Journal Club By Ben Selph, Mercer COPHS April 6, 2012 SEGA Geriatrics.
19
Journal Club By Ben Selph, Mercer COPHS April 6, 2012 SEGA Geriatrics
-
Upload
sherman-lester -
Category
Documents
-
view
216 -
download
2
Transcript of Journal Club By Ben Selph, Mercer COPHS April 6, 2012 SEGA Geriatrics.

Journal ClubBy Ben Selph, Mercer COPHS
April 6, 2012SEGA Geriatrics

Each year more than 1.2 million people will experience an ACS event (unstable angina, heart attack). 220,000 will die of a heart attack (myocardial
infarction-MI). Optimum treatment for a heart attack
depends on timely recognition of symptoms and treatment of the event. Goals—for fibrinolytic treatment (medication
to bust clot): within 30 minutes For stint placement (PCI): within 90 minutes.
Hallmark symptom of a heart attack: CHEST PAIN/DISCOMFORT.
However, a large number of patients with MI do not present with chest pain. These patients tend to present later, are
treated less aggressively, and have almost twice the short-term mortality compared with those with typical symptoms.
Younger women with MI may have higher mortality risk than men; lack of CP may contribute.
Women are generally older than men at hospitalization for MI. May be related to whether they present with CP But studies measuring sex differences in
presentation are limited in number. Goal: answer question of whether lack of
chest pain was associated with higher mortality observed in younger women with MI.
Purpose and objectives: examine relationship among patients hospitalized with MI between sex and symptom presentation (primary) and sex, symptom presentation, and hospital mortality rate (secondary) after accounting for age.
Restrospective observational study Patient population: NRMI patient population
of 2,160,671 patients admitted with confirmed MI at 1977 participating hospitals from 1994-2006.
Diagnosis of acute MI: clinical presentation consistent with acute MI, determined by HC providers at each hospital. Diagnostic code 410.X1 or supporting evidence
(elevated cardiac biomarker level, electrocardiographic evidence, or other enzymatic, nuclear, or autopsy evidence of acute MI).
Excluded patients: transferred patients, patients with missing info on sex, age, or symptomatic presentation, and patients with secondary diagnosis of MI.
Study variables: only symptom recorded in study was presence/absence of chest pain/discomfort Any symptom of chest discomfort, sensation, pressure,
or tightness; or arm, neck, or jaw pain occurring before hospital arrival or preceding diagnosis of acute MI
Classified as present or absent before admission, during admission, or both; may have included SOB, N/V, palpitations, syncope, or cardiac arrest
Statistical methods Chi square—differences between categorical
variables of study groups Compares percentages on outcomes between 2 or
more groups (nominal data); used for frequencies T test—differences between continuous variables
of study groups Compares data values that are continuous between 2
groups. Wilcoxan rank sum test—differences between
median values (ordinal data) of study groups Compares values of two groups where data is ordinal
P value < 0.001 was considered significant
Statistical analyses Multivariable adjusted regression and logistic
regression models—used to assess factors associated with MI presentation w/o CP in different age groups and sex differences in hospital mortality in the different age groups.
Odds ratio—calculated to determine odds of MI presentation w/o CP in different age groups for women compared with men.
Primary objective—relationship between sex and symptom presentation Secondary objective—relationship between sex,
symptom presentation, and hospital mortality

Study population: 1,143,513 patients Women with MI older than men at hospital
presentation (mean age 73.9 vs 66.5 years, p<0.001). Background baseline and presenting
characteristics MI with no chest pain: more likely to have diabetes,
have delayed hospital arrival, and present with Killip classification III and IV
No chest pain: more likely to present with NSTEMI; chest pain: more likely to present with STEMI
No chest pain: less likely to receive acute reperfusion therapy (fibrinolytic or PCI) and significantly less likely to receive therapy in timely manner
Primary objective: sex differences in symptom presentation Proportion of patients presenting with NO
chest pain significantly higher for women than men (42.0% vs 30.7%; 95% CI 41.8%-42.1% vs. 30.6%-30.8%; p < 0.001)
Age specific multivariable analyses showed signifcant interaction between sex and age Sex specific differences in MI presentation
without chest pain became progressively smaller with advancing age (next page).

Figure. JAMA Feb 22/29, 2012. 307;8: 818.

Table 5. JAMA Feb 22/29, 2012. 307;8: 818.

Table 6. JAMA Feb 22/29, 2012. 307;8: 818.
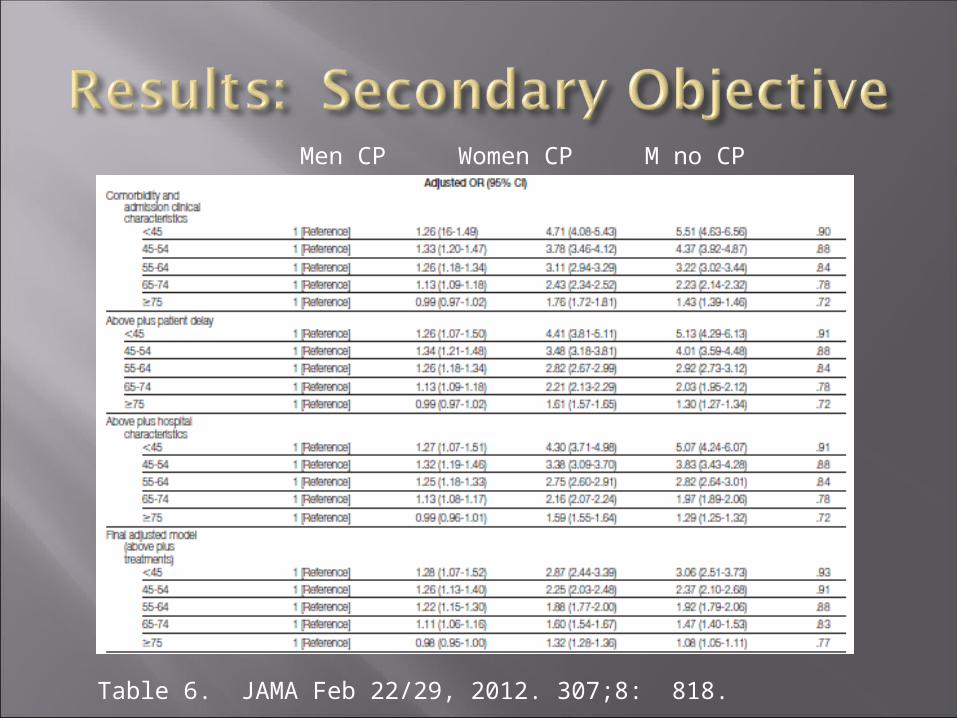
Table 6. JAMA Feb 22/29, 2012. 307;8: 818.
Men CP Women CP M no CP W no CP
What does the study show? Women with MI more likely than men to present
w/o chest pain Adjusted sex and age differences in presentation
w/o chest pain were greater in younger MI patients, and difference reduced with advancing age.
Results also suggest that absence of chest pain is associated with a higher mortality risk, especially in younger women with MI. All of which were statistically significant.
Age may actually be the more important factor in presentation w/o chest pain but needs to be confirmed in other studies.
Limitations NRMI patients and hospitals may not be
representative of all MI patients in U.S. Retrospective, observational study=results may be
limited by bias/confounders. Other MI symptoms in absence of chest pain was
not identified or noted in the data. No patients without MI to compare symptom
presentation and generalize results to all patients with suspected MI.
Symptom information obtained from medical record review, no standard (potential bias).
Also, updated version of MI definition and diagnosis in 2007 not used in this study (1994-2006).
Study results show women more likely than men to present without chest pain and also had higher mortality rates, especially in the younger age groups.
Sex differences in MI presentation and mortality decreased with increasing age.
Further research is needed to determine atypical symptom presentation in different ages and how these symptoms affect patients’ ability to get appropriate care.
Canto JG, Rogers WJ, Goldberg RJ, Peterson ED, Wenger NK, Vaccarino V, Kiefe CI, Frederick PD, Sopko G, and Zheng ZJ. Association of Age and Sex with Myocardial Infarction Symptom Presentation and In-Hospital Mortality. JAMA, Feb 22/29 2012. 307;8: 813-822.
Spinler SA, DENUS S. Chapter 24. Acute Coronary Syndromes. In: Talbert RL, DiPiro JT, Matzke GR, Posey LM, Wells BG, Yee GC, eds. Pharmacotherapy: A Pathophysiologic Approach. 8th ed. New York: McGraw-Hill; 2011. http://www.accesspharmacy.com/content.aspx?aID=7972196. Accessed April 3, 2012.