively) greater reductions in whole mouth plaque scores.There was no statistically significant difference between the PGand PH groups in whole mouth plaque reduction.
Gingival Margin. Relative to the PG and the PH groups,the TC group exhibited statistically significantly (14.5% and18.9%, respectively) greater reductions in gumline (gingivalmargin) plaque scores. There was no statistically significantdifference in gingival margin plaque scores between the PG
and PH groups.Interproximal. Relative to the PG and PH groups, the TC
group exhibited statistically significantly (160.0% and 136.4%,respectively) greater reductions in interproximal plaque scores.There was no statistically significant difference between the PGand PH groups in interproximal plaque scores.
Facial. Relative to the PG and PH groups, the TC groupexhibited statistically significantly (17.9% for both) greaterreductions in facial plaque scores. There was no statisticallysignificant difference between the PG and PH groups in facialplaque scores.
Lingual. Relative to the PG and PH groups, the TC groupexhibited statistically significantly (29.2% for both) greaterreductions in lingual plaque scores. There was no statisticallysignificant difference between the PG and PH groups in lingualplaque scores.
Interproximal Lingual. Relative to the PG and PH groups,the TC group exhibited statistically significantly (200.0% and350.0%, respectively) greater reductions in interproximallingual
Table IISummary of the Plaque Scores for Subjects Who Completed the Four-Week Study
DifferencePost-Single Pre- to Post- % Difference
Pre-Brushing Brushing Brushing after Single Four-Week % DifferenceScores1 Scores after Single Brushing2 Scores Four-Week after Four Weeks3
Parameter Toothbrush N (Mean ± SD) (Mean ± SD) Brushing PG PH (Mean ± SD) Difference PG PH
TC 62 0.68 ± 0.05 0.29 ± 0.07 0.39 ± 0.08 21.9% 25.8% 0.40 ± 0.07 0.28 ± 0.08 47.4% 40.0%
PG 60 0.67 ± 0.05 0.35 ± 0.06 0.32 ± 0.06 NS 0.48 ± 0.08 0.19 ± 0.09 NS
PH 62 0.67 ± 0.04 0.36 ± 0.05 0.31 ± 0.06 0.47 ± 0.07 0.20 ± 0.07
TC 62 1.00 ± 0.02 0.37 ± 0.14 0.63 ± 0.14 14.5% 18.9% 0.62 ± 0.15 0.38 ± 0.15 46.2% 40.7%
PG 60 1.00 ± 0.01 0.45 ± 0.17 0.55 ± 0.17 NS 0.74 ± 0.17 0.26 ± 0.17 NS
PH 62 0.99 ± 0.02 0.46 ± 0.15 0.53 ± 0.15 0.72 ± 0.16 0.27 ± 0.17
TC 62 1.00 ± 0.02 0.74 ± 0.22 0.26 ± 0.23 160% 136% 0.85 ± 0.15 0.15 ± 0.16 650% 1400%
PG 60 0.99 ± 0.07 0.89 ± 0.10 0.10 ± 0.13 NS 0.97 ± 0.07 0.02 ± 0.10 NS
PH 62 0.99 ± 0.08 0.88 ± 0.12 0.11 ± 0.12 0.98 ± 0.06 0.01 ± 0.01
TC 62 0.70 ± 0.07 0.24 ± 0.07 0.46 ± 0.09 17.9% 17.9% 0.39 ± 0.09 0.31 ± 0.01 47.6% 40.9%
PG 60 0.70 ± 0.07 0.31 ± 0.09 0.39 ± 0.08 NS 0.48 ± 0.08 0.21 ± 0.10 NS
PH 62 0.69 ± 0.05 0.30 ± 0.06 0.39 ± 0.07 0.47 ± 0.09 0.22 ± 0.09
TC 62 0.65 ± 0.06 0.34 ± 0.08 0.31 ± 0.09 29.2% 29.2% 0.40 ± 0.07 0.25 ± 0.10 47.1% 31.6%
PG 60 0.64 ± 0.05 0.40 ± 0.07 0.24 ± 0.07 NS 0.47 ± 0.09 0.17 ± 0.09 NS
PH 62 0.65 ± 0.06 0.41 ± 0.07 0.24 ± 0.08 0.46 ± 0.06 0.19 ± 0.09
TC 62 1.00 ± 0.01 0.82 ± 0.27 0.18 ± 0.28 200% 350% 0.82 ± 0.24 0.18 ± 0.24 350% 500%
PG 60 1.00 ± 0.03 0.94 ± 0.15 0.06 ± 0.15 NS 0.96 ± 0.14 0.04 ± 0.14 NS
PH 62 1.00 ± 0.01 0.96 ± 0.13 0.04 ± 0.13 0.97 ± 0.12 1.03 ± 0.12
Whole Mouth
Gumline(gingival margin)
Interproximal
Plaque Facial
Plaque Lingual
PlaqueInterproximalLingual
1 Groups are not statistically significantly different from each other at baseline (pre-brushing scores).2 After the initial brushing, statistically significant (p < 0.05) percentage differences based on the difference from pre-brushing values are indicated as per the ANCOVAcomparison of the differences from pre-brushing values are shown. NS indicates groups are not statistically different.3After four weeks of brushing, statistically significant (p < 0.05) percentage differences based on the four-week difference from pre-brushing values are indicated as perthe ANCOVA comparison of the four-week values. NS indicates groups are not statistically different.
Vol. XXIII, Spec. Iss. AThe Journal of Clinical DentistryA8
plaque scores. There was no statistically significant differencebetween the PG and PH groups in interproximal lingual plaquescores.
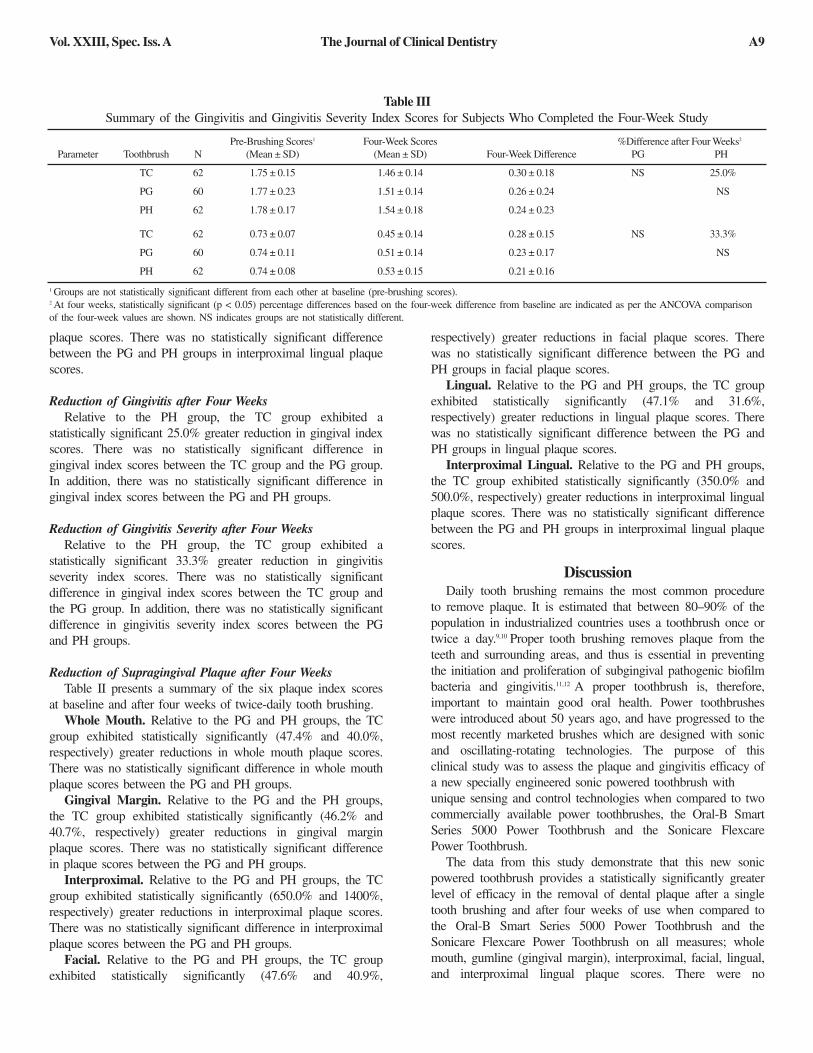
Reduction of Gingivitis after Four WeeksRelative to the PH group, the TC group exhibited a
statistically significant 25.0% greater reduction in gingival indexscores. There was no statistically significant difference ingingival index scores between the TC group and the PG group.In addition, there was no statistically significant difference ingingival index scores between the PG and PH groups.
Reduction of Gingivitis Severity after Four WeeksRelative to the PH group, the TC group exhibited a
statistically significant 33.3% greater reduction in gingivitisseverity index scores. There was no statistically significantdifference in gingival index scores between the TC group andthe PG group. In addition, there was no statistically significantdifference in gingivitis severity index scores between the PGand PH groups.
Reduction of Supragingival Plaque after Four WeeksTable II presents a summary of the six plaque index scores
at baseline and after four weeks of twice-daily tooth brushing.Whole Mouth. Relative to the PG and PH groups, the TC
group exhibited statistically significantly (47.4% and 40.0%,respectively) greater reductions in whole mouth plaque scores.There was no statistically significant difference in whole mouthplaque scores between the PG and PH groups.
Gingival Margin. Relative to the PG and the PH groups,the TC group exhibited statistically significantly (46.2% and40.7%, respectively) greater reductions in gingival marginplaque scores. There was no statistically significant differencein plaque scores between the PG and PH groups.
Interproximal. Relative to the PG and PH groups, the TCgroup exhibited statistically significantly (650.0% and 1400%,respectively) greater reductions in interproximal plaque scores.There was no statistically significant difference in interproximalplaque scores between the PG and PH groups.
Facial. Relative to the PG and PH groups, the TC groupexhibited statistically significantly (47.6% and 40.9%,
respectively) greater reductions in facial plaque scores. Therewas no statistically significant difference between the PG andPH groups in facial plaque scores.
Lingual. Relative to the PG and PH groups, the TC groupexhibited statistically significantly (47.1% and 31.6%,respectively) greater reductions in lingual plaque scores. Therewas no statistically significant difference between the PG andPH groups in lingual plaque scores.
Interproximal Lingual. Relative to the PG and PH groups,the TC group exhibited statistically significantly (350.0% and500.0%, respectively) greater reductions in interproximal lingualplaque scores. There was no statistically significant differencebetween the PG and PH groups in interproximal lingual plaquescores.
DiscussionDaily tooth brushing remains the most common procedure
to remove plaque. It is estimated that between 80–90% of thepopulation in industrialized countries uses a toothbrush once ortwice a day.9,10 Proper tooth brushing removes plaque from theteeth and surrounding areas, and thus is essential in preventingthe initiation and proliferation of subgingival pathogenic biofilmbacteria and gingivitis.11,12 A proper toothbrush is, therefore,important to maintain good oral health. Power toothbrusheswere introduced about 50 years ago, and have progressed to themost recently marketed brushes which are designed with sonicand oscillating-rotating technologies. The purpose of thisclinical study was to assess the plaque and gingivitis efficacy ofa new specially engineered sonic powered toothbrush withunique sensing and control technologies when compared to twocommercially available power toothbrushes, the Oral-B SmartSeries 5000 Power Toothbrush and the Sonicare FlexcarePower Toothbrush.
The data from this study demonstrate that this new sonicpowered toothbrush provides a statistically significantly greaterlevel of efficacy in the removal of dental plaque after a singletooth brushing and after four weeks of use when compared tothe Oral-B Smart Series 5000 Power Toothbrush and theSonicare Flexcare Power Toothbrush on all measures; wholemouth, gumline (gingival margin), interproximal, facial, lingual,and interproximal lingual plaque scores. There were no
Table IIISummary of the Gingivitis and Gingivitis Severity Index Scores for Subjects Who Completed the Four-Week Study
Pre-Brushing Scores1 Four-Week Scores %Difference after Four Weeks2
Parameter Toothbrush N (Mean ± SD) (Mean ± SD) Four-Week Difference PG PH
TC 62 1.75 ± 0.15 1.46 ± 0.14 0.30 ± 0.18 NS 25.0%
PG 60 1.77 ± 0.23 1.51 ± 0.14 0.26 ± 0.24 NS
PH 62 1.78 ± 0.17 1.54 ± 0.18 0.24 ± 0.23
TC 62 0.73 ± 0.07 0.45 ± 0.14 0.28 ± 0.15 NS 33.3%
PG 60 0.74 ± 0.11 0.51 ± 0.14 0.23 ± 0.17 NS
PH 62 0.74 ± 0.08 0.53 ± 0.15 0.21 ± 0.16
1 Groups are not statistically significant different from each other at baseline (pre-brushing scores).2 At four weeks, statistically significant (p < 0.05) percentage differences based on the four-week difference from baseline are indicated as per the ANCOVA comparisonof the four-week values are shown. NS indicates groups are not statistically different.
Vol. XXIII, Spec. Iss. A The Journal of Clinical Dentistry A9

statistically significant differences between the twocommercially available power toothbrushes on any of theplaque measurements. The new sonic powered toothbrushprovides a statistically significantly greater level of efficacy inthe reduction of gingivitis and gingival bleeding than theSonicare FlexcarePower Toothbrush; however, it was not significantly differentfrom the Oral-B toothbrush on these measures. The Oral-BSmart Series 5000 Power Toothbrush was equivalent to theSonicare Flexcare Power Toothbrush in the reduction ofgingivitis and gingival bleeding.
ConclusionThis new specially engineered sonic powered toothbrush
with unique sensing and control technologies provides superiorcleaning as measured by plaque removal when compared totwo commercially available power toothbrushes after one useand after four weeks of use. It is also superior in efficacy toone of the commercially available power toothbrushes after fourweeks with respect to gingivitis and gingival bleeding.
Acknowledgement: This study was funded by the Colgate-PalmoliveCompany.
For correspondence with the authors of this paper, contactMs. Patricia Chaknis – [email protected].
References1. Rose LF, Mealey BL, Genco RJ, Cohen DW. Periodontics: Medicine,
Surgery and Implants 1st Ed. Elsevier Mosby, 2004.2. Iacono VJ, Aldredge WA, Lucks H, Schwartzstein S. Modern supragingival
plaque control. Int Dent J 1998;48(3 Suppl 1):290-7.3. Singh SM, Deasy MJ. Clinical plaque removal performance of two manual
toothbrushes. J Clin Dent 1993;4(Suppl D):D13-6.4. van der Weijden F, Slot DE. Oral hygiene in the prevention of periodontal
diseases: the evidence. Periodontol 2000 2011;55:104-23.5. Rustogi KN, Curtis JP, Volpe AR, Kemp JH, McCool JJ, Korn LR.
Refinement of the Modified Navy Plaque Index to increase plaque scoring efficiency in gumline and interproximal tooth areas. J Clin Dent 1992;3(Suppl C):C9-12.
6. Löe H, Silness J. Periodontal disease in pregnancy. I. Prevalence and severity. Acta Odontol Scand 1963;21:533-51.
7. Talbott K, Mandel ID, Chilton NW. Reduction of baseline gingivitis scores in repeated prophylaxes. J Prev Dent 1977;4:28-9.
8. García-Godoy F, García-Godoy F, DeVizio W, Volpe AR, Ferlauto RJ,Miller JM. Effect of a triclosan/copolymer/fluoride dentifrice on plaque formation and gingivitis: A 7-month clinical study. Am J Dent 1990;3(Spec No):S15-26.
9. Saxer UP, Yankell SL. Impact of improved toothbrushes on dental diseases. I. Quintessence Int 1997;28:513-25.
10. Saxer UP, Yankell SL. Impact of improved toothbrushes on dental diseases. II. Quintessence Int 1997:28:573-93.
11. Westfelt E, Rylander H, Dahlén G, Lindhe J. The effect of supragingival plaque control on the progression of advanced periodontal disease. J Clin Periodontol 1998;25:536-41.
12. Ximénez-Fyvie LA, Haffajee AD, Som S, Thompson M, Torresyap G,Socransky SS. The effect of repeated professional supragingival plaque removal on the composition of the supra-and subgingival microbiota. J Clin Periodontol 2000;27:637-47.
Vol. XXIII, Spec. Iss. AThe Journal of Clinical DentistryA10

A Clinical Study Comparing the Supragingival Plaque and Gingivitis Efficacy of a Specially Engineered Sonic
Powered Toothbrush with Unique Sensing and Control Technologies to a Commercially Available
Manual Flat-Trim Toothbrush
Salim Nathoo
Oral Health Clinical ServicesPiscataway, NJ, USA
Patricia Chaknis, Foti Panagakos
Colgate-Palmolive Technology CenterPiscataway, NJ, USA
Abstract• Objective: This study was designed to evaluate the efficacy of a new specially engineered sonic powered toothbrush with unique
sensing and control technologies, as compared to a manual flat-trim toothbrush on supragingival plaque and established gingivitis.• Methods: This examiner-blind, two-treatment, parallel clinical research study assessed plaque removal via the comparison of pre- to
post-brushing after a single use, and again after four- and 12-weeks’ use using the Rustogi Modification of the Modified Navy Plaque Index. This study also assessed gingivitis at four and 12 weeks using the Löe and Silness Gingival Index. Qualifying adult male and female subjects from the southern Florida area reported to the study site after refraining from any oral hygiene procedures for 24 hours, and from eating, drinking, and smoking for four hours. Following an examination for plaque (pre-brushing) and gingivitis, they were randomized (for both plaque and gingivitis) into two balanced groups, each group using one of the two study toothbrushes. Subjects were instructed to brush their teeth for two minutes under supervision with their assigned toothbrush according to the manufacturer’s instructions, and commercially available toothpaste (Colgate® Cavity Protection Toothpaste), after which they were again evaluated for plaque (post-brushing). Subjects were then dismissed from the study site with the toothpaste and their assigned toothbrush to use at home twice daily for the next 12 weeks. They again reported to the study site after four and 12 weeks of product use, at which time they were evaluated for plaque and gingivitis.
• Results: Seventy-six out of 82 enrolled subjects complied with the protocol and completed the clinical study. The new specially engineered sonic powered toothbrush with unique sensing and control technologies provided statistically significant reductions in gingival and gingivitis severity index scores after four and 12 weeks of product use. The manual toothbrush provided a statistically significant reduction in gingival index score only at the 12-week time point. Relative to the manual toothbrush group, after a single tooth brushing and after four and 12 weeks, the new sonic powered toothbrush provided statistically significantly greater reductions in whole mouth plaque index scores (1.6, 2.05, and 1.9 times, respectively), gingival margin plaque index scores (12.0, 90.0, and 8.2 times, respectively), and interproximal plaque index scores (2.0, 3.2, and 2.1 times, respectively). Relative to the manual toothbrush group after four and 12 weeks, the new sonic powered toothbrush provided statistically significant reductions in gingival index scores of 11.0 and 7.0 times, respectively, and in gingivitis severity index scores of 3.0 and 3.5 times, respectively. All statistically significant reductions were at the p ≤ 0.05 level.
• Conclusion: The new specially engineered sonic powered toothbrush with unique sensing and control technologies provides statistically significant and clinically relevant levels of efficacy in the removal of supragingival dental plaque after a single tooth brushing, and after four and 12 weeks’ use. The new sonic powered toothbrush also provides statistically significantly greater levels of efficacy in the reduction of supragingival plaque, gingivitis, and gingival bleeding when compared to a manual flat-trim toothbrush.
(J Clin Dent 2012;23[Spec Iss A]:A11-A16)
A11
Suru Mankodi Luis R Mateo
Dental Products TestingWest Palm Beach, FL, USA
LRM Statistical ConsultingHoboken, NJ, USA

IntroductionIt is well understood that plaque removal by way of an effective
daily home care regimen is an important element of oral health.Dental plaque affects both pathologic and cosmetic conditions,among them caries, gingivitis, periodontitis, and mouth odor.1,2
Even with effective tooth cleaning, bacteria re-colonize the toothsurface, most notably around the gingival margin and interdentalspaces.3 The developing biofilm (plaque) releases a variety ofbiologically active products that diffuse into the gingivalepithelium to initiate the host response that, if persistent, can resultin gingivitis. Left untreated, periodontal pockets may form, bonecould resorb, and eventually teeth might be lost. Further, currentresearch has shown that oral inflammation caused by prolongedexposure of the gum tissues to bacteria in dental plaque isassociated with various systemic diseases, including diabetes,coronary heart disease, peripheral arterial disease, cardiovasculardisease, ischemic stroke, low birth weight, preterm babies, andosteoporosis.4,5
The most common method of supragingival plaque control isby tooth brushing, which is the mechanical removal of plaque.Tooth brushing is an essential tool in keeping teeth clean and inmaintaining good oral hygiene. The problem is that most peopledo not brush effectively, i.e., frequently enough, for long enough,or with appropriate brushing technique to achieve sufficient plaqueremoval. Because tooth brushing is so important to oral health,toothbrush design is important to the effectiveness of any brush inremoving plaque.6 That is why it is very important that consumerschoose a brush they will actually use and use effectively. For along time, the only available toothbrush type was a manual one.Electric toothbrushes were then introduced, and subsequentlycomparisons among the various types of toothbrushes eliciteddiscussion and study.
Numerous clinical studies have been reported that compare theplaque and gingivitis efficacy of a manual toothbrush to that of apower or electric toothbrush with varied results.7-11 PublishedCochrane systematic reviews in 2003 and 2005 suggest one typeof powered brush was superior to manual tooth brushing for theremoval of plaque and reduction of gum inflammation.12,13
However, that review did not allow direct comparison between thedifferent types of powered toothbrushes. A subsequent review hasreported that brushes with a rotation oscillation action reducedplaque and gingivitis more than those with a side-to-side action inthe short term.14 However, the difference was small and its clinicalimportance unclear. Due to the low numbers of trials using othertypes of powered brushes, no other definitive conclusions can bedrawn regarding the superiority of one type of powered toothbrushover another.
The newer power toothbrushes have other benefits. They arenow available with timers to help increase brushing time, andsome have smaller and lighter heads to improve brushingtechnique, thus creating a more enjoyable brushing experience. Inaddition, power toothbrushes have been shown to have anadvantage for special needs patients, including those withorthodontics, those who are debilitated, the elderly, andchildren.16,17 As previously mentioned, further trials of good qualityare required to establish if other types of powered brushes arebetter at reducing plaque and gingivitis.15
A new specially engineered sonic powered toothbrush withunique sensing and control technologies has been introduced bythe Colgate-Palmolive Company. This examiner-blind, two-treatment, parallel clinical study evaluated the efficacy of this newsonic powered toothbrush in removing dental plaque and reducinggingivitis over a 12-week period as compared to a manual flat-trimtoothbrush. This study assessed plaque in the whole mouth, at thegingival margin, and at interproximal sites by comparing pre- andpost-brushing plaque levels using the Rustogi Modification of theModified Navy Plaque Index18 after a single use and again afterfour-weeks’ and 12-weeks’ twice-daily use. Additionally, acomparison of the occurrence of gingivitis using the Löe andSilness Gingival Index19 and gingival bleeding using the GingivitisSeverity Index20 prior to the pre-brushing plaque examination andagain after four and 12 weeks of product use was evaluated. Thestudy protocol was submitted to and approved by an InstitutionalReview Board.
Materials and MethodsThis independent clinical study employed an examiner-blind,
two-treatment, parallel design. Adult male and female subjectsfrom the southern Florida area were enrolled into the study basedupon the following criteria:
1. Subjects had to be between the ages of 18 and 70, inclusive,in generally good health, and possess a minimum of 20 uncrownedpermanent natural teeth (excluding third molars). They needed tobe available for the duration of the study, and to sign an informedconsent form.
2. Subjects were required to present a mean RustogiModification of the Modified Navy Plaque Index score of 0.6 orgreater and a Löe and Silness Gingival Index score of at least 1.0at their screening examination.
3. Subjects were excluded from the study if they hadorthodontic appliances, removable prostheses or partial dentures,tumors of the soft or hard tissues of the oral cavity, advancedperiodontal disease, or five or more carious lesions requiringrestorative treatment.
4. Subjects were also excluded if they had received a dentalprophylaxis within one month prior to entry into the study, or ifthey had received antibiotic therapy or steroids any time duringone month prior to entry into the study. Pregnant or lactatingwomen were also excluded.
5. Subjects were excluded if they had a history of allergies tooral care products, personal care consumer products or theiringredients, or if they had any medical condition that wouldpreclude them from not eating and drinking for four hours prior totheir examination.
Subjects reported to the study site after refraining from any oralhygiene procedures for 24 hours and from eating, drinking, orsmoking for four hours. Following an examination for gingivitis(baseline) and supragingival plaque (pre-brushing), qualifiedsubjects were randomized based on their plaque scores into twobalanced groups. Groups were assigned one of the two studytoothbrushes:
1. TC: Colgate® ProClinical™ A1500 Power Toothbrush with the Triple Clean Brush Head (Colgate-Palmolive Company, New York, NY, USA) using the Auto Mode; and
Vol. XXIII, Spec. Iss. AThe Journal of Clinical DentistryA12
2. I: Manual flat-trim toothbrush; Oral-B® Indicator Toothbrush (Procter & Gamble Company, Cincinnati, OH, USA).
Subjects were provided with their assigned toothbrush andcommercially available fluoride toothpaste (Colgate® CavityProtection, Colgate-Palmolive Company, New York, NY, USA)and were instructed to brush their teeth for two minutes accordingto the manufacturer’s instructions under supervision, after whichtime they were again evaluated for plaque (post-brushing).Subjects were then given their assigned toothbrush and toothpastefor use at home for the next 12 weeks. Subjects were instructed torefrain from using any other oral hygiene products such as otherdentifrices or toothbrushes, mouthrinses, dental flosses, andinterdental stimulators while they were participating in the study.There were no restrictions regarding diet and smoking habitsduring the course of the study. Subjects returned to the study sitefor an evaluation of plaque and gingivitis after four and 12 weeks,again refraining from any oral hygiene procedures for 24 hoursand from eating, drinking, or smoking for four hours.
Clinical Scoring ProceduresGingivitis. Gingivitis was scored according to the Löe-Silness
Gingival Index as modified by Talbott, et al.21 Each tooth was scoredin six areas: mesiofacial, midfacial, distofacial, mesiolingual,midlingual, and distolingual as follows:
0 = Absence of inflammation1 = Mild inflammation: slight change in color and little
change in texture2 = Moderate inflammation: moderate glazing, redness,
edema, hypertrophy; tendency to bleed on probing3 = Severe inflammation: marked redness and hypertrophy;
tendency to bleed spontaneouslyThird molars and teeth with cervical restorations or prostheticcrowns were excluded from the scoring procedure. Whole mouthmean scores were obtained by averaging the values recorded fromall scoreable tooth surfaces.
Gingivitis Severity Index. In addition to calculating a meanLöe-Silness Gingival Index score for each subject, a meanGingivitis Severity Index was also calculated for each subject.20
This index allows for a comparison of the gingival sites that
received Löe-Silness Gingival Index scores, i.e., scores of 2 and 3(bleeding sites). The mean Gingivitis Severity Index wascalculated for each subject by dividing the total number of gingivalsites scored 2 or 3 by the total number of teeth scored in the mouth.
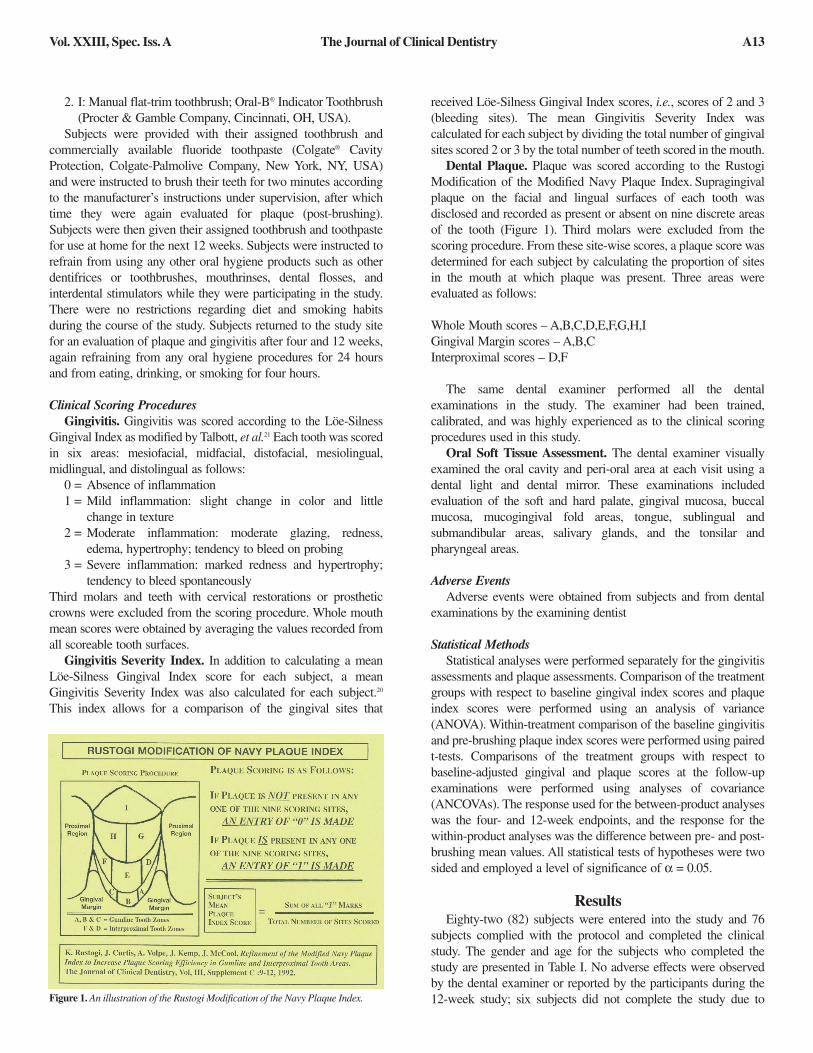
Dental Plaque. Plaque was scored according to the RustogiModification of the Modified Navy Plaque Index. Supragingivalplaque on the facial and lingual surfaces of each tooth wasdisclosed and recorded as present or absent on nine discrete areasof the tooth (Figure 1). Third molars were excluded from thescoring procedure. From these site-wise scores, a plaque score wasdetermined for each subject by calculating the proportion of sitesin the mouth at which plaque was present. Three areas wereevaluated as follows:
Whole Mouth scores – A,B,C,D,E,F,G,H,IGingival Margin scores – A,B,CInterproximal scores – D,F
The same dental examiner performed all the dentalexaminations in the study. The examiner had been trained,calibrated, and was highly experienced as to the clinical scoringprocedures used in this study.
Oral Soft Tissue Assessment. The dental examiner visuallyexamined the oral cavity and peri-oral area at each visit using adental light and dental mirror. These examinations includedevaluation of the soft and hard palate, gingival mucosa, buccalmucosa, mucogingival fold areas, tongue, sublingual andsubmandibular areas, salivary glands, and the tonsilar andpharyngeal areas.
Adverse EventsAdverse events were obtained from subjects and from dental
examinations by the examining dentist
Statistical MethodsStatistical analyses were performed separately for the gingivitis
assessments and plaque assessments. Comparison of the treatmentgroups with respect to baseline gingival index scores and plaqueindex scores were performed using an analysis of variance(ANOVA). Within-treatment comparison of the baseline gingivitisand pre-brushing plaque index scores were performed using pairedt-tests. Comparisons of the treatment groups with respect tobaseline-adjusted gingival and plaque scores at the follow-upexaminations were performed using analyses of covariance(ANCOVAs). The response used for the between-product analyseswas the four- and 12-week endpoints, and the response for thewithin-product analyses was the difference between pre- and post-brushing mean values. All statistical tests of hypotheses were twosided and employed a level of significance of α = 0.05.
ResultsEighty-two (82) subjects were entered into the study and 76
subjects complied with the protocol and completed the clinicalstudy. The gender and age for the subjects who completed thestudy are presented in Table I. No adverse effects were observedby the dental examiner or reported by the participants during the12-week study; six subjects did not complete the study due toFigure 1. An illustration of the Rustogi Modification of the Navy Plaque Index.
Vol. XXIII, Spec. Iss. A The Journal of Clinical Dentistry A13

either protocol non-compliance or an event unrelated to the use ofthe test products.
Table II presents a summary of the mean plaque scores for eachof the three plaque indices measured at each of the measurementtime points. Table III presents a summary of the mean gingivitisand mean gingivitis severity scores measured at each of themeasurement time points. Tables II and III also contain acomparison of the differences in the each of the treatments at eachof the time points. No statistically significant differences were
indicated among the two toothbrush groups with respect to any ofthe plaque or gingivitis scores at the pre-brush examination.
Removal of Supragingival Plaque After a Single Tooth BrushingWhole Mouth Plaque. Toothbrush TC exhibited a statistically
significantly (p < 0.05) greater reduction in whole mouth plaquescores of 0.40 as compared to 0.25 for Toothbrush I.
Gingival Margin Plaque. Toothbrush TC exhibited a statis-tically significantly (p < 0.05) greater reduction in gingival marginplaque scores of 0.12 as compared to 0.01 for Toothbrush I.
Interproximal Plaque. Toothbrush TC exhibited a statisticallysignificantly (p < 0.05) greater reduction in interproximal plaquescores of 0.74 as compared to 0.37 for Toothbrush I.
Reduction of Gingivitis After Four WeeksGingivitis. Toothbrush TC exhibited a statistically significantly
(p < 0.05) greater reduction in gingival index scores of 0.09 ascompared to an increase of 0.01 for Toothbrush I.
Table ISummary of Age and Sex Characteristics for Subjects Who
Completed the Clinical Study
Toothbrush Male Female Total Mean Range
TC 15 25 40 44 18-65
I 10 26 36 42 20-66
Number of Subjects Age
Table IIISummary of the Gingivitis and Gingivitis Severity Scores for Subjects Who Completed the 12-Week Study.
Parameter Toothbrush N Pre-Brushing 4-Week 4-Week Reduction2 12-Week 12-Week Reduction3
Scores1 Scores Difference Scores Difference(Mean ± SD) (Mean ± SD) (Mean ± S.D.)
TC 40 1.16 ± 0.20 1.07 ± 0.29 0.09 ± 0.20 11x 0.74 ± 0.29 0.42 ± 0.24 7x
I 36 1.11 ± 0.13 1.12 ± 0.14 -0.01 ± 0.05 1.05 ± 0.18 0.06 ± 0.11
TC 40 0.18 ± 0.21 0.15 ± 0.20 0.03 ± 0.04 3x 0.04 ± 0.09 0.14 ± 0.15 3.5x
I 36 0.15 ± 0.17 0.14 ± 0.15 0.01 ± 0.11 0.11 ± 0.14 0.04 ± 0.12
Gingivitis
GingivitisSeverity
1Groups are not statistically significantly different from each other at baseline (pre-brushing scores). 2At four weeks, statistically significant (p < 0.05) reductions based on the four-week difference from baseline are indicated as per the ANCOVA comparison of the four-week valuesare shown.3At 12 weeks, statistically significant (p < 0.05) reductions based on the 12-week difference from baseline are indicated as per the ANCOVA comparison of the 12-week values areshown.
Table IISummary of Pre- and Post-Brushing Four-Week and 12-Week Plaque Scores for Subjects Who Completed the 12-Week Study
Parameter Toothbrush N Pre-Brushing Post-Initial Initial Reduction2 4-Week 4-Week Reduction3 12-Week 12-Week Reduction4
Scores1 Brushing Scores Difference Scores Difference Scores Difference(Mean ± SD) (Mean ± SD)
TC 40 0.75 ± 0.09 0.35 ± 0.08 0.40 ± 0.08 1.6x 0.30 ± 0.09 0.45 ± 0.08 2.05x 0.20 ± 0.06 0.55 ± 0.08 1.9x
I 36 0.74 ± 0.09 0.49 ± 0.08 0.25 ± 0.05 0.52 ± 0.09 0.22 ± 0.07 0.45 ± 0.12 0.29 ± 0.09
TC 40 1.00 ± 0.00 0.88 ± 0.10 0.12 ± 0.10 12x 0.82 ± 0.14 0.18 ± 0.14 90x 0.59 ± 0.16 0.41 ± 0.16 8.2x
I 36 1.00 ± 0.00 0.99 ± 0.01 0.01 ± 0.01 0.998 ± 0.01 0.002 ± 0.01 0.95 ± 0.13 0.05 ± 0.13
TC 40 0.99 ± 0.05 0.25 ± 0.27 0.74 ± 0.28 2x 0.12 ± 0.21 0.87 ± 0.22 3.2x 0.02 ± 0.07 0.97 ± 0.08 2.1x
I 36 0.99 ± 0.04 0.62 ± 0.25 0.37 ± 0.24 0.72 ± 0.24 0.27 ± 0.23 0.53 ± 0.36 0.46 ± 0.36
Whole Mouth
Gumline(gingival margin)
Interproximal
1Groups are not statistically significantly different from each other at baseline (pre-brushing scores). 2After the initial brushing, statistically significant (p < 0.05) reductions based on the difference from pre-brushing values are indicated as per the ANCOVA comparison of thedifferences from pre-brushing values are shown.3After four weeks of brushing, statistically significant (p < 0.05) reductions based on the four-week difference from pre-brushing values are indicated as per the ANCOVAcomparison of the four-week values. 4After 12 weeks of brushing, statistically significant (p < 0.05) reductions based on the 12-week difference from pre-brushing values are indicated as per the ANCOVA comparisonof the 12-week values.
Vol. XXIII, Spec. Iss. AThe Journal of Clinical DentistryA14

Gingivitis Severity. Toothbrush TC exhibited a statisticallysignificantly (p < 0.05) greater reduction in gingivitis severityindex scores of 0.03 as compared to 0.01 for Toothbrush I.
Removal of Supragingival Plaque After Four Weeks Whole Mouth Plaque. Toothbrush TC exhibited a statistically
significantly (p < 0.05) greater reduction in whole mouth plaquescores of 0.45 as compared to 0.22 for Toothbrush I.
Gingival Margin Plaque. Toothbrush TC exhibited astatistically significantly (p < 0.05) greater reduction in gingivalmargin plaque scores of 0.18 as compared to 0.002 for Toothbrush I.
Interproximal Plaque. Toothbrush TC exhibited a statisticallysignificantly (p < 0.05) greater reduction in interproximal plaquescores of 0.87 as compared to 0.27 for Toothbrush I.
Reduction of Gingivitis After Twelve WeeksGingivitis. Toothbrush TC exhibited a statistically significantly
(p < 0.05) greater reduction in gingival index scores of 0.42 ascompared to 0.06 for Toothbrush I.
Gingivitis Severity. Toothbrush TC exhibited a statisticallysignificantly (p < 0.05) greater reduction in gingivitis severityscores of 0.14 as compared to 0.04 for Toothbrush I.
Removal of Supragingival Plaque After Twelve WeeksWhole Mouth Plaque. Toothbrush TC exhibited a statistically
significantly (p < 0.05) greater reduction in whole mouth plaquescores of 0.55 as compared to 0.29 for Toothbrush I.
Gingival Margin Plaque. Toothbrush TC exhibited astatistically significantly (p < 0.05) greater reduction in gingivalmargin plaque scores of 0.41 as compared to 0.05 for Toothbrush I.
Interproximal Plaque. Toothbrush TC exhibited a statisticallysignificantly (p < 0.05) greater reduction in interproximal plaquescores of 0.97 as compared to 0.46 for Toothbrush I.
DiscussionThe removal of supragingival plaque (biofilm) is essential in
preventing gingivitis. The mechanical removal of plaque by toothbrushing is still the best way to attain a plaque-free mouth. TheAmerican Dental Association recommends twice-daily, two-minute tooth brushing as being effective to remove plaque anddeliver fluoride. When brushing, most people tend to form patternsthat miss areas, such as the interproximal and gum margin areas.There are basically two types of toothbrushes: manual and power.Power brushing is designed to mechanically remove as muchplaque as possible, particularly in inaccessible areas of the oralcavity, such as fissures, interproximal, and sub-gingival areas. Themotion from a power toothbrush has been demonstrated in vitro todrive fluid dynamic forces beyond the reach of the toothbrushbristles into inaccessible interproximal spaces, resulting inimproved biofilm removal in these areas.22
The purpose of this clinical study was to assess the plaque andgingivitis efficacy of a new specially engineered sonic poweredtoothbrush with unique sensing and control technologies whencompared to a commercially available manual flat-trim toothbrush.The data from this study demonstrate that the new sonic powered
toothbrush provides statistically significantly greater levels ofefficacy in the removal of dental plaque after a single toothbrushing and after four and 12 weeks of use when compared to amanual flat-trim toothbrush on all measured sites: whole mouth,gumline (gingival margin), and interproximal. The new sonicpowered toothbrush also provides statistically significantly greaterlevels of efficacy in the reduction of gingivitis and gingivalbleeding when compared to the manual flat-trim toothbrush afterfour and 12 weeks of use.
It can be concluded that this new specially engineered sonicpowered toothbrush with unique sensing and control technologiesprovides statistically significantly greater levels of efficacy in theremoval of dental plaque after a single tooth brushing and afterfour and 12 weeks, and greater levels of efficacy in the reductionof gingivitis and gingival bleeding after four and 12 weeks of usewhen compared to a manual flat-trim toothbrush.
Acknowledgement: This study was supported by the Colgate-PalmoliveCompany.
For correspondence with the authors of this paper, contactPatricia Chaknis – [email protected].
References1. Moore WE, Holdeman LV, Cato EP, Smibert RM, Burmeister JA, Ranney
RR. Bacteriology of moderate (chronic) periodontitis in mature adult humans. Infect Immun 1983;42:510-5.
2. Paster BJ, Boches SK, Galvin JL, Ericson RE, Lau CN, Levanos VA,Sahasrabudhe A, Dewhirst FE. Bacterial diversity in human subgingival plaque. J Bacteriol 2001;183:3770-83.
3. Kolenbrander PE. Oral microbial communities: biofilms, interactions, and genetic systems. Ann Rev Microbiol 2000;54:413-37.
4. Scannapieco FA. Periodontal inflammation: from gingivitis to systemic disease? Compend Contin Educ Dent 2004;25(7 Suppl 1):16-25.
5. Taylor G. Consensus statement on oral and systemic health. Inside Dent2006;2(Spec Iss):1-6.
6. Ash Jr MM, Rainey BL, Smith WA. Evaluation of manual and motor-driven toothbrushes. J Am Dent Assoc 1964;96:321-5.
7. Sharma NC, Galustians HJ, Qaqish J, Cugini M. Safety and plaque removal efficacy of a battery-operated power toothbrush and a manual toothbrush. Am J Dent 2001;14:9B-12.
8. Farrell S, Terezhalmy GT, Bartizek RD, Biesbrock AR. Comparative plaque removal efficacy of a dual-action power toothbrush and a manual toothbrush: Effects by tooth type. Am J Dent 2006;19:195-200.
9. Zimmer S, Didner B, Roulet JF. Clinical study on the plaque-removing ability of a new triple-headed toothbrush. J Clin Periodontol 1999;26:281-5.
10. Zimmer S, Fosca M, Roulet JF. Clinical study of the effectiveness of two sonic toothbrushes. J Clin Dent 2000;11:24-7.
11. Versteeg PA, Timmerman MF, Paraskevas S, van der Weijden GA. Evaluation of several brushing motion combinations in relation to plaque-removing efficacy with Oral-B Cross Action Power: a professional brushing study. Int J Dent Hyg 2006;4:204-8.
12. Heanue M, Deacon SA, Deery C, Robinson PG, Walmsley AD,Worthington HV, Shaw WC. Manual versus powered toothbrushes for oral health. Cochrane Database Syst Rev 2003;(1):CD002281.
13. Robinson PG, Deacon SA, Deery C, Heanue M, Walmsley AD,Worthington HV, Glenny AM, Shaw WC. Manual versus powered tooth brushing for oral health. Cochrane Database Syst Rev2005;(2):CD002281.
14. Deacon SA, Glenny AM, Deery C, Robinson PG, Heanue M, Walmsley AD, Shaw WC. Different powered toothbrushes for plaque control and gingival health. Cochrane Database Syst Rev 2010 Dec 8;(12):CD004971.
15. Putt MS, Milleman JL, Jenkins W, Olson M, Schmitt PJ. Plaque removal efficacy of sonic versus manual toothbrushes in children. Int J Ped Dent
Vol. XXIII, Spec. Iss. A The Journal of Clinical Dentistry A15

2009;19(Suppl S1):P08-14.16. Warren PR, Ray TS, Cugini M, Chater BV. A practice-based study of a
power toothbrush: assessment of effectiveness and acceptance. J Am Dent Assoc 2000;131:389-94.
17. Williams K, Rapley K, Haun J, Walters P, Grender J, He T, Biesbrock AR. Benefit of the power component of sonic and rotation-oscillation modes of action for plaque removal using power toothbrushes. Am J Dent 2010;23:60-4.
18. Rustogi KN, Curtis JP, Volpe AR, Kemp JH, McCool JJ, Korn LR. Refinement of the Modified Navy Plaque Index to increase plaque scoring efficiency in gumline and interproximal tooth areas. J Clin Dent1992;3(Suppl C):C9-12.
19. Löe H, Silness J. Periodontal disease in pregnancy. I. Prevalence and severity. Acta Odontol Scand 1963;21:533-51.
20. Garcia-Godoy F, Garcia-Godoy F, DeVizio W, Volpe AR, Ferlauto RJ,Miller JM. Effect of a triclosan/copolymer/fluoride dentifrice on plaque formation and gingivitis: A 7-month clinical study. Am J Dent1990;3:S15-26.
21. Talbott K, Mandel ID, Chilton NW. Reduction of baseline gingivitis scores in repeated prophylaxes. J Prev Dent 1977;4:28-9.
22. Aspiras M, Elliott N, Nelson R, Hix J, Johnson M, deJager M. In vitroevaluation of interproximal biofilm removal with power toothbrushes. Compend Contin Educ Dent 2007;28(9 Suppl 1):10-4.
Vol. XXIII, Spec. Iss. AThe Journal of Clinical DentistryA16

Laboratory Evaluation of Plaque Removalat Interproximal Sites by a Specially Engineered Powered Toothbrush
with Unique Sensing and Control Technologies
James H. Kemp
Colgate-Palmolive Technology CenterPiscataway, NJ, USA
Caren M. Barnes
Department of Dental Hygiene, University of Nebraska College of DentistryLincoln, NE, USA
Christine M. Spirgel, Xiuren Shi, Samuel L. Yankell
YRC Inc.Moorestown, NJ, USA
Abstract• Objective: This laboratory study compared a specially engineered sonic powered toothbrush with unique sensing and control tech-
nologies and having two different brush heads to a manual flat-trim toothbrush for their ability to remove plaque at interproximal sites.• Methods: Interproximal access efficacy (IAE) was measured as the maximum width of plaque removed from the artificial plaque
substrate around the teeth. Six brushes of each product were tested four times for a total of 24 tests. Results from these tests were statistically analyzed using an analysis of variance (ANOVA). A post hoc Tukey test for pair-wise comparisons, with a minimum significance level of 0.05, was used to identify significant mean differences between the test products.
• Results: Relative to the manual flat-trim toothbrush, the sonic powered toothbrush, equipped with either the Triple Clean or Sensitive refill brush head, had statistically significantly higher IAE means (p < 0.001). In addition, when equipped with the Sensitive refill brush head, the new sonic powered toothbrush showed increased efficiencies compared to when it was equipped with the Triple Clean brush head with respect to IAE means.
• Conclusion: The specially engineered sonic powered toothbrush with unique sensing and control technologies had higher interproximal access efficacy compared to a manual flat-trim toothbrush, particularly with the Sensitive brush head.
(J Clin Dent 2012;23[Spec Iss A]:A17-A20)
A17
IntroductionIt has been accepted that the two most common dental
diseases, dental caries and periodontal disease, can be prevented or alleviated by adequate removal of dental plaque. These deposits accumulate primarily at interproximal sites and on the gingival third of the premolar and molar teeth, and thenproliferate below the gingival margin. The primary reason why dental plaque thrives in these areas is that they are the most difficultareas to access when brushing.1 These are the same areaspredominantly associated with gingivitis and related periodontaldiseases, because of this plaque accumulation.2-6
There have been many oral hygiene devices designed to augmentdental plaque removal via tooth brushing, such as interdental brushesand various types of floss. While these adjunct devices are readilyavailable, they are underutilized, which leaves the toothbrush as theprimary plaque removal device for most individuals.6 The challengehas been to design a toothbrush with enhanced capability to removedental plaque from hard-to-reach areas, such as the gingival margin,the gingival sulcus, and interdental surfaces, and thereby improve
general oral health.5,7-9 The past fifty years has seen the developmentof many manual toothbrush designs based on scientific research thathave focused on all aspects of the toothbrush.10,11 Toothbrush handleshave been redesigned to be more ergonomically acceptable, and haveadditions such as thumb rests and ripples in the handle to improvegrip and control. Toothbrush heads have been designed in a varietyof sizes and shapes that include circular, oval, and diamond-shaped,as well as angulation of the head placement. Notably, toothbrushbristles have received the most attention in reconfiguration and newdesigns. Examples of toothbrush bristle designs include flat, bi-level,multi-level, multi-tufted,V-shaped, curved, rippled, angled, tapered,and bristles that change color to indicate length of use (or wearindicators).12
Toothbrush stiffness depends on several factors, including bristlediameter, tuft hole diameter, tuft hole packing factor, tuft height, andthe product trim profile. Generally, the higher the tuft or trim heightthe softer the product will be. Conversely, the shorter the tuft ortrim height the stiffer or firmer the product will be. The longer afilament/strand/bristle the more pliable or flexible it will be. The

shorter the filament/strand/bristle the less pliable or more rigid orstiffer it will be.
Regarding bristle stiffness, the soft bristle has been establishedas the professional standard for recommendation to patients. Whilemedium and hard bristle toothbrushes are still available, toothbrushmanufacturers and dental professionals have focused on providingthe soft texture bristle toothbrushes. With proper tooth brushingtechnique, soft bristle toothbrushes have many advantages over stifferbristled brushes, as the soft bristles can remove dental plaque andbiofilm more efficiently in the cervical, proximal, and marginal areasof the tooth, as well as being safe for cleaning the gingival sulcuswithout causing soft tissue trauma, as a result of their pliability.
The first modern powered toothbrush was reported in the literaturein 1938, and a more advanced version, Broxodent by E.R. Squibb& Sons Company, was introduced after World War II in Switzerland.In 1961, General Electric introduced a rechargeable cordless poweredtoothbrush.13 Each of these toothbrushes had basic designs modeledafter manual toothbrushes. Both models had similar reciprocalbrushing actions. Clinical research on these powered toothbrushescompared them to manual toothbrushes, with the results rangingfrom no significant difference between manual and poweredtoothbrushes14,15 to reporting that powered toothbrushes improvedgingivitis.16 These early powered toothbrushes were notoverwhelmingly popular with dental professionals because they feltthat compulsive brushers would use them excessively and damagesupporting soft tissues.16
Interest in powered toothbrushes was renewed in the 1980s whenseveral technological advances were made; additional advances havecontinued to date.17-24 The speed at which some powered bristlesvibrate is now labeled as sonic or ultrasonic.The brush head motions currently available include simple rotary,vertical vibration, three-dimensional counter-rotational pulsationplus oscillation, and one particular brush that has individual tufts ofbristles that rotate 1.5 turns in one direction and 1.5 turns in theopposite direction.12 Many of the shapes of powered brush headsmirror those of manual toothbrushes, but some powered brushes alsoinclude round brush heads.
The majority of the changes that appear in all aspects ofcontemporary toothbrush design and materials have focused onimproving dental plaque removal, especially in the hard-to-reachareas, at the gingival margin, the gingival sulcus, and the interproximalspaces. There have been numerous clinical trials and laboratorystudies comparing the efficacy and safety of these new, unique, orenhanced toothbrushes. Many studies, both clinical and laboratory,have concluded that powered toothbrushes are safe and equal to orsuperior to manual toothbrushes in dental plaque removal.25-30
The purpose of this laboratory study was to evaluate a newspecially engineered sonic powered toothbrush with unique sensingand control technologies using two different refill brush heads, incomparison to an ordinary manual flat-trim toothbrush for their abilityto remove plaque at interproximal sites. Since 1983, an in vitro methodhas been used to evaluate interproximal access. The InterproximalAccess Efficacy assay (IAE) assesses the ability of toothbrush bristlesto penetrate between simulated teeth and remove plaque duringthe tooth brushing procedure. Overall IAE results have been predictiveof clinical plaque removal efficacy.31-54
Materials and MethodsA specially designed sonic powered toothbrush with unique
sensing and control technologies, with two different brush heads,was compared to a manual flat-trim toothbrush for their ability toremove plaque at interproximal sites using a laboratory assay knownas Interproximal Access Efficacy (IAE).37,55 The following test productswere used.
TC: Colgate®ProClinical™A1500 Power Toothbrush with Triple Clean Brush Head (Colgate-Palmolive Company, New York,NY, USA)
S: Colgate® ProClinical™ A1500 Power Toothbrush with Sensitive Brush Head (Colgate-Palmolive Company, New York, NY, USA)
I: Manual flat-trim toothbrush; Oral-B® Indicator Toothbrush (Procter & Gamble Company, Cincinnati,OH, USA)
In the assay, six brushes from each test product group wereevaluated four times for a total of 24 tests. All toothbrushes werestored in the laboratory at a temperature of 67–70o for at least 48hours before testing. The laboratory equipment was fabricated to thedesign of Nygaard-Ostby, et al.37 and was further modified to thedesign of Shi, et al. to affix toothbrushes by the handle.54
In the IAE assay, the brushing technique involved independentevaluations of each toothbrush in a vertical and horizontal brushingmotion with tooth shapes simulating anterior and posterior teeth.The brushing apparatus was set to brush for 15 seconds at two strokesper second with a 50 mm stroke. The maximum width of artificialplaque removed from the plaque substrate placed around the teethwas recorded in centimeters (cm). Toothbrushes TC and S wereevaluated using the Auto Mode, i.e., with the power on.
Before and after the assay completion, the brush heads werevisually examined for bristle integrity. The same examiner performedboth efficacy and toothbrush integrity evaluations.
Results for all brushing comparisons were statistically analyzedusing an analysis of variance (ANOVA). A post hoc Tukey test forpair-wise comparisons with a minimum significance level of 0.05was used to identify significant mean differences between the testproducts.
ResultsToothbrush Bristle Integrity
A summary of IAE means for both anterior- and posterior-shapedteeth is presented in Table I. The IAE means on anterior and posteriortooth shapes with vertical brushing are statistically significantlyhigher for the TC and S groups than for the I group (p < 0.001).On both anterior and posterior tooth shapes, the S group hasstatistically significantly higher mean IAE compared to the TC group(p < 0.001). With horizontal brushing, the mean IAE on anterior tooth shapes is statistically signifi cantly higher for the TC and S groups than for the I group (p < 0.001). Overall resultscombining IAE data using vertical and horizontal brushing motionsand anterior and posterior tooth shapes are depicted graphically inFigure 1. The overall IAE means for the TC and S groups arestatistically signifi cantly higher compared to the overall mean IAE value for the I group (p < 0.001). The S group has statisticallysignificantly higher mean IAE compared with the TC group (p < 0.001).
Vol. XXIII, Spec. Iss. AThe Journal of Clinical DentistryA18

DiscussionThere are many clinical methods to assess plaque removal with
toothbrushes and other oral hygiene aids and devices. These methodsare based on plaque indices because they provide a quantitativemeasure for analyzing dental conditions in individuals and groups.Most clinical studies are designed to evaluate plaque removal onspecific surfaces of the teeth, especially the areas that individualshave a hard time reaching with a toothbrush, such as the gingivalmargin, the gingival sulcus, and the interproximal areas. Therefore,plaque indices that focus on these areas are selected to use as partof the study design. Popular plaque indices used in clinical toothbrushevaluations and comparisons include the Turesky Modification ofthe Quigley-Hein Index, the Proximal Marginal Index, the Green andVermillion Oral Hygiene Index, and the Rustogi Modification of theModified Navy Plaque Index.56
The laboratory method used in this study has been predictive ofclinical efficacy for toothbrushes.4,39,42,47,57 A key element of thesemethods is the use of a pressure-sensitive plaque substrate54 that canbe used on tooth contours and under the gingival margin with wetbrushing conditions. The gingival margins for the laboratory modelswere replicated according to textbook descriptions, and the artificialplaque material was adhered to the substrate in order to providecomparative measures of the removal of perigingival and/orsupragingival artificial plaque. Toothbrushes can be tested usingsimulated clinical brushing conditions. The toothbrushes can be testedin vertical and horizontal directions of artificial anterior and posteriorteeth, and in a wet environment with brushing timed in seconds.
Clinical studies are usually tightly controlled, but standardizationand uncontrollable variables are vulnerable areas. Some variables
that are impossible to control are subject-to-subject differences intooth brushing and variations in brushing pressures and techniques.These particular variables have been eliminated with the laboratorymethods used in this study to evaluate interproximal access. Further,laboratory testing is economical, faster, and more standardized thana clinical trial.
The results of the laboratory assessments of a new speciallyengineered sonic powered toothbrush with unique sensing and controltechnologies with either of two different brush heads indicate that thetoothbrush bristles penetrate into interproximal areas. Since dentalplaque is difficult to remove in these areas, and they are vulnerableto dental caries, gingivitis, and more advanced forms of periodontaldisease, the new sonic powered toothbrush with either brush head isexpected to be highly efficacious for plaque removal in vivo and may,therefore, offer advantages in the prevention of dental caries andperiodontal disease.
ConclusionRelative to the manual flat-trim toothbrush, the specially engineered
sonic powered toothbrush with unique sensing and controltechnologies, equipped with either the Triple Clean or Sensitive refillbrush head, has statistically significantly higher IAE means (p < 0.001). In addition, when equipped with the Sensitive refill brushhead, this new sonic powered toothbrush shows increased efficienciesas compared to when it is equipped with the Triple Clean brush headwith respect to IAE means.
Acknowledgement. This study was sponsored by the Colgate-PalmoliveCompany.
For correspondence with the authors of this paper, contactJames A. Kemp – [email protected] or Dr. S. L.Yankell – [email protected].
References1. Cugini M, Warren PR. The Oral-B CrossAction manual toothbrush: a 5-year
literature review. J Can Dent Assoc 2006;72:323a.2. Löe H, Theilade E, Jensen SB. Experimental gingivitis in man. J Periodontol
1965;36:177-87.3. Armitage GC. Periodontal diseases: diagnosis. In: Annals of Periodontology World
Workshop in Periodontics. Genco RJ, ed. American Academy of Periodontology,Chicago pp. 37-215, 1996.
4. Saxer UP,Yankell SL. Impact of improved toothbrushes on dental diseases. II. Quintessence Int 1997;28:573-93.
5. Schiff T, Proskin HM, Zhang YP, Petrone M, DeVizio W. A clinical investigation of the efficacy of three different treatment regimens for the control of plaque and gingivitis. J Clin Dent 2006;17:138-44.
6. Yost KG, Mallatt ME, Liebman J. Interproximal gingivitis and plaque reduction by four interdental products. J Clin Dent 2006;17:79-83.
7. Biesbrock AR, Barzitek RD, Walters PA. Improved plaque removal efficacy with a new manual toothbrush. J Contemp Dent Prac 2008;9:1-8.
8. Térezhalmy GT, Biesbrock AR, Walters PA, Grender JM, Barzitek RD. Clinical evaluation of brushing time and plaque removal potential of two manual toothbrushes. Int J Dent Hyg 2008;6:321-7.
9. Yankell SL, Barnes CM, Shi X, Cwik J. Laboratory efficacy of three compact toothbrushes to reduce artificial plaque in hard to reach areas. Am J Dent
2011;24:195-9.10. Beals D, Ngo T, Feng Y, Cook D, Grau DG, Weber DA. Development and
laboratory evaluation of a new toothbrush with a novel brush head design. Am J Dent 2000;13(Spec No):5A-14.
11. Barnes CM, Covey DA, Shi X,Yankell SL. Laboratory evaluations of a bi-level,extremely tapered bristled toothbrush and a conventional uniform bristled toothbrush. Am J Dent 2009;22:84-8.
Figure 1. Overall mean IAE (±SD)
Table IInterproximal Access Effi cacy on Anterior and
Posterior Shaped Teeth
Toothbrush Anterior Posterior Anterior PosteriorGroup Teeth Teeth Teeth Teeth
TC 1.20 ± 0.05 1.38 ± 0.08 0.97 ± 0.03 0.94 ± 0.04
S 1.34 ± 0.07 1.58 ± 0.08 1.12 ± 0.07 1.44 ± 0.06
I 0.87 ± 0.09 1.08 ± 0.04 0.70 ± 0.06 0.97 ± 0.09
Vertical Brushing Horizontal Brushing
Mean IAE (cm) ± SD
Vol. XXIII, Spec. Iss. A The Journal of Clinical Dentistry A19
12. Wilkins EM. Clinical Practice of the Dental Hygienist. 11th Ed. Lippincott,Williams & Wilkins, Philadelphia, pp. 386-91, 2012.
13. Barnes CM. Devices for oral self-care. In: Mosby’s Dental Hygiene Concepts,Cases and Competencies, Daniel SJ, Harfst SA, Wilder RS, eds. Mosby Inc.,St. Louis, pp. 450-6, 2008.
14. Chilton NW, DiDio A, Rothner JT. Comparison of the clinical effectiveness of an electric and a standard toothbrush in normal individuals. J Am Dent Assoc 1962;64:777-82.
15. Smith WA,Ash MM. A clinical evaluation of an electric toothbrush. J Periodontol 1963;20:127-36.
16. Barnes CM. Powered toothbrushes: a focus on the evidence. Compend Oral Hyg 2002;7:3-10.
17. Mueller LJ, Darby ML,Allen DS, Tolle SL. Rotary electric toothbrushing. Clinical effects on the presence of gingivitis and supragingival dental plaque. Dent Hyg (Chic) 1987;61:546-50.
18. Babb DA, Johnson RH. The effect of a new electric toothbrush on supragingival plaque and gingivitis. J Periodontol 1989;60:336-41.
19. Barnes CM, Weatherford TW 3rd, Menaker L. A comparison of the Braun Oral-B Plaque Remover (D5) electric and a manual tooth brush in affecting gingivitis. J Clin Dent 1993;4:48-51.
20. Van der Weijden GA, Timmerman MF, Nijboer A, Lie MA,Van der Velden U. A comparative study of electric toothbrushes for the effectiveness of plaque removal in relation to toothbrushing dura tion. Timer study. J Clin Periodontol 1993;20:476-81.
21. Stanford CM, Srikantha R, Wu CD. Efficacy of the Sonicare toothbrush fluid dynamic action on removal of human supragingival plaque. J Clin Dent 1997;8(1 Spec No):10-4.
22. Driesen GM,Warren PR, Hilfinger P. Cleaning efficacy of a new electric toothbrush. Am J Dent 1998;11(spec No):S7-11.
23. Biesbrock AR, Walters PA, Barzitek RD, Goyal CR, Qaqish JG. Plaque removal efficacy of an advanced rotation-oscillation power toothbrush versus a new sonic toothbrush. Am J Dent 2008;21:185-8.
24. Yankell SL, Shi X, Spirgel CM, Stiller S. Interproximal access efficacy of one vibrating and two powered oscillating-rotating toothbrushes. J Clin Dent 2011;22:55-8.
25. Walters PA, Cugini M, Biesbrock AR, Warren PR. A novel oscillating-rotating power toothbrush with SmartGuide; designed for enhanced performance and compliance. J Contemp Dent Pract 2007;8:1-9.
26. Cugini M, Thompson M, Warren PR. Correlations between two plaque indices in assessment of toothbrush effectiveness. J Contemp Dent Pract 2006;7:1-9.
27. Robinson PG, Deacon SA, Deery C, Heanue M,Walmsley AD,Worthington HV,Glenny AM, Shaw WC. Manual versus powered toothbrushing for oral health. Cochrane Database Syst Rev 2005;(2):CD002281.
28. Deery C, Heanue M, Deacon S, Robinson PG, Walmsley AD, Worthington H,Shaw W, Glenny AM. The effectiveness of manual versus powered toothbrushes for dental health: a systematic review. J Dent 2004;32:197-211.
29. Sharma N, Galustians HJ, Qaqish JG, Rustogi KN, Petrone ME, Volpe AR. Comparative efficacy on supragingival plaque and gingivitis of a manual toothbrush (Colgate Plus) and a battery-powered toothbrush (Colgate Actibrush) over a 30-day period. Compend Contin Educ Dent 2000;31(Suppl):S9-13.
30. Moran JM,Addy M, Newcombe RG. A comparative study of stain removal with two electric toothbrushes and a manual brush. J Clin Dent 1995;6:188-93.
31. Schifter CC, Emling RC, Seibert JS,Yankell SL. A comparison of plaque removal effectiveness of an electric versus a manual toothbrush. Clin Prev Dent 1983;5:15-9.
32. Yankell SL, Green PA, Greco PM, Stoller NH, Miller MF. Test procedures and scoring criteria to evaluate toothbrush effectiveness. Clin Prev Dent 1984;6:3-8.
33. Yankell SL, Shi X, Emling RC. Comparative laboratory evaluation of three toothbrushes regarding interproximal access efficacy. J Clin Dent 1992;3(Suppl C):C5-8.
34. Yankell SL, Shi X, Emling RC. Laboratory interproximal access efficacy comparison of a rippled bristled toothbrush and a flat manual toothbrush. J Clin
Dent 1993;4:82-4.35. Emling RC,Yankell SL, Shi X, Smith JC. Three laboratory assessments of a new
triple-head toothbrush and the Oral-B 40 toothbrush. J Clin Dent 2005;16:6-10.36. Yankell SL, Shi X, Spirgel CM. Laboratory interproximal access efficacy of four
elmex caries protection toothbrushes. J Clin Dent 2012;23:27-31.37. Nygaard-Ostby P, Edvardsen S, Spydevold B. Access to interproximal tooth
surfaces by different bristle designs and stiffness of toothbrushes. Scand J Dent Res 1979;87:424-30.
38. Yankell SL, Nygaard-Ostby P. Evaluating cleaning efficiency of different toothbrush designs and textures. J Soc Cosmet Chem 1983;34:151-7.
39. Volpe AR, Emling RC,Yankell SL. The toothbrush – a new dimension in design,engineering, and clinical evaluation. J Clin Dent 1992;3(Suppl C):C29-33.
40. Yankell SL, Shi X, Emling RC. Comparative laboratory evaluations of two new toothbrushes regarding interproximal access efficacy. J Clin Dent 1993;4(Suppl D):D1-4.
41. Battista GW, Petrone DM. Comparison of the laboratory interproximal access efficacy of the Colgate Precision toothbrush and the Crest Complete toothbrush. J Clin Dent 1993;4(Suppl D):D5-7.
42. Yankell SL, Shi X, Emling RC, Blatz B, Biesbrock AR. Laboratory evaluations of two battery-powered toothbrushes and a manual toothbrush for efficacy and safety. J Clin Dent 2002;13:187-90.
43. Yankell SL, Shi X, Emling RC. Laboratory evaluations of two toothbrushes for removal of artificial plaque above, around and below the gingival margin. J Clin Dent 2003;14:19-22.
44. Balanyk TE, Sharma NC, Galustians J. A clinical study of comparative plaque removal performance of two manual toothbrushes. J Clin Dent 1993;4(Suppl D):D8-12.
45. Singh SM, Deasy MJ. Clinical plaque removal performance of two manual toothbrushes. J Clin Dent 1993;4(Suppl D):D13-6.
46. Haun J, Williams K, Friesen L, Ferrante A, Walters PA, Bartizek RD, Biesbrock AR. Plaque removal efficacy of a new experimental battery-powered toothbrush relative to two advanced-design manual toothbrushes. J Clin Dent 2002;13:191-7.
47. Biesbrock AR,Walters PA, Bartizek RD: The relative effectiveness of six powered toothbrushes for dental plaque removal. J Clin Dent 2002;13:198-202.
48. Dörfer CE, von Bethlenfalvy ER, Hugel B, Pioch T. Cleaning efficacy of a manual toothbrush with tapered filaments. Oral Health Prev Dent 2003;1:111-8.
49. Mankodi S, Wachs GN, Petrone DM, Chaknis P, Petrone M, DeVizio W, Volpe AR. Comparison of the clinical efficacy of a new manual toothbrush on gingivitis reduction and plaque removal. Compend Contin Educ Dent 2004;25:28-36.
50. Nathoo S, Chaknis P, Petrone M, DeVizio W, Volpe AR. A clinical comparison of the gingivitis reduction and plaque-removal efficacy of a new manual toothbrush. Compend Contin Educ Dent 2004;25(10 Suppl 2):37-45.
51. Sgan-Cohen HD,Vered Y. A clinical trial of the meridol toothbrush with conical filaments: evaluation of clinical effectiveness and subjective satisfaction. J Clin Dent 2005;16:109-13.
52. Sowinski J, Petrone DM, Wachs GN, Chaknis P, Kemp J, Sprosta AA, DeVizio W. Efficacy of three toothbrushes on established gingivitis and plaque. Am J Dent 2008;21:339-45.
53. Sgan-Cohen HD, Livny A, Vered Y. The elmex SENSITIVE toothbrush: effect on plaque reduction and subjective satisfaction after two months. J Clin Dent 2008;19:22-7.
54. Shi X, Emling RC,Yankell SL. A new laboratory method for in vitro evaluation of the interproximal penetration of manual toothbrushes. J Dent Res 1995;74:49.
55. Yankell SL, Shi X, Emling RC, Harris M. Laboratory evaluation of the Reach Tooth & Gum Care toothbrush and three additional manual toothbrushes for subgingival access. J Clin Dent 1998;9:1-4.
56. Dababneh RH, Khouri AT, Smith RG,Addy M. A new method of plaque scoring:a laboratory comparison with other plaque indices. J Clin Periodontol 2002;29:832-7.
57. Saxer UP,Yankell SL. A review of laboratory methods to determine toothbrush safety and efficacy. J Clin Dent 1997;8:114-9.
Vol. XXIII, Spec. Iss. AThe Journal of Clinical DentistryA20
Laboratory Evaluation of Extrinsic Stain Removal by a Specially Engineered Sonic Powered Toothbrush with
Unique Sensing and Control Technologies
Venda P. Maloney, James Kemp, Fotinos Panagakos
Colgate-Palmolive Technology CenterPiscataway, NJ, USA
Luis R. Mateo
LRM Statistical ConsultingHoboken, NJ, USA
Abstract• Objective: The purpose of this laboratory study was to evaluate extrinsic stain removal from teeth by a specially engineered sonic
powered toothbrush with unique sensing and control technologies, using the Triple Clean and the Sensitive refill brush heads, in comparison to a manual flat-trim toothbrush.
• Methods: Twelve (12) artificially stained bovine teeth were tested with each product. The percentage of stain removed by each product was calculated by taking the ratio of the amount of stain removed by brushing for 800 strokes to the total amount of stain removed by subsequent application of a dental prophylaxis. The stain was quantified by measuring the light reflected by the stained teeth with a spectrophotometer. Data were reported as L*, lightness of the stain, and as W*, a whiteness index comprising the lightness, hue, and chroma of reflected light. Statistical analyses were performed separately for the ∆L* and ∆W* scores. Comparisons of the toothbrushes with respect to baseline-adjusted ∆L* and ∆W* scores were performed using an analysis of covariance (ANCOVA). Post-ANCOVA pair-wise comparisons of the study toothbrushes were performed using Tukey’s test for multiple comparisons. All statistical tests of hypotheses were two-sided, and employed a minimum level of significance of 0.05.
• Results: The percentage of stain removed by the sonic powered toothbrush, using either the Triple Clean brush head or the Sensitive brush head under laboratory test conditions, is superior (p < 0.05) to the percentage of stain removed by the manual flat-trim toothbrush when analyzed for both the ∆L* and ∆W* scores. The mean percentage of stain removed was 62.10 for the power toothbrush with the Triple Clean brush head, 49.01 for the power toothbrush with the Sensitive brush head, and 30.56 for the manual flat-trim toothbrush when calculated using ∆L* scores. The mean percentage of stain removed was 59.89 for the power toothbrush with the Triple Clean brush head, 46.83 for the power toothbrush with the Sensitive brush head, and 29.25 for the manual flat-trim toothbrush when calculated using ∆W* scores.
• Conclusions: This new specially engineered sonic powered toothbrush with unique sensing and control technologies effectively removes extrinsic stains from the surface of teeth under laboratory test conditions with both the Triple Clean and the Sensitive brush heads. The effectiveness of stain removal with either brush head is significantly greater than the effectiveness of stain removal of a manual flat-trim toothbrush under these conditions.
(J Clin Dent 2012;23[Spec Iss A]:A21-A25)
IntroductionTooth whitening is a growing category in oral care. Various
product forms, including strips, trays, mouthwashes, dentifrices,and toothbrushes all claim to deliver tooth whitening benefits ofvarious magnitudes to the consumer. These products providewhitening through various modes of action. Bleaching agents,such as peroxide, are commonly applied to teeth with a strip ortray, but they can also be added to mouthwash and dentifriceproducts.1-3 Bleaching agents are known to be effective againstboth intrinsic and extrinsic stains as they chemically react withstain molecules to render stains colorless.2 Other whiteningingredients, including detergents and chelating molecules, areused in dentifrices and mouthwashes to assist in the removal ofloosely bound extrinsic stains.2,3 Abrasives are used in
dentifrices to mechanically remove extrinsic stain.1-3 To cleaneffectively, abrasives are scrubbed against the tooth by atoothbrush.2 The design of a toothbrush can influence themotion of the abrasive particles during brushing and haveresulting impact on the effectiveness of stain removal. An invitro brushing model was created to follow the movement ofabrasive particles against toothbrush bristles during the actionof brushing.4 Using this model, it was determined that whenfilament tufts were designed so that they deploy evenly overthe surface during use, good particle trapping by the toothbrushwas observed. Bristles with rounded tips were also found to bemore effective than bristles with flat tips in trapping abrasiveparticles. Finally, power toothbrushes were found to causegreater particle movement and trapping than manual brushes.
A21

Clinical studies have confirmed that power toothbrushes arecapable of removing more extrinsic stain than manualtoothbrushes.5-7 A clinically significant reduction in stain frombaseline has been measured with different types of powertoothbrushes.8-10
In order to optimize dentifrice formulas and toothbrushdesign to maximize stain removal, in vitro models have beendeveloped. The general procedures described in mostpublications are adapted from the method developed byStookey, et al. known as the Pellicle Cleaning Ratio (PCR)method.11 In this method, enamel blocks are cut from bovinecentral incisors and mounted in a resin so that only the enamelis exposed. The enamel is cycled through a staining brothconsisting of food stains, salivary proteins, and bacteria thatpromote stain formation, until a dark, substantive film isformed on the enamel. The stained teeth are brushed on a V-8cross-brushing machine to ensure experimental control over theapplied force, speed, and slurry dilution. The Stookey, et al.study found that the amount of stain removed after brushingfor 800 double strokes in this model correlated well with theclinically measured stain removal for 22 different dentifriceproducts.11 Since the publication of the PCR method in 1982, ithas been accepted as the industry standard method to evaluatethe cleaning performance of dentifrice formulas in thelaboratory. It has also been adapted to test the stain removalperformance of toothbrushes. Common changes to the methodinclude a reduction in the applied force from 250 g to 150 gwhen testing power toothbrushes to model consumer usage ofthese products.12-14 Often, the brushing machine must alsoundergo a change to the geometry to accommodate differenttoothbrush handles.13,14 In addition, rather than reporting thestain removal relative to brushing with a standard abrasive ordentifrice control, the stain removed by brushing has beenreported against the total amount of stain that can be removedby treatment with an abrasive dental prophylaxis.15 Finally,there have been changes in grading from visual grading of stainintensity to instrumental grading of stain intensity through themeasurement of reflected light.13-15 This paper describes the invitro stain removal efficacy of a new specially engineered sonicpowered toothbrush with unique sensing and controltechnologies, and details the adaptations made to the PCRmethod in this study. The stain removal performance of twodifferent refill brush head designs is reported and compared tothe performance of a flat-trim manual toothbrush. Thepercentage of stain removed by all three test products isreported relative to the total amount of stain removed by adental prophylaxis.
Materials and MethodsThe specially engineered sonic powered toothbrush with
unique sensing and control technologies (Colgate® ProClinical™
A1500 Power Toothbrush, Colgate-Palmolive Company, NewYork, NY, USA), fitted with either the Triple Clean refill brushhead (TC) or the Sensitive refill brush head (S), was evaluatedand compared to the Oral-B® Indicator 40 manual toothbrush(I) labeled “soft texture” (Procter & Gamble Company,Cincinnati, OH, USA). The in vitro method to measure
extrinsic stain removal used in this study closely followed thatdescribed by Stookey, et al.11 Modifications to the method weremade to accommodate the geometry and usage conditions ofthe power toothbrush, in the use of a spectrophotometer, and inthe use of a dental prophylaxis to determine the reference formaximum stain removal.
Artificially stained bovine dental enamel blocks werepurchased from Therametric Technologies, Inc. (Indianapolis,IN, USA). The 10 mm2 blocks were mounted in a methacrylateresin so that only the enamel was exposed to the stain. Thestaining procedure closely followed that described by Stookey,et al. in that enamel blocks were cycled between air and astaining broth containing coffee, tea, mucin, soy broth, andSarcina Lutea, in a 37ºC incubator, until the L* value of thespecimen was between 25 and 40.11
The amount of stain on the teeth was quantified bymeasuring the light reflected off of the surface of the toothwith a spectrophotometer (Spectroshade Micro, MHTTechnologies, Milan, Italy). Measurements over the entirevisible color spectrum were obtained and reported as L*, a*,and b* values in the CIELab color scale.16 L* is the lightnessof color with L* = 100 representing diffuse white and L* = 0representing black. The second parameter, a*, represents thepositioning of the color between red and green. A positive a*value is red while a negative a* value is green. Likewise, b*is the position of a color between yellow and blue. A positiveb* value is yellow while a negative b* value is blue. Together,the L*, a*, and b* values make up the coordinate of a colorin CIELab space. L*, a*, and b* can be combined tocalculate a whitening index. One such whitening index is W*which is a representation of how far a given color is fromwhite light (L* = 100, a* = 0, b* = 0).1
W* = ((a*-0)2 + (b*-0)2 + (L* - 100)2)1/2
To take a measurement, the spectrophotometer waspositioned so that a single tooth was in the instrument’s field ofvision and then the image was captured. The images weretransferred to a computer for analysis, and software from MHTwas used to define the perimeter of the entire tooth and reportthe L*, a*, and b* values for this area. Before baseline stainmeasurements were conducted, the teeth were rinsed withdeionized water and air dried for 30 minutes. Reflectance datawere collected with the spectrophotometer three times for eachtooth and the average of these measurements was defined asthe baseline L*, a*, and b* values for each tooth which wereused to calculate the baseline W* value. Thirty-six teeth weresorted into three groups so that the distribution of averagebaseline W* values for each group was balanced. Each groupwas assigned to one of the test toothbrushes.
The brushing study was conducted using a V-8 mechanicalcross-brushing machine. Four sample holders on the machinewere each enlarged and extended to accommodate the handle ofthe sonic power toothbrush (Figure 1a). The remaining foursample holders were left in their original position to hold themanual flat-trim toothbrushes (Figure 1b). In order to minimizemechanical variations between test cycles, two teeth were treated
Vol. XXIII, Spec. Iss. AThe Journal of Clinical DentistryA22
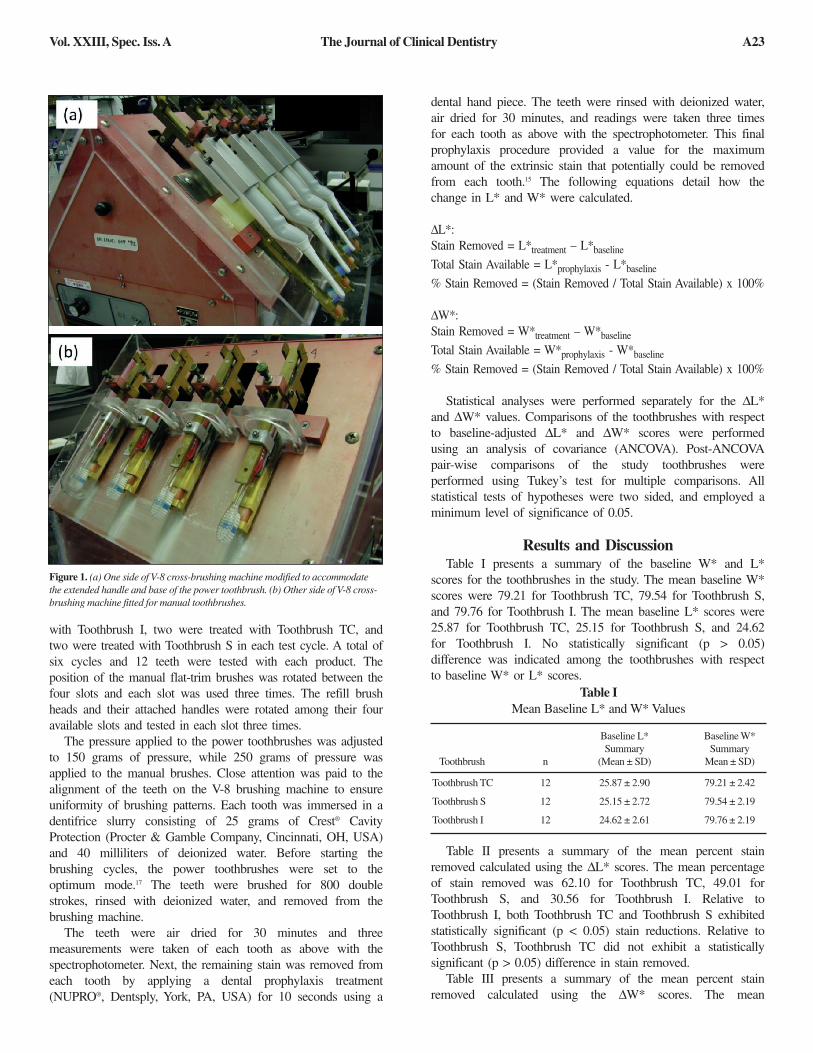
with Toothbrush I, two were treated with Toothbrush TC, andtwo were treated with Toothbrush S in each test cycle. A total ofsix cycles and 12 teeth were tested with each product. Theposition of the manual flat-trim brushes was rotated between thefour slots and each slot was used three times. The refill brushheads and their attached handles were rotated among their fouravailable slots and tested in each slot three times.
The pressure applied to the power toothbrushes was adjustedto 150 grams of pressure, while 250 grams of pressure wasapplied to the manual brushes. Close attention was paid to thealignment of the teeth on the V-8 brushing machine to ensureuniformity of brushing patterns. Each tooth was immersed in adentifrice slurry consisting of 25 grams of Crest® CavityProtection (Procter & Gamble Company, Cincinnati, OH, USA)and 40 milliliters of deionized water. Before starting thebrushing cycles, the power toothbrushes were set to theoptimum mode.17 The teeth were brushed for 800 doublestrokes, rinsed with deionized water, and removed from thebrushing machine.
The teeth were air dried for 30 minutes and threemeasurements were taken of each tooth as above with thespectrophotometer. Next, the remaining stain was removed fromeach tooth by applying a dental prophylaxis treatment(NUPRO®, Dentsply, York, PA, USA) for 10 seconds using a
dental hand piece. The teeth were rinsed with deionized water,air dried for 30 minutes, and readings were taken three timesfor each tooth as above with the spectrophotometer. This finalprophylaxis procedure provided a value for the maximumamount of the extrinsic stain that potentially could be removedfrom each tooth.15 The following equations detail how thechange in L* and W* were calculated.
∆L*:Stain Removed = L*treatment – L*baseline
Total Stain Available = L*prophylaxis - L*baseline
% Stain Removed = (Stain Removed / Total Stain Available) x 100%
∆W*:Stain Removed = W*treatment – W*baseline
Total Stain Available = W*prophylaxis - W*baseline
% Stain Removed = (Stain Removed / Total Stain Available) x 100%
Statistical analyses were performed separately for the ∆L*and ∆W* values. Comparisons of the toothbrushes with respectto baseline-adjusted ∆L* and ∆W* scores were performedusing an analysis of covariance (ANCOVA). Post-ANCOVApair-wise comparisons of the study toothbrushes wereperformed using Tukey’s test for multiple comparisons. Allstatistical tests of hypotheses were two sided, and employed aminimum level of significance of 0.05.
Results and DiscussionTable I presents a summary of the baseline W* and L*
scores for the toothbrushes in the study. The mean baseline W*scores were 79.21 for Toothbrush TC, 79.54 for Toothbrush S,and 79.76 for Toothbrush I. The mean baseline L* scores were25.87 for Toothbrush TC, 25.15 for Toothbrush S, and 24.62for Toothbrush I. No statistically significant (p > 0.05)difference was indicated among the toothbrushes with respectto baseline W* or L* scores.
Table II presents a summary of the mean percent stainremoved calculated using the ∆L* scores. The mean percentageof stain removed was 62.10 for Toothbrush TC, 49.01 forToothbrush S, and 30.56 for Toothbrush I. Relative toToothbrush I, both Toothbrush TC and Toothbrush S exhibitedstatistically significant (p < 0.05) stain reductions. Relative toToothbrush S, Toothbrush TC did not exhibit a statisticallysignificant (p > 0.05) difference in stain removed.
Table III presents a summary of the mean percent stainremoved calculated using the ∆W* scores. The mean
Table IMean Baseline L* and W* Values
Baseline L* Baseline W*Summary Summary
Toothbrush n (Mean ± SD) Mean ± SD)
Toothbrush TC 12 25.87 ± 2.90 79.21 ± 2.42
Toothbrush S 12 25.15 ± 2.72 79.54 ± 2.19
Toothbrush I 12 24.62 ± 2.61 79.76 ± 2.19
Figure 1. (a) One side of V-8 cross-brushing machine modified to accommodatethe extended handle and base of the power toothbrush. (b) Other side of V-8 cross-brushing machine fitted for manual toothbrushes.
Vol. XXIII, Spec. Iss. A The Journal of Clinical Dentistry A23

percentage of stain removed was 59.89 for Toothbrush TC,46.83 for Toothbrush S, and 29.25 for Toothbrush I. Relative toToothbrush I, both Toothbrush TC and Toothbrush S exhibitedstatistically significant (p < 0.05) stain reductions. Relative toToothbrush S, Toothbrush TC did not exhibit a statisticallysignificant (p > 0.05) difference in stain removed.
It is generally believed that a toothbrush can only scrubaway stain molecules and cannot alter the hue or chroma ofstains. In the literature, data are typically reported as changes inL* for in vitro stain removal studies,13,14 as a change in L* isthought to correlate with extrinsic stain removal. In the currentstudy, a whitening index, W*, is also reported as it iscalculated using all three descriptors of a color (L*, a*, andb*). In order to report that a color has actually become whiter,it is necessary to account for changes to all three coordinateswhich describe the color, even if there is no significant changein a* or b*. In this study, L* became lighter and W* becamewhiter after brushing with each toothbrush. In addition, thechange in L* and W* was greater for Toothbrush TC andToothbrush S than for Toothbrush I, indicating that the newsonic powered toothbrush, using either of the refill brush heads,was better than the manual flat-trim toothbrush in terms of theremoval of extrinsic stain as well as an increase in whiteness.
ConclusionA new specially engineered sonic powered toothbrush with
unique sensing and control technologies, with either the TripleClean refill brush head or the Sensitive refill brush head, wassignificantly more effective (p < 0.05) than a manual flat-trimtoothbrush at removing extrinsic stain in this laboratory study.This sonic powered toothbrush demonstrated a greaterpercentage of stain removed when the results were calculatedusing ∆L* and when results were calculated using thewhitening index, ∆W*. These results show that removing
extrinsic stain by brushing can be a meaningful way to increasethe whiteness of teeth. There were no significant differences inthe in vitro stain removal efficacy between the powertoothbrush with the Triple Clean refill brush head and thepower toothbrush with the Sensitive refill brush head.
Acknowledgement: These studies were sponsored by the Colgate-PalmoliveCompany, Piscataway, NJ, USA. The authors would like to thank JeffreyGraham and Gerald Gontarz for assistance with modifications to the V-8 cross-brushing machine.
For correspondence with the authors of this paper, contactVenda P. Maloney – [email protected]
References1. Joiner A, Hopkinson I, Deng Y, Westland S. A review of tooth colour and
whiteness. J Dent 2008;36S:S2-7.2. Joiner A. Whitening toothpastes: A review of the literature. J Dent
2010;38S:e17-24.3. Baig A, He T, Buisson J, Sagel L, Suszcynsky-Meister E, White DJ.
Extrinsic whitening effects of sodium hexametaphosphate – A review including a dentifrice with stabilized stannous fluoride. Compend Contin Educ Dent 2005;26(9 Suppl 1):47-53.
4. Lewis R, Dwyer-Joyce RS, Pickles MJ. Interaction between toothbrushes and toothpaste abrasive particles in simulated tooth cleaning. Wear2004;257:368-76.
5. Moran JM, Addy M, Newcombe RG. A comparative study of stain removal with two electric toothbrushes and a manual brush. J Clin Dent 1995;6:188-93.
6. Grossman E, Cronin M, Dembling W, Proskin H. A comparative clinical study of extrinsic tooth stain removal with two electric toothbrushes (Braun D7 and D9) and a manual brush. Am J Dent1996;9:S25-9.
7. Emling RC, Yankell S, Johnson B, McInnes C. Clinical stain removal properties of a new sonic toothbrush. J Dent Res 1994;73:434.
8. Karpinia K, Magnusson I, Biesbrock AR, Walters PA, Bartizek RD. The effectiveness of two different battery-powered toothbrushes on whitening through removal of stain. J Clin Dent 2002;13:215-8.
9. Terezhalmy G, Stookey GK, Mason S, Bartizek RD, Biesbrock AR. Tooth
Table IIPercentage Stain Removed with Each Toothbrush as Calculated Using the ∆L* Value
Treatment n % Stain Removed Summary Percent Sig Percent Sig(Mean ± SD) Difference Difference
Toothbrush TC 12 62.10 ± 10.83 26.7% NS 103.2% p < 0.05
Toothbrush S 12 49.01 ± 12.33 — — 60.4% p < 0.05
Toothbrush I 12 30.56 ± 24.18 — — — —
Between-Toothbrush Comparisonvs. Toothbrush S vs. Toothbrush I
Table IIIPercentage Stain Removed with Each Toothbrush as Calculated Using the ∆W* Value
Treatment n % Stain Removed Summary Percent Sig Percent Sig(Mean ± SD) Difference Difference
Toothbrush TC 12 59.89 ± 10.60 27.9% NS 104.8% p < 0.05
Toothbrush S 12 46.83 ± 12.00 — — 60.1% p < 0.05
Toothbrush I 12 29.25 ± 23.72 — — — —
Between-Toothbrush Comparisonvs. Toothbrush S vs. Toothbrush I
Vol. XXIII, Spec. Iss. AThe Journal of Clinical DentistryA24

whitening through the removal of extrinsic stain with a power toothbrush:Results of four randomized, examiner blind, positive controlled clinical studies. Am J Dent 2004;17:18A-24.
10. Garcia-Godoy F, Ellacuria J. Effectiveness of Sonicare power toothbrush to remove chlorhexidine stains. Am J Dent 2002;15:290-2.
11. Stookey GK, Burkhard TA, Schemehorn BR. In vitro removal of stain with dentifrices. J Dent Res 1982;61:1236-9.
12. McConnell D, Conroy CW. Comparisons of abrasion produced by a simulated manual versus a mechanical toothbrush. J Dent Res 1967;46:1022-7.
13. Schemehorn BR. The effect of an oscillating/rotating electric toothbrush and a sonic toothbrush on removal of stain from enamel surfaces. J Clin Dent 1995;6:194-7.
14. Hunt SA, Bartizek RD. Relative extrinsic stain removal effectiveness of a new battery-powered toothbrush and a flat trim manual toothbrush. Am J Dent 2004;17:13A-7.
15. Kleber CJ, Kemp JH, Moore MH, Mintel TE. Laboratory Investigation of Colgate 360 Toothbrush and Oral-B Indicator Toothbrush for the removal of dental stains. Compend Contin Educ Dent 2004;25:46-50.
16. Commission Internationale de L’Eclairage “CIE.” Recommendations on uniform color spaces. Color difference equations. Psychometric color terms. Suppl 2 to CIE publication 15 (E-13.1) 1971/(TC-1.3),1978, Paris: Bureau Central de la “CIE,” 1978.
17. Gatzemeyer J, Panagakos F. Intelligent technology for superior cleaning of teeth and gums. J Clin Dent 2012;23(Spec Iss A):A1-4.
Vol. XXIII, Spec. Iss. A The Journal of Clinical Dentistry A25

Ergonomic Audit of a Specially Engineered Sonic Powered Toothbrush with Unique Sensing and Control Technologies,the Sonicare FlexCare, and the Oral-B Smart Series 5000
Gail Hunter, Laurie Burns, Brian Bone
Metaphase Design Group, Inc.St. Louis, MO, USA
Thomas Mintel, Eduardo Jimenez
Colgate-Palmolive Technology CenterPiscataway, NJ, USA
Abstract• Objective: The presence of ergonomic features can impact the marketplace success of a new product. Metaphase Design Group, Inc.,
in partnership with the Colgate-Palmolive Company, conducted an ergonomic audit on three electric toothbrushes: a specially engineered sonic powered toothbrush with unique sensing and control technologies, the Sonicare™ FlexCare, and the Oral-B® Smart Series 5000.
• Methods: The ergonomic audit was conducted by Metaphase Design Groups’s ergonomic and usability experts. Two experts used the toothbrushes over a one-week period and assessed the performance of each brush against a set of ergonomic principles.
• Results: The three toothbrushes have some solid ergonomic features. They each have adequate grip zones, provide grip security with elastomeric materials, and provide easy access to the on/off button. The most distinctive feature is the longitudinal shape of the handle of the specially engineered sonic powered toothbrush with unique sensing and control technologies. This handle angles downward at the top end and provides additional advantages through improved grip security and visibility. Yet all three toothbrushes have different opportunities for improvement. The Sonicare Flex Care toothbrush has a cluttered and complicated user interface that is difficult to read. The disadvantages of the Oral-B Smart Series 5000 toothbrush are related to its physical dimensions and audible feedback.
• Conclusion: The specially engineered sonic powered toothbrush with unique sensing and control technologies is surprising to use with its changes in speeds, brush movements, and resulting changes in audible feedback.
(J Clin Dent 2012;23[Spec Iss A]:A26-A30)
IntroductionErgonomics is the application of what is known about
human capabilities and limitations (both physically andcognitively) to the design of products in order to facilitate amore efficient, safe, and satisfactory use. Ergonomic evaluationsfocus on design features that are not obvious to the end user,yet add significant benefits to the design of a toothbrush.
When evaluating ergonomics, a product is examined todetermine if it meets ergonomic principles. If the productviolates these principles it then compromises its usability.
When assessing the ergonomic factors, the evaluationsexamine both the presence of these ergonomic features as wellas the perception of ergonomic features. The perception ofergonomics is important at point-of-purchase where consumersare not able to physically handle the product, but are searchingfor products that appear to be easy and comfortable to use.Often, perceived ergonomics results from the use of soft touchmaterial, generous radii on the form, uncluttered interfaces,minimal buttons, etc.
Prior to conducting an ergonomic audit, it is critical todefine the target user population as well as understand theusage environment. For electric toothbrushes, it is assumed thetarget population is male and female adults aged 35–50 years,
and the product will be used in a possibly wet, bathroomenvironment.
This article discusses the results from an ergonomic audit ofthree electric toothbrushes: a specially engineered sonicpowered toothbrush with unique sensing and controltechnologies, the Sonicare FlexCare, and the Oral-B SmartSeries 5000.
Materials and MethodsTwo ergonomic experts from Metaphase Design Group used
the test toothbrushes for approximately one week, and assessedthe performance against a standard set of ergonomic principlesthat are familiar to the experts based on their experience in thefield. These experts had each toothbrush’s instructional manualto use during the trials. There was no pre-determined order inwhich the experts used the toothbrushes.
The ergonomic principles considered in this audit were asfollows:
• The product is intuitive to use; that is, the product operation needs to be designed to match how users typically think, how users typically process information, as well as users’ previous experience with products.1
• The physical design of the device (e.g., size, form,
A26
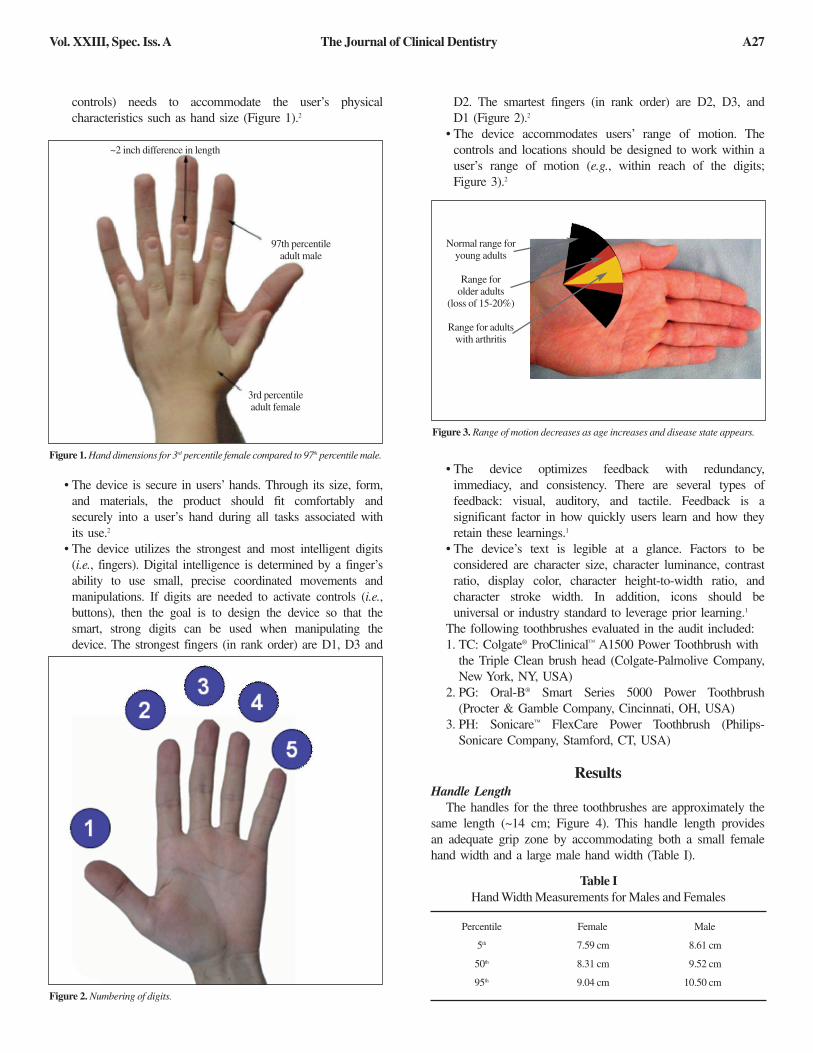
controls) needs to accommodate the user’s physical characteristics such as hand size (Figure 1).2
• The device is secure in users’ hands. Through its size, form,and materials, the product should fit comfortably and securely into a user’s hand during all tasks associated with its use.2
• The device utilizes the strongest and most intelligent digits (i.e., fingers). Digital intelligence is determined by a finger’s ability to use small, precise coordinated movements and manipulations. If digits are needed to activate controls (i.e.,buttons), then the goal is to design the device so that the smart, strong digits can be used when manipulating the device. The strongest fingers (in rank order) are D1, D3 and
D2. The smartest fingers (in rank order) are D2, D3, and D1 (Figure 2).2
• The device accommodates users’ range of motion. The controls and locations should be designed to work within a user’s range of motion (e.g., within reach of the digits; Figure 3).2
• The device optimizes feedback with redundancy,immediacy, and consistency. There are several types of feedback: visual, auditory, and tactile. Feedback is a significant factor in how quickly users learn and how they retain these learnings.1
• The device’s text is legible at a glance. Factors to be considered are character size, character luminance, contrast ratio, display color, character height-to-width ratio, and character stroke width. In addition, icons should be universal or industry standard to leverage prior learning.1
The following toothbrushes evaluated in the audit included:1. TC: Colgate® ProClinical™ A1500 Power Toothbrush with
the Triple Clean brush head (Colgate-Palmolive Company,New York, NY, USA)
2. PG: Oral-B® Smart Series 5000 Power Toothbrush (Procter & Gamble Company, Cincinnati, OH, USA)
3. PH: Sonicare™ FlexCare Power Toothbrush (Philips-Sonicare Company, Stamford, CT, USA)
ResultsHandle Length
The handles for the three toothbrushes are approximately thesame length (~14 cm; Figure 4). This handle length providesan adequate grip zone by accommodating both a small femalehand width and a large male hand width (Table I).
Table IHand Width Measurements for Males and Females
Percentile
5th
50th
95th
Female
7.59 cm
8.31 cm
9.04 cm
Male
8.61 cm
9.52 cm
10.50 cm
Figure 1. Hand dimensions for 3rd percentile female compared to 97th percentile male.
Figure 3. Range of motion decreases as age increases and disease state appears.
Figure 2. Numbering of digits.
~2 inch difference in length
97th percentileadult male
Normal range foryoung adults
Range for older adults
(loss of 15-20%)
Range for adultswith arthritis
3rd percentileadult female
Vol. XXIII, Spec. Iss. A The Journal of Clinical Dentistry A27

Handle CircumferenceThe cross-sectional size and shape are the biggest
differences between the three toothbrushes with regard to theirform (Figure 5). Toothbrush TC has a cylindrical-shaped handleand the narrowest handle, making it easy to rotate andmanipulate in the fingers. Toothbrush PH also has a narrow,cylindrical-shaped handle making it easy to rotate andmanipulate in the fingers. Toothbrush PG has the largest handlecircumference and it is more rectangular-shaped compared tothe other two handles. This size and shape make the handle ontoothbrush PG feel bulky in the hand and more difficult tograsp, rotate, and manipulate with the fingers than ToothbrushesTC and PH.
Elastomeric MaterialsPresence. Grip security is an important feature on a device
that is used in wet, bathroom environments. All three brusheshave elastomeric materials applied to the back side of thehandles (Figure 6) that provide grip security. These materialsalso offer a perception of grip security and comfort at firstglance.
Texture. The elastomeric material on Toothbrush PG hasrough (tight radii) texture that detracts from the perception ofcomfort. The elastomeric material on Toothbrush PH has subtletexture, while the elastomeric material on Toothbrush TC doesnot have any texture (Figure 7). In addition, the presence oftexture does not necessarily increase the grip security providedby the elastomeric materials (the elastomeric material itself is agood source of grip security). Angle
The longitudinal shape of the handle of Toothbrush TC isdistinct from the other two handles. It angles downward at the
Figure 4. Handle length for the three toothbrushes.
Figure 6. Elastomeric materials applied to each toothbrush.
Figure 7. The elastomeric material applied has various types of texture.
Figure 8. Shape of toothbrush handles and brush heads.
Toothbrush TC Toothbrush PG Toothbrush PH
Handle Cross-section Width (mm) TC PG PH
bottom 24 33 28
mid 27 27 25
top 27 27 27
Handle Cross-section Depth (mm)
bottom 26 39 30
mid 29 34 28
top 28 31 28
Width
Depth
Bottom Mid Top
Figure 5. Handle dimensions for each toothbrush.
Vol. XXIII, Spec. Iss. AThe Journal of Clinical DentistryA28
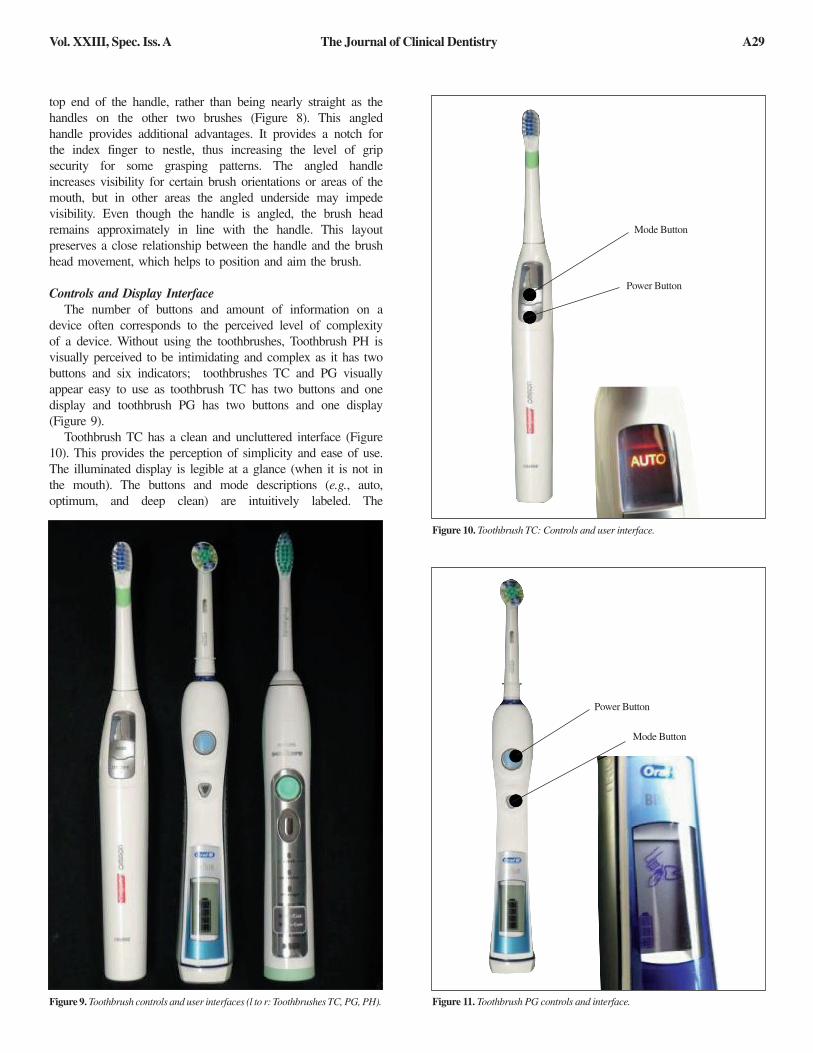
top end of the handle, rather than being nearly straight as thehandles on the other two brushes (Figure 8). This angledhandle provides additional advantages. It provides a notch forthe index finger to nestle, thus increasing the level of gripsecurity for some grasping patterns. The angled handleincreases visibility for certain brush orientations or areas of themouth, but in other areas the angled underside may impedevisibility. Even though the handle is angled, the brush headremains approximately in line with the handle. This layoutpreserves a close relationship between the handle and the brushhead movement, which helps to position and aim the brush.
Controls and Display InterfaceThe number of buttons and amount of information on a
device often corresponds to the perceived level of complexityof a device. Without using the toothbrushes, Toothbrush PH isvisually perceived to be intimidating and complex as it has twobuttons and six indicators; toothbrushes TC and PG visuallyappear easy to use as toothbrush TC has two buttons and onedisplay and toothbrush PG has two buttons and one display(Figure 9).
Toothbrush TC has a clean and uncluttered interface (Figure10). This provides the perception of simplicity and ease of use.The illuminated display is legible at a glance (when it is not inthe mouth). The buttons and mode descriptions (e.g., auto,optimum, and deep clean) are intuitively labeled. The
Figure 9. Toothbrush controls and user interfaces (l to r: Toothbrushes TC, PG, PH).
Power Button
Mode Button
Figure 11. Toothbrush PG controls and interface.
Figure 10. Toothbrush TC: Controls and user interface.
Mode Button
Power Button
Vol. XXIII, Spec. Iss. A The Journal of Clinical Dentistry A29
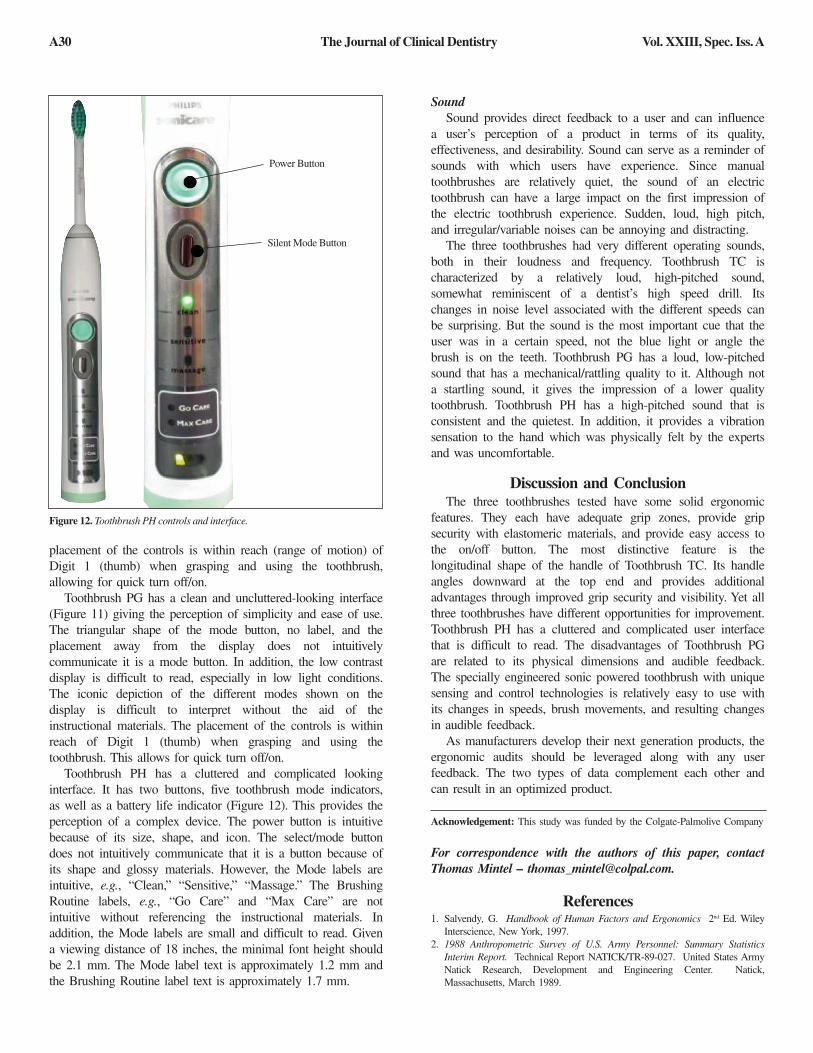
placement of the controls is within reach (range of motion) ofDigit 1 (thumb) when grasping and using the toothbrush,allowing for quick turn off/on.
Toothbrush PG has a clean and uncluttered-looking interface(Figure 11) giving the perception of simplicity and ease of use.The triangular shape of the mode button, no label, and theplacement away from the display does not intuitivelycommunicate it is a mode button. In addition, the low contrastdisplay is difficult to read, especially in low light conditions.The iconic depiction of the different modes shown on thedisplay is difficult to interpret without the aid of theinstructional materials. The placement of the controls is withinreach of Digit 1 (thumb) when grasping and using thetoothbrush. This allows for quick turn off/on.
Toothbrush PH has a cluttered and complicated lookinginterface. It has two buttons, five toothbrush mode indicators,as well as a battery life indicator (Figure 12). This provides theperception of a complex device. The power button is intuitivebecause of its size, shape, and icon. The select/mode buttondoes not intuitively communicate that it is a button because ofits shape and glossy materials. However, the Mode labels areintuitive, e.g., “Clean,” “Sensitive,” “Massage.” The BrushingRoutine labels, e.g., “Go Care” and “Max Care” are notintuitive without referencing the instructional materials. Inaddition, the Mode labels are small and difficult to read. Givena viewing distance of 18 inches, the minimal font height shouldbe 2.1 mm. The Mode label text is approximately 1.2 mm andthe Brushing Routine label text is approximately 1.7 mm.
Sound Sound provides direct feedback to a user and can influence
a user’s perception of a product in terms of its quality,effectiveness, and desirability. Sound can serve as a reminder ofsounds with which users have experience. Since manualtoothbrushes are relatively quiet, the sound of an electrictoothbrush can have a large impact on the first impression ofthe electric toothbrush experience. Sudden, loud, high pitch,and irregular/variable noises can be annoying and distracting.
The three toothbrushes had very different operating sounds,both in their loudness and frequency. Toothbrush TC ischaracterized by a relatively loud, high-pitched sound,somewhat reminiscent of a dentist’s high speed drill. Itschanges in noise level associated with the different speeds canbe surprising. But the sound is the most important cue that theuser was in a certain speed, not the blue light or angle thebrush is on the teeth. Toothbrush PG has a loud, low-pitchedsound that has a mechanical/rattling quality to it. Although nota startling sound, it gives the impression of a lower qualitytoothbrush. Toothbrush PH has a high-pitched sound that isconsistent and the quietest. In addition, it provides a vibrationsensation to the hand which was physically felt by the expertsand was uncomfortable.
Discussion and ConclusionThe three toothbrushes tested have some solid ergonomic
features. They each have adequate grip zones, provide gripsecurity with elastomeric materials, and provide easy access tothe on/off button. The most distinctive feature is thelongitudinal shape of the handle of Toothbrush TC. Its handleangles downward at the top end and provides additionaladvantages through improved grip security and visibility. Yet allthree toothbrushes have different opportunities for improvement.Toothbrush PH has a cluttered and complicated user interfacethat is difficult to read. The disadvantages of Toothbrush PGare related to its physical dimensions and audible feedback.The specially engineered sonic powered toothbrush with uniquesensing and control technologies is relatively easy to use withits changes in speeds, brush movements, and resulting changesin audible feedback.
As manufacturers develop their next generation products, theergonomic audits should be leveraged along with any userfeedback. The two types of data complement each other andcan result in an optimized product.
Acknowledgement: This study was funded by the Colgate-Palmolive Company
For correspondence with the authors of this paper, contactThomas Mintel – [email protected].
References1. Salvendy, G. Handbook of Human Factors and Ergonomics 2nd Ed. Wiley
Interscience, New York, 1997.2. 1988 Anthropometric Survey of U.S. Army Personnel: Summary Statistics
Interim Report. Technical Report NATICK/TR-89-027. United States Army Natick Research, Development and Engineering Center. Natick,Massachusetts, March 1989.
Figure 12. Toothbrush PH controls and interface.
Power Button
Silent Mode Button
Vol. XXIII, Spec. Iss. AThe Journal of Clinical DentistryA30

Usability Research Study of a Specially Engineered Sonic Powered Toothbrush with Unique Sensing and Control Technologies
Gail Hunter, Laurie Burns, Brian Bone
Metaphase Design Group, Inc.St. Louis, MO, USA
Thomas Mintel, Eduardo Jimenez
Colgate-Palmolive Technology CenterPiscataway, NJ, USA
Abstract• Objective: This paper summarizes the results of a longitudinal usability research study of a specially engineered sonic powered
toothbrush with unique sensing and control technologies. • Methods: The usability test was conducted with fourteen (14) consumers from the St. Louis, MO, USA area who use manual
toothbrushes. The study consisted of consumers using the specially engineered sonic powered toothbrush with unique sensing and control technologies for three weeks. During the study, users participated in four toothbrush trials during weekly visits to the research facility. These trials were videotaped and were analyzed regarding brushing time, behavior, and technique. In addition, the users were required to use the toothbrush twice a day for their at-home brushing.
• Results: The toothbrush had a positive impact on consumers’ tooth brushing behavior. Users spent more time brushing their teeth with this toothbrush as compared to their manual toothbrush. In addition, users spent more time keeping the sonic toothbrush in the recommended angle during use. Finally, users perceived their teeth to be cleaner when using the specially engineered sonic powered toothbrush with unique sensing and control technologies.
• Conclusion: The specially engineered sonic powered toothbrush with unique sensing and control technologies left a positive impression on the users. The users perceived the toothbrush to clean their teeth better than a manual toothbrush.
(J Clin Dent 2012;23[Spec Iss A]:A31-A34)
IntroductionUsability studies provide insight into how potential
customers will interact with a new product. This article presentsthe results from a usability study of a specially engineeredsonic powered toothbrush with unique sensing and controltechnologies from the Colgate-Palmolive Company. Thepurpose of the study was to understand how tooth brushingbehavior changed over the course of the study; specifically:
• Change in brushing time when using a manual toothbrush to using an electric toothbrush;
• Change in brushing technique when using a manual toothbrush as compared to using an electric toothbrush; and
• Change in time spent in a 45° angle over the course of the study.
Materials and MethodsFourteen (14) adult male and female subjects from the St.
Louis, Missouri, USA area were enrolled into the study fromApril 16 through May 10, 2012 based upon the following criteria:
• 50% female and 50% male between the ages of 35 and 50;
• No dental work such as braces, dentures, removable bridge, caps, etc.;
• Brush two to three times a day;• Use a manual toothbrush;• Interested in using a plug-in rechargeable toothbrush (a
score of 7-10 on a 10-point scale where 1 was “Not at all interested” and 10 was “Extremely interested”);
• Household income of at least $55,000;• Completed at least two years of college; and• Represented a distribution of glove/hand sizes.Subjects were provided with a specially engineered sonic
powered toothbrush with unique sensing and controltechnologies and the Triple Clean refill brush head (“TC” – Colgate® ProClinical™ A1500 Power Toothbrush,Colgate-Palmolive Company, New York, NY, USA). This model has an Auto Mode feature, and the users were asked tokeep it in this mode. Auto Mode has three speeds withcorresponding brush actions. The angle of the brush headagainst the teeth changes the speed of the brush head.
• Low speed occurs when cleaning vertical surfaces. The brush head automatically moves side-to-side.
A31

• Mid speed occurs when the brush head is positioned approximately 45° to the gum line. The brush head automatically pivots from side-to-side and up and down.
• High speed occurs when cleaning horizontal chewing areas. The brush head automatically moves up and down.
ProtocolBefore their initial visit to the test site, subjects were
provided with a video camera to videotape themselves at homebrushing their teeth with their manual toothbrush, which servedas a baseline for the study.
During the initial visit to the test site (Trial 1), each subjectwas given their assigned toothbrush for use during the study.
• The instructional materials were reviewed with the respondent before being videotaped using toothbrush TC.
• All users were instructed to keep toothbrush TC in the Auto Mode during the study.
• A “fin” was attached to the bottom of toothbrush TC prior to brushing to facilitate analysis of which angle the toothbrush was in.
• After use, the users completed a brief questionnaire and participated in an interview.
Subjects were asked to complete a journal when they usedtoothbrush TC at home. No restrictions were placed on the useof toothpaste. The journal asked them to record the length oftime they used the toothbrush and any comments regardingtheir experience. The journals were returned and reviewed ateach visit.
All users returned to the test site after an additional week ofbrushing with toothbrush TC at home and were videotaped atthe test site brushing their teeth with toothbrush TC (Trial 2).After brushing, they completed a brief questionnaire.
At week 4 (Trial 4), the users again were videotaped usingtoothbrush TC, completed a questionnaire, and were asked aseries of questions about their experience.
Finally, eight users were asked to brush again with a manualtoothbrush (Colgate® 360° Toothbrush, Colgate-PalmoliveCompany, New York, NY, USA) and describe the differencesthey experienced between manual and electric toothbrushes.
ResultsBrushing Time
Users increased their brushing time using toothbrush TC.During review of the at-home videotapes, it was determinedthat the average time users spent brushing their teeth at homewith their manual brush was 54 seconds. The average timeusers spent using toothbrush TC ranged from an average of 99to 107 seconds during Trials 1, 2, and 4 (Figure 1).
Brushing TechniqueThe users were videotaped during each trial. Analyses of the
videotapes were conducted following the study. Times wererecorded from the videotapes and observations were noted. Inaddition, the facilitators took handwritten notes during theinterviews with the users.
After Trial 1, users had begun to allow toothbrush TC to dothe work and spent a longer period of time in each quadrant(Figure 2). Users were observed gliding the brush head overtheir teeth with either a slight back and forth motion or a small
circular motion. Many users commented that it took severaldays for them to change their behavior and let the toothbrushdo the work versus having themselves do the work. As a result,users stayed in the various quadrants longer than they did when using a manual toothbrush. However, some users wereobserved going back to manual brushing behavior (faster,medium strokes) when in the low speed to augment thecleaning of toothbrush TC.
Brushing AnglesThe Auto Mode feature on toothbrush TC has three speeds
with corresponding brush actions. The angle of the brush headagainst the teeth changes the speed of the brush head. Usersincreased their time with the brush head at a 45° angle (therecommended angle1) over the course of the study (Figure 3).
The users commented during the trials that they were ableto detect differences in the speed of the brush because of theaudible and tactile feedback from toothbrush TC. Few userspaid attention to the blue light that turned on when toothbrushTC was at a 45° angle. Many users stated that they preferred
Figure 1. Time spent brushing teeth at home with their manual brush and atTrials 1, 2, and 4 with toothbrush TC.
Figure 2. Average amount of time users spent in one quadrant beforeswitching to a different quadrant. Less time indicates quick movements aroundthe mouth, while more time indicates keeping the brush in place.
A32 The Journal of Clinical Dentistry Vol. XXIII, Spec. Iss. A
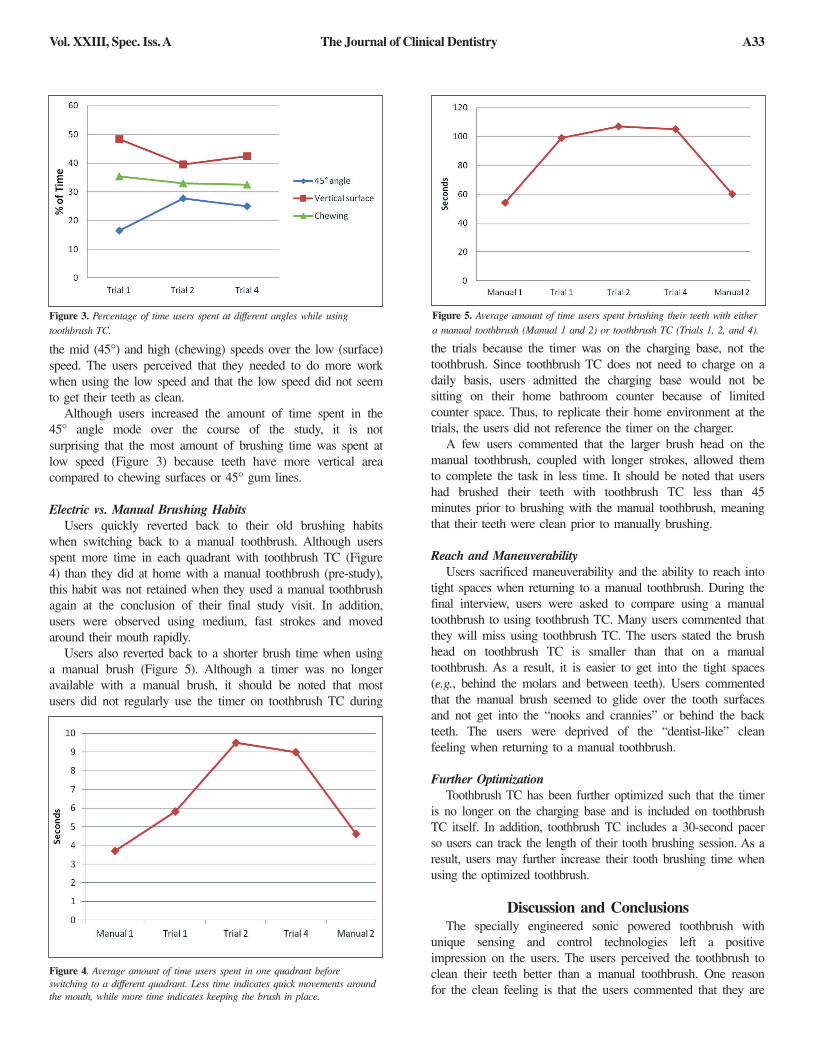
the mid (45°) and high (chewing) speeds over the low (surface)speed. The users perceived that they needed to do more workwhen using the low speed and that the low speed did not seemto get their teeth as clean.
Although users increased the amount of time spent in the45° angle mode over the course of the study, it is notsurprising that the most amount of brushing time was spent atlow speed (Figure 3) because teeth have more vertical areacompared to chewing surfaces or 45° gum lines.
Electric vs. Manual Brushing HabitsUsers quickly reverted back to their old brushing habits
when switching back to a manual toothbrush. Although usersspent more time in each quadrant with toothbrush TC (Figure4) than they did at home with a manual toothbrush (pre-study),this habit was not retained when they used a manual toothbrushagain at the conclusion of their final study visit. In addition,users were observed using medium, fast strokes and movedaround their mouth rapidly.
Users also reverted back to a shorter brush time when usinga manual brush (Figure 5). Although a timer was no longeravailable with a manual brush, it should be noted that mostusers did not regularly use the timer on toothbrush TC during
the trials because the timer was on the charging base, not thetoothbrush. Since toothbrush TC does not need to charge on adaily basis, users admitted the charging base would not besitting on their home bathroom counter because of limitedcounter space. Thus, to replicate their home environment at thetrials, the users did not reference the timer on the charger.
A few users commented that the larger brush head on themanual toothbrush, coupled with longer strokes, allowed themto complete the task in less time. It should be noted that usershad brushed their teeth with toothbrush TC less than 45minutes prior to brushing with the manual toothbrush, meaningthat their teeth were clean prior to manually brushing.
Reach and ManeuverabilityUsers sacrificed maneuverability and the ability to reach into
tight spaces when returning to a manual toothbrush. During thefinal interview, users were asked to compare using a manualtoothbrush to using toothbrush TC. Many users commented thatthey will miss using toothbrush TC. The users stated the brushhead on toothbrush TC is smaller than that on a manualtoothbrush. As a result, it is easier to get into the tight spaces(e.g., behind the molars and between teeth). Users commentedthat the manual brush seemed to glide over the tooth surfacesand not get into the “nooks and crannies” or behind the backteeth. The users were deprived of the “dentist-like” cleanfeeling when returning to a manual toothbrush.
Further OptimizationToothbrush TC has been further optimized such that the timer
is no longer on the charging base and is included on toothbrushTC itself. In addition, toothbrush TC includes a 30-second pacerso users can track the length of their tooth brushing session. As aresult, users may further increase their tooth brushing time whenusing the optimized toothbrush.
Discussion and ConclusionsThe specially engineered sonic powered toothbrush with
unique sensing and control technologies left a positiveimpression on the users. The users perceived the toothbrush toclean their teeth better than a manual toothbrush. One reasonfor the clean feeling is that the users commented that they are
Figure 3. Percentage of time users spent at different angles while usingtoothbrush TC.
Figure 5. Average amount of time users spent brushing their teeth with eithera manual toothbrush (Manual 1 and 2) or toothbrush TC (Trials 1, 2, and 4).
Figure 4. Average amount of time users spent in one quadrant beforeswitching to a different quadrant. Less time indicates quick movements aroundthe mouth, while more time indicates keeping the brush in place.
A33The Journal of Clinical DentistryVol. XXIII, Spec. Iss. A

able to maneuver the toothbrush in their mouth easier andreach more places. The improved maneuverability and reachare a result of the smaller brush head.
The brush also changed the behavior of the users in apositive way. They spent more time brushing their teeth, moretime on individual sections of the teeth, and spent more time ina 45° angle (the recommended angle).
Acknowledgement: This study was funded by the Colgate-Palmolive Company
For correspondence with the authors of this paper, contactThomas Mintel – [email protected].
Reference1. http://www.ada.org/sections/publicResources/pdfs/teeth_materials_brush.pdf.
A34 The Journal of Clinical Dentistry Vol. XXIII, Spec. Iss. A
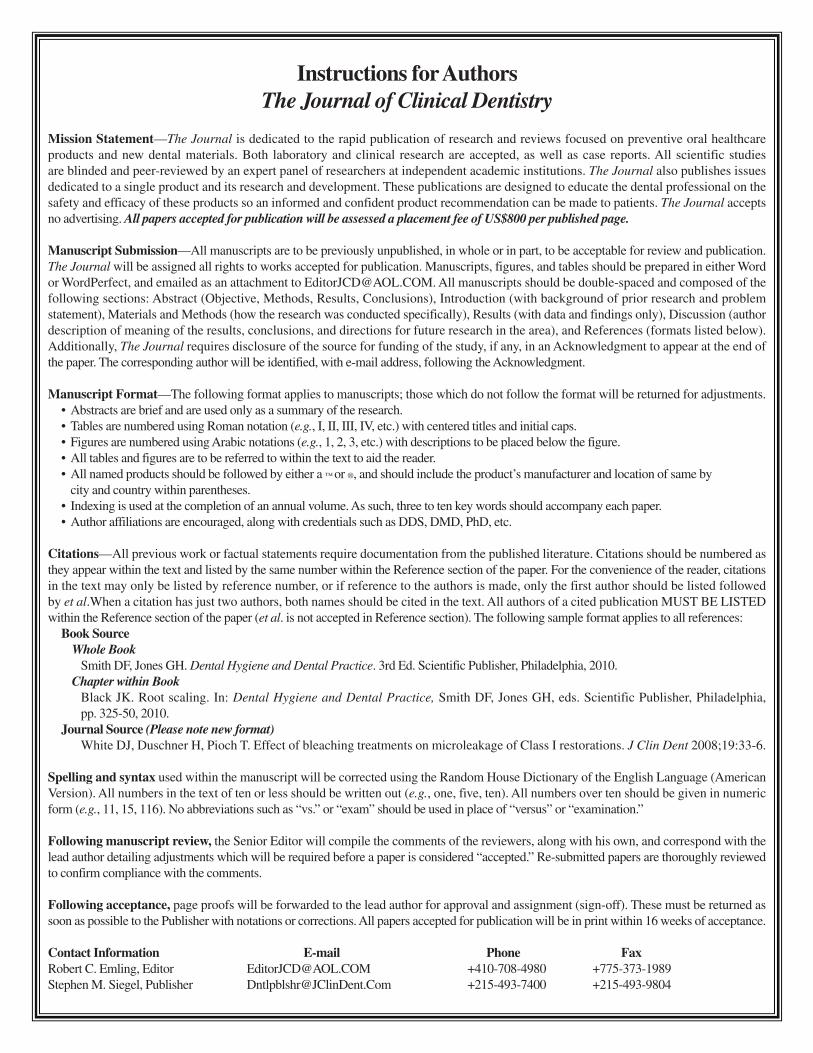
Instructions forAuthorsThe Journal of Clinical Dentistry
Mission Statement—The Journal is dedicated to the rapid publication of research and reviews focused on preventive oral healthcareproducts and new dental materials. Both laboratory and clinical research are accepted, as well as case reports. All scientific studiesare blinded and peer-reviewed by an expert panel of researchers at independent academic institutions. The Journal also publishes issuesdedicated to a single product and its research and development. These publications are designed to educate the dental professional on thesafety and efficacy of these products so an informed and confident product recommendation can be made to patients. The Journal acceptsno advertising. All papers accepted for publication will be assessed a placement fee of US$800 per published page.
Manuscript Submission—All manuscripts are to be previously unpublished, in whole or in part, to be acceptable for review and publication.The Journal will be assigned all rights to works accepted for publication. Manuscripts, figures, and tables should be prepared in either Wordor WordPerfect, and emailed as an attachment to [email protected]. All manuscripts should be double-spaced and composed of thefollowing sections: Abstract (Objective, Methods, Results, Conclusions), Introduction (with background of prior research and problemstatement), Materials and Methods (how the research was conducted specifically), Results (with data and findings only), Discussion (authordescription of meaning of the results, conclusions, and directions for future research in the area), and References (formats listed below).Additionally, The Journal requires disclosure of the source for funding of the study, if any, in an Acknowledgment to appear at the end ofthe paper. The corresponding author will be identified, with e-mail address, following the Acknowledgment.
Manuscript Format—The following format applies to manuscripts; those which do not follow the format will be returned for adjustments.• Abstracts are brief and are used only as a summary of the research.• Tables are numbered using Roman notation (e.g., I, II, III, IV, etc.) with centered titles and initial caps.• Figures are numbered using Arabic notations (e.g., 1, 2, 3, etc.) with descriptions to be placed below the figure.• All tables and figures are to be referred to within the text to aid the reader.• All named products should be followed by either a ™ or ®, and should include the product’s manufacturer and location of same by
city and country within parentheses.• Indexing is used at the completion of an annual volume. As such, three to ten key words should accompany each paper.• Author affiliations are encouraged, along with credentials such as DDS, DMD, PhD, etc.
Citations—All previous work or factual statements require documentation from the published literature. Citations should be numbered asthey appear within the text and listed by the same number within the Reference section of the paper. For the convenience of the reader, citationsin the text may only be listed by reference number, or if reference to the authors is made, only the first author should be listed followedby et al.When a citation has just two authors, both names should be cited in the text. All authors of a cited publication MUST BE LISTEDwithin the Reference section of the paper (et al. is not accepted in Reference section). The following sample format applies to all references:
Book SourceWhole Book
Smith DF, Jones GH. Dental Hygiene and Dental Practice. 3rd Ed. Scientific Publisher, Philadelphia, 2010.Chapter within Book
Black JK. Root scaling. In: Dental Hygiene and Dental Practice, Smith DF, Jones GH, eds. Scientific Publisher, Philadelphia,pp. 325-50, 2010.
Journal Source (Please note new format)White DJ, Duschner H, Pioch T. Effect of bleaching treatments on microleakage of Class I restorations. J Clin Dent 2008;19:33-6.
Spelling and syntax used within the manuscript will be corrected using the Random House Dictionary of the English Language (AmericanVersion). All numbers in the text of ten or less should be written out (e.g., one, five, ten). All numbers over ten should be given in numericform (e.g., 11, 15, 116). No abbreviations such as “vs.” or “exam” should be used in place of “versus” or “examination.”
Following manuscript review, the Senior Editor will compile the comments of the reviewers, along with his own, and correspond with thelead author detailing adjustments which will be required before a paper is considered “accepted.” Re-submitted papers are thoroughly reviewedto confirm compliance with the comments.
Following acceptance, page proofs will be forwarded to the lead author for approval and assignment (sign-off). These must be returned assoon as possible to the Publisher with notations or corrections. All papers accepted for publication will be in print within 16 weeks of acceptance.
Contact Information E-mail Phone FaxRobert C. Emling, Editor [email protected] +410-708-4980 +775-373-1989Stephen M. Siegel, Publisher [email protected] +215-493-7400 +215-493-9804
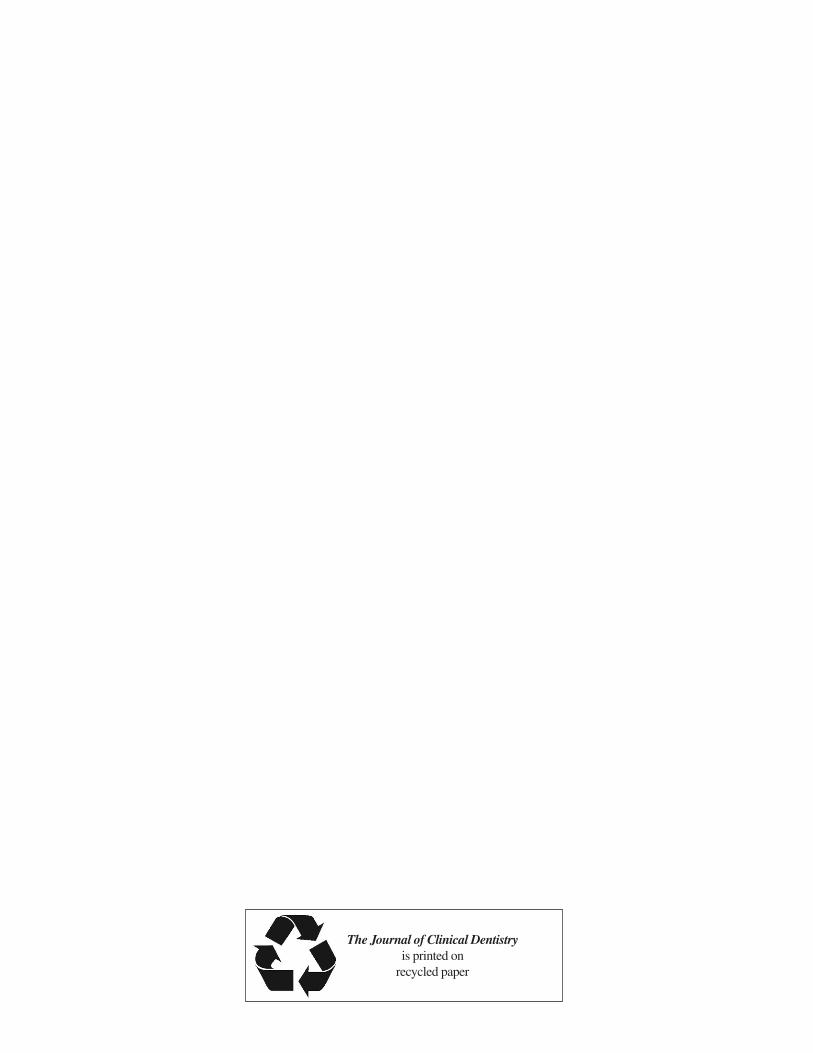
The Journal of Clinical Dentistryis printed on
recycled paper