Joelle Glick, MD; Jason Kass, MD, PhD; Marita S. Teng, MD ...Joelle Glick, MD; Jason Kass, MD, PhD;...
1
Novel Application of Ostomy Paste for Closure of Complex Salivary Fistulas Joelle Glick, MD; Jason Kass, MD, PhD; Marita S. Teng, MD Department of Otolaryngology- Head & Neck Surgery, Mount Sinai Hospital, New York, NY Joelle Glick, MD Department of Otolaryngology- Head & Neck Surgery Mount Sinai Hospital Email:[email protected] Contact 1. Fleischmann W, Strecker W, Bombelli M, Kinzl L. Vacuum sealing as treatment of soft tissue damage in open fractures [in German]. Unfallchirurg 1993;96:488-492. 2. Thompson JT, Marks MW. Negative pressure wound therapy. Clin Plast Surg 2007;34(4):673-84. 3. Glass GE, Murphy GF, Esmaeili A, Lai LM, Nanchahal J. Systemic review of molecular mechanism of action of negative-pressure wound therapy. Br J Surg 2014;101(13):1627-36. 4. Timmons J, Russell F. The use of negative pressure wound therapy to manage enteroatmostpheric fistulae in two patients with large abdominal wounds. Int Wound J 2014;11(6):723-9. 5. Asher SA, White HN, Illing EA, Carroll WR, Magnuson JS, Rosenthal EL. Intraluminal negative pressure wound therapy for optimizing pharyngeal reconstruction. JAMA Otolaryngol Head Neck Surg 2013;140(2):143-149. 6. Asher SA, White HN, Golden JB, Magnuson JS, Carroll WR, Rosenthal EL. Negative pressure wound therapy in head and neck surgery. JAMA Facial Plast Surg 2014;16(2):120-126. 7. Dhir K, Reino AJ, Lipana J. Vacuum-assisted closure therapy in the management of head and neck wounds. Laryngoscope 2009;119:54-61. 8. Yang YH, Jeng SF, Hsieh CH, Feng GM, Chen CC. Vacuum-assisted closure for complicated wounds in the head and neck region after reconstruction. J Plast Reconstr Surg Aesthet Surg 2013;66:e209-e216. 9. Braakenburg A, Obdejn MC, Feitz R, van Rooij Ia, van Griethnysen AJ, Klinkenbijl JH. The clinical efficacy and cost effectiveness of the vaccum-assisted closure technique in the management of acute and chronic wounds: a randomized control trial. Plast Reconstr Surg 2006;118:390-397. References The end points for discontinuation of NPWT were the development of healthy granulation tissue and wound contracture in all cases. All wounds demonstrated adequate control of wound infection, rapid growth of granulation tissue, and contracture of the wound using the VAC system with ostomy paste. An adequate seal was maintained after the application of the VAC system and ostomy paste in all three patients. The airway did not need to be included in the negative pressure dressing in any patient. No adverse events occurred as a result of the VAC system or ostomy paste. There were no cases of pressure dressing application where the seal could not adequately be maintained with the additional use of ostomy paste. Three patients who had complicated wounds with either (1) salivary contamination or (2) a laryngectomy stoma that had previously failed conventional use of negative pressure wound therapy (NPWT) were included. Retrospective medical chart review was performed from September 2014 to March 2015 when the patients were treated. Application was performed at Mount Sinai Hospital and its affiliates in three patients. Data were collected including demographics, indications for NPWT, details of negative pressure dressing use, adverse events, wound healing results, potential risk factors for compromised wound healing, and wound characteristics. The InfoVAC (Kinetic Concepts, Inc, San Antonio, TX) wound VAC system was employed in all patients. Negative pressure was set at 125 mm Hg, in the continuous mode setting available with these devices. A standard polyurethane sponge was used in all cases. Stomadhesive (ostomy paste, ConvaTec Inc, Skillman, NJ) was used in all cases to reinforce the adhesive drape. In some cases, Tegederm transparent film dressings (3M, St Paul, Minnesota) were used on the surrounding skin prior to application of the wound VAC system. The VAC system was applied with the addition of ostomy paste around the wound to create a seal from the laryngectomy site or other salivary contamination (Fig. 1). Subsequent dressing changes were performed at a maximum of three days after application. Methods and Materials Postoperative fistulas in the head and neck region are common and related to multiple factors including: previous radiation exposure, malnutrition, and salivary contamination. Conventional wound management techniques that involve serial debridements, local/regional flaps, and free tissue transfers are burdensome for both the patient and healthcare providers. NPWT is an appealing and effective option in these patients as prolonged hospitalization due to postoperative fistula is associated with increased healthcare costs 9 . The use of NPWT to accelerate wound healing in the head and neck has previously been limited by the complex topography of the head and neck region as well as salivary contamination. Specifically, wounds with salivary contamination and those around a stoma are particularly challenging because an adequate seal cannot be maintained within the VAC system. In this study, we found that the addition of ostomy paste aided in our application of the VAC system to wounds contaminated with saliva. This method proved to be feasible and safe, and eliminated the need to use an artificial airway. Visualization of the overall wound was excellent using this technique because the stoma was not covered. Based on this preliminary data, we believe that the addition of stoma paste aids in the application of the wound VAC system around laryngectomy stomas, and provides an excellent addition to the otolaryngologist’s armamentarium for complex wound care. Larger prospective trials examining the use of stoma paste and VAC therapy in complex wounds of the head and neck will help support the data from this feasibility study. Discussion Until recently, the use of VAC system in the head and neck has been limited around stomas and in the presence of salivary contamination. We present a novel technique that is feasible, safe, and has potential to be a useful tool for complex wounds of the head and neck that involve either salivary contamination or peristomal application after laryngectomy. Conclusions The principles of local wound care have been utilized in the treatment of chronic wounds for over centuries. Negative pressure wound therapy (NPWT), first described by Fleischman et al in 1993, involves the application of suction, or negative pressure, to wounds that are healing 1 . NPWT has been shown to accelerate healing by promoting angiogenesis and granulation through improved local blood flow, reduction of chronic edema, and decreased wound bed bacterial counts. The benefits of this type of wound management include more rapid wound healing time and facilitation of wound care in situations that would otherwise be difficult or challenging 2,3 . While NPWT was used for many years in the treatment of chronic wounds, such as leg ulcers and bedsores, its use has now been modified for the use with surgical wounds 4 . Numerous applications have been reported throughout the body, however, there is little data on treatment of complex wounds in the head and neck region. Recent data, however, suggests that NPWT is safe and has the potential to be a useful tool for complex wounds of the head and neck 5,6,7,8 . The complex topography of wounds in the head and neck has previously precluded the use of the Vacuum Assisted Closure (VAC) system in this region. The most common challenge has been maintaining a seal around wounds that are in close proximity to a tracheostomy or laryngectomy stoma 7 . If the seal cannot be maintained, local wound care must be used instead of the VAC system. Peristomal application of the VAC system after laryngectomy by using an artificial airway has recently been described in thirty-two patients by Asher et al 6 . An artificial airway, fashioned from an endotracheal tube, is incorporated into the wound VAC system in these cases. At our institution, we have used this excellent technique for challenging wounds around stomas. However, we sought to modify this method by using stoma paste to facilitate an adequate seal, thereby avoiding the need for an artificial airway. Ostomy paste has conventionally been used to help maintain a seal with abdominal ostomies 4 . In the current study, we use ostomy paste in conjunction with the wound VAC system to maintain an adequate seal around laryngectomy stomas with salivary contamination. Results Figure 1. A, B, C: Patients before and after wound VAC and stoma paste application. D: Stoma paste Introduction STOMA STOMA SALIVARY LEAK SALIVARY LEAK STOMA PASTE STOMA PASTE WOUND VAC WOUND VAC A B C D STOMA SALIVARY LEAK STOMA PASTE WOUND VAC
Transcript of Joelle Glick, MD; Jason Kass, MD, PhD; Marita S. Teng, MD ...Joelle Glick, MD; Jason Kass, MD, PhD;...

Poster Print Size: This poster template is 44” high by 44” wide. It can be used to print any poster with a 1:1 aspect ratio.
Placeholders: The various elements included in this poster are ones we often see in medical, research, and scientific posters. Feel free to edit, move, add, and delete items, or change the layout to suit your needs. Always check with your conference organizer for specific requirements.
Image Quality: You can place digital photos or logo art in your poster file by selecting the Insert, Picture command, or by using standard copy & paste. For best results, all graphic elements should be at least 150-200 pixels per inch in their final printed size. For instance, a 1600 x 1200 pixel photo will usually look fine up to 8“-10” wide on your printed poster.
To preview the print quality of images, select a magnification of 100% when previewing your poster. This will give you a good idea of what it will look like in print. If you are laying out a large poster and using half-scale dimensions, be sure to preview your graphics at 200% to see them at their final printed size.
Please note that graphics from websites (such as the logo on your hospital's or university's home page) will only be 72dpi and not suitable for printing.
[This sidebar area does not print.]
Change Color Theme: This template is designed to use the built-in color themes in the newer versions of PowerPoint.
To change the color theme, select the Design tab, then select the Colors drop-down list.
The default color theme for this template is “Office”, so you can always return to that after trying some of the alternatives.
Printing Your Poster: Once your poster file is ready, visit www.genigraphics.com to order a high-quality, affordable poster print. Every order receives a free design review and we can deliver as fast as next business day within the US and Canada.
Genigraphics® has been producing output from PowerPoint® longer than anyone in the industry; dating back to when we helped Microsoft® design the PowerPoint® software.
US and Canada: 1-800-790-4001
Email: [email protected]
[This sidebar area does not print.]
Novel Application of Ostomy Paste for Closure of Complex Salivary Fistulas
Joelle Glick, MD; Jason Kass, MD, PhD; Marita S. Teng, MD
Department of Otolaryngology- Head & Neck Surgery, Mount Sinai Hospital, New York, NY
Joelle Glick, MD Department of Otolaryngology- Head & Neck Surgery Mount Sinai Hospital Email:[email protected]
Contact 1. Fleischmann W, Strecker W, Bombelli M, Kinzl L. Vacuum sealing as treatment of soft tissue damage in open fractures [in German]. Unfallchirurg 1993;96:488-492. 2. Thompson JT, Marks MW. Negative pressure wound therapy. Clin Plast Surg 2007;34(4):673-84. 3. Glass GE, Murphy GF, Esmaeili A, Lai LM, Nanchahal J. Systemic review of molecular mechanism of action of negative-pressure wound therapy. Br J Surg 2014;101(13):1627-36. 4. Timmons J, Russell F. The use of negative pressure wound therapy to manage enteroatmostpheric fistulae in two patients with large abdominal wounds. Int Wound J 2014;11(6):723-9. 5. Asher SA, White HN, Illing EA, Carroll WR, Magnuson JS, Rosenthal EL. Intraluminal negative pressure wound therapy for optimizing pharyngeal reconstruction. JAMA Otolaryngol Head Neck Surg 2013;140(2):143-149. 6. Asher SA, White HN, Golden JB, Magnuson JS, Carroll WR, Rosenthal EL. Negative pressure wound therapy in head and neck surgery. JAMA Facial Plast Surg 2014;16(2):120-126. 7. Dhir K, Reino AJ, Lipana J. Vacuum-assisted closure therapy in the management of head and neck wounds. Laryngoscope 2009;119:54-61. 8. Yang YH, Jeng SF, Hsieh CH, Feng GM, Chen CC. Vacuum-assisted closure for complicated wounds in the head and neck region after reconstruction. J Plast Reconstr Surg Aesthet Surg 2013;66:e209-e216. 9. Braakenburg A, Obdejn MC, Feitz R, van Rooij Ia, van Griethnysen AJ, Klinkenbijl JH. The clinical efficacy and cost effectiveness of the vaccum-assisted closure technique in the management of acute and chronic wounds: a
randomized control trial. Plast Reconstr Surg 2006;118:390-397.
References
The end points for discontinuation of NPWT were the development of healthy granulation tissue and wound contracture in all cases. All wounds demonstrated adequate control of wound infection, rapid growth of granulation tissue, and contracture of the wound using the VAC system with ostomy paste. An adequate seal was maintained after the application of the VAC system and ostomy paste in all three patients. The airway did not need to be included in the negative pressure dressing in any patient. No adverse events occurred as a result of the VAC system or ostomy paste. There were no cases of pressure dressing application where the seal could not adequately be maintained with the additional use of ostomy paste.
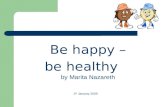
Three patients who had complicated wounds with either (1) salivary contamination or (2) a laryngectomy stoma that had previously failed conventional use of negative pressure wound therapy (NPWT) were included. Retrospective medical chart review was performed from September 2014 to March 2015 when the patients were treated. Application was performed at Mount Sinai Hospital and its affiliates in three patients. Data were collected including demographics, indications for NPWT, details of negative pressure dressing use, adverse events, wound healing results, potential risk factors for compromised wound healing, and wound characteristics. The InfoVAC (Kinetic Concepts, Inc, San Antonio, TX) wound VAC system was employed in all patients. Negative pressure was set at 125 mm Hg, in the continuous mode setting available with these devices. A standard polyurethane sponge was used in all cases. Stomadhesive (ostomy paste, ConvaTec Inc, Skillman, NJ) was used in all cases to reinforce the adhesive drape. In some cases, Tegederm transparent film dressings (3M, St Paul, Minnesota) were used on the surrounding skin prior to application of the wound VAC system. The VAC system was applied with the addition of ostomy paste around the wound to create a seal from the laryngectomy site or other salivary contamination (Fig. 1). Subsequent dressing changes were performed at a maximum of three days after application.
Methods and Materials
Postoperative fistulas in the head and neck region are common and related to multiple factors including: previous radiation exposure, malnutrition, and salivary contamination. Conventional wound management techniques that involve serial debridements, local/regional flaps, and free tissue transfers are burdensome for both the patient and healthcare providers. NPWT is an appealing and effective option in these patients as prolonged hospitalization due to postoperative fistula is associated with increased healthcare costs9. The use of NPWT to accelerate wound healing in the head and neck has previously been limited by the complex topography of the head and neck region as well as salivary contamination. Specifically, wounds with salivary contamination and those around a stoma are particularly challenging because an adequate seal cannot be maintained within the VAC system. In this study, we found that the addition of ostomy paste aided in our application of the VAC system to wounds contaminated with saliva. This method proved to be feasible and safe, and eliminated the need to use an artificial airway. Visualization of the overall wound was excellent using this technique because the stoma was not covered. Based on this preliminary data, we believe that the addition of stoma paste aids in the application of the wound VAC system around laryngectomy stomas, and provides an excellent addition to the otolaryngologist’s armamentarium for complex wound care. Larger prospective trials examining the use of stoma paste and VAC therapy in complex wounds of the head and neck will help support the data from this feasibility study.
Discussion
Until recently, the use of VAC system in the head and neck has been limited around stomas and in the presence of salivary contamination. We present a novel technique that is feasible, safe, and has potential to be a useful tool for complex wounds of the head and neck that involve either salivary contamination or peristomal application after laryngectomy.
Conclusions
The principles of local wound care have been utilized in the treatment of chronic wounds for over centuries. Negative pressure wound therapy (NPWT), first described by Fleischman et al in 1993, involves the application of suction, or negative pressure, to wounds that are healing1. NPWT has been shown to accelerate healing by promoting angiogenesis and granulation through improved local blood flow, reduction of chronic edema, and decreased wound bed bacterial counts. The benefits of this type of wound management include more rapid wound healing time and facilitation of wound care in situations that would otherwise be difficult or challenging2,3. While NPWT was used for many years in the treatment of chronic wounds, such as leg ulcers and bedsores, its use has now been modified for the use with surgical wounds4. Numerous applications have been reported throughout the body, however, there is little data on treatment of complex wounds in the head and neck region. Recent data, however, suggests that NPWT is safe and has the potential to be a useful tool for complex wounds of the head and neck5,6,7,8. The complex topography of wounds in the head and neck has previously precluded the use of the Vacuum Assisted Closure (VAC) system in this region. The most common challenge has been maintaining a seal around wounds that are in close proximity to a tracheostomy or laryngectomy stoma7. If the seal cannot be maintained, local wound care must be used instead of the VAC system. Peristomal application of the VAC system after laryngectomy by using an artificial airway has recently been described in thirty-two patients by Asher et al6. An artificial airway, fashioned from an endotracheal tube, is incorporated into the wound VAC system in these cases. At our institution, we have used this excellent technique for challenging wounds around stomas. However, we sought to modify this method by using stoma paste to facilitate an adequate seal, thereby avoiding the need for an artificial airway. Ostomy paste has conventionally been used to help maintain a seal with abdominal ostomies4. In the current study, we use ostomy paste in conjunction with the wound VAC system to maintain an adequate seal around laryngectomy stomas with salivary contamination.
Results
Figure 1. A, B, C: Patients before and after wound VAC and stoma paste application. D: Stoma paste
Introduction
STOMA
STOMA
SALIVARY LEAK
SALIVARY LEAK
STOMA PASTE
STOMA PASTE
WOUND VAC
WOUND VAC
A
B
C
D
STOMA
SALIVARY LEAK
STOMA PASTE
WOUND VAC