JLHQH 3URJUDPPH 56+3 · sdwlhqfh lq wkh idfh ri xqzduudqwhg ghod\v lq frpsohwlqj wkh hydoxdwlrq ,q...
202
Evaluation of UNICEF Viet Nam Rural Sanitation and Hygiene Programme (RSHP) 2012 – 2016 Evaluation Period: June 2017 – June 2018 FINAL EVALUATION REPORT July 05, 2018 Evaluation Commissioned By: UNICEF Country Office Viet Nam Prepared by Prepared for AAN Associates Islamabad, Pakistan www.aanassociates.com UNICEF Country Office in Viet Nam
Transcript of JLHQH 3URJUDPPH 56+3 · sdwlhqfh lq wkh idfh ri xqzduudqwhg ghod\v lq frpsohwlqj wkh hydoxdwlrq ,q...

Evaluation of UNICEF Viet Nam Rural Sanitation and Hygiene Programme
(RSHP) 2012 – 2016
Evaluation Period: June 2017 – June 2018
FINAL EVALUATION REPORT
July 05, 2018
Evaluation Commissioned By: UNICEF Country Office Viet Nam
Prepared by Prepared for
AAN Associates Islamabad, Pakistan www.aanassociates.com
UNICEF Country Office in Viet Nam

Acknowledgements The Evaluation Team is grateful to the Ministry of Agriculture and Rural Development (MARD), Ministry of Health (MoH), associated departments and relevant provincial governments of Viet Nam, for their support and contributions to the evaluation. We are thankful to the members of the Evaluation Reference Group (ERG) for oversight and valuable inputs to the evaluation. We are also thankful to other stakeholders including representatives from donors group, civil society, and communities for finding time to meet with the evaluators and sharing their impressions and reflections. This would not have been possible without the support from UNICEF Viet Nam. Thanks are due to the team members from Planning, Monitoring, Evaluation & Research and WASH teams for facilitating access to materials, relevant officials, and communities. This indeed enabled us to plan and implement a robust, objective and impartial evaluation. Moreover, for their understanding and patience in the face of unwarranted delays in completing the evaluation. In particular, thanks are due to Ms. Hoa Ngo (Chief of PME), Mr. Friday Nwaigwe (Chief CSD), Ms. Sevara Hamzaeva (Interim PME), Mr. Lalit Patra (WASH), Ms. Nguyen Thanh Hien (WASH), and Mr. Viet Xuan (WASH), for their support throughout the evaluation. We take the opportunity to thank our local partner M/s DEPOCEN, for taking on the responsibility of field data collection and coordination with stakeholders. Special thanks to Ms. Ha Nguyen Thu, Mr. Hoang Kim, and Ms. Luc Thi Phoung. We take the opportunity to thank all field team members for hard work and dedication. On behalf of AAN, we express thanks to our team that worked on the evaluation comprising of Mr. Asmat Ali, Mr. Saad Ibrahim, Mr. Aemal Khan, Ms. Amna Ijaz, Mr. Jibran Raja, Mr. Asad Ullah Khan, and Mr. Faisal Shahzad. We gratefully acknowledge the advice and support extended by Ms. Simone Klawitter and Mr. Sarmad Khan for finalising the report. We wish UNICEF and Government of Viet Nam success in their joint efforts in future and sincerely hope that this evaluation provides deeper insights to inform and guide future collaboration. The findings and analysis in this report are informed by opinions from multiple stakeholders, however the evaluators take full responsibility for the contents of this report. Nadeem Haider Evaluation Lead/Managing Director AAN Associates

List of Acronyms C4D Communication for Development CATS Community Approaches to Total Sanitation CCPD Common Country Programme Document CHE Provincial Centre for Health Education CLTS Community Led Total Sanitation CPM Centre for Preventive Medicines CSD Child Survival and Development DANIDA Danish International Development Agency DARD Department for Agriculture and Rural Development DFAT Department of Foreign Affairs and Trade (Australia) DOF Department of Finance DoH Department of Health DPI Department of Planning and Investment GDP Gross Domestic Product GOVN Government of Viet Nam HH Household HHS Household Survey HWTS Household Water Treatment and Storage HWWS Handwashing with Soap INGO International Non-Governmental Organization JMP Joint Monitoring Programme KAP Knowledge, Attitude and Practices MARD Ministry of Agriculture and Rural Development MDG Millennium Development Goals LMIC Lower Middle-Income Country MICS Multiple Indicator Cluster Survey MNCH Maternal, New-born and Child Health MOF Ministry of Finance MOFA Ministry of Foreign Affairs MoH Ministry of Health MOJ Ministry of Justice MOLISA Ministry of Labour, Invalids and Social Affairs MoRES Monitoring Results for Equity System MPI Ministry of Planning and Investment NCERWASS National Centre for Rural Water Supply and Sanitation NGO Non-Governmental Organization NTP National Target Program O&M Operation and Maintenance OD Open Defecation ODF Open Defecation Free PCERWASS Provincial Centre for Water Supply and Sanitation RSHP Rural Sanitation and Hygiene Programming RWSS Rural Water Supply and Sanitation RWSSP Rural Water Supply and Sanitation Partnership SanMark Sanitation Marketing SDG Sustainable Development Goals SEA South East Asia SEDP Socio-Economic Development Plan SPSS Statistical Package for Social Sciences TVD Triggered, Verified and Declared USD United States Dollar VBSP Viet Nam Bank of Social Policy VIHEMA Viet Nam Health and Environmental Agency WASH Water, Sanitation and Hygiene WHO World Health Organization WSP Water and Sanitation Programme

Table of Contents Executive Summary .......................................................................................................................... I
1 Context and Object of the Evaluation ....................................................................................... 1
Context .............................................................................................................................. 1
WASH Sector Context and Evolution ............................................................................... 2
National Water and Sanitation Strategy and Standards................................................... 3
Rural Sanitation and Hygiene Programme (RSHP) 2012–2016 (Object of Evaluation) .. 5
RSHP Significance ........................................................................................................... 5
RSHP (Projects) Objectives & Outputs ............................................................................ 6
RSHP Components .......................................................................................................... 8
RSHP Geographic Coverage ........................................................................................... 8
RSHP Target Groups / Beneficiaries ................................................................................ 8
Key Stakeholders and RoleS ............................................................................................ 9
Theory of Change (TOC) ................................................................................................ 11
2 Evaluation Purpose, Scope and Methodology ....................................................................... 15
Evaluation Purpose ......................................................................................................... 15
Objectives ....................................................................................................................... 15
Evaluation’s Significance ................................................................................................ 15
Evaluation Audience, Utilization, and Dissemination ..................................................... 16
Evaluation Criteria and Key Questions ........................................................................... 16
Evaluation design, Methodology, approach and Limitations .......................................... 18
Evaluation Methods ........................................................................................................ 19
Data Processing and Consolidation ............................................................................... 23
Quality Assurance (Internal and external) ...................................................................... 24
Limitations, Constraints & Mitigation Strategies ............................................................. 26
Evaluation Implementation, Management, & Team Composition .................................. 28
3 Evaluation Findings ................................................................................................................ 30
Relevance ....................................................................................................................... 30
Effectiveness ................................................................................................................... 35
Effectiveness of Public Sector Delivery Mechanisms .................................................... 43
Efficiency ......................................................................................................................... 63
Sustainability ................................................................................................................... 65
Equity, Gender, Resilience and HRBA ........................................................................... 70
WASH-MalNutrition (Children) Nexus in Viet Nam ........................................................ 75
4 Conclusion, Lessons Learned and Recommendations .......................................................... 79
Conclusion ...................................................................................................................... 79
Lessons Learned ............................................................................................................ 80
Recommendations .......................................................................................................... 81
Appendix 1: Terms of Reference ................................................................................................... 85
Appendix 2: Evaluation Matrix ....................................................................................................... 94
Appendix 3: Sampling Frame (Sampling Rationale and Strategy) ................................................ 97

Appendix 4: Inception Phase Data Collection Format ................................................................... 99
Appendix 5: Questionnaire for the Household Survey ................................................................ 100
Appendix 6: Qualitative Toolkit .................................................................................................... 120
Appendix 7: Field Staff Training, Pre-Testing and Translation of the Finalized Tools ................ 130
Appendix 8: List of Key Informant Interviews .............................................................................. 132
Appendix 9: List of Participants in Key Informant Interviews ...................................................... 133
Appendix 10: List of Focus Group Discussions ........................................................................... 134
Appendix 11: List of Participants in Focus Group Discussions ................................................... 135
Appendix 12: List of Documents Reviewed ................................................................................. 142
Appendix 13: Household Survey Results .................................................................................... 145
Appendix 14: Evaluation Team .................................................................................................... 166
Appendix 15: Evaluation Norms and Compliance ....................................................................... 167
Appendix 16: Glimpse of Evaluation Data Collection .................................................................. 170
Appendix 17: Results framework and activity-wise project description of seven provinces ....... 173
List of Tables Table 1.1: RSHP Projects & Results Hierarchy ............................................................................... 6
Table 1.2: Stakeholder Roles and Contribution ............................................................................... 9
Table 2.1: Evaluation Audience and Utilization ............................................................................. 16
Table 2.2: Evaluation Criteria and Corresponding Evaluation Questions ..................................... 17
Table 2.3: Overall Sample Distribution by Districts and Villages .................................................. 20
Table 2.4: Geographic Scope of the Post-KAP Survey ................................................................. 20
Table 2.5: Distribution of Head of households by gender and province ....................................... 21
Table 2.6: Percent distribution of Head of households within province by gender ....................... 21
Table 2.7: Key Informant Interviews Administrative Distribution ................................................... 21
Table 2.8: Key Informant Interviews Distribution ........................................................................... 22
Table 2.9: Evaluation Limitations and Mitigation Measures .......................................................... 27
Table 2.10: Evaluation Phases, Activities and Deliverables.......................................................... 28
Table 3.1: Percent distribution of respondents reporting water safety and quality ....................... 33
Table 3.2: Percentage of HHS reporting community participation in programme activities .......... 49
Table 3.3: Percentage distribution of households' access to sanitation........................................ 51
Table 3.4: Percent distribution of respondents reporting their knowledge regarding place where sanitary materials and supplies for constructing toilets are available for purchase ...................... 52
Table 3.5: Percentage of households reporting level of awareness about available assistance options to build a latrine ................................................................................................................. 52
Table 3.6: Percentage of respondents reporting type of assistance received to build a latrine ... 52
Table 3.7: Percent distribution of respondents reporting reasons for using a toilet facility ........... 54
Table 3.8: Percentage distribution of respondents regarding their preferences and trust of the source of information about hygiene and toilets by end line (province) ........................................ 54
Table 3.9: Percent distribution of respondents reporting times for handwashing ......................... 55
Table 3.10: Percent distribution of respondents reporting items usually used for washing hands56

Table 3.10A: Percent distribution of respondents observed for presence of water for handwashing by province and gender ........................................................................................... 56
Table 3.10B: Percent distribution of households observed for place of Handwashing ................. 56
Table 3.11: Percent distribution of households observed with some cleansing agent at specific place for handwashing ................................................................................................................... 56
Table 3.12: Percent distribution of respondents reporting reasons for washing of hands ............ 56
Table 3.13: Percent distribution of respondents reporting awareness of ways to protect children against diarrhoea ........................................................................................................................... 57
Table 3.14: Percent of respondents reporting type of water source for drinking and cooking ...... 59
Table 3.15: Percentage of respondents reporting access to water sources – throughout the year by province ..................................................................................................................................... 60
Table 3.16: Percentage distribution of households' access to sanitation...................................... 61
Table 3.17: Percent distribution of respondents reporting nature of toilet facility ......................... 61
Table 3.18: Percentage distribution of households observed for existence of latrine ................... 61
Table 3.19: Percentage distribution of households observed for some sign of latrine use .......... 61
Table 3.20: Provincial child friendly projects approval/start dates ................................................ 63
Table 3.21: Financial Summary for the An Giang Child Friendly Project ...................................... 64
Table 3.22: Percent distribution – extent of slippage by province ................................................. 68
Table 3.23: Social norm analysis ................................................................................................... 69
Table 3.24: Percent distribution of respondents reporting natural disaster in last 2 years by province .......................................................................................................................................... 73
List of Figures Figure 1.1: Viet Nam - Geographic coverage of UNICEF Programme ........................................... 1
Figure 1.2: Public Sector Water and Sanitation Services Institutional Apparatus in Viet Nam (overall state management) ............................................................................................................. 3
Figure 2.1: TOC 01 - Rural Sanitation Projects with MoH/VIHEMA and Provincial Projects ........ 13
Figure 2.2: TOC 02 - Rural Water Safety Project with MARD. ...................................................... 14
Figure 2.3: Evaluation Methods for Primary Data Collection ........................................................ 19
Figure 3.1: UNICEF WASH Sector Enabling Environment Framework ........................................ 36
Figure 3.2: Percentage of Rural HHs having access of Improved Water ..................................... 59
Figure 3.3: Percentage of Rural HHs using improved Sanitation .................................................. 60
Figure 3.4: Percentage of households by availability of soap ....................................................... 62
Figure 3.5: UNICEF funds to national ministries and provincial child friendly projects ................. 64
Figure 3.6: Distribution of funds by region, programme component and province ....................... 65

I
Executive Summary Sector Context: Viet Nam is a mid-income country located in Southeast Asia. With a population of 92 million1, it is the thirteenth (13th) most populous country in the world. In recent decades, the country has made impressive progress in reducing poverty and improving access to public services including water and sanitation. For instance, access to improved water supply increased from 50% in 1990 to 94% by 2011. Similarly, access to improved sanitation has surged twice i.e. from 30% to 67% for the same time period2. The significant policy actions taken include: approval of ‘National Rural Clean Water Supply and Sanitation Strategy 2000-2020’ (revised in 2016); three (03) rounds of ‘National Target Programme’ for water and sanitation (from 1998 to 2015); and approval of standards concerning water quality and hygienic toilets. There are evident inequities in poor3 and ethnic minorities (in Central Highlands, Northern Mountains and Mekong river delta) still deprived of services. It is in these areas and groups that UNICEF prioritised to work with4. The country envisions to achieve ‘country-wide ODF’ by 2025, and ‘universal access to safe drinking water’ by 2030 respectively. The country has concluded a loan agreement with World Bank for rural water and sanitation programme i.e. Results-Based Scaling Up Rural Sanitation and Water Supply Programme, to be implemented in 21 under-developed provinces. Rural Sanitation and Hygiene Programme (2012–2016): Object of Evaluation: A total of 10 national and sub-national (provincial) projects (2 national and 8 sub-national) constitute the UNICEF supported Rural Sanitation and Hygiene Programme (RSHP). Of the two national projects one focuses on rural water and the other rural sanitation, whereas all provincial projects are multi-sector (called Child Friendly Projects) of which WASH is a part. For rural water, the key partner is Ministry of Agriculture & Rural Development (MARD), whereas Ministry of Health (MoH) is the lead partner for rural sanitation. The provinces where projects were implemented include Dien Bien, Lao Cai, Ninh Thuan, Gia Lai, Kon Tum, An Giang, Dong Thap, and Ho Chi Minh City. Except Ho Chi Minh (an urban project), the remaining seven provincial projects are covered in the evaluation. The projects were implemented from 2012- to 2016. The national projects envisioned to strengthen the water and sanitation services. The provincial projects were driven to improve the provision of child survival and development services for disadvantaged children. The programming interventions evaluated could be grouped into: i) WASH enabling environment ii) Capacity development iii) Technological innovation & sanitation marketing iv) Behaviour change communication (BCC) and v) Advocacy for child rights/development. Key stakeholders and beneficiaries include MARD, MoH, Ministry of planning and Investments (MPI), UNICEF, communities, especially children (boys and girls), and businesses associated with rural water and sanitation services. Together with UNICEF two TOCs (ex-post - illustrations 2.1 and 2.2) were framed (one each for rural water rand rural sanitation) and used for the evaluation. The evaluation hypothesis is: “UNICEF projects (national and sub-national) resulted in accelerating access to improved water sources, hygienic latrines (as per GOVN approved standards) and practice of hand washing with soap in (rural) areas where seven sub-national projects were implemented from 2012 to 2016”. Evaluation Purpose, Objectives, Significance, Criteria and Scope For a balanced focus on both ‘accountability’ and ‘learning’ purpose, the evaluation has been tagged as ‘Summative-Formative’ evaluation. More specific purposes were to: ‘generate evidence of success for RSHP (2012-16), and document learning to inform UNICEF-GOVN upcoming cooperation programme’5. The objectives included to: i) generate evidences of Programme’s successes ii) inform UNICEF management of continuity and direction of future WASH assistance iii) contribute to regional and global discourse and learning and iv) map out the extent of slippage i.e. reversal to open defecation free (ODF) communities and assessment of social norm creation of latrine use. On the request of UNICEF management, the evaluators added a commentary on (mostly based secondary sources) WASH-Malnutrition Nexus (for children) in Viet Nam, and the extent to which UNICEF provincial projects have affected child malnutrition.
1 World Bank (2016) 2 World Bank | Water Supply and Sanitation in Viet Nam, Turning Finance into Services for the Future, December 2014 3 ADB (2010) 4 For a more detailed outline of the WASH sector see UNICEF, 2015. “WASH Outcome Paper”, developed within the 2016-2021 CCP process – including a comprehensive stakeholder overview. 5 United Nations Children’s Fund (UNICEF), 2017. Statement of Work and Terms of Reference – Evaluation of UNCEF Viet Nam’s Rural Sanitation and Hygiene Programming 2012-2016.

II
Both the Programme and its evaluation hold value to UNICEF. The Programme is valuable for applying technical assistance approach in a mid-income country with focus on accelerating water safety and community-based sanitation. Also, for introducing the community led total sanitation (CLTS) approach and demonstrating success of integrated child development approach. The evaluation is significant for being first systematic and independent assessment of UNICEF contributions to strengthening governance and improving access to safe water and hygienic latrines for rural Vietnamese. Moreover, it holds significance in terms of demonstrating UNICEF’s commitment to accountability to its partners, donors, and communities. Furthermore, it shall be the first to map out the extent of slippage (in ODF communities) and assessment of social norm creation of latrine use. The key audiences include UNICEF, key government counterparts such as MoH, MARD, MPI, donors, and NGOs involved in WASH. The evaluation criteria included standard OECD-DAC (Organisation for Economic Cooperation and Development-Development Assistance Committee) criteria except for impact i.e. focusing on relevance, effectiveness, efficiency, and sustainability/scalability. The Non-DAC criteria included equity, gender, resilience, and Human Rights Based Approach (HRBA) to programming (to assess compliance to UNICEF normative programming principles). The scope includes evaluation of all rurally focused projects (except one for Ho Chi Minh city) of RSHP, implemented from 2012-16. The social norms assessment included only the assessment of practice of exclusive latrine use. Evaluation Design, Methodology, Approach and Limitations: Keeping in view the evaluation objectives and questions, an overarching ‘Theory Based’ evaluation approach has guided the evaluation. Within that a ‘Hybrid Evaluation Design’ comprising ‘Descriptive’ and the ‘Social Norms Theory’ designs have been applied to asses Programme’s contributions. The ‘before and after’ sub-design was used to assess supply side interventions. The standard principles of ‘Social Norms Theory’ have guided the social norms assessment. ‘Mixed-method’ and ‘Participatory’ approaches were applied for data collection, analysis and evaluation management. Besides the secondary data both qualitative and quantitative methods were used for data collection. The key methods applied included: household survey (Post-KAP), key informant interviews (34 KIIs), focus group discussions (24 FGDs including men, women, boys and girls), field observations, and field photographs. Stratified-random and purposive sampling techniques were applied for respondents’ and stakeholders’ selection. A series of processes were evolved and implemented to ensure compliance with established research and ethical standards. A Hanoi based research institute and think-thank, DEPCON, was contracted for field work as local partner. The process was participatory as it sought to take views from all key stakeholders (over 600 people including public officials, donors, UNICEF, NGOs, and communities were consulted). An Evaluation Reference Group (ERG) comprising key stakeholders was formed to provide steerage and approve deliverables. The evaluation faced some delays subject to some issues with regards to accessing secondary data, securing visa for team, securing approvals for field data collection, changes in UNICEF team, and multiple rounds of feedback to finalise report.
Evaluation Findings
Relevance: The RSHP is assessed to be relevant in terms geographic targeting (of under-developed regions and marginalised groups); addressing priority needs of the intended beneficiaries; coherence with the national and UNICEF’s global WASH strategic priorities; and focusing on the institutional capacity gaps of relevant public stakeholders. The Programme targeted the most deprived regions and provinces including community groups that needed the assistance most i.e. ethnic minorities in Northern Mountains and Central Highlands regions. The provinces where Programme was implemented are relatively under-developed with highest concentration of ethnic minorities. The secondary evidences suggest higher poverty rates (almost double the national average), limited accessibility to safe water and hygienic sanitation services, and higher child stunting rates amongst the ethnic minorities, which illuminates relevance in terms of geographic and group targeting and UNICEF’s own focus on equitable services.

III
The issues that the Programme sought to address including the approaches such as CLTS, were found to be relevant and aligned with national priorities and policies such as ‘National Rural Clean Water Supply and Sanitation Strategy to 2000-2020’. Moreover, these were found to be consistent with the priorities under the ‘National Target Programmes for WASH’ implemented from 1998-2015 in three phases. The prioritisation to shift focus from infrastructure (a preferred choice of public stakeholders) to community approaches was found to be relevant to the context. The focus to institutionalise CLTS in the public sector was assessed to be appropriate and relevant to the context. The Programme’s support to ‘Innovative and Low-costs’ solutions for both water safety and sanitation further added to its relevance. Effectiveness: Overall, the Programme was assessed to be largely effective vis a vis evolving participatory mechanisms to identify needs, causes and solutions e.g. Bottleneck Analysis exercises undertaken with provinces. The exercises helped prioritising interventions around causes and not symptoms, often confused with causes. The support and approach used to advocate, and support adoption of policy shift for rural sanitation (in terms of replicating the CLTS) proved relatively more effective than one for rural water. Overall, the achievements highlighting Programme’s effectiveness include: lobbying a support for the revision of National WASH Strategy 2000-2020 (in 2016); formulation of Provincial ODF Road Maps; securing political commitments for Universal access to safe Water and Sanitation; initiation of SDG Baselines; review of National Water Quality Standards (NQS); and institutionalisation of CLTS. UNICEF support has contributed to improved sector coordination as evident in the creation of new forum in 2014 in the form of “Working Group on Operations and Maintenance” (O&M)’ of rural water supply. Also, it kept alive the ‘Working Group on Sanitation’ (formed in 2010). The forums provided opportunities to the stakeholders to discuss issues of common interest. As regard to improving sector monitoring, it could be concluded that the rural water supply monitoring has shown improvements, and analysis suggests that O&M systems should be strengthened. Rural sanitation related monitoring processes are still evolving and may require support in coming years to help government agencies track pre and post ODF monitoring, including social norms creation and slippage. The current monitoring system has not capitalised on the potential offered by the latest information technology options, to offer real-time monitoring data and analysis, including visual presentation. Moreover, the current system lacks capacities to perform cross-sectoral analysis such as linking water and sanitation to health and nutrition. The relevant ministries need technical assistance to improve monitoring systems and perform cross-sectoral analysis to advocate for relevant sector reforms. In terms of strengthening services, the contributions in improving rural sanitation services are relatively more significant and visible, highlighting Programme’s effectiveness. For rural water, UNICEF supported the annual ‘Joint Water Sector Review’ events from 2012 until 2015. These reviews helped pull out key issues for policy debates and advocacy. The reviews discontinued after UNICEF withdrawal of support. The advocacy to rationalise water quality standards (or parameters of assessment) could not make much headway. The most notable successes were witnessed in the form of developing national and provincial ‘Water Safety Plans’, recognizing ‘water safety’ as one of the challenges meriting interventions, and government’s replication of RSHP BCC products for community education around water treatment and safe storage, though at a limited scale. Furthermore, the successful demonstration of finding ‘Entrepreneur led Low Cost Water Filtration Solutions’ also comes across as a notable milestone of the Programme. For rural sanitation, one key contribution is in terms of defining the mandate and placing MoH/VIHEMA as lead for rural sanitation public agency. The Programme has shifted focus from government preferred and supported (subsidy and infrastructure led) sanitation to community led programming. The successful roll-out of CLTS with enabling guidance through disseminating Communication for Development (C4D) training materials and guidelines for ODF certification etc. has facilitated institutionalisation of CLTS approach in Viet Nam. The national and provincial governments are better placed (in terms of institutional capacities) today to replicate and scale-up the (Programme) initiatives. The draft ODF plan (provincial) has been developed, however it would require regular follow-up for allocation of resources and pro-active implementation to help realise the vision of country-wide ODF. The interest and capacities of relevant public-entities to improvise the BCC approaches and implementation (because of involvement in CLTS implementation in pilot provinces and villages), is

IV
high. Furthermore, the Programme has contributed towards developing low-cost latrine designs and encouraged entrepreneurial activity around it. Limited evidence was available to substantiate successful integration of gender and disability considerations and disaster resilience in latrine designs offered. The Programme has largely achieved the outcome level results i.e. accelerated access to improved sanitation (by encouraging people to construct latrines and abandon OD practice), and increased understanding of personal and environmental hygiene and associated behaviours (including water safety). However, due to limited documentation the extent to which outcomes have been achieved remains unknown. Primarily, the qualitative evidences suggest the plausibility of the programme logic model or Theory of Change (TOC). The Programme produced a series of unintended results both positive and otherwise. The most significant of the unintended results emerged in the form of: a) wider awareness of health risks and mitigative actions demonstrated through adoption of water safety practices and improved hygienic behaviours , enabling communities in reducing the risks of post-emergency epidemics in RSHP supported areas; b) wider acknowledgement and recognition within government (on both national and provincial levels) for integration and replication of community-based approaches in other sectors such as health, immunization, nutrition, child protection, risk reduction and others, especially in emergency situations and; c) added work-load for women and girls in finding sufficient water to keep latrines functional and clean in water scarce areas, particularly in drought situations. Efficiency: The RSHP implementation is assessed as efficient in terms of timely completion of planned activities, funds utilisation, and leveraging public sector funds for shared results. The provinces did well to implement activities despite having lag time of 6-18 months between signing of contract and approval of Action Plans. For instance, despite delayed kick-off, Dien Bien province (18 months lag time) managed to implement and complete 98% of the planned activities. Similarly, the funds utilisation at 85% (of allocated budgets) is satisfactory also. The funds distribution between provinces and national projects was found to be balanced as well. In terms of sectoral allocations (within provincial budgets), the CSD activities (of which WASH is a sub-component) received maximum share i.e. 43%, which points to adequacy of resources also. Some provinces exhibited insufficient allocations for certain activities. Others like Lao Cai did not have any allocations at all for M&E beyond 2013. Limited financial tracking and level of disaggregation impeded drawing value for money (cost per beneficiary) analysis. Moreover, no in-country and regional data is available to draw meaningful comparisons to assess efficiency. Sustainability: For rural water, the formulation of ‘Water Safety Plans’ is a step in the right direction and bodes well for sustainability. The joint implementation of BCC/C4D campaigns for water safety with provincial health authorities has evidently enhanced capacities and are likely to sustain beyond Programme’s life. The campaigns have raised community’s knowledge and increased adoption of practices, which are likely to sustain. The ‘Entrepreneur led Water Safety Model’ (ceramic filter) remains one of the major highlights of the Programme and if given the added support in establishing rural markets, may prove useful and sustainable. The practice of holding sector reviews exclusively for water was discontinued. The O&M Working Group is likely to sustain; however, the PO MARD will require added support to keep coordination forum alive and relevant in the face of an evolving context. For rural sanitation, the Programme has demonstrated the success of CLTS as an approach which in view of the planned/anticipated scale-up of CLTS is likely to sustain. The other results that may sustain include: ‘National WASH Strategy’ (as guidance document); the redefining of MoH/VIHEMA mandate as the lead rural sanitation implementer; availability of tested training manuals; and improved standards for ODF verification and certification. The SanMark related achievements, however, vary across provinces and are likely to continue beyond projects. The enhanced capacities of MoH/VIHEMA are likely to sustain, however they may require continuous support. The issue of ‘Slippage’ (communities reverting to open defecation in ODF certified communities) is very much present, amounting to15% of certified communities. This may appear reasonable, especially in a context where only limited post ODF support was given by the government. The availability of household latrines at 97% presents very encouraging situation and suggests success of RSHP in accelerating latrine construction. The frameworks of ‘Social Norms Theory’ was used for the assessment of social norm status. The results point to the existence of a ‘weak’ or an ‘unstable’ social norm’ for latrine use; partly due to significant inconsistencies between empirical and normative expectations. The sanctions for delinquent behaviours (such as OD) within communities are insignificant i.e. 32%. Such a state of affairs merit rethinking of CLTS implementation approach and added guidance from UNICEF on social norms programming.

V
Equity, Gender, Resilience and HRBA
Equity: The Programme’s adherence to equity dimensions varies in terms of design, targeting, interventions and results. The prioritisation of poorest and most deprived regions and provinces adds to equity integration. The Programme interventions benefitted all, including women and children, often considered as disadvantaged. Limited use of minority language in BCC interventions demonstrates reduced coherence with equity. The low-cost water filtration and latrines options continue to benefit poor, hence illuminating equity integration. The latrine designs were found to be disability neutral, downgrading equity integration. The loans for water and sanitation are available, however the criteria and processes work to exclude most poor. The Programme monitoring systems failed to capture benefits for poor and disadvantaged groups. Gender: The RSHP design and delivery approaches were assessed as gender-sensitive as evident from involving ‘Women Unions’ in triggering and C4D activities. The C4D products included contents that focused on women and girl’s issues e.g. hygiene, health and others (including children), hence amplifying gender integration. The child-focused interventions particularly at schools add further to programme being gender-sensitive. The monitoring system did not capture fully the results from a gender-focused perspective. Resilience: Viet Nam being a disaster-prone country merits a concerted focus on ‘resilience integration’ in designing future programmes, which to a degree is evident from different interventions undertaken. For instance, support was given to NCERWASS to help improve capacities of staff to integrate ‘resilience’ into regular and humanitarian response services. Regulations were issued for controlled water use during droughts. Technical support was provided to assist with updating the ‘Provincial DRR/Climate Change Adaptation Plans’. The SanMark interventions did include resilient designs e.g. septic tanks, while school interventions integrated resilience lens. The BCC/C4D campaigns also included messages on dealing with emergency situations. Human Rights: The Programme supported the government to deliver services prescribed as Rights, which adds to the coherence with rights-based programming. The focus on child development and survival which Viet Nam subscribes to by being the signatory to the Convention on the Rights of Children (CRC), 1989, further emphasizes coherence with rights principles. The coherence with human rights programming is evident through its balanced focus on both the duty bearers (public agencies) and right holders (men, women, boys and girls). The focus on minorities and poor added further to its adherence to the rights approach/es. WASH-Malnutrition Nexus: The WASH-Malnutrition nexus is well established and holds grounds for Viet Nam also. A UNICEF study generated evidence of adoption of water safety, personal hygiene, and latrine use (practices) contributing to reduced diarrhoea and worm infections, in project communities. Another report suggests that in Viet Nam not all malnutrition is poverty driven or from food inaccessibility. Based on secondary evidences, the Evaluators may argue that there are considerable evidences to prove and reinforce WASH-Child Malnutrition in Viet Nam. However, Evaluators may advise to commission a separate study for detailed assessment.
Conclusion, Lessons and Recommendations
Conclusion: The Programme has largely been relevant, effective, and efficient. The contributions and successes for rural sanitation have been relatively more profound and enabled the institutionalisation of CLTS within the public domain. The policy and capacity development related interventions and results appear more sustainable than others. The interventions like water safety and ODF plans would need further support. The monitoring system needs to develop the sustainability lens particularly with reference to tracking slippage and norms creation. The qualitative evidences reinforce the plausibility of ToC. Despite data limitations, the evaluators could argue that the Programme has contributed to accelerating access to safe water and hygienic latrines. There are secondary evidences that support an inverse correlation between WASH-Malnutrition, however it is advised to commission a separate study to assess UNICEF’s work in reducing child-malnutrition in selected provinces. The public-sector partners anticipate continued technical support from UNICEF. The upcoming World Bank funded programme offers opportunities for UNICEF to dovetail technical inputs such as research, monitoring, training and others. Lessons Learned: The key lessons learned centre around: i) 1. The community-based development interventions must attempt to leverage the existing community platforms and the representatives, to

VI
benefit fully from their good-will and influence; ii) Social entrepreneurship is critical to achieving social impact; iii) The ‘Integrated (multi-sector) Approach’ for provincial projects has evidently created value in leveraging thematic overlaps, complementarities, and optimisation (of resources); iv) Evidence creation holds key to effective advocacy; and, v) The availability of adequate and qualified team is critical to successful implementation of technical assistance initiatives. Recommendations: Following are the key recommendations outlined for UNICEF to guide the focus of future assistance of UNICEF Viet Nam for Rural Water Supply, Safety and Rural Sanitation:
1. Monitoring System Support (Water): Align and harmonize the current monitoring indicators, tools and reporting system for water safety and quality with SDG 6.1 targets and indicators.
2. Water Safety Products and Promotion (Water): Continue advocacy with MARD to support local businesses and entrepreneurs for innovation and cost reductions for localised water-safety products and additional public-sector investments for BCC campaigning to influence people’s behaviour.
3. Research and Innovation (Water and Sanitation): Enable relevant public-sector partners to explore, establish and support partnerships with private sector research entities, academia, and businesses for technology innovation and contextualisation.
4. Coordination, Partnerships, Advocacy (Water and Sanitation): Encourage and where required extend technical support to PO MARD to play its due role effectively in public advocacy, sector coordination, increased resources allocation and research and evidence creation.
5. Resource Mobilization and Provision of Equitable Services (Sanitation): Continue advocating and lobbying with national and provincial governments for approval of ‘Provincial ODF Plans’ and allocation of adequate resources for implementation of plans; also provide technical support to VIHEMA/DoH where required for effective CLTS/CATS implementation.
6. Social Norm Integration (Sanitation): Review the successes, bottlenecks and opportunities in the implementation of CLTS/CATS for creation of ‘social norm’ (for handwashing with soap and latrine use) considering the existing capacities of local government tiers and the communities as well.
7. Strengthening Monitoring System (Sanitation): Extend technical assistance in revamping of rural sanitation related Monitoring System to enable sector partners draw relevant, usable and timely (monitoring) information and evidences to facilitate informed decision-making.

1
1 CONTEXT AND OBJECT OF THE EVALUATION
CONTEXT
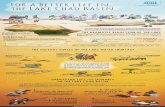
Viet Nam, a member of ASEAN, is ranked as the 3rd fastest developing nation in Asia after China and Indonesia. It is located on the Indochinese Peninsula in the heart of Southeast Asia, with a total land area of 331,210 square km. Viet Nam shares border in the North with China, Cambodia and Lao PDR in the West, while in South it faces the Gulf of Thailand and the South China Sea in the East. The long coastline of 3,444 km in addition to the densely disposed networks of lakes and rivers in the Mekong delta and the Red River delta. Likewise, the Central Highlands is home to numerous export products such as coffee, cashew nuts, pepper and rubber. Viet Nam is strategically located especially for international trade6. According to World Bank 2016 estimates, Viet Nam has a population of more than 92 million7 and is ranked as 13th most populous country in the world. Viet Nam has attained middle income country status in 2010 and is home to a wide range of ethnic groups. Among these, Kinh people are the majority and are also the most affluent and influential. Viet Nam is also home to 54 different minority groups including the Hmong, Dao, Tay, Thai and Nung. In the last two decades, the country has opened up to civil participation. The Vietnamese government has demonstrated commitment to economic progress and global integration. The economy has diversified and focused on embracing more aggressive, export-driven industries. The accelerated economic development has brought an unprecedented decrease in poverty, with poverty levels coming down from 58% in the early 1990s8 to 7% in 2015 (Asian Development Bank’s 2018)9. While standards of living have improved for the majority, not all groups have benefited equally. For instance, in 2014, 13.8% of ethnic minority group members continued to live in poverty ($1.90-a-day poverty)10 compared to 1% of majority group.
6 http://evbn.org/Viet Nam-info/ 7 World Bank (2016) 8 Badiani (2012) 9 Asian Development Bank: Poverty in Viet Nam. https://www.adb.org/countries/viet-nam/poverty (Accessed April 2, 2018) 10 Fujii, T. 2017. Has the Development Gap between the Ethnic Minority and Majority Groups Narrowed in Viet Nam? Evidence from Household Surveys. ADBI Working Paper 661. Tokyo: Asian Development Bank Institute. Available: https://www.adb.org/publications/development-gap-ethnic-minority-majority-groupsnarrowed-viet-nam
CHINA
LAOS
THAILAND
Hanoi
HàGiangCaoBằng
BắcKạnTuyênQuang
LàoCai
ĐiệnBiên
LaiChâu
SơnLa
YênBái
HòaBình
TháiNguyên
LạngSơn
QuảngNinh
BắcGiangPhúThọ
VĩnhPhúc
BắcNinh
HảiDương
HaiphongHưngYên
TháiBìnhHàNam
Nam ĐịnhNinhBình
ThanhHóa
NghệAn
HàTĩnh
QuảngBình
QuảngTrị
ThừaThiên–Huế
DaNang
QuảngNam
QuảngNgãi
BìnhĐịnh
PhúYên
KhánhHòa
NinhThuận
BìnhThuận
KonTum
GiaLai
ĐắkLắk
ĐắkNông
Lâm ĐồngBìnhPhước
TâyNinh
BìnhDương
ĐồngNai
BàRịa–VũngTàu
HoChiMinh
LongAn
TiềnGiang
BếnTre
TràVinh
VĩnhLong
ĐồngThápAnGiang
KiênGiang
CầnThơ
HậuGiang
SócTr ăng
BạcLiêu
CàMau
150km
100mi
©d
-map
s.co
m
Province Name# of
InterventionDistricts
# of Intervention Districts# of
InterventionCommunes
An Giang 4 An Phu, Tri Ton, Thoai Son, TinhBien
41
Dong Thap 2 Tan Hong & Hong Ngu 20
Gia Lai 2 K’Bang, and KrongPa 8
Kon Tum 2 Tu Mo Rong and Dak Ha 8
Ninh Thuan 2 Thuan Bac, Bac Ai 9
Dien Bien 4 Dien Bien Dong, Muong Cha, TuanGiao and Dien Bien
21
Lao Cai 4 Si Ma Cai, Muong Khuong, Sa Paand Bac Ha
15
122
Figure 1.1: Viet Nam - Geographic coverage of UNICEF Programme

2
WASH SECTOR CONTEXT AND EVOLUTION
The Joint Monitoring Programme (JMP)11 analysis suggests that the country has taken extraordinary steps in terms of increasing access to enhanced water supply and sanitation. Nevertheless, there are still inconsistencies in access and service quality between urban, peri-urban and rural areas12. In rural areas, access to improved water supply has increased from 50% in 1990 to 94% by 2011. Only 9% have house associations. The most widely used sources are boreholes or tube wells, protected wells and rain water collection – each representing around one quarter of improved water facilities13. Access to improved sanitation has jumped from 30% to 67% over the same time period. Levels of open defecation have seen a phenomenal reduction from 44% to only 5% by 2011. Of the improved toilets, the most common types are pour-flush and septic tank (60%), trailed by composting toilet (21%) and pit latrines with slabs (17%). Of the unimproved facilities, 66% are hanging toilets and 30% pit latrines without slabs14. Reportedly (as per Multiple Indicator Cluster Survey – MICS 2014), there are regional and ethnic disparities in terms of access to water and sanitation. The numbers suggest that the central highlands, northern mountains, and Mekong river delta regions are the most deprived with the highest numbers of open defecators and lowest access to hygienic latrines. In comparison to the national average of 5.8%, central highlands have open defecation rates of 21.9%, followed by the northern mountainous region at 12.9%. Moreover, 26.8% of ethnic minority groups defecate in the open as opposed to only 2.4% of Kinh (majority group) households. Also, the prevalent use of unimproved sanitation, such as open pit-latrines and latrines without slabs, is highest in the northern mountains at 10.7%, followed by in the central highlands at 9.4%. Similarly, 16.5% of ethnic minority households use open pit-latrines and latrines without slabs, as against 1.5% of Kinh. In the Mekong river delta region, 36.5% households use hanging latrines, relaying excreta directly into the water bodies15. In Viet Nam, limited knowledge and practices around personal and environmental hygiene are causing diseases such as diarrhoea, pneumonia and parasitic infections. Reportedly, diarrhoea and pneumonia are responsible for 10% and 12% of under-five child mortality, respectively. One-third of children’s deaths in Viet Nam are attributed to malnutrition, which in turn is linked to frequent incidences of diarrhoea and nematode infections. The MICS 2014 reported that over a quarter of under-five Vietnamese children are stunted, possibly because of diarrhoea, nematode infection and environmental enteropathy. Again, the incidence of diarrhoea is higher in areas that show lower levels of development and access to improved water and sanitation. Reportedly, the incidence of diarrhoea is reported to be as high as 14.1% in the northern mountains and 12.7% in the central highlands16. During the 1990s, approximately 2 out of 5 people in Viet Nam did not have access to improved drinking water sources. Improved sources – mostly tap water and protected wells – were easy to find in urban communities, however 80% of the populace lived in provincial territories where tap water was non-existent and protected wells and springs were rare17. Similarly, 3 out of 5 individuals did not have access to improved sanitation facilities that keep human excreta far from human contact. Moreover, 2 out of 5 individuals defecated in the country’s forests, fields and rivers. 11 JMP (2013) 12 ADB (2010) 13 General Statistics Office (2011a) 14 World Bank | Water Supply and Sanitation in Viet Nam, Turning Finance into Services for the Future, December, 2014 15 For a more detailed outline of the WASH sector see UNICEF, 2015. “WASH Outcome Paper”, developed within the 2016-2021 CCP process – including a comprehensive stakeholder overview. 16 World Health Organization (WHO), 2016. Pneumonia Fact Sheet. [webpage] Available at: http://www.who.int/mediacentre/factsheets/fs331/en/ [Accessed: 3 July 2017]. 17 WHO | Closer to bringing drinking water and sanitation to all; http://www.who.int/features/2015/viet-nam-water-sanitation/en/

3
While signing up for the MDGs, the government demonstrated resolve to see improvements in access to and quality of water and sanitation services as part of socio-economic development. A series of policy, institutional and operational measures were taken to bring improvements in the situation. Viet Nam set an example by achieving the relevant MDG targets, as it managed to provide access to improved water and sanitation to 82% and 68% people respectively. Today, 98% of Viet Nam’s more than 90-million people have access to improved drinking water sources and 78% of the population uses latrines and toilets that meet international standards18,19. As illustrated in Figure 1.2, the NCERWASS at the national level and PCERWASS at provincial level provide technical guidance, standards and policy advices to the MARD for managing the water supply services. At the operational level, the Department of Construction and Public Works is held responsible for establishing infrastructure to the point where the water supply services are transferred to the other entities for routine operations and management to keep the schemes functional. NCERWSS estimates that about 30% of all water supply schemes in Viet Nam are dysfunctional of which 14% are completely non-functional and 16% are operating with high inefficiencies due to poor operation and maintenance (O&M). O&M issues are more common in remote and mountainous areas in comparison to urban or semi-urban areas. The stakeholders are of the view that GOVN is more inclined towards investing in new water supply schemes rather than in the repair and maintenance of existing schemes due to poor tariff collection and low user fees. Moreover, the rural water supply scheme operators and communities lack technical skills and operational capacities to manage O&M, which is negatively affecting the continued operations of the schemes.
NATIONAL WATER AND SANITATION STRATEGY AND STANDARDS
Key steps taken to improve water and sanitation include the formulation of the ‘National Rural Clean Water Supply and Sanitation Strategy 2000-2020. This strategy set the basis for all the government agencies (see Figure 1.2 above) to work towards universal access to water and sanitation – a higher goal than the MDGs. Under the strategy, a three-stage National Target
18 WHO | Closer to bringing drinking water and sanitation to all; http://www.who.int/features/2015/viet-nam-water-sanitation/en/ 19 https://www.wsp.org/sites/wsp.org/files/publications/WSP-Viet Nam-WSS-Turning-Finance-into-Service-for-the-Future.pdf
RURAL SANITATION and HYGIENE PROMOTION
URBAN WATER SUPPLY
URBAN SANITATION (WASTE WATER)
RURAL WATER SUPPLY
Ministry of Agriculture and Rural Development
Ministry of Health
Ministry of Construction
Directorate of Water Resources VIHEMA
nCERWASS (for NTP3)
Provincial People’s Committee (PPC)
Department of Agriculture and Rural Development
Department of Health
Department of Construction
Health Division
CPC and Services Product
National
Provincial/ City
District
Community
Figure 1.2: Public Sector Water and Sanitation Services Institutional Apparatus in Viet Nam (overall state management)

4
Programme was executed to scale the country’s progress. Moreover, standards for ‘drinking water quantity and quality’ and ‘sanitation facilities’ were established. Post 2015, the GOVN has transitioned from ‘Sector-based Programming to ‘Integrated Rural Development Programming’. In 2008, the government of Viet Nam issued policies and regulations to all urban water companies to implement water safety designs – a proposal developed under the WHO standards and guidelines. Development partners such as WHO and UNICEF supported the government’s efforts to help implement these standards, in both urban and rural areas. UNICEF has been assisting the MARD to advocate and promote the practices of water safety – treatment and storage, where people don’t have access to improved water sources, resulting in 10% of rural households now having access to piped water. The access to improved sanitation facilities in Viet Nam has increased dramatically – from 36% in 1990 to 78% in 201520. Open defecation rates have come down from 39% to 1% over the same time period21 (however, national OD rate is reported at 4% in WHO-UNICEF 2017 JMP report22). Despite unprecedented progress, there are still pockets of deprivation (OD rate at 5% for rural and 2% for urban areas). These include minorities, people in mountain regions, central highlands and communities in the Mekong delta. An estimated 1-10% of the people in the Mekong delta region continue using hanging latrines, discharging excreta directly into lakes, streams, and river. Viet Nam, after achieving the water and sanitation-specific MDG targets, has set its sights on achieving universal access to safe water and sanitation. The country envisions achieving country-wide ODF status by 2025. And by 2030, intends to ensure access to safe drinking water to all Vietnamese. The GOVN has sought loans from the World Bank for improving rural water supply and sanitation services. With the Bank’s assistance, the GOVN is set to launch a Results-Based Scaling Up Rural Sanitation and Water Supply Programme, to be implemented in 21 under-developed provinces. UNICEF has been assisting the GOVN within the overarching UN assistance framework called ‘Common Country Programme Document’ (CCPD 2012-2016). The rural water and sanitation related assistance portfolio was part of UNICEF’s ‘Child Survival and Development Section’, aimed at strengthening the health system and services. Between 2012-16, UNICEF has implemented a Rural Sanitation and Hygiene Programme (RSHP). The Programme consists of 10 national and sub-national projects, implemented with MARD, MoH and provincial governments. RSHP is the object of this evaluation and the Programme has been elaborated below.
20 WHO | Closer to bringing drinking water and sanitation to all; http://www.who.int/features/2015/viet-nam-water-sanitation/en/ 21 WHO & UNICEF: 25 Years Progress on sanitation and drinking water – 2015 update and MDG assessment; https://data.unicef.org/wp-content/uploads/2015/12/Progress-on-Sanitation-and-Drinking-Water_234.pdf 22 WHO-UNICEF JMP: Progress on Drinking Water, Sanitation and Hygiene; Update and SDG Baselines 2017. https://www.unicef.org/publications/files/Progress_on_Drinking_Water_Sanitation_and_Hygiene_2017.pdf
Box # 02: ‘In 2014, the country made a strong commitment in the global Sanitation and Water for All partnership to eliminate open defecation by 2025. Today, Viet Nam has declared 250 villages open defecation free and many more villages are working on it,”
Mr. Lalit Patra, Team Leader of the Water Sanitation and Hygiene UNICEF Viet Nam.
Box # 01: ‘Viet Nam’s efforts over the years have been strong. Before water safety plans were applied, water quality testing was only done at the point of users and there was no way of controlling risks that could occur in the water supply system,’ Ms. Tuan Nghia Ton, National Professional Officer, WHO Viet Nam. “Today the country is following the WHO Guidelines for drinking-water quality and implementing water safety plans.”

5
RURAL SANITATION AND HYGIENE PROGRAMME (RSHP) 2012–2016 (OBJECT OF EVALUATION)
This section offers an overview of the UNICEF’s RSHP implemented through 2012-16. The description of the Programme includes sections on objectives and results, programme components, geographic coverage, beneficiaries, timelines, budget, and key stakeholders. RSHP was not a stand-alone Programme but a collection of national and sub-national multi-sector projects, where water and sanitation interventions were part of the Child Survival & Development (CSD) portfolio or section. RSHP comprised 02 national and 08 sub-national multi-sector (provincial) projects. The details of the RSHP constituent projects are as under:
1. Project 01: National project on ‘Water and Sanitation for Children’. The project was implemented through MARD (2012-2016).
2. Project 02: National project on ‘Child Survival and Development’. The WASH component of this project was implemented with VIHEMA, an arm of MoH.
3. Projects 03-10: Series of multi-sector sub-national projects i.e. eight (08) in total. These projects had a common objective and have been termed ‘Child Friendly Projects’. Water and sanitation interventions were part of the CSD component. These were implemented in Dien Bien, Lao Cai, Ninh Thuan, Gia Lai, Kon Tum, An Giang, Dong Thap provinces. The one implemented in Ho Chi Minh city, is excluded from evaluation, as this evaluation was meant to assess projects implemented for rural water and sanitation.
RSHP SIGNIFICANCE
As a middle-income country, Viet Nam mostly has to mobilize its own resources for equitable WASH service delivery; however, some soft loans like those from the World Bank are available to meet the resource gaps. With such status of the Country, UNICEF’s role in direct service delivery has diminished with the focus shifted to provide technical assistance for improving the enabling environment and enhance the capacities of the government and all other stakeholders involved in service delivery. Subject to the stated context, the RSHP Programme carries high significance for UNICEF for the following reasons:
• To make the best use of WASH programming by implementing an integrated cross-sectoral programme (RSHP is a part of Child Survival and Development Programming) and to support the objectives of stunting reduction, early childhood care and development, and cognitive development of school-age children ensuring inter-sectoral programme integration.
• To enhance government’s capacity at national level and in the targeted provinces to improve services delivery of the sustainable water supply services, household water treatment and safe storage, hand-washing with soap, open defecation free villages, sustained use of improved latrines, to deliver resilient WASH services to protect children in humanitarian settings, thereby supporting the government in its transition from MDGs to SDGs era.
• To demonstrate the effectiveness of community-based approaches (CATS/CLTS and others) to take collective action for the wellbeing of children and their families. In doing so the focus was to bring a policy shift in Government’s approach to rural sanitation.
• To support the government in introducing affordable, context relevant technologies, and strengthening the rural sanitation markets by promoting local entrepreneurs and communities.
• To collaborate with relevant ministries and other strategic partners to support the government in its planned transformation from multiple national target programmes (NTP) to a singular integrated new rural development and poverty reduction programme while leveraging the cross-sectoral linkages of WASH, Health & Nutrition, Resilience and Gender norms in programming.

6
RSHP (PROJECTS) OBJECTIVES & OUTPUTS
RSHP (2012-16) implementation coincided with the implementation of the National Targeted Programme (NTP) 3 for rural water and sanitation, implemented through 2012-15. The NTP 3 has had national outreach i.e. implemented in all 63 provinces of Viet Nam. The two (02) national projects, implemented with MARD and MoH respectively, have had a common objective. Similarly, the remaining eight (08) implemented in selected provinces have had identical objectives, which are as below:
1. Objective of Project 01-02: Strengthened national commitment, accountability and institutional capacity for scaling-up equitable and sustainable water and hygienic sanitation (WASH).
2. Objective of Project 03-10: By 2016, the most vulnerable and disadvantaged children of the province will benefit from improved public services in the areas of health & nutrition, sanitation and hygiene, early childhood & basic education and protection.
Review of the Program documents does not indicate the availability of any consolidated results framework for UNICEF’s RSHP. The RSHP comprises two national level and seven provincial projects. All these projects involve two national ministries and seven different provincial governments and therefore, a singular results framework for all constituent projects of RSHP as well as a uniform start-up timeline is not visible. The absence of a consolidated results framework either reflects the lack of prioritization of this aspect at UNICEFs’ part, or the non-applicability of consistent standards, planning guidelines and varying operational challenges at provincial level due to varied context and development priorities. The evaluators are of the view that the availability of a unified/combined results framework should have been prioritized once all 9 projects under RSHP have taken-off. The need for the availability of such a consolidated results framework is necessary to track and compare progress across all targeted regions. Please see Result Framework in Appendix 17 and also below Table 1.1 offers a consolidated summary of the planned results and targets (where available) of multiple projects that constituted RSHP23,24.
Table 1.1: RSHP Projects & Results Hierarchy
Projects Titles Results Hierarchy (Outcomes and Outputs) Objectives
Project 01: Water and Sanitation for Children Project with MARD
Strengthened national commitment, accountability and institutional capacity for scaling-up equitable and sustainable water and hygienic sanitation (WASH)
Main Results (Outputs):
SwAP/sector coordination: RWSS are well coordinated to promote harmonization and sector governance including resource mobilization with particular focus on vulnerable and ethnic minority children and their care givers.
Policy Framework: Water Quality Management Policy frameworks and appropriate technologies for water treatment are disseminated and fully operational for implementation targeting specifically vulnerable and ethnic minority children and their caregivers.
Capacity Development: National & sub ‒ national counterparts, especially
that of UNICEF focussed provinces capacity in planning, managing and
23 United Nations Children’s Fund Viet Nam (UNICEF Viet Nam), 2012. 2012-2016 Work Plan Water and Sanitation for Children Project Child Survival and Development Programme. 24 United Nations Children's Fund Viet Nam (UNICEF Viet Nam), 2012a. Viet Nam – UNICEF Country Programme of Cooperation Child Survival and Development Programme – Multi-Year Work Plan 2015-2016

7
Table 1.1: RSHP Projects & Results Hierarchy
Projects Titles Results Hierarchy (Outcomes and Outputs) Objectives
scaling up models of HTWS, the Water Safety Programme, O&M, and M&E is enhanced.
C4D (Communication for Development): C4D guidelines and strategies on key WASH behaviours and partnerships approaches are developed and disseminated at national and subnational level and fully operational with enabling participation of communities in planning, implementing and monitoring.
Monitoring and Evaluation (M&E): M&E for policy influencing and decision making is enhanced, supporting operational M&E systems and the use of data for decision making, especially in selected provinces of Dien Bien, Lao Chai, Kon Tum, Gia Lai, Ninh Thuan, An Giang, and Dong Thap
EPRP/Climate Change Adaptation: Strengthened and well-coordinated mechanism and system fully operational for emergency preparedness and response, and climate change adaptation related to WASH technical support and supervision is provided to 7 PCERWASSS for effective implementation of WASH projects in 7 UNICEF focused provinces
Project 02: CSD Project with MoH (WASH component with VIHEMA)
Strengthened national commitment, accountability and institutional capacity for scaling-up equitable and sustainable water and hygienic sanitation (WASH)
Main Results (Outputs)
By 2016, sanitation and hygiene policy frameworks on CLTS (Community Led Total Sanitation), sanitation marketing and HWWS (Handwashing with Soap) are disseminated and fully operational for implementation targeting specifically vulnerable and ethnic minority children and their caregivers living in rural setting.
By 2016, behaviour change strategies and action plan on hand washing, CLTS, social marketing and partnership approaches are disseminated and fully operational enabling participation of communities in planning, implementing and monitoring sanitation services in rural setting.
By 2016, 65% of rural households have access to hygienic latrines meeting MoH standards.
By 2016, 40% of rural population washes hands with soap after defecation, after handling children’s faeces, related to food handling and before eating.
Projects 03-10: Provincial Child Friendly Projects
Note: The provincial projects were multi-sector whereby water and sanitation interventions were part of CSD component. The projects have had common results.
Main Results:
By 2016, the most vulnerable and disadvantaged children of the province will benefit from improved public services in the area of health & nutrition, sanitation and hygiene, early childhood & basic education and protection.
The provincial projects aim to develop capacity of sub-national government authorities to tackle children’s issues in a comprehensive manner, focusing on

8
Table 1.1: RSHP Projects & Results Hierarchy
Projects Titles Results Hierarchy (Outcomes and Outputs) Objectives
the marginalized, poorest and vulnerable. It works directly with the local authorities at the provincial, district and commune levels and brings together interventions in health and nutrition, water & sanitation, education and protection to ensure that children’s issues are addressed in a holistic manner.
RSHP COMPONENTS
The projects that constitute RSHP don’t have a defined list of components, however those listed below are drawn based on literature review and discussions with relevant stakeholders. Please note that these are specific to the water and sanitation sector and include the following:
1. Enabling Environment: This component relates to both national and sub-national projects, whereby a series of interventions were planned and implemented to promote and strengthen an enabling environment by focusing on policies and plans, institutions, finances, coordination, and capacity development. The interventions primarily focused on revision/formulation of national strategies and plans, setting standards and systems, improved sector coordination, and advocacy and support to clarify mandate and operational spheres for key public-sector entities.
2. Capacity Development: This component included developing a series of training modules and delivering training to different cadres of staff and volunteers to roll-out community-based programmes. This included creating a cadre of trainers.
3. Technological Innovation & Sanitation Marketing: This component entailed interventions around improved technological options (for both water safety and latrines) and up-scaling by involving entrepreneurs and businesses. This included support to entrepreneurs to develop and market low cost water filters, low cost latrines, and SanMark manuals.
4. Behaviour Change Communication/Communication for Development (BCC/C4D): This component included interventions to enable public stakeholders to develop and implement public education and awareness campaigns for behaviour change.
5. Advocacy for Child Rights/Development: This component included research and advocacy for the promotion of child health and nutrition, early childhood & basic education, and protection (excluded from evaluation scope, as this focuses on rural water and sanitation interventions).
RSHP GEOGRAPHIC COVERAGE
The RSHP included projects that have had national and sub-national coverage. The projects 01-02, each being implemented with MARD and MoH, have had national level outreach, hence can be considered national projects. The other eight projects (03-10) have had a sub-national or provincial focus, and hence, may be called sub-national projects. These were implemented in 8 provinces including An Giang, Dong Thap, Ninh Thuan, Kun Tum, Gia Lai, Lao Cai, Dien Bien, and Ho Chi Minh city (the only urban project). The provincial projects included demonstrative or pilot implementations of concepts such as CLTS, water safety, SanMark, and others. The sub-national projects have been implemented in relatively poor and underdeveloped provinces of northern mountains and central highlands. The ethnic minorities inhabit these provinces in sizable numbers. The subnational projects were implemented in two (02) provinces each from northern mountains & Mekong Delta, and another three (03) from central highlands.
RSHP TARGET GROUPS / BENEFICIARIES
Find below the list of beneficiaries that this Programme intended to and benefited. The key beneficiaries include the public-sector entities involved in planning and delivery of WASH services. The public-sector beneficiaries include MPI, MARD, and MoH and their subsidiary entities at

9
provincial and district levels. These public entities have benefitted in varied aspects such as improved regulations, standards and plans, exposure to implementing new approaches and tools (e.g. CLTS), adoption of interactive communication approaches, and trained human resources at all levels. The RSHP benefitted private businesses and entrepreneurs by encouraging and supporting them to explore innovative and low costs technologies for water safety and hygienic sanitation. The national project for water safety extended support to an entrepreneur to develop a low-cost and locally relevant model for water treatment, which given scale-up could open more opportunities for businesses involved in supply chain. The heightened demand for latrine supplies helped local businesses. Communities comprising men, women, boys and girls, are the ultimate beneficiaries of RSHP. The communities have benefitted in terms of improved public services, improved access to water safety and hygienic sanitation, knowledge and adoption of hygiene behaviours such as hand washing with soaps, and exclusive latrine use. The projects’ indirect benefits include improved health. The documents shared do not carry details of the intended and actual community beneficiary, hence this has not been included in this commentary. RSHP has benefitted both I/NGOs and CSOs by standardising the CLTS concepts and practices, which are available for replication.
KEY STAKEHOLDERS AND ROLES
The RSHP drew support from a range of public and non-public stakeholders, who contributed to both the programme design and delivery. These included public sector entities, public/elected office holders at different levels, international development partners (UN agencies and donors), businesses, and communities. The following matrix summarizes the role and contributions of different stakeholders.
Table 1.2: Stakeholder Roles and Contribution
S# Stakeholder Nature & Level of
Engagement Roles and Contributions
1 Ministry of Agriculture and Development and Allied Departments at Provincial and District Level (MARD & DARD)
National & subnational
Lead partner for Project 01. Public / Duty bearer
MARD (including subsidiaries such as PO and DARD) is the lead public sector partner for planning and coordination of WASH sector in Viet Nam. MARD was the lead partner for Project 01 (on water safety) delivery. MARD (including PO) took lead in revision of National WASH Strategy, Co-chaired the O&M Working Group, joint water/WASH reviews (annually from 2012-15). At provincial level, the Department of Agriculture and Rural Development (DARD) has hosted Secretariat for all provincial projects and provided oversight.

10
Table 1.2: Stakeholder Roles and Contribution
S# Stakeholder Nature & Level of
Engagement Roles and Contributions
2 Ministry of Health (MoH/VIHEMA, DoH - including CHE + CPM)
National & sub-national
Lead partner for Project 02. Public / Duty bearer
The MoH and its subsidiaries (at sub-national level) have been the key partner for roll-out of rural sanitation and BCC (C4D) campaigns. The Viet Nam Health and Environment Management Agency (VIHEMA) of MoH was lead implementing partner for Project 02 on rural sanitation. The key tasks or contributions include training delivery for CLTS, manual or guidelines on low cost latrines and SanMark, and developing Provincial ODF Plans. At provincial level the DoH has been one of the lead implementers of provincial projects. The contributions have come from Provincial Centres for Preventative Medicine (CPM) who supported facilitators’ trainings, field level roll-out of rural sanitation, and design/rollout of BCC/C4D campaigns (undertaken by Community Health Education CHE Units). In total, 900 facilitators (for CLTS roll-out) have been trained.
3 Ministry of Planning and Investment (MPI)
National & sub-national
Coordinating agency for all projects. Public / Duty bearer
The MPI, both at national and particularly at sub-national level, has been involved with coordination and oversight functions. At provincial level MPI has been part of the multi-stakeholder’s oversight body referred to as Provincial Project Management Units.
4 Provincial/District Peoples Committee & Commune Head
Sub-national/Provincial Public / Representative forums
At the provincial level, the provincial’s people’s committees (PPP) were the lead entity that approved or signed off the projects. The PPP remained involved with planning, oversights, and arranging support wherever required to get projects delivered. The projects received support from district committees and Head of Commune also. The Head of Commune remained involved in roll-out of BCC and CLTS activities
5 UNICEF International/national Development partner Technical and financial support
UNICEF Viet Nam, as a development partner has contributed both technically and financially to RSHP. Support has been extended to public sector partners and entrepreneurs to accelerate services delivery, improve coordination, and businesses to offer low-cost and innovative technological solutions. UNICEF support has focused on strengthening enabling environment, improve coordination, and build capacities at all levels to enable public entities (and partly businesses) to help improve achieve access to safe water and hygienic sanitation. Financial assistance has been provided to both public entities at national and sub-national level including an entrepreneur.

11
Table 1.2: Stakeholder Roles and Contribution
S# Stakeholder Nature & Level of
Engagement Roles and Contributions
6 Viet Nam Bank of Social Policy
National Public/Duty bearer
Microfinance Bank
The Viet Nam Bank of Social Policy, though not directly involved, played a role in providing loans for rehabilitation of water supply schemes, and building/upgrading latrines. The focus was to enable poor to access services. The projects however did not reach out to VBSP for specialised products for absolute poor.
7 World Health Organization
International/national Development partner
The WHO worked in collaboration with UNICEF to help review/develop ‘Water Quality Standards’ and advocated with UNICEF for adoption of more realistic water quality standards and procedures with MoH.
8 Communities Local
Participants/beneficiaries and right holders
The communities participated in the programme as ultimate beneficiaries. They contributed to the programme results by taking on the costs for latrine construction/upgradation.
9 Entrepreneur/Businesses
National & local Business
The entrepreneur and businesses were engaged in the projects to work on producing low cost and innovative technologies for water safety and hygiene sanitation. An entrepreneur was supported to produce low cost local water filter. The entrepreneurs and businesses benefitted from increased sales.
10 Plan International & Other NGOs (Child Funds)
International & National Development partners
The INGOs like Plan and CF are implementing WASH interventions and contributed in scaling the CLTS implementation.
THEORY OF CHANGE (TOC)
A ‘theory of change’ (TOC) explains how activities are understood to produce a series of results that contribute to achieving the final intended impacts. It can be developed for any level of intervention – an event, a project, a programme, a policy, a strategy or an organization.25 The projects that form RSHP have been implemented without any documented TOC. The evaluators, as part of the evaluation, developed two ex-post TOCs separately for rural water and rural sanitation projects. The first TOC is for rural sanitation projects implemented with MoH/VIHEMA (including WASH components from provincial projects) and second is for rural water safety project with MARD. The Evaluators may want to underline also that when RSHP projects were initially conceived, the practice of developing of TOCs was not much common within UNICEF Offices. The Evaluators developed the ex-post TOCs based on literature review and discussions with UNICEF team. The drafts were shared as part of Inception Report for inputs and finalisation. The Evaluators made efforts to develop TOCs which are complete in all respects so that could be used for the evaluation. The linkages or pathways of change are clearly established; and where
25 United Nations Children’s Fund (UNICEF), 2014b. Supplementary Program Note on the Theory of Change for the UNICEF Strategic Plan, 2014 -2017. [.pdf, online] Available at: https://www.unicef.org/strategicplan/files/2014-CRP_14-Theory_of_Change-7May14-EN.pdf [Accessed: 7 August 2017].

12
needed, across project components or intervention areas. The result indicators comply with the prescribed SMART criteria i.e. specific, measurable, accurate, realistic and time-bound; and are coherent with the established WASH sector indicators. The working assumptions or conditions for change have also been included in the TOCs. As part of evaluation planning, the two TOCs were assessed for established evaluability assessment criteria i.e. plausibility, utility, and feasibility. The TOCs were found plausible for clarity of results and defined linkages between and across results hierarchy, activities and strategies. Moreover, the TOC was used to identify data required, availability of national data/information, and possibility to collect primary data for missing indicators. The stakeholders’ views were found to be coherent and there was an all-round commitment to contribute to the evaluation. The key stakeholders were found to have shared understanding and intent in terms of objectives of the evaluation and key evaluation questions.
Evaluation Hypothesis
The Evaluators framed one hypothesis for all the projects while keeping in view the interventions and anticipated results for rural water safety, sanitation and hygiene practices.
‘The UNICEF projects (national and sub-national) resulted in accelerating access to improved water sources, hygienic latrines (as per GOVN approved standards) and practice of
handwashing with soap in project (rural) areas where 07 sub-national projects were implemented (from 2012-16)’.
This hypothesis focused on three dependent variables i.e. access to improved water, access to hygienic latrines, and practice of handwashing with soap. The indicators have been assessed based on proxy indicators of availability of handwashing stations and soap in households. To address the information gaps, the national rural averages in 2011 are used (form MICS and JMP) as baseline and compared with national averages in 2014 and beyond. The results of Post-KAP HHS have also been used for longitudinal analysis.

13
Figure 2.1: TOC 01 - Rural Sanitation Projects with MoH/VIHEMA and Provincial Projects
MoH
: The
ory
of C
hang
e 20
12-2
016
Out
com
eW
ASH C
P (In
term
edia
te)
Out
puts
Key
Activ
ities
Impact
OP Outcome 2.2: By 2016, increased quality and effective management of a comprehensive national health system, including health promotion and health protection with a focus on ensuring more equitable access for the most vulnerable and disadvantaged groups OP Outcome 3.3: By 2016, improved performance of the public sector institutions at national /subnational level, trough enhance coordination, accountability transparency and anti corruption efforts, will reduce disparities nd ensure access to public services for the most vulnerable and disadvantaged groups
MDG GOAL 7: Half the proportion of people without access to safe drinking water and basic sanitation
OP Output 2.2.5: National and sub – national capacities enhanced to improve evidence and the equitable access to and demand for quality und sustainable water supply and hygienic sanitation
OP Output 2.2.1: Policy advise and technical support provided to strengthen the building blocks of human and animal health systems, including information systems and the generation of evidence, at national and sub – national level
Strengthened national commitment, accountability and institutional capacity for scaling-up equitable and sustainable water and hygienic sanitation WASH (Intermediate Result = IR)Main Project Objective: Increased quality and effective management of a comprehensive national health system, including health promotion and health protection with a focus on ensuring more equitable access for the most vulnerable and disadvantaged groupsObjective 4 (Hygienic sanitation): By 2016, identified beneficiaries benefit equitably from increased access to sustainable and hygienic sanitation.(WP Milestones)1. By 2016, sanitation and hygiene policy frameworks on CLTS, sanitation marketing and HWWS are disseminated and fully operational for implementation targeting specifically
vulnerable and ethnic minority children and their caregivers living in rural setting.2. By 2016, behavior change strategies and action plan on hand washing, CLTS, social marketing and partnership approaches are disseminated and fully operational enabling
participation of communities in planning, implementing and monitoring sanitation services in rural setting.3. By 2016, 65% of rural households have access to hygienic latrines meeting MOH standards.4. By 2016, 40% of rural population washes hands with soap after defecation, after handling children’s faeces, related to food handling and before eating.
Realizing the rights of every child, especially the most disadvantaged.
• Develop WASH related policy options and guidelines to benefit the un-reached and ethnic minority children.• Conduct research and studies of differences of impacts of poor WASH and good WASH on children.• Support for continuation of improving implementation of WASH Sector assessment and using its data for decision making.• Support in design and implement the National Communication Action Plan under the RWSS NTP III via introduction of C4D initiatives to promote social mobilization, behavior and
social change in hygiene and sanitation.• Support capacity development for better planning, implementing and managing WASH C4D strategies focusing on sanitation including CLTS and sanitation marketing, and
dissemination and education on relevant policies and legal document in hygienic sanitation.• Coordinate with NCERWAHS to implement the rural water and hygienic sanitation. program• Support for better coordination between interested donors and related government agencies for more effective supports for sanitation.
20151. The post 2015 sanitation program, plan, strategy and budgeting developed addressing the equity
issues and submitted for approval by the National Assembly that will benefit children and women in the most disadvantaged areas with low level sanitation coverage
2. Oriented decision makers and managers in the northern mountains and central highlands provinces prepared to take up Scaling up Sanitation initiative
3. Improved policy environment to support scaling up sanitation including issuance of simplified ODF verification /certification guidelines and effective WASH in schools implementation procedure
20161. Improved inst. capacity in 25 provinces to introduce CATS for province wide sanitation promotion
with oriented managers /decision makers2. System's/procedures to scale up sanitation with ODF verification /certification procedures in
place in under developed provinces3. At least 50% of CASTS intervention villages declared ODF villages, contributing to the GoV target
of ODF by 20125
20141. One Directive for ODF Viet
Nam by 2010 from Prime Ministers Office and national guidelines on Sanitation Marketing, which targets specifically vulnerable and ethnic minority children and their caregivers living in remote areas drafted and presented to MOH
2012-20131. National guideline on CLTS
and Sanitation Marketing drafted and pretested (MoH)
Bott
lene
cks
Inadequate policy directive and guidance for sustainable WASH
Wide cultural acceptability of ‘open defecation’
Adherence to low quality latrines, water treatment and storage
Inadequate arrangements for financing household sanitation and water
Low affordability among lowest quintile population for sanitation and water-filtration
Limited program supplies for affordable sanitation and drinking water safety
Unregulated private sector– quality standard, tariff setting,
Poor alignment between ‘capital’ and ‘recurring' budget.
Improper use of resource – mostly used for ‘refurbishment’ water services and spending on ‘expensive options’
WASH sector receives low priority with poor budget and investments incl. for ‘soft’ interventions.
Weak institutional capacity for: demand creation, supply chain strengthening, collaboration with private sector
Poor commitment and coordination – SEDP yet to include sanitation as an indicator
Key
Stra
tegi
es
• Capacity development• Evidence generation and evidence-based policy dialogue and advocacy• Partnerships• South-South and triangular cooperation
• Identification and promotion of innovation• Support to integration and cross-sectoral linkages• Service delivery
WASH Key Indicators (WP MoH, Provinces)2012-131. Availability and dissemination of National Guideline on CLTS
and Sanitation Marketing20141. Approval by MoH of updated policy documents on sanitation
and hygiene incorporating the latest approach and techniques on CLTS, sanitation marketing and HWWS that target specifically vulnerable and ethnic minority children and their caregivers living in rural areas
2. # of national counterparts trained on sanitation planning2014-20151. % of CATS intervention villages certified ODF2. # of villages certified ODF (no direct implementation support)
Province: (e.g. Ninh Thuan)2012-20131. % increase of latrine and handwashing coverage2. # district implemented CLTS, HWWS, sanitation marketing2014# of communities that have scaled up sanitation marketing, HWWS, HWTS2015-2016 (no specific indicators listed)(based on Outputs)1. Lessons from ODF villages documented for influencing
provincial budgeting and investment2. ODF villages in non project areas replicated by local budgets on
the basis of successful evidence of UNICEF demonstration model
3. Provincial WASH sustainability compact 2016 – 2020 approved by DARD and DoH and applied in Province
4. UNICEF HWTS demonstration model documented and used for leveraging local government budgets
Cross cutting Provinces (2012-2016): 1. Availability of provincial plan on natural disaster preparedness,
response and mitigation (%)2. Availability and implementation of provincial C4D action plan
for low cost high impact behavioral interventions for nutrition, Maternal and child health, water, hygiene and sanitation practices implemented (%)
3. Availability of inter sectoral monitoring (WASH, Nutrition, MNCH) (%)
WASH Key Indicators (MoH Project Document)% of rural population with hygienic latrines meeting MoH standards% of people in project supported areas especially mothers and children practice hand washing with soap
Key Risk and Assumptions (CCPD):1. Cont. and strengthened support for One UN by all agencies
and by GoVN2. Availability of funding (ODA, private sector)3. Retention and recruitment of staff with adequate expertise
and experience level4. Balance between critical monitoring child rights in evolving
socio – political context and solid partnership with and program support to GoVN

14
Figure 2.2: TOC 02 - Rural Water Safety Project with MARD.
MAR
D: T
heor
y of
Cha
nge
2012
-201
6
20151. Framework for sustainable O&M of water systems and action plan to support
underdeveloped provinces on sustainable O&M management of water and sanitation systems developed for community systems, health care centers and schools
2. A guideline on PPP on household water treatment and storage (HWTS) promotion developed
3. Improved knowledge/skills for relevant stakeholders regarding the application of effective behavior promotion approaches to HTTS and HWWS promotion in UNICEF focus provinces
4. An Interagency Contingency Plan on WASH for emergencies endorsed by Cluster members, and example community based plan on CC adaptation, and DRR
20161. At least 7 underdeveloped provinces implement sustainable approaches to school WASH
services with support from national level2. PPP of ceramic and other cost effective filters expanded to two more UNICEF focus
provinces by counterparts3. Improved effectiveness of C4D interventions in promoting desired WASH behavior
among poor and disadvantaged group of population4. Community resilient capacity and adaptation ability to emergencies and climate change
is increased in selected communes of UNICEF focus Provinces
20141. One Prime Ministers Directive on ODF Viet Nam by 2025 is issued2. Meetings to present convincing reason why provincial authorities
should invest more in Sanitation and Hygiene conducted to at least 3 provinces by MoH, So, UNICEF – link to MoH WP
3. Provincial implementation plan for promotion of HWTS and HWWS for at least 7 focused provinces produced for implementation
4. One model of marketing for HWTS and HWWS for Mountainous Areas developed and tested
5. Four provinces have DRR/CCA Plan of Action submitted to PPC for approval and two of them have started its implementation
20121. Guidelines/Circular supporting water quality for the disadvantaged
group of population finalized and submitted for approval2. Art least 80 staff of all provincial PCERWASS , priority 7 PCFP have
attended trainings on HWTS and are efficiently developing, implementing, and monitoring HWTS in their provinces
3. The communication initiative using WASH Good Will Ambassador is disseminated, revised and implemented
4. Institutional capacity assessment report on C4D for WASH sector completed and disseminated to interesting partners
20131. A model of effective WASH Communication to be replicated
nationwide is developed2. Institutional Capacity Plan developed , and key counterparts
trained in WASH communication and monitoring of provincial C4D3. At least 160 staff of all provincial PCERWASS, priority 7 PCFP have
attended trainings in HWTS and WSP, are efficiently implementing HWTS in their selected districts and discuss/prepare for up scaling of HWTS to other 4 provinces
Strengthened national commitment, accountability and institutional capacity for scaling-up equitable and sustainable water and hygienic sanitation WASH (Intermediate Result = IR) * different WP Milestones per planning time frame1. SwAP/sector coordination: RWSS are well coordinated to promote harmonization and sector governance including resource mobilization with particular focus on vulnerable and ethnic minority
children and their care givers2. Policy Framework: Water Quality Management Policy frameworks and appropriate technologies for water treatment are disseminated and fully operational for implementation targeting
specifically vulnerable and ethnic minority children and their caregivers3. Capacity Development: National & sub – national counterparts, especially that of UNICEF focussed provinces capacity in planning, managing and scaling up models of HTWS, WSP, O&M, and
M&E is enhanced4. C4D: C4D guidelines and strategies on key WASH behaviours and partnerships approaches are developed and disseminated at national ad subnational level and fully operational with enabling
participation of communities in planning, implementing and monitoring5. M&E: M&E for policy influencing and decision making is enhanced, Supporting operational M&E systems and the use of data for decision making, especially in selected provinces of Dien Bien,
Lao Chai, Kon Tum, Gia Lai, Ninh Thuan, An Giang, and Dong Thap6. EPRP/Climate Change Adaptation: Strengthened and well coordinated mechanism and system fully operational for emergency preparedness and response, and climate change adaptation related
to WASH technical support and supervision is provided to 7 PCERWASSS for effective implementation of WASH projects in 7 UNICEF focussed provinces
Out
com
e OP Outcome 2.2: By 2016, increased quality and effective management of a comprehensive national health system, including health promotion and health protection with a focus on ensuring more equitable access for the most vulnerable and disadvantaged groups OP Outcome 3.3: By 2016, improved performance of the public sector institutions at national /subnational level, trough enhance coordination, accountability transparency and anti corruption efforts, will reduce disparities nd ensure access to public services for the most vulnerable and disadvantaged groups
MDG GOAL 7: Half the proportion of people without access to safe drinking water and basic sanitation
OP Output 2.2.5: National and sub – national capacities enhanced to improve evidence and the equitable access to and demand for quality und sustainable water supply and hygienic sanitation
OP Output 2.2.1: Policy advise and technical support provided to strengthen the building blocks of human and animal health systems, including information systems and the generation of evidence, at national and sub – national level
WAS
H C
P (In
term
edia
te)
Out
puts
Impact Realizing the rights of every child, especially the most disadvantaged.
Bott
lene
cks
Inadequate policy directive and guidance for sustainable WASH
Wide cultural acceptability of ‘open defecation’
Adherence to low quality latrines, water treatment and storage
Inadequate arrangements for financing household sanitation and water
Low affordability among lowest quintile population for sanitation and water-filtration
Limited program supplies for affordable sanitation and drinking water safety
Unregulated private sector– quality standard, tariff setting,
Poor alignment between ‘capital’ and ‘recurring' budget.
Improper use of resource – mostly used for ‘refurbishment’ water services and spending on ‘expensive options’
WASH sector receives low priority with poor budget and investments incl. for ‘soft’ interventions.
Weak institutional capacity for: demand creation, supply chain strengthening, collaboration with private sector
Poor commitment and coordination – SEDP yet to include sanitation as an indicator
Key
Stra
tegi
es
• Capacity development• Evidence generation and evidence-based policy dialogue and advocacy• Partnerships• South-South and triangular cooperation
• Identification and promotion of innovation• Support to integration and cross-sectoral linkages• Service delivery
2014 (WP)Activity 1: Support policy dialogue, knowledge networking and coordination trough Sanitation Working Group through RWSS Partnership Office Activity 2: Work with UNICEF Good Will Ambassador for the promotion of personal hygiene, sanitation, and HH water quality management during Global Hand Washing Campaign, trough Mass Media and field campaignsActivity 3: Develop provincial implementation plans for the promotion of HWTS, HWWS based on national plans and formative researchActivity 4: Support capacity development towards implementation of provincial plans on HWTS promotion, incl. behavioural change communication and M&E system developmentActivity 5: Provide a critical analysis incl. WASH BAT, develop set of criteria for measurement of sustainability and reliability of WASH servicesActivity 6: Develop concept note with vision and strategy for promotion of PPP in HWTS based on 7 focussed provincial SitAnsActivity 7: Support follow up actions for improvement of M&E systemsActivity 8: Support finalization and approval of DRR/CCA plans and facilitate provincial budget allocation to focus provincesActivity 9: Support development of DRM/CCA plan to selected provincesActivity 10: WASH Cluster prep. measures Activity 11: Support development of new creative approaches to promote healthy actions (HWT, HWWS) based on formative research findings, and pretestingActivity 12: Support development of community and institutional M&E Plans with focus provinces, include in C4D plan
2015-16 (WP)Activity 1: Promote sustainable and effective community based O&M water and sanitation systems in under developed 25 provinces incl. UNICEF focus provinces Activity 2: Promote PPP in production, marketing and use of HWT, HWWS in remote areasActivity 3: Promote production and use of low cost options for HWTS, sanitation and handwashingActivity 4: Develop rural water action plan for post 2015 period and supportive monitoring systemsActivity 5: Support coordination and review of sector progress and plan for sustainable water supply and water safety and sanitation promotionImprove local capacity of DRR/CCA in WASH in rural areas
2012-13 (WP)1. Policy advocacy and adviseTechnical and financial support guideline drafting to promote equitable access to improved water and sanitation2. Capacity development and systems strengtheningTechnically and financially support training manual guidelines, institutional TOT courses/workshops (WSP, HWTS) Strengthen capacity of of central and local WASH counterparts on planning, risk management, response related to WASH emergencies, climate change3. Knowledge generationGeneration of studies: Children's vulnerability to CC and disaster, impact of WASH on education, C4D capacity assessmentSupport sanitation working groupTechnical and financial support to strengthen evidence based monitoring of implementation of NTP3 (workshop, M&E software design, monitoring trips to focus districts)4. Emergency Preparedness / climate changeSupport implementation of WASH emergency preparedness, response and CC adaptation plans5. C4DTechnical and financial support to communication campaignsInstitutionalize capacity building on C4D planning, implementation, M&ETechnical and financial support to national level counterparts to monitor C4D activities, international and national study visits, WASH models in other countries
Prog
ram
Key
Act
iviti
es
WASH Key Indicators (WP MARD)2015-2016No specific monitoring indicators developed20141. New national guidelines on sanitation
marketing, hygiene are developed and disseminated to Provinces
2. # of provincial budgets and operational plans for sanitation/hygiene promotion that are in accordance with national guidelines and with equity focus
3. Availability of provincial implementation plan for HWTS and HWWS for mountainous areas
4. DRR and CC framework and action plan available for implementation
5. Implementation of WASH behavior change action plans
2012-20131. Availability of final/draft guideline/circular
supporting water quality for disadvantaged groups of population, spec. Women and children
2. # of provincial PCERWASS staff of all provinces who have adequate knowledge and skills related to HWTS, WSP
3. Development and implementation of WASH communication in partnership with international and national organizations
4. Availability and dissemination of C4D capacity building plan for national and subnational counterparts to implement Communication Action Plan, NTP3
Key Risk and Assumptions (CCPD):1. Cont. and strengthened support for One UN
by all agencies and by GoVN2. Availability of funding (ODA, private sector)3. Retention and recruitment of staff with
adequate expertise and experience level4. Balance between critical monitoring child
rights in evolving socio – political context and solid partnership with and program support to GoVN

15
2 EVALUATION PURPOSE, SCOPE AND METHODOLOGY This section comprises two distinct parts, whereby the first part describes the evaluation purpose, objectives, and significance, audiences, uses and dissemination, criteria and key questions, and scope and coverage. The second part explains evaluation design, methodology, data consolidation and processing. It also includes a discussion on quality assurance and ethical safeguards, limitations and mitigation measures, evaluation approach in terms of key stages and tasks, and evaluation management.
EVALUATION PURPOSE
This is a ‘Summative-Formative’ evaluation. The evaluation has been commissioned to ‘generate evidence of success of RSHP (2012-16), document learning to inform UNICEF-GOVN upcoming cooperation programme’26, and for accountability purpose.
OBJECTIVES
There are multiple evaluation objectives as given below: To provide evidence of success or otherwise to UNICEF and UNICEF partners for
assistance extended under RSHP at national and sub-national levels. To inform and enable management decision-making as to the continuity and design of the
future UNICEF WASH programme i.e. 2017-21, while aligning it to UNICEF’s global priorities and strategies.
To contribute to the regional and global discourse and discussions by sharing learning and questions on accelerated access to improved sanitation, addressing open defecation, sector coordination, and sustainable hygiene behavioural change;
To assess the extent of slippage (reversal to open defecation in ODF certified villages) and social norm creation for exclusive latrine use (behaviour) to inform its inclusion into future rural sanitation programming in Viet Nam.
The Evaluators were requested (towards the end of field work) to appraise if there is any connection between WASH and child malnutrition in Viet Nam with a purpose to generate secondary sources-based evidence of the nexus between WASH and nutrition. Also, to explore if UNICEF work has made any contributions to addressing the child malnutrition problem in RSHP operational provinces. The Evaluators informed the country management that it is too late to address this in the evaluation design and also for the fact that malnutrition assessment requires different methodological framework. Nevertheless, the Evaluators did conditionally agree to look into the secondary data, and given availability of usable data/information, add commentary on WASH-Malnutrition and UNICEF contributions.
EVALUATION’S SIGNIFICANCE
The evaluation holds significance for both UNICEF as well as GOVN for varied reasons. First and foremost, this is the first and only review or evaluation commissioned for RSHP 2012-16. Also, this was the first systematic and independent assessment to determine how and to what extent UNICEF assistance under RSHP has contributed to enable the government in strengthening services around rural water safety and rural sanitation in Viet Nam. This shall facilitate establishing what value UNICEF assistance has added to the delivery of services. The evaluation is important as it contributes to establishing and auguring UNICEF’s commitment to accountability to its partners, donors, and communities. The evaluation is significant for systematically assessing the extent of slippage (in ODF certified villages) over time. Furthermore, it is the first study that looked in to the creation of social norms (for exclusive latrine use) in ODF certified villages.
26 United Nations Children’s Fund (UNICEF), 2017. Statement of Work and Terms of Reference – Evaluation of UNCEF Viet Nam’s Rural Sanitation and Hygiene Programming 2012-2016.

16
The evaluation is important as it informs the continuity, scope and shape of future UNICEF assistance and engagement with the GOVN for the WASH (including CLTS approach) sector. It is likely to add to the body of knowledge available to help share future discourse around concepts and practices for accelerated and improved rural water safety and sanitation services, both nationally and internationally.
EVALUATION AUDIENCE, UTILIZATION, AND DISSEMINATION
Table 2.1: Evaluation Audience and Utilization
Evaluation Audience Utilization and Interest/use
Primary Audience
UNICEF Viet Nam Country Office and Regional Office for East Asia and Pacific Region (EAPRO)
For UNICEF, the evaluation is expected to give an independent view of successes, challenges, gaps, and learning by also contributing to accountability and learning. The evaluation shall be used to demonstrate the ‘value addition’ of UNICEF assistance to rural water safety and sanitation. Moreover, the evaluation shall inform the continuity of UNICEF-GOVN engagement and scope and scale of UNICEF WASH assistance 2017-21. The UNICEF-GOVN Country Program Document (CPD 2017-21) is framed and adopted already, however the evaluation findings are likely to be used for necessary revisions. The evaluation may also contribute to setting baseline (for critical WASH performance indicators) and enable monitoring of the future UNICEF-GOVN CCP 2017-21. The evaluation learning will be shared regionally and globally within UNICEF Regional and Country Offices, to inform future WASH programming.
Ministry of Agriculture and Rural Development, Ministry of Health, and Ministry of Planning and Investment
For primary audiences within the GOVN (MARD, MoH and MPI), the evaluation is expected to generate evidence of how far the government-led rural water and sanitation efforts are contributing towards access to clean water and hygienic latrines. Moreover, it is to offer insights into the efficacy of different approaches and models. Furthermore, the findings and recommendations are to be used for adapting the approaches and models to the local context, including looking into possible replication, and up scaling. The public stakeholders could possibly use the evaluation to re-assess planning and resource allocation decisions to achieve ODF and provision of safe water targets i.e. country-wide ODF by 2025 and universal safe water access by 2030.
Secondary Audience
Ministry of Finance, Ministry of Labour, Invalids and Social Affairs (MOLISA), Viet Nam Bank of Social Policy (VBSP) and World Bank
The interests and potential uses by secondary stakeholders are varied. For the World Bank, the evaluation is to inform the planning and implementation of upcoming WB-GOVN programming. For VBSP, the evaluation could potentially trigger thinking and product development for reaching out to ‘most poor’. For INGOs and donors, the evaluation may inform programming and funding decisions.
The evaluation dissemination includes a planned session/presentation to the Evaluation Reference Group (ERG) once the report is finalized. The report shall then be distributed to other stakeholders and placed on UNCIEF’s Evaluation Database, an online portal where all evaluations are placed for easier and wider access.
EVALUATION CRITERIA AND KEY QUESTIONS
The evaluation followed the criteria given in the evaluation TORs. The listed criteria relate to standard OECD-DAC (Organisation for Economic Cooperation and Development-Development Assistance Committee) criteria except (excluding) impact. The evaluation focuses on four (out of five as given in OECD-DAC) criteria including relevance, effectiveness, efficiency, and

17
sustainability/scalability. The impact criterion was excluded as the programme had recently been concluded and not yet ready for impact assessment. The evaluation includes multiple non-OECD-DAC criteria (often referred to as cross-cutting) comprising equity, gender, resilience, and Human Rights Based Approach (HRBA) to Programming. During the inception phase, evaluation questions as given in the TORs were reviewed and revised to formulate the Evaluation Matrix (refer Appendix 2 attached). The evaluation matrix was also reviewed and finalized together with the UNICEF team. The re-framing of the evaluation questions helped achieve clarity and focus, while keeping expectations more realistic and manageable. Below is the list of key evaluation questions under OECD-DAC and Non-OECD-DAC criteria.
Table 2.2: Evaluation Criteria and Corresponding Evaluation Questions
Question Number
Key Questions
OECD-DAC Evaluation Criteria: Relevance
EQ-1
To what extent has UNICEFs rural water, sanitation and hygiene programme (RSHP) been relevant (to context/beneficiaries needs, existing capacities, national priorities and the work of other sector partners) for improving rural water supply (access and quality), hygienic sanitation and personal hygiene i.e. handwashing with soap?
OECD - DAC Evaluation Criteria: Effectiveness
EQ-2
To what extent has UNICEF technical assistance effectively contributed to creating an enabling WASH Governance environment (policies, strategies, national M&E systems and Stakeholder coordination) for rural water supply, hygienic sanitation, and handwashing with soap?
EQ-3 To what extent has UNICEF strengthened the public-sector lead delivery and contributed to knowledge, attitudes and practices improvements around key water safety, latrine use and hygiene behaviours e.g. handwashing with soap?
OECD - DAC Evaluation Criteria: Efficiency
EQ-4 To what extent the level of achievements (outputs and outcomes) justify the financial and human resources used?
OECD - DAC Evaluation Criteria: Sustainability
EQ-5 To what extent are the ODF status and the associated social norm as well as hand washing practices likely to sustain?
Non-DAC Evaluation Criteria: Equity, Gender, Resilience and HRBA
EQ-6
What key approaches and strategies were adopted to enable RSHP projects and interventions priorities/integrate the needs of the vulnerable and marginalized groups (poor, remote communities, ethnic minorities, women, children, poor, elderly, people with disabilities) and results achieved?
Evaluation Scope and Coverage
The evaluation covers all rural water and sanitation activities planned and implemented as part of projects that constitute RSHP. The evaluation covers the complete RSHP implementation period i.e. 2012-16. The evaluation scope includes a total of nine (09) projects implemented at national and sub-national levels. These include two (02) national projects, one each implemented for rural water safety (with MARD) and rural sanitation (with MoH/VIHEMA). The sub-national projects include

18
seven (07) ‘Provincial Child Friendly Projects’ implemented in seven provinces namely Dien Bien, Lao Cai, Kon Tum, Gia Lai, Ninh Thuan, An Giang, and Dong Thap. The provincial projects, being rurally focused, excluded the one implemented in Ho Chi Minh City - the only urban project implemented under RSHP. The provincial projects were multi-sector, however the evaluation covered only the rural water and sanitation interventions, implemented as part of CSD portfolio. For the evaluation, data was collected in Ha Noi (capital), and three (03) districts in Dong Thap, Lao Cai, and Ninh Thuan provinces (one district per province per region) following sampling frame (see Appendix 3 for rationale and selection strategy) drawn in consensus with evaluation management team. The evaluation scope included mapping the extent of slippage (in ODF certified communities), which has been done for ODF certified communities. Similarly, the social norms analysis has been undertaken for only one behaviour i.e. exclusive latrine use by all family members in ODF certified communities. The social norms assessment excludes Handwashing with Soap (HWWS). The evaluation design did not include any rigorous analysis to establish connect between rural WASH and child malnutrition. The commentary in the report is drawn from the secondary sources only.
EVALUATION DESIGN, METHODOLOGY, APPROACH AND LIMITATIONS
Evaluation Framework and Conceptual Design
The Evaluators reviewed multiple evaluation/research designs to plan and implement a responsive (to the evaluation objectives) and robust evaluation. The focus remained on Non-experimental designs, for this being a ‘Summative-Formative’ rather an ‘Impact’ evaluation. Some of the designs looked into details and include: ‘Case Study’27, ‘Causal’28, and ‘Descriptive’29. The evaluation has used an overarching ‘Theory Based’ evaluation approach to undertake the evaluation. This approach is prescribed for evaluations where a pre-defined ‘Theory of Change (ToC)’ is available. Moreover, it comes with inherent advantage that it could be applied with any of the evaluation design available i.e. non-experimental and experimental. In theory-based approach, the causal pathways of ToC from inputs to highest level results e.g. outcomes and impact, are assessed to establish plausibility of programme or project’s design. The theory-based approach enables ascertaining programme or project’s ‘Contribution’ in realising ‘observed’ or ‘perceived’ change towards mostly outcomes and impact. The evaluator evolved and applied a ‘Hybrid Evaluation Design’ comprising partly of ‘Descriptive’ and ‘Social Norms Theory’ designs. The descriptive design has been used to establish and rationalise the intended outcome level changes in the TOC, whereas the social norms theory design helped to ascertain the extent to which programme interventions worked in creating social norm of latrine use. Theoretically, a ‘Descriptive’ research/evaluation design seeks to answer the ‘who, what, when, where, and how’ associated with a particular research problem. The design is prescribed to obtain information concerning the current status of the phenomena and to describe “what exists” with respect to variables or conditions in a situation. Out of different sub-designs options available within the larger frame of ‘Descriptive’ designs, this evaluation used ‘Before and After’ sub-design. This was preferred over others to establish programme’s ‘causality’ and ‘contributions’ in accelerated access to improved water, improved sanitation, and handwashing
27 A case-study is a top to bottom research design to answer a specific research issue as opposed to a comprehensive statistical survey. This kind of research design is utilized to constrain a comprehensive field of research into one or few easily researchable cases. 28 Causal research or explanatory research and it is conducted to identify the degree and nature of cause-and-effect relationships e.g. if X, then Y. Causal research can be conducted while keeping in mind the outcome to evaluate impact of a particular changes on existing standards, different procedures and so on. 29 Descriptive research design gives a precise depiction of record of characteristics of a specific individual, group or situation; these studies are a method of finding meaning, portraying what exists, defining the incidence with which something happens and/or categorizing information.

19
with soap. Moreover, the assumption/justification was that for such standard indicators, secondary data is/shall be available (including provincially desegregated) to draw longitudinal analysis (from 2011 to 2016/17) for key outcome level indicators. For social norms assessment, the principles and analytical framework of ‘Social Norms Theory’ has been applied. The design is used to measure the existence and/or strength of social norms for particular behaviours or practices in community under observation30. A cross-sectional survey was planned and implemented in ODF certified communities (21 communities in three provinces) to gather relevant primary information on different dimensions of social norms such as beliefs, expectations, sanctions, and others. These elements were then assessed and correlated to form an opinion on extent of slippage and existence/strength of social norm i.e. exclusive latrine use.
EVALUATION METHODS
The evaluation has employed ‘Mixed Method’ and ‘Participatory’ approaches to plan and implement this evaluation. Both qualitative and quantitative methods were applied to gather requisite information and undertake analysis to adequately respond to the evaluation questions. The mixed method approach has facilitated the leveraging of the strengths and complementarities of different social research methods, and parallel application helped in overcoming the method specific limitations. Moreover, the evaluation draws on extensive literature or secondary sources review. The evaluation applied the principle of ‘participation’, whereby all key stakeholders (national, sub-national, field, and communities) were reached out to for their experiences, views, and suggestions. A participatory evaluation management approach was followed, whereby an Evaluation Reference Group (ERG) was formed (comprising both UNICEF and public stakeholders). The ERG functioned as an oversight body to supervise the entire evaluation processes and outcomes that included quality assurance of evaluation design, methods, tools, data collection, analysis and reporting. ERG also served to ensure enhanced ownership and validity of the evaluation findings and recommendations and provided inputs and advice for key evaluation processes and milestones. Moreover, the evaluation process included consultations with all relevant stakeholders including the government, UNICEF, civil society organisations, donors, and communities – women, men, girls and boys. In total, over 600 individuals (at national, sub-national and field levels) were consulted during the evaluation to ensure sufficient participation. Figure 2.3 summarises the evaluation methods applied for this evaluation.
The primary data collection included a representative KAP/HHS (including observations and transact walk as part of survey administration), semi-structured interviews (SSIs) with key informants at varied levels (list drawn together with UNICEF) and focus group discussions (FGDs) with communities. Moreover, field photographs were taken to use for the communication purpose
30 IBID
Figure 2.3: Evaluation Methods for Primary Data Collection
Primary Methods
Quantitative Methods
KAP SurveyObservations
/ Transect Walk
Qualitative Methods
Focused Group
Discussions (FGDs)
Semi Structured Interviews
Case Studies Desk Review

20
and human-interest stories collected as case studies. The methods selection was driven by varied nature of the evaluation questions to overcome the weakness of any singular method and to leverage the complementarities of using multiple methods for cross verification and corroboration purpose. Children (boys and girls) were consulted as key respondents to seek their views and suggestions. This worked to generate complementary and comprehensive data for subsequent analysis and triangulation. Where applicable, secondary information has been used to corroborate the primary data. The field data collection (both quantitative and qualitative) has been carried out in three regions where projects were implemented including Viet Nam capital. The field work was carried out in the Ha Noi (Capital), and three (03) districts (one district per province per region - Dong Thap, Lao Cai, and Ninh Thuan) and twenty-one (21) villages. The three provinces, where data was collected, were selected in consultation with UNICEF WASH team while ensuring equal and appropriate representation of each geographic region where seven targeted provinces are located. Within each province, district selection was done through randomization (See Appendix 3 for sampling strategy and rationale).
All primary data collection tools were translated, pre-tested, and revised before field application. Field teams were trained through an extensive training for tools application.
Secondary Sources Review
Extensive secondary sources review was undertaken, which continued throughout the evaluation. Overall, roughly about 125 documents including proposals, strategies and policies, legal instruments, MoUs, reports, guidelines, budgets etc., were reviewed as part of the documents review. The information retrieved from the literature review has been referenced appropriately into the report.
Quantitative Methods - Household Survey
For quantitative data collection, a representative KAP/Household Survey (HHS) was administered. The survey was administered in (03) three out of (07) seven provinces where RSHP constituent projects were implemented. Statistically significant random sample of 434 HHs from 21 villages was selected. Three districts, one from each province (across three regions) was selected for data collection (See Appendix 3 for sampling strategy and rationale). The HH payload of each village was evenly distributed among community. The households in each village were selected using systematic sampling techniques i.e. starting from the centre point of the village, every fifth household was selected for administration of HHS questionnaire. Table 2.3 shows the distribution of villages and HHs by each of the administrative units, while Table 2.4 outlines the geographic scope of the HHS.
Table 2.3: Overall Sample Distribution by Districts and Villages
Table 2.4: Geographic Scope of the Post-KAP Survey
Units Number Province Districts
Districts 3 Dong Thap Tan Hong
Villages 21 Lao Cai Bac Ha
HHs 434
Ninh Thuan Thuan Bac
The KAP questionnaire used for the HHS (Appendix 5) was developed with the view to assess current level of knowledge, attitudes and practices around key performance indicators for RSHP. The questionnaire included series of questions for assessing the strengthening of the social norm for latrine use. The survey has been administered in ODF certified villages only. The respondents included adult family members (both men and women) from selected households. The field surveys were administered while using the mobile applications. The data was gathered through pre-designed questionnaire on tablets and transmitted to central data on regular basis. This enabled keeping track of field data results and take corrective actions where required.

21
Table 2.5: Distribution of Head of households by gender and province
Table 2.6: Percent distribution of Head of households within province by gender
Province M F Total Province M F Total Dong Thap 99 40 139 Dong Thap 23 9 32 Lao Cai 129 15 144 Lao Cai 31 4 35 Ninh Thuan 89 51 140 Ninh Thuan 21 12 33 Total 317 106 423 Total 75 25 100
Observations & Transect Walk The questionnaire included observation questions performed as part of the KAP Survey. These included observations at household and community levels. The field enumerators were guided to walk around the village to observe evidence of open defecation and make photographs. This was done to ascertain the compliance with ODF certified status.
Qualitative Methods
The qualitative data was collected using multiple methods i.e. semi-structured/key informant Interviews, focus group discussions, and observations. The interviews/discussions were guided by semi-structured interview/discussion guides, attached as Appendix 6.
Semi-Structured/Key Informant Interviews (SSI/KIIs) In line with the scope and plan of qualitative methods that was agreed with UNICEF WASH team and that also conforms to evaluation needs, a total of 34 SSIs/KIIs were conducted (of which about one third were with female respondents, mostly government officials and representatives of world bank) with a range of key stakeholders including government, UNICEF, donors, and CSOs. The representatives were deployed at national and sub-national levels. These were conducted with relevant UNICEF staff, MARD (including PO) and MoH/VIHEMA at national level, field staff in provinces. The other key stakeholders included MPI, donors, and CSOs. The selection of stakeholders and representatives (for interview) was undertaken together with UNICEF Viet Nam, while applying ‘Purposive Sampling’ techniques. The sample included all key stakeholders and afforded sufficient level of repeated interaction with these stakeholders to achieve desired saturation. It was kept in mind to balance the geographic diversity. The interviews were conducted by senior team members, which enabled using the interview guides fully to generate comprehensive information. The interviews were (audio) recorded with prior consent of the participants, for subsequent transcription. The Table 2.7 lists the stakeholders interviewed during evaluation.
Table 2.7: Key Informant Interviews Administrative Distribution
Level Stakeholder/Respondents
National UNICEF (Individual & group Interviews) with Chief of WASH, WASH Specialist, Chief of PME (Planning, Monitoring, Evaluation), MoH, MARD, NCERWASS, MOLISA, VIHEMA, VBSP, Donors: World Bank, DFAT, and DANIDA
Provincial PCERWASS, CPM, DARD, DOLISA, Communication Official of CPM at district level, Provincial Steering Committee
District District Health Office, District Centre for Prevention, District Health Service Centre, Public Health Section, Commune staff in charge of culture, health and education; mass organization (Women's Union/Farmers Union), head of villages
Focused Group Discussions (FGDs) A total of 24 FGDs were undertaken particularly with communities including men, women, boys and girls (Appendix 10). Two FGDs were undertaken in each of the selected 21 villages (four communities per district), where KAP survey was administered. Separate group discussions were arranged with male and female respondents, which were guided by FGD guides. These

22
discussions were organized closer to the communities to enable participants to feel secure and share views with confidence and trust. On average 8-12 members participated in each discussion. The discussions helped capture the views of range of community level beneficiary groups as to projects contributions to improved services and changes in behaviours. The discussions were (audio) recorded with prior consent of the participants and used for transcription later on. The group discussions with children were moderated by the experienced staff, particularly trained in the application of child friendly tools/techniques while taking care of all related sensitivities that must be considered during interaction with children. The distribution of the FGDs is presented in Table 2.8 below. The list of FGDs conducted during the evaluation is attached as Appendix 10
Table 2.8: Key Informant Interviews Distribution
Group Type
Lao Cai Ninh Thuan Dong Thap
Total District: Bac Ha District: Thuan Bac District: Hong
Ngu Com.1 Com.2 Com.1 Com.2 Com.1 Com.2
Male 1 1 1 1 1 1 6 Female 1 1 1 1 1 1 6 Children 1 1 1 1 1 1 6 Field Staff, Commune Resource Persons
1 1 1 1 1 1 6
Total 4 4 4 4 4 4 24
Framework for Social Norm Assessment The evaluation benefitted with UNICEF’s guidance for assessment of social norm31. The assessment of social norm measures the prevalence of OD in communities that have been verified at different intervals in the past. The evaluation focused on assessing the consistent latrine-use behaviour through a quantitative lens by integrating the following specific questions in the household survey questionnaire. Additionally, to the extent possible, findings were enriched with qualitative findings about the application of MoH/VIHEMA guidance for ODF certification and verification for triangulation purposes. The social norm analysis considers the entire duration of RSHP implementation (4 Years) for ODF verification at the time of Evaluation. Furthermore, the social norm assessment32 was supplemented with: a) making physical observation as part of the HHS interview for any signs of latrine use, b) through self-reported frequency of latrine use when at home, and c) self-reported OD practice in the last 7 days by the survey respondent. The matrix below presents specific elements of social norm assessment framework.
UNICEF’s Social Norm Assessment Framework
Q# Key elements Assessment Parameters
1 Empirical Expectations33
What is the prevalence of empirical expectations of latrine use?
2 Normative Expectations34
What is the prevalence of normative expectations of latrine use?
3 Existence of Sanctions What is the prevalence of belief in the existence of sanctions for OD?
31 (a) SUSTAINABILITY CHECKS - guidance to design and implement sustainability monitoring in WASH (13.06.2017) and (b) UNICEF HQ Programme Division/ WASH, New York; UNDP-SIWI Water Governance Facility, Stockholm. 32 Presentation (14.12.2016): 'How to integrate social norm approach in future, classical UNICEF WASH/CLTS program evaluations?' - A tentative model. Jérémie Toubkiss WASH Evaluation Specialist, Evaluation Office, UNICEF NYHQ and Julianna Westerblom, WASH Specialist, UNICEF Chad; 33 Empirical expectations correspond to community members' beliefs concerning the behaviour of other members in the community; 34 Normative expectations correspond to the community members' beliefs about what other members of the community think should be done;

23
UNICEF’s Social Norm Assessment Framework
Q# Key elements Assessment Parameters
4 Consensus and Consistency
Analysis of consistency and consensus between empirical and normative expectations and prevalence of personal normative belief
Note: The other elements of the social norm theory i.e. analysis of the ‘conditional preferences’ and ‘reference network’ is excluded from the scope of the evaluation.
Drawn from the above framework, specific questions were included in HHS for social norm assessment as are listed in below matrix. For minimising any biases and to improve accuracy of data collection, the HHS questionnaire was administrated by appropriately trained and locally hired enumerators using their native language. Moreover, the questions were pretested, and necessary amendments were made before final application of the questionnaire.
Specific Questions Included in Post-KAP HHS for Slippage and Social Norm Assessment
Q# Question Response Options
1 Some people use a latrine and other people do not. How often do members of your household use a latrine? Note: The overall response to ‘options-5’ will indicate the slippage rate; 100% result for option-5 will indicate 0% slippage Will be used to triangulate / verify responses against question on OD practices by household members in the baseline
1. Never 2. Rarely 3. Sometimes 4. Often 5. Always
2 Think about the people in your village, such as your family, friends, and neighbours. Out of 10 people in your village, how many do you think said that the members of their household always use a latrine?
Number: _________
3 Do you believe that people in your village should use a latrine?
1. Yes 2. No - SKIP Next
Why do you think people in your village should use a latrine? 1. Because it is the right thing to do 2. Other reasons
Think about the people in your village, such as your family, friends, and neighbours. Out of 10 people in your village, how many do you think said that people should use a latrine because it is the right thing to do?
Number: ___________
4 If someone in your village was observed defecating in the open, what would happen to her/him. Are people punished for defecating in the open, and if YES, how?
1. Financial penalty 2. Legal penalty 3. Community members scorn / punish 4. Other 5. Nothing happens - SKIP Next Specify: __________
Please note that positive reinforcement is tackled in earlier sections of the questionnaire
Absence of a baseline constrained the evaluators in making any comparative analysis of findings on social norm assessment.
DATA PROCESSING AND CONSOLIDATION
Data processing of the quantitative data (filled questionnaire) commenced immediately at the end of actual data collection. All the questionnaires were manually screened for consistency and quality at two stages – once in the field upon completion of daily activity (by the enumerator and/or district supervisor), and a second time when questionnaire was handed over to the quality assurance staff on daily basis for 100% editing/coding to ensure data accuracy and completeness. Once cleared from the field quality assurance staff, all filled forms were dispatched to the central data entry point.

24
The data entry was carried out using specialized software, i.e. Census and Survey Processing System (CSPro). Post-data entry, editing and cleaning, and statistical analysis were done using interactive data analysis techniques, the Statistical Package for the Social Sciences (SPSS) and MS Excel.
Data Analysis
Quantitative Data: All tabulations of the HHs were based on a variety of stratifications, i.e. disaggregation by sex, gender, ethnicity, income levels, administrative parameters (region, province and district), period of ODF declaration etc., for all key elements of the investigation like OD practice, latrine use, and supply side elements etc. The tabulations were produced using statistical techniques such as frequency tables, and cross tabulations. Moreover, secondary quantitative data has been used for baseline and end line. The comparison techniques have been used to compare baseline with end line results (including KAP/HHS results) for key outcome level indicators including improved water access. Qualitative Data: the qualitative findings were scrutinized and examined by core team members to identify key themes and trends occurring in the responses from KIIs/FGDs. The qualitative data from the KIIs, FGDs and Field Observation were analysed manually by going through transcripts developed from notes taken during the KII and FGD sessions. Afterwards, data was summarized, coded and categorized into themes (data reduction). Continuous iterative revision of texts was carried out to identify and code the main patterns and categories in the data. Matrices were used to organize the data and interpret and synthesize it into conclusions (data display). Conclusions were then verified by going back to the transcripts (conclusion drawing and verification). The process yielded some specific success stories or case studies on Programme achievements to further enrich the analysis on outcome level and other significant change/s on the ‘Social Norm’. Triangulation: All data collected through multiple sources and methods was collated, consolidated and corroborated for cross verification and validation of field findings and other information retrieved from review of programme documents. This triangulation enabled the evaluators to ascertain the reliability and credibility of the analysis. Furthermore, post-field data collection, a detailed briefing was done with ERG members including the chief of CSD at UNICEF CO to cross check and validate initial filed impressions. Also, written feedback was sought on field findings to seek factual corrections and to take inputs from UNICEF WASH team and other key members of PME section to inform further data analysis and reporting.
QUALITY ASSURANCE (INTERNAL AND EXTERNAL)
The following key steps were taken to ensure quality assurance of all processes that were realized during evaluation, particularly for the field data collection:
Comprehensive Training: A comprehensive training for all the field staff was ensured. At the provincial level; the core team trained the master trainers, who, in turn, trained the other staff.
Continued Supervision: With support from the local partner, continued support and supervision was ensured by the Evaluators (both internationally and nationally). The Evaluators also provided technical support and supervision to our local data collection teams in the field whenever necessary.
Experienced Staff: Field data was collected with the engagement of experienced field staff.
Audio Recordings: Where permission was granted, the KIIs and FGDs were digitally (audio) recorded and transcribed to avoid loss of field information.
Informed consent was a critical pre-requisite for HH level interviews. Evidence Collection: Photographs of the key locations and events were collected with
prior consent from the concerned community members or the respondents/participants of the KIIs and FGDs.
Transcriptions and Field Notes: At data consolidation stage, transcriptions were prepared using the audio-recorded data collected during meetings with the KII’s and FGDs.

25
The electronic devices were used for online data collection and data entry/recording. All enumerators were provided sufficient training to correctly use these devices. The field team supervisors were appointed at district level in each province to ensure quality control during the fieldwork; some key aspects of quality assurance during field data collection are mentioned in Appendix 15. The evaluators, through the local partner, provided a team of independent field monitors, who carried out the following activities:
Interview observation: the monitoring team, through its local partner, observed all the enumeration teams, particularly in the early stages of the data collection process. This was to check that the asking of questions, the recording of responses and the treatment of respondents was carried out correctly.
Protocol observation: the survey supervisors observed fieldwork protocols to ensure that respondents were selected appropriately, and that the replacement procedure was carried out according to guidelines.
External Quality Assurance (Evaluation Reference Group)
As part of external quality assurance measures, the Evaluation Reference Group (ERG) was formed by UNICEF Country Office Viet Nam with a view to maximizing the credibility and hence the utility of the evaluation. The ERG comprising the representatives of the key public stakeholders (MoH, MARD) and UNICEF WASH and Evaluation specialists at the Country Office, regional and HQ levels. The ERG served as main consultation platform with oversight and advisory functions. Key responsibility included to facilitate the participation of all stakeholders, provide feedback and technical inputs for key evaluation outputs (evaluation design, methodology, data collection tools and processes, and reporting) and to facilitate the evaluation team’s access to all information and documentation.
Compliance with UNEG/UNICEF Evaluation Norms, Standards
The evaluation has been undertaken while keeping in view the UNEG Norms and Standards of Evaluation35. The evaluation adheres to these standards i.e. UNEG Norms and Standards of Evaluation (2016), UNICEF adopted UNEG quality standards for evaluation reports (2017) and UNICEF Procedure for Ethical Standards in Research, Evaluation, Data Collection and Analysis (2015). The evaluation process and the output i.e. report, took a considered view of the expectations and thus instituted mechanisms to comply with the expectations around cultural sensitivity; utility; credibility; confidentiality; transparency; and gender, equity and HRBA. For this purpose, the Evaluators maintained their independence, impartiality, and credibility. The Evaluators avoided any possibility of conflicts of interest and considered themselves accountable for their conduct during evaluation processes. Key ethical principles followed during evaluation include respect for dignity and diversity, right to self-determination, fair representation, compliance with codes for vulnerable groups particularly children, and avoidance of harm for all participants of the evaluation events (KIIs, FGDs, etc.). All these considerations guided the tools development, selection of respondents, and planning and implementation of field activities. All field staff was sensitized and trained on the actual application of these principles during actual data collection. In this regard, following considerations were given due attention and below listed actions were ensured:
Informed consent was ensured by all participants of the KIIs and FGDs. The process was facilitated by local Partners’ staff. Key elements of the consent included: a) brief introduction of the Programme; b) sharing the purpose of meeting (KIIs/FGDs); c) Participants’ willingness to participate on voluntarily purpose; d) expected time duration for the meeting; and sharing the Consultants’ expectations and other protocols of the meeting;
35 United Nations Evaluation Group (UNEG), 2016a. Norms and Standards of Evaluation. [.pdf, online] Available at: http://www.unevaluation.org/document/detail/1914

26
Appropriate and relevant permissions were sought, where applicable and required, before any action/event by the Evaluators and associated field staff. Particularly while using the audio recordings of the meetings (KIIs, FGDs), taking Photographs (respondents/participants, place and any action) for evidence generation purpose.
Data confidentiality and anonymity was ensured by taking the following actions; a) separating the respondents’ identity from the actual data; b) any identifiable information was erased immediately after data mining was completed; c) only authorized manager/s and data management team were granted access to datasets for data analysis and data management during data analysis, reporting and even at later stages after assignment closure.
Attention was paid to ensure adherence to the following protocols:
All meetings (KIIs and FGDs) were organized in close coordination with the designated focal points (within each government department and community); the convenience and comfort of the participants/respondents was prioritized in scheduling all interaction with relevant government staff, community members and other respondents.
Questions were phrased in a manner ensuring respect and integrity of the respondent/participants. Attention was paid to avoid any irrelevant discussions which could trigger their emotions.
Cultural norms and traditions were respected during visits to public places, schools and interaction with community members.
Participants/respondents were guided and encouraged for their active participation in discussions and were guided to respect the point of view of each participant regardless of his/her Grade and ethnicity.
Gender balanced field teams were employed to ensure that female staff should interact with female respondents to elicit their natural response.
Where it was required, feasible, and contextually relevant, the Evaluators organized separate group discussions for male and female respondents (men, women, boys and girls); all group discussions were held in the safe environment of Commune Administration Offices or at some other place suggested by community.
Interaction with Children: The data collection also involved FGDs with Children. Application of the following ethical standards were taken care of and given due focus:
To incorporate the views and opinions of the children; meetings with children were organized in safe environment of schools.
Discussions with Children were moderated by experienced Evaluators and senior members of the national team using child-friendly approaches and methods. All relevant staff was given appropriate briefing on the use of child-friendly approach while dealing with children. The moderators ensured that ice-breaking sessions were convened before starting the actual discussion with children.
All relevant information about data collectors; purpose and utility of the activity was shared with children prior to start of any discussion.
Children were clearly told that they can refuse or withdraw from the activity, and this will not have any bearing against them in any way.
Discussions with children were moderated in a manner that they felt themselves protected and comfortable while interacting with Evaluators.
Similarly, a code of conduct for the group discussion was agreed upon with children and was implemented. It ensured equal and active participation in discussion from all children. For more details on compliance to UNEG principles and standards, please refer Appendix 15.
LIMITATIONS, CONSTRAINTS & MITIGATION STRATEGIES
Find below the list of key evaluation limitations and constraints, together with the mitigation measures evolved and applied to prevent and/or minimise any resultant impact on evaluation.

27
Table 2.9: Evaluation Limitations and Mitigation Measures
S# Limitations & Constraints Management and Mitigation Measure
1 The transmission of information and documents from UNICEF and other stakeholders remained slow and patchy. Some essential records such as investments in and beneficiaries of water and sanitation interventions within provincial projects were not provided. This affected the deeper comprehension of programme and results and hindered any meaningful efficiency analysis.
Repeated and pointed requests were made to secure information and documents. As the documents arrived in parts, the literature review remained an ongoing activity. The efficiency analysis remains weak for information or data gaps.
2 The sampling approach for HHS is non-representative (for the total number of ODF communities), hence results may need to be cautiously generalised e.g. extent of slippage and social norms creation.
This remains a methodological constraint driven by the financial constraints. The sampling approach used has enabled producing results that may provide insights into it and to measure the extent of slippage. Similarly, for social norms analysis, a considered decision was taken to have enough sample (number of households) from selected ODF villages to offer more general analysis around the strength of the social norm for latrine use.
3 Field survey was stopped by the public authorities in Dong Thap Province, which delayed data gathering and consequently delayed the data processing and reporting.
The field teams were guided to continue working while contacts were made with PPPs in provinces where exercise was halted. The teams were advised not to collect information which the provincial authorities found sensitive. The data collection tools in Vietnamese were shared with provinces to avoid any confusion. The villages missed in the first round (for selected information) were covered in the second round, for which the contracts were signed with relevant provincial authorities for data collection.
4 Availability of reliable, current, and usable secondary data/information (in particular quantitative) data impeded longitudinal assessment, disabling Evaluators to draw meaningful comparisons for plausibility for design and ascertain RSHP’s contributions in any accelerated change at outcome level. Moreover, the data limitations did not enable Evaluators to establish if and to what extent UNICEF provincial projects impacted on child malnutrition.
The Evaluators have referred to multiple data sources such as MICS, JMP and World Bank (World Development Indicator sheet) to extract current and usable data, however found could find data from 2011 until 2015. Moreover, the unavailability of provincial disaggregated data remained a major constraint to track, analyse and comment on changes (to establish projects’ contributions) in accelerating accessibility (to improved water and sanitation) and the adoption of practices. This remained a key challenge in establishing projects causality and contributions. However, to the extent possible, triangulation technique was employed to ascertain the evidence collected from field and review of programme documents to inform evaluation findings and recommendations.
5 The transition in UNICEF VCO, specifically for PME team and later of WASH team, delayed the timely start of field work, which eventually affected the overall evaluation timeline. Visa issuance process for the International team
Evaluators kept regular contact with the different focal points that took over the evaluation supervision role at UNICEF VCO. The field work was adjusted to enable the new focal point to settle in. Additional resources were deployed for

28
Table 2.9: Evaluation Limitations and Mitigation Measures
S# Limitations & Constraints Management and Mitigation Measure
also took longer than usual time due to (issuance of) visa carrying incorrect travel dates. Later, long holidays, both in Viet Nam and Pakistan, marking various national and/or religious events, also resulted in delayed reporting and feedback loop.
field data collection (HHs and FGDs) to compensate the time loss due to delayed visa approvals. The evaluation timeline was extended through a ‘no cost extension’ in the contract to enable the evaluators to produce a quality evaluation report.
EVALUATION IMPLEMENTATION, MANAGEMENT, & TEAM COMPOSITION
The execution of the evaluation was divided into five phases; each phase comprised of series of activities contributing directly and/or indirectly to a particular transit or contractual deliverable or a set of deliverables. Table 2.10 contains details of the phases of the evaluation, the main activities within each phase and the corresponding Outputs (transit deliverables) or the contractual deliverables.
Table 2.10: Evaluation Phases, Activities and Deliverables
S# Phase Title &
Timeline Activities Outputs/Deliverables
1 Pre-Inception Phase
(Jun-Sep 2017)
Key activities include: - Series of skype meetings - Initial literature review - Evaluation matrix development and - Sharing and drafting of Inception report
Draft Evaluation Matrix and Tools
Draft Inception Report prepared and shared with UNICEF for feedback
2 Inception Phase
(Sep-Oct, 2017)
Key activities include: - Development of evaluation toolkit and
translation - Finalization of Inception Report after
feedback - Field planning and advance approvals
and coordination with relevant stakeholders
- Visa processing for international team
Inception Report finalized Field activities were planned and
local partner i.e. DEPOCEN, identified and locked.
3 Field Data Collection
(10- 27 Oct 2017)
Key activities include: - Translation of tools and training of field
teams - Pre-testing and tools revision - Development of mobile application
software and testing - Micro-field planning and rollout - Development of evaluation toolkit and
translation - Quality assurance mechanisms - Field data collection - Field and Hanoi debriefs - A short debrief note shared with
UNICEF.
Field teams were trained, and Micro-field plans prepared
Field data collected Field debrief was organised and
short debrief note prepared and shared with UNICEF (for sharing with ERG)
4 Data Processing & Analysis
Key activities include: - Data consolidation - Literature review - Preliminary data analysis
Data consolidated, and data sets and sheets prepared
Data processed, and preliminary findings discussed for reporting

29
Table 2.10: Evaluation Phases, Activities and Deliverables
S# Phase Title &
Timeline Activities Outputs/Deliverables
(November 2017 – December 2017)
- Internal reviews and discussions - Discussions with UNICEF team and
requests for additional documents
5 Reporting and Dissemination
(January 2018 -June 2018)
Key activities include: - Drafting for Evaluation Report and
sharing - Feedback and incorporation to finalise
report - Presentation of key findings
(dissemination event)
Draft Evaluation Report produced and shared with UNICEF
Evaluation Report Finalised Dissemination session (with
presentation of key findings and recommendations) was moderated
Evaluation Management, Team Composition, and Timeline
The evaluation was managed and supervised by UNICEF Viet Nam Office. The PME Chief was the contract manager with support from WASH team. UNICEF WASH team coordinated with national and provincial stakeholders for scheduling field activities and seeking data from public stakeholders. The relevant public agencies supported with field visits to villages and interaction with communities. Regular communication was maintained between the Evaluation Team and UNICEF. The entire evaluation was conducted in a participatory manner, whereby in addition to the involvement of multiple stakeholders at varied levels, an ‘Evaluation Reference Group’ (ERG) was formed and kept involved in the evaluation at all key stages (inception phase, data collection and reporting). The core function of the ERG was quality assurance of the evaluation processes and outputs. The ERG members reviewed the key deliverables and provided their feedback and advice to improve the final deliverables. The involvement of key public officials in the ERG helped in enhancing the evaluation ownership and credibility of evaluation findings and recommendations. The evaluation was undertaken by a team of international and national experts with demonstrated experience in evaluations and coupled with demonstrated knowledge of the WASH sector including the application of social norm theory for WASH evaluations in varied contexts. The roles of the evaluation team members are described in Appendix 14. A local partner i.e. DEPOCEN, one of the leading national economic and policy research entities in Viet Nam, was taken on board for the field data collection, data entry, data processing and local coordination. This evaluation was implemented from June 2017 – June 2018. The field work for the evaluation was carried out in October 2017.

30
3 EVALUATION FINDINGS This section describes evaluation findings and analysis. The description is structured as per the Evaluation Matrix (Appendix 2), whereby each question (under OECD-DAC criteria) has been addressed separately. A separate section is included to respond to Non-OECD-DAC criteria i.e. equity, gender and HRBA. Moreover, commentary on WASH-Malnutrition (relating to children child) is included as a separate section also. The findings and analysis are based upon using the mixed-methods and triangulation of data. These include a representative household survey (administered to 434 respondents) and series of discussions with a range of public and non-public stakeholders at the national, provincial and district levels including communities. Overall, 23 FGDs in 12 ODF communities of six direct districts in three provinces were conducted. During these consultations, 175 community members were consulted including men, women and children. Furthermore, 34 KIIs were conducted at national, provincial, district and community levels. Overall, about 600 individuals were consulted during evaluation to inform the evaluation findings.
RELEVANCE
EQ#1: To what extent has UNICEFs rural water, sanitation and hygiene programme (RSHP) been relevant (to context/beneficiaries needs, existing capacities, national priorities and the work of other sector partners) for improving rural water supply (access and quality), hygienic sanitation and personal hygiene i.e. handwashing with soap?
Summary Assessment: The RSHP is assessed to be relevant in terms geographic targeting (of under-developed regions and marginalised groups); needs of the intended beneficiaries; coherence national and UNICEF’s global WASH strategic priorities; institutional capacities of relevant public stakeholders and global commitments under Sustainable Development Goals (SDGs) particularly the SDGs 6.1 & 6.2. RSHP prioritised and targeted the most deprived regions and provinces including community groups that needed assistance the most i.e. ethnic minorities in northern mountains and central highlands regions. Moreover, the provinces where RSHP implementation represent relatively the under-developed provinces. For instance, in 2012 as against the national poverty levels of 9.6%, the poverty rates for Norther Mountain and Central Highland regions were reported to be double i.e. 24% and 18% respectively. The average income of ethnic minorities was reported to be as low as one-sixth of the national average. The ethnic minorities constitute almost half of the total population in two regions. Similarly, for the minorities the accessibility rates for water and sanitation services are significantly lower than the national average for rural Viet Nam. Consequently, the child stunting rates amongst ethnic minorities are a staggering 41%36 compared to national rural average of 25%. For the focus on ethnic minorities with significantly lower accessibility rates (to improved water and improved sanitation), the programme could be argued as relevant to ground realities and needs. Also, this makes it coherent with UNICEF’s approach to equity, focusing on most poor and disadvantaged. The issues that were prioritised in RSHP such as water safety (for access to clean drinking water), safe sanitation, and community-based approaches to sanitation (CLTS/CATS), all are relevant to the listed priorities in ‘National Rural Clean Water Supply and Sanitation Strategy to 2000-2020’. The RSHP priorities took forward the agenda set under three cycles of ‘National Target Programme i.e. NTP I, II, and III for Rural Water Supply and Sanitation, implemented from 1998-2015. The RSHP implementation coincides with the implementation of NTP III (2012-2015). The introduction of CLTS is appreciated as relevant as it shifted governments focus to community-based models. The RSHP provided impetus and necessary technical support in institutionalising CLTS/CATS, amplifying the relevance of the programme to the context. The Programme’s support to ‘Innovative and Low-costs’ solutions for both water safety and sanitation further added to its relevance, by offering low cost and efficacious solutions. RSHP priorities and approaches
36 Viet Nam Nutrition Surveillance Profiles (2013) National Institute of Nutrition (source: Viet Nam - WASH Outcome Paper – Analysis by SP Outcome – RSHP Programme Document shared by UNICEF)

31
corresponds to UNICEF WASH Strategy, regional and country priorities. The summary assessment for relevance is elaborated below;
Relevance to the Context (Prioritisation of Deprived Regions - Provinces and Communities)
Despite being a ‘low Middle Income Country’, Viet Nam represents a context where rural areas are lagging far behind in development compared with the urban areas. Where it applies to other development indicators, it extends to the access to improved water and sanitation services. Some regions are more deprived than others, such as the northern mountains (NM) and central highlands (CH) regions. The Mekong delta region has its own set of challenges. Within provinces that lie in these regions, there are pockets of extreme deprivation, mostly inhabited by ethnic minorities. The disparities are outlined below:
1. In 2012, where the national poverty average was 9.6%, the poverty rates of NM and CH regions were as much as double, or more i.e. 24% and 18% respectively.
2. Reportedly, the average income of ethnic minorities was as low as one-sixth of the national average. Ethnic minorities constitute almost half of the total population in the NM and CH regions.
3. Sanitation and health related indicators are at their lowest in the two regions, particularly for the ethnic population. For instance, as per MARD Report (2014) the latrine existence in NM region was at 83% with 52% as hygienic toilets. Similarly, for CH regions, the situation is even more disappointing i.e. latrine prevalence at 78% with only half (50%) being hygienic.
4. The child stunting rates for ethnic minorities are an alarming 41%37 compared with the national rural average of 25%. The diarrhoea and parasitic infections related morbidity rates are also highest for ethnic minorities in these regions.
The Mekong delta region, prioritised for UNICEF support, may not be as poor, however, it has its own unique challenges. Hanging latrines are widely used in this region, which poses environmental risks to water bodies. In terms of prioritisation of disadvantaged and deprived areas, the RSHP could be argued as being very relevant. This is evident from the fact that out of 7 provinces (for rural water and sanitation support), 3 lie in NM region, whereas 2 lie in each of the CH and Mekong Delta regions. Moreover, all relevant public officials and staff from UNICEF met during evaluation endorsed the Programme’s relevance particularly for its targeting strategy. This underlines the integration of equity in the selection of intervention areas for RSHP.
Relevance to the Beneficiary Needs
The Programme could be argued as being relevant to the beneficiary needs, as inhabitants of 7 provinces where the RSHP was implemented continued to face low levels of access to improved water and sanitation. This could be attributed to limited outreach and capacities to deliver services in hard to reach areas and communities e.g. areas inhabited by ethnic minorities. The lowest quintiles or most poor face severe deprivation.
37 Viet Nam Nutrition Surveillance Profiles (2013) National Institute of Nutrition (source: Viet Nam - WASH Outcome Paper – Analysis by SP Outcome – RSHP Programme Document shared by UNICEF)
Box # 03: Reportedly, the Northern Mountain and Central Highland regions represent highest level of deprivation. The performance on development indicators for ethnic minorities (constitute half of the population) is even more dismal. For instance, against the national poverty rate of 9.6%, the poverty rates in these regions are double or more i.e. 24% for NM and 18% for CH.
(World Bank. Program Appraisal Document: Results-Based Scaling Up Rural Sanitation and Water Supply Program. Report No:70529-Vn, 2015, Viet Nam.)

32
Despite notable achievements from 1990 to 2011 for access to basic sanitation (rates jumped from 30% to 67%), 33% of the rural population in Viet Nam did not have access to improved toilets38. The access to hygienic latrines is even lower at 58% (NTP III - 2013). There are staggering differences between the rich and the poor. Reportedly (MICS 2011), almost half (58%) of the poorest quintiles do not have access to improved toilets in comparison to 100% for the richest quintile. Moreover, approximately half of the population (52%) of ethnic minorities are either practicing open defecation, or using unhygienic latrines compared to national average of 18% for ethnic majority i.e. Kinh/Hoa groups39. The fact that the regions prioritised for RSHP have higher concentrations of ethnic minorities, remote settlements, and hence deeper deprivation, makes it relevant. UNICEF’s Programme is highly relevant since it is benefitting a significant proportion of the ethnic minorities and the poor population residing in these regions. The rates of stunting, malnutrition, and water and sanitation related diseases particularly among children, are considerably higher40 than the national averages in the targeted regions or provinces, which amplifies the relevance of the programme further. The JMP Report 2017 ‘Progress on drinking water, sanitation and hygiene and SDG Baseline’ indicates that in Viet Nam basic access to drinking water41 stood at 91% in the year 2015, therefore, basic access is not a major concern. The problem lies in expanding the access of safe drinking water to deprived regions and vulnerable minority groups to reduce existing inequities. Though aggregate estimates for safely managed water supplies (SDGs baseline) are not yet available, however, the constituent relevant indicators on safely managed water supplies present a depressing situation. For example, 72% of the rural population is using non-piped water compared to 55% at the national level, and 20% for the urban population. Overall, 7% of the rural population is still dependent on unimproved water sources, and an additional 1% of rural population is still reliant on drinking surface water42. This state of affairs strongly advocates for the need of a programme like the UNICEF’s RSHP to focus on improving the quality of rural water and sanitation services. The results of the household survey conducted as part of the evaluation, indicate that a significant proportion, 79% and 73% of the respondents (see Table 3.1), perceive that they have access to a ‘clean’ and ‘safe’ drinking water source respectively. The pattern across the three provinces is almost even, and ranges between 67% to 76%. However, on the perceived quality of water (taste, odour/smell, appearance), the results demonstrate that water quality is an issue for the surveyed communities. Furthermore, two third (67%) of the respondents expressed the view that the quality of water is acceptable in terms of taste, odour/smell and appearance. These results again correspond to the Programming priorities (improving water quality and safety) set by UNICEF and the Government for these communities and therefore establish the relevance of the RSHP for the targeted communities.
38 Lalit Patra, C Badloe & A Tran. Scaling up rural sanitation in Viet Nam: A collective analysis and recommended actions. Briefing Paper, 37th WEDC International Conference, Hanoi, Viet Nam, 2014 39 Ibid 40 Viet Nam Nutrition Surveillance Profiles (2013) National Institute of Nutrition (source: Viet Nam - WASH Outcome Paper – Analysis by SP Outcome – RSHP Programme Document shared by UNICEF) 41 World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF). Progress on drinking water, sanitation and hygiene: 2017 update and SDG baselines. Geneva. 2017. https://www.unicef.org/publications/files/Progress_on_Drinking_Water_Sanitation_and_Hygiene_2017.pdf 42 Ibid
Box # 04: Sanitation: 33% of rural population is still deprived of
improved toilets. 58% of the poorest quintile do not have
access to improved toilets. 52% of ethnic minorities are either
practicing open defecation or are compelled to use unhygienic latrines.
(Briefing Paper, 37th WEDC International Conference, Hanoi, Viet Nam, 2014)
Water Quality: 72% of rural population is forced to use
non-piped water compared to national average at 55%
7% of rural population is using water from unimproved water sources
1% population is still reliant on drinking surface water.
(WHO and UNICEF. Progress on drinking water, sanitation and hygiene: 2017 update and SDG baselines.)

33
Table 3.1: Percent distribution of respondents reporting water safety and quality
Drinking water source Overall Drinking water from
source is of acceptable quality (N = 434)
Overall
N % Yes
%
Drinking water source – clean (Yes)
343 79
Taste 291 67
Drinking water source – safe (Yes)
313 73
Odour/smell 289 67
Appearance 291 67
Relevance of RSHP Approach (Design and Implementation) to UNICEF’s WASH Global Strategy (2006-15 and 2016-30)
The RSHP gives priority to addressing WASH sector bottlenecks to accelerate the provision of access to improved water, sanitation, and hygiene in Viet Nam. Box 05 lists key barriers as reported by the sanitation demand research study, jointly conducted by UNICEF, WB-WSP and VIHEMA. The priorities and strategies of the RSHP are coherent with UNICEF’s Global WASH Strategies (2006-15 and 2016-2030). The coherence is evident particularly for UNICEF’s efforts to strengthen the WASH Enabling Environment. The RSHP has prioritised parallel interventions for governance, institutional and structural factors, which is in line with the global strategy (explained in detail in the next section). The focus on softer or behavioural change is again consistent with the global guidance. Moreover, the prioritisation of interventions to strengthen the supply side i.e. SanMark, low-cost solutions, and advocating to and empowering communities to demand safe water and sanitation facilities, is found to be coherent with global priorities. To turn these into reality, the Programme focused on encouraging a departure from cost heavy supply-side and hardware driven solutions, to developing low cost, community driven and behaviour change interventions. This includes institutionalisation of CLTS/CATS for rural sanitation; hygiene promotion to achieve behavioural changes through application of C4D; and initiatives to develop and promote low cost models of water safety and latrines. The RSHP approach at design level is considered ‘highly relevant’ as it focused on enabling the relevant public-sector agencies by training and creating aids to establish models of successful implementation for eventual scaling-up of rural water (safety) and sanitation services. This approach complies with UNICEF’s global priority of strengthening the ‘Enabling Environment’, to facilitate relevant stakeholders in delivering services effectively and efficiently. At the implementation and operational level, the RSHP focused on building the capacities at the national and sub-national levels. It looks relevant as it emerged as a priority during a transition from NTP-II to NTP-III (2012-2015). The government’s own reports point to weaker provincial capacities43 with respect to understanding, planning and implementation of programming shifts. The reports highlighted serious capacity gaps and extremely low levels of understanding of community led programming approaches (CLTS/CATS) and the limited availability of appropriate skills, tools, standards and guidelines to enable relevant government departments to mobilize and
43 L Patra (Viet Nam), C Badloe & A Tran: Scaling up rural sanitation in Viet Nam: A collective analysis and recommended actions; Briefing Paper: 37th WEDC International Conference, Hanoi, Viet Nam, 2014: Sustainable Water and Sanitation Services
Box # 05: The key barriers to rural water and sanitation sector
- Subsidy led approach - Weak sanitation marketing - Low priority on hygiene promotion - OD an acceptable social norm - Consumer behaviour (low willingness to
pay - Gap between buying power and
aspirational choices for improved latrine, - Low awareness on low-cost sanitation
services and products
(Sanitation demand research study in Viet Nam; Jointly conducted by UNICEF, WB-WSP and VIHEMA)

34
support communities for rural sanitation initiatives. By and large, all public officials acknowledged and were appreciative that RSHP has contributed significantly in enabling the government to adopt the community led approach towards rural sanitation. Moreover, the introduction of standards and operational guidelines further aided the CLTS institutionalisation process and therefore demonstrate the relevance of the Programme.
Coherence with National Priorities
UNICEF’s RSHP is highly relevant to various national commitments made by the GOVN, for improving the overall wellbeing of its population. UNICEF’s Programme directly contributes to the vision, strategies and rural water and sanitation related national priorities as stipulated in the ‘National Rural Clean Water Supply and Sanitation Strategy to 2020’. At the same time, the Programme results will indirectly contribute in achieving other development priorities (such as improved health, reduction in poverty, education and livelihood) as highlighted in the Socio-Economic Development Plan (SEDP 2011 - 2015) and Socio-Economic Development Strategy (SEDS 2011 - 2020). Furthermore, UNICEF efforts in scaling-up rural sanitation are highly relevant to GOVN efforts to achieve the two key national commitments under the ‘Sanitation for All (SWA)’ partnership 2014, specifically 1) Elimination of OD from the country by 2025 and 2) Ensuring universal access for safe water by 2030 in Viet Nam. The UNICEF Programme is highly relevant to the Government’s efforts in shifting its programming approach from a supply-driven approach to behaviour change programming, thereby, enabling the Government in scaling-up rural sanitation and water supply services. By the end of NTP II, the advocacy efforts of UNICEF and other partners had resulted in greater recognition by the government of the need for behavioural change approaches (SanMark, CLTS, C4D) to scaling-up rural WASH sector interventions. Within this context, UNICEF’s RSHP 2012-2016, aimed to introduce a programming shift. The efforts were acknowledged by all stakeholders as most relevant and responsive in the scaling-up of rural sanitation and water supply provision (mostly donors shared this during interaction with the evaluation team including World Bank). UNICEF supported the relevant ministries MARD, NCERWASS, MoH, VIHEMA and other related entities in designing, planning and implementing NTP-III (2012-2015) with these new approaches, thereby enhancing the relevance of the RSHP.
Adherence with International Commitments
UNICEF’s RSHP is in line with the various international commitments of the GOVN and the joint priorities set by UN agencies which are outlined in the ‘One Plan 2012-2016’44, particularly with the Outcome 2.2 and Output 2.2.545. The relevance’ of the UNICEF’s Programme is proven because of its contributions to achieving the Millennium Development Goals (MDGs) by 2015 and setting the appropriate foundation for planning and achieving UN Sustainable Development Goals (SDGs) particularly the SDGs 6.1 & 6.2, and the Viet Nam Development Goals (VDGs) on rural water and sanitation by 2030. The Programme was initiated in 2012 at a time when NTP-III was taking-off and achieving the water and sanitation related targets of MDGs required a strong push by the GOVN and other sector partners. Currently, UNICEF’s Programme is highly relevant to supporting the government’s efforts in achieving the sanitation related Sustainable Development Goals (SDGs). UNICEF’s technical assistance is highly relevant in achieving various strategic objectives and targets promised through the international commitments of the GOVN such as the Scaling Up
44 ONE PLAN 2012-2016 Between the Government of the Socialist Republic of Viet Nam And The United Nations in Viet Nam; Ha Noi, 27 March 2012. http://apps.who.int/iris/bitstream/10665/206609/1/one_un_vnm_2012-2016_eng.pdf?ua=1 45 Outcome 2.2: By 2016, increased quality and effective management of a comprehensive national health system, including health promotion and health protection, with a focus on ensuring more equitable access for the most vulnerable and disadvantaged groups); Output 2.2.5: National and sub-national capacities enhanced to improve evidence and the equitable access to and demand for quality and sustainable water supply and hygienic sanitation)

35
Nutrition (SUN) movement, A Promise Renewed for Child Survival and Sanitation and Water for All (SWA)46. The relevance of UNICEF’s RSHP is also demonstrated by the fact that it is in line with the development priorities, implementation approaches and strategic objectives of the work of other WASH sector partners, donors,47 International and local NGOs.
EFFECTIVENESS
EQ#2: To what extent has UNICEF technical assistance effectively contributed to creating an enabling WASH Governance Environment (policies, strategies, national M&E systems and Stakeholder coordination) for rural water supply, hygienic sanitation, and handwashing with soap?
Summary Assessment: This criterion had two evaluation questions addressed separately in the report. Overall, the programme has proved effective on multiple counts. The approach to identify priorities through ‘Multi-stakeholder Consultations’ (series of provincial level Bottleneck Analysis exercises) worked quite well in identifying challenges, causes and developing consensus on priority issues and approaches. These consultations included a wide range of public and non-public stakeholders. Under the framework of WASH Governance related Enabling Environment (EE), UNICEF’s support to improvise and make the policies more responsive proved effective. In relative terms, the support and approaches to policy changes for rural sanitation proved relatively more effective in terms of overall achievements around rural water. The key achievements include:
Revision of National WASH Strategy 2000-2020 in 2016 Formulation of Provincial ODF Road Maps Reinforcing political commitment for universal access to safe Water and Sanitation; Initiation of SDG Baselines Review of National Water Quality Standards (NQS) and Institutionalisation of CLTS. The public stakeholders at all levels expressed their
satisfaction with UNICEF’s contributions in improving policy environment. The contributions to strengthening sector coordination are evident and have been widely acknowledged. The key contributions (along with other stakeholders) have taken effect by establishing a separate Working Group for ‘Operations and Maintenance’ of rural water supply under the leadership of MARD Partnership Office. The group was formed in 2014 and provided platform for sectoral discussions. Moreover, UNICEF efforts kept alive the existing ‘Working Group on Sanitation’ (formed in 2010). UNICEF Co-Chaired the group with MARD PO. The forum provided platform to discuss and institutionalise CLTS. The success around establishing and/or strengthening the monitoring systems has been mixed. Apparently not much has changed for rural water monitoring, however the rural sanitation monitoring is taking shape as part of CLTS implementation. Currently the monitoring is pre-ODF focused with limited attention being paid to post-ODF monitoring for sustainability. The monitoring system does not capture the quality of inputs (outcome assessment) such as triggering. Moreover, it lacks tracking slippage and social norms. The use of technology in this case is minimal. The access to monitoring information is limited particularly outside the public domain. The monitoring system for both water supply and quality (including safety practices in rural areas) and rural sanitation may continue to need assistance to address gaps and challenges. The research and data analysis capacities within the existing monitoring system are insufficient and more so with respect to cross-sectoral domains such as WASH-Nutrition and others. The capacity building efforts were perceived effective, as far as the public stakeholders’ views are concerned. The focus has been on trainings with limited attention paid to other facets of institutional or capacity development. UNICEF’s efforts have contributed in an increased buy-in within government to new concepts such as CLTS and water safety, which will be helpful in accelerating public sector financing on these initiatives. The research and knowledge management remained at low priority
46 [Summary Report: Mid Term Review - Government of Viet Nam and UNICEF Country Programme of Cooperation; 31 January 2015. [File Name; 2014 UNICEF-Govt Viet Nam MTR Report Final_(Nov2015) en] 47 Such as DANIDA, Department for Foreign Affairs and Trade (DFAT), AusAID, JICA, Unilever, World Bank and I/NGOs like SNV, IDE (International Development Enterprises), Plan International and others.

36
hence is noted as the weakest link. This is evident in the form of insufficient documentation and use of government or development partners’ data for analysis, triangulation and dissemination.
Effectiveness of approach: Identification of Priority Challenges
The approach to identify and prioritise areas of assistance has been effective. It involved the use of a consultative process within the national and sub-national projects to seek inputs from the public sector and build ownership. A series of consultations in the form of ‘Bottleneck Analysis Exercises’ were undertaken with national and sub-national stakeholders (through 2013-14) to identify problems and causes and to prioritise areas of assistance for RSHP. Those consulted included MoH, MARD and MOPI at both the national and provincial levels.
These consultations helped evolve priorities for national and sub-national projects, based on needs on the ground. Thus, in this way the RSHP followed a structured and consultative approach, which proved largely effective. The RSHP prioritized the key issues that emerged from multiple Bottleneck Analysis exercises conducted around water and sanitation. Most significant challenges are outlined below:
1. Rural Water Supply: A significant issue faced by rural water services in Viet Nam is the compliance with MoH prescribed standards for safe/clean water. Other issues include the O&M of water supply schemes, lack of clarity on private sector role in the rural water services, poor application of water tariffs and recovery along with the limited financial resources for provinces to operate water supply schemes.
2. Rural Sanitation: The major issues in relation to rural sanitation included ‘high costs’ for latrine construction (approximately USD 300/latrine); limited subsidies or support for poor; weak supply chain; and limited availability and awareness of low cost sanitation options.
To improve equity, the focus of RSHP has been on creating a balance between interventions around access and quality, with promotion of pro-poor (low cost) solutions for water and sanitation. These were then prioritised in the supply chain related interventions for both sectors.
Policy, Standards and Guidelines
UNICEF’s support, both directly and indirectly, to policy level interventions has largely been effective. The key contributions in the policy domain are listed below:
Figure 3.1: UNICEF WASH Sector Enabling Environment Framework

37
1. Revision of the National WASH strategy (2001 – 2020): UNICEF and the World Bank successfully advocated for, and later provided assistance in the revision of ‘National Rural Clean Water Supply and Sanitation Strategy’. The document was finalised in 2016, with a road map for 2030, however it awaits final approval. The national rural water supply and sanitation strategy focuses on ensuring sustainable water supply; water safety; water quality; operations and maintenance (O&M) of the rural water supply schemes (RWSS); managing and connecting to households; and safe water storage and water treatment.
2. Rural Sanitation – Provincial ODF Roadmaps: UNICEF supported consultations in 2016 to encourage provinces to develop ODF road maps using community approaches to total sanitation. The provinces committed to developing such plans, and by the end of 2017, reportedly half of the provinces had developed the plans. UNICEF extended technical assistance to the provinces to support the development of the plans.
3. Creating National Commitment: UNICEF along with some other actors advocated and supported the formulation of national commitments specifically a) Elimination of OD from the country by 2025 and b) Ensuring universal access for safe water by 2030 in Viet Nam. The country made these commitments to the international community at ‘Sanitation and Water for All’ forum in 2014.
4. SDGs Roll Out and Baseline for Water and Sanitation: UNICEF is key technical partner for SDG roll-out as well as working with the National Bureau of Statistics and other relevant public entities (MPI, MoH, MARD etc.) to help establish baseline for SDG WASH targets.
5. Water Quality Regulations & Public Education: UNICEF and WHO supported to review and enact revised water quality and monitoring guidelines and regulations. Besides this, the provinces supported C4D activities for the promotion of water safety practices.
6. Institutionalization of CLTS/CATS Approach for Rural Sanitation: UNICEF has been successful in advocating the integration of community models such as CLTS/CATS into the national strategy. Additional support has been provided in developing operational and training manuals which are widely in use. UNICEF supported the national government in developing, applying and finalising the ‘ODF Verification and Certification’ guidelines (2016).
7. Resilient WASH Programming at policy and strategy level: UNICEF has been advocating for integration of DRR into the health, education and WASH programmes of the provincial governments. Ninh Thuan Province has integrated DRR into SEDP i.e. the provincial socio-economic development plan. The WASH Contingency Plan for the WASH Cluster is another example of DRR integration into preparedness planning.
8. Reinforcing Commitment by Commemorating WASH Days: UNICEF and UNILEVER partnered in 2012 to support VIHEMA at the national and provincial levels to organize events to celebrate ‘Global Handwashing Day’ (October 2012)48 and hygiene promotion activities on ‘World Toilet Day’. This has been done to reinforce the public-sector commitment to national objectives.
There is wide acknowledgement in the public sector of UNICEF’s technical and financial assistance being enabling and relevant. The representative from MoH/VIHEMA shared that UNICEF’s assistance has enabled the government in institutionalization of CLTS in terms of standardisation of processes and documentation, besides encouraging adoption and scaling up on national level. It will help the provincial governments in eliminating OD in line with Viet Nam’s commitment to eliminating OD by 2030 under SDG 6. The officials from VIHEMA admitted the fact that before UNICEF’s support, there was less awareness of the impact of OD on the environment and human health; nor were there any activities or action plans in place for eliminating OD. UNICEF’s engagement with VIHEMA has enabled it to put the sanitation issue on the national agenda, demonstrated by many meetings with National Parliament. As a result, sanitation was prioritized and included in Socio-Economic Development Plan. At the same time, the officials expressed their concerns about the pace of progress in achieving the national goal.
48 https://www.unicef.org/vietnam/media_19725.html; https://www.unicef.org/vietnam/media_19452.html

38
Sector Coordination
Viet Nam, while realising the significance of international development partners and the need to make public agencies plan and deliver in a more coordinated way, established a ‘Partnership Office’ (PO) at MARD in 2005. UNICEF has been instrumental in establishing and supporting the functions of this office. From 2012 to 2016 (under RSHP), UNICEF supported the PO in planning and organizing series of national and regional level seminars and workshops. UNICEF has been highly active in advancing the role of PO for effective sector coordination. This includes advocating and co-chairing the ‘Working Group on Sanitation’ (formed in 2010) along with MoH. The platform remained active through 2012-16 and facilitated rounds of discussions on critical issues to help improve coordination between stakeholders. UNICEF along with other donors/stakeholders i.e. DFAT, WB, DANIDA, and others, advocated for creating a working group for the O&M of rural water supply. The group, now consisting of 27 members, was established in 2014 and remained active by providing a discussion platform to raise critical issues around O&M policies and practices and offering advice for improvement. Most of the government officials (met during evaluation) were appreciative of the UNICEF’s coordination role at central and provincial level. The UNICEF’s coordination support at both levels has enabled the provincial governments for better planning, resource mobilization and implementation of multi-year and annual work plans. Discussions with the relevant public officials clearly points to an increased ownership, joint planning and responsibility for accomplishments of the intended targets for RWSS among MARD, PO, MoH, UNICEF and WB. The Water and Sanitation sector in Viet Nam has been persistently challenged by the conflicting roles of the MARD and MoH. The MARD being better resourced and more influential, considers itself superior for the sectoral initiatives. Resultantly, a weak coordination and engagement is noted between the two ministries. UNICEF and WHO worked closely with each other and invested a lot in terms of their advocacy and coordination efforts to involve the two ministries in jointly providing technical inputs for the preparation of the ‘National Water Safety Plan’. Later, the Ministry of Construction (MoC) was also involved in the finalization and approval of the plan. The plan requires water safety to be assured at three levels i.e. at the source, during distribution, and at the point of use. The implementation and operationalization of the plan, however, is a big challenge. Currently, MoC is the lead designated entity to implement water safety standards through MARD, because of its significant experience of water safety related work. An official from the WB shared the view that at the national level, the MoH is overworked and also has a limited budget. The nature of the collaboration between the MARD and MoH is unclear, and there is a need for increased collaboration and coordination between the two ministries and to work with other ministries, such as the MoET as well.
Sector Monitoring
Improving monitoring system within MARD has long been a priority that development partners, including UNICEF, have been working on. The monitoring, both as a public priority and process, has seen improvements, whereby a significant focus has been laid on strengthening monitoring for decision making. Rural Water Supply (Water Quality) For rural water supply, the focus has been on improving monitoring around water delivery, O&M, and quality. This has seen changes in the indicators, recording and reporting tools and practices and development of a ‘database’. Apparently, UNICEF’s contributions are limited in improving rural water supply monitoring. The Government monitoring system does not capture or at least report on UNICEF supported interventions (water treatment and storage), making Evaluators unable to comment on effectiveness of UNICEF assistance. Within the ambit of UNICEF’s CSD support, the monitoring for the areas of interest is distributed across a variety of stakeholders like MARD, MoH, MoET and allied provincial departments. For

39
instance, while the O&M related RWSS monitoring is responsibility of NCERWASS/PCERWASS, the water quality monitoring is the responsibility of MoH. The overlapping roles, and at times weaker coordination, makes it challenging to have regular monitoring and wider dissemination of monitoring information. The major contribution of UNICEF has been in advocating for rationalisation of the water quality indicators/Standards (MoH’s QCVN 02: 2009/BYT) from 20 plus to 11 only. The focus has been on prioritising those indicators that are critical for human health (such as e-coli, arsenic, nitrates and others), easy to manage and would require less resources. These, however, have not yet been approved. For UNICEF the key indicators of interest focus on O&M of RWSS, water quality and safety, safe sanitation (hygienic latrines), behavioural changes around water safety, hand washing, and latrine use. The NCERWASS official interviewed during the evaluation shared that prior to NTP-III there was only a very simple criterion for water quality. During the transition from NTP-II to NTP-III, UNICEF played an active role in securing the approval for NTP-III and shifting the focus of the GOVN from infrastructural support to water quality and safety. Under NTP-III, the monitoring system was centralized and internal, and was not accessible to external stakeholders, mainly covering the project. With the end of the NTP-III, the monitoring system was merged with the new rural development programme, a joint responsibility of all government entities according to their mandates. Review of Programme documents indicated that at national level, 30-40% rural water supply schemes are non-functional, which points to weaker O&M arrangements. The Evaluators did not have access to ‘MARD/NCERWASS managed Database developed with support of donors group, to ascertain this. However, the stakeholders that worked behind establishing the database are of the view that probably it is not being maintained as regularly as was the case during NTP III. The regular monitoring and updating of the database to keep track of functionality of schemes is apparently an unresolved issue, for which multiple models have been applied (like engaging private sector). Multiple stakeholders referred to the challenges around O&M for sustainable water supply and suggested that this challenge warrants an immediate and sustainable solution. The monitoring has substantiated the need for fixing the issue of O&M adequately. Together with Partnership Office and relevant ministries, UNICEF has facilitated developing common set of monitoring indicators for standardising the monitoring and reporting for water safety and quality, considered a major challenge earlier. Currently, no specific monitoring system exists that can collect, analyse and report on the progress in water treatment and storage practices by HHs, plausibly because of UNICEF’s interventions in the target provinces. Rural Sanitation (CLTS/ODF) Monitoring The monitoring system for rural sanitation has evolved ever since the public sector has taken lead in implementing CLTS/CATS. There are some elements of pre and post ODF monitoring, however, with significant gaps. The pre ODF monitoring is mostly community led, however, it lacks monitoring of triggering and progress on construction of new latrines. Periodic visits are undertaken by the local health workers, responsible for triggering. The monitoring system lacks tracking of social norm or slippage. The monitoring is paper based and consolidated at the provincial level and shared with VIHEMA for national level consolidation. Apparently, no centralised database exists for pre and post ODF monitoring. The most critical contribution by UNICEF so far has been the consolidation and finalisation of ODF verification, certification criteria and guidelines. The guidelines were approved in 2016 with an aim to assist in standardising the verification and certification processes, as and when provinces start implementing the drafted ‘Provincial ODF Plans’.

40
The hand washing with soap is being tracked through proxy indicators, such as availability of hand washing station (at household level) and availability of soap near the station. This practice is not being covered through regular ODF monitoring but through various national surveys. Viet Nam is one country where enormous amounts of data is gathered through regular monitoring and periodic surveys on children health, education, hygiene behaviours. The data is normally retained by the agencies that undertake data collection, however, it is not being used in a systematic way to correlate information across multiple indicators or sectors. For instance, the Evaluators, despite interest and focus on correlating WASH related information with child nutrition and health, could not carry out any meaningful analysis as a result of not having access to varied information sources. In view of the above, it could be concluded that the rural water supply monitoring has shown improvements, and analysis suggests that O&M systems should be strengthened. Rural sanitation related monitoring processes are still evolving and may require support in coming years to help government agencies track pre and post ODF monitoring, including social norms creation and slippage. The current monitoring system has not capitalised on the potential offered by the latest information technology options, to offer real-time monitoring data and analysis, including visual presentation. Moreover, the current system lacks capacities to perform cross-sectoral analysis such as linking water and sanitation to health and nutrition. The relevant ministries need technical assistance to improve monitoring systems and perform cross-sectoral analysis to advocate for relevant sector reforms. In regard to rural sanitation monitoring, pre and post ODF monitoring arrangements have taken some shape and are yet evolving and are therefore a ‘Work in Progress’. At Commune and community level, monitoring is currently implemented by the village health motivator, the Community Health Club (CHC), and the health system from the village to the provincial level. No formal checklists are in use for monitoring of progress and identification of key challenges during post-triggering and/or post-verification phase, instead the monitoring has been merged with the communication activities, where VHCs uses IEC materials during their door-to-door visits for motivating households to follow the sanitation practices. The guidelines on ODF verification and certification processes clearly articulate the mechanism for monitoring the ODF progress at village level and the flow of information to the upper levels to province. Generally, the process of upward communication from the Commune to the CPM at district level, to the provincial authorities, is unnecessarily lengthy and may take 1-2 months in routine and even more in some cases for ODF verification. MoH criteria for ODF verification requires that 70% of people in a community should have the hygienic latrines, and 95% of people should have improved latrines (including pour flush etc.), and the remaining 5% can have shared latrines. The monitoring checklist for inspecting a hygienic latrine is a simple/basic tool requiring the marking of certain parameters without providing any space to note down any other important observations, or qualitative findings about the usage of the latrines. Thus, no data is available on latrine usage and/or slippage (doing OD despite having latrine at home). A senior official from VIHEMA interviewed during evaluation expressed the need for continued support from UNICEF around monitoring and evaluation. Opportunities for Improving the Rural Sanitation Monitoring System: Some of the areas for improvements in the existing monitoring arrangements are discussed as follows:
1. Currently, there is no indicator on OD at the national level, the existing indicators are on the percentage of households with latrines and hygienic latrines, a significant gap in the monitoring system of rural sanitation. In the absence of a direct indicator for OD, the indicators for latrine availability and hygienic latrines are used as proxy indicators to calculate the rate of OD. VHIEMA views this gap as an area that requires UNICEF’s advocacy support to the relevant government departments to include an exclusive indicator to measure the OD rate, in the monitoring checklist. In most provinces, this data is on

41
hygienic latrines and not on ODF (which is not included in the monitoring templates), as ODF is a thematic reporting requirement and not a routine one. However, in the 32 provinces that have developed and adopted provincial ODF action plans, it has become mandatory. The province of Lao Cai has not yet formally adopted an ODF action plan.
2. The existing monitoring system for sanitation is not yet geared up to fulfil the safe sanitation standards of the SDG indicator #6. The MoH, VIHEMA, Department of Statistics and other related Ministries are working on preparing the baseline for the SDGs indicators. Simultaneously, the country is collaborating with the UNICEF/WHO Joint Monitoring Programme (JMP) to share progress updates on sanitation and other related indicators.
3. The current monitoring system around CLTS neither tracks the number of triggering events required in a village to achieve ODF, nor the average time taken for a community to achieve ODF status. The lack of focus on these aspects of CLTS implementation does not create any evidence on the effectiveness or quality of triggering and other CLTS processes, a significant gap that needs attention to help improve the overall effectiveness.
4. UNICEF Viet Nam CO faces limitations in its ability to conduct national level surveys due to availability of limited financial resources. Therefore, UNICEF is focusing mainly on upstream work along with some small projects to generate evidence. UNICEF is working with the Government to improve data collection and reporting systems. Viet Nam is facing challenges in evidence creation on the linkages between children’s health, nutrition, sanitation and hygienic behaviours. So far, only a few research initiatives49 by UNICEF and/or the government have been undertaken to assess the impact or outcome of water and sanitation related programmes on the health and nutrition status of children under five in particular.
Capacity Building of Public Stakeholders
UNICEF’s RSHP is primarily focused on developing government’s capacity at various levels in the delivery of rural water and sanitation services. UNICEF’s capacity development approach was not limited to only the conventional means of capacity development through training events etc., instead, it was multifaceted and comprised of initiatives such as providing technical inputs to government officials and entities to enhance their overall technical knowledge, planning and management skills. For example, in certain cases, UNICEF officials provided general guidance to public officials on how to develop the action plans on various aspects of the programme and then providing technical inputs in the form of review and feedback. Similarly, the advocacy meetings undertaken with government officials to highlight the importance of behaviour change communication, enhanced their understanding and led to the integration of communication activities into their routine implementation. UNICEF has been working in Viet Nam for a few decades and various capacity development initiatives under UNICEF’s RSHP were linked with the foundation of UNICEF’s earlier work with the government. For instance, since the introduction of CLTS to Viet Nam in 2008/9, UNICEF helped the national government (MoH, VIHEMA etc.) in organizing a ToT programme, the development of two manuals (CLTS manual and manual for CLTS Trainers) between 2009 to 2011. At the initiation of the current Programme (2012 – 2016), UNICEF also supported the targeted provinces to organize Training of Facilitators (ToF), a two-days long training. ToF also involved designated staff from MoET and teachers; and for a limited number of representatives from mass organizations (Women’s Union and Farmer’s Union etc.). The trained facilitators in turn deliver trainings to the village level ‘collaborators’, mostly health workers at the district and commune levels, volunteers from mass organizations, and teachers and members of the People’s Committee at the commune level. The training focuses on both enhancing the theoretical aspects of CLTS concepts (planning, triggering, communications etc.) and skill building through practical
49 In 2015, UNICEF Viet Nam supported MoH to conduct a study on” Impact Assessment of Water Supply and Sanitation Programmes on the Health and Diseases of Under Five Children” in Viet Nam; In 2010, UNICEF Viet Nam also supported MoH to conduct a study on “The Correlation between Household Environmental Sanitation, Household Water Supply, and Mothers’ Hygiene Behaviour for Children Under 5 and the Status of Child Nutrition in Viet Nam”. (Information shared by UNICEF Viet Nam Official)

42
demonstration of a triggering session, - a half day long session that helps participants gain real-life experience of how to prepare for and conduct triggering sessions. To strengthen VIHEMA’s technical and planning capacity for CLTS/ODF, UNICEF supported the engagement of a technical consultant in preparing the guidelines for the development of ODF action plans. In October 2016, VIHEMA organized training workshops in 19 provinces to guide the relevant officials in ODF action planning. Similarly, UNICEF has worked closely with MARD/NCERWASS to build their capacity in terms of introducing relevant policies and regulations around the water and sanitation subsectors. UNICEF’s engagement with the provincial governments has resulted in improved capacities for implementation at the lower tiers of government (district, commune, village). For example, some improvements are noted in the capacity development arrangements by the DHC at the district level during the period 2012 – 2016. The training duration for the village health collaborators (VHC) was extended from three months to six months and then further increased to nine months in 2016. UNICEF’s capacity development approach around conventional means is limited to financial and technical (content finalization, moderation support, coordination etc.) support in organizing training events, workshops etc., mostly at the national level and partially in some selected provinces. The provincial governments are responsible for mobilizing the required money and providing training for the staff at the district and sub-district levels. For CLTS implementation, the government follows a cascading model for capacity development of relevant staff (DHC, CPM, CHE, CHC, selected members of the CPC, village heads and the VHC) at various levels. Currently, the government has not yet allocated enough resources to train all health workers involved in hygiene promotion communication and triggering. The roll-out of CLTS cycle from ToT to ToF is dependent on the availability of funds from different programmes and projects which can be mobilized by a commune health centre within its own domain. There is a greater need to increase specific funds at health centre level for capacity development of the health workers involved in health education communication. It is anticipated that with the approval of the provincial ODF plans, health centres will get appropriate funds for CLTS implementation. A few officials including a representative from the World Bank, interviewed during the Evaluation, expressed their positive opinion on UNICEF’s role in enhancing the government’s capacity at the national and provincial levels. The WB’s representative also highlighted UNICEF’s role in solidifying the WB’s concept of commune-wise sanitation as part of the WB’s rural sanitation programming in Viet Nam. Furthermore, UNICEF’s efforts in improving the content developed for capacity development around rural sanitation (CLTS manual, SanMark manual and a booklet on latrine designs etc.) and knowledge sharing were also appreciated by senior officials of VIHEM, Master Trainers (CLTS) and the representative of WB. As per the feedback from the stakeholders, it could be concluded that the training-centric capacity development has proven effective in enabling public servants deliver on their anticipated or designated roles. Nevertheless, in absence of training assessment records and subsequent performance reviews, the Evaluators feel constrained to comment on the effectiveness of training. The institutionalisation of CLTS has been relatively more effective in cultivating ownership of approach and tools such as ODF standards, certification and verification guidelines, action plans etc. The government now owns CLTS as future approach for rural sanitation and has started exploring options for nurturing sanitation marketing as the vehicle to develop innovative solutions for water treatment and storage. RSHP implementation and results have persuaded national and provincial governments on the adoption, promotion and scale-up of these approaches for achieving national targets of water and sanitation. The evidence suggests weak research and knowledge management capacities in the public sector. The Programme has not addressed this gap adequately. This is evident from gaps in the documentation and knowledge management of UNICEF’s own programme and in particular capacity development initiatives, which would have bearing on leveraging future benefits of these

43
initiatives. For instance, database development remained a low priority to keep track of the number of CD events held, participant details etc. It is still unclear whether such records and information exist with the relevant public agencies.
EFFECTIVENESS OF PUBLIC SECTOR DELIVERY MECHANISMS
EQ#3: To what extent has UNICEF strengthened the public-sector lead delivery and contributed to knowledge, attitudes and practices improvements around key water safety, latrine use and hygiene behaviours e.g. handwashing with soap? Summary Assessment: To respond to the question of effectiveness vis-à-vis strengthening the public-sector delivery, Evaluators looked at rural water safety and rural sanitation separately. In relative terms, UNICEF’s contributions to improve rural sanitation are more visible, hence reflecting effectiveness, compared to rural water safety. Though UNICEF’s efforts have set the foundation well, achievements around improving the public services delivery for water safety are not much evident. The key contributions include supporting the annual ‘Joint/Water Sector Review’ events from 2012 until 2015. These reviews have enabled the government in identifying and flagging policy and operational issues around rural water supply and were used as advocacy tools by UNICEF. The advocacy to rationalise water quality standards (or parameters of assessment) could not make much headway. The ‘O&M Working Group’ was formed and continued functioning but with little success. Subject to limited documentation vis-à-vis results, the Evaluators are unable to comment on its effectiveness beyond a platform for discussion and advocacy. UNICEF succeeded in adding profile and recognition of water safety as a challenge and leveraged that sensitization to advocate and later assist in developing national and provincial ‘Water Safety Plans’. The plans are in draft form, however given their implementation these could potentially transform the water safety practices and support. One key contribution is evident in the form of government’s adoption and use of BCC interventions for water treatment and safe storage, which they have already started implementing in selected locations through public funds. The most significant and striking contribution has come in the form of supporting the ‘Entrepreneur led Low Cost Water Filtration Solution’. This is in the final stages of quality checks and approvals before its scale-up and stands out as a key achievement carrying huge potential in shaping up the future private sector involvement for water safety. However, the issues of O&M still remain unaddressed. The UNICEF’s contributions under RSHP to improve services delivery for rural sanitation are a highlight of UNICEF’s support and proved relatively more successful. The key contributions are in terms of defining the mandate and placing MoH/VIHEMA as lead for rural sanitation. Moreover, this has shifted focus from government supported (subsidy led) sanitation to community led programming. The successful roll-out of CLTS with enabling guidance such as training materials, C4D materials, guidelines for ODF certification etc, has facilitated institutionalisation of CLTS approach in Viet Nam. Consequently, implementation capacities of the government have increased and are somewhat adequate for up-scale with the possibility of being further enhanced. The increased capacities of the national ministries and the provincial governments is evident through the formulation of ‘Provincial ODF Plans’ (currently in draft form for some of the Provinces) and their implementation in near future will contribute to realising the vision of universal sanitation access in Viet Nam. The interest and capacities of relevant public-entities to improvise the BCC approaches and implementation (because of involvement in CLTS implementation in pilot provinces and villages), is high. Furthermore, the Programme has contributed in terms of promoting low cost designs and creating entrepreneurial interest within rural private sector to link up with the Programme, which will help future implementation and up-scaling of CLTS. The RSHP has contributed in accelerating the thirst for local solutions by encouraging improvisation of sanitary products and materials, also benefitting the local entrepreneurs by accelerating demand for sanitation goods and services. The technology innovation has yet to accomplish gender friendly, disability and disaster resilient latrine designs. Although, a few localised solutions to varied disaster risks have been offered, those have not been technically assessed thus far for resilience to multitude of disaster risks e.g. floods, landslides, etc. and compliance to MoH hygienic standards. Regarding RSHP effectiveness in realizing outcome level results i.e. accelerated access to improved sanitation (by encouraging people to construct latrines and abandon OD practice), and increased understanding of personal and environmental hygiene and associated behaviours

44
(handwashing with soap and the water safety practices), the qualitative interactions with provincial stakeholders suggest that the Programme has contributed in an increased access to water and sanitation services and an enhanced knowledge on water safety and other hygienic practices. When these qualitative assertions were corroborated with quantitative data, similar inferences can be drawn. However, due to limited documentation, the extent to which outcomes have been achieved remains unknown. Based on the qualitative evidences primarily, the evaluators may argue that the programme logic model or ToC is plausible. The Post-KAP HHS results demonstrate effectiveness of BCC/C4D campaigns and strong internalisation of messages translating into practice level changes. The effectiveness of behavioural change efforts through hygiene promotion is also demonstrated by the results of household survey, conducted as part of the evaluation. The HHS results indicate a significant level of practice of handwashing (67% and 62%) among survey respondents particularly before eating and after defecation respectively. Of those who practice handwashing, 83% of the responses indicate the use of soap, while 20% responses mentioned the use of powdered or liquid detergent for handwashing, indicating a very positive situation in the targeted communities. Find below the elaboration on the summary assessment for effectiveness (for Q 3).
Rural Water Services: Key Challenges & UNICEF Priorities
Viet Nam has been able to achieve MDG targets for water accessibility. As per MARD report (2015), 86% have had access to water. The access may not have been a challenge, but water quality has always been. Reportedly, only 37%- 40% water for domestic use meets the standards set by MoH. For rural areas, it is further aggravated by low piped water coverage; and reliance on un-protected water sources. The poor, including those living in remote areas, are the ones that are more likely to be using unclean/unprotected water, thus, having highest exposure to gastro-intestinal diseases (water borne) such as diarrhoea, cholera and others. Moreover, there are issues with O&M of public sector supported water schemes. For RSHP, at the national level the focus has been on advocating for rationalising the water quality monitoring standards and improving coordination between stakeholders to improve coordinated efforts to address O&M related challenges. At sub-national level, the support was intended to advocate and enable provincial governments to prioritise water safety (quality monitoring) in local planning. Moreover, UNICEF enabled provinces to formulate and implement behavioural change campaigns for safe water treatment and storage, as to create workable models of delivery to address water safety issues. UNICEF has supported with finding low cost and localised technology solutions. With UNICEF support, a local entrepreneurial venture has produced low cost i.e. 23 $ complete kit, ‘Clay Pot Ceramic Filter’ for household-based water treatment. The product was introduced to bring affordable household water safety solutions. The product has gone through trials and now awaits final accreditation before formal launch for scaling-up.
RSHP Contributions in Improved Public Services Delivery (Water Supply) Advocacy for Better Water Quality through Joint Sector Reviews: The first and foremost contribution has been the facilitation to organise ‘Joint Sectoral Reviews’ (yearly) for water supply sector from 2012-15. These have been jointly facilitated with other stakeholders such as the World Bank, DFID, DFAT and others. These reviews helped in identifying policy and operational challenges and generating debates on range of different solutions available. In a way, these enabled UNICEF to craft advocacy agenda with the government.
Support for Water Safety / Quality Standards: UNICEF has been advocating with MoH to rationalise the water quality monitoring standards (currently comprising of approximately 20-25 parameters including levels of calcium, potassium etc., the testing of which requires sophisticated technology) and focus on fewer parameters/indicators while ensuring that minimum standards of WHO for water safety and quality are fulfilled. This has been done to ease the water quality monitoring and ensure regularity. The advocacy efforts haven’t produced any significant results thus far.

45
Creation of O&M Working Group: UNICEF has been successful in advocating and creating an ‘O&M Multi-Stakeholders Working Group’ in 2014. The group has been created together with National Partnership Office at MARD and has been meeting regularly to debate around O&M issues and coordinating efforts of different stakeholders involved. UNICEF has been advocating for increased role of private sector for O&M in rural areas, and better contracting practices by the relevant authorities. So far, not much headway is made into setting guidelines for private sector engagement.
Development of Water Safety Plans: Another key achievement is the successful advocacy with national and provincial governments to formulate ‘National’ and ‘Provincial Water Safety Plans’. The plans are still in the draft form and not been approved to seek public financing; nevertheless, the plans have set the direction for prioritising water safety as part of public services delivery.
Promotion of Technology Innovation - Low Cost Water Treatment Options: One of the most significant contributions have come in the form of introducing low-cost technology options for water treatment. For that UNICEF has given support to a local entrepreneur to manufacture ‘Clay Pot Water Filter’, using local materials and technology. The filter has been pilot tested in one of the provinces and produced acceptable results. The complete kit would cost about 20$-25$, which is almost half the price of other branded filters available. The product is going through final accreditation tests before national launch. The product offers a good solution for people who don’t have access to more costly options and at the same time carries potential to generate jobs.
Enhanced focus on Behavioural Change Communication (BCC): The most salient contribution of UNICEF has been the increased focus on communication for behaviour change to influence the knowledge, attitudes and practices of households who are still relying on using unclean drinking water. In doing so, UNICEF succeeded in integrating safe water treatment and storage messages into communication activities of all sectoral programmes such as health, education, water and sanitation and DRR/climate change (emergency preparedness) etc. UNICEF has supported MoH to develop and implement BCC strategy and interventions for water safety. The public education programmes have disseminated messages around safe water storage and treatment. The KAP results demonstrate good understanding of significance of water treatment and how (options) to safely treat and store water. The stakeholders involved in field implementation are appreciative of UNICEF’s technical assistance in design and implementation of newer concepts and approaches for behaviour change.
Resource Mobilization: UNICEF's advocacy with the targeted provincial governments was successful in mobilizing some public funds for such activities. Regardless of the volume of funds channelized so far, the initiation of the trend to allocated public funds for BCC is a significant achievement. Qualitative findings reflect that the local governments in the targeted provinces are now improvising their means to secure appropriate funds for water related communication activities by appropriating funds from other sectoral programmes.
Private Sector Involvement for RWSS: UNICEF is supporting the MARD and the Partnership Office in their advocacy efforts to define and promote the role of the private sector in rural water and sanitation. In 2012, a technical consultant was engaged to support the formulation of the private sector related policy in 2012. UNICEF also supported the MARD, the MoH and the related departments (NCERWASS and VIHEMA) in the preparation and issuance of various directives and regulations in pursuit of the Prime Minister’s Decree on the increased socialization of the private sector in rural water supply sector.

46
Technology Innovation: A Success Story of Low Cost Entrepreneur led Water Filtration Solution: UNICEF’s most significant achievement is demonstrated by the introduction of a clay pot ceramic filter model to get safe drinking water for household consumption. Using regional experience from Cambodia and China, the ceramic filter model was adopted to fit in the Viet Nam context. UNICEF’s approach was to embed the promotion and use of this innovative model for water safety within government system.
Rural Sanitation Services: Challenges and UNICEF Priorities
UNICEF has made more significant contributions in strengthening the rural sanitation sector in Viet Nam. Rural sanitation faced multiple challenges, most significant being unclear policy on rural sanitation and in particular community led approaches, overlapping institutional mandates (between MARD and MoH), limitations around public sector approved training and operational guidelines and standards, limited trained human resource at all levels, disrupted and weak supply chain including high latrine construction costs i.e. around 300 USD/latrine, and insufficient awareness on low-cost latrine options. UNICEF worked at both national and sub-national levels to strengthen and accelerate the rural sanitation services. A significant contribution acknowledged by public stakeholders has been the revision of National WASH Strategy 2001-2020, whereby community led approaches (CLTS/CATS) have been recognised officially as preferred strategies for public sector support for rural sanitation. Also, UNICEF has apparently been instrumental in formulating a vision or target for rural sanitation. Viet Nam has pledged to turn the whole country ODF by 2025. This pledge was made during the ‘Sanitation and Water for All’ Summit in 2014. To facilitate the institutionalisation of CLTS, UNICEF has extended technical assistance to develop series of guidelines, standards
A Success Case under UNICEF’s RSHP UNICEF’s advocacy efforts succeeded in securing the endorsement and backstopping role of the NCERWASS and PCERWASS and DARD in An Giang province where this model was successfully implemented. For execution, UNICEF supported the NCERWASS in preparing the TORs for the engagement of a private sector entrepreneur for its pilot testing and onward implementation. UNICEF provided only a part of the overall required funds for the initiative and convinced the government to provide the remaining funds and take the overall responsibility for its management. Currently, the model is widely appreciated by the relevant authorities, and the communities who are now able to access clean and safe drinking water in the selected areas. The ceramic water filter is proving to be particularly valuable in the mountainous areas, where the use of untreated water continues to be an issue; in such areas, the ceramic water filters are replacing are replacing the slow sand filters which were previously promoted. The most salient feature of this ceramic filter is its ability to yield 99.99% bacteria free water, at a one-time cost of around 23-25 USD. Consultations with the entrepreneur are underway to further reduce the cost to 20 USD. The filters are disaster resistant, and each one is capable of filtering 2-4 litres per hour; the standard attached plastic container has a storage capacity of 30 litres and the system is simple to set up. So far, only one entrepreneur is involved in manufacturing of the ceramic filters and based on the success of his business, attempts are underway to expand its scope to include receptacles in the package through the involvement of the plastic manufacturing agencies. UNICEF plans to distribute Ceramic Filters free of cost in the rural schools and health centres with coordination and support from Women’s Union, and the Farmer’s Union to ensure that these filters only reach to the target institutions, but not to the individuals. At next step, UNICEF has plan to involve VBSP to introduce loan facility to help individual households who want to have water filter but cannot afford to buy it. “…developments regarding an increasing use of ceramic filters carries very good future for water safety and quality. Every home, and individuals who don’t have access to the pipe water, and the people who only have access to the surface wells, can still get 100% bacterial free water with the use of ceramic filter at household level” (A UNICEF Official). “…developments regarding an increasing use of ceramic filters carries very good future for water safety and quality. Every home, and individuals who don’t have access to the pipe water, and the people who only have access to the surface wells, they can still get 100% bacterial free water with the use of ceramic filter at household level”. (quote)

47
and training packages, including group of trained trainers. Moreover, UNICEF has worked with VIHEMA to formulate and apply ‘ODF verification and certification standards 2016’, while also helping provincial and district authorities through in field roll-out of CLTS in selected provinces. The pilot roll-outs have enabled assessing the effectiveness of operational guidelines and training modules, facilitating reviews and finalisation. The pilot roll-out and advocacy at national level has been pivotal in establishing MoH as the primary implementer of rural sanitation. In a way, this has helped addressing the ambiguities around institutional roles. UNICEF has successfully advocated and facilitated the development of ‘Provincial ODF Plans’, which are ready for final endorsement. Reportedly, only half of the provinces have produced these plans thus far. UNICEF has extended support in design and roll-out of low-cost latrine models and have produced guidelines for SanMark. The models are relatively more successful in the Mekong Delta region compared to others. A working group on SanMark at national level was created to accelerate dialogue and discussion for coordinated actions on SanMark. The uptake of low costs models in other areas is relatively slow for perception of family’s social status with that of latrine.
RSHP Contributions in Improved Public Services Delivery (Sanitation) Strengthening the International Collaboration: UNICEF has played a positive role in enhancing the visibility and participation of Viet Nam at the international forums and programmes such as ‘Sanitation and Water for All’ (SWA). With UNICEF’s support, the MARD and the MoH/VIHEMA joined SWA in 2014 and now Viet Nam is a member of the steering committee for the Programme. This partnership enabled the national government to set its national goal to eliminate OD by 2025 that was announced by the Vice-Minister for the MARD in a presentation soon after joining the Programme; prior to this announcement, Viet Nam did not have any such specific target for achieving nation-wide ODF.
Institutionalization of CLTS/CATS Approach for Rural Sanitation: UNICEF’s value additions are demonstrated through its financial support and technical inputs to MoH and VIHEMA for institutionalisation of the CLTS implementation processes within government system to make these effective at field level. Overall, the officials from MoH and VIHEMA were very appreciative of the fact that now the government departments are acknowledging the importance and value of CLTS processes for achieving better results. Starting from 2013, UNICEF supported MoH/VIHEMA in the development and piloting the ODF guidelines and procedures for verification and certification. Finally, in 2016, VIHEMA issued the ODF Verification/Certification Guidelines with the approval of MoH for country wide application. With UNICEF advocacy, MoH has also issued various administrative directives to all provinces for more investments into CLTS implementation and other aspects of rural sanitation.
Clarifying Institutional Mandates & Setting Road Maps: UNICEF’s coordination with the two key ministries, namely MARD and MoH, has helped in establishing a clear mandate for rural water and sanitation service delivery. UNICEF and WHO collaborated to involve the two ministries in applying joint efforts and providing technical inputs for the preparation of the national water safety plan. Later, the Ministry of Construction (MoC) was also involved in the finalization and approval of the plan. The plan requires that water safety be assured at three levels: at the source, during distribution, and at the point of use. The implementation and operationalization of the plan is a considerable challenge, with MoC as the lead designated entity to implement water safety standards through MARD for its significant experience of water safety related work. An official from the WB shared that at the national level, the MoH is overworked and has a limited budget. The nature of the collaboration between the MARD and MoH is unclear, and there is a need for increased collaboration and coordination between the two ministries and to work with other ministries, such as the MoET, as well.
Development of Provincial ODF Plans: Keeping the 2025 commitment to eliminate OD under ‘high’ priority and with the ODF Verification Guidelines in hand, UNICEF’s current efforts are focused on strengthening VIHEMA’s role in enabling the provincial CPMs to develop the provincial ODF action plans by improving their understanding of the importance and processes of ODF. On completion and approval of the ODF plans, the CPMs will be required to mobilize sufficient resources for the

48
planned ODF activities. At present, VIHEMA is supporting between 30-35 provinces in developing five-years ODF action plans. Reportedly, only half of the UNICEF targeted provinces have produced these plans thus far. At the national level, UNICEF is supporting the MoH in developing a multi-year (2017-2021) umbrella programme called the Budgeted Sanitation Programme. The programme will incorporate the provincial ODF action plans and will include them in the budget; this budget will be used to support the provinces in implementing the provincial ODF action plans. VIHEMA also considers the ODF national roadmap as a crucial document since it sets yearly targets for ODF. At provincial level, Department of Health (DoH) is mainly responsible for overall planning, guidance, standardization, supervision and financing etc. and CPM is the actual implementer of CLTS processes. UNICEF’s technical inputs have improved the planning and resource mobilization processes by the provincial and district governments in setting their current and future ODF agenda. The ODF targets for the district level are set at the provincial level as part of the provincial ODF action plan.
ODF Verification and Certification Guidelines: Contradictory to the ODF guidelines, the verification and certification process is very slow and may take 1-2 years after the village has declared itself as ODF. The major reasons are the weak follow-up of the procedural requirements from Commune level to district government and the waiting time for organizing a district-level ODF Ceremony event for multiple villages that has been verified as ODF. Though, the ODF guidelines by MoH duly emphasize on post-triggering monitoring, but in practice, it is done by the community level monitoring team in coordination with the head of village. No dedicated staff from local health facility has been assigned this responsibility. For ODF certification, the team goes to every household to find the level of compliance with the ODF criteria. In case if some non-compliance is found, the certification can be denied making sure that self-declaration should not happen until the entire situation is fully ODF in practice. No assessment or study has been conducted to see the extent of slippage over time in ODF communities. The ODF certification so far is done at village level only (with exceptions of only two communes with its all villages achieving ODF status; one each in Dien Bien and Ninh Thuan Provinces), even though the ODF guidelines (issued by MoH) also refers to commune level and district level ODF certification. The ODF certifications at these two levels (commune and district) is not in practice yet, reflecting a gap in the compliance with the ODF certification guidelines.
Improving Community Mobilisation Processes and Ownership: At community level, formal forums/groups (commune/village level sanitation and/or water supply group/forum/committee) that are officially recognized by and held accountable to local government have not been established to implement and oversee the CLTS implementation. The establishment of such formal forums with defined composition, role and responsibilities i.e. specific TORs, standard operating procedures, and stipulated requirements for proper record keeping and documentation, (activity register for the planned and completed activities, meeting minutes and reporting formats etc.) adds to the effectiveness of the CLTS processes by strengthening the community-led planning, execution and monitoring of ODF progress and rate of slippage overtime (post-ODF sustainability). Establishing such forums and linking them formally with local administration at commune level enhances accountability within community itself and creates opportunities for maintaining documentation of good practices and lessons learnt in the application of CLTS among these communities. With the presence of formally recognised forum/s at community level, the decision makers can plan better the capacity development of and technical support to the communities. This approach for community engagement also corresponds to basic principles of CLTS as prescribed by Kamal Kar’s CLTS handbook50. It is important that the community committee is created to mobilize and monitor the entire community throughout the process until certification is achieved and for planning and implementing post-ODF activities.
50 Kamal Kar & Robert Chambers (2008); Handbook on Community-led Total Sanitation. http://www.communityledtotalsanitation.org/sites/communityledtotalsanitation.org/files/cltshandbook.pdf

49
However, an informal group comprising of 6-8 people has been formed at village and commune level to facilitate the overall planning and implementation of CLTS activities. These people are selected because they are from within the community and are familiar with community members and the local context. These selected people play a key role in logistics and technical planning of the activities. Some communes have larger memberships; for example, in certain communes where local government has partnership with Red Cross, the team may have around 12 CLTS members including the village heads.
Community Participation in Programme Activities: The HHS results reflect a satisfactory level (63%) of involvement and participation of communities in CLTS activities, such as follow-up visits to households, village level meetings and behaviour change communication sessions. Overall results are encouraging since greater community participation is a key determinant of the ODF achievements and is fundamental to sustain the achievements. Two third (63%) level of community participation strongly corresponds to the participatory implementation approach by the implementers.
Table 3.2: Percentage of HHS reporting community participation in programme activities
Indicator Overall
(%) Percent distribution of households reporting participation in meeting about sanitation and during visit of government official regarding construction of a latrine.
63
Percent distribution of households received sufficient information (awareness messages, supplies, mason etc.) helpful to construct a latrine by province
73
Distribution of households able to recall three key messages learned/practice in the participated meeting.
40
On the outreach of communication messages, a significant level (73%) of respondents claimed that they have received sufficient information regarding latrine construction (See Table 3.2). This situation is in line with the views of the officials interviewed by the evaluations that most people have access to the required information and skills to construct latrines. Of those who did participate in meeting, 40% reported that they are able to recall the key messages of the meetings attended by them.
CLTS Implementation Challenges: The current CLTS implementation approach faces few challenges in relation to the local context and the communities. For example, the villagers (after triggering) are introduced to different models of hygienic latrines. At the same time, many villagers tend to feel that the pour-flush model is the most desirable model, but not all poor households can afford pour-flush latrines. In addition, some ethnic minorities live in water scarce areas (where water is mostly available in the rainy season) and pour-flush latrines are not the best option for such areas, as the design requires availability of sufficient water for its proper cleaning and overall functioning. People can fail to anticipate the long-term consequences of choosing the expensive pour-flush design over one which is more suitable to their environment. To address the issue, people living in such water-scarce areas were educated during triggering sessions that ‘dry latrine’ is the only appropriate option for these areas, and so they were encouraged to use dry pit latrine instead of using other pour-flush designs. Another challenge is that routine cleaning and maintenance of pour-flush latrine design can be difficult for people not used to owning standardized latrines. Community participation in the triggering event is generally low, varying from area to area and depends upon: the number of households in any village level; the level and quality of initial planning and preparatory work, the skills, training and motivation of the personnel involved in socialization; and mobilization of community members. Some other factors are the presence of ethnic minorities and the community’s general perception and understanding about the sanitation issue. For example, in areas where people from ‘Tay’ minority group are more concentrated, the participation is good because the community values sanitation and demonstrate a good level of awareness of sanitation issues. Whereas, for some areas such as those inhabited by ‘Hmong’ people, the level of participation is less, due to their low perceived value of the sanitation issue. Overall, the average

50
level of community participation in a typical triggering session is not very encouraging and varies from a quarter to one half of the total number of households in the village; generally, one household is represented by one member. Most officials met during interviews showed their concerns about the quality of triggering. Despite years-long investments for preparing a large pool of master trainers, there are only a handful of people who can conduct effective triggering which calls for the attention of the provincial/district level planners. One plausible reason shared is the unwillingness of most people to moderate triggering session, even those who have received trainings on CLTS. The possible factors for such unwillingness is the lack of confidence and practical experience of undertaking triggering. Such a situation raises questions on the outcome of the training and needs deliberations on changing the capacity development strategy to make it more effective and efficient.
Sanitation marketing – latrine designs, low costs models
Development of SanMark Manual In order to achieve and/or improve the outcomes of CLTS, effective triggering is only the first step to create demand for sanitation; post-triggering actions are key to increasing the commitment of communities and building awareness of the importance of sanitation and hygiene. In post-triggering phase, in order to effectively respond to the heightened demand, it is vital to ensure the availability of appropriate skills, sanitation supplies and other enabling environment at village/community level to help households start constructing latrines. For this reason, UNICEF advocated with MoH/VIHEMA to focus on strengthening the supply chain through SanMark promotion. In doing so, UNICEF worked with the MoH to engage a Civil Engineering Institute/University for developing a SanMark manual. Resultantly, the availability of manual has provided the basis for the promotion and strengthening of sanitation marketing, since the manual development process included a formative research on the available options for low-cost sanitation. The university undertook a series of consultations in 6 provinces (covering different geographic regions and contexts across the country) to study commonly used and available materials, latrine types etc., to inform the manual development. At the same time, UNICEF drew upon its knowledge of best practices form other countries, such as Bangladesh, Laos and Cambodia, to determine the best superstructure and sub-structure options for latrines in the context of Viet Nam. Once developed, the manual was shared with the provinces to guide the planning and implementation of activities related to improve the supply chain situation (SanMark). The provincial governments were encouraged to adapt the guidelines provided by the MoH to the local context. The manual covers various kinds of low-cost latrine designs to be used in different contexts, such as drought prone regions and areas at risk of flooding. It must be noted however that the adoption of these designs by relevant local authorities is not much visible and could not go beyond introducing these designs during awareness raising sessions while implementing the CLTS activities.
Accelerating Private Sector Engagement through Sanitation Entrepreneurs SanMark is a relatively new addition to the rural sanitation approach in Viet Nam and involvement of private entrepreneurs at community level for sanitation were previously non-existent before UNICEF’s Programme. UNICEF advocated with VIHEMA to promote and engage (with a relative degree of success) private entrepreneurs to make low-cost latrine designs commercially available. Currently, in the UNICEF’s targeted communes many such enterprises have emerged and gradually increased with time. Nevertheless, UNICEF was unable to develop any notable model of engagement with private sanitation enterprises or manufacturers for improved access to sanitation materials. This could be attributed to limited focus and inadequate dissemination of sanitation marketing related interventions. On a whole, UNICEF’s collaboration with MoH/VIHEMA has enabled VIHEMA in understanding the need for and the concept of SanMark and therefore integrating SanMark into the sanitation policy and developing SanMark guidelines for the provinces. Currently, VIHEMA through CPM at provincial and district levels is supporting the local government in operationalization of the guidelines for establishing supply chains.

51
Low Cost Latrine Designs and Sanitation Supplies UNICEF’s efforts were focused in reducing the average cost for latrine construction. In doing so, UNICEF supported provincial governments in undertaking training for local masons and other artisans to enhance their skills in the use of local materials for latrine construction. The officials from VIHEMA and UNICEF have highlighted the shared opinion based on their filed observations during field visits, that the trained masons are applying their new skills for low-cost latrine construction. Partly because of these efforts, the average construction cost of a normal latrine has dropped from 50-100 USD to 30 – 50 USD in some of UNICEF’s intervention areas - a notable achievement. However, for expensive type of latrines, average cost is still high at around 300 USD and even more depending on the design. A notable example is the Dien Bien province where UNICEF worked with a local architect to design a low-cost alternative to the usual type of latrine constructed in schools. Making use of local materials such as bamboo, the architect was able to design a latrine with a total (estimated) cost of 4000-5000 USD, significantly lower than the 20,000 USD required to construct the traditional kind of latrine51 in public schools. UNICEF did note however that there is a need to study this low-cost model to check the degree of compliance with safety parameters before considering replication and scale-up in other locations. Beside these improvements/developments, commonly used sanitary materials - often required for the construction of generally preferred latrine types - are easily available to communes close to the urban areas. The access to sanitary materials in rural areas is generally a challenge since these are mostly available at the district level. Yet, certain sanitary materials like ‘concrete ring’ which is the most integral part of the latrine, is generally locally manufactured and thus easily available. Therefore, the availability of commonly used sanitary materials is not a high-priority issue in most areas of Viet Nam, except for the remote rural communes.
Findings from Household Survey (HHS): The success of UNICEF’s and the Government’s focus on rural sanitation, particularly SanMark, is also reflected by the fact that a reasonable proportion (17%) of respondents have claimed to have upgraded their latrine in the last three years (Table 3.3).
Table 3.3: Percentage distribution of households' access to sanitation
Indicator Overall (%) Latrine Existence 97
Practice of Sharing of Toilet Facility 2
Respondents that Claim that they have Upgraded their Latrine in last 3 years
17
Overall, the situation around the availability of sanitary materials and supplies for constructing toilet is not encouraging as almost half of the respondents (43%) indicated that they have to travel at district level for purchasing sanitary supplies/items required for the construction of toilets. Such a situation contributes to increasing the overall latrine construction costs due to the high logistics costs involved. Moreover, the access to sanitary supplies is not encouraging at village and commune level since, only one in three (33%) person can purchase such sanitary items within or nearby their village whereas one in four (22%) can access these supplies at commune level (See Table 3.4). Although survey results indicate that sanitary supplies are available at three levels, a lot of efforts are required to further strengthen supply chain of sanitary supplies, particularly at village and commune level. For this purpose, the role of the local entrepreneurs needs to be enhanced. Such a development can help the poor to access sanitary supplies without spending much on logistics, thereby contributing to improving the equity aspects of the programming.
51 Extracted from ddiscussion with UNICEF WASH Officer – exact number of latrine is unknown – it could be latrine set comprising of multiple compartments?)

52
Table 3.4: Percent distribution of respondents reporting their knowledge regarding place where sanitary materials and supplies for constructing
toilets are available for purchase Place of Availability of Sanitary Materials and Supplies to
be Purchased Overall
% Within or nearby your village/community 33
At commune level 22
At district level 43
Don’t know 2
Total 100
Survey results indicate that of those who have latrine at home, a majority (66%) of respondents were aware of the options to receive any kind of assistance (including loans, grants/gifts/ subsidies or in-kind support). The awareness level (56%) decreases among those who do not have not yet constructed latrine at home. Overall, the awareness level seems at reasonable level (56% to 66%) for those who wants to get any assistance for latrine construction. The plausible reasons could be, the existence of a general awareness about VBSP’s loan options for water and sanitation at community level, and exposure of community members to governments’ other ‘social support’ programme/s for financial assistance or other subsidies in past. Further analysis shows, 57% of those who are aware of any form of assistance, have received assistance, however, the source of the received assistance is not established through the survey. In general, it can be inferred that the SanMark promotion related efforts of the programme have contributed to a satisfactory level of awareness at community level, however, it needs further improvements because availability of any form of assistance is a crucial aspect for equity focused programming (See Table 3.5).
Table 3.5: Percentage of households reporting level of awareness about available assistance options to build a latrine
Indicator Overall
% *Awareness of any available options to receive any assistance to build a latrine (have latrine at home)
66
**Recipient of any assistance to help you build a latrine (respondents have latrine at home)
57
Awareness of any available options to receive any assistance to build a latrine (respondents without any latrine at home)
56
The survey results endorse the above stated plausible reason of awareness for options to receive assistance, where 65% of respondents (see Table 3.6) who have received any assistance reported to have received loan, however, it does not necessarily reflect VBSP loan.
Table 3.6: Percentage of respondents reporting type of assistance received to build a latrine
Type of Assistance Received to Build a Latrine Overall
% Loan 65
Grant/gift/subsidy 31
Construction material/in-kind support 4
Total 100
Collaborative Work with World Bank’s Rural Sanitation Programming Another key achievement of UNICEF’s rural sanitation Programme in Viet Nam is its role in influencing the World Bank’s approach on rural sanitation. The collaboration between two entities has resulted in the concept of “one stop sanitary shop” within WB’s sanitation Programme. Currently, WB is supporting the local administration in establishing such sanitary outlets in rural areas to facilitate easy access to sanitary materials particularly in the rural areas of the remote and deprived regions in 21 Provinces under the WB’s Programme.

53
Communication for Development
One of the key features of the CLTS approach is its focus on changing people’s behaviour, rather than just focusing on latrine construction. UNICEF’s programming approach in Viet Nam prioritized this aspect to bring about a programming shift in the rural water and sanitation sector. The success is demonstrated by a change in the Government’s (MoH and VIHEMA) attitude on the prioritization of behaviour change communication in the Government’s programming. The MoH was initially reluctant to increase its focus on anti-OD BCC due to a lack of evidence for the effectiveness of such strategies in the context of Viet Nam, despite the proven effectiveness of such strategies across many countries with similar contexts. UNICEF spent around a year demonstrating the success of BCC in Viet Nam through pilots and convincing the MoH to adopt the approach. In doing so, UNICEF advocated to provincial governments for an increased focus on communication activities, emphasizing on two-way interactions with the target groups at the community level and to integrate the social norm approach into the communication approach. UNICEF’s key accomplishments in strengthening the communication approach of the Government are as follows:
UNICEF developed a national communication strategy to promote water safety and quality at the household level. The strategy includes messages on household water treatment, such as the use of the boiling technique in the absence of other appropriate solutions for making water clean and drinkable. These messages were integrated into water safety plans being implemented at the district and commune levels.
UNICEF helped VIHEMA in developing BCC guidelines and messages. UNICEF supported the VIHEMA in the development of a manual on low-cost latrines,
including the images and relevant information on latrine designs. Using this manual, the provincial CPMs developed communication materials that fit the provincial context. Key aspects highlighted through these materials are the features of hygienic latrines, the appropriate use of latrines, four types of latrines and the costs involved.
In order to strengthen the Government’s capacity to implement BCC, UNICEF conducted behaviour change communication trainings in the seven selected provinces on water, sanitation, health, nutrition and education. Additionally, some advocacy materials, such as video clips, were developed by UNICEF to target high-level decision-makers including members of Parliament.
During the RSHP period, UNICEF focused on strengthening the communication for development (C4D) component to improve the cross-sectoral integration of communication. An integrated package of C4D was developed by UNICEF through the collaborative efforts of all sections. UNICEF worked closely with the provincial governments for the adoption of this integrated package. For example, UNICEF succeeded in incorporating hygiene education messages, including messages on HWWS, into school-based activities while working with the MoET and MoH.
In 2016, during drought and salt intrusion at multiple locations in the Mekong Delta and the South-Central Highlands, UNICEF’s communication team collaborated with other members of the WASH working group (led by UNICEF) in the design and implementation of the communication activities. In addition to the DRR messages and the promotion of healthy behaviours (especially HWWS), the messages on water treatment and storage were integrated because ensuring the availability of drinking water of acceptable quality in drought affected areas or water scarce areas is challenging.
Qualitative findings suggest that Government officials were positive about the use of IEC materials in making communication effective. For example, in one particularly challenging area of the Bac Ha district in Lao Cai, with a Hmong people majority, the DHC noted a significant increase in public awareness about the importance of maintaining sanitary conditions by building hygienic latrines due to the use of IEC materials and interactive communication methods. The HHS results indicate
Box # 06: “wherever behaviour change communication was emphasized and applied appropriately, it is marked with significant success. A significant change in communities’ behaviours is visible in the field but that is not a major concern, the real challenge is how to scale it up.”

54
that: 1) 63% of households reported participation in meeting about sanitation and during visit of government official regarding construction of a latrine; 2) 73% of households received sufficient information (awareness messages, supplies, mason etc.) helpful to construct a latrine; 3) 40% of households were able to recall three key messages learned/practice in the participated meeting; and 4) almost half (45%) of respondents claimed that they have received hygiene and toilet related required information from interaction with village level leadership and/or by attending some village level meeting, indicating the outreach and effectiveness of the communication approaches as well as the participatory nature of the programme implementation. The HHS results indicate the latrine presence at 97% of HHs respondents; of those respondents who reported having a toilet in the home, the three most commonly stated reasons of having latrine at home are: 1) ‘cleaner and healthier living in our home’ (70%); 2) ‘convenience’ (48%) and 3) ‘for good health/disease prevention’ (36%). Taken together, it suggests that a significant proportion of people (36 to 70%) are aware of the health, hygiene and convenience related benefits of having and using latrines at home (Table 3.7).
Table 3.7: Percent distribution of respondents reporting reasons for using a toilet facility
Reasons for Using Toilet Facility Overall
Yes % For good health/disease prevention 157 36 Cleaner and healthier living in our home 304 70 Convenience 210 48
Multiple response question (N=434)
Hygiene Promotion - Behavioural Change Communication The HHS results indicate that in addition to the electronic medium such as television and radio, the local authorities and the village meetings are the most cited sources of information. Collectively, a high proportion (45%) of respondents claim that they get hygiene and toilet related required information from interaction with village level leadership and/or by attending some village level meeting (see Table 3.8), indicating the participatory nature of the programme implementation. These trusted sources should be continuously emphasized in future in the design and execution of behaviour change communication campaigns. However, further results indicate a worrying element in the form of limited reference made to health workers (8%) and ‘local public-address system’ (4%) as a means to get required information. Apparently, the effectiveness of the involvement of health workers for dissemination of communication messages needs to be assessed for taking corrective actions, to enhance the role of the health workers.
Table 3.8: Percentage distribution of respondents regarding their preferences and trust of the source of information about hygiene and toilets by end line (province)
What are the Sources of Information Through Which You Get Information About Hygiene and Toilet
Dong Thap
Lao Cai Ninh
Thuan Overall
% % % %
Television/Radio 15 22 25 21
Commune/Village meetings 13 22 13 16
Local authority (head of village) 30 34 22 29
Which sources of information you trust/prefer the most than others?
Television/Radio 27 18 37 28
Commune/Village meetings 10 21 11 14
Local authority (head of village) 26 32 29 29

55
Handwashing with Soap (HWWS) The description below indicates key findings on handwashing practice at household level. In addition to self-reporting by the survey respondents, the findings are supported by ‘direct observations’, made by enumerators as part of HHS. The enumerators were asked to seek permission and make four (04) key observations52 that relate to handwashing practice and situation at household level. The promotion of HWWS is a critical element of hygiene promotion. The HHS results indicate a significant level of the practice of handwashing particularly before eating and after defecation. Out of all responses, two in every three people (67% and 62%) responded practicing handwashing before eating and after defecation respectively. This reflects the high level of awareness on the importance of handwashing and correspondingly the practice as well. However, handwashing practices at other key instances (mostly related with female members), require more improvements as reported by the HHS results at 32% for ‘before cooking’, 11% ‘before feeding a baby/child’, and 6% ‘after cleaning a baby (see Table 3.9). Collectively, 49% of respondents were practicing handwashing at these crucial moments while dealing with the children. The survey results visibly demonstrate the success of the hygiene promotion contributing to the improved status of the awareness and practices of the respondents.
Table 3.9: Percent distribution of respondents reporting times for handwashing
When do you usually wash your hands Overall
N % When they are visibly dirty 206 47
When they smell or are sticky 55 13
Before cooking 138 32
Before eating 292 67
Before feeding a baby/child 47 11
After defecation 268 62
After cleaning a baby after that has defecated 27 6
After work 201 46
Others 87 20
Multiple response question (N=434)
The benefits of handwashing are increased manifold when done by using soap or any other cleansing agent for handwashing, therefore promotion of HWWS is noted as one of the focus areas under hygiene promotion component. Of those who claim to practice handwashing, 83% of the responses (see Table 3.10) were about the use of soap for handwashing, while 20% responses mentioned the use of powdered or liquid detergent. An important observation is the fact that the Programme had failed to promote any traditional method such as Ash and Dirt/mud/sand etc., for handwashing in case of unavailability of soap. The use of any such traditional method does not involve any costs for its use, hence needs to be promoted in parallel as an alternate to soap or liquid detergent. This aspect is of particular importance for the poor who cannot always afford to buy soap. The above mentioned self-reported survey results mostly correlate with ‘direct observations’ made by the enumerators (see Table 3.10A and 3.10B) as almost all (99%) HHS have some designated or non-designated place for handwashing (located within 10 paces of kitchen at 33%; within 10 paces of the toilet facility at 44%; and 22% elsewhere in home/yard or some other place) and almost all (98%) HHS were observed having water for handwashing. Moreover, 85% HHS (see Table 3.11) were observed with some cleansing agent (soap 40% and/or powdered or liquid detergent 44% and others 1%) for handwashing purpose.
52 *OHW1 - Can you show me where members of your family most often wash their hands? *OHW2 - Is water present at the specified place for hand washing? *OHW3 - Is soap or detergent present at the specific place for hand washing? *OHW4 - Can you now show me how you usually wash your hands?

56
Table 3.10: Percent distribution of respondents reporting items usually used for
washing hands
Table 3.10A: Percent distribution of respondents observed for presence of water for
handwashing by province and gender
Self-Reported Item Usually Used for Washing
Hands
Overall Observation Based Water presence for handwashing
Overall
N % N %
Soap 357 83 Water is available 419 98
Powdered or liquid detergent 87 20 Water is not available 9 2
Ash 2 0 Dirt/mud/sand 2 0 Others 11 3 Multiple response question (N=432)
Table 3.10B: Percent distribution of households observed for place of Handwashing
Observed Location of Handwashing place
Overall N N
Within 10 paces of the kitchen/cooking place
142 33
Within 10 paces of the toilet facility 184 44 Elsewhere in home or yard 17 4 Outside of yard 58 14 No specific place 1 0 No permission to see 2 1 Others 23 4
Total 427 100
Table 3.11: Percent distribution of households observed with some
cleansing agent at specific place for handwashing
Soap/detergent for handwashing Overall
N % Bar Soap 171 40 Detergent (Powder/liquid/paste) 134 31 Liquid Soap (including shampoo) 54 13 None available 64 15 Others 5 1
The most commonly reported reasons for choosing to wash hands include ‘to be clean’ (85%) and ‘to prevent the spread of diseases’ (59%) as shown in Table 3.12. However, the cumulative response to the reasons that ‘it was the right thing to do’ and ‘that is what everyone does’ are weak aspects of the respondents’ awareness and understanding of the issue. Such a weakness can be addressed by integrating relevant messages in the behavioural change communication messages to enhance the overall understanding of the communities.
Table 3.12: Percent distribution of respondents reporting reasons for washing of hands
Reasons for Washing Hands Overall
N % To prevent the spread of disease 254 59
To be clean 368 85
To smell good 61 14
To get rid of dirt/smell/sticky/ things on my hands 90 21
Religious reasons/beliefs 1 0
Was told it was the right thing to do 25 6
Because that is what everyone does 25 6

57
Table 3.12: Percent distribution of respondents reporting reasons for washing of hands
Reasons for Washing Hands Overall
N % Others 18 4
Multiple response question (N=434)
Overall, the results of the KAP relating to HWWS indicate that further efforts are required to strengthen handwashing related interventions, both to encourage the use of soap and to ensure that hands are always washed at ‘critical moments’ by all community members to the extent that the practice of HWWS is established as a social norm.
Awareness for Protecting Children from Diarrhoea With respect to level of awareness on ways to protect young children against diarrhoea, out of all responses the highest proportion (52%) of responses were about water treatment methods. This shows a reasonable level of understanding of the respondents on the importance of boiling or of using any other water treatment methods. The other highest recorded category of responses is the ‘hand washing with soap’ practice. Almost every third response (39%) highlighted this, indicating towards a satisfactory level of understanding of the respondents about the need for ‘handwashing with soap’ as crucial for protecting children from diarrhoea. Moreover, a high proportion of responses were about food handling and storage practices, indicating the respondents’ understanding on the importance of appropriate food handling in relation to protecting children from diarrhoea. However, despite such a good level of overall understanding on multiple aspects of water treatment and food handling, a low percentage (13%) of responses were recorded about respondents’ attitude for ‘disposing the Children’s faeces in latrines’ as a protective measure to safeguard children’s’ health, a situation requiring more concentrated efforts to include such messages in hygiene promotion campaigning (see Table 3.13).
Table 3.13: Percent distribution of respondents reporting awareness of ways to protect children against diarrhoea
Ways to Protect Children Against Diarrhoea Overall
N % Boil or treat your water 224 52%
Use latrines/dispose faeces of children in latrines 57 13%
Wash hands with soap and water 169 39%
Cook food well 201 46%
Store food properly/cover well 70 16%
Buy from a clean place/not buying food from random place 37 9%
Wash fruits/vegetables with potable water 48 11%
There is not nothing you can do 2 0%
Others 68 16%
Multiple response question (N=434)
At the same time, some government officials highlighted the challenges in the tracking of BCC outcomes, as there is no tool available to the Government to regularly assess behavioural changes before and after the BCC interventions, albeit some proxy-indicators, such as the number of people with latrines, are used to assess the effectiveness of BCC interventions. Overall, UNICEF succeeded in shifting the Government’s focus towards BCC. Some of UNICEF’s key accomplishments include the development of a national communication strategy to promote water safety and quality at the household level; integration of these messages into water safety plans and development of BCC guidelines and various IEC materials by VIHEMA; trainings on BCC at the provincial level. UNICEF also supported the cross-sectoral integration of

58
communication internally (across the CP, WASH, nutrition, health and education sections). UNICEF promoted the integration of communication on water safety and quality during emergencies and in regular school activities. The assessment of the effectiveness of the communication is largely an ignored area. In the absence of outcome level tracking, proxy-indicators (increasing trend of latrine existence and usage) are used to judge the effectiveness of the communication efforts. However, qualitative findings show that the government officials find BCC interventions to be successful. The Evaluators are of the view that the current BCC approach does not fully leverage the potential of key influencers, such as mothers, in bringing about behaviour change. Simply raising awareness of hygiene issues or ensuring that a handwashing point is available is not enough to bring about long-term behaviour change. A successful communication strategy must be built on a deep understanding of the context and awareness of the enablers (such as key influencers) and disablers of the behaviour to be changed.
Programme Effectiveness vis a vis Results against Key Indicators
A Post-KAP household survey (HHS) was conducted by the Evaluators as part of the end line component of this evaluation. The HHS was administered to a total of 434 households in all the three provinces (Dong Thap, Lao Cai, Ninh Thuan). The Sampling methods and distribution applied for the HHS is attached as Appendix 3; only ODF communities were initially planned for inclusion in the survey. Out of the total HHS covered, equal number of respondents were selected from all the three provinces (Dong Thap 33%; Lao Cai 34%; Ninh Thuan 33%). Around 56% of the respondents are female and 44% are males. The analysis of HHS is done separately for all the three provinces and key results of HHS have been presented in Appendix 13. Where appropriate, findings of HHS have been related to UNICEF contributions to improved knowledge, attitudes and practices around access and practices of households/communities around water, sanitation, and hygiene. The non-availability of baseline data on the indicators that have been referred to in the section below, limits evaluators’ judgement on the extent/degree of improvements owing to, and, during RSHP implementation. However, HHS results intend to give a reflection of the current situation post-RSHP implementation. The provincial stakeholders in all three provinces referred to the Programme as whole to have contributed towards accelerated access to sanitation (by encouraging people to construct latrines and abandon OD practice), and increased understanding of personal and environmental hygiene and associated behaviours (including water safety) and to a degree the practice level changes. The communities shared similar views in terms of Programme interventions encouraging families to construct/upgrade latrines. There was wider appreciation for community education interventions contributing to understanding significance and desired practices to avoid disease. As part of the evaluation, the evaluators referred to the reliable secondary data (MICS and UNICEF/WHO JMP, other national surveys report and Post-KAP HHS results) to ascertain and quantify these perceived changes. The assessment took three key indicators i.e. access to improved water, access to improved sanitation, and adoption of (practice) handwashing with soap to track and rationalise changes over time i.e. from 2011 to 2016 (as part of before and after sub-design used for evaluation). The evaluators looked at different reliable WASH related secondary sources and found out that MICS data is available for 2011 and 2014 only. The JMP data is available for 2011 to 2015, so was the WDI data. None of these had data for 2016-17. The JMP data offered limited desegregation, as the evaluators could either find national averages or rural averages. MICS data offered the disaggregated data for regions but not for provinces (the preferred unit of assessment for evaluation). This came across as a key limitation and constrained the evaluators to do any meaningful longitudinal and comparative analysis for indicators of interest. The data limitations constrained the evaluators to establish conclusively if and to what extent RSHP contributed towards accelerated access to improved water and sanitation, and practice of handwashing with soap. Nevertheless, whatever information was available, it was used to help readers understand

59
the situation. The following three graphs (Fig 3.2, 3.3 and 3.4) drawn from MICS, JMP and Post-KAP/HHS data (administered as part of the evaluation in 3 provinces in 2017) provide insight into changes that have occurred over time and the current situation in provinces where projects were implemented.
Access to Improved Water For this indicator, the JMP data suggests an incremental change from 87.8% to 92.2 (almost 5% points) from 2011 to 2015 respectively. The MICS however suggests a downward change from 89.4% to 89.2%, from 2011 to 2014. The Post-KAP/HHS results from the three provinces (2017) suggest the overall number of 80.8%, which is lower than both MICS and JMP data. As shared above, the results could be argued as incomparable for reasons such as data currency (reliable 2016 data is unavailable), and level of data disaggregation (unavailability of provincially desegregated data). Despite a stated position on data incomparability, it could be explained that the minority dominated regions lag behind in development indicators from non-minority regions and for that it could be argued that when the RSHP started these provinces (especially in Northern Mountains and Central Highlands) had lower accessibility rates (to improved water) compared to national or rural averages. The evaluators may conclude that due to data limitations, it is not possible to take any substantiated position on RSHP’s contributions in accelerated access to improved water, in provinces where projects were implemented.
Overall, a significant proportion of households (81%) claimed to have access to drinking water from improved water sources. The highest reported improved source of drinking water is piped water at 46%, whereas another significant proportion (27%) access water from a protected spring (see Table 3.14).
Table 3.14: Percent of respondents reporting type of water source for drinking and cooking
(1) Improved Sources (%) (2) Unimproved Sources (%) Piped into dwelling, plot or yard 46 Unprotected spring 1
Public tap/standpipe 0 Bottled water 13
Tube well/borehole 4 Surface water (river/dam/lake/pond/stream/canal)
3
Protected dug well 1 Other (specify) 2
Protected spring 27
Managed rainwater collection 3
Overall 81 Overall 19
Further analysis indicates that a sizable proportion (12%) lack access to drinking water sources throughout the year, an issue that needs to be addressed. The problem is highest in Lao Cai (21%) in comparison to Dong Thap and Ninh Thuan at 5% and 8% respectively (see Table 3.15).
75
80
85
90
95
2 0 1 1 2 0 1 2 2 0 1 3 2 0 1 4 2 0 1 5 2 0 1 7
% A G E O F R U R A L H H S H A V I N G A C C E S S O F I M P R O V E D W A T E R
JMP MICs AAN
Figure 3.2: Percentage of Rural HHs having access of Improved

60
Table 3.15: Percentage of respondents reporting access to water sources – throughout
the year by province
Indicator Yes / No
Dong Thap (%)
Lao Cai (%)
Ninh Thuan
(%)
Overall (%)
Access to water sources for drinking – throughout the year
No 5 21 8 12
Access to water sources for sanitation (bathing, cleaning, toilet use etc.) – throughout the year
No 0 22 2 8
Access to Improved Sanitation For improved sanitation, despite data limitations the evaluators find a similar pattern as is noted for improved water. The data suggests incremental change over time for both JMP and MICS results. The JMP data suggests increased access to improved sanitation (for rural Viet Nam) from 68.1% to 75.9 (almost 8% points) from 2011 to 2015 respectively. The MICS data suggest change from 71.4% to 76.6%, from 2011 to 2014. The Post-KAP/HHS results from the three provinces (2017) however suggest the overall number of 55.1%. The Post-KAP/HHS numbers are considerably lower than the MICS and JMP results for 2014 and 2015, and understandably represent regions with limited coverage. The reasons listed above for rural water vis a vis incomparability stand valid for rural sanitation results. However, one could argue that RSHP may have contributed to accelerating latrine construction (as 97% households reported to have latrines), however not necessarily all newly built latrines could meet the standards of improved/hygienic latrines.
The overall situation of latrine existence in the surveyed communities across all three provinces is significantly high, a positive outcome of the efforts of the Government, UNICEF and other sector partners. The HHS results indicate that overall latrine existence stands at 97% (Table 3.16). A similar pattern of latrine existence is observed across Dong Thap, Lao Cai and Ninh Thuan at 96%, 97% and 98% respectively. The End line survey results are better than the national values as indicated by the latest data of the UNICEF/WHO Joint Monitoring Programme report 2017. The practice of latrine sharing at the household level is not very common (2%), which is illustrated by the high prevalence (97%) of latrine existence. Further analysis of the HHS results indicates that almost half (45%) of the respondents in the surveyed communities are using unimproved53 toilets. The survey results correspond to the fact
53 Unimproved toilet facility (UNICEF-WHO JMP categories); VIP latrine, Pit latrine with slab, Hanging latrine and Composting latrine
50556065707580
2 0 1 1 2 0 1 2 2 0 1 3 2 0 1 4 2 0 1 5 2 0 1 7
% A G E O F R UR AL H HS U S I N G I M P R O VED S A N I T A T I O N
JMP MICS AAN
Figure 3.3: Percentage of Rural HHs using improved Sanitation

61
that in the targeted deprived provinces, basic access is not a major issue, rather the critical issue is the lack of use of hygienic latrines (improved toilet facilities are reported at 55%) (refer to Table 3.17). This fact also points to the appropriate prioritization of issues by UNICEF and the government for the promotion of SanMark to support people in moving up the sanitation ladder. Overall, among the unimproved toilet facility category, ‘composting latrine’ type is the most common, whereas ‘flush (connected to septic tank or pit latrine)’ type latrines are the most common in the improved toilet facility category.
Table 3.16: Percentage distribution of households' access to sanitation
Indicator Overall (%) Latrine Existence 97
Practice of Sharing of Toilet Facility 2
Table 3.17: Percent distribution of respondents reporting nature of toilet facility
Nature of Toilet Types of Toilet Overall N %
Unimproved Toilet Facility
VIP latrine 9 3
Pit latrine without slab 0 0 Hanging latrine 4 1 Composting latrine 136 41 Total 149 45
Improved Toilet Facility
Flushed to piped sewer system
13 4
Flushed to septic tank 91 27 Flushed to pit latrine 71 21 Flush, don’t know where 6 2 Pit latrine with slab 2 1 Total 183 55
Overall 332 100
Moreover, self-reported HHS results correlate with ‘observation-based’ findings from the household survey as enumerators were able to observe availability of latrine at 93% of the households. Similarly, for above 91% of households, enumerators were able to observe some sign of latrine use (see Table 3.18).
Table 3.18: Percentage distribution of households observed for existence of latrine
*Observation for Latrine Existence Overall (%)
In own courtyard 32
In own dwelling/attached to own dwelling 61
Refused/Not able to observe 1
Others 6
Total 100
*OS1 - Where is the toilet facility used by members of your family located? Can you show me where it is now?
Table 3.19: Percentage distribution of households
observed for some sign of latrine use
*Observation for Latrine Existence Overall (%)
Yes 91 No 8 Refused/unable to observe 1 Total 100 *OS3 - if one or more signs below are selected, then the answer will be “YES”

62
Hygiene Promotion (handwashing with soap) For handwashing with soap, the indicators/questions used for analysis vary for JMP, MICS and Post-KAP/HHS54. The JMP results for availability (observed/verified during survey) of handwashing station with soap in the household have stayed stagnant at 82.2% from 2011 to 2015. The numbers for MICS (for percentage distribution of households by availability of soap – assuming washing station is available) however decreased from 84.2% to 82.4% from 2011 to 2014 respectively. The Post-KAP/HHS results are lower than both JMP and MICS at 78.6%. Once again, the reasons for incomparability as listed above stay valid for this indicator also. The difference however is not much than national rural average.
Programme Un-intended Results
The Programme produced a series of unintended results both positive and otherwise. The most significant of the unintended results include:
The relevant authorities shared that in RSHP supported areas, the communities were found to be practicing water safety and hygiene behaviours e.g. safe storage, hand washing with soap, containing human faeces and others, during emergency situations, particularly in floods. To the authorities, the wider awareness of health risks and mitigative actions that RSHP contributed to, enabled communities to adopt such practices that helped to prevent large-scale post-emergency epidemics.
The UNICEF team shared that the results of RSHP have positively influenced the governments to replicate community-based approaches in other sectors such as nutrition, child protection, risk reduction and others. To UNICEF, the national and sub-national governments are now more receptive to integrating community-based approaches into other public services. This however would need continuous lobbying and technical support where required, to enable governments to implement such models. This was highlighted as an opportunity for the new CPD also.
Reportedly, the women in water-stress areas complained of added worked-load to fetch sufficient water to keep latrines functional and clean. The drought situation, which some areas experience on regular basis, exacerbates the situation further. To them, this adds to the stress for women, mostly the ones responsible to water collect and cleaning of latrines. This came out as an un-intended negative result of the Programme.
54. MICS: Percentage distribution of households by availability of soap; JMP; Post-KAP/HHS: Handwashing facility with water and soap; What do you usually use to wash your hands?
75
78
81
84
87
2 0 1 1 2 0 1 2 2 0 1 3 2 0 1 4 2 0 1 5 2 0 1 7
%A GE DI ST RI BUT ION OF HO USEHOL DS BY A VA I LA BI L ITY OF SO A P
JMP MICS AAN
Figure 3.4: Percentage of households by availability of soap

63
EFFICIENCY
EQ#4: To what extent the level of achievements (outputs and outcomes) justify the financial and human resources used? Summary Assessment: Except for the assessment of value for money, the RSHP implementation is noted as ‘efficient’ on other counts such as completion of projects, funds consumption, and leveraging public sector funds. The provincial projects have been completed in time despite lag time of 6-18 months for some provinces (between signing of contract and approval of Action Plans). For instance, despite delayed kick-off, Dien Bien province (18 months lag time) managed to implement and complete 98% of the planned activities. For this it could be argued to have been implemented efficiently. The financial efficiency in terms of allocations vs consumption looks reasonable at over 85%. The provinces received more funds compared to national projects that also corresponds to increased scope of provincial projects. The distribution of allocations across different targeted regions corresponds to the number of provinces covered in each region. The distribution pattern for provincial allocations is noted as justified and balanced as each province on an average received between 11-19%. RSHP could be argued as efficient since the provinces managed to leverage 28% resources for RSHP activities from public sector partners. In terms of sectoral allocations (within provincial budgets), the CSD activities (of which WASH is a sub-component) received maximum share i.e. 43%. In terms of adequacy of funds, the public officials expressed mixed opinions. There are some well noted deficiencies (for various provinces) for different project(s) components such as Lao Cai did not have any allocations for M&E beyond 2013. Similarly, stakeholders referred to limited fund allocations for training and creating water safety demonstrative models. Limited financial tracking and level of disaggregation impeded drawing value for money (cost per beneficiary) analysis. Moreover, no in-country and regional data is available to draw meaningful comparison to assess efficiency. Find below the elaboration on the summary assessment for efficiency. This evaluation covers rural water and sanitation related activities of nine (09) different projects/partnerships (2 national and 7 Provincial) between government and UNICEF, grouped as UNICEF’s RSHP (2012-16). The records suggest that provincial projects (titled as Child Friendly Projects), were approved more or less at the same time but took-off late subject to delays in approval of actions plans. The documents and interaction with stakeholders suggest that for most of the projects, the actual implementation took on average 6-18 months for different provinces (refer Table 3.20 below).
Table 3.20: Provincial child friendly projects approval/start dates
Province Approval Date/Start
Date Comments & Observations
An Giang July 2012 It took almost seven months to kick-start the project.
Dien Bien 3 June 2011 27 May 2013 (Action plan approved).
The action plan took 18 months to get approved.
Dong Thap N/A No clear timeline available in reports. Gia Lai 5 October 2012
25 June 2013 (Project Start Date)
The project started after 18 months, in comparison to RSHP timeline
Kon Tum N/A Reporting inconsistency
Lao Cai 5 October 2012 Took 10 months to kick-start the project Ninh Thuan 20 July 2012 Took 06 months to kick-start the project
The critical review of the documents points to the limited clarity on outputs and outcomes, particularly for water and sanitation (under CSD component). The provinces were able to

64
implement activities despite a delayed start. For instance, Dien Bien, despite having a delayed start (of 18 months), was able to implement 122 activities from listed 125 (98% progress). The efficiency analysis has been drawn on the financial information extracted from ‘Detailed Project Outlines’ and ‘Final Progress Reports’ shared by UNICEF Viet Nam. The information made available did not help much to relate more meaningfully the financial information with the progress on programmatic outcome and outputs. This could partly be attributed to limited clarity on programmatic outputs and outcomes across projects, and inability of the financial system (desegregated financial information across programmatic components) to enable tracking of finances vis-a-vis programmatic achievements e.g. outputs and outcomes. The financial consumption figures (disbursements vs allocations for An Giang province) further consolidates the assertion that provinces were able to implement the planned activities and consumed the allocated budgets. Based on an assumption that all disbursed amounts have been utilized, the provincial burn-out rate (for allocated resources and given considerable time lags in initiation) at 88% is good. For Dien Bien and Lao Cai the disbursement pattern is more or less similar i.e. 82% and 94% respectively. Overall, UNICEF’s partnership with provincial governments has enabled the mobilization of a significant amount of public funds at 26% of the total funds for the provincial projects - a commendable contribution by UNICEF (see Table 3.21).
Table 3.21: Financial Summary for the An Giang Child Friendly Project
Total (USD)
UNICEF Government
Counter Partner
UNICEF Contribution
(%)
Government Contribution
(%) Commitment 1758691 1295650 463041 76% 26%
Disbursed 1548493 1171630 376863 Disbursed (%) 88% 90% 81%
Despite demonstrating successes through implementation of the work plans and consuming allocated budgets, there are some noted observations around inadequacy of resources for provincial projects. For instance, the final progress report of ‘Lao Cai Child Friendly Project’ states that no M&E budgetary support was available beyond 2013 in addition to insufficient funding for creating demonstrative models for water safety, which affected the delivery. Also, that the staff training in new concepts and practices such as CLTS, was not enough to enable quality delivery. The new cycle must invest more in regular training of front-line staff such as health workers (involved in triggering) to do effective mobilization. On funding allocation across administrative tiers and programmatic priorities, the rural water (MARD at national level) received lowest allocation i.e. 5%, compared to 17% to MoH for rural sanitation. This, in a way, highlights the tilt in favour of rural sanitation. Provinces received the maximum allocations i.e. 78% (refer Figure 3.5). The funding distribution across provinces followed a balanced approach as it varies between 11-19% (on average) of total available funds for provinces.
Distribution of Funds by National and Provincial Programme
Distribution of Funds by Programme Components
Distribution of Funds for CSD Component by Provinces
Figure 3.5: UNICEF funds to national ministries and provincial child friendly projects

65
In terms of programmatic focus, the CSD component, which includes the rural water and sanitation activities, is the heaviest compared to others i.e. policy and social governance, child protection, and education. For instance, in Dien Bien Province, out of 125 planned activities in the provincial action plan, 46 (more than 33%) belonged to CSD. Similarly, the financial records suggest that CSD components received maximum funding at provincial level i.e. on average 43%. This, by default, suggests that more funds were available within provincial budgets for water and sanitation activities.
By Regions By Programme Component and Province
Figure 3.6: Distribution of funds by region, programme component and province At regional level, the pattern for distribution of funds across three regions namely NM, CH and Mekong Delta, is balanced also (See Figure 3.6). The available financial information offers limited disaggregation to relate it to component/strategy e.g. C4D etc. to the results achieved such as changes in behaviours. Subsequently, the evaluators are unable to offer strategy and component specific (within rural water and sanitation) efficiency analysis of project. This has seriously impeded drawing comparison with other national and regional efficiency related results.
SUSTAINABILITY
EQ#5: To what extent is the ODF status and the associated social norm as well as hand washing practices likely to sustain? Summary Assessment: Sustainability has been assessed separately for rural water and rural sanitation. The assessment dimensions covered policy level achievements; institutional capacities to continue implementation; changes in knowledge, attitudes and capacities; extent of slippage (in ODF communities) and status of social norm creation (for latrine use). For rural water safety, at policy level and for institutional strengthening, the RSHP contributions are insignificant and hence given less focus. Among key accomplishments, the most significant is the formulation of draft ‘Water Safety Plans’, yet to seek approvals for allocation of public funds. This achievement would require continuous follow-up and push to seek financial allocations for advancing the cause of water safety. The integrated and joint implementation of BCC/C4D campaigns for water safety practices by provincial health authorities, has resulted in enhancing capacities, giving confidence and trust (to implement), and a flavour of what practical challenges and improvisations could be done, which is likely to sustain beyond Programme’s life. The enhanced implementation capacities will enable implementation of planned roll-out of ‘Water Safety Plans’. The water safety campaigns have added to knowledge, attitudes and practices of communities as evident from Post-KAP/HHS results and will certainly sustain. Post-KAP nevertheless, requires continuous follow-up and frequent messaging to the communities. The

66
‘Entrepreneur led Water Safety Model’ (ceramic filter) remains one of the highlights, and if given the added support in establishing rural markets, will prove useful and sustainable. The practice of holding sector reviews exclusively for water was discontinued. The O&M Working Group is likely to sustain; however, the PO MARD will require added support to keep coordination forum alive and relevant, in the face of evolving context. For rural sanitation, the Programme has demonstrated the success of CLTS as an approach which in view of the planned/anticipated scale-up of CLTS is likely to sustain. The other results that may sustain include: ‘National WASH Strategy’ (as a guidance document); the refined and clear mandate of MoH/VIHEMA as the lead rural sanitation implementer; availability of tested training manuals, trainers; and improved standards for ODF verification and certification. The ‘Draft ODF Plans’ will serve as a push-factor for the national and provincial governments to allocate resources for rural sanitation and continuity/upscaling of CLTS. The SanMark related achievements, however, vary across provinces, and are likely to continue beyond projects. The involvement of MoH/VIHEMA in planning and roll-out of CLTS has given much needed experience and confidence and raised operational capacities within national and sub-national authorities to implement such projects in future. These enhanced capacities will certainly sustain as referred to by the public officials during interviews. The MoH/VIHEMA may continue to seek assistance from development partners to improve the standardisation and implementation (including documentation) of CLTS. The phenomenon of ‘Slippage’ (communities reverting to open defecation in ODF certified communities) is very much a reality as revealed from HHS results in targeted communities. The Post- KAP HHS results point to 15% slippage rate in ODF certified communities (no cut-off date for ODF certification was set for non-availability of timeline for ODF villages), which is satisfactory in comparison to Plan International multi-country study that noted variable rates e.g. from 8% in Ethiopia to 22% in Kenya55 (for one criteria56 only i.e. households to have a functioning latrine).However, given more efforts made for post-ODF follow-up and monitoring within ODF certified communities, the slippage rate can be further controlled or reduced to a level that indicates the presence of a social norm for latrine use. The availability of household latrines at 97% is very encouraging and suggests success of RSHP in accelerating latrine construction. The frameworks of ‘Social Norms Theory’ were used for the assessment of social norm status. The results point to existence of a ‘weak’ or an ‘unstable’ social norm’ for latrine use partly due to significant inconsistencies between empirical and normative expectations. The sanctions for delinquent behaviours (such as OD) within communities are insignificant i.e. 32%. Such a state of affairs merit rethinking of CLTS implementation approach and added guidance from UNICEF on social norms programming. Find below the elaboration on the summary assessment for sustainability.
Sustainability of Rural Water Supply and Safety Achievements The formulation of (draft) ‘Provincial Water Safety Plans’ is a significant policy contribution; however, this must only be seen as a beginning, for the commitment to allocate funds is yet to come. The other notable contributions are in terms of potentially replicable C4D products (for water safety), improved knowledge of communities (around water safety practice), and improved sector coordination. The low-cost ceramic filters carry potential for replication and scale-up. Communication for Development (C4D) Campaigns and Products: At strategic level, the key contributions have been the formulation and roll-out of BCC/C4D products around water safety and quality. The MoH/DoH staff shared that engagement with UNICEF proved useful as it offered much needed exposure and experience to the relevant staff/units in conceptualising, developing, and rolling out interactive communication campaigns. The communication products are likely to sustain, and so are the trained human resources as have been mentioned frequently by various public officials during KIIs.
55 Plan ODF Sustainability Study. Multi Country Study, December 2013. http://www.communityledtotalsanitation.org/sites/communityledtotalsanitation.org/files/Plan_International_ODF_Sustainability_Study.pdf 56 However, if all five criteria [1) A functioning latrine with a superstructure; 2) A means of keeping flies from the pit (either water seal or lid); 3) Absence of excreta in the vicinity of the house; 4) Hand washing facilities with water and soap or soap-substitute such as ash; 5) Evidence that the latrine and hand washing facilities were being used (e.g. a welltrodden path)], are applied the reversion rate is alarmingly high with a range of 75% to 90% for Tororo, Kenya, Ethiopia and Sierra Leone.

67
Improved Knowledge, Attitude and Practices: At community level, the BCC/C4D campaigns have evidently contributed to improved knowledge and visible attitudinal changes for hygienic practices. For example, the HHS results indicate a significant level of practice of handwashing (67% and 62%) among survey respondents (particularly) before eating and after defecation respectively. Of those who practice handwashing, 83% of the responses indicate the use of soap, while 20% responses mentioned the use of powdered or liquid detergent for handwashing, indicating a very positive situation in the targeted communities. Such achievements in hygienic practices are likely to continue beyond project life. However, such changes don’t stay long unless the messages are continuously reinforced. For that, there is apparently no plan available at present. Water Safety and Quality: UNICEF has supported a local entrepreneur to develop low-cost water filters for possible scale-up. The results have been quite encouraging and the model now awaits final approval by MoH before national scale-up. This stands out as one of the most significant achievement of RSHP (for rural water safety), which may not only sustain but offers promise for scale-up. The model may need follow-up and support to enable the entrepreneurs to successfully scale this product. Given national scale-up, the intervention offers huge potential for job creation and entrepreneurship. The demonstration of successful model of ‘Ceramic Filter’ highlights UNICEF’s success in its advocacy and technical support to strengthen the enabling environment particularly in terms of establishing Public Private Partnership between government, private entrepreneurs and UNICEF for improving water safety and quality. This initiative has great potential for scalability given the efforts are continued to resolve some issues of its accreditation by relevant public authorities, and further backstopping to expand its market within rural communities first, before reaching out to urban localities. Detailed deliberations on developing a long-term strategy and scale-up plan for strengthening the local market (setting standards, price and quality regulatory functions, regular monitoring) can ensure long-term benefits of this initiative for the communities. Improved Coordination – Operation and Maintenance Group: UNICEF has supported PO MARD in re-activating O&M Technical Group, to improve coordination between stakeholders on O&M issue. The support is acknowledged and appreciated by the PO and other stakeholders. The group is likely to remain active in near future, however in the absence of a clear agenda and PO-MARD itself being resource-constrained, may affect its sustainability in long- run.
Rural Sanitation The RSHP has worked successfully to register community led approaches such as CLTS and CATS, as preferred strategy options for the future in the country’s WASH strategy. This could be argued as the most sustainable contributions of RSHP. With that, the support to institutionalise CLTS/CATS implementation such as development of training modules, operational guidelines, ODF verification and certification, and cadre of master trainers etc. have all sustained and are likely to sustain in future. Moreover, the RSHP has helped addressing the struggles around mandate and establishing MoH as lead implementer, which adds to sustainability of the achievements. The formulation of draft ODF plans at sub-national level, is a step in the right direction with potential to transform rural sanitation in Viet Nam. For this to realise, the plans require necessary official approvals and allocations. Unless and until financial allocations are made, much of what RSHP was able to achieve will remain at risk. The involvement of MoH/DoH in design and implementation of CLTS/CATS at pilot scale has helped building technical capacities and giving confidence to the staff in their abilities, at both national and sub-national levels. The capacities built in a new domain are likely to sustain and may prove useful in scale-up of CLTS. These skills would be useful for the upcoming World Bank funded rural water and sanitation programme. RSHP has worked to create practical models of sanitation marketing to improve access to latrine designs, materials, and services. The results across regions vary, with more encouraging results produced in the Mekong Delta regions. Overall, the SanMark component could demonstrate limited success with accelerated adoption of low-cost and disaster resilient latrine designs and products, and situation seems less likely to improve and sustain.

68
ODF Slippage & Creation of Social Norm (of exclusive latrine use) In response to one element of the evaluation question ‘to what extent is the ODF status and the associated social norm as well as hand washing practices likely to sustain?’, the evaluators took note of the current RSHP implementation particularly the communication model and interventions (including those for pre-and-post ODF) vis-à-vis behavioural transformation to the extent of creating/upgrading social norms of latrine use. To complement that, social norms questions were added to the Post-KAP/HHS particularly around latrine access and practice of using latrine, beliefs, normative and empirical expectations, and existence of sanctions, and were analysed accordingly to assess existence of norm of exclusive latrine use. This section entails analysis around extent of slippage in the ODF certified villages. The Table 3.22 below illustrates the extent of ‘slippage’ (all members of a household do not always use latrine for defecation) in the surveyed communities across the three provinces where the EHHS was administered. The analysis of the survey results is based upon the assumption that the surveyed communities were verified and certified ODF, a state when 100% of households were reported to be always using latrines (Question SN1). The overall survey results show that 54% of the respondents reported that ‘all household members always use a latrine”. Given the working assumption, the survey results suggest that the slippage rate in the surveyed communities is at least 15% (latrine use is reported as often, sometimes and/or rarely). Furthermore, the results for consistent latrine use (all members always use latrine) vary across provinces e.g. the highest proportion is 74% in Lao Cai and is lowest (36%) in Ninh Thuan (Table 3.22). The variations across provinces are significant, however the evaluators are unable to offer any substantiated rationale for these differences. It is important to note that the ‘latrine prevalence’ numbers in all the three provinces is reportedly very high at 97% compared with the actual practice of ‘consistent latrine use’ (54%) by all members of the households. The pattern seems uniform across three provinces with 96%, 97% and 98% for Lao Cai, Dongthap and Ninh Thuan respectively. This inconsistency between latrine prevalence and consistent latrine use suggests that probably people are more adaptive to material culture (infrastructure) and adopt it more readily than practices or behavioural change (non-material culture). The results for ‘always latrine use by all’ vary significantly across the three provinces, which needs further probing at the district level to understand the phenomenon causing this variation. To the evaluators, one plausible reason is the variation in the effectiveness of behaviour change communication efforts imbedded in varying capacities of the staff involved in triggering and BCC activities. Furthermore, slippage at 15% implies that overall ‘one in every seven households’ has slipped back to practicing open defecation in the surveyed communities. This also points to weaker post-ODF follow up and monitoring within ODF certified communities.
Table 3.22: Percent distribution – extent of slippage by province
Indicators
S1 (Latrine Prevalence)
SN1 - Extension of slippage
Yes Latrine Use
(Always) Latrine Use = (Rarely +
Sometimes + Often) Overall 97% 54% 15% Dong Thap 97% 51% 16% Lao Cai 96% 74% 8% Ninh Thuan 98% 36% 21%
The social norms analysis has been done across a range of elements of social norms theory i.e. empirical expectations, normative expectations, personal normative beliefs, and existence of sanctions. As indicated in Table 3.23, the empirical expectations results exhibit that 81% of the respondents claimed that they think above 80% (out of 10 people, the respondent replied 8 or

69
more, i.e. threshold set at 80%57 or more), of other community members always use latrine in their community. Overall, the survey results indicate a high latrine prevalence (97%) among surveyed communities and, by and large, match with people’s belief about other people’s practice (empirical expectations) that they are using latrine as 81% of respondents believe that all other community members are using latrines. Such a high level of consistency between ‘latrine prevalence’ and respondents’ beliefs about ‘other people’s practice’, is one of the positive indications towards the presence of a ‘norm’ within the community for latrine usage. Similarly, ‘all’58 respondents believe (or at least appear to believe) that ‘latrine should be used (normative expectations)’. Such a reasonably high level of consistency between respondents’ personal belief and their belief about other people’s practice, again infers the existence of a ‘collective behaviour’ among community members that latrine usage is a ‘norm’ within the surveyed community. However, further analysis of the other question (about people’s personal normative believe – the underlying belief that latrine should be used because it is the right thing to do) reveals a contradiction between respondents’ personal beliefs about the underlying reason/motivation for latrine usage. Only, one in three respondents (33%) holds the belief that ‘latrine should be used because it is the right thing to do’ and thus oppose the inference that there exists a ‘social norm’ for latrine usage. Furthermore, survey results indicate a lower level of ‘sanctions’ (32%) for those who are still not using latrine (practice open defecation) and thus provide sufficient basis to disprove the existence of ‘social norm’. Finally, a combined analysis of all these determinants of the ‘social norm’ provide sufficient basis to ascertain a ‘weak’ or an ‘unstable’ social norm for latrine use among surveyed communities. This situation requires attention from the implementers to revisit their overall implementation approach for norms creation around ODF.
Table 3.23: Social norm analysis
Indicators
SN2* (Empirical
Expectations) (80% and Above)
SN3** (Normative
Expectations) (Yes)
SN3.1*** (Personal Normative Believe)
SN3.2**** (Personal Normative Believe – Vignette Question
SN 4***** (Existence of Sanctions) (Nothing
Happens)
Overall 81% 100% 33% 93% 68%
Dong Thap 75% 100% 18% 91% 82%
Lao Cai 81% 100% 11% 88% 64%
Ninh Thuan 87% 100% 69% 98% 60%
* SN2. Think about the people in your village, such as your family, friends, and neighbours. Out of 10 people in your village, how many do you think said that all their family members always use a latrine? – Analysis done for above 80% (10,9,8) of the people who always use latrine ** SN3. Do you believe that people in your village should use a latrine? – analysis done for (Yes)
*** SN3.1 Why do you think people in your village should use a latrine? - Because it is the right thing to do
**** SN3.2 Think about the people in your village, such as your family, friends, and neighbours. Out of 10 people in your village, how many do you think said that people should use a latrine because it is the right thing to do? - Above 80% (10,9,8) - because it is the right thing to do
***** SN4. If someone in your village was observed defecating in the open, what would happen to her/him? Analysis done for (Nothing happens) option
The survey results reinforce that social norm creation (of latrine use) was not fully integrated into RSHP implementation. Moreover, the implementers lack understanding of theory and practice of social norms. The VIHEMA needs guidance to integrate the concepts into the current CLTS implementation particularly around sanctions. These constraints require that MoH/VIHEMA and
57 80% is the threshold for the comparison of results and it is calculated as total number of people out of 10 in a village who think that their family members always use a latrine. To check the respondent’s beliefs and norms, we have selected only (8,9 and 10) members of the households. 58 SN3** Do you believe that people in your village should use a latrine? – (Yes – 100%); (Normative Expectations)

70
UNICEF need to review their overall programming priorities, unreached areas, and the available resources keeping in view the fast-approaching deadline of OD elimination by 2025. Furthermore, the evaluators assessed that the social norms creation/up-gradation requires considerably longer time for communities to internalise new norms and associated actions. The expectations to create/upgrade norms in two years programming cycles needs re-thinking with clear programming and implementation guidance. UNICEF may have, to a certain extent, succeeded in persuading the government counterparts, however for this to realise UNICEF may be required to invest more in unbundling the theory and assisting governments to understand, develop, and implement interventions for social norms creation. UNICEF COs and their implementing partners need guidance around standards and benchmarks for norms creation, interventions, training, BCC, monitoring systems, and other programming aspects to help governments adopt effective programming for creating ‘Stable Social Norms’. The guidance may need to factor-in the possibility of open defecation in perhaps the ‘Special Circumstances’, as it is happening in ODF communities and may continue so.
EQUITY, GENDER, RESILIENCE AND HRBA
EQ#6: What key approaches and strategies were adopted to enable RSHP projects and interventions prioritise/integrate the needs of the vulnerable and marginalized groups (poor, remote communities, ethnic minorities, women, children, poor, elderly, people with disabilities) and results achieved? Summary Assessment: The section presents the summary-assessment of Non-OECD DAC criteria elements used for the evaluation, followed by a separate commentary on equity, gender, disaster resilience and HRBA. The Programme’s adherence to equity dimensions varies in terms of its design, targeting, interventions and results. The prioritisation of poorest and most deprived regions and provinces make the programme equitable. This is further augmented by the fact that these provinces have maximum caseload of ethnic minorities, the most deprived group in Viet Nam. The Programme interventions have benefitted all including women and children, often considered disadvantaged. The BCC interventions are assessed to be less relevant to the ethnic minorities in terms of contents and delivery mechanisms. The involvement of locals preferably from ethnic minorities, would have possibly helped more with effective dissemination and adoption of message. The low-cost water filtration and latrines options continue to benefit poor, as these options are priced less than half or in some cases even 1/3 the costs of products available in the market. The latrine designs that were promoted are at best disability neutral, hence less equitable. This is irrespective of the fact that people have demonstrated preference for high-end/cost latrines. The loans for households and communities are available for water and sanitation interventions. The Viet Nam Bank for Social Policy (VBSP) remains the key player, however the pre-qualifications make them look more suited to non-poor. The programme monitoring systems failed to capture benefits for poor and disadvantaged groups. The RSHP design and delivery approaches are mostly gender-sensitive. This is evident in the shape of active involvement of ‘Women Unions’ for triggering and C4D interventions, thus connecting them with women and girls. The communication products developed are assessed as being relevant and sensitive to women and girl’s issues e.g. hygiene, health and others (including children), hence making them gender-sensitive. RSHP has leveraged fully the potential of women as ‘Change Agents’ which has been duly referred to and acknowledged at all levels. The Programme benefitted all, however the interaction with women and children suggestions greater appreciation of involvement and benefits by the women, girls and boys. The women referred to Programme as making valuable contributions to improved health, clean environment, and other issues that are mostly dealt with by women and girls. Some even referred to reduction in episodes of sickness, however this remains unsubstantiated. Where women referred to additional workload (for water collection, treatment, and cleaning of latrines), they shared that the benefits outweigh the added burden and they are happy to see children and adults living healthy and happy. The child-focused interventions particularly at schools, have worked to benefit children. The

71
communities particularly children appreciated the school related WASH interventions whereby minor rehabilitation of latrines and water points was done in selected communities. The children made special references to BCC/C4D messages for making them rethink and change practices to avoid germs and disease. It is important to note, however, that the monitoring system did not capture fully the integration and results with gender lens. Viet Nam is a disaster-prone country and experiences repeated floods, droughts and landslides. This made resilience integration a priority for RSHP interventions. The resilience integration offers mixed results. UNICEF advocated with stakeholders of DRR integration as one of the key members of ‘WASH Cluster’ (formed as part of humanitarian reforms). Moreover, technical support was extended to NCERWASS to help improve capacities of staff to integrate resilience lens to regular and humanitarian response services. The advocacy efforts contributed to issuance of ‘Regulations’ around water use in emergency situations. Some humanitarian response activities have also been performed with MARD e.g. Salt-Water Intrusion in 2016. Technical support was provided to assist with updating the ‘Provincial DRR/Climate Change Adaptation Plans’, particularly with health activities. The SanMark interventions supported design of disaster resilient septic tank designs at higher costs i.e. the school interventions integrated resilience lens. The BCC/C4D campaigns and messages included advice on dealing with emergency situation. The Programme design and delivery demonstrate coherence with human rights programming principles and approaches. Foremost is the Programme’s supports for the government to fulfil its commitment to enable access to water and sanitation, which by law is a right of every Vietnamese. This stems from Viet Nam subscription to ‘International Covenant on Economic, Social and Cultural Rights (ICESCR) 59 i.e. Article 12. The adoption of UN General Assembly Resolution 64/292 (July 2010), cements it further. Viet Nam, for being signatory to Convention on the Rights of Children (CRC),1989, the UNICEF support extended as part of RSHP is coherent with CRC provisions, hence advancing the children rights. The ‘integrated model’ with interventions around education, health, CP, and CSD, further amplifies coherence with children rights. The RSHP’s adherence to principles of human rights programming is evident from focus and interventions around both the duty bearers (public agencies) and right holders (men, women, boys and girls). The focus on minorities and poor adds further to its alignment with enabling access to rights and particularly the disadvantaged groups. Find below the elaboration on the summary assessment for equity, gender, resilience and HRBA.
Equity There is considerable evidence that highlights RSHP’s coherence with equity principles. First and foremost is the geographic targeting. The Programme has targeted regions and communities that ranked amongst the most impoverished and remote. These are the regions that have highest concentration of minority groups especially those in Northern Mountains (NM) and Central Highlands regions (CH). These provinces in general represent the lowest levels of development across spectrum of development indicators including access to safe water and hygienic latrines. The Programme components such as CLTS processes, SanMark, hygiene education messages for household water treatment and storage and promotion of health behaviours like HWWS benefitted the women and children, amongst others. Therefore, equity has remained a focus during design and implementation. However, the implementation strategies and the availability of appropriate resources has potentially affected some aspects of equity. For example, the communication strategies and approaches used to bring behavioural change at community level can further be strengthened. In some minority-populated areas, the execution of behaviour change campaigns during CLTS processes and hygiene education sessions was facilitated by staff who were mostly from Kinh Group (the majority group) and could not communicate effectively in a language that is understandable to minority population, thereby compromising the benefits of the Programme for minority groups. Despite these operational challenges, the fact that Programme has targeted EQUALLY all groups is a laudable fact demonstrating its equity focus.
59 United Nations, 2018. International Covenant on Economic, Social and Cultural Rights. [webpage] Available at: https://treaties.un.org/Pages/ViewDetails.aspx?src=IND&mtdsg_no=IV-3&chapter=4&lang=en [Accessed: 9 January 2018].

72
The Programme has focused on creating low-cost models to improve accessibility to safe/clean water and hygienic latrines. The entrepreneur led water filter model is available at almost half the cost (at 23-25 $) of other filters available in the market. The costs for demonstrative low-costs latrines (promoted by the programme) are 1/3 (less than 100$) of most preferred latrines that are being constructed (at approximately 300$). At the same time, the Evaluators may want to highlight that programme could achieve limited success with wider adoption of low-cost latrines. This could be attributed to local preferences for high-end (costly) latrines, as latrines are taken as status symbol. On the whole, it could be argued that the programme made investments to produce and disseminate low cost models, to make safe water and hygienic latrines more accessible for most poor, often ones without access. The evaluators noted that microcredit/loans are available from VBSP for the individual households and also at the community level for construction/repair of water (mostly for community level) and sanitation (at household) facilities. For household loans, the bank seeks approval by the community/group (formed by the bank) to assess the overall financial capability (income, assets and other social aspects) of the individual/household to pay-back the bank loan. The poorest often struggle to get such communal endorsements, hence remain excluded. The exclusion of the poorest from banking facility underscores non-compliance with equity principles. The RSHP did not engage with the bank at all through its implementation. This aspect merits detailed assessment. One more equity fact is that the Programme did not achieve much inroads towards improving latrine access to the people with special needs e.g. older persons, disabled etc. Furthermore, the Programme monitoring systems did not capture fully the improved access to services (water safety and hygienic latrines) and changes in hygiene behaviours for the poorest, which remains a design/operational gap.
Gender Equality The design and delivery of RSHP has largely been gender sensitive. This is evident from the fact that ‘Women Unions’ were actively engaged in commune level roll-out of triggering and behavioural change interventions. The review of the BCC campaigns indicates a due gender focus in terms of deciding communication mediums and messages. The influencing role of young girls and other women as members of the women association in the dissemination of Programme messages was fully acknowledged and realized as ‘change agents’ for behaviour change. Qualitative discussions with the male and female groups at community level reveal that recipients of the Programme benefits are, by and large include all members of the community including men, women, boys and girls. The community interactions further points to greater appreciation by women and children in terms of clean and improved environment. During discussions, some indirect references were made by the group participants to point out an observed declining trend in the disease incidence amongst children. However, this could not be verified from schools and children. The women did acknowledge to additional workload (for cleaning latrines and fetching extra water), but at the same appreciated this as contributing to improved family health. Children were focused through interventions in schools such as minor rehabilitation of latrines and water points. The integrated campaigns, particularly those targeting children, helped improve awareness of personal hygiene amongst children. Parents referred to as school going children as ‘agents of change’, thereby, encouraging and coaching younger siblings of hygiene behaviours such as handwashing with soap. The survey results and qualitative interactions don’t point to ‘need for privacy’ for women as a driver for families to construct latrines. The review of the monitoring data and discussions with provincial teams indicate limited focus on tracking gender results for the Programme. This has emerged as key gaps in the monitoring system.

73
Disaster Resilience Viet Nam is one of the most disaster-prone countries, thus, adding significance of resilience integration into civic service planning and delivery. The fact this project was implemented in areas which are at greater risk to cyclic disasters. This further amplified the significance of disaster integration in programme interventions. About the occurrence of natural disasters, particularly floods and droughts, in provinces where RSHP implemented, survey results indicate, 17% of the total respondents shared that they (family or village) had experienced some type of natural disaster during the past two years. Out of those, 43% and 39% reported experiencing both, the floods and droughts. Ninh Thuan seems most disaster prone, followed by Dong Thap and Lao Cai (refer Table 3.24 for details).
Table 3.24: Percent distribution of respondents reporting natural disaster in last 2 years by province
Disaster Occurrence Disaster Type
Disaster Occurrence
Overall
Type of Natural Disaster
Province
Overall
Dong Thap
Lao Cai
Ninh Thuan
Total Total Total
N % N % N % N % N % Flood 7 29 11 40 23 60 41 43
Yes 69 17 Drought 10 48 13 31 14 38 37 39
No 313 80 Earthquake 0 0 1 2 0 0 1 1
Don’t know 9 3 Others 4 23 7 26 1 2 12 17
Total 391 100 Total 21 100 32 100 38 100 91 100
Overall, the Programme put due focus on integrating disaster risk reduction concepts and principles into both the design and delivery. At national level, UNICEF contributed actively to the ‘WASH Cluster’ formed to lead national level WASH preparedness planning. UNICEF extended technical assistance to NCERWASS (part of MARD) to develop its capacities in emergency preparedness and mitigating climate change. Moreover, it was due to UNICEF advocacy that regulations have been issued for disaster situation specific water resources use. These regulations are applicable both nationally, and in particular, to the targeted regions. UNICEF worked with PO (MARD) to coordinate disaster response activities by relevant ministries i.e. Salt-Water Intrusion in 2016. UNICEF has been assisting and guiding MoH/VIHEMA with integration of health interventions into the ‘Provincial DRR/Climate Change Adaptation Plans. The focus to link latrines to septic tanks demonstrates resilience focus to mitigate impact of floods. The septic tank construction, however, is expensive, costing approximately 600 USD, which in a way contravenes equity integration. In provinces, the demonstrative activities focusing on rehabilitation of water and sanitation facilities at schools (a place used as temporary shelter in floods and cyclones) adds further to Programme being resilience centric. The behavioural change communication campaigns have integrated disaster specific messaging. This reinforces the resilience or DRR integration. The knowledge gained and the consequent change in behaviours (around water safety and defecation) is likely to affect community responses in disaster situations, which augments Programme’s coherence with DRR.
Human Rights Based Approaches (HRBA) The Programme is coherent with HRBA programming principles at varied levels. First, it relates to a domain which is considered as a ‘right’ for Vietnamese to enjoy access to safe drinking water
Box # 07: “Improving DRR in schools is also to make sure that in case of a flood or a cyclone, schools can become a shelter for survival. We want to take this initiative everywhere to every school, to make sure that schools become centres for risk reduction.”
(A representative of WASH team, UNICEF Viet Nam)

74
and sanitation facilities. For instance, Viet Nam has signed up for International Covenant on Economic, Social and Cultural Rights (ICESCR) 60. Article 12 of the ICESCR states that “the States Parties to the present Covenant recognize the right of everyone to the enjoyment of the highest attainable standard of physical and mental health.” This implies that access to clean drinking water, and sanitary conditions, being integral to quality life, is a right of all Vietnamese. Similarly, Viet Nam has adopted UN General Assembly Resolution 64/292 (July 2010) which formally recognises ‘the right to safe and clean drinking water and sanitation as a human right that is essential for the full enjoyment of life and all human rights’61,62. Also, the Prime Minister’s resolution 05/2014/NQ-CP and the National Environmental Protection Act recognised the provision of water and sanitation as a human right and acknowledged its centrality for improved health outcomes. The RSHP contributions are evident in terms of an improved access to clean drinking water and sanitation services (both considered as right), hence it could be argued to have coherence to HRBA principles. Viet Nam is signatory to CRC (1990), which enshrines children rights to life, safety and development. The Programme for having multi-faceted interventions (education, health, CP, and CSD) enables government to improve children’s access to rights. This improves the alignment of the Programme with rights-based programming. At another level, the balanced focus on both the duty bearers and rights holders further supports Programme’s compliance with the HRBA principles. Both national and sub-national projects are driven by the goal to enable relevant duty bearers i.e. MARD, MoH, and others, by strengthening systems and capacities to improve services delivery. The BCC activities focus on building understanding and capacities of the right holders to ask for rights. On the whole, the RSHP corresponds to key aspects of human rights-based programming principles, however, with varying degree of compliance for different components of the Programme. At the design, planning and implementation stages, geographic targeting is largely seen following a problem analysis by analysing the existing disparities across regions (provinces, districts and communes at sub-district level) for rights to safe water and sanitation. By and large, poor regions (targeted Provinces) were prioritized, and most of the selected regions (province and district) are among the poorer regions of Viet Nam. Moreover, within districts, UNICEF has prioritized difficult to reach communes/villages as part of all interventions under health, education, WASH, nutrition and CP. Furthermore, a balanced mix of interventions, addressing the needs of both the duty bearers (GoVN agencies, schools at central and local levels, private sectors) and rights holders (communities, men, women, boys and girls.), was designed and implemented under RSHP. The adoption of an integrated approach (for multi-sector services) also complies with the primary focus of HRBA, by ensuring that duty bearers take ownership and responsibility for appropriate resource mobilization in responding to all basic needs (health, education, WASH, nutrition and Child Protection/Rights) of the rights holders. Another facet that supports coherence with HRBA is in terms of Programme contributing to developing capacities of duty-bearers (public stakeholders) to enable them to deliver on their mandate. At the same time, it focused on educating and sensitising communities (as right holders) of their responsibilities and entitlements. Through enhanced capacities at the government and community levels, the delivery of the basic services such as water, hygiene and sanitation, ultimately benefits the rights holders on the one hand and improves the service delivery capability of the duty-bearers on the other, thus demonstrating compliance with HRBA programming principles.
60 United Nations, 2018. International Covenant on Economic, Social and Cultural Rights. [webpage] Available at: https://treaties.un.org/Pages/ViewDetails.aspx?src=IND&mtdsg_no=IV-3&chapter=4&lang=en [Accessed: 9 January 2018]. 61 United Nations General Assembly: Resolution 16/2; The human right to safe drinking water and sanitation (A/HRC/RES/16/2). Human Rights Council Sixteenth session, Agenda item 3. http://www.refworld.org/pdfid/4dc108202.pdf 62 http://www.un.org/waterforlifedecade/pdf/human_right_to_water_and_sanitation_milestones.pdf

75
By supporting coordination mechanisms such as the working group on sanitation and the working group on O&M, UNICEF efforts have resulted in placing some form of accountability for the duty-bearers, the most critical element of HRBA programming. UNICEF’s efforts towards improving the BCC element of the government’s WASH programming has increased the level of awareness of the rights-holders of their rights to basic services, such as water, hygiene and sanitation and has empowered them to demand those services in-line with HRBA principles. The only limitation related to compliance with HRBA principles is the absence of any formal or informal mechanisms for the rights-holders at the community level to raise their voices to the duty bearers if they encounter some grievance or conflict during Programme implementation. For example, the Programme did not prioritize the establishment of a complaint redressal and conflict resolution mechanism during community-community and Programme staff-community interactions. UNICEF supported the MARD to develop a WASH monitoring system that can collect data on poor households. However, the extent of its application for any equity analysis is unknown. MARD is implementing this monitoring system in 50 provinces out of 63. Good practices around South Asia indicate that a fast and reasonably robust method of poverty profiling can be undertaken e.g. targeting poor communities for social welfare programmes such as Benazir Income Support Programme in Pakistan uses poverty score card method. The poverty score card helps in identifying the poor, living below the national poverty line. The World Bank verified method has proved as an efficient way of targeting the poor. A similar process of using poverty score card by adapting to context of Viet Nam can be undertaken with the support of the World Bank. The current monitoring system lacks appropriate tools and strategies to track, assess and report on outcome level progress because of behavioural change efforts. Behavioural monitoring is an important aspect to fulfil the needs of the rights holders as it allows the duty bearers to devise context specific effective strategies and tools for bringing the desired behavioural changes at individual and community level. Currently, UNICEF Country Office lacks resources to provide financial support for undertaking such behavioural monitoring survey and studies. The needed resources can come from the government. UNICEF and stakeholders thus need to influence the government to make these resources available. Furthermore, the current reporting system is heavily dependent on the monitoring and reporting capacities of health centres at commune level. Key issues are weak technical capacities of the staff, the multiplicity of the indicators, reliability and accuracy of the data collected and reported, and a weak feedback system from the higher levels (National and Provincial) to lower tiers of implementation at district and sub-district levels. Review of the available project closure reports of all provinces indicates notable inconsistencies in formats and content. The final reports are not comprehensive enough to provide information on access, coverage, safety/quality of services disaggregated by gender and socio-economic conditions of the right holders, and therefore a disabling factor for an appropriate future planning by the right holders. A performance bench marking system by introducing key performance indicators can be identified by stakeholders. A regular reporting against these can be placed as an online system (dashboards) for review of practitioners and policy makers. This added feature of monitoring will help in creating healthy competitions of better performance amongst provinces and will highlight challenges for addressing them. UNICEF can help provide support in getting to design, test, create capacities and help review progress on this for more programme effectiveness.
WASH-MALNUTRITION (CHILDREN) NEXUS IN VIET NAM
This section has been incorporated in response to the request by the country management to look into WASH-Malnutrition in Viet Nam and establish, if possible, the RSHP’s contributions in addressing child malnutrition issues in provinces where it was implemented. This section draws on the secondary data only.

76
The secondary evidences re-affirm a direct and strong correlation between WASH and malnutrition. The global evidence available on WASH-Nutrition nexus suggests that almost half of child-malnutrition is linked to unsafe water, inadequate sanitation and poor hygiene (WHO 2008). The estimated financial impact of malnutrition globally is US$3.5 trillion per year, and approximately US$500 per individual. The poor water, sanitation and hygiene conditions lead to disease e.g. diarrhoea, which in turn triggers malnutrition. Children are more susceptible to such diseases and as a result suffer from malnutrition. There is variety of evidence that confirms this for Viet Nam. Reportedly, there are 41% under-five children in Viet Nam that suffer from stunting with significant regional and ethnic disparities. Diarrhoea stands at number seven (07) in terms of national disease burden (for diseases), resulting in a loss of 107,000 healthy years of life every year. A UNICEF study carried out to map the results of CLTS confirmed that improvement in water safety, personal hygiene, and latrine use has contributed towards lowering the rates of diarrhoea and worm infections in project communities. There are evidences that suggest that in Viet Nam not all malnutrition is poverty driven or from food inaccessibility. To address the child malnutrition, Viet Nam has joined the Scaling Up Nutrition (SUN) Movement in 2014 and policy directives have been issued by the Prime Minister. In conclusion, the evaluators may state that there are considerable evidences to prove and reinforce WASH-Child Malnutrition for Viet Nam. For data limitation, the evaluators are unable to track and take any substantiated position on impact of UNICEF interventions in reducing child malnutrition in Viet Nam.
Global and Regional Evidence of WASH-Nutrition Nexus
As per WHO/UNICEF (2017) an estimated 29% of world’s population (2.1 billion) is deprived of safely managed drinking water services i.e. one located on premises, available when needed, and free from contamination. Similarly, 61% (4.4 billion) people are using unsafely managed sanitation facilities (i.e. excreta safely disposed of or treated off-site) as per the relevant SDGs standards. These challenges are translating into significant health impact, as on average 2300 people die every day from diseases caused by unsafe water, inadequate sanitation and hygiene. Faecal contaminated drinking water renders the population at risk of contracting cholera, dysentery, typhoid and polio. More than 340,000 children under five (U5) die annually (or about one thousand every day) from diarrhoeal diseases caused by poor sanitation, hygiene, and unsafe drinking water (WHO/UNICEF 2015)63. The economic impact of health varies and for some countries has evidently gone up to 5% of GDP. WASH related investments bring the best value in return. For instance, every $1 invested in water and sanitation on average brings return of at least $4 is the form of increased productivity. As per World Bank (2016), global evidences suggest hygiene promotion as most cost-effective health intervention. The evidence suggests that universal access to safe drinking water and adequate sanitation and hygiene, would work to reduce the global disease burden by 10% (WHO 2012)64. The global evidences available on WASH-Nutrition nexus suggest that almost half of child-malnutrition is linked to unsafe water, inadequate sanitation and poor hygiene (WHO 2008). The estimated financial impact of malnutrition globally is US$3.5 trillion per year, and approximately US$500 per individual65. The linkages between public health-nutrition are long established. There is an established cyclical relationship between diseases and nutrition. The poor water, sanitation and hygiene conditions lead to disease which in turn triggers malnutrition. Children are more susceptible to disease and as a consequence malnutrition. The cycle of mal/undernutrition particularly in children under five, worsens diarrhoea and as result leads to its perpetuation. Pneumonia and diarrhoea are the two biggest killers of children under five in Asia. The two are largely preventable through adequate nutrition, hand washing with soap, safe drinking water and basic sanitation, vaccinations, and other measures under public health66. Other evidences suggest that nearly half of all deaths in children
63 UN WATER Water, Sanitation and Hygiene http://www.unwater.org/water-facts/water-sanitation-and-hygiene/ (Accessed on March 3, 2018) 64 Ibid 65 Global Panel. The Cost of Malnutrition: Why Policy Action is Urgent. TECHNICAL BRIEF No. 3 | July 2016 https://www.glopan.org/sites/default/files/pictures/CostOfMalnutrition.pdf 66 Multi-sectoral Approaches to Nutrition: The Case for Investment by Public Health, water, sanitation, and hygiene; https://www.unicef.org/eapro/Brief_HealthNutrition.pdf

77
under 5 globally, are attributable to under-nutrition, translating into the loss of about 3 million young lives a year. The East Asia and Pacific region faces the same challenges. Overall, the region has made significant progress over the past few decades in improving water and sanitation access; however, a significant proportion does not have access to improved services. At end of 2015, an estimated 130 million people in the region still lacked access to improved water supplies. Another 659 million are without improved sanitation. The OD rates are high at 10%, if China is excluded. Disparities and inequities are high across countries and within countries, with the richer or urban households being more likely to use improved sanitation or wash their hands with soap as compared to poorer or rural households67. The above evidence establishes and reinforces WASH-Nutrition linkages and particularly for children.
Viet Nam: Case of WASH-Nutrition Relationship
Viet Nam presents similar context whereby reportedly 41% children (under five) suffer from stunting with significant disparities across regions and provinces including different groups. Limited sanitation services, unsafe drinking water, and poor hygiene practices are the leading causes of diarrhoea and pneumonia which account for nearly one-third of deaths among children under five in Viet Nam. Diarrhoea stands at number seven (07) in terms of national disease burden (for diseases), resulting in loss of 107,000 healthy years of life every year. This is highest amongst rural and ethnic minorities68. This works to reinforce the reality of WASH-Nutrition linkages. Reportedly (2015), the national stunting rate is recorded at 24.9% with regional and ethnic disparities. For instance, it stands at 15% for Kinh (majority group) compared to 30.4% for ethnic minorities. In Central Highlands it is as high as 40.6% amongst some ethnic minorities, vis a vis 15.8% amongst the Kinh69. The regions with poor WASH indicators represent the highest rates of malnutrition (for children). For example, in Dak Nong province, where access to hygienic latrines is 42%, one in every five children under five (U5), is underweight70. The natural calamities are further exacerbating the situation and reportedly, an estimated 150,000 children U5 are counted at ‘risk of malnutrition’ due to cyclic nature of natural calamities71. The financial impact is significant, as country losses over US$544 million annually due to vitamin and mineral deficiencies. The World Bank report outlines that and estimated investment in scaling up core micronutrient interventions would cost less than US$33 million per year, far less than the annual loss. In Viet Nam, under-nutrition is not merely restricted to poor households as over one-fifth of children in richest households are under-nourished. Thus, it is argued that under-nutrition is not only because of food access, but also due to caring practices and diseases (caused by unsafe water and sanitation and inadequate hygiene)72. Viet Nam joined the Scaling Up Nutrition (SUN) Movement in 2014, thus committing to end all forms of malnutrition i.e. stunting, underweight, wasting, obesity and others, by 2030. There is wider realisation of the problem of malnutrition and GOVN started implementing the Prime Minister’s directives on ‘strengthening multi-sectoral collaboration for nutrition’ in the country. Two new policy directives namely ‘Communist Party’s Resolution No. 20 / NQ-TW’ and the ‘Prime Minister Directive No. 46 / CT-TTg’ have been invoked. The key stakeholders are of the view to
67 Equity in Public Financing of Water, Sanitation and Hygiene (WASH) Analysis from INDONESIA, MONGOLIA and VIET NAM; How better sub-national financing can contribute to improved water, sanitation and hygiene in East Asia and the Pacific. UNICEF East Asia and Pacific Regional Office June 2016. https://www.unicef.org/eapro/UNICEF_WASH_Financing_and_Synthesis.pdf 68 PSI/Viet Nam: Social Marketing for Improved Water, Sanitation, and Hygiene; 2017. www.psi.org/wp-content/uploads/2017/04/WASH-Brief-FINAL.pdf 69 Viet Nam: Launch of the Scaling Up Nutrition (SUN) Movement (31 Jan 2018); https://www.unicef.org/vietnam/media_27385.html 70 PSI/Viet Nam: Social Marketing for Improved Water, Sanitation, and Hygiene; 2017. www.psi.org/wp-content/uploads/2017/04/WASH-Brief-FINAL.pdf 71 https://www.unicef.org/vietnam/media_27141.html 72 World Bank: Nutrition at Glance Viet Nam. http://siteresources.worldbank.org/NUTRITION/Resources/281846-1271963823772/Vietnam.pdf

78
increase public financing for nutrition-specific and nutrtion-sensitive investments including WASH. In view of the above, it could be concluded that poor WASH indicators are contributing to malnutrition in Viet Nam. There is a need to advocate and extend technical support to the government in formulating and implementing WASH-Nutrition-Hygiene integrated programmes73. For a lack of information/data, the evaluators are unable to conclude the impact of UNICEF’s ‘Provincial Integrated Projects’ in curbing child malnutrition. UNICEF commissioned an assessment which demonstrates effectiveness of CLTS contributing to reduction in incidence of (children under 5) diarrhoea and worm infection, resulting in reduced malnutrition rates in children. The study found that diarrhoeal and worming infection rates in children under 5 in project communities were at least 1.8 and 2 times lower than in non-project communities. The study attributed these changes to strong BCC/C4D campaigns resulting in adoption of hygienic practices including water treatment and storage. There are opportunities in the form of recently approved World Bank Programme for Sanitation i.e. Program for Results (P4R), to incorporate WASH-Nutrition monitoring and cross sectoral research. Moreover, The MoH/DoH needs assistance in tracking and analysis of sanitation and nutrition. Currently, District Health Centres (DHC) are doing child growth-curve monitoring. This monitoring data can be used to calculate percentage of stunted children (i.e., low height for age) to better plan and prioritize the sanitation-hygiene-nutrition interventions at the village level. Some DHCs are already implementing this approach, however this needs to be standardised (with tools such as databases) scaled-up for evidence creation. The impact of UNICEF integrated approach on child nutrition is an aspect that needs to be explored further.
73 Viet Nam: Launch of the Scaling Up Nutrition (SUN) Movement (31 Jan 2018); https://www.unicef.org/vietnam/media_27385.html

79
4 CONCLUSION, LESSONS LEARNED AND RECOMMENDATIONS
CONCLUSION
The discussion under conclusion is structured into key evaluation criteria elements such as relevance, effectiveness, efficiency and sustainability. Relevance: The Programme has been found largely relevant for issues it intended to address vs needs identified on the ground; targeting of deprived regions and groups; selection of approaches and interventions such as integrated child development; CLTS and focus on promoting innovative and low-cost models. The prioritization of issues and implementation approaches remain relevant even today especially where country envisions to achieve ‘universal access to safe water’ and ‘countrywide ODF’, by 2030 and 2025 respectively. Effectiveness: On a whole, the Programme could be argued as effective for improving ‘enabling environment’ leaving behind capacities within the public apparatus to continue to provide responsive and sustainable services. At macro level, the rural sanitation projects achieved relatively more compared to rural water safety, as is evident from the results around improvements in enabling environment and strengthening of systemic capacities within relevant public agencies. The Programme has been successful in placing rural water safety (treatment and storage at household level) as a public policy priority in Viet Nam. The formulation of ‘Water Safety’ and ‘ODF’ Plans is a step in the right direction to achieve water and sanitation related national goals. The idea to support ‘Entrepreneur led Technology Innovation’ (in particular for low cost water filters) remains a key highlight of Programme’s effectiveness and would require continued support for scale-up. The contributions towards offering systemic solutions for ‘chronic’ water supply system O&M issue, are minimal. The contributions to rural sanitation are more systemic, as the Programme has visibly contributed towards institutionalisation of a new approach i.e. CLTS/CATS. The enabling tools and operational guidelines including pool of master trainers and implementers have been created and bodes well for future replication and scale-up. The Programme has come to resolve the mandate related issues as MoH/VIHEMA now stand as primary implementer(s) of rural sanitation. MoH/VIHEMA may continue to need technical assistance to improve processes and introduce innovation. The monitoring systems are nascent and evolving, hence would need support together with research, documentation and knowledge management. The field evidences suggest that the programme has contributed towards accelerating access to safe water and hygienic latrines, however the extent to which this has increased remains unknown. This confirms the viability of the hypothesis and the programme logic model (ToC). Efficiency: The Programme is assessed to be largely efficient for timely completion (of activities despite significant delays in approval of work plans); consumption rates (funds); leveraging of public resources; and balanced allocation of resources. For limited desegregation of financial information, the evaluators could not perform ‘value for money’ assessment. Sustainability: The Programme has largely been successful in cultivating public sector approval for new initiatives with demonstrated results, which bodes well for sustainability of interventions. Various policy and strategic level accomplishments of RSHP for both water and sanitation, are likely to sustain, though requiring continued technical support and nurturing (by the government) for sustainability and scale-up. Key issues that merit continued support and follow-up from UNICEF and donors are: the certifications of ‘clay-pot ceramic filter’, formulation of standards and guidelines to govern WASH related public-private partnerships, continued assurance of the quality of the ceramic filter in scale-up phase, formulation of water-safety and ODF plans for the remaining provinces, and most importantly, the continued financing of these plans from government sources. The Programme has certainly contributed towards increased access to latrines, however, the success for fostering ‘social norm’ for exclusive latrine use is not much visible; and whatever has been achieved around ‘social norm’ creation is less likely to sustain due to lack of a clear post-

80
ODF agenda within government led implementation. Slippage has come up as an issue which may require changes in CLTS delivery approach particularly with respect to inclusion of post-ODF interventions and monitoring. WASH Nutrition: The cross sectoral impact of WASH interventions remains largely unknown, despite the fact that considerable data is gathered around key indicators regularly. The literature from the recent past suggests an ‘inverse correlation’ between sanitation and child malnutrition (e.g. stunting) in Viet Nam. However, in lieu of limited evidence (including the unavailability of anecdotal accounts), the evaluators are unable to establish the extent of UNICEF’s contributions in denting child malnutrition in the selected provinces. The evaluators may advise to commission a separate study to establish conclusive evidence around WASH and malnutrition in Viet Nam for new programming and advocacy. Cross-cutting Priorities: The Programme approaches and interventions suggest coherence with the principles of equity, gender, resilience and HRBA. In the end, the evaluators emphasize that public sector partners anticipate continued technical assistance from UNICEF for realising the vision of universal access to safe water and country-wide ODF. There are opportunities such as World Bank funded ‘Water and Sanitation Programme’, where UNICEF Viet Nam could provide specialised and complementary technical inputs to steer the direction and leverage public financing for water and sanitation results. This underpins continued relevance of and need for UNICEF to continue with WASH sector support, albeit specialised technical inputs.
LESSONS LEARNED
This section outlines key lessons including the good practices. These have been drawn based on the field evidences and by the key stakeholders themselves. The fact that the guidance and practices vary around documenting lessons learnt, the evaluators followed the guidance provided by Maurer. R (2012)74 to frame lessons learnt. For Maurer, the quality lessons learnt must entail four ingredients or elements i.e. rationale; pre-conditions; lessons or suggestion; and the applicable task.
1. The community-based development interventions must attempt to leverage the existing community platforms and the representatives, to benefit fully from their good-will and influence. The Programme demonstrated successful application by engaging with ‘Village Head’ and other community forums such as Farmers Associations, Women Groups, etc. to mobilise communities; however, there is a need for further strengthening the role of these influential actors and forums. Implementation in contexts like Viet Nam, where recognised representatives and community forums are available, must actively consider engaging and utilizing such forums (instead of creating parallel forums) for sustained interest and motivation through built-in incentives (both monetary and non-monetary) for them.
2. Social entrepreneurship is critical to achieving social impact. The Programme has applied a good practice of ‘Entrepreneur-led Technology Innovation’ (for low cost water filters), and merits replication in other sectors for achieving child and community well-being e.g. sanitation, nutrition, etc. The model offers opportunities for innovation, localisation, livelihoods, and sustainable results amongst others. The future work must encourage relevant public agencies to explore avenues to engage more meaningfully with private sector to demonstrate successful models of ‘Public-Private Partnership’ and ‘Social-Entrepreneurship’.
3. The ‘Integrated (multi-sector) Approach’ for provincial projects has evidently created value in leveraging thematic overlaps, complementarities, and optimisation (of resources). One example is the integrated C4D campaigns which facilitated wider outreach through
74. Maurer, R. (2012). 'Lessons Learned: Utilizing lessons learned from project evaluations in policy decision making.' i-eval THINK Piece (No. 1). Retrieved from: http://www.ilo.org/wcmsp5/groups/public/---ed_mas/---eval/documents/publication/wcms_180328.pdf

81
complementary messages on a range of child well-being issues including water safety, safe sanitation, hygiene promotion particularly handwashing with soap, nutrition and child protection. Public agencies can explore and implement integrated models and approaches for evident benefits.
4. Evidence creation holds key to effective advocacy. The Programme did neither focus on evidence creation nor developing the capacities of relevant public partners in knowledge management, research and evidence creation. In Viet Nam and elsewhere with similar context, the upstreaming work must allocate adequate resources for research and evidence creation including capacity development of relevant public agencies to sustain the momentum. This becomes even more relevant to contexts like Viet Nam where donors’ interest is waning, and grant-funding is facing a squeeze.
5. The availability of adequate and qualified team is critical to successful implementation of technical assistance initiatives. A critical appraisal of resource costing suggests that limited human resource capacities were available (within UNICEF) to manage a Programme of this scale and complexity. Where it strained the existing resources, it cost the Programme in terms of not being able to extend adequate guidance and support (to the partners) in areas such as documentation. The downstream work (technical assistance interventions) must take a considered view of having sufficient and adequately qualified resources in the team to justify the varied expectations (both of UNICEF and partners) and to extend desired level of technical inputs and oversight in all programmatic areas.
RECOMMENDATIONS
A series of strategic and operational level recommendations are listed below. These have been framed based on field evidences, stakeholders’ suggestions, and in relation to the sectoral priorities of the GOV and UNICEF. On that count these could be argued as a product of ‘participatory’ discussions with range of different stakeholders namely UNICEF, MARD/DARD, MoH/VIHEMA, donors, communities and others. The recommendations are also informed by the suggestions and views discussed during a ‘Briefing Session’ with the senior officials of the Country Office and Programme Management of UNICEF Viet Nam, held on October 27, 2017 towards the end of the field mission in Viet Nam. Furthermore, the feedback received from ERG members on the brief note on field findings (post field debrief) did contribute to framing the recommendations also. The feedback received on the draft report helped fine-tune the recommendations further. Keeping in view the objectives of the evaluation, the recommendations have been framed primarily for UNICEF to guide its future engagement with key water and sanitation sector public entities. The recommendations have been grouped into broader thematic areas. Within those, there are key or overarching recommendations with series of associated actions. Relevant public and non-public stakeholders have also been identified for UNICEF to partner with. Moreover, each recommendation has been classified based on priority order or timeline i.e. immediate (preferably within 6 months), medium-term (preferably within 1-2 years) and Long-term (preferably within 2-3 years). The responsible entities to follow up have also been tagged. Recommendations for UNICEF (Rural Water Supply, Safety and Rural Sanitation)
Recommendations / Actions Relevant Stakeholders
Priority
Monitoring System (Water) 1. Align and harmonize the current monitoring indicators, tools and
reporting system for water safety and quality with SDG 6.1 targets and indicators;
I. Continue to remain engaged with MoH (preferably in partnership with WHO) to advocate for review and rationalisation of water quality standards for regular water quality testing/monitoring and timely dissemination of results for necessary action by MARD/DARD.
MoH, MARD, NCERWASS, PCERWASS, VIHEMA, Provincial PMUs,
Immediate (6-12 Months)

82
II. Extend technical assistance to the DoH including any other relevant agencies (involved in health data collection) to add behavioural monitoring aspects (at HH level) into the current monitoring system and use data to inform design of future BCC campaigns.
Water Safety Products and Promotion (Water) 2. Continue advocacy with MARD to support local businesses and
entrepreneurs for innovation and cost reductions for localised water-safety products and additional public-sector investments for BCC campaigning to influence people’s behaviour. In this connection, the proposed actions are as follows:
I. Extend requisite support to the entrepreneur involved in ‘ceramic filter’ to acquire necessary approvals and certifications from the government as to market the product nationally. Given need, help drawing the marketing/scale-up plans for the low-cost water filters.
II. Advocate with World Bank and relevant public agencies involved in upcoming WB-GOVN Programme to allocate adequate resources for BCC (preferably as part of integrated and if not then stand-alone) for water safety practices. Encourage relevant stakeholders to leverage and integrate learning from RSHP supported C4D and replicate where appropriate.
MARD, NCERWASS, PCERWASS, MoH / VIHEMA Provincial PMUs
Immediate to Medium-term (1 to 2 Years)
Research and Innovation (Water and Sanitation) 3. Enable relevant public-sector partners to explore, establish and
support partnerships with private sector research entities, academia, and businesses for technology innovation and contextualisation. The support should include:
I. Together with MRD and MoH undertake a mapping exercise to identify research, academia and businesses involved in WASH technology research and services. Encourage MARD and MoH to form partnerships (and where possible get involved directly) to support research for technology and services innovation (for water safety, hygienic and low costs latrines, disability and disasters resilient inclusive designs, on-site and off-site safe excreta management and others).
II. Support PO to undertake supply chain assessments (for water and sanitation related products and services) to identify bottleneck and gaps and use the information to guide relevant government departments to engage constructively to address the challenges.
III. Enable relevant Government Ministries/departments (MPI, MoH and MARD and others) to develop, review and/or revise partnership guidelines and manuals, to facilitate the involvement of private sector/businesses in planning and delivery of rural water and sanitation services (uninterrupted water supply; local production of sanitary items, low-cost solutions for latrine construction, pit emptying etc.)
MoH, MARD, MPI, Provincial PMUs, Sector partners (WB etc.).
Medium-term to long-term (2-3 Years)
Resource Mobilization and Provision of Equitable Services (Sanitation) 4. Continue advocating and lobbying with national and provincial
governments for approval of ‘Provincial ODF Plans’ and allocation of adequate resources for implementation of plans; and provide technical support to VIHEMA/DoH where required for
MoH, MARD, MPI, Provincial PMUs, Sector
Immediate to Medium-term

83
effective CLTS/CATS implementation. The support could also include:
I. Involve central Ministry of Planning (MPI) to support the relevant ministries for resource planning and mobilization (to ensure financing of ODF plans) using the available monitoring data, reports and analysis for decision-making by the management.
II. Initiate a dialogue with VSPB to influence their loan policy to introduce progressive microfinance/loans products, for WASH facilities/services, that ensure bank products/services are accessible to poor, the poorest of the poor and including the minorities.
partners (WB etc.).
(1 to 2 Years)
Social Norm Integration (Sanitation) 5. Review the successes, bottlenecks and opportunities in the
implementation of CLTS/CATS for creation of ‘social norm’ (for handwashing with soap and latrine use) considering the existing capacities of local government tiers and the communities as well.
I. Engage with MoH and MARD to take a considered view of the social norms approaches and make decision about inclusion into CLTS/CATS programming. Given positive decision, enable key government functionaries understand the concepts and practices of social norm creation and provide technical support in integrating social norms theories/practices into CLTS/CATS delivery. This will require a detailed review/revision of the existing CLTS training and operational manuals to include module on ‘social norm’ theory principles and approaches; and to improve other content based on the learnings from RSHP implementation.
II. Undertake capacity needs assessment of the front-line staff involved in triggering and BCC campaigning, to identify gaps in their development communication and dissemination capacities, followed by a comprehensive regular training agenda to enhance their capacities for effective triggering.
MoH, MARD, MPI, Provincial PMUs, Sector partners (WB etc.).
Immediate to Medium-term (1 to 2 Years)
Coordination, Partnerships, Advocacy (Water and Sanitation) 6. Encourage and where required extend technical support to PO
MARD to play its due role effectively in public advocacy, sector coordination, increased resources allocation and research and evidence creation. The technical support should prioritize;
I. Comprehensive capacity assessment of PO (around mandated functions) to identify key bottlenecks and capacity gaps, and to inform future UNICEF-PO engagement in areas of common interest. UNICEF should lobby for added focus and resources for PO to strengthen capacities of PO to embrace stewardship.
II. Encourage and support greater MARD- MoH joint working in areas where they can complement each other and advocate for separate and additional public allocations to MoH at national and sub-national levels to maintain the momentum created for rural sanitation.
III. Support research and evidence creation (by PO MARD) for O&M to use that for advocacy with relevant national/provincial authorities to address causes rather than symptoms around chronic O&M challenge e.g. rationalisation of water tariff (where required include variable), strengthening of tariff collection
MARD, MoH, MPI, Provincial PMUs, Sector partners (WB etc.).
Medium-term (1 to 2 Years)

84
mechanisms, improving skills (at local level), strengthening supply chain (for parts availability), and others.
IV. Extend support to and build capacities of PO to undertake/commission cross -sectoral research such as WASH-Education, WASH-Health etc, to generate evidence to highlight the linkages and garner added support for WASH prioritisation and resources allocations.
Monitoring System (Sanitation) 7. Extend technical assistance in revamping of rural sanitation
related ‘Monitoring System’ to enable sector partners draw relevant, usable and timely (monitoring) information and evidences to inform the decision-making. This may involve:
I. Review and revamping of the current monitoring system (including data collection tools, templates, reporting formats and technology integration for monitoring and reporting) while keeping in view the SDG 6.2 targets & indicators as well as the MoH criteria/standards and national targets.
II. The revamped system must have distinct pre and post ODF monitoring mechanisms and guidelines including assessment of the slippage in ODF certified communities.
III. Enhancing technical capacities of the monitoring units within MoH/DoH to produce regular analytical reports, case studies for innovative work, cross-sectoral impact and efficiency analysis.
MARD, MPI, Provincial PMUs
Medium-term (1 to 2 Years) to long-term (2-3 Years)

85
Appendix 1: Terms of Reference RFP 2017-03 7
Evaluation of the UNICEF Viet Nam’s Rural Sanitation and Hygiene Programming 2012-2016 1. Background status of water and sanitation in Viet Nam With three decades of rapid economic growth, Viet Nam’s GDP (Gross Domestic Product) has expanded five-fold and per capita incomes quadrupled to US$1,908. As Viet Nam qualified as a lower middle-income country (LMIC) in the year 2010, the international aid for development programming started to decline. The drop-in aid also reduced technical assistance that used to come through the donors. Under these circumstance, to meet its commitment towards the MDGs and to eliminate open defecation by 2025 and to ensure sustainable water supply for all by 2030, Government of Viet Nam (GOVN) had increasingly called for UNICEF’s technical assistance while taking action to increase coverage in the field. While UNICEF has been providing assistance to GOVN in W ASH programming for over last four decades, the nature of support has changed – from the provision of water points to more focus on sanitation, hygiene and developing enabling environment for universal and equitable coverage of water and sanitation. During last five years, the assistance has been mostly upstream in nature, including influencing policy and investment decisions through best practice demonstrations, introduction of innovations and programme advocacy. Viet Nam has met the water supply related MDG target and access to improved water sources in now quasi universal. Quality and sustainability of water supply services remain an issue however. Viet Nam is one of the countries were the MDG target for sanitation was also ultimately met and where open defecation (OD) rates have dropped the most in the MDG period, with a reduction of 38.5 percentage points nationally between 1990 and 2015. Viet Nam has made significant progress with respect to increasing coverage on sanitation over last decade and half. In rural areas, access to an improved sanitation facility is 77.7%, with open defecation (OD) in the fields at 5.8%. In addition, 36.5 per cent households in Mekong delta use hanging latrines that releases excreta directly to the water bodies (MICS, 2014). Thus, over 12 Million people release their excreta to their immediate vicinity that come in their contact – 6 Million defecating on open field and another 6 Million on water bodies. However, 16% of the population still use unimproved sanitation facilities, mainly households located in rural areas. Disparities are significant especially among one-third of the provinces i.e. 21 of total 63 provinces in the country, mostly in the northern mountains and central highlands where most ethnic minorities reside. Inequities persist also by income category, with only 60% of the population in the poorest quintile having access to improved sanitation, against 80-100% for all other quintiles. Improvements have been made among the poorest quintile, but more needs to be done (JMP 2015 report). At the same time, there is a need to help households claim up the sanitation ladder. Viet Nam is now also challenged with the ambitious targets with ‘safely managed’ water supply and sanitation targets set with the Sustainable Development Goals (SDGs). In many respect, personal hygiene is still an issue in Viet Nam but handwashing with soap practices has increased. It is estimated that 86% of households have a dedicated place for handwashing with water and soap present. This percentage is lower in rural areas (83%), in the Northern Midlands and Mountainous Area (75%) and in households of the poorest quintile (around 65%). Institutional context Ministry of Agriculture and Rural Development (MARD) is the overall responsible ministry for rural water supply and sanitation programme, mostly involved in the policy and investment decisions, and sector coordination. The lead department at national level assisting MARD is the National Centre for Rural Water Supply and Sanitation (NCERWASS). NCERWASS is providing planning and implementation support – including assistance to MARD in developing related policy and strategy. NCERWASS is providing technical assistance to the provincial centre for rural water

86
supply and sanitation (PCERWASS) across all the 63 provinces. PCERWASS, operating under the department of agriculture and rural development (DARD), is responsible for overall planning, designing, implementing rural water supply and sanitation in their respective provinces. Although MARD is the lead ministry for the WASH sector, the responsibility for sanitation and hygiene is assigned to the Viet Nam Health and Environment Management Agency (VIHEMA) under the Ministry of Health (MoH). VIHEMA is providing technical assistance to all the 63 provincial Centre for Preventive Medicines (CPM) on sanitation and hygiene. CPM, operating under the department of health (DoH), is responsible for overall planning, designing, implementing rural sanitation and hygiene promotion in their respective provinces. The CHE (Provincial Centre for Health Education), also under the DoH, supports hygiene promotion alongside several other life-saving health behaviours. At the province level, DARD remains responsible as the overall WASH sector lead. Ministry of Planning & Investment (MPI) and Ministry of Finance (MOF) play the role to support planning and budgeting of the WASH programme. MPI primarily finances infrastructure development, whereas MOF supports recurring expenses. Similar arrangements prevail in the provinces with corresponding counterparts such as Department of Planning & Investment (DPI) and Department of Finance (DOF). The much-needed recurring budget is often low, although the sector demands relatively high investments in the ‘soft’ components such as for community mobilization, training, monitoring, etc. Moreover, coordinated planning and investment in the sector is a matter of concern. Ministry of Foreign Affairs (MOFA) supports the development cooperation and partnership with international agencies. There are technical working groups supporting the sub-sector coordination such as: sanitation working group and O&M working group. The membership in these groups include participants from relevant private sector, non-governmental organizations, academic institutions, UN agencies and the World Bank. The national rural water supply and sanitation partnership looks after the coordination of all sectorial agencies through various working groups. Several international NGOs such as Child Fund, Church World Service, East Meets West, Plan International, SNV Netherlands and World Vision operate with sporadic presence in limited scale. UNICEF continues to provide a co-lead role to various coordination mechanisms and influence the agenda and content of the technical working groups. Provincial coordination is managed by Provincial Steering Committees (PSCs) with equivalent partners such as PCERWASS, PCPM, NGOs, mass organizations, etc. The coordination is weak in most of the provinces due to inadequate intent and low capacity of provincial governments (Joint Annual Review, 2015). The Viet Nam Bank of Social Policy (VBSP) provides subsidized loan for sanitation and non- subsidized loan for water. Mass organizations like Women’s Unions and Farmers Unions coordinate community involvement in financing, construction and management of facilities. Despite the engagement of these national actors, the W ASH sector has constantly faced low public funding especially for rural sub-sectors. UNICEF recently assisted GOV to mobilize a soft loan of US$200 million from the World Bank for the investment in rural WASH for the upcoming five- year period 2016-20, in 21 underdeveloped provinces, where the challenge related to inequities and sustainability continues to remain high. The rural WASH monitoring system was embedded in the national target programme with the technical assistance from several donors including UNICEF, DFAT (Australian Department of Foreign Affairs and Trade and DANIDA (Danish International Development Agency). However, several limitations exist in the ongoing monitoring mechanism (to be distinguished from household surveys) such as: definitions used in the monitoring systems are inconsistent with global MDG definitions, and monitoring system does not provide information regarding functionality and use of W ASH services. The newly defined monitoring indicators for SDG targets is going pose further challenge. Therefore, there is a need to overhaul the monitoring system.

87
Overview of UNICEF rural sanitation and hygiene programming UNICEF has introduced community approaches to total sanitation (CATS, inspired by the community-led total sanitation approach, CLTS) in 2008 and sanitation marketing (SanMark, aiming to support the supply of sanitation goods and services to meet the demand) later through VIHEMA and provincial CPMs that has yielded positive results in triggering over 800 villages and in achieving over 400 Open Defecation Free (ODF) villages in 7 UNICEF’s focus provinces so far. Handwashing promotion has been integrated in the CATS approach. Based on equity considerations, UNICEF advocated to change the position of MoH/VIHEMA from high-cost specifications to low-cost improved sanitation options to meet to the low capacity and willingness to pay of the poorest quintile1. The Ministry of Health (MoH) realized the potential of this success and is on its way to scale up CATS and SanMark across the country with the introduction of national guidelines on ODF verification and certification. However, like in other countries, there are issues around sustainability of the ODF. Under UNICEF’s 2012-2016 country programme with the Government of Viet Nam, the WASH programme aims to contribute to the following objective (named ‘outcome’ in UNICEF’s internal planning system) “By 2016, increased quality and effective management of a comprehensive national health system, including health promotion and health protection, with a focus on ensuring more equitable access for the most vulnerable and disadvantaged groups”. Under this outcome, the rural sanitation and hygiene is reflected in the following ‘outputs’ at national and sub-national levels. National level: Output 4 (National WASH): By 2016, identified beneficiaries benefit equitably from increased access to sustainable and hygienic sanitation and water supply. Sub-national level: 1 CATS in Viet Nam primarily deploys community led total sanitation (CLTS) and school led total sanitation (SLTS). Some of the pilot projects supported by NGOs promote some more approaches including PHAST. Usually CATS and SanMark are used simultaneously. Recent support from UNICEF has helped promotion of pro-poor SanMark, allowing poorest quintile households to build and use latrines. This in turn has helped achieve ODF.
Output 6 to 12 (one for each of the seven rural provinces): By 2016, identified beneficiaries in focus province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic Child Survival and Development (CSD: nutrition, WASH & Maternal, New born and Child Health) services, to reduce infant mortality and malnutrition and improve child development. A theory of change for the rural sanitation and hygiene component of the UNICEF WASH programme was not developed at the outset of the programme cycle. A simplified one (graphical representation of its result chain) will have to be reconstructed for the purpose of this evaluation during the inception phase, spelling out key inputs, activities, outputs, outcomes and impacts. In order to deliver on the sanitation and hygiene component of its programme, UNICEF has supported the government partners since 2012 through the following projects, adopting the CATS and SanMark approach:
1) Water and Sanitation for Children Project with MARD
2) CSD Project with MoH (WASH component with VIHEMA)
3) CSD components of 8 provincial projects (Dien Bien, Lao Cai, Ninh Thuan, Gia Lai, Kon
Tum, An Giang, Dong Thap and Ho Chi Minh City).
The main provinces where UNICEF intervened in rural sanitation and hygiene over the 2012-2016 period are: An Giang, Dong Thap, Ninh Thuan, Kun Tum, Gia Lai, Lao Cai and Dien Bien. UNICEF also provided technical assistance support to the GOVN at national and subnational levels with the aim of: improving policy environment, strengthening sector coordination, demonstrating innovative approaches/strategies with replicable potential. UNICEF has supported the sector to

88
mobilize resource and committed to assist GOVN to meet to the MDGs related challenges – and more recently, the new SDG targets. The main donors of the sanitation and hygiene component of UNICEF’s WASH programme are: Unilever, SIDA – as thematic fund, and several National Committees. Although CATS and
SanMark approaches are deployed across all seven focus provinces, the degree of success in achieving ODF varied. The provinces that are relatively successful are An Giang, Dien Bien, Kun Tum and Lao Cai, whereas Dong Thap and Gia Lai found it challenging to arrive at ODF villages. UNICEF is now entering in a new programming cycle, with a new Country Programme Document (CPD) signed with the GOVN for the period 2017-2021. This is an opportunity for UNICEF to report to its donors and partners on the achievement and quality of what has been done so far, and to re-think or refine its WASH programming and more particularly its strategy to rural sanitation and hygiene. Moreover, the social norms approach recently an area of investigation in UNICEF for all types of interventions aiming to tackle issues related to collective behaviour such as open defecation and lack of handwashing. UNICEF Viet Nam is interested in adopting this lens to guide its reflection toward improved rural sanitation and hygiene programming.
2. Evaluation purpose, objectives, and scope Purpose The evaluation’s main purpose is to generate substantive evidence on the results of the rural sanitation and hygiene programme component in the period 2012-2016 for accountability purposes to the various UNICEF’s partners, to inform the new cooperation programme between UNICEF and the GOVN, and to influence the government policies, strategies and funding priorities. More specifically, the evaluation will:
1) Promote accountability: to provide evidence to UNICEF’s partners on the performance around the implementation of CATS, SanMark, and hygiene promotion, both at downstream
and upstream level.
2) Support evidence-based decision making: to inform management decision on adjustment,
cessation, continuation or scaling up of current approaches.
3) Contribute to develop detailed WASH programme planning to align the new Viet Nam WASH
programme to the new Global WASH strategy for the upcoming period 2017-2021.
4) Contribute to the global learning: to contribute to the overall global rural sanitation and
hygiene knowledge base with additional learnings from Viet Nam.
Objectives and scope The specific objectives of the evaluation are to evaluate the achievement and quality of UNICEF’s strategy and programming in the following areas, encompassing both upstream and downstream work, and both national and subnational interventions:
1) Sector policy, strategies, M&E and coordination, with focus on rural sanitation and hygiene
2) Community approaches to total sanitation
3) Sanitation marketing
4) Handwashing promotion
The evaluation will also aim to improve the general understanding in Viet Nam and within UNICEF around collective sanitation and hygiene practices and the social norms approach and will apply this social norm approach to help improve the effectiveness of the rural sanitation and hygiene programming.

89
The timeframe for the evaluation is the country programme period from 2012 to 2016. Target Audience The primary target audiences of the evaluation include the UNICEF Country Office (CO), the Government of Viet Nam (GOVN), particularly relevant line ministries (MARD, MoH), but also the Ministry of Labour, Invalids and Social Affairs (MOLISA), Ministry of Planning & Investment (MPI), Ministry of Finance (MOF), Ministry of Foreign Affairs (MOFA) and selected provincial line departments. The secondary audience may include other UN agencies and donor agencies working in the area of sanitation, hygiene and health/nutrition in Viet Nam, NGOs, mass organizations, Private Sector agencies and development partners, particularly the World Bank. Other stakeholders in the WASH sector more generally (outside Viet Nam) may be interested to learn from this evaluation in Viet Nam, particularly from the integration of the social norms approach in the evaluation design. The dissemination and use of the evaluation will be supported with a communication plan. A summary note will also be presented to the Prime Minister’s Office to receive necessary coordination and policy decision supports, as the evaluation result may call for. Other sector partner agencies such as the World Bank and international/national NGOs and mass organizations will also be presented with the findings of the evaluation. Depending on the request of line ministries, the result will be shared with the provinces to influence financing, planning and implementation support in the field. The recommendations of the evaluation will also constitute the basis for UNICEF’s management response and be used by UNICEF and the GOVN to develop a detailed plan of actions to improve future WASH / rural sanitation and hygiene policies, plans and programmes. 3. Evaluation criteria and key questions The objective of this evaluation is to assess the relevance, effectiveness, efficiency, scalability and sustainability of the rural sanitation and hygiene component of the WASH programme as well as the extent to which it contributed to equitable results for children. The evaluation will therefore be guided by the OECD DAC and UNICEF evaluation criteria of relevance, effectiveness, efficiency, equity & gender, and sustainability/scalability. These criteria are defined in brackets the table below in the form of broad questions, and more specific evaluation questions are proposed that will need to be further refined for the purpose of this evaluation during the inception phase. Questions related to social norms are indicated in italic. Criteria Definitions and generic evaluation questions
Relevance
[Did the programme do the right thing? Relevance to the local context, needs and capacities; internal relevance of the programme design] To what extent has the UNICEF rural sanitation and hygiene programme been (and is still) relevant given the improving conditions in the country, the remaining WASH challenges especially in the 2012-2016 intervention areas, the factors that explain these remaining challenges (including people’ s beliefs and expectations regarding open defecation), the higher ambitions set out by the SDGs, the decreasing funding capacity of UNICEF, the increasing but still limited funding capacity in-country (GOVN, local authorities, households, private sector, other players), and the probable shift in external aid from grants to loans?
Has it added value to what others sector stakeholders were doing – and does it still do?
How could UNICEF adjust its strategy and programming in the sector to better target its contribution to the WASH SDGs (notably to safely managed sanitation) where there is a stronger need and where it has an added value and comparative advantage, and use its limited funding capacity to leverage other external and national resources?
In general, were the various components and activities well designed, necessary and sufficient in order to create the targeted outputs and logically lead to the achievement of the intended outcomes related to the eradication of open

90
defecation, use of improved sanitation, handwashing practices, and sector coordination (as per the theory of change)?
In particular, did the program set the creation of a new social norm for ODF as an intended objective (formally or informally) and was it designed and implemented in order to modify beneficiaries’ beliefs and expectations?
Effectiveness
[Did the programme do it right? Level of achievement and quality of programme activities, outputs and outcomes; reasons for success and failures] To what extent did the collective practice of OD disappear and the practice of handwashing at critical moments has taken up as a result of CATS (at the time of certification, or shortly before or after)? To what extent the SanMark component has effectively helped households climb up the sanitation ladder and improve the quality of their latrines? What are the main internal and external factors explaining success and failure? Internal factors: programme design and implementation fidelity (including the robustness of the CATS triggering and verification/certification process, and the frequency and quality of post- triggering monitoring, including on aspects related to handwashing); external factors: technical, financial, institutional, environmental/ physical, and social, at the local level and in the enabling environment Among the social factors; to what extent a social norm for ODF was created? To what extent has UNICEF effectively contributed to improving policies, strategies, national M&E systems, and stakeholder coordination in the area of rural sanitation and hygiene?
Efficiency
[Relationship between achieved results and inputs invested by the programme] Is the level of achievement of outputs and outcomes related to the eradication of open defecation, use of improved sanitation, handwashing practices, and sector coordination satisfactory when compared to the level of financial and human resources mobilized/used?
Has the rural sanitation and hygiene programme been designed and managed in a way that aimed to reduce unit cost (without compromising on quality and sustainability of results)?
More specifically, is UNICEF sufficiently integrating rural sanitation and hygiene with its other WASH interventions to maximize results and impacts while reducing operational costs?
Has there been any significant delays in programme implementation and achievement of results, and if so, why?
Sustainability and scalability
[Have the result sustained or are they likely to sustain over time? Is the programmatic approach designed in such a way that it can be taken up to a larger scale in-country?] To what extent did the ODF status and the associated social norm sustain since certification (in communities certified in the earlier years of the evaluation period)? To what extent did the handwashing practices sustain since certification (in communities certified in the earlier years of the evaluation period)? What are the technical, financial, institutional, environmental/physical, and social factors, in the field and in the enabling environment, that enabled or constrained the sustainability of handwashing, of ODF, and of the supporting social norm for ODF - or that are likely to influence it in the future? Are there any elements in the programme design and implementation arrangements that should be improved to strengthen the social norm for ODF and enhance sustainability? Understanding that there are reports on slippage as some sections of the communities return to their original habit of open defecation, despite their
villages attain/accredited with ODF status. How such slippage be managed as this may lead to a reputational/ branding risk for UNICEF?

91
To what extent can and should the geographical reach of the rural sanitation and hygiene programme be augmented in the future? Where should UNICEF and the GOVN focus their effort in terms of upscaling going forward?
Equity & gender
[Has the programme benefitted the most in need with the intention of reducing inequities? Have equity considerations been integrated at each stage of the programme cycle?] Did CATS and SanMark interventions adequately target and take into account the needs of the poorest quintile, the remote populations and the ones with the worst sanitation and hygiene conditions in the Northern midlands and Mountainous areas, the ethnic minorities, the women, and the elderly and disable people, at each stage of the programme cycle (situation analysis, targeting of geographical areas and villages, programme design and implementation, monitoring and evaluation)?
To what extent have they been included in the activities/processes that aimed to create a social norm for ODF?
Are these population groups the ones who have not embraced the new social norm for ODF and who have reverted back to OD?
Is the cost burden generated by the rural sanitation and hygiene interventions –especially CATS, SanMark, and handwashing – too high for those population groups (affordability of promoted latrines, soap etc.)?
How have they been adequately addressed in UNICEF’s upstream work (policy advocacy, stakeholder coordination, and support to national M&E systems)?
NOTE: These questions are a loose guide for the development of a proposal for bidding submission; they can be further refined by the selected consultancy team at inception phase. 4. Evaluation design and methodology overall design The evaluation should employ mixed methods combining quantitative and qualitative methods using a combination of tools for data collection and analysis. A special focus will be put on the social norms component of this evaluation. The overall methodological approach should be utilization focused and participatory and should ensure that the various groups including the most disadvantaged, will be reached and their voices elicited. The following outlines some key methodological requirements for the proposed evaluation. On this basis, a more detailed methodology will be proposed by bidders in their technical proposal and finalized in collaboration with UNICEF and partners during the inception phase. Key data sources and data collection methods The key data sources and data collection method that may come in use include the following depending on the logic of results: Re-construction of the programme theory of change, assessment of its logical/result framework, SWOT analysis
Desk review of secondary information/ documents: including UNICEF programme documents, annual reports, progress/ completion reports, implementing partners’ report, joint assessment reports, best practice documentations, key meeting notes and field monitoring visits reports, past surveys and evaluations, assessments undertaken by the line ministries and sector partners, etc. A preliminary list of key documents to be reviewed is provided in appendix 1.
Key informants’ interviews to receive inputs from individuals/groups who have institutional memories and direct work experience in and around the sector. This will be guided by a set of semi-structured interview questionnaires – adjusted depending on the respondent category. Key
informants include UNICEF WASH programme staff, line ministries representatives at national and subnational levels listed in the background section of this TOR, implementing partners such as NGOs and CBOs, service providers such as private sector companies and entrepreneurs involved

92
in the SanMark activities, WASH donors, academicians and sector experts, local authorities/constituencies, frontline workers, and beneficiaries.
Various social research tools are possible including national/sub-national workshops, questionnaires, PRAs and focus group discussions.
Field visit to a representative sample of districts/ communes within selected provinces – to observe infrastructures and behaviours and to collect primary information from communities especially from women and children. Observation checklists and household survey questionnaires will be designed in a way that ensures accuracy of data collected, minimization of bias, and triangulation between various data sources and categories of respondents.
It is proposed that three out of seven UNICEF’s focus provinces (Dien Bien, Lao Cai, Kon Tum, Gia Lai, Ninh Thuan, An Giang, and Dong Thap) are selected at the subnational level for more in-depth analysis – each of these provinces representing three distinct regions Northern Mountains, Central Highlands and Mekong Delta. The suggested provinces are those where technical and financial resources from UNICEF have predominantly focused; and also because of their diversity, representing different regions of Viet Nam. However, the Evaluators may decide to adjust this list of provinces based on additional criteria (to be included in their technical proposal) to meet to the evaluation objectives. UNICEF will provide any information requested on programme size, spending, context, etc. to permit the consultants to develop a sampling method that is both robust and useful.
It is proposed that (at least) two professionals from the evaluation team will be on each field mission, one of them having proficiency in Vietnamese. Field visits in each province may take at least 4 to 5 days depending on the selected locations which may be hard-to-reach. The technical proposal from the bidders must indicate how long a visit should be, who will participate, and why this is recommended.
The evaluation team is invited to consider the need to visit other areas where UNICEF has not intervened or where other non-UNICEF supported players have intervened, but comparison purposes (some villages in one/two districts in each visited province). Meetings with other sector players than UNICEF are also possible.
Bidders are invited to propose additional data sources and innovative data collection methods. For the social norms component of this evaluation, further methodological guidance is provided in appendix 5. Methodological support will be provided by UNICEF country office, regional office and HQ upon request. Data analysis and reporting Triangulation of methods and data is required, preferably through the analysis of both quantitative and qualitative data and with a range of stakeholders. The evaluation will analyse any trends and evolutions in the period covered by the evaluation. Analysis of disparities across population groups of interest (listed further above) will also be central to the methodology. Any variation across geographical areas will be highlighted and processes and results will be compared with those of other programmes/projects when possible. The bidders are asked to provide in their technical proposals how they will include this comparative or external perspective – for example how CATS and SanMark results or practices be compared to the other sanitation programming approaches. Good or bad practice that will be documented. Towards the end of the reporting phase, a workshop will be organized to present and discuss/validate preliminary findings and discuss/formulate recommendations. Design and implementation issues Potential organizational and methodological challenges to the evaluation need to be identified by bidders in their technical proposal, and appropriate mitigation measures proposed. They will be further refined by the evaluation team and UNICEF during the inception phase. Not all contingencies can be forecast, so dialogue will be required. The following are a few specific points that can already be stated. On an as-needed basis, consultants will be granted access to UNICEF databases and necessary software to utilize them. This will include access to the UNICEF

93
Intranet and permission to freely access all material found there. As noted earlier, certain telecommunications support can be expected (teleconferences, survey distribution) but the consultants must fully manage the events/processes that utilize these means. For field visits, UNICEF Viet Nam will support to the extent possible, especially in items like security advisories and facilitating contact with key informants. During field visits, the consultants are expected to handle their accommodation, food, travel (including vehicles), organizing workshops – related per diem, translators, renting premises, tape-recorders, videographer, and appropriate insurance of the contractor’s workers. Consultants will travel under a consultant Travel Authorization, per UN regulations. Ethical consideration As per United Nations Evaluation Group (UNEG) Norms and Standard and Ethical Guidelines for UN Evaluators, Evaluators’ Code of Conduct, as well as UNICEF’s revised Evaluation Policy, and UNICEF Procedure for Ethical Standards in Research, Evaluation and Data Collection and Analysis, the evaluation team should be sensitive to beliefs, manners and customs, and act with integrity and honesty in relationships with all stakeholders. Furthermore, consultants should protect the anonymity and confidentiality of individual information. Respondents will not be provided any reward or financial compensation for their participation that may influence their response. Consultants should respect the confidentiality of the information which is being handled during the assignment. Consultants are allowed to use documents and information provided only for the tasks related to the terms of reference of this evaluation. Data will be stored in a secure location, kept confidential with access restricted to principal investigators. The study data will be used only for the purpose of this study. 5. Activities, deliverables and timeline The assignment is scheduled from April to September 2017. Key tasks and expected deliverables with corresponding indicative timeline T asks Deliverables Timeline Inception phase
Final inception report in English and Vietnamese, including Evaluation tools (questionnaires, interview forms, guidelines etc.), endorsed by UNICEF, MARD and MoH (Deliverable 1)
Review existing documents & meeting key people in UNICEF/ Ministry/Department
Week 1-6
Refine and finalize evaluation questions, methodology, matrix, criteria for evaluative judgment, and sampling strategy Develop tools for interviewing, field visits etc. Draft and finalize inception report including appendices and final report outline, in consultation with UNICEF and stakeholders Data collection and report drafting phase
1st draft report produced in Vietnamese and English (Deliverable 2)
Week 7-11
Conduct data collection at national and sub- national level Conduct sampling and organize field visits Analyse and validate data/information collected Draft the evaluation report Finalization phase
Final evaluation report in Vietnamese and English (including recommendations, plus appendices and 4-7-page Executive Summary) endorsed by UNICEF, MARD and MoH
PowerPoint presentation in Vietnamese and English with key findings and recommendations of the evaluation report
(Deliverable 3)
Week 12-17
Present findings and validate recommendations with stakeholders, once the draft report is produced Solicit and integrate comments into revised draft report Finalize and submit the evaluation report and presentation

94
Appendix 2: Evaluation Matrix
Key Evaluation Questions (Modified) as provided in ToRs
Key Indicators Data Collection
Tool Information
Sources
RELEVANCE
EQ1: To what extent has UNICEFs rural water, sanitation and hygiene programme (RSHP) been relevant (to context/beneficiaries needs, existing capacities, national priorities and the work of other sector partners) for improving rural water supply (access and quality), hygienic sanitation and personal hygiene i.e. handwashing with soap?
% of rural population having access to (government approved numbers) clean water, hygienic sanitation, and practicing handwashing with soap, in particular 7 provinces where UNICEF extended technical and financial assistance;
Evidence of poor rural water supply, hygienic sanitation and hygiene’s impact for women and children in particular e.g. health, economic, education and others
Evidence of rural water supply, hygienic sanitation, and handwashing with soap as national priority in terms of sector plans and allocation of resources
Evidence of adequate focus of both public and sector partners to address needs of most vulnerable groups e.g. ethnic minorities, people from remote regions and Mekong delta
Stakeholders’ views of UNICEF’s technical assistance being relevant in terms enabling relevant public entities with formulating sector policies, standards and plans, innovation and scaling (including SanMark), and capacity development, and sector coordination
Stakeholders’ views of appropriateness of UNICEF technical assistance delivery approach
Stakeholders’ views of state of sector coordination across public agencies and sector partners and areas of improvement/assistance
Availability of Programme TOC and assessment of logic/pathways of change
Stakeholders’ views of policies, plans and practices being informed of equity considerations including disaster and climate change risks
- Key Informant Interviews (KIIs);
- Secondary Sources Review (SSR)
- MoH (national & provincial level), VIHEMA, MoF, WSSP Provincial Steering Committees and working groups
- WSP, DANIDA, SIDA, Plan)
- Selected CHE, CPM< DARD, MARD
- NCERWASS/PCERWASS
- UNICEF and other WASH sector experts;
EFFECTIVENESS

95
EQ2: To what extent has UNICEF technical assistance effectively contributed to creating an enabling WASH Governance environment (policies, strategies, national M&E systems and Stakeholder coordination) for rural water supply, hygienic sanitation, and handwashing with soap?
Number of national and subnational, new/existing policies, plans, training materials, and standards related to rural water supply, hygienic sanitation, and handwashing with soap (behavioural change, are either formulated and/or revised and approved
Evidence of heightened focus on improving operations and maintenance (O&M) of rural water supply schemes, water safety (better treatment and storage) e.g. new policies, practices and finances for O&M, engagement of private sector, and monitoring and accountability
Introduction of new approaches, plans, training contents, and practices and/or strengthening of existing approaches for rural (hygienic) sanitation and hygiene education e.g. handwashing with soap;
Availability and implementation of new BCC/C4D approaches and actions plans for low cost high impact behavioural interventions for water safety, latrine use, and handwashing with soap
Improved monitoring (including resources) and data management and use of monitoring data/analysis for decision making
Evidences of new policies, plans, and practices being more informed of equity, disaster risk reduction and climate change considerations e.g. for most poor, ethnic minorities, remote and hard to reach communities, and others;
Stakeholders views of research and development in development of innovative and low-cost technologies and products for rural water supply (water treatment and storage) and hygienic sanitation, and extent these are in use;
New coordination forums created, and/or existing coordination forums strengthened at national and sub-national levels e.g. rural sanitation, O&M, and PPP others;
- KIIs;
- SSR;
- FGDs;
- Relevant Government Departments as mentioned above
- Programme Beneficiaries
- Programme related staff (Sanitarians/frontline workers, entrepreneurs; masons, religious leaders)
EQ3: To what extent has UNICEF strengthened the public-sector lead delivery and contributed to knowledge, attitudes and practices improvements around key water safety, latrine use and hygiene behaviours e.g. handwashing with soap?
Change in numbers/percentage of rural households (from 2012 to 2016) for rural households reached out through water safety education campaigns and have understood and apply hygiene behaviours (stop OD, latrine usage and maintenance, handwashing with soap) water safety practices i.e. better treatment and storage practices;
Evidences of progress made in terms of villages triggered, declared or certified, new latrines built/upgraded, and people reached out with improved BCC/C4D campaigns
Change in numbers of people reported sick and sought health advice for water borne diseases and those linked to unhygienic practices
Evidence of decrease in water-borne diseases including stunting (in children) in ODF certified communities and those where water safety practices are common
- KIIs
- FGDs
- SSR
- Post-KAP Household Survey (HHS)
- Relevant Government Departments as mentioned above
- Programme Beneficiaries
- Programme related staff of the UNICEF, IPs, NGOs/VBOs, (Sanitarians/ frontline workers, entrepreneurs; masons, religious leaders)

96
EFFICIENCY
EQ4: To what extent the level of achievements (outputs and outcomes) justify the financial and human resources used?
Stakeholders’ views of timely completion of UNICEF interventions
Proportional costs across intervention areas i.e. water safety, ODF, and HWWS
Costs per beneficiary for water safety, ODF, and HWWS
- KIIs
- SSR
- Project Financial records/reports and Government Departments
- Programme staff
SUSTAINABILITY
EQ5: To what extent did the ODF status and the associated social norm as well as hand washing practices are likely to sustain?
Evidence in relation to planning, executing and use of a sustainability compact. Post-ODF capacities and monitoring mechanisms at community level and within Government system
Evidences of ODF/CLTS implementation integrating social norms creation and post ODF monitoring and reporting
% of ODF verified/certified communities that are maintaining ODF its ODF status one year after /verification/certification
Evidences of slippage and actual erosion of ODF status over time (prevalence of latrine existence and use; prevalence of empirical and normative expectations; and correlation of empirical/normative expectations with the latrine usage)
Stakeholders’ views of achievements that shall sustain beyond RSHP completion e.g. policies, plans, standards, training materials and trained human resources, innovative products, and others
- KIIs
- FGDs
- SSR
- Post-KAP Household Survey (HHS)
- Relevant Government Departments as mentioned above
- Programme Beneficiaries
- Programme related staff of the UNICEF, IPs, NGOs/VBOs, (Sanitarians/ frontline workers, entrepreneurs; masons, religious leaders)
EQUITY, GENDER, DISASTER AND HRBA
EQ6: What key approaches and strategies were adopted to enable RSHP projects and interventions priorities/integrate the needs of the vulnerable and marginalized groups (poor, remote communities, ethnic minorities, women, children, poor, elderly, people with disabilities) and results achieved?
- Evidences and stakeholders’ views of RSHP projects and interventions prioritizing the under-developed regions and vulnerable groups for support
- Evidences of RSHP advocating prioritization of poor, disabled, women and children, and minority groups in national and sub-national policies and plans
- Stakeholders’ views of RSHP strategies and interventions prioritizing vulnerable groups (poor, minority groups, hard to reach communities, and others)
- Evidences and stakeholders’ views of results tracked and reported for poor, disabled, women and children, and minority groups
- KIIs
- FGDs
- SSR
- Post-KAP Household Survey (HHS)
- Relevant Government Departments as mentioned above
- Programme Beneficiaries
- Programme related staff of the UNICEF, IPs, NGOs/VBOs, (Sanitarians/ frontline workers, entrepreneurs; masons, religious leaders)

97
Appendix 3: Sampling Frame (Sampling Rationale and Strategy)
Sample Size Calculation The intention of the Household survey is to get a representative indication about WASH interventions (in particular post-ODF 'latrine use' and 'handwashing practice' for social norm assessment) within the targeted communes (the study universe). The study aims to predict the pertinent proportion of the universe. A parsimonious and representative sample is very important to get true idea about population parameter(s). In absence of any specific information on exact population size or the number of households in each commune/village, and assuming the 'normal distribution' of the total population across the study universe and adopting a conservative baseline, the population size doesn’t matter in calculation of sample size. To get the optimal sample size our calculation is based upon designated margin of error, level of confidence and baseline level of the indicator. In the calculation provided below we have calculated the sample size using the 95% confidence level and 5% margin of error. Table below explains the parameters used in the formula to calculate an optimal sample size.
Level of Confidence (LOC)
Describes the level of uncertainty in the sample mean or prevalence as an estimate of the population mean or prevalence. Recommended value: 1.96 (for 95% confidence level)
Margin of Error (MOE)
The expected half-width of the confidence interval. The smaller the margin of error, the larger the sample size needed. Recommended value: 0.05
Baseline levels of the indicators (Ind)
The estimated prevalence of the risk factors within the target population. Values closest to 50% are the most conservative. Recommended value: 0.5 if no previous data on population, else value closest to 0.5 from previous data
Formula: for LOC = 1.96 (95% Confidence Level); MOE = 5% and Ind = 0.5
Sample Size (n) = LOC 2 x Ind x (1 – Ind)
MOE 2
Sample Size (n) ≈ 384 In order to control the other methodological errors or biases, the Consultants propose to increase the sample by approximately 5% of the total calculated number, thus, the total proposed sample size equals 400 HHs for the Household Survey. List of Randomly Selected Triggered, Verified and Declared Districts Note: The villages in the table below were chosen from the list of Triggered, Verified and Declared (TVD) villages in the selected districts and provinces. The district and province, in turn, were randomly selected from those intervention provinces and districts which had a majority of TVD villages. Note that the district of Hồng Ngự has been replaced with Thuận Bắc based on feedback received from the government on health-related security risks.
E# Region RS Province District Village CLTS check
Rand
2 C S1 Ninh Thuận Thuận Bắc Ba Tháp TVD 0.233 3 S2 Gò Sạn TVD 0.377 8 S3 Kiền Kiền 1 TVD 0.616 5 S4 Hiệp Thành TVD 0.675 6 S5 Bình Tiên TVD 0.706 7 S6 Hiệp Kiết TVD 0.875 4 S7 Giác Lan TVD 0.927 1 Mỹ Nhơn TVD 0.978
34 N S1 Lào Cai Bắc Hà Cốc Môi TVD 0.110 33 S2 Na Áng B TVD 0.113 44 S3 Háng Dê TVD 0.125 43 S4 Phéc Bủng 2 TVD 0.127 29 S5 Km 3 TVD 0.168 30 S6 Km 6 TVD 0.198 45 S7 Làng Mới TVD 0.304 47 Bản Phố 2A TVD 0.314 35 Dì Thàng 2 TVD 0.332

98
E# Region RS Province District Village CLTS check
Rand
38 Nậm Mòn TVD 0.349 39 Cốc Cài Hạ TVD 0.471 40 Lèng Phàng –Làng Mương TVD 0.482 36 Na Hối Tày TVD 0.505 28 Na Hối Nùng TVD 0.634 46 Phéc Bủng 1 TVD 0.715 31 Chỉu Cái TVD 0.786 37 Sín Chải A TVD 0.816 41 Cốc Cài Thượng TVD 0.920 32 Nhìu Lùng TVD 0.932 42 Bản Phố 2B TVD 0.998
120 S S1 Đồng Tháp Hồng Ngự Phú Lợi A TVD 0.249 121 S2 Phú Lợi B TVD 0.251 122 S3 Thị TVD 0.350 126 S4 Trung 1 TVD 0.512 119 S5 Phú Trung TVD 0.534 115 S6 Long Hòa TVD 0.547 116 S7 Long Thạnh TVD 0.557 124 Ấp Ba TVD 0.567 125 Thượng 1 TVD 0.702 123 Trà Đư TVD 0.703 118 Phú Hòa A TVD 0.758 117 Long Thới B TVD 0.862 114 Long Hậu TVD 0.901
List of Selected Districts in the Target Population
Table 1: List of sampled provinces, districts and villages
Province District Commune Village TVD flag Rand
Đồng Tháp Tân Hồng TT Sa Rài Khóm 1 123 0.639 Khóm 2 123 0.306 Xã An Phước An Phát 123 0.208 Án Thọ 123 0.214 Xã Bình Phú Gò Da 123 0.682 Xã Tân
Phước Hoàng Việt 123 0.597
Tân Bảnh 123 0.523 Lào Cai Bắc Hà Bản Phố Háng Dê 123 0.125 Làng Mới 123 0.304 Phéc Bủng 2 123 0.127 Na Hối Cốc Môi 123 0.110 Km 3 123 0.168 Km 6 123 0.198 Na Áng B 123 0.113 Ninh Thuận
Thuận Bắc Bắc Phong Ba Tháp 123 0.233
Gò Sạn 123 0.377 Công Hải Bình Tiên 123 0.706 Giác Lan 123 0.927 Hiệp Kiết 123 0.875 Hiệp Thành 123 0.675 Lợi Hải Kiền Kiền 1 123 0.616

99
Appendix 4: Inception Phase Data Collection Format This document contains a set of formats in which the data/information needed for the evaluation can be organized. These can be used directly or simply as a guide to outline what precisely is needed. Each format is accompanied by an explanatory note. Please feel free to add any information available/necessary.
Format 1: Overview/Status of Availability of Information / Datasets
Type of Information / Dataset Availability Status
(Yes / No)
Baseline Survey
Mid-term Survey
Monitoring Data
List of ODF Certified Villages/Communes
District wise list of staff involved in implementation
Contact list of District Level Programme managers
List of VSC (Village forums) formed during Programme
List of sanitary marts/entrepreneurs involved in Programme
…
…
…
Explanatory note: a list of datasets (generated by various kinds of contracts, monitoring systems and tools) that are available and relevant to the evaluation).

100
Appendix 5: Questionnaire for the Household Survey RSHP Evaluation - Household Survey Questionnaire
Project Name RSHP Viet Nam Type of questionnaire Post-KAP Survey
Job Number Version Revised
AAN Associates Pakistan Address: 108, Executive Heights, F-11/1, Islamabad, Pakistan www.aanassociates.com
Questionnaire number
RESPONDENT DETAIL
Name of Respondent (Mr./Mrs/Miss/Ms)
Address
Phone Hand phone
RECORD OF INTERVIEW
Name of Interviewer/ Recruiter
No. ID
Supervisor name No. ID
Day of the Week Mon 1 Tue 2 Wed 3 Thu 4 Fri 5 Sat 6 Sun 7
Date of Interview Date Month Year Time Began Time Ended
Total Length of Interview
INTRODUCTION Hello, my name is __________________________ and I am working with DEPOCEN and AAN Associates, Pakistan, on behalf of UNICEF, Country Office, Viet Nam. We are conducting a survey that asks households about various Water, Sanitation, Hygiene and Health conditions at their home. Your house has been selected to do an interview for our project. We would very much appreciate your participation in this survey. This information will be used to help UNICEF and the Ministry of Health plan for and later evaluate the sanitation project in this area. The survey should take about 45 minutes to complete. The information you provide will be kept confidential and will not be shared with anyone other than members of our project team. Your responses will also be anonymous and not tied back to you in anyway. Participation in the survey is voluntary. If we ask you any questions you don’t want to answer let me know and I will go on to the next question. You can also stop the interview at any time. We hope that you will participate in this survey, as your input is important to us. Do you have any questions about the survey at this time? May I begin the interview now? IF RESPONSE IS NO – THANK THE RESPONDENT AND STOP INTERVIEW

101
G1. Name of Province – Circle Answer (SA) G2. Name of District - Circle Answer (SA) Lao Cai 1 Bac Ha 1
Ninh Thuan 2 Thuan Bac 2
Dong Thap 3 Tan Hong 3
G3 Commune
G4 Village
G5 Name of Head of Household
G6 Sex of the Head of Household Male 1 Female 2 G7 Age of a Head of household
G8 Ethnic group (of the Head of the Household)
QUOTA: 50% MALES AND 50% FEMALES G9: What is your relationship to the Head of Household? (SA)
Self - Head of Household 1 Father-in-law 10
Wife/Mother 2 Grandfather 11 Mother-in-law 3 Son 12 Grandmother 4 Son-in-law 13
Daughter 5 Brother 14 Sister 6 Nephew 15 Niece 7 Cousin 16
STOP INTERVIEW AND SAY THANK YOU
Daughter-in-law 8 Not Related 17 Husband/Father 9 Unknown 99
INSTRUCTIONS Priority to be interviewed should be given to the head of the family or the housewife. If either of them are available, it is allowed to interview other member of the family aged ≥18 years who know about the topic of the interview the most. G10: The confidentiality statement has been read to me. I understand it and give my verbal permission to
proceed with the interview. (SA)
Yes 1
No 2 STOP INTERVIEW AND SAY THANK YOU
DEMOGRAPHIC INFORMATION
I1: May I know your current age? INTERVIEWER: THE RESPONDENT IS ELIGIBLE FOR INTERVIEW IF HIS/ HER AGE IS ≥18 I2: Respondent’s gender (SA)
Male 1 Female 2
I3: How many people live/or stay in this house today? Not including guest or relatives who stayover for a
few days. __________ persons. (SA)

102
I4: Now I’d like to know in detail the age and sex of people living in your household today, but not including guest or relatives who stay over for few days.
INTERVIEWER ASK FOR EACH AGE GROUP AND GENDER.THEN WRITE DOWN THE ANSWER AND THE TOTAL IN THE COLUMN GIVEN. THE TOTAL NUMBER OF PEOPLE LIVING IN THE HOUSEHOLD SHOULD BE THE SAME AS THE ONE MENTIONED IN I3.
AGE MALE FEMALE TOTAL 5 years and under 6 – 15 years 16 – 45 years 46 years or above TOTAL
I5. What is the highest level of schooling you completed? (SA)
No formal education 1
Not completing primary school 2
Primary 3
Pre-Secondary 4
Secondary 5
Higher 6
I6: Does your household own any of the following items? (MA)
READ AND ASK FOR EACH ITEM - MULTIPLE ANSWERS
Radio 1 Bicycle 7 Television 2 Animal drawn cart 8
Mobile phone 3 Car/truck 9 Telephone 4 Boat with motor 10
Refrigerator 5 Own agriculture land 11 Motorcycle/scooter 6 Own farm animals 12
I7: What is Average monthly income from all sources, of your households? (SA PER CELL) ASK FOR SPECIFIC ANSWER I.E. NOT A RANGE OF AMOUNT
Which of following activities are your household income sources in 2016? 1. Yes 2. No 99. Do not know/ Refuse to answer
If yes, total Income in 2016
I7 I7A
1 Crop production
2 Livestock production
3 Temporary wage
4 Regular salary
5 Processing agricultural products; Trading; and small business
6 Work as craftsmen
7 Support from the relatives
8 Support from the government
96 Other sources (specify)
10 Total

103
ND1. Did your village/family experience any natural disaster/s during last two years, which may have caused destruction (including water sources) and human/economic losses?
Yes 1
No 2 GO TO W1
Don’t know 99 ND1A. If Yes, Please specify;
Flood 1
Drought 2
Earthquake 3
Other (specify) 88
WATER ACCESS
READ OUT “NOW I WANT TO ASK YOU ABOUT ACCESS TO WATER FOR YOUR FAMILIES USE”. SHOW CARD W1: What is your current primary source of water for drinking and cooking? (SA)
CIRCLE ONLY ONE PRIMARY SOURCE
(1) Improved Sources (2) Unimproved Sources
Piped into dwelling, plot or yard 1.1 Unprotected dug well 2.1
Public tap/standpipe 1.2 Unprotected spring 2.2
Tube well/borehole 1.3 Cart with small tank/drum 2.3
Protected dug well 1.4 Bottled water 2.4
Protected Spring 1.5 Tanker Truck 2.5
Rainwater collection 1.6 Surface water (river/dam/lake/pond/stream/canal) 2.6
Other (specify) 88 W1A: Do you always have access to this drinking water source year-round? (SA)
Yes 1
No 2
Don’t know 99
W1B: Is the drinking water from your main source clean?
Yes 1
No 2
Don’t know 99
W1B1. Is the drinking water from your main source of acceptable quality in terms of? (Record separately for each option)
a. Taste 1. Yes 2. No 99. Don’t know
b. Odour/Smell 1. Yes 2. No 99. Don’t know
c. Appearance 1. Yes 2. No 99. Don’t know
W1C: Is the drinking water from your main source safe?
Yes 1

104
No 2
Don’t know 99
W2: What is your current main source of water for bathing, toilet flushing, cleaning etc.? (SA)
(1) Improved Sources (2) Unimproved Sources
Piped into dwelling, plot or yard 1.1 Unprotected dug well 2.1
Public tap/standpipe 1.2 Unprotected spring 2.2
Tube well/borehole 1.3 Cart with small tank/drum 2.3
Protected dug well 1.4 Bottled water 2.4
Protected Spring 1.5 Tanker Truck 2.5
Rainwater collection 1.6 Surface water (river/dam/lake/pond/stream/canal) 2.6
Other (specify) 88 W3: Do you always have access to this water source for household needs (bathing, toilet flushing, cleaning
etc) year-round? (SA)
Yes 1 GO TO W3C & W3D
No 2 GO TO W3A & W3B
Don’t know 99 GO TO W3C & W3D
W3A: If NO, when do you NOT have access to this water source? (SA)
During the dry season 1
During the rainy season 2
Don’t know 99
W3B. When this source is not available, what other main sources do you usually use? (SA)
(1) Improved Sources (2) Unimproved Sources
Piped into dwelling, plot or yard 1.1 Unprotected dug well 2.1
Public tap/standpipe 1.2 Unprotected spring 2.2
Tube well/borehole 1.3 Cart with small tank/drum 2.3
Protected dug well 1.4 Bottled water 2.4
Protected Spring 1.5 Tanker Truck 2.5
Rainwater collection 1.6 Surface water (river/dam/lake/pond/stream/canal) 2.6
Other (specify) 88 W3C: Is your current main source of water for bathing, toilet flushing, cleaning etc. clean?
Yes 1
No 2
Don’t know 99
W3D: Is your current main source of water for bathing, toilet flushing, cleaning etc. safe?
Yes 1
No 2
Don’t know 99
WSS. Is Water Supply Scheme available in your commune/ village?
Yes 1

105
No 2 TO S1
Don’t know 99
W4. Who manages/operates (takes care of operations and maintenance of water source) the Water Supply Scheme (for drinking water) in your village? Note: For those villages/households where the water is provided by the public sector/private sector piped water schemes and others.
Provincial Agriculture & Rural Development Depart 1 Village Water User Committee/Group 2 Private Contractor 3 Don’t Know 99
W5. Is a trained technician/plumber available locally (within village or neighbouring village) to operate and undertake minor repair/maintenance of Rural Water Supply Scheme?
Yes 1
No 2
Don’t know 99
W5.1. Are commonly used spare parts for Rural Water Supply Scheme available locally (in the village or neighbouring village)?
Yes 1
No 2
Don’t know 99
W6. Is loan (facility) available to install and/or major repair/upgrade Rural Water Supply Scheme?
Yes 1
No 2 GO TO W7
Don’t know 99
W6A. If ‘Yes’ who provides the loan?
Government Depart 1 Micro-finance institution 2 Bank 3 Local lender 4 Others (please specify) 88
W7. Are there charges in your village to access water from a Rural Water Supply scheme?
Yes 1
No 2 GO TO W8
Don’t know 99
W7.1. If someone in your village did not pay to access water from the water supply scheme, what would happen to them? (MA)
Legal/financial penalty 1
Community members scorn/punish 2
Nothing happens 3
Other, specify 88
W7.2. How are people punished for not paying for access to water from the water supply scheme? Specify: ________________________

106
Ask this question ONLY IF, Water Tariff/payment system exists in village W8. How much do you pay for getting water (for all purposes) per month? VND _____________ If household pays water tariff, W8A. Who do you pay to access water?
Water User Committee/Community Organization
1
GOVERNMENT 2
PRIVATE OPERATOR 99
Other (specify) 88
If household pays water tariff, W8B. Do you pay as?
Fixed water tariff (monthly/daily) 1
Usage Based (or consumption) 2
Other, specify 88
W8.1. Did Government/Private Contractor/Water User Committee consult the community while setting water tariff/fee?
Yes 1
No 2
Don’t know 99
W8.2. Are subsidies/discounts available to these groups (from water tariff/fee)? (MA)
Poor 1 Women/Children headed households 2 Households with disabled members 3 Other minority groups 4 No exemptions/subsidies for any group 5 Don’t know 99
W9. How many times was Water Supply Scheme non-functional (broken down) during the last six months? Write number: ___________________ (-99. Don’t Know) W9.1. How long does it usually take to repair (make functional) in case of breakdown of Water Supply Scheme? (MA)
Never had breakdown 1 Less than a Day 2 1-3 days 3 4-6 days 4 Over a week but less than month 5 Over a month 6 Don’t Know 99
W9.2. Does the WSS remain functional (continue to provide water) during natural disasters (drought, floods and others)?
Yes 1
No 2
Don’t know 99
W10. Did you receive awareness message for water storage/treatment in last one year?

107
Yes 1
No 2 GO TO S1
Don’t know 99
W10A. If ‘Yes’, are message/s understandable to the following (MA)?
Women 1 Children 2 Illiterate (having no formal education) 3 Disabled (Visually impaired) 4 Disabled (audibly impaired) 5 Don’t know 99
W11. Do you treat drinking (water) in any way to make it safer to drink?
Yes 1
No 2 GO TO W3
Don’t know 99
W12. What do you usually do to make the water safer to drink? (MA)
Boil 1 Add bleach/chlorine 2 Strain it through a cloth 3 Use a water filter (ceramic, sand, composite, etc.) 4 Solar disinfection 5 Let it stand and settle 6 Other (specify) 88 Don’t Know 99
W13. How drinking water in your household is stored? (What type of containers you use for drinking water storage?)
Open Mouth Containers 1 Close mouth Containers 2 Don’t Know 99 Other (specify) 88
SANITATION
READ OUT - “NOW I WANT TO ASK YOU SOME QUESTIONS ABOUT THE TOILET FACILITY YOUR FAMILY USES”. S1: Does your house currently have a toilet? (SA)
Yes 1 GO TO S2
No 2 GO TO S9
INTERVIEWER: IF THE HOUSEHOLD HAS A TOILET FACILITY ASK: CAN YOU SHOW ME THE TOILET FACILITY YOUR FAMILY MEMBERS USUALLY USE AT THE END OF OUR INTERVIEW? AT THE END COMPLETE OBSERVATION QUESTION AND CAPTURE TYPE OF LATRINE. S2 – S7 IF HOUSEHOLD HAS FACILITY ASK THESE QUESTIONS
S2: Do you share this facility with other families outside of your home? (SA)

108
No. Facility only used by my household 1 GO TO S3
Yes. Shared 2 GO TO S2A
S2A: If shared, how many families use this toilet/WC facility? _____ families. (SA) S3: Why does your family use a toilet facility? (MA)
DO NOT READ OPTIONS OUT LOUD. CIRCLE ALL RESPONSES
For good health/disease prevention 1 To avoid disturbing others 8
Cleaner and healthier living in our home 2 To avoid embarrassment/humiliation 9
Convenience 3 It’s what everybody is doing 10
To have privacy when use the facilities 4 We were told it was the right thing to have 11
To be modern 5 Don’t know 99
To be accepted well by others (pride/status) 6 Other (specify) 88
To avoid sharing with others 7
S4: Which members of your immediate family usually DO NOT use this toilet? (MA)
Member Use DO NOT use
Don’t know
Not applicable
Self - Respondent 1 2 99 6 Wife/Mother 1 2 99 6 Mother-in-law 1 2 99 6 Grandmother 1 2 99 6 Daughter 1 2 99 6 Sister 1 2 99 6 Niece 1 2 99 6 Daughter-in-law 1 2 99 6 Husband/Father 1 2 99 6 Father-in-law 1 2 99 6 Grandfather 1 2 99 6 Son 1 2 99 6
Son-in-law 1 2 99 6
Brother 1 2 99 6 Nephew 1 2 99 6 Cousin 1 2 99 6 Other members 1 2 99 6
S5: How often do members of your immediate family use this toilet to defecate when at home? (SA PER ROW)
Never / Rarely
Sometimes / Occasionally
Usually / Mostly
Always Don’t know
Not applicable
Myself 1 2 3 4 99 6
My husband/ father 1 2 3 4 99 6
My wife/ mother 1 2 3 4 99 6
Children five years and younger
1 2 3 4 99
6
Children over age 5 1 2 3 4 99 6
Elderly 60 years old and older 1 2 3 4 99 6

109
Persons with disability 1 2 3 4 99 6
ES1. What type of toilet does your household have? (SA)
INTERVIEWER: SELECT APPROPRIATE ANSWER BASED ON THE DESCRIPTION PROVIDED BY THE RESPONDENT.
(1) Flush or Pour Flush Toilet
(2) Pit Latrine (3) Insanitary
latrine (4) Composting Toilet
(5)
Flushed to piped sewer
system 1.1 VIP latrine 2.1
Hanging latrine
3.1 Composting Toilet
4.1 Refused/Not able to observe
5
Flushed to septic tank
1.2 Pit latrine with
slab (concrete, wood/bamboo)
2.2
Other (specify)
88
Flushed to pit latrine
1.3 Pit latrine
without slab/open pit
2.3
Flush, don’t know where
1.4
ES2: When did your household construct latrine FIRST time? (Record estimated year, month or both) (SA)
_____ year _____ month Don’t know (99)
ES3: Have you improved/upgraded this latrine in last THREE years? If yes, when did it happen? (SA)
Yes 1
_____ years _____ months
Don’t know when improved (99)
No 2 -
Don’t know 99 -
ES4: What is your major reason for improvement/upgrading? (SA)
Construction is poor 1
Toilet location is inconvenient to use 2
Water is not available close to the toilet 3
Too many household members for one toilet (i.e. not available when you try to use it)
4
Toilet is dirty / dark / smelly 5
Other (specify) 88
Don’t know 99 ES4.1: What do you think about quality of this latrine construction? (SA)
Excellent 1 Poor 4
Good 2 Very poor 5
Fair 3
ES5: Are you aware of any available options to receive any assistance (loan, financing, gifts/grants,
Construction Material/in- kind support etc.) to help you build the latrine? (SA)
Yes 1
No 2 GO TO ES7
Don’t know 99 GO TO ES7

110
ES6: Did you receive any assistance (loan, financing, gifts/grants, Construction Material/in- kind support etc.) to help you build the latrine? (SA)
Yes 1 GO TO S6.1
No 2 GO TO ES7
Don’t know 99 GO TO ES7 ES6.1. What type of Assistance you received? (MA)
Loan 1 Please specify the kind/type of Loan? (for example, cash) Specify AMOUNT: (VND)
Grant / Gift / subsidy
2 Please specify the kind/type of Grant/Gift/subsidy? (for example, cash, cost-sharing, free labour cost of the mason) Specify:
Construction Material/in- kind
support 3
Please specify the kind/type of support? (for example, sanitary material, free labour cost of the mason) Specify:
Don’t know 99
ES7: How much did you spend (in total) on constructing your toilet? (SA) - VND. _________________________
ES7.1 Out of this, how much of this was subsidised (in cash or kind)? (SA) VND _______________ S7: Who in your family made the decision to have a latrine built for your household? (MA)
DO NOT READ OPTIONS OUT LOUD. CIRCLE ALL RESPONSES
Father/Male head of family 1
Mother/Female head of family 2 N/A latrine was in the house when we bought/rented
it 3
Don’t know/Refused 99
Other (specify) 88
TM1. Who in the family members, frequently cleans the latrine? (SA)
Boys 1
Girls 2
Women 3
Men 4
Other (specify) 88
Don’t know 99
TM2. How often latrine in your household is cleaned? Daily 1
Alternate day 2
Weekly 3
Other 88
Don’t know 99
SKIP TO S12 AFTER COMPLETING TM2

111
IF HOUSEHOLD HAS NO FACILITY ASK THESE QUESTIONS S8 – S11 DO NOT READ OPTIONS OUT LOUD S8: You said you had no toilet facility in your house, where do you and members of your family
defecate most of the time? (MA)
Bush/Field 1 Behind our house 6
Pig Pen 2 Neighbourhood toilet 7
Fish Pond 3 Communal latrine 8
River 4 Don’t know/Refused 99
Beach 5 Other (specify) 88
DO NOT READ OPTIONS OUT LOUD S9: What keeps your family from having a toilet facility at your home? (MA)
No money to construct 1
No materials to construct 2
Not enough water available 3
Don’t know how to construct 4
Don’t like the latrines I’ve seen constructed 5
Not interested/Prefer to use what we currently do 6
No land/space available to construct/Unable to construct on our land (renter, rocky soil/flood plain, not enough land, etc.)
7
Waste feeds fish/other animals 8
Don’t know/Refused 99
Other (specify) 88
10: If you decide to construct a latrine, do you know approximately how much it WILL cost you to construct your preferred type of latrine? (SA) Amount: ____________ (VND)
ASK FOR BEST GUESS BY GIVING ONE PRICE, NOT A RANGE) S11: Are you aware of any available options to receive any assistance (loan, financing, gifts/grants,
Construction Material/in-kind support etc.) to help you build the latrine? (SA)
Yes 1
No 2
Don’t know 99
ASK OF ALL RESPONDENTS DO NOT READ OPTIONS OUT LOUD S12: What do you do with the stools of babies and young children (ages 0-5)? (MA)
Thrown in toilet facility/latrine 1
Thrown in the bushes/field/animal pen river/beach/drain
2
Not disposed of/left on the ground 3
Buried in yard/field 4
Thrown in garbage/rubbish bin 5
Don’t know 99

112
N/A household does not have young children this age 7
Other (specify) 88
Community Participation and Communication Channels CC1: Has anyone in your family participated in a meeting about sanitation and or has any government
staff (e.g. sanitarian) visited your home (in last five years) to talk about building a latrine? SA
Yes 1
No 2 GO TO CC3
Don’t know 99 SKIP TO CC3
CC1a: Did you receive sufficient/useful information (awareness messages, supplies, mason etc.) to help
to construct a latrine at your home?
Yes 1
No 2
Don’t know 99
CC2b: Can you recall THREE key messages, which you have learned and/or learned and practice due to your participation in that meeting/activity?
Yes 1
No 2
Don’t know 99 CC3: What are the sources of information through which you get information about hygiene and toilet?
DO NOT READ OPTIONS OUT LOUD. CIRCLE FIRST, SECOND AND THIRD RESPONSES IN EACH COLUMN. ONLY ONE ANSWER PER COLUMN
First Answer
(SA)
Second Answer
(SA)
Third Answer
(SA) Television/Radio 1 1 1 Newspaper/Tabloid, Magazine 2 2 2 Print Materials (posters, leaflets, etc.) 3 3 3 Neighbours/Friends 4 4 4 From School Children in the family 5 5 5 Family members/relatives 6 6 6 Local authority (head of village) 7 7 7 Local Public-Address System 8 8 8 Government health workers (local health workers, etc.) 9 9 9 Sanitary Mart/Shop, local Mason 10 10 10 Commune/village meetings 11 11 11 Mass organisation (e.g. Women’s Union, Farmers’ Union, Youth Union)
12 12 12
Don’t know 99 99 99 Other (specify) 88 88 88
CC4: Which sources of information you trust/prefer the most than others?
DO NOT READ OPTIONS OUT LOUD. CIRCLE FIRST, SECOND AND THIRD RESPONSES IN EACH COLUMN. ONLY ONE ANSWER PER COLUMN
First Answer
(SA)
Second Answer
(SA)
Third Answer
(SA) Television/Radio 1 1 1 Newspaper/Tabloid, Magazine 2 2 2 Print Materials (posters, leaflets, etc.) 3 3 3 Neighbours/Friends 4 4 4 From School Children in the family 5 5 5 Family members/relatives 6 6 6 Local authority (head of village) 7 7 7
If ‘YES’, please specify any Three key messages; (Probe for stop open defecation, Construction/maintenance of latrine, continued use of latrine, any other
1 2
3

113
Local Public Address System 8 8 8 Government health workers (local health workers, etc.) 9 9 9 Sanitary Mart/Shop, local Mason 10 10 10 Commune/village meetings 11 11 11 Mass organisation (e.g. Women’s Union, Farmers’ Union, Youth Union)
12 12 12
Don’t know 99 99 99 Other (specify) 88 88 88
Questions about CATS/CLTS processes CP1: Is there any Village Sanitation Committee/Association (Forum or group of active volunteers or
other organized group of community members) involved in continuous promotion of sanitation75 (in particular latrine availability and continued use)?
Yes 1
No 2 GO TO CP3
Don’t know 99 GO TO CP3 NOTE: ON INDICATOR: PARTICIPATION OF A HIGH/LOW PERCENTAGE OF COMMUNITY MEMBERS FROM ALL CATEGORIES INCLUDING MEN, WOMEN, CHILDREN, PEOPLE WITH DISABILITIES, EOPLE FROM POOREST HOUSEHOLDS, PEOPLE FROM MINORITY GROUPS, DECISION MAKERS, OPINION LEADERS, ELDERLY, ETC) CP1a: Who are the members of Village Sanitation Committee/Association (Please mark all those
represented in the group/committee)?
1 Men 2 Women 3 Girls 4 Boys 5 People from Poor households 6 Elderly people 7 Village leader 8 People with disabilities 9 People from Minority
groups 10 Religious
people 11 Professional/Workers (sanitarian,
teacher) 99 Don’t know
CP2: Do you know, if this community has Sanitation Action Plan to achieve ODF (post-triggering action
planning and activities/actions) and for maintaining the ODF status? SA
Yes 1
No 2 GO TO CP3
Don’t know 99 GO TO CP 3 CP2a: Who were the key actors/groups involved in developing this Sanitation Action Plan? (MA)
General Community members were involved 1 Community based sanitation forum/committee or group of volunteers
2
Government Department (health facility staff etc.) 3 UNICEF or its partners staff/team 4 Other NGO/CBO was involved. Specify the name 5 Name: Don’t know 99
CP2b: Which key actor/group was in the MAIN LEADERSHIP role for developing the community action plan? (SA)
General Community members 1 Community based sanitation forum/committee or group of volunteers
2
75 SUSTAINABILITY CHECKS - guidance to design and implement sustainability monitoring in WASH: UNICEF HQ Programme
Division/ WASH, New York; UNDP-SIWI Water Governance Facility, Stockholm.

114
Government Department (health facility staff etc.) 3 UNICEF or its partners staff/team 4 Other NGO/CBO was involved. Specify the name 5 Name: Don’t know 99
CP3: Have you ever seen any map or sign in your community to stop open defection?
Yes 1 No 2
Don’t know 99 CP4. Are you aware if this community is verified as ODF verified community? If yes, do you know when did community achieve ODF Verification?
Yes 1 _____ year _____ month
No 2 GO TO CP5
Don’t know 99 GO TO CP5
CP4A: Do you know if your community as a whole received any reward or incentive for achieving ODF
status? (Positive reinforcement of rules, instructions, commitments)
Yes 1
No 2
Don’t know 99 CP4B. Do you know, if after the ODF verification, anyone come to your household/village to follow-up
and share the message/s of keep using/improving the toilet?
Yes 1 No 2
Don’t know 99 CP4C. Do you know if community members are involved in maintaining/sustaining the ODF status (post-
ODF monitoring)?
Yes 1 No 2
Don’t know 99 CP5. Where can sanitary materials and supplies for constructing toilet be purchased? (Single Answer)
Within or nearby your village/community 1
At Commune level 2
At district level 3
Don’t know 99 CP6 How do you rate the quality of the sanitary supplies (pipe, commode, etc.) and other construction
materials required to build/maintain latrine?
Excellent 1 Poor 4
Good 2 Very poor 5
Fair 3 Don’t know 99
IF ‘YES’ Please specify the type of reward/incentive awarded to your community? (Multiple answers)
1. Public recognition
2. Financial rewards
3. In-kind or material support
4. Any other Incentive or reward Specify:

115
CP7 What do you think about the pricing of the commonly available/used sanitary materials/supplies?
Very Costly 1 Cheap 4
Costly 2 Very Cheap (most economical) 5
Affordable (economical) 3 Don’t know 99
Diarrhoea Knowledge/Practice/Child Health D1: You may/may not have children 0-5, that’s fine. But you may know ways to protect young children
against diarrhoea. Please tell me all of the ways you know to protect young children (age 0-5) against diarrhoea in? (MA)
DO NOT READ OPTIONS OUT LOUD
Boil or treat your water 1
Use latrines/dispose faeces of children in latrines 2
Wash hands with soap and water 3
Cook food well 4
Store food properly/ cover the food 5
Buy food from a clean place/ not buying food from random place 6
Wash fruits and vegetables with potable/safe water 7
There is nothing you can do, it’s a normal part of life 8
Don’t know 99
Other (specify) 88
ASK ONLY IF HH HAS YOUNG CHILDREN ≤ 5 – SEE I4 D2: In the past two weeks has your child/children under the age of five had diarrhoea (defined as
three or more watery stools in a 24 period/same day or blood in the stool)? (SA)
Yes 1
No 2
Don’t know 99
Hand Washing READ OUT: “NOW I WANT TO ASK YOU SOME QUESTIONS ABOUT HAND WASHING” HW1: When do you wash your hands? (MA)
DO NOT READ OPTIONS OUT LOUD
When they are visibly dirty 1
When they smell or are sticky 2
Before cooking 3
Before eating 4
Before feeding a baby/child 5
After defecation 6
After cleaning a baby that has defecated 7
After work 8
Does not wash hands 9 GO TO HW6

116
Other (specify) 88
Don’t know 99
HW2: What do you usually use to wash your hands? (MA)
DO NOT READ OPTIONS OUT LOUD
Soap 1
Powdered or liquid detergent 2
Ash 3
Dirt/sand/mud 4
Do not use anything (cleansing agent) to wash hands 5 GO TO HW4
Other (specify) 88
Don’t Know 99
HW3: When do you usually use soap, powder/liquid detergent, ash, dirt/sand/mud or other material to
wash your hands? (MA)
When they are visibly dirty 1
When they smell or are sticky 2
Before cooking 3
Before eating 4
Before feeding a baby/child 5
After defecation 6
After cleaning a baby that has defecated 7
After work 8
Don’t know 99
Other (specify) 88
HW4: Can you share why you wash your hands (what motivates you to wash your hands)? (MA) DO NOT READ OPTIONS OUT LOUD
To prevent the spread of disease 1
To be clean 2
To smell good 3
To get rid of dirt/smell/sticky things on my hands 4
Religious reasons/beliefs 5
Was told it was the right thing to do 6
Because that’s what everyone does 7
Don’t know 99
Other (specify) 88 IF THE RESPONDENT ANSWERED OPTION 2 OR 3 IN HW2 (WASH HANDS WITH SOAP OR POWDERED / LIQUID DETERGENT) THEN ASK HW5 HW5: You said you use soap/powdered or liquid detergent to wash your hands, do you have any in your
home today? (SA)
Yes 1
No 2 GO TO R1
Don’t know 99 GO TO R1
HW5A: (SA) IF YES ASK “CAN YOU PLEASE SHOW IT TO ME” AND OBSERVE IF THE SOAP/POWDERED OR LIQUID DETERGENT TO WASH HANDS IS AVAILABLE AT THE TIME OF INTERVIEW THEN CIRCLE CODE 1 (YES)

117
IF THE SOAP/POWDERED OR LIQUID DETERGENT TO WASH HANDS IS NOT AVAILABLE AT THE TIME OF INTERVIEW THEN CIRCLE CODE 2 (NOT AVAILABLE)
Yes, available 1
No, not available 2
Unable to observe 3
IF RESPONDENT DOES NOT WASH HANDS (CODE 10 AT HW 1) ASK HW6. You said that you do not wash your hands. Can you share the reasons why you don’t wash your
hands? (MA) DO NOT READ OPTIONS OUT LOUD
No/insufficient water to wash hands 1
No soap available to wash hands 2
No ash available to wash hands 3
Don’t understand the purpose/not important 4
Don’t have time to 5
Don’t know when to 6
Don’t know 99
Other (specify) 88
SHOW CARD AND READ OUT THE FOLLOWING: “PLEASE TAKE A LOOK AT THIS CARD. IT HAS 5 BOXES ON IT. THE ONE ON THE LEFT IS STRONGLY DISAGREE AND THE ONE THE RIGHT IS STRONGLY AGREE. SHOW CUE CARDS FOR EACH STATEMENT AND WHAT EACH BOX REPRESENTS FOR THE FIELDS BELOW. I WILL NOW ASK YOU SOME THINGS THAT PEOPLE HAVE SAID ABOUT USING TOILETS AND WASHING HANDS. IF YOU AGREE WITH THE STATEMENT, PLEASE POINT TO ONE OF THE BOXES ON THE RIGHT BASED ON YOUR PERSONAL LEVEL OF AGREEMENT (AGREE OR STRONGLY AGREE). IF YOU DISAGREE WITH THE STATEMENT, PLEASE POINT TO ONE OF THE BOXES ON THE LEFT BASED ON YOUR PERSONAL LEVEL OF DISAGREEMENT (DISAGREE OR STRONGLY DISAGREE). IF YOU NEITHER AGREE NOR DISAGREE WITH THE STATEMENT, PLEASE POINT TO THE BOX IN THE MIDDLE. LET’S START FROM THE FIRST STATEMENT.” CIRCLE ONLY ONE ANSWER FOR EACH ATTRIBUTE READ OUT THE FOLLOWING STATEMENT: HOW FAR DO YOU AGREE OR DISAGREE THAT ……… (GO TO R1)
ROTATE STATEMENTS Strongly Disagree
Disagree
Neither Agree
nor Disagree
Agree Strongly Agree
R1 A lot of people think it is too expensive to have a toilet in their house
1 2 3 4 5
R2 It’s embarrassing when community members can see other people defecating in the open
1 2 3 4 5
R3 Many people don’t want to build a toilet in their house because it smells
1 2 3 4 5
R4 There is no relationship between defecating in the open and people having diarrhoea
1 2 3 4 5
R5 Most people think that it is necessary to wash their hands with soap especially after defecation
1 2 3 4 5
R6 You only need to wash your hands when they look/feel dirty
1 2 3 4 5
Social Norm Assessment
Q# Question Response Options

118
SN1 Some people use a latrine and other people do not. How often do ALL members of your household use a latrine? Note: The overall response to ‘options-5’ will indicate the slippage rate
1. Never 2. Rarely 3. Sometimes 4. Often 5. Always
SN2 Think about the people in your village, such as your family, friends, and neighbours. Out of 10 people in your village, how many do you think said that all their family members always use a latrine? (Assessment of Empirical Expectations)
Number: _________
SN3 Do you believe that people in your village should use a latrine?
1. Yes 2. No – GO TO SN4
SN3.1 Why do you think people in your village should use a latrine?
1. Because it is the right thing to do 2. Other reasons (please specify – record only 2 max)
SN3.2 Think about the people in your village, such as your family, friends, and neighbours. Out of 10 people in your village, how many do you think said that people should use a latrine because it is the right thing to do? (Assessment of Normative Expectations)
Number: ___________
SN4 If someone in your village was observed defecating in the open, what would happen to her/him? Are people punished for defecating in the open, and if YES, how?
1. Financial penalty 2. Legal penalty 3. Community members scorn / punish 4. Other 5. Nothing happens Specify ‘Other’: ___________
OBSERVATION HAND WASHING
ONLY FOR RESPONDENTS THAT REPORT TO WASH HANDS IN HW1 (CIRCLED OTHER THAN CODE 7 / 8 IN HW 1) IF THEY REPORTED TO NOT WASH HANDS IN Q HW1 9CODE 7/ 8) SKIP TO OS1 OHW1: Can you show me where members of your family most often wash their hands? SA
Within 10 paces of the toilet facility (inside or outside)
1
No specific place 5
Within 10 paces of the kitchen/cooking place 2 Other (specify) 88
Elsewhere in home or yard 3 No permission to see 6
Outside of yard 4 OHW2: OBSERVE: Is water present at the specified place for hand washing? SA
Water is not available 1
Water is available 2
OHW3: OBSERVE: Is soap or detergent present at the specific place for hand washing? SA
None available 1
Bar soap 2
Detergent (powder/liquid/paste) 3
Liquid soap (including shampoo) 4
Other (specify) X
OHW4. Can you now show me how you usually wash your hands? MA
ASK AND OBSERVE. CIRCLE ALL DEMONSTRATED
Water only 1 Used visibly clean cloth to dry 7
Soap and water 2 Used visibly dirty cloth to dry 8
Powdered or liquid detergent and water 3
Cannot demonstrate (lacks resources to demonstrate)
9
Ash 4 Unwilling/Refused to demonstrate 10

119
Dirt/sand/mud 5 Other (specify) 88
Shook hands to dry 6
OBSERVATION SANITATION ONLY FOR RESPONDENTS WITH A LATRINE IN S1 (CODE 1) IF NO LATRINE INTERVIEW IS COMPLETED – THANK THEM FOR THEIR TIME! OS1. OBSERVE: Where is the toilet facility used by members of your family located? Can you show me
where it is now? SA In own dwelling/attached to own dwelling 1
In own courtyard 2
Refused/Not able to observe 3
Other (specify) 88 OS2. What kind of toilet facility does the family have?
OBSERVATION. REFER TO THE INFORMATION IN THE SHOW CARD (1) Flush or Pour
Flush Toilet GO TO OS2A
(2) Pit Latrine (3) Insanitary
latrine (4) Composting Toilet
(5)
Flushed to piped sewer
system 1.1 VIP latrine 2.1
Hanging latrine
3.1 Composting Toilet
4.1 Refused/Not able to observe
5
Flushed to septic tank
1.2 Pit latrine with
slab (concrete, wood/bamboo)
2.2
Other (specify)
88
Flushed to pit latrine
1.3 Pit latrine
without slab/open pit
2.3
Flush, don’t know where
1.4
IF CIRCLED CODE 1 (FLUSHED TOILET) IN OS2 → ASK OS2A OS2A: Is the water you have access to adequate to meet your toilet flushing needs?
Yes 1
No 2
Don’t know 99
OS3. OBSERVE – IF ONE OR MORE SIGNS BELOW ARE SELECTED, THEN THE ANSWER WILL BE “YES”
- Path to latrine is walked on - Visibly used anal cleansing material - If Pour Flush water is available - Detected faeces in pit using flashlight - Slab is wet - Smelly
Yes 1 N/A No latrine 3
No 2 Refused/Unable to observe 4

120
Appendix 6: Qualitative Toolkit
Key Informant Interview – Local Government Departments
Key Informant Interview (Governments at Provincial level, District/Sub-district level
Officials) Informed Consent: Hi my name is __________________________ and I am working with DEPOCEN (Viet Nam) and AAN Associates (an international consulting company). On behalf of UNICEF, Country Office Viet Nam, AAN Associates is conducting an Endline Evaluation of UNICEF’s ‘Rural Sanitation & Hygiene Programme’ implemented at national level and 7 provinces (including your) from 2012-16. As part of data collection, we are speaking to you and shall ask questions on ‘Rural Water, Sanitation, and Hygiene’ situation in your province/district. We would very much appreciate your active participation in the discussion. The information that you will share will be used to synthesize evaluation findings and recommendations. The evaluation findings and recommendations will help GOVN and UNICEF to better plan and implement the national sanitation programme in future. The information you provide will be kept confidential and will not be shared with anyone other than the evaluation team members. Your responses will also be kept anonymous and not tied back to you in anyway. The group discussion will take 60-90 minutes to complete. Your cooperation would be highly appreciated. Your participation for this interview is voluntary. If we ask you any questions you don’t want to answer let me know and I will go on to the next question. You can also stop the interview at any time. We hope that you will allow us to interview you for this evaluation, as your inputs are important to us. Do you have any questions about the evaluation or the Interview now? May I begin the interview now? Note: The interviewer to adapt questions based on the specific role of the interviewee/depts. they represent, level of understanding and the nature of UNICEFs support to the different projects. Date:
Respondent Name (Mr. /Mrs.):
Organization/Department:
Designation/Position:
Province: District:
Village: Community:
Interviewer Name (Mr. /Mrs.):
Moderator Name:
Note Taker:

121
Questions: Mandate of Organization, Challenges in Services Planning, Delivery, Financing, Coordination,
1. What is the mandate and key functions of your department/organization and particularly your unit, please elaborate? Are you aware that UNICEF has been supporting the GVN (your dept.) for improved water, sanitation, hygiene promotion services? If yes, what kind of assistance did UNICEF provide?
2. Please share the key challenges your office/agency faces (or continue to face) in delivery of water/sanitation/hygiene education services in rural areas (water for DARD, Sanitation for CPM, and hygiene education for CHE)? Please elaborate on the key challenges or problem your office/agency faces in terms of planning, implementation, monitoring of services, allocation of public funds, coordination with other agencies, public education and awareness campaigns, for water, sanitation and hygiene education services for rural areas)? Please ask specifically about these areas of assistance and take note and ask for other areas if they received assistance?
3. In your view what particular groups and communities don’t have adequate water, sanitation, and hygiene education services e.g. children, women, older people, ethnic minorities, disable people, and others, (like diseases etc.) and why? How did your office/organization has planned or planning to improve services for these groups? Take note and ask for evidence if any?
4. Did you receive assistance from other organizations for their services improvement, If yes, which other agencies are those and what kind of assistance are they/have they provided and did it anyway complemented the assistance provided by UNICEF, please elaborate how?
Policies, Strategies, Action Plans, Sector Coordination, Finances (for services)
5. In the last four years (since 2012), has there been any significant changes in the a). Policies, b). Strategies c). Plans d). Coordination (within and other organizations including international agencies for WASH services) e). Increased public allocations for services for following:
I. Rural water supply (more relevant to provincial and district DARD, PSC, and PCERWASS)
II. Rural Sanitation (CPM and district DoH) III. Rural Hygiene Education (CHE and district DoH)
If yes, what are those changes and ask for evidences of any policies, regulations etc.? Also, ask for how children, women, minority groups, disabled have been prioritized in these policies, strategies, plans, coordination, and public allocations? Please share any examples and evidences (plans, budgets, strategies, regulations etc.) that support these groups etc. 6. Please share with us if UNICEF provided any assistance in improving policies,
strategies, plans, coordination and public allocations? Ask for more details of where did and how UNICEF provided assistance and if possible ask for any evidences?
7. In your view the assistance extended by UNICEF in last four years, was relevant (to your needs) and adequate (timely and complete) to your needs? Do you find any gaps in UNICEF assistance? Was you/organization consulted in planning and delivery of UNICEF assistance? If yes, please do share any examples or/and evidences?
8. Do you find any signs of improved sector coordination at provincial/district/field levels (amongst government agencies and with other international partners) and if yes, can you elaborate on that?
9. Can you share with us if the public allocations or funding for water, sanitation, and hygiene education activities (of your office/organization) has increased in past four years? Can you elaborate on this funding increase and also share any evidence of increased allocations or funding available (ask for budgets etc. and sources of these funds, donors funds etc.)?
10. How has UNICEF assistance (changes in policies, plans, coordination etc.) improved your office/organization’s abilities to the plan and implement better water, sanitation, and hygiene services? Please elaborate on what improvements you see in planning and delivery of services to rural communities? Have improvement in policies, strategies, plans, coordination, etc. helped to prioritise and offer improve services for vulnerable groups like children, women, disabled, older persons, minority groups etc.? Please explain and share any examples or evidences?
11. In your view what has worked well and what did not (lessons learnt)? Please elaborate why and share examples? Do you think that these policies, plans, coordination mechanisms continue to function (or are functioning) after UNICEF assistance is completed (to assess sustainability)? Which elements have discontinued or likely to not continue after completion of UNICEF project? Ask for evidences and examples.

122
12. Are there still areas where your office/organization continue to need UNICEF assistance (in terms of policies, strategies, actions plans, coordination) for improved water, sanitation and hygiene promotion services? What are those areas of further assistance (recommendations) and what should/could UNICEF do about those (in next 3-4 years)? Please ask for specific examples?
[For MoH/CPM focus on support in planning and during preparatory phase, pre-triggering, triggering (counselling, simulation, socialization) and post-triggering activities/processes.]
UNICEF’s Assistance for Capacity Development & Monitoring & Evaluation (overall Impact)
1. Are you aware of UNICEF assistance in Capacity Development of your office/organization? Please share more details of where UNICEF contributed to the capacity development? Share examples and evidences?
2. Can you please share how did dept./UNICEF identify the capacity development needs for your office/organization (training, systems, equipment, practices, guidelines etc.)? To what extent your office/organization was involved in the process of capacity development needs and delivery of capacity development (e.g. involvement of organization’s training unit involvement in designing and delivery of training packages)?
3. In your view, has UNICEF capacity development assistance contribute to improved services delivery to rural communities i.e. adequate and quality water (for DARD/PCERWASS, PSC), turning communities into ODF and helping them sustain ODF status (CPM, DoH, PSC), adoption of hygiene practices (CHE hand washing with soap at critical times), and others? Please share examples and evidences?
4. Please elaborate the specific activities undertaken/support extended by UNICEF for improving the depts.. monitoring and evaluation activities (services and results)? if yes, what assistance has been provided and how did it improve the office/organizations monitoring enable gathering information to make decisions (financial allocations, ODF sustainability etc.)? Do you feel there are areas where monitoring system need to be improved, please share where and how you feel those could be improved?
5. In your view, how has the monitoring improved for functionality of rural water supply schemes, operations and maintenance, quality of water etc. (this question is for DARD/PCERWSS, PSC only)?
6. In your view has monitoring improved for continuity of ODF status in those communities which have achieved ODF status? Is there any evidence of ODF certified communities reverting to OD practice? If yes, what % of communities are reverting to OD? (this question is for MoH/CPM, PSC only)
7. Post ODF Follow up: Are you aware and/or involved in any post-triggering follow-up providers/partners equipped with and trained in communication aids and training for informed-choice facilitation in communities?
8. Do you note/see any significant impact on the health, nutrition, and education, of rural people particularly children, because of improved water, sanitation, and hygiene education services in your province/district? Please share your thoughts, examples and evidences? Has there been any negative impact of these improved services?
9. In your view what has worked well and what did not (lessons learnt)? Please elaborate why and share examples? Do you think that capacity development and monitoring practices (changes or improvements) continue to function (or are functioning) after UNICEF assistance is completed? Which elements have discontinued or likely to not continue after completion of UNICEF project? Ask for evidences and examples.
10. Are there still areas where your office/organization continue to need UNICEF assistance (in terms of capacity development and monitoring) for improved water, sanitation and hygiene promotion services? What are those areas of further assistance (recommendations) and what should/could UNICEF do about those? Please ask for specific examples?
Communication for Behaviour Change – and Norms Creation
1. What are your traditional practices for hygiene education for behaviour change? Has UNICEF provided any assistance in improving the hygiene education activities of your office/organization? If yes, please share more details of UNICEF assistance?
2. How did UNICEF assistance improve the hygiene education services/activities of your office/organization? Do you feel that hygiene education is more effective now and may kindly share why you feel they are more effective? Ask for evidence and examples?
3. What particular elements/activities have been added to hygiene education to create social norm of latrine use and handwashing with soap? Can you please elaborate more on that?
4. Is there any mechanism to monitor/report on the creation of social norm or behaviour change such as continuous latrine use by all family members, handwashing with soaps? Is there monitoring evidence that may suggest that 65% households hygienic latrines (as defined by MoH) and 40% people practice handwashing with soap after critical moments (after defecation, after treating child faeces, after/before handling food)? Please share if these evidences are available with you and can you share those?
5. Existence of Sanctions: Are you aware of any community based sanctions (social & financial) that are in place to stop OD practices/no handwashing (at critical times) at

123
household or community level? How effective are these sanctions in confining community members from defecating in open? Please give examples to elaborate
6. In your view what has worked well and what did not (lessons learnt)? Please elaborate why and share examples? Do you think that communication for behaviour change activities would continue to function (or are functioning) after UNICEF assistance is completed? Which elements have discontinued or likely to not continue after completion of UNICEF project? Ask for evidences and examples.
7. Are there still areas where your office/organization continue to need UNICEF assistance (in terms of hygiene awareness/communication) for improved water, sanitation and hygiene promotion services? What are those areas of further assistance (recommendations) and what should/could UNICEF do about those? Please ask for specific examples?
Sustaining Demand Trough Supply Side Interventions, and Innovation
1. SanMark Strategy: Are you aware of any sanitation marketing strategy developed, including product options, price and payment options, place (Who will deliver to consumers and where?) and promotion (Who will inform consumers about options and how?(specifically for DoH/CPM)?
2. Service Providers: Are adequate trained sanitation service providers (masons, pit cleaning etc.) available at village/community level? If yes, please elaborate more, and if not are there any plans to train masons and other private sector partners?
3. Low cost latrine options: In your view the latrine construction costs are affordable to most people in rural areas? In last few years, if new latrine designs/technologies introduced (cheaper) and what is the cost of low cost options?
4. Disaster Resistant Latrine options: In your view the new designs are disaster resistant (withstand floods etc.) rural areas? Please elaborate on new designs and there disaster resilience?
5. Supply Chain: Are most latrine related materials are locally available (in the village or nearby villages), if not, where do people go to buy latrine materials? Has your office or UNICEF assistance helped introducing measures to strengthen the availability of materials in the village? Please elaborate and share examples?
6. Financial Support/Micro – financing: Do you know if any financial support (loan, grant, cost-sharing, in-kind assistance) is available for the poor households and other vulnerable groups to help them construct/upgrade latrine or repair of water supply services? If yes, who is providing this support? What criteria and process is used for identification of poor households? Do people access those services or are easy to access?
7. In your view what has worked well and what did not (lessons learnt)? Please elaborate why and share examples? Do you think that Sanitation Marketing activities (changes or improvements) continue to function (or are functioning) after UNICEF assistance is completed? Which elements have discontinued or likely to not continue after completion of UNICEF project? Ask for evidences and examples.
8. Are there still areas where your office/organization continue to need UNICEF assistance (in terms of Sanitation Marketing) for improved water, sanitation and hygiene promotion services? What are those areas of further assistance (recommendations) and what should/could UNICEF do about those? Please ask for specific examples?
Equity, Inclusion and Gender 1. In your view, to how do different groups were targeted, involved and benefitted (children, poor, disabled, older person, women, minority groups) from rural water, sanitation, and hygiene education (activities)? Can you explain more of how were they prioritized, involved and benefitted more? Share examples and evidences also?
2. In your opinion, what were/are the limiting factors, challenges faced by those groups (children, women, girls, elderly, disabled, minority groups), who are not responsive and motivated to; a) build and use latrine for defecation, and b) adopt improved hygiene practices, washing hands etc.
3. What are your recommendations to eliminate these constraining factors for these groups? What challenges/barriers exist that make it difficult for the poor households to construct and use latrine consistently and handwashing with soap (behaviours)?

124
Focus Group Discussion
Community Members (Male / Female Beneficiaries & Sanitation/Community Group)
[Separate group discussion to be held with male and female community members. Given availability of the Village Sanitation Group/Committee a separate session to be organized with them including other notables]
Informed Consent: Hi my name is __________________________ and I am working with DEPOCEN and AAN Associates (an international consulting company). On behalf of UNICEF, Country Office Viet Nam, AAN Associates is conducting an Endline Evaluation of UNICEF’s ‘Rural Sanitation & Hygiene Programme’ implemented at national level and 7 provinces (including this). As part of data collection, we are speaking to you and shall ask questions on ‘Rural Water, Sanitation, and Hygiene’ situation in your community. We shall ask questions related with the processes adopted for achieving and maintaining Open Defecation Free (Status) and adopting practice of Handwashing with Soap (behaviour). We would like to know your thoughts, if and what impact have the improved (or otherwise) in water, sanitation, and hygiene services and behaviours have had on you and other family members. We would very much appreciate your active participation in the discussion. The information that you will share will be used to synthesize evaluation findings and recommendations. The evaluation findings and recommendations will help GOVN and UNICEF to better plan and implement the national sanitation programme in future. The information you provide will be kept confidential and will not be shared with anyone other than the evaluation team members. Your responses will also be kept anonymous and not tied back to you in anyway. The group discussion will take 60-90 minutes to complete. Your cooperation would be highly appreciated. Your participation for this group discussion is voluntary. If we ask you any questions you don’t want to answer let me know and I will go on to the next question. You can also stop the discussion at any time. We hope that you will allow us to interview you for this evaluation, as your inputs are important to us. Do you have any questions about the evaluation or the group discussion at this time? May we begin the group discussion now?
Note/Instructions: The Moderator to adapt questions based on the types of the participants, total number of participants and anticipated level of understanding about the Programme or the topic under discussion. The Moderator will ensure;
Equal opportunity is given to each participant for sharing his/her opinion.
Views of each participant are listened and given due respect while maintaining the dignity for each member participating in the discussion regardless of the difference of opinion.
Group discussion is held in secure and safe place in a pleasant/comfortable environment.
Date: Village/Community; Province: Commune District: ODF Status?
Declared; Yes/ No Verified: Yes/No
ODF Declaration Date Estimated time period (Moth / Year)
FGD Moderator Name: FGD Facilitator Name: Note Taker: Other Detail:

125
Possible Types of FGD Participants: Community head: Religious leader Representative of local health/village sanitation group: Health workers/Sanitarians Community mobilizer/teacher/champions of sanitation Male heads of households Female heads of households/mothers of young kids Female community worker Disabled, community members with special needs
Members of households with and without latrines (at least 2 members from each group) Group Type: Male / Female/ Village Sanitation Committee/Group Participants Details S# Name Age
(Years) Profession Role in the
Community / Programme
1 2 3 4 5 6 7 8 9 10 11
Questions76
[Ask always all questions in each FGD session.]
1. Sanitation Awareness a. Are you aware if poor hygiene conditions (personal and environment) such as
open defecation, not washing hands with soaps, can have negative consequence for people? If yes, how you think these can impact people (probe if it could cause disease and what diseases are common because of poor hygiene)?
2. Latrine Existence a. How many of you have latrines in your households? )Take note of actual number
who have latrines and those who don’t have or used shared latrines) b. In your view how many households (preferably in %) in your village don’t have
latrine at home (make a guess)? Can you share what are the reasons e.g. social, economic and others, that these households don’t have latrines?
3. Open Defecation (OD) Practice a. Are there any households or members in the community e.g. minority groups,
older people, children, people with disabilities or others, who are practicing Open Defecation (OD)? If yes, are these few, many, most of the community members,
76. This tool lists the key elements that are of interest to AAN and should be essentially covered by each facilitator in each FGD discussion with men, women, and local Village Sanitation Group (if available) formed for/maintenance the ODF status. The summary notes expected must cover all these elements. This has been developed to guide field data collection teams in facilitation and documentation. All the summary sheets shall be assessed based on this and please make sure that you respond to each question in your summary sheet.

126
almost all, all? (Probe further on, who are these people (in the community) who continue to defecate in open?
b. In your view what are the 3 most important reasons for these people to defecate in open?
c. When and in under what situations/circumstances do these people defecate in open e.g. while in the field (with no latrine nearby etc.)? Do people cover excreta/faeces (with sand) when they defecate outside/in fields?
4. Shared Latrine existence and use a. In your village what is the proportion of households/families (% preferably) who
are using shared latrine? What could be the reasons for using shared latrines? b. How do people with household latrines feel for families/people who use shared
latrines? Is ‘use of shared latrine’ a common practice and acceptable to others/community, who have their own latrine?
5. Water availability & Quality a. Is sufficient water (for all purpose) available in the community throughout the
year? Explore if there is any particular seasons when village face water shortage, if yes, how do community deal with water shortages?
b. What are the most common sources of drinking water (wells, springs, canals, public water distribution system etc.)? Those who receive water from public water system (piped water from government), do you feel that drinking water quality from public water system improved in last 3-4 years? If yes, how do you know/assess that (less disease, colour or taste has changed)?
6. Awareness financing/subsidies for the poor and other vulnerable groups a. Are you aware if Did your village (or selected households without latrines) know
about or have receive any support (materials, charity, cash, labour, credit/loan, etc. - from government or VBSP other agencies) to construct latrine? Explore further what kind of assistance was provided, when and how those households were chosen and assisted?
7. Social Norm of Latrine Use (expectations and beliefs) a. In your view how many community members (in your village) think/believe that ‘all
other community members’ use latrines always, please suggest if these are few, many, most of the community members, almost all, all (register one option)?
b. In your view, how many community members think that latrine ‘SHOULD’ always be used? Do you think that they believe that using latrines (for defecation) is the right/appropriate (and explore why do they think latrines should be used always)?
8. Sanctions for Open Defecators a. What would happen if you/any other community member finds another person
(from the village) defecating in open/fields? What would be your reaction or what would you do (probe further by asking if he/she would feel of as inappropriate, complain to the family, complain to the head of the village)?
b. Are you aware if the whole village has agreed on sanctions for those defecating in open (explore by asking if there are financial or social penalties, boycott, and share last time someone found defecating in open and what had happened )?
9. Sanitary Mart (for Sanitary Materials) & Latrine Types a. Is there ‘sanitary materials shop/sanitary mart’ available in the village? Yes/No, If
no, where do people go to get the sanitary materials (cement, sand, commode, pipes etc. explore they go to nearby village or town or city, how far is it and does it cost extra for transportation)?

127
b. What are the most common latrine types in the village? Are all latrine related materials (pipes, commode, cement, bricks, etc.) for common latrine type available in the village/nearest shop (explore if those materials manufactured/produced locally)?
c. Are most common latrines connected to septic tank/pit/sewage system? Is support available for septic tank/pit emptying/cleaning services? If yes, is it easily available and are considered affordable?
10. Pricing and quality a. What is the average cost for construction of common (type) latrine, if possible ask
for materials and labour costs separately (note down the amounts)? b. Do people think the average latrine construction cost for common (type) latrine is:
Very costly, costly, affordable, cheap, very cheap (take note)? In your view what should be the price (for complete latrine construction) that is affordable for everyone?
c. What do you think of the quality of the available sanitary materials (pipe, commode, cement, etc.… and ask/note if very good, good, reasonable, poor, very poor?
d. Have you heard of (been constructed in the village) low costs latrines? If yes, how much is it costs, and if you find it hygienic/safe (note down the price difference between common type latrine and low cost latrines)?
11. Availability of the skilled Mason a. Is there mason (skilled worker) available in the village/nearby village to
construct/repair common type latrine? Are you satisfied with the quality of service/skill of the mason?
12. Equity Integration – Disability and disasters a. Can the most common (type) latrine be used by all family members (ask
specifically if that could be used by older persons, children and people with disabilities in family)? If yes, explore what additional support is included in the latrine that makes it usable by people with special needs?
b. Can the most common (type) latrine/water system withstand the common natural disasters (that strike this area) like earthquakes, floods, etc. Has there been any new latrine and water system designs/technologies and materials which are more disaster resistant? Can you please explain this more?
13. Role of the relevant government workers (who were involved in triggering, post triggering and post ODF monitoring)
a. Please share if your village is ODF certified village (explore more by asking what it means to be ODF and how/when there village became ODF and what role was played by community and by local health department/staff? Did community prepare plan for ODF and do they have plan to sustain ODF status (explore more by asking questions on what is the plan and how is that being implemented)?
14. Sanitation forum a. For ODF achievement/sustainability, is there any Village Sanitation
Forum/Committee? If yes, explore more about mandate/tasks and composition (members and their selection including training) of the forum/committee?
b. Does this Forum/Committee meet regularly and organize activities for post ODF also? Probe more on activities of the forum/committee in past one year?
15. Community volunteer/Community Resource Persons

128
a. Are there any designated community members/volunteers who were/are involved for ODF and sustainability of ODF village? Who are they and what was/is their role in achieving and sustaining ODF certification?
16. Specific questions for women group a. Who (in the household) is generally responsible for latrine cleaning? if it is
women/girls, do they feel burdened with an additional task of latrine cleaning at home?
b. How usually mothers/women mange the faeces of their young children? How common is the practice of using pampers and dispose them off?
17. Social Norms of Handwashing with Soap a. Do people generally wash hands with soap after/before certain daily activities
(explore what are those daily activities and if required give them clues about after defecation, before handling food, after cleaning child faeces etc.)?
b. In your view how many households (few, many, most of the community members, almost all, all) have handwashing stations and soap available? Are aware of risks/consequences of disease for not washing hands with soap at critical events, if yes what are those risks/consequences?
c. In your view, how many community members think that ‘other community members’ are always washing hands after/before routine activities after defecation, before handling food, after cleaning child faeces etc. e.g. few, many, most of the community members, almost all, all?
d. Did they receive any health messages (water cleaning, latrine use, and handwashing with soap) in last one year? If yes, what was the source/s of those message/s e.g. TV, radio, public address system, health worker, brochures etc.? Did you find the message/medium easily understandable and useful, if yes, please share more?
e. In your view what are the most reliable sources of health information/education (TV, radio, health worker, head of the village) and why you feel they are more reliable (explore more the reasons for reliability)?
18. Overall Impact – Health, Nutrition, Education a. Do you feel that there are improvements in water, sanitation, and hygiene
education service and behaviours (access and quality) in last three years?, if yes, please share what makes you say things have improved and how?
b. How has the improved water (quality and access) impacted the lives of the community members (probe in terms of better health – diarrhoea incidence, other water borne diseases, nutrition, etc.)? Are there any particular groups (like children, women, older people, ethnic minorities etc.) who have benefitted more because of improved water quality, and how?
c. How has the improved sanitation and allied behaviours (latrine availability and use) impacted the lives of the community members (probe in terms of better health – diarrhoea incidence, other water borne diseases, nutrition, etc.)? Are there any particular groups (like children, women, older people, ethnic minorities etc.) who have benefitted more because of improved sanitation and hygiene, and how?
d. Are you aware if there are any negative impact/consequences of improved water, sanitation, and hygiene awareness and for any particular group/s e.g. extra workload for women to fetch water, cleaning latrines etc. (probe more what negative impacts and who has been impacted)?

129

130
Appendix 7: Field Staff Training, Pre-Testing and Translation of the Finalized Tools The collection of primary data from the field commenced after approval of the Inception Report including the data collection tools and detailed field plan. The core team (International Evaluators) was joined by National staff (National Consultant, the interpreters, and support staff to conduct FGDs, etc.) and the local partner. all field data collection (complete HHS and part of FGs and KIIs) was done through the local staff under the direct control and supervision of the local partner. the international team undertook most of the KIIs at the national, provincial and district levels, along with FGDs in selected communities. The international team visited two of the three provinces for selected districts. The questionnaire for the Endline survey was developed by the evaluation specialists using various questionnaire design and tools, it did not require additional pre-testing. However, the tools were tested for reassurance during the training of field staff (data collectors, interpreters and other staff to be involved in survey monitoring and quality assurance of the data collection processes) through mock exercises. The HHs questionnaire was modified to incorporate the feedback received during training event for the field survey team. The finalized tools were shared with UNICEF. The finalized tools were translated in local languages before application in field. The training event was also attended by a member of UNICEF WASH team. The field data collection phase started with the training of enumerators and data entry operators. The field enumerators were rigorously trained. A comprehensive training plan was developed, containing information on all aspects of the survey, including evaluation purpose, methodology, questions, survey protocols, role of the field (district) supervisors, separate staff for quality assurance of the data collection processes, and field security protocols. The field training focused on comprehension of all sections by the entire field staff; with added focus on understanding and how to ask questions related to social norms. The field data collection process, particularly the field survey, included quality assurance mechanisms such as formation of tele-sheets to validate key questions, spot checks, and telephonic validations from respondents who have shared their mobile numbers. Daily data editing was done to keep check on quality and completeness of data collected from the field. Quality control during fieldwork The field team supervisors (was appointed at district level in each province) had a key role in maintaining quality control during the fieldwork:
During the initial day/s of field work, field teams was accompanied by a senior staff member of the National partners (DEPOCEN) to observe the team in the field, checking the interview process at least once for all the enumerators designated in the team. Feedback to the enumerators was given on daily basis.
Supervisors had use a questionnaire log sheet which was used to record the number of questionnaires assigned to each of the enumerators and each questionnaire (electronic form) had an identification number. When questionnaires (on electronic devices) were handed back to the supervisor, he had checked and record the completed questionnaires.
An interview log sheet was given to enumerators on a daily basis. This sheet was used to record successfully completed questionnaires per day. When an enumerator was unable to find an interviewee, they recorded the 1st visit and the time for the second appointment. If the interview was not taken place, this was also indicated in the interview log sheet and verified by the supervisor.
On a daily basis, supervisors ensured checking of all the completed questionnaires (using the electronic devices) thoroughly and take note of every mistake. Each evening each enumerator team had a meeting where all the day’s experiences was discussed and simple corrections, such as wrong additions, was made. For major mistakes, the data-collector

131
had to re-visit respondents the following morning. It was expected that frequency of mistakes had reduce throughout the lifecycle of the survey through this process.
All recorded data was sent to the server in batches, after clearance from the Quality Assurance staff was housed in local partner’s office. Before compilation of all the forms, data was checked for any inconsistencies, incompleteness. Where required, the enumerators asked to revisit some specific HH to collect data due to any noted error, which was unacceptable for further processing. This was helped to identify errors and mistakes that were missed by the field team supervisors.
All processes be complemented by support and supervision in the field by AAN staff.

132
Appendix 8: List of Key Informant Interviews
S#
Date Provin
ce Distri
ct Interview with
2nd Interview
ee 1 20/10/
2017 Ninh Thuan
Thuan Bac
Than Thi Kim Hanh - Preventive medicine team NA
2 20/10/2018
Ninh Thuan
NA Tran Thi Luyen - Planning and Investment Department Tran Thi Ha
3 NA Ninh Thuan
NA Mr. Luong Van Tri - Vice head of Health and Environment Division, Centre for Disease Control.
Mrs. Le Hoang Thu
4 NA Ninh Thuan
NA Mr. Nguyen Hoang Son - Head of Division, Ninh Thuan Provincial Water Supply Centre
Mrs. Mai Thị Xuan Hoang
5 20/10/2017
Ninh Thuan
NA Nguyen Van Binh - Vice director, Labour, Invalids and Social Affairs Department of Ninh Thuan Province
NA
6 NA NA Thuan Bac
Mr. Thap Buu Thien - Project coordinator in the district NA
7 25/10/2017
NA NA Ms. Nguyen Thi Kim Ngan - Department of Planning and Investment NA
8 25/10/2017
NA NA Mr. Dinh Van Suu - PCERWASS NA
9 NA Bac Ha NA Mrs. Duong Thi Nguyet - Director of Health Centre in Bac Ha Province
NA
10 25/10/2017
NA NA Mr. Trinh Kim Thanh - Centre for disease control and prevention NA
11 25/10/2017
Lao Cai Bac Ha
Nguyen Thi Thanh Ngan - Deputy Head of Health Education and Communication Division
NA
12 17/10/2017
Dong Thap
NA Nguyễn Ngọc Năm - Vice Director Health Department NA
13 NA Dong Thap
NA Ms. Nguyễn Thị Liên Chi - Head of Division of environmental health and health in school, Provincial Preventive Health Centre of Dong Thap province
NA
14 NA Dong Thap
Tan Hong
Mr. Nguyễn Văn Sĩ - State official of Public health division, DHC – Tan Hong district
NA
15 17/10/2017
Dong Thap
Tan Hong
Trần Văn Truyền - Head of division Communication NA
16 NA NA NA Mr. Nguyễn Thái Bình - General official, in charge of Communication - Planning
NA

133
Appendix 9: List of Participants in Key Informant Interviews
S# Province District KII Type Name - Position
Department 1 Nin Thuan Thuan Bac Staff of CPM Thành Thị Kim Hạnh - Second-in-command
Preventive medicine team
2 Nin Thuan fpr Provincial Steering Committee
1) Tran Thi Luyen - Coordinator Planning and Investment Department 2) Tran Thi Ha - Specialist Child survival field
3 Nin Thuan fpr Provincial Centre for Disease Control
1) Mr. Luong Van Tri - Vice head of Health and Environment Division Centre for Disease Control 2) Mrs. Lê Hoang Thu - Specialist of Medical Division Department of Health
4 Nin Thuan fpr PCERWASS 1) Mr. Nguyen Hoang Son - Head of Division Ninh Thuan Provincial Water Supply Centre 2) Mrs. Mai Thị Xuan Hoang - Staff Ninh Thuan Provincial Water Supply Centre
5 Nin Thuan fpr DOLISA Nguyễn Văn Bình - Vice director Labour, Invalids and Social Affairs Department of Ninh Thuan Province
6 Nin Thuan Thuan Bac CPM at provincial level Mr.Thap Buu Thien - Project coordinator in the district Preventive health centre in Thuan Bac district
7 Lao Cai fpr Provincial Steering Committee
Ms. Nguyen Thi Kim Ngan - fpr Department of Planning and Investment
8 Lao Cai fpr PCERWASS Mr. Dinh Van Suu - fpr PCERWASS
9 Lao Cai Bac Ha CPM of Bac Ha District Mrs. Dương Thị Nguyệt - Director Health centre in Bac Ha Province
10 Lao Cai fpr CPM at provincial level Mr. Trinh Kim Thanh - fpr Centre for disease control and prevention
11 Lao Cai Bac Ha Communication official of CPM at district level
1) Nguyen Thi Thanh Ngan - Deputy Head Health Education and Communication Division 2) Pham Duc Sang - Public Health Division Bac Ha Preventive Health Centre
12 Dong Thap fpr Department of Health Nguyễn Ngọc Năm - Vice director Health Department
13 Dong Thap fpr CPM at provincial level Ms. Nguyễn Thị Liên Chi - Head of Division of environmental health and health in school Provincial Preventive Health Centre of Dong Thap province
14 Dong Thap Tan Hong CPM at district level Mr. Nguyễn Văn Sĩ - State official of Public health division DHC – Tan Hong district
15 Dong Thap Tan Hong Communication official of CPM at district level
Ms. Trần Văn Truyền - Head of division Communication
16 Dong Thap fpr PCERWASS Mr. Nguyễn Thái Bình - General official Water supply centre of Cao Lanh city communication - Planning

134
Appendix 10: List of Focus Group Discussions
S# Date Focus Group Discussion with Provin
ce Distri
ct Village / Vol
Commune
ODF Status
1 NA Children group in Tan Phuoc primary school in Tan Phuoc commune
Dong Thap
Tan Hong
NA Tan Phuoc
NA
2 20/10/2017
Children group in primary school in Cong Hai commune
Ninh Thuan
Thuan Bac
NA Cong Hai
NA
3 NA Children group in My Nhon primary school in Bac Phong commune
NA NA NA Bac Phong
NA
4 NA Children group of Ban Pho secondary school NA NA NA Ban Pho
NA
5 26/10/2017
Children group of Na Hoi secondary school Lao Cai Bac Ha NA Na Hoi NA
6 NA Children group in Nguyen Quang Dieu secondary school in An Phuoc commune
NA NA NA An Phuoc
NA
7 18/10/2017
Male group in An Phuoc commune Dong Thap
Tan Hong
An Thọ An Phuoc
NA
8 16/10/2017
Male group in Tan Phuoc commune Dong Thap
Tan Hong
Viet Hong
Tan Phuoc
NA
9 26/10/2017
Male group in Na Hoi commune Lao Cai Bac Ha NA Na Hoi NA
10 21/10/2017
Male group in Bac Phong commune Ninh Thuan
Thuan Bac
Go San Bac Phong
NA
11 16/10/2017
Female group in Tan Phuoc commune Dong Thap
Tan Hong
NA Tan Phuoc
NA
12 18/10/2017
Female group in An Phuoc commune Dong Thap
Tan Hong
An Phát An Phuoc
NA
13 21/10/2017
Female group in Cong Hai commune Ninh Thuan
Thuan Bac
NA Cong Hai
Yes
14 22/10/2017
Female group in Loi Hai commune Ninh Thuan
Thuan Bac
Kien Kien 1
Loi Hai NA
15 26/10/2017
Female group in Na Hoi commune Lao Cai Bac Ha NA Na Hoi Yes
16 22/10/2017
Mixed group in Loi Hai commune Ninh Thuan
Thuan Bac
Kien Kien 1
Loi Hai Yes
17 25/10/2017
Mixed group in Ban Pho commune Lao Cai Bac Ha NA Bản Phố
Yes
18 21/10/2017
Local government of Cong Hai commune Ninh Thuan
Thuan Bac
NA Cong Hai
Yes
19 21/10/2017
Local government of Bac Phong commune Ninh Thuan
Thuan Bac
NA Bac Phong
NA
20 25/10/2017
Local government in Na Hoi commune Lao Cai Bac Ha NA Na Hối Yes
21 25/10/2017
Local government in Ban Pho commune Lao Cai Bac Ha NA Ban Pho
NA
22 18/10/2017
Local government of An Phuoc commune Dong Thap
Tan Hong
NA An Phuoc
Yes
23 16/10/2017
Local government of Tan Phuoc commune Dong Thap
Tan Hong
NA Tan Phuoc
NA

135
Appendix 11: List of Participants in Focus Group Discussions
FGD# Province District Commune Village FGD type
S #
Name - Job Age
1 Nin Thuan Thuan Bac
Loi Hai Kien Kien
Mixed 1 Nguyen Thi Anh Đong - Trader Age 47
Mixed 2 Nguyen Trang - Farmer Age 78
Mixed 3 Truong Ich Hong - Farmer Age 69
Mixed 4 Ho Xuan Phuong - Trader Age 50
Mixed 5 Luong Thi Lan - Trader Age 55
Mixed 6 Đinh Thi Phuong - Farmer Age 53
Mixed 7 Nguyen Thanh Trung - Employed Age 21
Mixed 8 Tran Thi Que - Farmer Age 34
2 Nin Thuan Thuan Bac
Loi Hai Kien Kien
Female 9 Trịnh Thị Mỹ Nga - Tailor Age 62
Female 10 Đặng Thị Nhiên - Farmer Age 52
Female 11 Lương Thị Hạnh - Farmer Age 47
Female 12 Nguyễn Thị Hương - Farmer Age 50
Female 13 Võ Thị Ngọc - Farmer Age 53
Female 14 Trương Thị Nhung - Worker Age 34
Female 15 Võ Thị An - Trader Age 59
Female 16 Dương Thị Ngọc Oanh - Farmer Age 49
Female 17 Nguyễn Thị Xuân Mai - Animal husbandry Age 45
Female 18 Trần Thị Tuyết - Trader Age 38
3 Nin Thuan Thuan Bac
Bắc Phong Gò Sạn Male 19 Nguyễn văn Nghĩa - Farmer Age 51
Male 20 Phạm Hoàng Linh - Farmer Age 58
Male 21 Nguyễn Kim Hùng - Farmer Age 60
Male 22 Phạm Văn Dịu - Farmer Age 64
Male 23 Phan Thanh Sự - Farmer Age 70
Male 24 Lê Bá Chi - Farmer Age 64
Male 25 Lê Văn Hấn - Construction worker Age 45
4 Nin Thuan Thuan Bac
Cong Hai fpr Local Govt.
26 Tran Đang Tuan - Commune Social Culture staff Age fpr

136
FGD# Province District Commune Village FGD type
S #
Name - Job Age
Local Govt.
27 Mau Thi Hien - Vice Chairman of Commune People's Committee Age fpr
Local Govt.
28 Nguyen Ky Phuc - Chairman of Farmer’s Union Age fpr
Local Govt.
29 Tran Trung Dung - Vice head of Commune health station Age fpr
Local Govt.
30 Kator Thi Biet - Chairman of the commune women's union Age fpr
Local Govt.
31 Nguyen Thi Nga - Headmaster of My Nhon Primary School Age fpr
5 Nin Thuan Thuan Bac
Bắc Phong fpr Local Govt.
32 Trần Văn Phúc - Official Age 28
Local Govt.
33 Nguyễn Văn Tú - Official Age 36
Local Govt.
34 Tôn Nữ Kim Phương - Official Age 52
Local Govt.
35 Lê Thị Thu - Farmer Age 55
Local Govt.
36 Trần Thị Hằng Nga - Official Age 48
Local Govt.
37 Phạm Thị Giao Thủy - Official Age 45
6 Nin Thuan Thuan Bac
Cong Hai fpr Female 38 Nguyen Thi Lan - Farmer Age 57
Female 39 Nguyen Thi Sau - Worker Age 44
Female 40 Đao Thi Hop - Farmer Age 56
Female 41 Tran Thi Thu Thao - Accountant Age 29
Female 42 Tran Thi Hanh - Employed Age 54
7 Nin Thuan Thuan Bac
Cong Hai fpr Children 43 Cao Nhật Linh - Student Age 9
Children 44 Đá Mài Thụy Phương - Student Age 10
Children 45 Kator Thị Y Ly - Student Age 10
Children 46 Chamalea Thị Khinh - Student Age 10
Children 47 Nguyễn Chí Thiên - Student Age 9
Children 48 Hồ Anh Khoa - Student Age 9
Children 49 Nguyễn Minh Thư - Student Age 10
Children 50 Lý Hoài Uyên Như - Student Age 10
8 Nin Thuan NA Bac Phong fpr Children 51 Vo Thi Thao Nguyen - Student Age fpr
Children 52 Nguyen Ngoc Thuy Tram - Student Age fpr

137
FGD# Province District Commune Village FGD type
S #
Name - Job Age
Children 53 Nguyen Thi Xuan Tien - Student Age fpr
Children 54 Phan Duy Khang - Student Age fpr
Children 55 Phan Thanh Cuong - Student Age fpr
Children 56 Nguyen Duy Dan - Student Age fpr
Children 57 Pham Ngoc Dat - Student Age fpr
Children 58 Pham Thi Thanh Hieu - Student Age fpr
9 Lao Cai Bac Ha Na Hoi fpr Local Govt.
59 Vàng Thị Nhâm - Vice chairman of Commune Women’s Union Age fpr
Bac Ha Local Govt.
60 Sùng Thị Hoa - Chairman of Commune People’s Committee Age fpr
Bac Ha Local Govt.
61 Vàng Thị Lan - Official of Commune health station Age fpr
Bac Ha Local Govt.
62 Vàng Thị Hợi - Chairman of Commune Farmer’s Union Age fpr
Bac Ha Local Govt.
63 Thàn Đặng Quyền - Commune culture official Age fpr
Bac Ha Local Govt.
64 Bùi Văn Muôn - Teacher of Na Hối Secondary school Age fpr
10 Lao Cai Bac Ha Na Hoi fpr Female 65 Tran Thi Thu Ha - Farmer Age 42
Bac Ha Female 66 Hoang Thi Tranh - Farmer Age 26
Bac Ha Female 67 Sung Thi Diem - Farmer Age 51
Bac Ha Female 68 Nong Thi Nga - Freelancer Age 20
Bac Ha Female 69 Tai Thi Hong - Farmer Age 34
Bac Ha Female 70 Tai Thi Nga - Farmer Age 36
Bac Ha Female 71 Vu Thi Thu - Farmer Age 50
Bac Ha Female 72 Luc Thi Minh - Freelancer Age 40
Bac Ha Female 73 Sung Thi Bich - Farmer Age 38
11 Lao Cai Bac Ha Na Hoi fpr Children 74 Hoang Thi Lan Anh - Student Age 11
Bac Ha Children 75 Sung Thi Chau - Student Age 12
Bac Ha Children 76 Ma Seo Thái - Student Age 14
Bac Ha Children 77 Vang Thi Nhung - Student Age 14
Bac Ha Children 78 Vang Van Kiet - Student Age 11

138
FGD# Province District Commune Village FGD type
S #
Name - Job Age
Bac Ha Children 79 Vang Minh Khue - Student Age 11
Bac Ha Children 80 Pham Thuy Linh - Student Age 13
Bac Ha Children 81 Lam Thi Quynh Nhu - Student Age 14
12 Lao Cai Bac Ha Na Hoi fpr Male 82 Then Van Huy - Farmer Age 27
Bac Ha Male 83 Trieu Xuan Hieu - Farmer Age 21
Bac Ha Male 84 Sen Van May - Farmer Age 38
Bac Ha Male 85 Ho A Cho - Farmer Age 27
Bac Ha Male 86 Giang Seo Tong - Farmer Age 45
Bac Ha Male 87 Giang Seo Sai - Farmer Age 28
Bac Ha Male 88 Tai A Vang - Farmer Age 53
Bac Ha Male 89 Vang Seo Phong - Farmer Age 26
Bac Ha Male 90 San Van Dung - Farmer Age 31
13 Lao Cai Bac Ha Ban Pho fpr Mixed 91 Giàng Thị Mai - Farmer Age 29
Bac Ha Mixed 92 Ma Thị Sáu - Farmer Age 30
Bac Ha Mixed 93 Thào Thị Mú - Farmer Age 28
Bac Ha Mixed 94 Vàng Thị Chứ - Farmer Age 31
Bac Ha Mixed 95 Vàng Thị Dung - Farmer Age 23
Bac Ha Mixed 96 Vàng Seo Sẻng - Farmer Age 40
Bac Ha Mixed 97 Lý Seo Chia - Farmer Age 30
Bac Ha Mixed 98 Vàng Thị Dung - Freelancer Age 21
14 Lao Cai Bac Ha Ban Pho fpr Local Govt.
99 Thao Seo Su - Official in charge of household registration Age 27
Bac Ha Local Govt.
100 Ly Seo Sang - Cadastral Officia Age 33
Bac Ha Local Govt.
101 Nguyen Van Son - Head of Health Station Age 41
Bac Ha Local Govt.
102 Sung Thi Pang - Chairman of the Women's Union Age 41
Bac Ha Local Govt.
103 Ly Seo Gia - Chairman of the Farmer’s Union Age 40
Bac Ha Local Govt.
104 Vang Seo Chu - Health staff Age 42

139
FGD# Province District Commune Village FGD type
S #
Name - Job Age
Bac Ha Local Govt.
105 Chu Hoang Yen - Vice President of Ban Pho Secondary School Age 39
Bac Ha Local Govt.
106 Vu Ngoc Hieu - Culture Official Age 45
Bac Ha Local Govt.
107 Giang Seo Chua - Head of Go Dau village Age 35
15 Lao Cai Bac Ha Ban Pho fpr Children 108 Cư Thị Xuân - Student Age fpr
Bac Ha Children 109 Lý Thị Nhung - Student Age fpr
Bac Ha Children 110 Giàng Thị Dỉ - Student Age fpr
Bac Ha Children 111 Vàng Thị Duyên - Student Age fpr
Bac Ha Children 112 Vàng Seo Hiếu - Student Age fpr
Bac Ha Children 113 Lý Thị Diệu Nga - Student Age fpr
Bac Ha Children 114 Cư Quyết Thắng - Student Age fpr
Bac Ha Children 115 Giàng Seo Lua - Student Age fpr
16 Dong Thap Tan Hong
An Phuoc fpr Local Govt.
116 Nguyễn Văn Tước - Head of An Tài village Age fpr
Tan Hong
Local Govt.
117 Trương Thị Diễm Trinh - Vice chairman of Commune People’s Council Age fpr
Tan Hong
Local Govt.
118 Nguyễn Văn Được - Head of An Phát village Age fpr
Tan Hong
Local Govt.
119 Nguyễn Văn Hoàng - Head of commune health station Age fpr
Tan Hong
Local Govt.
120 Nguyễn Hoài Hận - Head of An Thọ village Age fpr
Tan Hong
Local Govt.
121 Võ Thị Hồng Nga - President of commune Women’s Union Age fpr
Tan Hong
Local Govt.
122 Phan Văn Tùng - Vice chairman of commune People’s Committee Age fpr
17 Dong Thap fpr fpr fpr Children 123 Dương Khả Thi - Student Age fpr
fpr Children 124 Nguyễn Thị Tú Anh - Student Age fpr
fpr Children 125 Nguyễn Ngọc Thanh Thanh - Student Age fpr
fpr Children 126 Bùi Thị Diễm Phúc - Student Age fpr
fpr Children 127 Cao Nguyễn Thành Phú - Student Age fpr
fpr Children 128 Nguyễn Nhu Em - Student Age fpr

140
FGD# Province District Commune Village FGD type
S #
Name - Job Age
fpr Children 129 Nguyễn Thị Nu Ngân - Student Age fpr
fpr Children 130 Nguyễn Lê Anh Thư - Student Age fpr
18 Dong Thap Tan Hong
An Phuoc An Tho Male 131 Nguyễn Phước Lộc - Farmer Age 27
Tan Hong
Male 132 Lê Tiền Giang - Farmer Age 49
Tan Hong
Male 133 Phan Văn Tuấn - Farmer Age 41
Tan Hong
Male 134 Trần Hữu Quy - Farmer Age 28
Tan Hong
Male 135 Phan Văn Tâm - Farmer Age 34
Tan Hong
Male 136 Lâm Thành Sang - Farmer Age 60
19 Dong Thap Tan Hong
An Phuoc An Phat Female 137 Phạm Thị Trúc Nhi - Housewife Age 26
Tan Hong
Female 138 Dương Thị Diệu - Farmer Age 43
Tan Hong
Female 139 Trương Thị Liên - Housewife Age 65
Tan Hong
Female 140 Nguyễn Thị Diễm My - Farmer Age 22
Tan Hong
Female 141 Trịnh Thị Tiền - Farmer Age 31
Tan Hong
Female 142 Đặng Thị Tươi - Employee Age 62
Tan Hong
Female 143 Lê Thanh Thúy - Farmer Age 54
Tan Hong
Female 144 Đoàn Thị Sen - Trader Age 69
Tan Hong
Female 145 Trần Thị Ánh Sang - Housewife Age 31
Tan Hong
Female 146 Trần Thị Thanh Tú - Housewife Age 31
20 Dong Thap Tan Hong
Tan Phuoc Viet Hong
Male 147 Hồ Thanh Sơn - fpr Age fpr
Tan Hong
Male 148 Võ Văn Chấm - fpr Age fpr
Tan Hong
Male 149 Huỳnh Văn Buôn - fpr Age fpr
Tan Hong
Male 150 Võ Văn Bụng - fpr Age fpr
Tan Hong
Male 151 Lâm Văn Tâm - fpr Age fpr
Tan Hong
Male 152 Nguyễn Văn Phường - fpr Age fpr
Tan Hong
Male 153 Bùi Văn Hiểu - fpr Age fpr
Tan Hong
Male 154 Ngô Hồng Tuấn - Vice leader of Hoang Viet village Age fpr
21 Dong Thap Tan Hong
Tan Phuoc fpr Local Govt.
155 Ngô Hồng Tuấn - Vice leader of Hoang Viet village Age fpr

141
FGD# Province District Commune Village FGD type
S #
Name - Job Age
Tan Hong
Local Govt.
156 Lê Thị Cẩm Tú - Chairwomen of Tan Phuoc Commune Women’s Union Age fpr
Tan Hong
Local Govt.
157 Đào Bảo Quốc - Chairman of Tan Phuoc Commune Farmers’ Union Age fpr
Tan Hong
Local Govt.
158 Nguyễn Văn Ngự - Head of Communal Health Centre Age fpr
Tan Hong
Local Govt.
159 Nguyễn Thị Thu Hồng - Vice Chairwomen of Tan Phuoc commune People’s Committee Age fpr
Tan Hong
Local Govt.
160 Trần Toàn Miền - Leader of Tan Banh village Age fpr
22 Dong Thap Tan Hong
Tan Phuoc fpr Female 161 Trần Thị Kim Yến - fpr Age fpr
Tan Hong
Female 162 Võ Thị Đèo - fpr Age fpr
Tan Hong
Female 163 Nguyễn Thị Thu Ánh - fpr Age fpr
Tan Hong
Female 164 Lê Thị Hà - fpr Age fpr
Tan Hong
Female 165 Nguyễn Thị Út - fpr Age fpr
Tan Hong
Female 166 Nguyễn Thị Ở - fpr Age fpr
Tan Hong
Female 167 Nguyễn Thị Oanh - fpr Age fpr
Tan Hong
Children 168 Truong Quoc Thinh - Student Age fpr
Tan Hong
Children 169 Nguyen Hoai Phuc - Student Age fpr
Tan Hong
Children 170 Nguyen Nhut Thang - Student Age fpr
Tan Hong
Children 171 Nguyen Nhut Tinh - Student Age fpr
Tan Hong
Children 172 Huynh Thi Nhu - Student Age fpr
Tan Hong
Children 173 Nguyen Thi Tuong - Student Age fpr
Tan Hong
Children 174 Lam Khanh Nguyen - Student Age fpr
Tan Hong
Children 175 Pham Thi Kim Anh - Student Age fpr

142
Appendix 12: List of Documents Reviewed # Filename
Tag: Location
1 2014 UNICEF-Govt Viet Nam MTR Report Final_(Nov2015)_en.docx Ref Docs 2 ADB 2009 IED Urban WASH Evaluation Viet Nam.pdf Ref Docs 3 ADB 2015 VN Urban sanitation issues.pdf Ref Docs 4 DEPOCEN Map AnGiang_province_adminastrative_map Ref Docs 5 DEPOCEN Map DienBien_province_adminastrative_map Ref Docs 6 DEPOCEN Map DongThap_province_adminastrative Ref Docs 7 DEPOCEN Map GiaLai_province_adminastrative_map Ref Docs 8 DEPOCEN Map KonTum_province_adminastrative_map Ref Docs 9 DEPOCEN Map LaoCai_province_adminastrative_map Ref Docs 10 DEPOCEN Map NinhThuan_province_adminastrative_map Ref Docs 11 GoVN 2012 Sustainable Development Report.pdf Ref Docs 12 GoVN MoPI 2016 8th_NSEDP_2016-2020.pdf Ref Docs 13 GoVN OPM 2012 VN GreenGrowth-Strategy.pdf Ref Docs 14 GOVN UN 2011 Socio-Economic Development Plan.pdf Ref Docs 15 GOVN UN 2012-2016 One Plan.pdf Ref Docs 16 JMP 2012 WASH Update.pdf Ref Docs 17 JMP 2015 Viet Nam WASH Estimates.xls Ref Docs 18 JMP 2015 WASH Update and MDG Assessment.pdf Ref Docs 19 MPI 2013 PETS.pdf Ref Docs 20 MPI 2015 Viet Nam Country Report.pdf Ref Docs 21 OECD 2016 Viet Nam Country Profile.pdf Ref Docs 22 UN 2011 VN Draft CCPD 2012-16.pdf Ref Docs 23 UN 2012 Viet Nam Trade System.pdf Ref Docs 24 UN 2012-2016 VN CCPD.pdf Ref Docs 25 UN 2016-2021 VN CCPD.pdf Ref Docs 26 UNICEF 2007 VN Baseline Environmental Sanitation and Hygiene.pdf Ref Docs 27 UNICEF 2009 VN Evaluation Report.pdf Ref Docs 28 UNICEF 2011 MICS VN.pdf Ref Docs 29 UNICEF 2011 WASH-Nutrition Study.PDF Ref Docs 30 UNICEF 2014 MICS VN.pdf Ref Docs 31 UNICEF 2015 VN SitRep Flooding.pdf Ref Docs 32 UNICEF 2016 VN SitRep Humanitarian.pdf Ref Docs 33 UNICEF VN COAR 2012.pdf Ref Docs 34 UNICEF VN COAR 2013.pdf Ref Docs 35 UNICEF VN COAR 2014.pdf Ref Docs 36 UNICEF VN COAR 2015.pdf Ref Docs 37 WB 2017 Viet Nam Overview.docx Ref Docs 38 WB WSP 2014 VN WSS-Turning-Finance-into-Service-for-the-Future.pdf Ref Docs 39 WHO 2015 Vietnnam WSS Overview.docx Ref Docs 40 WSP 2008 Economic Impact of Sanitation in Viet Nam.pdf Ref Docs 41 Patra EtAl 2014 Briefing Paper WEDC_Scaling up sanitation 20140525.pdf Batch-1 42 UNICEF 2012 Survey on sanitation marketing in Viet Nam EN.pdf Batch-1 43 UNICEF 2015 Desk Study Sanitation Demand Study WB-WSP 20150910.doc Batch-1 44 UNICEF 2015 Desk Study Supply Chain 20151008.docx Batch-1 45 UNICEF 2015 Outcome Paper WASH_CSD 20151012 LP.docx Batch-1 46 UNICEF 2015 Study Formative Research and Recos for SupRWSFINAL 20150901.docx Batch-1 47 UNICEF 2015 Study Sanitation Demand Study WB-WSP 20150910.doc Batch-1 48 WB 2015 ProDoc SupRSWS P152693 PAD Board package_WB.pdf Batch-1 49 MARD UNICEF DPO_ENG_FINAL.submitted to MPI.doc Batch-2 50 MoH DPO-Final_E.doc Batch-2 51 MOJ DPO EN Version Submitted to MPI.doc Batch-2 52 UNICEF 2016 Presentation Review of BAT Recommendations.pptx Batch-2 53 UNICEF 2016 Presentation Review of Results 2012-2015.PPTX Batch-2 54 UNICEF DPO An Giang 2012-2016.docx Batch-2 55 UNICEF DPO Child-Sensitive Social Protection 2012-2016 final English.doc Batch-2 56 UNICEF DPO Dien Bien 2012-2016.doc Batch-2

143
57 UNICEF DPO Dong Thap 2012-2016.docx Batch-2 58 UNICEF DPO Edu 2012-2016 Final Eng.doc Batch-2 59 UNICEF DPO Gia Lai 2012-2016.doc Batch-2 60 UNICEF DPO HCMC 2012-2016.docx Batch-2 61 UNICEF DPO Kon Tum 2012-2016.doc Batch-2 62 UNICEF DPO Lao Cai 2012-2016.doc Batch-2 63 UNICEF DPO MOLISA children's department - ENG - 04 08 2012.doc Batch-2 64 UNICEF DPO Ninh Thuan 2012-2016.doc Batch-2 65 UNICEF DPO Parliamentary Governance 2012-2016 final ENG.doc Batch-2 66 UNICEF DPO with MPI-EN-14 Mar.doc Batch-2 67 UNICEF VN CPPA 2012-2016 27 December 2011 .docx Batch-2 68 EAPRO-EquityCaseStudies2016-V2.pdf Batch-3 69 UNICEF_WASH_Financing_Viet_Nam.pdf Batch-3 70 2014 UNICEF-Govt Viet Nam MTR Report Final_(Nov2015)_en.docx Batch-4 71 2016-PL19-Viet Nam-CPD-ODS-EN-8Aug16.pdf Batch-4 72 EAPRO-EquityCaseStudies2016-V2.pdf Batch-4 73 FINAL_UN_VERSION_of_draft_CCPD_for_Viet_Nam_including_results_and_resources_frameworks.pdf Batch-4 74 JAR 2012 RAM final Eng.pdf Batch-4 75 JAR 2013 AM v8final.pdf Batch-4 76 JAR 2014 AM Draft 5.docx Batch-4 77 MTR_CSD Narrative (11 Sep 14)_Revised_LP.docx Batch-4 78 NCAP - Final (EN).doc Batch-4 79 ODF verification & certification review (06 Nov 14).pptx Batch-4 80 ODF verification and certification guideline_Viet Nam_EN_31.05.2016.doc Batch-4 81 Outcome Paper_WASH_CSD (12 Oct 15).docx Batch-4 82 Scaling-up Rural WASH in VN (28 Aug 16).pptx Batch-4 83 Strategy2020(1).pdf Batch-4 84 summary aspects UpdatedRWSSS.doc Batch-4 85 Summary_WASH Outcome paper (18 Oct 15).docx Batch-4 86 UNICEF_WASH_Financing_Viet_Nam.pdf Batch-4 87 UNICEF 2017 Viet Nam VfM Quantitative+Qualitative WASH Assessment.xlsx Batch-5 88 Format 3_RSHP_UNICEF WASH Viet Nam_20170705_EN_An Giang.docx Batch-6 89 Format 3_RSHP_UNICEF WASH Viet Nam_20170705_EN_Dien Bien.xls Batch-6 90 Format 3_RSHP_UNICEF WASH Viet Nam_20170705_EN_Dong Thap.docx Batch-6 91 Format 3_RSHP_UNICEF WASH Viet Nam_20170705_EN_Gialai.docx Batch-6 92 Format 3_RSHP_UNICEF WASH Viet Nam_20170705_EN_Kon Tum.docx Batch-6 93 Format 3_RSHP_UNICEF WASH Viet Nam_20170705_EN_Lao Cai.docx Batch-6 94 Format 3_RSHP_UNICEF WASH Viet Nam_20170705_EN_Ninh Thuan.docx Batch-6 95 2012 - 2013 AG MYWP.pdf Batch-7 96 2012 - 2013 KT WP.pdf Batch-7 97 2012 - 2013 LC WP.pdf Batch-7 98 2012- 2013 DB MYWP.pdf Batch-7 99 2012- 2013 DT MYWP.pdf Batch-7
100 2012- 2013 NT MYWP.pdf Batch-7 101 2012-2013 GL MYWP.pdf Batch-7 102 2012-2013 HCMC WP.pdf Batch-7 103 2012-2013 MARD MYWP.pdf Batch-7 104 2012-2013 MoH MYWP.pdf Batch-7 105 2014 AG AWP English.pdf Batch-7 106 2014 AWP_MARD_WASH.pdf Batch-7 107 2014 AWP_MoH_CSD.pdf Batch-7 108 2014 Dien Bien AWP English.pdf Batch-7 109 2014 DT WP - English.pdf Batch-7 110 2014 GL WP - English.pdf Batch-7 111 2014 HCMC AWP - english.pdf Batch-7 112 2014 Kon Tum AWP - English.pdf Batch-7 113 2014 Lao Cai AWP.pdf Batch-7 114 2014 Ninh Thuan AWP - English.pdf Batch-7 115 2015-16 Dong Thap MYWP_English.pdf Batch-7 116 2015-2016 An Giang MYWP English.pdf Batch-7 117 2015-2016 Dien Bien MYWP English.pdf Batch-7 118 2015-2016 Gia Lai MYWP English.pdf Batch-7

144
119 2015-2016 HCMC MYWP English.pdf Batch-7 120 2015-2016 Kon Tum MYWP English.pdf Batch-7 121 2015-2016 Lao Cai MYWP English.pdf Batch-7 122 2015-2016 MARD MYWP En.pdf Batch-7 123 2015-2016 MoH AWP En.pdf Batch-7 124 2015-2016 Ninh Thuan MYWP English.pdf Batch-7 125 RSHP ODF list with baseline data (evaluation) (Lalit) 20170807 Data
x x x
Document Count
Tag Type Tag Count
Location Ref Docs 40
Location Batch-1 8
Location Batch-2 19
Location Batch-3 2
Location Batch-4 17
Location Batch-5 1
Location Batch-6 7
Location Batch-7 30
Location Data 1
Total (UNICEF) 85
Total 125

145
Appendix 13: Household Survey Results Demographic Section:
Table 1: Frequency and Percentage distribution of households by province, Sex of respondents and head of households
Indicator
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
Respondents
M 45 50 37 44
F 55 50 63 56
Total 100 100 100 100 Head of Households
M 71 90 64 75
F 29 10 36 25
Total 100 100 100 100
* G1 - Name of Province * G7 - Sex of the head of the household * I2 - Respondent’s gender
Table 2: Percentage distribution of respondents by province and Age
Age of respondents
Dong Thap
Lao Cai Ninh Thuan Overall
% % % %
21 years <30 10 16 8 12
31 years <50 33 41 41 38
51 years <65 41 35 35 37
66 years <80 9 6 12 9
81 years <95 2 1 3 2
>95 years 2 1 1 1
Total 100 100 100 100
* G1 - Name of Province
* I1 - Respondent current age
* I2 - Respondent’s gender
Table 3: Distribution of respondents by province and Age
Age of head of households
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
21 years <35 12 9 8 10
36 years <50 33 46 38 39
51 years <65 37 26 36 33
66 years <80 13 15 13 14
81 years <95 3 3 4 3
>95 years 3 0 1 1
Total 100 100 100 100
* G1 - Name of Province
* G7 - Age of a head of the household
* I2 - Respondent’s gender

146
Table 4: Distribution of respondents reporting their relationship to the head of the household by province
Relationship to the head of the household
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
Self - Head of Household 64 50 56 57
Wife/Mother 24 31 26 27
Mother-in-law 0 1 0 0
Grandmother 0 0 0 0
Daughter 3 1 6 3
Daughter in law 0 0 1 0
Sister 4 5 2 3
Niece 0 1 0 0
Husband/Father 3 2 3 3
Father-in-law 0 1 0 0
Grandfather 0 0 0 0
Son 2 8 6 5
Son in law 2 0 0 1
Brother 0 0 1 0
Nephew 0 0 0 0
Cousin 0 0 0 0
Total 100 100 100 100
* G1 - Name of Province
* G9 - What is your relationship to the Head of Household? * I2 - Respondent’s gender
Table 5: Distribution of respondents reporting their highest level of school completed by province
Level of education
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
No formal education 5 18 6 10 Not completing primary school 22 12 7 14
Primary 25 18 37 27
Pre-Secondary 19 30 24 24
Secondary 20 13 16 17
Higher 9 8 9 9
Total 100 100 100 100
* G1 - Name of Province * I5 - What is the highest level of schooling you completed? * I2 - Respondent's gender

147
Table 6: Distribution of respondents by province, income quintiles and level of education
Income quintiles Level of education
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
Highest quintile
No formal education 0 2 1 1 Not completing primary school 5 1 0 2
Primary 6 4 4 4
Pre-Secondary 5 7 7 6
Secondary 6 3 5 5
Higher 7 3 7 6
2nd highest quintile
No formal education 1 2 2 1 Not completing primary school 4 4 5 4
Primary 7 7 12 9
Pre-Secondary 2 9 8 6
Secondary 6 4 7 6
Higher 1 1 1 1
Medium quintile
No formal education 1 11 3 5 Not completing primary school 11 2 2 5
Primary 11 6 15 11
Pre-Secondary 10 7 9 8
Secondary 7 5 4 6
Higher 1 3 1 1
2nd lowest quintile
No formal education 1 1 1 1 Not completing primary school 2 6 0 2
Primary 1 1 2 1
Pre-Secondary 2 4 1 2
Secondary 0 1 0 0
Higher 0 2 0 1
Lowest quintile
No formal education 1 3 1 1 Not completing primary school 1 1 0 1
Primary 2 0 3 2
Pre-Secondary 0 2 0 1
Secondary 2 0 0 1
Higher 0 0 0 0
Total 100 100 100 100
* G1 - Name of Province
* I5 - What is the highest level of schooling you completed?
* I2 - Respondent's gender
* I7 - What is average monthly income from all sources, of your households?
Table 7: Distribution of respondents reporting items owned by province
Items owned by households
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
Radio 3 1 2 2
Television 18 16 17 17
Mobile phone 18 18 17 18
Telephone 1 1 1 1
Refrigerator 14 9 16 13
Motorcycle 18 17 16 17

148
Table 7: Distribution of respondents reporting items owned by province
Items owned by households
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
Bicycle 11 7 9 9
Animal drawn cart 0 1 0 0
Car/truck 1 1 1 1
Boat with motor 1 0 1 1
Own agriculture land 9 14 10 11
Own farm animals 5 16 10 10
Total 100 100 100 100
* G1 - Name of Province
* I6 - Does your household own any of the following items? * I2 - Respondent's gender
Table 8: Distribution of households showing average income by Province
Average monthly income
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
0M -- 10M 11 26 7 15
11M -- 30M 27 16 14 19
31M -- 60M 21 19 29 23
61M -- 100M 17 16 26 20
101M -- 200M 20 18 16 18
> 200 M 4 5 8 5
Total 100 100 100 100
* G1 - Name of Province
* I7 - What is the average monthly income from all sources, of your households?
* G6 - Sex of the head of the household
Table 9: Distribution of respondents by Province and Income quintiles
Income quintiles
Dong Thap Lao Cai Ninh Thuan Overall
% % % %
Highest quintile 28 19 24 24
2nd highest quintile 21 27 35 28
Medium quintile 40 33 34 36
2nd lowest quintile 5 15 3 8
Lowest quintile 5 6 4 5
Total 100 100 100 100
* G1 - Name of Province
* I7 - What is average monthly income from all sources, of your households?
* I2 - Respondent's gender

149
Table 10: Distribution of head of households by Province and Income quintiles
Income quintiles
Dong Thap Lao Cai Ninh Thuan Overall
% % % %
Highest quintile 24 23 23 23
2nd highest quintile 21 21 31 25
Medium quintile 43 30 38 37
2nd lowest quintile 4 14 3 7
Lowest quintile 7 12 4 8
Total 100 100 100 100
* G1 - Name of province
*G6 - Sex of the head of the household
*I7 - What is your average monthly income from all sources, of your households?
Water Sources:
Table 11: Percent distribution of respondents reporting available water sources for drinking and cooking by province
Nature of Water sources
Drinking Water Sources
Dong Thap Lao Cai Ninh Thuan Overall
% % % %
Unimproved water sources
Bottled water 35 0 5 13
Other 1 3 1 1
Surface water (river / dam / lake / pond / stream / canal) 8 1 0 3
Unprotected spring 0 3 0 1
Total 44 8 6 19
Improved water sources
Piped into dwelling, plot or yard 45 5 87 46
Protected Spring 0 82 0 27
Protected dug well 1 2 1 1 Public tap/stand pipe 0 1 0 0 Rain water collection 2 0 6 3
Tube well/borehole 8 3 0 4
Total 56 92 94 81
Overall 50 50 50 100
*G1 - Name of the Province?
*W1 - What is your current primary source of water for drinking and cooking?
*I2 - Respondent sex

150
Table 12: Percent distribution of respondents reporting access to this drinking water source by province
Drinking water
sources
Dong Thap Lao Cai Ninh Thuan Overall
% % % %
Yes 95 79 92 88
No 5 21 8 12
Total 100 100 100 100
*G1 - Name of the Province?
*W1A - Do you always have access to this drinking water source year-round?
*I2 - Respondent sex
Table 13: Percent distribution of respondents reporting access to clean drinking water source by province
Drinking water source
- clean
Dong Thap Lao Cai Ninh Thuan Overall
% % % %
Yes 70 81 87 79
No 16 17 9 14
Don't know 15 2 4 7
Total 100 100 100 100
*G1 - Name of the Province? *W1B -Is the drinking water from your main source clean? *I2 - Respondent sex
Table 14: Percent distribution of respondents reporting access to safe drinking water source by province
Drinking water source - safe
Dong Thap Lao Cai Ninh Thuan Overall
% % % %
Yes 67 76 76 73
No 13 21 10 15
Don't know 20 3 14 12
Total 100 100 100 100
*G1 - Name of the Province? *W1C - Is the drinking water from your main source safe? *I2 - Respondent sex
Table 15: Percent distribution of respondents reporting drinking water from source is of acceptable quality by province
Quality of drinking water from source
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
Taste 31 34 34 33
Odour/smell 37 33 32 34
Appearance 32 33 34 33
Total 100 100 100 100
*G1 - Name of the Province? *W1B1 - Is the drinking water from your main source of acceptable quality in terms of? (Record separately for each option) *I2 - Respondent sex

151
Table 16: Percent distribution of respondents reporting available water sources for bathing, cleaning and toilet by province
Nature of water
sources Water sources for toilet use
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
Unimproved water
sources
Bottled water 0 0 0 0
Other 0 23 0 8
Surface water (river / dam / lake / pond / stream / canal) 93 20 0 38
Unprotected spring 0 58 0 19
Unprotected dug well 7 0 50 19
Total 100 100 50 83
Improved water
sources
Piped into dwelling, plot or yard 60 4 93 52
Protected Spring 0 89 0 30
Protected dug well 1 3 6 3
Public tap/stand pipe 0 1 1 0
Tube well/borehole 40 3 1 14
Total 100 100 100 100
Overall 100 100 75 100
*G1 - Name of the Province? *W2 - What is your current main source of water for bathing, toilet flushing, cleaning etc.? *I2 - Respondent sex
Table 17: Percent distribution of respondents reporting access to this water source for household needs by province
Household access to water
source
Dong Thap Lao Cai Ninh Thuan Overall
% % % % Yes 100 78 98 92 No 0 22 2 8 Total 100 100 100 100 *G1 - Name of the Province? *W3 - Do you always have access to this water source for household needs (bathing, toilet flushing, cleaning etc.) year-round? *I2 - Respondent sex
Table 18: Percent distribution of respondents reporting no access to water source for household needs by province
No access to water source for household needs
Dong Thap Lao Cai Ninh Thuan Overall
% % % %
During dry season (Y) 0 42 0 14
During rainy season (Y) 0 58 100 53
Total 0 100 100 67
*G1 - Name of the Province? *W3A - If NO, when do you NOT have access to this water source? *I2 - Respondent sex

152
Table 19: Percent distribution of respondents reporting other main sources by province
Nature of water
sources
Drinking water sources
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
Improved water
sources
Public tap/stand pipe 0 23 0 17
Tube well/borehole 0 0 50 3
Protected dug well 0 0 50 3
Protected Spring 0 26 0 20
Rain water collection 0 4 50 6
Total 0 23 100 49
Unimproved water
sources
Unprotected spring 0 12 0 9
Others 0 65 0 43
Total 0 77 0 51
Overall 0 50 50 100
*G1 - Name of the Province? *W3B - What this source is not available, what other main sources do you usually use? *I2 - Respondent sex
Sanitation: Table 20: Percent distribution of respondents reporting latrine existence by province
Latrine Existence
Dong Thap Lao Cai Ninh Thuan Overall
% % % %
Yes 96 97 98 97
No 4 3 2 3
Total 100 100 100 100
*G1 - Name of province *I2 - Respondent sex *S1 - Does your house currently have a toilet?
Table 21: Percent distribution of respondents reporting sharing of latrine by province
Share toilet facility with others
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
No 96 100 99 98
Yes 4 0 1 2
Total 100 100 100 100
*G1 - Name of province
*I2 - Respondent sex *S2 - Does you share this facility with other families outside of your home?

153
Table 22: Percent distribution of respondents reporting type of toilet household have by province and gender
Nature of Toilet
Types of toilet
G1. Name of Province
Total
Overall Dong Thap Lao Cai Ninh Thuan
M F Total M F Total M F T M F
N % N % N % N % N % N % N % N % N % N % N % N %
Unimproved Toilet
VIP latrine 0 0 0 0 0 0 3 11 0 0 3 6 2 4 4 4 6 4 5 5 4 1 9 3
Pit latrine without slab
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Hanging latrine 0 0 4 5 4 3 0 0 0 0 0 0 0 0 0 0 0 0 0 0 4 2 4 1
Composting latrine
37 60 32 41 69 50 2 7 3 13 5 10 25 49 37 41 62 45 64 39 72 32 136 41
Total 37 60 36 46 73 53 5 19 3 13 8 16 27 53 41 46 68 49 69 44 80 35 149 45
Improved Toilet
Flushed to piped sewer system
4 6 6 8 10 7 1 4 1 4 2 4 1 2 0 0 1 1 6 4 7 4 13 4
Flushed to septic tank
2 3 4 5 0 4 13 48 12 50 0 49 19 37 41 46 60 41 34 30 57 34 91 27
Flushed to pit latrine
16 26 29 37 45 31 6 22 8 33 14 28 4 8 8 9 12 8 26 19 45 26 71 21
Flush, don’t know where
3 5 2 3 5 4 1 4 0 0 1 2 0 0 0 0 0 0 4 3 2 1 6 2
Pit latrine with slab
0 0 1 1 1 1 1 4 0 0 1 2 0 0 0 0 0 0 1 1 1 0 2 1
Total 25 40 42 54 60 46 22 81 21 88 17 83 24 47 49 54 73 51 70 55 111 65 183 55
Overall 62 100 78 100 133 50 27 100 24 100 25 49 51 100 90 100 141 50 139 49 191 50 332 100
*G1 - Name of the Province?
*ES1 - What type of toilet does your household have?
*I2 - Respondent sex

154
Table 23: Percent distribution of respondents reporting improved/upgraded latrine in last 3 years by province
Improved/upgraded latrine in last 3 years
Dong Thap Lao Cai Ninh Thuan Overall
% % % %
Yes 16 22 14 17
No 83 78 86 82
Don't know 1 0 0 0
Total 100 100 100 100
*G1 - Name of province *I2 - Respondent sex *ES3 - Have you improved/upgraded this latrine in last THREE years? If yes, when did that happen?
Table 24: Percent distribution of respondents reporting the quality of this latrine construction by province
Reasons for improvement/upgrading
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
Construction is poor 35 17 25 26
Toilet location is inconvenient to use 4 23 18 15
Water is not available close to the toilet 0 2 0 1 Toilet is dirty/dark/smelly 4 6 7 6 Others 58 51 50 53
Total 100 100 100 100
*G1 - Name of province *I2 - Respondent sex ES4: What is your major reason for improvement/upgrading?

155
Table 25: Percent distribution of respondents reporting the quality of this latrine construction by province
Defecation outside of home
Dong Thap Lao Cai Ninh Thuan Overall
% % % % Excellent 19 8 7 11 Good 59 46 71 59 Fair 20 37 19 25 Poor 2 8 3 4 Very Poor 0 0 1 0 Don’t know 0 1 0 0 Total 100 100 100 100
*G1 - Name of Province *ES4.1 - What do you think about quality of this latrine construction? *I2 – Respondent sex
Table 26: Percent distribution of respondents reporting reasons of using a toilet facility by province
Reasons for using toilet facility
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
For good health/disease prevention 16 18 15 16
Cleaner and healthier living in our home 27 42 26 32
Convenience 27 13 20 20
To have privacy when use the facility 5 5 8 6
To be modern 2 3 3 2
To be accepted well by others 0 0 0 0
To avoid sharing with others 3 2 1 2
To avoid disturbing others 2 1 6 3
To avoid embarrassment/humiliation 0 1 5 2
It’s what everybody is doing 3 2 7 4
We were told it was the right thing to have 2 2 7 3
Others 13 11 3 9
Total 100 100 100 100
*G1 - Name of province *I2 - Respondent sex *S3 - Why does your family use a toilet facility?
Table 27: Percent distribution of respondents reporting of immediate family members using toilet to defecate when at home by province
Defecation outside of home
Dong Thap Lao Cai Ninh Thuan Overall
% % % %
Always 20 33 20 24
Never/Rarely 1 2 1 1
Sometimes/Occasionally 3 3 3 3
Usually Mostly 20 13 21 18
Don’t know 1 0 1 1
Not applicable 56 50 54 53
Total 100 100 100 100
*G1 - Name of Province *S5 - How often do members of your immediate family use this toilet to defecate when at home? *I2 - Respondent's gender

156
Table 28: Percent distribution of respondents reporting awareness of available options for the assistance received to help build a latrine by province
Awareness and assistance
received to help build a latrine
Dong Thap Lao Cai Ninh Thuan Overall
% % % % Yes 63 63 71 66 No 27 35 23 28 Don't know 10 2 6 6 Total 100 100 100 100
*G1 - Name of province *I2 - Respondent sex *ES5 - Are you aware of any available options to receive any assistance (loan, financing, gifts/grants, Construction Material/in- kind support etc.) to help you build the latrine?
Table 29: Percent distribution of respondents reporting of any assistance received to help build a latrine by province
Assistance received to build
a latrine
Dong Thap Lao Cai Ninh Thuan Overall
% % % % Yes 51 51 69 57
No 49 49 31 43 Don't know 0 0 1 0
Total 100 100 100 100
*G1 - Name of province *I2 - Respondent sex *ES6 - Did you receive any assistance (loan, financing, gifts/grants, Construction Material/in- kind support etc.) to help you build the latrine?
Table 30: Percent distribution of respondents reporting type of assistance received by province
Type of Assistance Received
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
Loan 91 11 93 65 Grant/Gift/Subsidy 7 78 7 31 Construction Material/in-kind support 2 11 0 4
Total 100 100 100 100
*G1 - Name of province *I2 - Respondent sex *ES6.1 - What type of Assistance you received?
Table 31: Percent distribution of respondents reporting family made decision to help build a latrine by province
Family made decision to help build a latrine
Dong Thap Lao Cai Ninh Thuan Overall
% % % % Father/Male head of family 39 39 45 41 Mother/Female head of family 55 55 48 53 Don’t know 6 7 7 6 Total 100 100 100 100
*G1 - Name of province *I2 - Respondent sex *S7 - Who in your family made the decision to have a latrine built for your household?

157
Table 32: Percent distribution of respondents reporting no toilet facility and place for defecation outside of their home by province
Defecation outside of home
Dong Thap Lao Cai Ninh Thuan Overall
% % % %
Bush/field 0 42 42 28
Pig Pen 0 25 0 8
Fish pond 33 0 0 11
River 0 0 25 8
Beach 0 0 0 0
Behind our house 0 0 17 6
Neighborhood toilet 67 33 0 33
Communal latrine 0 0 0 0
Others 0 0 17 6
Total 100 100 100 100
*G1 - Name of Province *S8 - You said you had no toilet facility in your house, where do you and members of your family defecate most of the time? *I2 - Respondent's gender
Table 33: Percent distribution of respondents reporting awareness of any available options for the assistance received to help build a latrine by province
Aware of any available options to receive any
assistance to help you build a latrine
Dong Thap Lao Cai
Ninh Thuan Overall
% % % % Yes 50 0 50 33 No 33 83 50 56 Don't know 17 17 0 11 Total 100 100 100 100
*G1 - Name of province *I2 - Respondent sex *S11 - Are you aware of any available options to receive any assistance (loan, financing, gifts/grants, Construction Material/in- kind support etc.) to help you build the latrine?
Table 34: Percent distribution of respondents reporting family members frequently clean the latrine by province
Family members frequently clean the latrine
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
Men 0 13 7 7
Women 0 70 88 53
Boys 0 1 0 0
Other 0 16 5 7
Total 0 100 100 67
*G1 - Name of province *I2 - Respondent sex *TM1 - Who in the family members, frequently cleans the latrine?

158
Diarrhea: Table 35: Percent distribution of respondents reporting awareness on ways to protect children against diarrhea by province
Ways to protect children against diarrhea
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
Boil or treat your water 28 25 24 26
Use latrines/dispose faeces of children in latrines 5 4 9 6
Wash hands with soap and water 21 18 19 19
Cook food well 24 28 19 24
Store food properly/cover well 4 6 12 7
Buy from a clean place/not buying food from random place 2 3 5 4 Wash fruits/vegetables with potable water 4 1 9 5
There is not nothing you can do 0 0 0 0
Others 10 14 3 9
Total 100 100 100 100
*G1 - Name of Province *D1 - You may/may not have children 0-5, that’s fine. But you may know ways to protect young children against diarrhea. Please tell me all of the ways you know to protect young children (age 0-5) against diarrhea in? *I2 - Respondent's gender
Table 36: Percent distribution of respondents reporting their children had diarrhea under the age of 5 by province
Respondents reporting children
had diarrhea under the age of 5
Dong Thap Lao Cai Ninh Thuan Overall
% % % %
Yes 0 10 4 5
No 96 90 96 94
Don't know 4 0 0 1
Total 100 100 100 100
*G1 - Name of Province *I2 - Respondent's gender *D2 - In the past two weeks has your child/children under the age of five had diarrhea (defined as three or more watery stools in a 24 period/same day or blood in the stool)?
Community Participation:
Table 37: Percent distribution of respondents reporting purchase of sanitary materials for construction of latrine by province
Purchase of sanitary materials for construction of latrine
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % % Within or nearby your village/community 46 6 48 33 At commune level 27 5 35 22 At district level 27 86 16 43 Don’t know 0 3 1 2 Total 100 100 100 100
*G1 - Name of Province *I2 - Respondent's gender CP5 - Where can sanitary materials and supplies for constructing toilet be purchased?

159
Table 38: Percent distribution of respondents reporting quality of sanitary supplies and construction material by province Quality of sanitary
supplies and construction
material
Dong Thap Lao Cai Ninh Thuan Overall
% % % %
Don’t Know 6 8 4 6
Excellent 8 6 10 8
Fair 32 34 23 30
Good 54 52 62 56
Poor 1 0 0 0
Very poor 0 0 1 0
Total 100 100 100 100
*G1 - Name of Province *I2 - Respondent's gender CP6 - How do you rate the quality of the sanitary supplies (pipe, commode, etc.) and other construction materials required to build/maintain latrine?
Hand Washing
Table 39: Percent distribution of respondents reporting washing of their hands by province
Washing of hands
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
When they are visibly dirty 16 10 20 15 When they smell or are sticky 2 1 8 4 Before cooking 9 9 12 10 Before eating 24 27 18 23 Before feeding a baby/child 2 2 5 3 After defecation 20 22 19 20 After cleaning a baby after that has defecated 1 1 4 2 After work 14 20 13 16 Others 12 7 2 7 Total 100 100 100 100
*G1 - Name of Province *HW1 - When do you wash your hands? *I2 - Respondent's gender
Table 40: Percent distribution of respondents reporting what they use for washing hands by province
Usually items use to wash their hands
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % % Soap 84 69 83 79 Powdered or liquid detergent 13 25 17 18
Ash 0 1 0 0 Dirt/mud/sand 0 1 0 0 Others 3 4 0 2 Total 100 100 100 100
*G1 - Name of Province *HW2 - What do you usually use to wash your hands? *I2 - Respondent's gender

160
Table 41: Percent distribution of respondents reporting reasons for washing of hands by province
Reasons for washing hands
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
To prevent the spread of disease 33 33 27 31
To be clean 45 52 37 45
To smell good 4 4 12 7
To get rid of dirt/smell/sticky/ things on my hands 14 7 11 10
Religious reasons/beliefs 0 0 0 0
Was told it was the right thing to do 1 2 5 3
Because that is what everyone does 0 1 7 3 Others 3 1 2 2
Total 100 100 100 100
*G1 - Name of Province *HW4 - Can you share why you wash your hands (what motivates you to wash your hands)? *I2 - Respondent's gender
Communication Channels:
Table 42: Percent distribution of respondents reporting of participation in meeting about sanitation by province
Respondent participation in meeting about
sanitation
Dong Thap Lao Cai Ninh Thuan Overall
% % % % Yes 70 66 54 63 No 27 29 40 32
Don't know 3 5 6 5 Total 100 100 100 100
*G1 - Name of Province *CC1 - Has anyone in your family participated in a meeting about sanitation and or has any government staff (e.g. sanitation) visited your home (in last five years) to talk about build a latrine? *I2 - Respondent's gender
Table 43: Percent distribution of respondents reporting of receiving sufficient/useful information to help construct a latrine by province
Received sufficient/useful
information to help to construct a latrine
Dong Thap Lao Cai Ninh Thuan Overall
% % % % Yes 82 48 90 73 No 11 47 8 22 Don't know 7 5 3 5 Total 100 100 100 100
*G1 - Name of Province *CC1a - Did you receive sufficient/useful information (awareness messages, supplies, mason etc.) to help to construct a latrine at your home? *I2 - Respondent's gender

161
Table 44: Percent distribution of respondents recalling three key messages by province
Respondents recalling three key messages
Dong Thap Lao Cai Ninh Thuan Overall
% % % %
Yes 50 31 39 40
No 35 50 46 44
Don't know 15 19 14 16
Total 100 100 100 100
*G1 - Name of Province *CC2b - Can you recall THREE key messages, which you have learned and/or learned and practice due to your participation in that meeting/activity? *I2 - Respondent's gender
Table 45: Percent distribution of respondents the source of information about hygiene and toilet by province
Source of information about hygiene and toilet
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % % Television/Radio 15 22 25 21 Commune/Village meetings 13 22 13 16 Family members/relatives 1 3 19 7 Government health workers 6 7 6 7 Local Public-Address System 2 3 9 5 Local authority (head of village) 30 34 22 29 Mass organization; Women's union, Farmer's union, youth union) 12 0 3 5 Neighbors/friends 7 7 4 6 Newspaper/Tabloid, magazine 4 0 1 2 Others 2 7 4 5 Print Materials (posters, leaflets) 0 0 2 1
Sanitary Mart/shop, local mason 0 1 1 0 Don't know 9 16 13 13
Total 100 100 100 100
*G1 - Name of Province *CC3 - What are the sources of information through which you get information about hygiene and toilet? *I2 - Respondent's gender
Table 46: Percent distribution of respondents the trusted/preferred source of information about hygiene and toilet by province
Trusted/preferred sources of information
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
Television/Radio 27 18 37 28
Commune/Village meetings 10 21 11 14
Family members/relatives 1 3 19 8
Government health workers 7 11 5 8
Local Public-Address System 5 0 7 4
Local authority (head of village) 26 32 29 29 Mass organization; Women's union, Farmer's union, youth union) 10 0 3 4
Neighbors/friends 1 6 5 4
Newspaper/Tabloid, magazine 2 1 1 1
Others 2 4 5 4
Print Materials (posters, leaflets) 0 1 2 1
Sanitary Mart/shop, local mason 0 1 1 0
Don't know 8 21 12 14
Total 100 100 100 100

162
*G1 - Name of Province *CC4 - Which sources of information you trust/prefer the most than others? *I2 - Respondent's gender
Natural Disaster: Table 47: Percent distribution of respondents reporting natural disaster in last 2 years by province
Natural Disaster experienced
Dong Thap Lao Cai
Ninh Thuan Overall
% % % %
Yes 15 14 23 17
No 78 85 77 80
Don’t know 7 1 1 3
Total 100 100 100 100
*G1 - Name of the Province? *ND1 - Did your village/family experience any natural disaster/s during last two years, which may have caused destruction (including water sources) and human/economic losses? *I2 - Respondent sex
Table 48: Percent distribution of respondents reporting natural disaster in last 2 years by province
Type of Natural Disaster experienced
in the last 2 years
Dong Thap Lao Cai Ninh Thuan Overall
% % % %
Flood 29 40 60 43
Drought 48 31 38 39
Earthquake 0 2 0 1
Others 23 26 2 17
Total 100 100 100 100
*G1 - Name of the Province? *ND1 - Did your village/family experience any natural disaster/s during last two years, which may have caused destruction (including water sources) and human/economic losses? *I2 - Respondent sex
Observation Hand Washing: Table 49: Percent distribution of respondents reporting washing of hands by family members by province
Family members wash hands
Dong Thap Lao Cai Ninh Thuan Overall
% % % % Within 10 paces of the kitchen/cooking place 22 40 36 33
Within 10 paces of the toilet facility 72 19 40 44
Elsewhere in home or yard 1 3 8 4
Outside of yard 5 23 13 14
No specific place 0 0 1 0
No permission to see 0 0 2 1
Others 0 15 1 5
Total 100 100 100 100
*G1 - Name of the Province? *OHW1 - Can you show me where members of your family most often wash their hands? *I2 - Respondent sex

163
Table 50: Percent distribution of respondents reporting presence of water for handwashing by province
Water presence for handwashing
Dong Thap Lao Cai Ninh Thuan Overall
% % % %
Water is available 99 96 98 98
Water is not available 1 4 2 2
Total 100 100 100 100
*G1 - Name of the Province?
*OHW2 - Is water present at the specified place for hand washing? *I2 - Respondent sex
Table 51: Percent distribution of respondents reporting of soap or detergent for handwashing by province
Soap/detergent for hand washing
Dong Thap Lao Cai Nin Thuan Overall
% % % %
Bar Soap 39 44 36 40
Detergent (Powder/liquid/paste) 27 31 36 31
Liquid Soap (including shampoo) 21 6 12 13
None available 13 19 14 15
Others 1 1 2 1
Total 100 100 100 100
*G1 - Name of the Province? *OHW3 - Is soap or detergent present at the specific place for hand washing? *I2 - Respondent sex
Table 52: Percent distribution of respondents reporting washing of hands by family members by province
Family Members wash hands
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
Water only 13 18 17 16
Soap and water 47 45 52 48
Powdered or liquid detergent and water 6 9 4 6
Ash 0 0 0 0
Dirt/sand/mud 1 0 0 0
Used visibly clean cloth to dry 20 20 17 19
Used visibly dirty cloth to dry 3 2 2 2 Cannot demonstrate (lacks resources to demonstrate) 0 2 0 1 Unwilling/refused to demonstrate 4 2 2 2
Others 6 2 7 5
Total 100 100 100 100
*G1 - Name of the Province? *OHW4 - Can you now show me how you usually wash your hands? *I2 - Respondent sex

164
Observation Sanitation Table 53: Percent distribution of respondents reporting toilet facility used by family members located by province
Toilet facility used by family members located
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % % In own courtyard 7 63 26 32
In own dwelling/attached to own dwelling 86 23 73 61 Refused/Not able to observe 1 1 1 1 Others 6 13 0 6 Total 100 100 100 100
*G1 - Name of the Province? *OS1 - Where is the toilet facility used by members of your family located? Can you show me where it is now? *I2 - Respondent sex
Table 54: Percent distribution of respondents reporting type of toilet household have by province
Nature of Toilet facility
Types of Toilet
Dong Thap
Lao Cai
Ninh Thuan Overall
% % % %
Improved Toilet
Flushed to piped sewer system 8 3 0 3
Flushed to septic tank 7 46 40 31
Flushed to pit latrine 31 24 9 18
Flush, don’t know where 23 2 0 6
Total 68 75 49 58
Unimproved toilet
VIP latrine 0 2 5 2
Pit latrine with slab 0 3 0 1
Pit latrine without slab 0 1 0 0
Hanging latrine 4 0 0 1
Insanitary latrine 1 0 0 0
Composting toilet 69 18 45 37
Don’t know 1 1 0 0
Others 1 0 1 0
Total 32 25 5 42
Overall 50 50 27 100
*G1 - Name of the Province? *ES1 - What type of toilet does your household have? *I2 - Respondent sex

165
Table 55: Percent distribution of respondents reporting water adequacy for flushing needs by province
Water adequacy for flushing needs
Dong Thap Lao Cai Ninh Thuan
Overall
% % % %
Yes 97 91 99 96
No 0 6 0 2
Don't know 3 3 1 2
Total 100 100 100 100
*G1 - Name of province *I2 - Respondent sex *OS2A – Is the water you have access to adequate to meet your toilet flushing needs?
Table 56: Percent distribution of respondents by province
OS3
Dong Thap Lao Cai
Ninh Thuan Overall
% % % %
Yes 92 97 83 91 No 7 2 16 8
Refused/unable to observe 1 1 1 1 Total 100 100 100 100
*G1 - Name of province *I2 - Respondent sex *OS3 - IF ONE OR MORE SIGNS BELOW ARE SELECTED, THEN THE ANSWER WILL BE “YES”

166
Appendix 14: Evaluation Team
Evaluation Team Position Name Role Description
Team Lead / Evaluation and Social Norm Expert
Nadeem Haider To manage the evaluation, with key tasks including literature review, design of evaluation methodology, inception report writing, data collection, data analysis (particularly relating to social norms), reporting, quality assurance, and external communication.
Deputy Team Lead / Social Norm Expert
Asmat Ali Gill To lead in development of the evaluation framework, design, methodology (in particular social norm/sustainability assessment), tools development, undertaking selected KIIs/FGDs, data consolidation, analysis, and report writing. Additionally, responsible to coordinate with the Client, international team members, national Evaluators and local partners to ensure smooth execution of all processes.
Principal Consultant Hussain Tawawalla
To support the Team Lead in evaluation design, literature review, report writing, data analysis, management and any other delegated responsibilities. To contribute expertise in conducting evaluations.
International WASH Expert
Simone Klawitter To contribute to evaluation design and literature review during the inception phase.
Statistical Analyst (Social Norm Expert)
Aemal Khan To support the team lead in the design and planning of data collection activities, to organise and process data and to analyse collected data.
Research Officer Saad Ibrahim Rasheed
To support the evaluation by carrying out literature review, report writing, communication, data collection/processing/analysis, fieldwork and any other delegated tasks.
Research Support Team
Faisal Shahzad and Nouma Hanif
To support the evaluation by carrying out literature review, report writing, communication, data collection/processing/analysis, fieldwork and any other delegated tasks.
National Partner DEPOCEN To facilitate the team in preparing for and conducting fieldwork by providing assistance with logistics, translations, interpretation, coordination with stakeholders, follow-up, monitoring and training (of master trainers for field staff training).

167
Appendix 15: Evaluation Norms and Compliance
Norm / Standard
Relevant Standard
Description of Standards Compliance Management
Culturally sensitive data collection
Not applicable
Ensuring that all aspects of data collection - tools, training of enumerators etc. reflect an understanding of the local cultural context.
Field data collection was facilitated by a local partner i.e. Depocen. Depocen is a known field and policy research entity of Viet Nam, with considerable national research experience. The local partner not only contributed to design of the evaluation to make it culturally sensitive and ensured that this get applied during data collection.
Report Writing
UNICEF-Adapted UNEG Evaluation Reports Standards
The standards require the Inception and Final Reports are produced as per UNICEF requirements.
The Consultants bring extensive experience of applying UNICEF adapted reporting standards and have produced high quality evaluations through last five years. The reports produced were reviewed against the guidelines and adapted where required.
Evaluation Utility
UNEG Norms and Standards of Evaluation 2016
In commissioning and conducting an evaluation, there should be a clear intention to use the resulting analysis, conclusions or recommendations to inform decisions and actions.
Evaluation could also be used to contribute beyond the organization by generating knowledge and empowering stakeholders."
The report has been drafted in a way to enable UNICEF and other primary users to use data, analysis, and recommendations to demonstrate accountability and use learning to inform future use.
Evaluation Credibility
UNEG Norms and Standards of Evaluation 2016
"Evaluations must be credible. Credibility is grounded on independence, impartiality and a rigorous methodology. Key elements of credibility include transparent evaluation processes, inclusive approaches involving relevant stakeholders and robust quality assurance Norms and Standards for Evaluation systems. Evaluation results (or findings) and recommendations are derived
Series of steps undertaken to ensure compliance to principle of credibility. Some of those include, reference check for field data collectors (for not having been involved in project in any role); check for field partners for not having been involved in the projects; instituting processes for data validation; and setting guidelines for field data collection. Where there were issues, these were

168
Norm / Standard
Relevant Standard
Description of Standards Compliance Management
from - or informed by - the conscientious, explicit and judicious use of best available, objective, reliable and valid data and by accurate quantitative and qualitative analysis of evidence. credibility requires that evaluations are ethically conducted and managed by Evaluators that exhibit professional and cultural competencies."
communicated clearly to the appropriate authority.
Confidentiality
UNICEF Procedure for Ethical Standards in Research, Evaluation, Data Collection and Analysis 2015.
"Confidentiality is the presence of protecting an individual's privacy. It pertains to the treatment of information that an individual has disclosed in a relation of trust, with the expectation that this information will not be divulged to others without permission."
The evaluation applied the principle of confidentiality starting from informed consent and ensuring complete confidentiality of the respondents post field work i.e. data cleaning, analysis and reporting. Personal information has been kept physically separate as much as possible and consolidated data is handled by as few people as necessary to reduce potential points of failure.
Transparency
UNEG Norms and Standards of Evaluation 2016
“Transparency is an essential element of evaluation that establishes trust and builds confidence, enhances stakeholder ownership and increases public accountability. Evaluation products should be publicly accessible.”
The evaluation has been guided by ERG and the forum has been kept involved through all stages of the evaluation. The report is likely to be made public (as per UNICEF commitment) which shall enable public access to the evaluation output.
Human Rights and Gender Equality
UNEG Norms and Standards of Evaluation 2016
“The universally recognized values and principles of human rights and gender equality need to be integrated into all stages of an evaluation. It is the responsibility of Evaluators and evaluation managers to ensure that these values are respected, addressed and promoted, underpinning the commitment to the principle of ‘no-one left behind’.”
This has been dealt with in the evolution design, processes and output. The evaluation matrix carries specific questions, which guided the tools design to capture relevant information around equity, gender and human rights. Specific questions related to cross-cutting programming priorities (gender, equity, HRBA) were asked from vulnerable groups particularly women, girls and older people to explore their awareness knowledge about basic rights of water, sanitation and others. The

169
Norm / Standard
Relevant Standard
Description of Standards Compliance Management
senior Evaluators being aware of the principals, trained and guided the field teams. The field teams included both male and female researchers. And a separate section is added to the report that highlights the key findings and results around these aspects.

170
Appendix 16: Glimpse of Evaluation Data Collection
DEPOCEN (Local Partner) Team Conducting Focus Group Discussion with Children’s
Focus Group Discussion with Children’s
Focus Group Discussion with Commune Committee

171
Key Informant Interview with Government Official
Key Informant Interview with CLTS Master Trainer
Key Informant Interview with CHE Specialist

172
Key Informant Interview with Representative of Women Association
Focus Group Discussion Community Members
Focus Group Discussion with Children’s

173
Appendix 17: Results framework and activity-wise project description of seven provinces The RSHP Programme documents does not specify any consolidated document to be treated as the results framework. However, the evaluators have extracted and consolidated all relevant information from the ‘Detailed Projects Outline (DPOs)’ and available ‘workplans’ of the Provicial Projects to prepare the resultas framework for RSHP, presented in below matrix. MINISTRY OF HEALTH – UNICEF COUNTRY PROGRAMME OF COOPERATION. CHILD SURVIVAL AND DEVELOPMENT PROGRAMME; DETAILED PROJECT OUTLINE; 2012 - 2016 Hygienic sanitation. Planned budget: 500,000 USD. 1. Main expected results By 2013, sanitation and hygiene policy frameworks on CLTS, sanitation marketing and HWWS are
disseminated and fully operational for implementation targeting specifically vulnerable and ethnic minority children and their caregivers living in rural setting.
By 2013, behaviour change strategies and action plan on hand washing, CLTS, social marketing and partnership approaches are disseminated and fully operational enabling participation of communities in planning, implementing and monitoring sanitation services in rural setting.
By 2016, 65% of rural households have access to hygienic latrines meeting MOH standards. By 2016, 40% of rural population washes hands with soap after defecation, after handling children’s faeces,
related to food handling and before eating. 2. Activities at national level: Support for better coordination between interested donors and related government agencies for more effective
supports for sanitation. Develop WASH related policy options and guidelines to benefit the un-reached and ethnic minority children. Conduct research and studies of differences of impacts of poor WASH and good WASH on children. Support for continuation of improving implementation of WASH Sector assessment and using its data for
decision making. Support in design and implement the National Communication Action Plan under the RWSS NTP III via
introduction of C4D initiatives to promote social mobilization, behaviour and social change in hygiene and sanitation.
Support capacity development for better planning, implementing and managing WASH C4D strategies focusing on sanitation including CLTS and sanitation marketing, and dissemination and education on relevant policies and legal document in hygienic sanitation.
Coordinate with NCERWAHS to implement the rural water and hygienic sanitation programme.
Abbreviation Description AGCFP An Giang Child-Friendly Project CSDP Child Survival and development programme DBCFP Dien Bien Child-Friendly Project DTCFP Dong Thap Child-Friendly Project GLCFP Gia Lai Child-Friendly Project KTCFP Kon Tum Child-Friendly Project with support for Maternal Health LCCFP Lao Cai Child-Friendly Project NTCFP Ninh Thuan Child-Friendly Project with support for Maternal Health
Province Name/ Title of Project
Workplan Start Year
- End Year
Project Component
OP Outcome Outcome OP Output (1) OP Output (2) OP Output (3) CP IR (1) CP IR (2) CP IR (3) CP IR (4)
National, MARD, Water and Sanitation for Children
2012-2013
CSDP Increased quality and effective management of a comprehensive national health system, including health promotion and health protection with a focus on ensuring more equitable access for the most vulnerable and disadvantaged groups.
NA Policy advice and technical support provided to strengthen the building blocks of human and animal health systems, including information systems and the generation of evidence, at national and sub national levels.
National and sub-national capacities enhanced to improve evidence and the quittable access to and demand for quality and sustainable water supply and hygienic sanitation.
NA By 2016, Identified beneficiaries benefit equitably from increased access to improved water and sustainable sanitation.
NA NA NA
National, MARD Water and Sanitation for Children
2014-NA CSDP Increased quality and effective management of a comprehensive national health system, including health promotion and health protection with a focus on ensuring more equitable access for the most
NA Policy advice and technical support provided to strengthen the building blocks of human and animal health systems, including information
National and sub-national capacities enhanced to improve evidence and the quitable access to and demand for quality and sustainable
NA By 2016, Identified beneficiaries benefit equitably from increased access to improved water and
NA NA NA

174
Province Name/ Title of Project
Workplan Start Year
- End Year
Project Component
OP Outcome Outcome OP Output (1) OP Output (2) OP Output (3) CP IR (1) CP IR (2) CP IR (3) CP IR (4)
vulnerable and disadvantaged groups.
systems and the generation of evidence, at national and sub national levels.
water supply and hygienic sanitation.
sustainable sanitation.
National, MARD Water and Sanitation for Children
2015-2016
CSDP Increased quality and effective management of a comprehensive natonal health sytem, including health promotion and health protection with a focus on ensuring more equitable access for the most vulnerable and disadvantaged groups.
NA Policy advice and technical support provided to strengthen the building blocks of human and animal health systems, including information systems and the generation of evidence, at national and sub national levels.
National and sub-national capacities enhanced to improve evidence and the quitable access to and demand for quality and sustainable water supply and hygienic sanitation.
NA NA NA NA NA
National, MOH Water and Sanitation for Children
2012-2013
CSDP refer to One Plan III with output number and text increased quality and effective management of a comprehensive national health system, including health promotion and health protection with a focus on ensuring more equitable access for the most vulnerable and disadvantaged groups.
NA Policy advice and technical support provided to strengthen the building blocks of human and animal health systems, including information systems and the generation of evidence, at national and sub national levels.
Policy advice and technical support provided to improve evidence about, prevent and effectively manage non-communicable conditions at national and sub national levles.
National and sub-national capacities enhanced to strengthen evidence and improve universal access to and utilization of a quality and gender-sensitive package of nutrition and sexual, reproductive, adoloscent, maternal, neonatal and child health care and services.
By 2016, identfied benficiaries are covered with social health insurance and benfit equitably from increased access to sstainable, quality and integrated basic MNCH services.
By 2016, identified beneficiaries benefit equitably from increased access to sustainable, quality and integrated nutrition services.
By 2016, identified beneficiaries benefit equitably from increased access to PMTCT services and paediatric treatment of HIV.
By 2016, identified beneficiaries benefit equitably from increased access to sustainable and hygienic sanitation.
National, MOH Water and Sanitation for Children
2014-NA CSDP refer to One Plan III with output number and text increased quality and effective management of a comprehensive national health system, including health promotion and health protection with a focus on ensuring more equitable access for the most vulnerable and disadvantaged groups.
NA Policy advice and technical support provided to strengthen the building blocks of human and animal health systems, including information systems and the generation of evidence, at national and sub national levels.
Policy advice and technical support provided to improve evidence about, prevent and effectively manage non-communicable conditions at national and sub national levles.
National and sub-national capacities enhanced to strengthen evidence and improve universal access to and utilization of a quality and gender-sensitive package of nutrition and sexual, reproductive, adoloscent, maternal, neonatal and child health care and services.
By 2016, identfied benficiaries are covered with social health insurance and benfit equitably from increased access to sstainable, quality and integrated basic MNCH services.
By 2016, identified beneficiaries benefit equitably from increased access to sustainable, quality and integrated nutrition services.
By 2016, identified beneficiaries benefit equitably from increased access to PMTCT services and paediatric treatment of HIV.
By 2016, identified beneficiaries benefit equitably from increased access to sustainable and hygienic sanitation.
National, MOH Water and Sanitation for Children
2015-2016
CSDP refer to One Plan III with output number and text increased quality and effective management of a comprehensive national health system, including health promotion and health protection with a focus on ensuring more equitable access for the most vulnerable and disadvantaged groups.
NA Policy advice and technical support provided to strengthen the building blocks of human and animal health systems, including information systems and the generation of evidence, at national and sub national levels.
Policy advice and technical support provided to improve evidence about, prevent and effectively manage non-communicable conditions at national and sub national levles.
National and sub-national capacities enhanced to strengthen evidence and improve universal access to and utilization of a quality and gender-sensitive package of nutrition and sexual, reproductive, adoloscent, maternal, neonatal and child health care and services.
By 2016, identfied benficiaries are covered with social health insurance and benfit equitably from increased access to sstainable, quality and integrated basic MNCH services.
By 2016, identified beneficiaries benefit equitably from increased access to sustainable, quality and integrated nutrition services.
By 2016, identified beneficiaries benefit equitably from increased access to PMTCT services and paediatric treatment of HIV.
By 2016, identified beneficiaries benefit equitably from increased access to sustainable and hygienic sanitation.
An Giang, 2012-2013
AGCFP By 2016, improved performance of the
NA Government agencies at the
The public administration
Systems to monitor the
By 2016, the An Giang
By 2016, identified
An Giang child Protection
By 2016, disadvantaged

175
Province Name/ Title of Project
Workplan Start Year
- End Year
Project Component
OP Outcome Outcome OP Output (1) OP Output (2) OP Output (3) CP IR (1) CP IR (2) CP IR (3) CP IR (4)
Child-Friendly Project
public-sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
provincial socio-economic development plan and underlying sector plans and budgets reflect provincial commitment to promote equitable realization of child rights.
beneficiaries in An Giang province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
system is effectively preventing and protecting children from neglect, abuse, violence and exploitation, in particular the most vulnerable children and children in conflict with the law.
children at pre-primary, primary and lower secondary education levels in An Giang benefit from relevant and quality preschool and basic education supported by the provincial education sector plans.
An Giang, Child-Friendly Project
2014-NA AGCFP By 2016, improved performance of the public-sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
NA Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, the An Giang provincial socio-economic development plan and underlying sector plans and budgets reflect provincial commitment to promote equitable realization of child rights.
By 2016, identified beneficiaries in An Giang province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
An Giang child Protection system is effectively preventing and protecting children from neglect, abuse, violence and exploitation, in particular the most vulnerable children and children in conflict with the law.
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in An Giang benefit from relevant and quality preschool and basic education supported by the provincial education sector plans.
An Giang, Child-Friendly Project
2015-2016
AGCFP By 2016, improved performance of the public-sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
NA Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, the An Giang provincial socio-economic development plan and underlying sector plans and budgets reflect provincial commitment to promote equitable realization of child rights.
By 2016, identified beneficiaries in An Giang province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
An Giang child Protection system is effectively preventing and protecting children from neglect, abuse, violence and exploitation, in particular the most vulnerable children and children in conflict with the law.
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in An Giang benefit from relevant and quality preschool and basic education supported by the provincial education sector plans.
Dien Bien, Child-Friendly Project
2012-2013
DBCFP By 2016, improved performance of the public-sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
NA Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, enhanced capacity for child sensitive planning, budgeting, monitoring and oversight of the Dien Bien socio-economic development an underlying sector plans.
By 2016, identified beneficiaries in Dien Bien province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
By 2016, Child Protection system strengthened to provide effective prevention and protection of children from neglect, abuse, and exploitation and being in conflict with the law.
By 2016, disadvantaged children particularly those of ethnic minority in Dien Bien province benefit from relevant and quality preschool and basic education supported by the provincial education sector plans.
Dien Bien, Child-Friendly Project
2014-NA DBCFP By 2016, improved performance of the public-sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
NA Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, enhanced capacity for child sensitive planning, budgeting, monitoring and oversight of the Dien Bien socio-economic development an underlying sector plan.
By 2016, identified beneficiaries in Dien Bien province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
By 2016, Child Protection system strengthened to provide effective prevention and protection of children from neglect, abuse, and exploitation and being in conflict with the law.
By 2016, disadvantaged children particularly those of ethnic minority in Dien Bien province benefit from relevant and quality preschool and basic education supported by the provincial education sector plans.

176
Province Name/ Title of Project
Workplan Start Year
- End Year
Project Component
OP Outcome Outcome OP Output (1) OP Output (2) OP Output (3) CP IR (1) CP IR (2) CP IR (3) CP IR (4)
Dien Bien, Child-Friendly Project
2015-2016
DBCFP By 2016, improved performance of the public-sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
NA Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, enhanced capacity for child sensitive planning, budgeting, monitoring and oversight of the Dien Bien socio-economic development an underlying sector plan.
By 2016, identified beneficiaries in Dien Bien province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
By 2016, Child Protection system strengthened to provide effective prevention and protection of children from neglect, abuse, and exploitation and being in conflict with the law.
By 2016, disadvantaged children particularly those of ethnic minority in Dien Bien province benefit from relevant and quality preschool and basic education supported by the provincial education sector plans.
Dong Thap, Child-Friendly Project
2012-2013
DTCFP By 2016, improved performance of the public-sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
NA Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, the Dong Thap provincial socio-economic development plan and underlying sector plans and budgets reflect provincial commitment to promote equitable realization of child rights.
By 2016, identified beneficiaries in Dong Thap province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
By 2016, Child Protection system strengthened to provide effective prevention and protection of children from neglect, abuse, and exploitation and being in conflict with the law.
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in Dong Thap…
Dong Thap, Child-Friendly Project
2014-NA DTCFP By 2016, improved performance of the public-sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
NA Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, the Dong Thap provincial socio-economic development plan and underlying sector plans and budgets reflect provincial commitment to promote equitable realization of child rights.
By 2016, identified beneficiaries in Dong Thap province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
By 2016, Child Protection system strengthened to provide effective prevention and protection of children from neglect, abuse, and exploitation and being in conflict with the law.
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in Dong Thap…
Dong Thap, Child-Friendly Project
2015-2016
DTCFP By 2016, improved performance of the public-sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
NA Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, the Dong Thap provincial socio-economic development plan and underlying sector plans and budgets reflect provincial commitment to promote equitable realization of child rights.
By 2016, identified beneficiaries in Dong Thap province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
By 2016, Child Protection system strengthened to provide effective prevention and protection of children from neglect, abuse, and exploitation and being in conflict with the law.
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in Dong Thap…
Gia Lai, Child-Friendly Project
2012-2013
GLCFP By 2016, improved performance of the public-sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
NA Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, the Gia Lai provincial socio-economic development plan and underlying sector plans and budgets reflect provincial commitment to promote equitable realization of child rights.
By 2016, identified beneficiaries in Gia Lai province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition,
Gia Lai child Protection system is effectively preventing and protecting children from neglect, abuse, violence and exploitation, in particular the most vulnerable children and children in
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in Gia Lai benefit from relevant and quality preschool and basic education supported by the provincial education sector plans.

177
Province Name/ Title of Project
Workplan Start Year
- End Year
Project Component
OP Outcome Outcome OP Output (1) OP Output (2) OP Output (3) CP IR (1) CP IR (2) CP IR (3) CP IR (4)
disadvantaged groups.
WASH and MNCH).
conflict with the law.
Gia Lai, Child-Friendly Project
2014-NA GLCFP By 2016, improved performance of the public sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
NA Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, the Gia Lai provincial socio-economic development plan and underlying sector plans and budgets reflect provincial commitment to promote equitable realization of child rights.
By 2016, identified beneficiaries in Gia Lai province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
Gia Lai child Protection system is effectively preventing and protecting children from neglect, abuse, violence and exploitation, in particular the most vulnerable children and children in conflict with the law.
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in Gia Lai benefit from relevant and quality preschool and basic education supported by the provincial education sector plans.
Gia Lai, Child-Friendly Project
2015-2016
GLCFP By 2016, improved performance of the public sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
NA Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, the Gia Lai provincial socio-economic development plan and underlying sector plans and budgets reflect provincial commitment to promote equitable realization of child rights.
By 2016, identified beneficiaries in Gia Lai province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
Gia Lai child Protection system is effectively preventing and protecting children from neglect, abuse, violence and exploitation, in particular the most vulnerable children and children in conflict with the law.
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in Gia Lai benefit from relevant and quality preschool and basic education supported by the provincial education sector plans.
Kon Tum, Child-Friendly Project with support for Maternal Health
2012-2013
KTCFP By 2016, improved performance of the public-sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
By 2016, increased quality and effective management of a comprehensive national health system, including health promotion, with a focus on ensuring more equitable access for the most vulnerable and disadvantaged groups.
Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, enhanced capacity for child sensitive planning, budgeting, monitoring and oversight of the Kon Tum socio-economic development an underlying sector plans.
By 2016, identified beneficiaries in Kon Tum province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
By 2016, Child Protection system strengthened to provide effective prevention and protection of children from neglect, abuse, and exploitation and being in conflict with the law.
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in Kon Tum benefit from relevant and quality preschool and basic education supported by the provincial education sector plans.
Kon Tum, Child-Friendly Project with support for Maternal Health
2014-NA KTCFP By 2016, improved performance of the public sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
By 2016, increased quality and effective management of a comprehensive national health system, including health promotion, with a focus on ensuring more equitable access for the most vulnerable and disadvantaged groups.
Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, enhanced capacity for child sensitive planning, budgeting, monitoring and oversight of the Kon Tum socio-economic development an underlying sector plans.
By 2016, identified beneficiaries in Kon Tum province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
By 2016, Child Protection system strengthened to provide effective prevention and protection of children from neglect, abuse, and exploitation and being in conflict with the law.
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in Kon Tum benefit from relevant and quality preschool and basic education supported by the provincial education sector plans.
Kon Tum, Child-Friendly Project with support for Maternal Health
2015-2016
KTCFP By 2016, improved performance of the public sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most
By 2016, increased quality and effective management of a comprehensive national health system, including health promotion, with a focus on
Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms
By 2016, enhanced capacity for child sensitive planning, budgeting, monitoring and oversight of the Kon Tum socio-economic development
By 2016, identified beneficiaries in Kon Tum province are covered with social health insurance and benefit equitably from increased access to sustainable
By 2016, Child Protection system strengthened to provide effective prevention and protection of children from neglect, abuse, and exploitation and being in
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in Kon Tum benefit from relevant and quality preschool and basic education

178
Province Name/ Title of Project
Workplan Start Year
- End Year
Project Component
OP Outcome Outcome OP Output (1) OP Output (2) OP Output (3) CP IR (1) CP IR (2) CP IR (3) CP IR (4)
vulnerable and disadvantaged groups.
ensuring more equitable access for the most vulnerable and disadvantaged groups.
delivery for the most vulnerable and disadvantaged groups.
accountability and transparency.
for citizens feedback.
an underlying sector plans.
and quality basic CSD services (nutrition, WASH and MNCH).
conflict with the law.
supported by the provincial education sector plans.
Lao Cai, Child-Friendly Project
2012-2013
LCCFP By 2016, improved performance of the public sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
NA Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, the Lao Cai provincial socio-economic development plan and underlying sector plans and budgets reflect provincial commitment to promote equitable realization of child rights.
By 2016, identified beneficiaries in Lao Cai province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
The child Protection system in Lao Cai is effectively preventing and protecting children from neglect, abuse, violence and exploitation, in particular the most vulnerable children and children in conflict with the law.
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in Lao Cai benefit from relevant and quality preschool and basic education supported by the provincial education sector plans.
Lao Cai, Child-Friendly Project
2014-NA LCCFP By 2016, improved performance of the public sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
NA Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, the Lao Cai provincial socio-economic development plan and underlying sector plans and budgets reflect provincial commitment to promote equitable realization of child rights.
By 2016, identified beneficiaries in Lao Cai province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
The child Protection system in Lao Cai is effectively preventing and protecting children from neglect, abuse, violence and exploitation, in particular the most vulnerable children and children in conflict with the law.
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in Lao Cai benefit from relevant and quality preschool and basic education supported by the provincial education sector plans.
Lao Cai, Child-Friendly Project
2015-2016
LCCFP By 2016, improved performance of the public-sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
NA Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, the Lao Cai provincial socio-economic development plan and underlying sector plans and budgets reflect provincial commitment to promote equitable realization of child rights.
By 2016, identified beneficiaries in Lao Cai province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
The child Protection system in Lao Cai is effectively preventing and protecting children from neglect, abuse, violence and exploitation, in particular the most vulnerable children and children in conflict with the law.
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in Lao Cai benefit from relevant and quality preschool and basic education supported by the provincial education sector plans.
Ninh Thuan, Child-Friendly Project with support for Maternal Health
2012-2013
NTCFP By 2016, improved performance of the public-sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
By 2016, increased quality and effective management of a comprehensive national health system, including health promotion, with a focus on ensuring more equitable access for the most vulnerable and disadvantaged groups.
Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, the Ninh Thuan provincial socio-economic development plan and underlying sector plans and budgets reflect provincial commitment to promote equitable realization of child rights.
By 2016, identified beneficiaries in Ninh Thuan province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
Ninh Thuan child Protection system is effectively preventing and protecting children from neglect, abuse, violence and exploitation, in particular the most vulnerable children and children in conflict with the law.
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in Ninh Thuan benefit from relevant and quality preschool and basic education supported by the provincial education sector plans.
Ninh Thuan, Child-Friendly Project with support for
2014-NA NTCFP By 2016, improved performance of the public-sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will
By 2016, increased quality and effective management of a comprehensive national health system,
Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-
By 2016, the Ninh Thuan provincial socio-economic development plan and underlying sector plans
By 2016, identified beneficiaries in Ninh Thuan province are covered with social health insurance and benefit
Ninh Thuan child Protection system is effectively preventing and protecting children from neglect,
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in Ninh Thuan benefit from

179
Province Name/ Title of Project
Workplan Start Year
- End Year
Project Component
OP Outcome Outcome OP Output (1) OP Output (2) OP Output (3) CP IR (1) CP IR (2) CP IR (3) CP IR (4)
Maternal Health
reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
including health promotion, with a focus on ensuring more equitable access for the most vulnerable and disadvantaged groups.
planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
customer-oriented approach and strengthened mechanisms for accountability and transparency.
based and include mechanisms for citizens feedback.
and budgets reflect provincial commitment to promote equitable realization of child rights.
equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
abuse, violence and exploitation, in particular the most vulnerable children and children in conflict with the law.
relevant and quality preschool and basic education supported by the provincial education sector plans.
Ninh Thuan, Child-Friendly Project with support for Maternal Health
2015-2016
NTCFP By 2016, improved performance of the public-sector institutions at national and sub-national levels, through enhanced coordination, accountability, transparency and anti-corruption efforts, will reduce disparities and ensure access to public services for the most vulnerable and disadvantaged groups.
By 2016, increased quality and effective management of a comprehensive national health system, including health promotion, with a focus on ensuring more equitable access for the most vulnerable and disadvantaged groups.
Government agencies at the national and sub-national level are able to apply participatory, evidence-based and cross-sectoral approaches in planning, implementation and monitoring the public services delivery for the most vulnerable and disadvantaged groups.
The public administration systems at national level and in selected provinces have enhanced human resources management systems, have a customer-oriented approach and strengthened mechanisms for accountability and transparency.
Systems to monitor the performance of government institutions and the delivery of basic public services are evidence-based and include mechanisms for citizens feedback.
By 2016, the Ninh Thuan provincial socio-economic development plan and underlying sector plans and budgets reflect provincial commitment to promote equitable realization of child rights.
By 2016, identified beneficiaries in Ninh Thuan province are covered with social health insurance and benefit equitably from increased access to sustainable and quality basic CSD services (nutrition, WASH and MNCH).
Ninh Thuan child Protection system is effectively preventing and protecting children from neglect, abuse, violence and exploitation, in particular the most vulnerable children and children in conflict with the law.
By 2016, disadvantaged children at pre-primary, primary and lower secondary education levels in Ninh Thuan benefit from relevant and quality preschool and basic education supported by the provincial education sector plans.

180
A. Activity-wise description of seven provinces
*CSD: Child Survival & Development
Province Start and End Date
Intermediate Result
number and title
Activity #
Statement
An Giang, 2012-2013
IR-3, CSD*
13 Support development and implementation of provincial plans on health and nutrition including the PMTCT, CWDs CIP, water and sanitation with focus on equity, ethnic minority and the poor, in line with the national targeted Programme and strategies
An Giang, 2012-2013
IR-3, CSD
14 Support institutional capacity development for scaling up high impact interventions in MNCH nutrition (breastfeeding & stunting reduction), including PMTCT, CWD, CIP, health insurance cards for under 6 children, social marketing of iron folic, scaling up water sanitation package for better child survival and development (CLTS), Sanitation marketing, HWWS, HWTS
An Giang, 2012-2013
IR-3, CSD
15 Support data collection on MNCH and nutrition to serve local planning that includes promotion of micro planning approach (RED) for improvement CSD minimum intervention package and emergency response, Support implementation of RWSS M&E system
An Giang, 2012-2013
IR-3, CSD
16 Support monitoring health nutation intervention that includes the coverage and used of health insurance cards among children under 6 in disadvantage locations, monitoring the implementation of the child health related national law & decrees (decree 21, law on advertisement of breast milk substitutes)
An Giang, 2012-2013
IR-3, CSD
17 Support mass media, hospital & community-based communication interventions to promote good practices in Maternal and Child Health, Nutrition (focusing on IYCF/exclusive breastfeeding), Hand washing with soap and HIV/AIDS
An Giang, 2014-2014
IR-3, CSD
7.1 Conduct data collection on child mortality among ethnic minority population.
An Giang, 2014-2014
IR-3, CSD
7.2 Assess the compliance with the revised national Decree # 21 on Marketing of Breast Milk Substitute and related component of the Law on Advertisement.
An Giang, 2014-2014
IR-3, CSD
7.3 Support annual meeting on the latest MNCH-Nutrition profile and reviewing of implementation /co-ordination status of the Provincial Action Plan on MNCH-Nutrition for reduction of child stunting (2013-2016) to address inequity in health care services.
An Giang, 2014-2014
IR-3, CSD
7.4 Conduct monitoring/supervision by the provincial team on implementation of social marketing activity for iron folic.
An Giang, 2014-2014
IR-3, CSD
7.5 Organize biannual review meeting of the partnership and progress on implementation of the social marketing iron folic.
An Giang, 2014-2014
IR-3, CSD
7.6 Support application of new MOH's hospital quality assessment with focus on BFHI counselling in three selective district hospitals.
An Giang, 2014-2014
IR-3, CSD
7.7 Support preventive Health and the MCH centre in implementation of Growth Watch Model for checking child malnutrition using cell phones and improve quality of data collection; increase quality of data collection in nutrition surveillance/ analysis/reporting to inform an equity approach.
An Giang, 2014-2014
IR-3, CSD
7.8 Support development of a provincial action plan on PMTCT.
An Giang, 2014-2014
IR-3, CSD
7.9 Support implementation of integrated mass media activities through provincial TV/Radio and commune loud speaker’s system, including nutrition messages (focusing on anemia prevention, EBF and IYCF); MCH (including Health insurance); and WASH.
An Giang, 2014-2014
IR-3, CSD
7.1 Support production of IEC materials on integrated CSD flagship topics.
An Giang, 2014-2014
IR-3, CSD
7.11 Support rolling out refresh communication skills trainings, including training on CWD.
An Giang, 2014-2014
IR-3, CSD
7.12 Support to conducting a rapid KAP survey on community -based supporting model on EBF in project communes
An Giang, 2014-2014
IR-3, CSD
7.13 Support contextualization and roll out of existing community based-breastfeeding and complementary feeding model to improve BF practices
An Giang, 2014-2014
IR-3, CSD
8.1 Support the development of provincial behavioral change communication action plans on flagship areas (handwashing & drinking water, diarrheal and pneumonia management; anemia prevention, IYCF, health insurance for children under 6
An Giang, 2014-2014
IR-3, CSD
9.1 Support updating NRWSS M&E system and conducting data analysis to understand inequity in sanitation and water safety
An Giang, 2014-2014
IR-3, CSD
9.2 Identify best practices on WASH and identify existing knowledge over low-cost sanitation options in communes/villages for documentation and dissemination
An Giang, 2014-2014
IR-3, CSD
9.3 Support trial of ODF verification and certification
An Giang, 2014-2014
IR-3, CSD
9.4 Organize training and triggering on CLTS/ sanitation marketing/ HWTS
An Giang, 2014-2014
IR-3, CSD
9.5 Support trained masons/artisans and entrepreneurs to carry out low-cost sanitation promotion/marketing
An Giang, 2014-2014
IR-3, CSD
9.6 Organize forums to facilitate interaction among private entrepreneurs, community leaders, and line department officials to help design products for low income communities and market existing products
An Giang, 2014-2014
IR-3, CSD
9.7 Support regular monitoring, review meetings and cross-learning visits within and outside the province on WASH (KG/CDSS)
An Giang, 2014-2014
IR-3, CSD
9.8 Support to organize community mobilization sessions for WASH through interpersonal communication (village meetings, household visits) in schools and on the occasion of GHWD.
An Giang, 2014-2014
IR-3, CSD
9.9 Promote sustainable school WASH initiatives involving school and community.
An Giang, 2014-2014
IR-3, CSD
9.1 Support development of DRR/CCA planning in WASH (with technical and financial support from NCERWASS)
An Giang, 2015-2016
IR-4, CSD
11 Advocate for and conduct supportive monitoring and supervision, and capacity building to ensure implementation and application of BFHI and nutrition related indicators (under mew MOH quality assessment criteria); and 4 early essential newborn care interventions (active management of the third stage of labor, delay cord clamping, immediate skin to skin contact, and early initiation of breastfeeding, kangaroo Management Care (KMC) in provincial and all district hospitals in the province:
An Giang, 2015-2016
IR-4, CSD
11.1 Support integrated monitoring/supervision of new practices
An Giang, 2015-2016
IR-4, CSD
11.2 Support capacity building for new practices, including KMC, new born mortality audit for provincial and district health staff
An Giang, 2015-2016
IR-4, CSD
12 Capacity building for strengthening nutrition surveillance, and for scaling up social marketing approach for improve coverage of iron folic supplementation among pregnant and none pregnant women in new districts (An Phu district, Thoai Son), and female worker in selective private production factories in An giang:
An Giang, 2015-2016
IR-4, CSD
12.1 Training for health staff on social marketing of to new districts
An Giang, 2015-2016
IR-4, CSD
12.2 Support field monitoring of the province and district staff
An Giang, 2015-2016
IR-4, CSD
12.3 Training of a provincial core team on nutrition data collection and analysis
An Giang, 2015-2016
IR-4, CSD
13 Conducting implementation review meeting of the provincial plan action MNCH-Nutrition for reduction of chill stunting (2013-2016) for lesson learnt, and for formulation of a new provincial action plan for 2017-2010 period.
An Giang, 2015-2016
IR-4, CSD
14 Support integrated nutrition communication using local media focusing on health and nutrition including breastfeeding and iron folic supplementation messages in the project districts of Phu Tan, An Phu, Tri Ton
An Giang, 2015-2016
IR-4, CSD
15 Implement Community Led Total Sanitation (CLTS) model in six communes in 3 districts of An Phu, Thoai Son and Tri Ton in 2015 and 6 new communes in 2016 and conduct ODF verification and certification in 5 districts of An Phu, Tin Bien, Tri Ton, Thoai Son, Chau Thanh:
An Giang, 2015-2016
IR-4, CSD
15.1 Conduct training on CLTS, SLTS, low-cost latrine construction and sanitation marketing and ODF
An Giang, 2015-2016
IR-4, CSD
15.2 Conduct survey and triggering of CLTS, School Led Total Sanitation (SLTS)
An Giang, 2015-2016
IR-4, CSD
15.3 Organize community mobilization activities, combined with hand washing with soap (HWWS), including household classifying and sanitation mapping and develop a video clip on ODF

181
Province Start and End Date
Intermediate Result
number and title
Activity #
Statement
An Giang, 2015-2016
IR-4, CSD
15.4 Organize forums/ design competition on low cost appropriate latrine models and promote for low-cost sanitation products.
An Giang, 2015-2016
IR-4, CSD
15.5 Verify and certify ODF villages
An Giang, 2015-2016
IR-4, CSD
16 Develop post 2015 provincial WASH plan, focusing on scaling up sanitation and sustainability of WASH facilities in communities and schools.
An Giang, 2015-2016
IR-4, CSD
17 Maintain HWTS in Tinh Bien district and scale up HWTS in Tri Ton and Thoai Son districts:
An Giang, 2015-2016
IR-4, CSD
17.1 Organize training on HWTS combined with HWWS
An Giang, 2015-2016
IR-4, CSD
17.2 Support communication activates such as village meeting, household visits, mass media communication on HWTS combined with HWWS
An Giang, 2015-2016
IR-4, CSD
17.3 Support survey, monitoring, evaluation of HWTS combined with HWWS.
An Giang, 2015-2016
IR-4, CSD
17.4 Pilot a model on private sector involvement in HWTS supporting entrepreneurs produce and promote Cambodian ceramic pot filters
An Giang, 2015-2016
IR-4, CSD
18 Support development and implementation of detailed provincial/commune WASH Disaster Risk Management/Climate Change Adaption (DRM/CCA) plan
Ninh Thuan, 2012-2013
IR-3, CSD
12 Provide technical and financial support to the development of the provincial action plan, focusing on equity, ethnic minority and the poor:
Ninh Thuan, 2012-2013
IR-3, CSD
12.1 Provincial RWSS NTP3 plans and strengthening coordination of RWSS NTP3 implementation
Ninh Thuan, 2012-2013
IR-3, CSD
12.2 Integrated MNCH and nutrition plan of action
Ninh Thuan, 2012-2013
IR-3, CSD
13 Strengthen the provincial capacity on:
Ninh Thuan, 2012-2013
IR-3, CSD
13.1 Health insurance for under-6 children
Ninh Thuan, 2012-2013
IR-3, CSD
13.2 CLTS, Hand washing with soap, household water treatment and storage and sanitation marketing and sanitation marketing
Ninh Thuan, 2012-2013
IR-3, CSD
13.3 MNCH and nutrition essential intervention package that includes community based and hospital based IYCF/IMAM activities
Ninh Thuan, 2012-2013
IR-3, CSD
13.4 Emergency responses
Ninh Thuan, 2012-2013
IR-3, CSD
14 Support for M&E, MNCH and RWSS data collection and studies.
Ninh Thuan, 2012-2013
IR-3, CSD
15 Support conduct of formative research and development/implementation of C4D integrated model to address behavioral and social change determinants on MNCH, Nutrition (focusing on IYCF/exclusive breastfeeding) and Hand washing with soap in targeted areas
Ninh Thuan, 2014-2014
IR-3, CSD
6.1 Support the provincial Center for Preventive Medicine to improve the quality of data collection and analysis in the annual nutrition data collection to inform the equity approach.
Ninh Thuan, 2014-2014
IR-3, CSD
6.2 Organize a review meeting on the latest MNCH-Nutrition profile, review of implementation/ coordination process of the provincial integrated MNCH-Nutrition Plan of action for reduction of child stunting for actions required to address inequity in MNCH-nutrition package.
Ninh Thuan, 2014-2014
IR-3, CSD
6.3 Conduct 01 TOT training on neonatal care for district and commune responsible workers.
Ninh Thuan, 2014-2014
IR-3, CSD
6.4 Support a training of ethnic minority midwives in Thuan Bac district
Ninh Thuan, 2014-2014
IR-3, CSD
6.5 Support outreach services for the most difficult communes and villages
Ninh Thuan, 2014-2014
IR-3, CSD
6.6 Support 01 Training on IMAM in patient care for Bac Ai and provincial hospitals & Purchase of HeBi products for IMAM implementation 2014 in Bac Ai district
Ninh Thuan, 2014-2014
IR-3, CSD
6.7 Conduct community market and demand assessment for application of social marketing in promotion of iron folic tablets in Ninh Hai district.
Ninh Thuan, 2014-2014
IR-3, CSD
6.8 Support application of new MOH's hospital quality assessment in selective districts with focus on BFHI criteria and counselling services.
Ninh Thuan, 2014-2014
IR-3, CSD
6.9 Organize a training workshop on Health-Nutrition Information Management, analysis of the data, and the use data for equity planning in health.
Ninh Thuan, 2014-2014
IR-3, CSD
6.1 Support Joint monitoring od the CSD programme components of WASH health and nutrition.
Ninh Thuan, 2014-2014
IR-3, CSD
6.11 Support supervisory monitoring of IMAM services at province, district, commune and village levels for consolidation and review of IMAM performance indicator and on job training
Ninh Thuan, 2014-2014
IR-3, CSD
6.12 Support implementation of the community based breastfeeding promotion and other MNCH and WASH issues in selective communes.
Ninh Thuan, 2014-2014
IR-3, CSD
7.1 Support the development of provincial behavioral change communication action plans on handwashing, drinking water, diarrheal and pneumonia management
Ninh Thuan, 2014-2014
IR-3, CSD
8.1 Support updating NRWSS M&E system and conducting data analysis to understand inequity in sanitation and water safety
Ninh Thuan, 2014-2014
IR-3, CSD
8.2 Identify best practices on WSAH in communes/villages for documentation and dissemination
Ninh Thuan, 2014-2014
IR-3, CSD
8.3 Support trial of ODF verification and certification
Ninh Thuan, 2014-2014
IR-3, CSD
8.4 Organize training and triggering on CLTS/ sanitation marketing/ HWTS
Ninh Thuan, 2014-2014
IR-3, CSD
8.5 Support trained masons/artisans and entrepreneurs to carry out low-cost sanitation promotion/marketing
Ninh Thuan, 2014-2014
IR-3, CSD
8.6 Organize forums to facilitate interaction among private entrepreneurs, community leaders, and line department officials to help design products for low income communities and market existing products
Ninh Thuan, 2014-2014
IR-3, CSD
8.7 Support regular monitoring, review meetings and cross-learning visits within and outside the province on WASH
Ninh Thuan, 2014-2014
IR-3, CSD
8,8 Support to organize WASH communication sessions through interpersonal communication (village meetings, household visits) in schools and on the occasion of GHWD.
Ninh Thuan, 2014-2014
IR-3, CSD
8.9 Promote sustainable school WASH initiatives involving school and community.
Ninh Thuan, 2014-2014
IR-3, CSD
8.1 Support development of DRR/CCA planning in WASH (with technical and financial support from NCERWASS)
Ninh Thuan, 2015-2016
IR-4, CSD
13 Support application of BFHI and nutrition related indicators (under new MOH quality assessment criteria); key essential newborn care interventions (active management of the third stage of labor, delay cord clamping, immediate skin to skin contact, and early initiation of breastfeeding, kangaroo Management Care (LMC)) in provincial and all district hospitals:
Ninh Thuan, 2015-2016
IR-4, CSD
13.1 Support integrated monitoring/supervision of new practices
Ninh Thuan, 2015-2016
IR-4, CSD
13.2 Support training for capacity building of new practices
Ninh Thuan, 2015-2016
IR-4, CSD
14 Conduct integrated outreach services (antenatal care, postnatal care, immunization, growth monitoring and communication, IMAM) in difficult communes

182
Province Start and End Date
Intermediate Result
number and title
Activity #
Statement
Ninh Thuan, 2015-2016
IR-4, CSD
14.1 Conduct micro-planning at commune level
Ninh Thuan, 2015-2016
IR-4, CSD
14.2 Conduct outreach services
Ninh Thuan, 2015-2016
IR-4, CSD
14.3 Conduct quarterly monitoring, supervision, reporting and sharing lesson learnt.
Ninh Thuan, 2015-2016
IR-4, CSD
15 Support implementation of nutrition and household food security activities for reduction of child stunting (in collaboration with the FAO/WHO:
Ninh Thuan, 2015-2016
IR-4, CSD
15.1 Support baseline assessment on food nutrition and infant and young child feeding in two selective communes.
Ninh Thuan, 2015-2016
IR-4, CSD
15.2 Support integrated planning activities on home gardening and food supply activities (FAO/DARD) with infant and young child feeding interventions.
Ninh Thuan, 2015-2016
IR-4, CSD
15.3 Support for additional training on infant and young child feeding in combination with enhanced household food production, communication and social mobilization skills.
Ninh Thuan, 2015-2016
IR-4, CSD
16 Support the design and production of communication materials on new nutrient rich foods available in localities for integrating agricultural and nutrition issues ( leaflets, flipcharts)
Ninh Thuan, 2015-2016
IR-4, CSD
17 Supporting communication activities at district commune and village levels on the infant and Young Child Feeding (IYCF) and mobilizing households to grow and use of local food products for improvement of quality of children meals (local food, complimentary food preparation using local agricultural products) (implemented jointly with the DARD):
Ninh Thuan, 2015-2016
IR-4, CSD
17.1 Club activities and group talks
Ninh Thuan, 2015-2016
IR-4, CSD
17.2 Local Radio message delivery
Ninh Thuan, 2015-2016
IR-4, CSD
17.3 Home visit
Ninh Thuan, 2015-2016
IR-4, CSD
17.4 Organize contests of good communities
Ninh Thuan, 2015-2016
IR-4, CSD
18 Capacity building in nutrition surveillance and local planning:
Ninh Thuan, 2015-2016
IR-4, CSD
18.1 Support data collection, data analysis and use of data for local planning
Ninh Thuan, 2015-2016
IR-4, CSD
18.2 Support a review meeting on implementation of the provincial action plan on MNCH-Nutrition for reduction of child stunting period 2013
Ninh Thuan, 2015-2016
IR-4, CSD
18.3 2016, and development the new cycle plan
Ninh Thuan, 2015-2016
IR-4, CSD
19 Support inter-sectoral monitoring of WASH, Nutrition, MNCH activities
Ninh Thuan, 2015-2016
IR-4, CSD
20 Maintaining CLTS in five communes of Thuan Bac and 4 communes of Bac Ai and verify and certify 20 ODF villages in three districts of Hai Ninh Thuan Bac and Bac Ai
Ninh Thuan, 2015-2016
IR-4, CSD
20.1 Conduct review meeting of 2014 achievement and plan for 2015-2016 combined with sharing ODF guidelines
Ninh Thuan, 2015-2016
IR-4, CSD
20.2 Organize training and triggering on CLTS and SLTS, low cost latrine construction and sanitation marketing and ODF
Ninh Thuan, 2015-2016
IR-4, CSD
20.3 Support community mobilization through village meetings, household visits and school activities
Ninh Thuan, 2015-2016
IR-4, CSD
20.4 Conduct regular monitoring, review meetings and study visits to best WASH practices in and outside the province
Ninh Thuan, 2015-2016
IR-4, CSD
20.5 Verify and certify ODF villages
Ninh Thuan, 2015-2016
IR-4, CSD
21 Develop post 2015 provincial WASH plan, focusing on scaling up sanitation and sustainability of WASH facilities in communities and at schools.
Ninh Thuan, 2015-2016
IR-4, CSD
22 Maintain household water treatment and storage in Bac Ai district
Ninh Thuan, 2015-2016
IR-4, CSD
22.1 Organize community mobilization (household visits, village meetings, radio, media campaigns ,…) integration of clean water, sanitation, and hygiene to promote and monitor the adoption of HWTS measures
Ninh Thuan, 2015-2016
IR-4, CSD
22.2 Support field water test kilts for water quality testing.
Ninh Thuan, 2015-2016
IR-4, CSD
22.3 Demonstrate HWTS options; provide water purification chemicals, water storage tank for about 20 poor households, households with children under 5 years of age in disadvantaged areas.
Ninh Thuan, 2015-2016
IR-4, CSD
22.4 Monitor project activities especially the HWTS communication activities and study visits to best practices
Ninh Thuan, 2015-2016
IR-4, CSD
22.5 Document and disseminate best practices for policy and budget influencing
Ninh Thuan, 2015-2016
IR-4, CSD
23 Update NRWSS M&E system
Ninh Thuan, 2015-2016
IR-4, CSD
24 Support development and implementation of provincial/communal detailed WASH DRR/CCA plan
Dien Bien, 2012-2013
IR-3, CSD
13 Provide policy advice and technical support for development of:
Dien Bien, 2012-2013
IR-3, CSD
13.1 Provincial RWSS NTP3 plan of 2013-2014
Dien Bien, 2012-2013
IR-3, CSD
13.2 Provincial MNCH and nutrition integrated action plans
Dien Bien, 2012-2013
IR-3, CSD
13.3 Provincial HIV/AIDS and PMTCT action plan under frame work of NTP of HIV/AIDs, focusing on equity, ethnic minority and the poor
Dien Bien, 2012-2013
IR-3, CSD
14 Support for implementation of:
Dien Bien, 2012-2013
IR-3, CSD
14.1 Model o micro-planning approach (RED) to increase coverage of essential MNCH and nutrition services
Dien Bien, 2012-2013
IR-3, CSD
14.2 Integrated management of acute malnutrition (IMAM)
Dien Bien, 2012-2013
IR-3, CSD
14.3 PMTCT and NTP for HIV/AIDS plans
Dien Bien, 2012-2013
IR-3, CSD
14.4 CLTS and HWWS
Dien Bien, 2012-2013
IR-3, CSD
14.5 Sanitation marketing
Dien Bien, 2012-2013
IR-3, CSD
14.6 Household water treatment and storage (HWTS) to provide minimum service packages to women and children of ethnic minorities in hard to reach areas
Dien Bien, 2012-2013
IR-3, CSD
16 Support for capacity building, coordination, data collection, and monitor the implementation of MNCH-nutrition package including PMTCT and pediatric HIV care, IMAM, RWSS NTP3, and emergency responses
Dien Bien, 2012-2013
IR-3, CSD
17 Support promotion of breast feeding and IYCF good practices among local health care network that includes strengthening of BFHI standards at local hospitals and health clinics

183
Province Start and End Date
Intermediate Result
number and title
Activity #
Statement
Dien Bien, 2012-2013
IR-3, CSD
18 Conduct a cross-sectoral base-line evaluation on CSD, CP and SPG
Dien Bien, 2012-2013
IR-3, CSD
19 Support conduct of formative research and development/implementation of C4D integrated model to address behavioral and social change determinants on MNCH, Nutrition (focusing on IYCF/exclusive breastfeeding) and Hand washing with soap in targeted areas
Dien Bien, 2014-2014
IR-3, CSD
7.1 Review of the latest provincial MNCH-Nutrition profile (including EPI), and status of implementation & coordination for implementation of the provincial MNCH-Nutrition Action Plan
Dien Bien, 2014-2014
IR-3, CSD
7.2 Support nutrition surveillance through strengthening quality of disaggregated data collection and analysis
Dien Bien, 2014-2014
IR-3, CSD
7.3 Conduct supervision of IMAM services at district, commune and village levels including consolidation and review of performance indicators and on the job training when required
Dien Bien, 2014-2014
IR-3, CSD
7.4 Support for interim purchasing of HEBI for IMAM services in community and hospital bases
Dien Bien, 2014-2014
IR-3, CSD
7.5 Conduct training in high impact interventions for maternal and child health:
Dien Bien, 2014-2014
IR-3, CSD
7.5.1 Management and administration of EPI
Dien Bien, 2014-2014
IR-3, CSD
7.5.2 Health information system and the use of data for equity planning (MNCH- nutrition-EPI)
Dien Bien, 2014-2014
IR-3, CSD
7.5.3 Ethnic minority midwives (1 training x 15 people)/ training, (knowledge and practices).
Dien Bien, 2014-2014
IR-3, CSD
7.5.4 IYCF
Dien Bien, 2014-2014
IR-3, CSD
7.6 Support application of new National Quality Assessment Criteria for Hospitals to guide nationwide expansion, including incorporate standards for Baby Friendly Hospital and nutrition examination, treatment and care
Dien Bien, 2014-2014
IR-3, CSD
7.7 Conduct integrated outreach services (pregnancy check-up, post natal visits, immunization, child growth monitoring, and C4D) in difficult communes
Dien Bien, 2014-2014
IR-3, CSD
7.8 conduct workshops to plan for the provision of maternal and child healthcare interventions to hard-to-reach areas
Dien Bien, 2014-2014
IR-3, CSD
7.9 Conduct integrated monitoring and supervision on reproductive health/safe motherhood, skilled birth assistance, nutrition, IMAM, BFHI in provincial and district hospital and commune health centers
Dien Bien, 2014-2014
IR-3, CSD
7.1 Support for roll out of KMC in provincial and district hospitals
Dien Bien, 2014-2014
IR-3, CSD
7.11 Design and disseminate cost effective latrine models appropriate for local settings
Dien Bien, 2014-2014
IR-3, CSD
8.1 Support the development of provincial behavioral change communication action plans on flagship areas(hand-washing & drinking water, diarrheal and pneumonia management; anemia prevention, IYCF, health insurance for children under 6)
Dien Bien, 2014-2014
IR-3, CSD
8.2 Conduct integrated C4D activities at community level on family planning, safe motherhood, child healthcare, immunization, nutrition, and water and hygienic sanitation, and HIV/AIDS (incorporated in village meetings, household visits)
Dien Bien, 2014-2014
IR-3, CSD
8.3 Conduct communication events to promote hand washing with soap, reproductive health education and nutrition in schools integrated with school health activities and school health check-up events (in collaboration with DOET)
Dien Bien, 2014-2014
IR-3, CSD
8.4 Develop and Implement the community participation platforms of clubs without malnourished children integrated with maternal and child healthcare, immunization, nutrition, HIV/AIDS and water and child healthcare, immunization, nutrition, HIV/AIDS and water and hygienic sanitation
Dien Bien, 2014-2014
IR-3, CSD
8.5 Promote cross-learning visits within and outside the province
Dien Bien, 2014-2014
IR-3, CSD
8.6 Develop exhibition areas of hygienic latrine models
Dien Bien, 2014-2014
IR-3, CSD
9.1 Support updating NRWSS M&E system and conducting data analysis to understand inequity in sanitation and water safety
Dien Bien, 2014-2014
IR-3, CSD
9.2 Identify best practices on WASH and identify existing knowledge over low-cost sanitation options in communes/villages for documentation and dissemination
Dien Bien, 2014-2014
IR-3, CSD
9.3 Support trial of ODF verification and certification
Dien Bien, 2014-2014
IR-3, CSD
9.4 Conduct a study for application of the CLTS model for among people
Dien Bien, 2014-2014
IR-3, CSD
9.5 Organize meetings with relevant authorities to advocate for increased allocation of resources, engagement of private sector and increased loans from Social Policy Bank to promote drinking water safety, sanitation, and hand-washing as social norm
Dien Bien, 2014-2014
IR-3, CSD
9.6 Organize training and triggering on CLTS/SLTS/sanitation marketing/HWTS
Dien Bien, 2014-2014
IR-3, CSD
9.7 Support the trained masons/artisans and entrepreneurs to roll-out low-cost sanitation promotion/marketing
Dien Bien, 2014-2014
IR-3, CSD
9.8 Organize forums to facilitate interaction among private entrepreneurs, community leaders, and line department officials to help design latrine products for low income communities and promote and market existing latrine products
Dien Bien, 2014-2014
IR-3, CSD
9.9 Support regular monitoring, review meetings and cross-learning visits within and outside the province on WASH
Dien Bien, 2014-2014
IR-3, CSD
9.1 Support the organization of WASH communication sessions through interpersonal communication (village meetings, household visits) and in schools and on the occasion of GHWD
Dien Bien, 2014-2014
IR-3, CSD
9.11 Promote sustainable school WASH (SLTS) initiatives involving school and community (in collaboration with DOET).
Dien Bien, 2014-2014
IR-3, CSD
9.12 Support development of DRR/CCA planning in WASH (with technical and financial support from NCERWASS)
Dien Bien, 2015-2016
IR-4, CSD
13 Advocate, conduct supportive monitoring and supervision to ensure implementation and application of BFHI and nutrition related indicators (under new MOH quality assessment criteria); and 4 early essential newborn care interventions (active management of the third stage of labor, delay cord clamping, immediate skin to skin contact, and early initiation of breastfeeding) in provincial and all district hospitals in the province.
Dien Bien, 2015-2016
IR-4, CSD
14 Advocate, conduct supportive monitoring and supervision to ensure implementation of KMC to support under-weight and premature newborns in the provincial and district hospitals.
Dien Bien, 2015-2016
IR-4, CSD
15 Conduct training for establishment of newborn care units in districts of Dien Bien, Nam Po, Muong Nhe.
Dien Bien, 2015-2016
IR-4, CSD
16 Conduct training for ethnic minority midwives on newborn care, skill birth assistance, safe motherhood; and training on management of diarrhea and pneumonia.
Dien Bien, 2015-2016
IR-4, CSD
17 Implement neonatal mortality audit.
Dien Bien, 2015-2016
IR-4, CSD
18 Conduct integrated outreach services (ANC, postnatal care, immunization, growth monitoring and communication, IMAM) in 11 difficult communes of Muong Cha.
Dien Bien, 2015-2016
IR-4, CSD
19 Support for integrated communication in project districts which included maintaining and scaling up the "no malnourished child club" in 03 project districts of Tuan Giao, Dien Bien Dong and Muong Cha.
Dien Bien, 2015-2016
IR-4, CSD
20 Support for implementation of voluntarily counselling and testing of HIV and AIDS for pregnant women and women at reproductive age which include capacity building, communication and supportive supervision at district hospital and outpatient clinics.
Dien Bien, 2015-2016
IR-4, CSD
21 Procure HEBI for 8 communes of Muong Cha district.
Dien Bien, 2015-2016
IR-4, CSD
22 Capacity building on nutrition surveillance for local monitoring and planning (linked with national nutrition surveillance system).
Dien Bien, 2015-2016
IR-4, CSD
23 Training on implementation of the BFHI and nutrition related criteria to facilitate district hospitals to achieve them at grade 3 or beyond (new hospital quality assessment criteria.

184
Province Start and End Date
Intermediate Result
number and title
Activity #
Statement
Dien Bien, 2015-2016
IR-4, CSD
24 Replicate CLTS to 7 communes in Tua Chua district and conduct ODF verification and certification in 122 villages of 4 districts of Dien Bien, Tuan Giao, Muong Cha and Tua Chua.
Dien Bien, 2015-2016
IR-4, CSD
24.1 Organize CLTS/ODF planning and review meetings
Dien Bien, 2015-2016
IR-4, CSD
24.2 Conduct CLTS/SLTS training and triggering, trainings on low cost latrine construction and sanitation marketing and develop ring molds for latrine construction for communes
Dien Bien, 2015-2016
IR-4, CSD
24.3 Organize community mobilization and communication
Dien Bien, 2015-2016
IR-4, CSD
24.4 Organize competition on low cost, locally appropriate latrine models
Dien Bien, 2015-2016
IR-4, CSD
24.5 Verify and certify ODF villages
Dien Bien, 2015-2016
IR-4, CSD
25 Support the development and implementation of provincial scaling up sanitation and sustainable water supply post 2015 plans in communities and at school.
Dien Bien, 2015-2016
IR-4, CSD
25.1 Develop the provincial sustainable water supply plan
Dien Bien, 2015-2016
IR-4, CSD
25.2 Support establishing operation and management committees for all piped water systems
Dien Bien, 2015-2016
IR-4, CSD
25.3 Training operation and maintenance of piped water supply for members of O&M committees
Dien Bien, 2015-2016
IR-4, CSD
25.4 Conduct monitoring the performance of O&M committees
Dien Bien, 2015-2016
IR-4, CSD
26 Sustain HWTS model in Dien Bien Dong and Muong Cha districts and replicate the model to the six communes in Tua Chua district.
Dien Bien, 2015-2016
IR-4, CSD
26.1 Review HWTS results in the two districts implementing HWTS of Dien Bien Dong and Muong Cha
Dien Bien, 2015-2016
IR-4, CSD
26.2 Training on HWTS for 7 communal staff in Tua Chua district
Dien Bien, 2015-2016
IR-4, CSD
26.3 Support the communication sessions in six communes and support HWTS demonstration models
Dien Bien, 2015-2016
IR-4, CSD
26.4 Collaborate with the private sector in the production and promotion of HWTS products.
Dien Bien, 2015-2016
IR-4, CSD
27 Support annual update and report of NRWSS M&E system.
Dien Bien, 2015-2016
IR-4, CSD
28 Support implementation of the provincial/communal detailed WASH DRR/CCA plan - Apply appropriate community-base climate resilient WASH technical options.
Dong Thap , 2012-2013
IR-3, CSD
12 Provide technical and financial support to the development of the following focusing on equity, and the poor:
Dong Thap , 2012-2013
IR-3, CSD
12.1 Provincial RWSS NTP3 plans and strengthening coordination of RWSS NTP3 implementation
Dong Thap , 2012-2013
IR-3, CSD
12.2 Provincial MNCH and nutrition plan of actions under the framework of national nutrition strategy 2011-2020
Dong Thap , 2012-2013
IR-3, CSD
13 Strengthen the provincial capacity on:
Dong Thap , 2012-2013
IR-3, CSD
13.1 Providing, promoting and monitoring the use of health insurance for under-6 children by family member, child care givers, and CIP.
Dong Thap , 2012-2013
IR-3, CSD
13.2 CLTS, Hand washing with soap, household water treatment and storage and sanitation marketing and sanitation marketing WWS and sanitation marketing
Dong Thap , 2012-2013
IR-3, CSD
13.3 Model development on integrated MNCH and nutrition intervention package that includes community based and hospital based IYCF activities.
Dong Thap , 2012-2013
IR-3, CSD
13.4 Management of child illness with ARI and CDD
Dong Thap , 2012-2013
IR-3, CSD
13.5 Scaling up of new approaches (social marketing in prevention and control of micronutrient deficiencies among target women and children)
Dong Thap , 2012-2013
IR-3, CSD
13.6 Scaling up approaches and experiences for PMTCT prevention
Dong Thap , 2012-2013
IR-3, CSD
13.7 Emergency responses
Dong Thap , 2012-2013
IR-3, CSD
14 Support for M&E, MNCH and RWSS data collection
Dong Thap , 2012-2013
IR-3, CSD
15 Support conduct of formative research and development/implementation of C4D integrated model to address behavioral and social change determinants on MNCH, Nutrition (focusing on IYCF/exclusive breastfeeding) and Hand washing with soap in targeted areas
Dong Thap , 2014-2014
IR-3, CSD
7.1 Support reviewing of the latest provincial MNCH-Nutrition profile, bottle neck analysis and co-ordination works in implementation of the provincial integrated action plan on reduction of child stunting (2013-2016) for corrective action addressing disparities.
Dong Thap , 2014-2014
IR-3, CSD
7.2 Assessment on the implementation of the free health care policy for children under 6 (in selective district) and planning meeting for improvement of the situation
Dong Thap , 2014-2014
IR-3, CSD
7.3 Support to strengthening the quality of IYCF indicators under the provincial Nutrition Surveillance frame work to inform an equity approach.
Dong Thap , 2014-2014
IR-3, CSD
7.4 Support to a 03 days training workshop on strengthening quality of routine data and reporting, and application of the data for equity focused planning (including MNCH, nutrition, EPI, HIV, WASH and communication
Dong Thap , 2014-2014
IR-3, CSD
7.5 Support application of new MOH's assessment criteria of hospitals (with focus on the 10 steps of the BFHI in 03 district hospitals and IYCF counseling)
Dong Thap , 2014-2014
IR-3, CSD
7.6 Support quarterly and project year-end review for implementation of CSD component
Dong Thap , 2014-2014
IR-3, CSD
7.7 Support data collection to fulfill the Annual WASH Data Base for the three new districts (TH, HN, Tahj ax Hong Ngu)
Dong Thap , 2014-2014
IR-3, CSD
7.8 Support TOT & training for capacity building in emergent/ new issues
Dong Thap , 2014-2014
IR-3, CSD
7.8.1 Early identification of ARI among infant & young children
Dong Thap , 2014-2014
IR-3, CSD
7.8.2 PMTCT(focus on increase VCT coverage)
Dong Thap , 2014-2014
IR-3, CSD
7.8.3 Integrated child health nutrition care
Dong Thap , 2014-2014
IR-3, CSD
7.8.4 Management of Immunization activities
Dong Thap , 2014-2014
IR-3, CSD
7.8.5 Water storage and treatment (in the three new districts)
Dong Thap , 2014-2014
IR-3, CSD
7.9 Support quarterly integrated monitoring of the programme activity on MNCH, nutrition, WASH and C4D
Dong Thap , 2014-2014
IR-3, CSD
7.1 Support the co-ordination meetings and field supervision on social marketing of iron folic supplementation in 05 districts

185
Province Start and End Date
Intermediate Result
number and title
Activity #
Statement
Dong Thap , 2014-2014
IR-3, CSD
7.11 Organize an exchange visit for experience sharing on model development and other MNCH-nutrition interventions
Dong Thap , 2014-2014
IR-3, CSD
8.1 Support implementation of periodic communication activities via local radio and TV (using the provincial health TV programme with focus on Iron folic and anemia, IYCF, New born care at home, hand washing with soap
Dong Thap , 2014-2014
IR-3, CSD
8.2 Support implementation of the media campaign on special occasions (children day & free health care, micro-nutrient days, WBW, and washing days)
Dong Thap , 2014-2014
IR-3, CSD
9.1 Support updating NRWSS M&E system and conducting data analysis to understand inequity in sanitation and water safety
Dong Thap , 2014-2014
IR-3, CSD
9.2 Identify best practices on WASH in communes/villages for documentation and dissemination
Dong Thap , 2014-2014
IR-3, CSD
9.3 Support trial of ODF verification and certification
Dong Thap , 2014-2014
IR-3, CSD
9.4 Organize training and triggering on CLTS/SLTS/sanitation marketing/HWTS
Dong Thap , 2014-2014
IR-3, CSD
9.5 Support trained masons/artisans and entrepreneurs to carry out low-cost sanitation promotion/marketing
Dong Thap , 2014-2014
IR-3, CSD
9.6 Organize forums to facilitate interaction among private entrepreneurs, community leaders, and line department officials to help design products for low income communities and promote and market existing products
Dong Thap , 2014-2014
IR-3, CSD
9.7 Support regular monitoring, review meetings and cross-learning visits within and outside the province on WASH
Dong Thap , 2014-2014
IR-3, CSD
9.8 Support to organize WASH communication sessions through interpersonal communication (village meetings, household visits) in schools and on the occasion of GHWD.
Dong Thap , 2014-2014
IR-3, CSD
9.9 Promote sustainable school WASH involving school and community
Dong Thap , 2014-2014
IR-3, CSD
9.1 Support development of DRR/CCA planning in WASH (with technical and financial support from NCERWASS)
Dong Thap , 2015-2016
IR-4, CSD
12 Support for capacity development for health workers on new nutrition and new born care practices:
Dong Thap , 2015-2016
IR-4, CSD
12.1 Integrated training on BFHI and new born care practices (KCM and 4 new practices)
Dong Thap , 2015-2016
IR-4, CSD
12.2 Organize exchange visits on the topics
Dong Thap , 2015-2016
IR-4, CSD
13 Support monitoring/supervision to provincial, district hospitals on nutrition related services (under new hospital quality assessment criteria newly issued by MOH); and support implementation of $ early essential new-boor care interventions (active management of the third stage of labor, delay cord clamping, immediate skin to skin contact, and early initiation of breastfeeding).
Dong Thap , 2015-2016
IR-4, CSD
14 Capacity development for scaling up of iron folic interventions among pregnant, none pregnant women, and female workers using social marketing approach in new locations of Dong Thao, including selective private factories.
Dong Thap , 2015-2016
IR-4, CSD
14.1 Support training for new health workers on social marketing
Dong Thap , 2015-2016
IR-4, CSD
14.2 Support bi-annual monitoring and review meeting on social marketing.
Dong Thap , 2015-2016
IR-4, CSD
15 Support integrated communication activities focusing on BF, iron folic supplementations for targeted women
Dong Thap , 2015-2016
IR-4, CSD
16 Conduct a review meeting on implementation of provincial Plan of action on MNCH-Nutrition for reduction of Child Stunting period 2013-2016, and formulation of a new Action Plan for 2017-2010
Dong Thap , 2015-2016
IR-4, CSD
17 Support DOH to conduct biannual programme meeting on implementation of the CSD component
Dong Thap , 2015-2016
IR-4, CSD
18 Maintaining CLTS in Tan Hong and Hong Ngu districts and verify and certify 4 ODF villages in Hong Ngu district:
Dong Thap , 2015-2016
IR-4, CSD
18.1 Organize CLTS and SLTS training and triggering, training on low-cost latrine construction, sanitation marketing
Dong Thap , 2015-2016
IR-4, CSD
18.2 Community mobilization activities such as village meeting, household visits, radio, sanitation festivals, school activities
Dong Thap , 2015-2016
IR-4, CSD
18.3 Conduct regular monitoring, review meetings and study visits to best WASH practices in and outside the province
Dong Thap , 2015-2016
IR-4, CSD
18.4 Verify and certify ODF villages
Dong Thap , 2015-2016
IR-4, CSD
19 Develop and Implement post 2015 provincial WASH plan, focusing scaling up of sanitation and sustainability of WASH facilities in communities and at school.
Dong Thap , 2015-2016
IR-4, CSD
19.1 Training workshop on planning development
Dong Thap , 2015-2016
IR-4, CSD
19.2 Review the current O&M status and O&M models
Dong Thap , 2015-2016
IR-4, CSD
19.3 Training on O&M for care takers
Dong Thap , 2015-2016
IR-4, CSD
19.4 Organize a workshop to share O&M experience
Dong Thap , 2015-2016
IR-4, CSD
20 Maintain household water treatment and storage in Hong Ngu and Tan Hong district:
Dong Thap , 2015-2016
IR-4, CSD
20.1 Training on HWTS and construction of low-cost HWTS options
Dong Thap , 2015-2016
IR-4, CSD
20.2 Organize community mobilization activities (household visits, village meetings, communication materials..)
Dong Thap , 2015-2016
IR-4, CSD
20.3 Support field water quality testing
Dong Thap , 2015-2016
IR-4, CSD
20.4 Demonstrate HWTS options in bordering communes, applying PPP.
Dong Thap , 2015-2016
IR-4, CSD
20.5 Monitor project activities especially the HWTS communication activities and study visits to best practices
Dong Thap , 2015-2016
IR-4, CSD
21 Update NRWSS M&E system
Dong Thap , 2015-2016
IR-4, CSD
22 Support implementation of provincial/ communal detailed WASH DRR/CCA plan
Gai Lai, 2012-2013
IR-3, CSD
13 Provide technical and financial support to the development of the provincial action plan, focusing on equity, ethnic minority and the poor:
Gai Lai, 2012-2013
IR-3, CSD
13.1 Provincial RWSS NTP3 plans and strengthening coordination of RWSS NTP3 implementation
Gai Lai, 2012-2013
IR-3, CSD
13.2 Integrated MNCH and nutrition plan of action
Gai Lai, 2012-2013
IR-3, CSD
14 Strengthen the provincial capacity on:
Gai Lai, 2012-2013
IR-3, CSD
14.1 MNCH

186
Province Start and End Date
Intermediate Result
number and title
Activity #
Statement
Gai Lai, 2012-2013
IR-3, CSD
14.2 Integrated management of acute malnutrition (IMAM)
Gai Lai, 2012-2013
IR-3, CSD
14.3 CLTS, sanitation marketing, Hand washing with soap and household water treatment and storage
Gai Lai, 2012-2013
IR-3, CSD
15 Support for data collection and M&E in MNCH, implementation of stunting reduction strategy and implementation of RWSS NTP3.
Gai Lai, 2012-2013
IR-3, CSD
16 Support conduct of formative research and development/implementation of C4D integrated model to address behavioral and social change determinants on MNCH, Nutrition (focusing on IYCF/exclusive breastfeeding) and Hand washing with soap in targeted areas
Gai Lai, 2014-2014
IR-3, CSD
6.1 Develop a provincial analysis and report on maternal and child health data for equity improvement in investment (maternal mortality verification and use of SITAN data included)
Gai Lai, 2014-2014
IR-3, CSD
6.2 Conduct a survey on people's satisfaction to healthcare services (CRS)(social audit). This activity will be arrived out in conjunction with activity 2.1
Gai Lai, 2014-2014
IR-3, CSD
6.3 Organize a provincial workshop on social health insurance to advocate for universal health coverage and provision of acid folic and essential medicine for pregnant women and children
Gai Lai, 2014-2014
IR-3, CSD
6.4 Review the latest MNCH-nutrition profile and the co-ordination mechanism of the implementation of the provincial Plan of action 2013-2016 on integrated MNCH-Nutrition for reduction of child stunting
Gai Lai, 2014-2014
IR-3, CSD
6.5 Purchase Hebi product for IMAM and support implementation and monitoring of IMAM in Krong Pa at province, district, commune and village levels.
Gai Lai, 2014-2014
IR-3, CSD
6.6 Support application of the new National Assessment Criteria for hospitals
Gai Lai, 2014-2014
IR-3, CSD
6.7 Support capacity development on diarrhea and pneumonia control, and on deliver skills for hamlet midwifes and/or traditional birth attendance
Gai Lai, 2014-2014
IR-3, CSD
6.8 Support outreach activities such as pregnancy check-up, immunization and health communication for remote communes and villages of Kobang and Krong Pa Districts
Gai Lai, 2014-2014
IR-3, CSD
6.9 Support sustainable elimination of birth tetanus in K'Bang and Krong Pa Districts
Gai Lai, 2014-2014
IR-3, CSD
6.1 Support integrated monitoring of maternal and child health care
Gai Lai, 2014-2014
IR-3, CSD
7.1 Support community-based integrated communication on IMAM, MNCH, HWTS and HWWS through communication sessions and household visits by community health workers.
Gai Lai, 2014-2014
IR-3, CSD
7.2 Support integrated communication on IMAM, MNCH, HWTS and HWWS for pregnant women and lactating mothers at local health centres through consultations and availability of communication materials
Gai Lai, 2014-2014
IR-3, CSD
7.3 Support integrated communication on nutrition and sanitation, and hygiene in schools through extra-curriculum hygiene promotion activities and events
Gai Lai, 2014-2014
IR-3, CSD
7.4 Support application of the community-based C4D model on IYCF promotion (replicated with adaption from An Giang province)
Gai Lai, 2014-2014
IR-3, CSD
8.1 Support an updating of the NRWSS M&E system and conduct data analysis to understand inequity in sanitation and water safety
Gai Lai, 2014-2014
IR-3, CSD
8.2 Identify best practices on WASH in communes/villages for documentation and dissemination
Gai Lai, 2014-2014
IR-3, CSD
8.3 Organize training and triggering on CLTS/SLTS/sanitation marketing/HWTS
Gai Lai, 2014-2014
IR-3, CSD
8.4 Support trained masons/artisans and entrepreneurs to carry out low-cost sanitation promotion/marketing
Gai Lai, 2014-2014
IR-3, CSD
8.5 Organize forums to facilitate interaction among private entrepreneurs, community leaders, and line department officials to help design water and sanitation related products for low income communities and marketing local low cost products
Gai Lai, 2014-2014
IR-3, CSD
8.6 Support regular monitoring, review meetings and cross-learning visits within and outside the province on WASH
Gai Lai, 2014-2014
IR-3, CSD
8.7 Support the organization of WASH communication sessions through interpersonal communication (village meetings, household visits) and in schools and on the occasion of GHWD
Gai Lai, 2014-2014
IR-3, CSD
8.8 Promote sustainable school WASH interventions involving schools and communities
Gai Lai, 2014-2014
IR-3, CSD
8.9 Support the development of DRR/CCA planning in WASH (with technical and financial support from NCERWASS)
Gai Lai, 2015-2016
IR-4, CSD
12 Support application of BFHI and nutrition related indicators (under new MOH quality assessment criteria); key essential newborn care interventions (active management of the third stage of labor, delay cord clamping, immediate skin to skin contact, and early initiation of breast feeding) in provincial and all district hospitals
Gai Lai, 2015-2016
IR-4, CSD
12.1 Support integrated monitoring/supervision of new practices
Gai Lai, 2015-2016
IR-4, CSD
12.2 Support training for capacity building of new practices
Gai Lai, 2015-2016
IR-4, CSD
13 Support to increase coverage of pregnant women and women at reproductive age receiving TT vaccination in the high risk districts of Gia Lai:
Gai Lai, 2015-2016
IR-4, CSD
13.1 Identify all women at child bearing age, who need TT vaccination;
Gai Lai, 2015-2016
IR-4, CSD
13.2 Organize village meetings to raise awareness of importance of TT vaccination among women at child bearing age;
Gai Lai, 2015-2016
IR-4, CSD
13.3 Organize meetings with people committees of district and commune for their support to TT vaccination;
Gai Lai, 2015-2016
IR-4, CSD
13.4 Support outreach vaccination
Gai Lai, 2015-2016
IR-4, CSD
14 conduct training on maternal mortality audit for provincial health workers
Gai Lai, 2015-2016
IR-4, CSD
15 Capacity building on nutrition surveillance for local monitoring and planning (linked with national nutrition surveillance system).
Gai Lai, 2015-2016
IR-4, CSD
16 Support transmission of IMAM services to be under support of national nutrition programme:
Gai Lai, 2015-2016
IR-4, CSD
16.1 Support integrated monitoring of Health and IMAM at community base and IMAM inpatient in hospitals (provincial and Kronpa);
Gai Lai, 2015-2016
IR-4, CSD
16.2 Purchase Hebi product for maintaining
Gai Lai, 2015-2016
IR-4, CSD
17 Organize School Sanitation Day for 03 lower secondary schools with EM children in K'Bang, Krong Pa and Kong Chro
Gai Lai, 2015-2016
IR-4, CSD
18 Organize orientation workshop on CLTS and ODF for provincial, district and commune leaders (both communes with on-going and future implementation of CLTS, and Social Policy Bank:
Gai Lai, 2015-2016
IR-4, CSD
18.1 Organize orientation workshop on CLTS and ODF
Gai Lai, 2015-2016
IR-4, CSD
18.2 Work with Social Policy Bank for increasing number of loans for household latrines
Gai Lai, 2015-2016
IR-4, CSD
19 Conduct ODF verification and certification in 5 communes K'Bang district
Gai Lai, 2015-2016
IR-4, CSD
19.1 Conduct training on sanitation mapping and ODF procedures in selected villages

187
Province Start and End Date
Intermediate Result
number and title
Activity #
Statement
Gai Lai, 2015-2016
IR-4, CSD
19.2 Organize meetings to classify households and undertake sanitation mapping
Gai Lai, 2015-2016
IR-4, CSD
19.3 Verify and certify ODF villages
Gai Lai, 2015-2016
IR-4, CSD
19.4 Develop a Video clip on ODF to be broadcasted in provincial, and district TV.
Gai Lai, 2015-2016
IR-4, CSD
19.5 Conduct community mobilization on ODF, combined with hand washing soap (HWWS).
Gai Lai, 2015-2016
IR-4, CSD
19.6 Organize ODF certification ceremonies;
Gai Lai, 2015-2016
IR-4, CSD
19.7 Organize forums for introduction of low cost latrine options and marketing of existing products
Gai Lai, 2015-2016
IR-4, CSD
20 Implement CLTS model in two more communes in the districts og K'Bang in 2016:
Gai Lai, 2015-2016
IR-4, CSD
20.1 Conduct training for commune staff, motivators and teachers on CLTS, SLTS
Gai Lai, 2015-2016
IR-4, CSD
20.2 Conduct survey and triggering of CLTS, SLTS
Gai Lai, 2015-2016
IR-4, CSD
20.3 Organize training on low-cost latrine construction and sanitation marketing
Gai Lai, 2015-2016
IR-4, CSD
20.4 Organize community mobilization activities, combined with HWWS
Gai Lai, 2015-2016
IR-4, CSD
20.4 Organize meetings with the Bank for Social Policies to increase loans for latrine construction
Gai Lai, 2015-2016
IR-4, CSD
21 Develop post 2015 provincial WASH plan, focusing sustainability of WASH facilities.
Gai Lai, 2015-2016
IR-4, CSD
22 Maintain HWTS K'Bang District and expand it to 3 communes of the District of Kong Chro:
Gai Lai, 2015-2016
IR-4, CSD
22.1 Organize training on HWTS combined with HWWS
Gai Lai, 2015-2016
IR-4, CSD
22.2 Support communication activates such as village meetings, household visits, mass media communication on HWTS combined with HWWS
Gai Lai, 2015-2016
IR-4, CSD
22.3 Support survey, monitoring, evaluation of HWTS combined with HWWS.
Gai Lai, 2015-2016
IR-4, CSD
22.4 Pilot a model on private sector involvement in HWTS, supporting promotion of the use of Cambodian ceramic pot filters
Gai Lai, 2015-2016
IR-4, CSD
23 Support development and approval of provincial WASH DRR/CCA plan
Gai Lai, 2015-2016
IR-4, CSD
24 Based on the CSD KAP study 2014, implement integrated C4D activities in the area of Nutrition (EBF), MNCH (immunization) and Water and Sanitation
Gai Lai, 2015-2016
IR-4, CSD
25 M&E and documentation of C4D interventions and practices
Gai Lai, 2015-2016
IR-4, CSD
26 Capacity development for C4D officials and community health workers
Gai Lai, 2015-2016
IR-4, CSD
27 Organize a workshop to disseminate the model of EBF mother support Group for other non-project districts of Gia Lai
Kon Tum, 2012-2013
IR-3, CSD
13 Provide policy advice and technical support for development of:
Kon Tum, 2012-2013
IR-3, CSD
13.1 Provincial RWSS NTP3 plan of 2012-2016
Kon Tum, 2012-2013
IR-3, CSD
13.2 Provincial MNCH and nutrition plan of actions under the framework of national nutrition strategy 2011-2020
Kon Tum, 2012-2013
IR-3, CSD
13.3 PMTCT and NTP for HIV/AIDS plans, focusing on equity, ethnic minority and the poor
Kon Tum, 2012-2013
IR-3, CSD
14 Support for implementation of:
Kon Tum, 2012-2013
IR-3, CSD
14.1 Micro-planning approach (RED) for increase coverage of minimum MNCH and nutrition interventions in a hard to reach areas
Kon Tum, 2012-2013
IR-3, CSD
14.2 CLTS and HWWS, sanitation marketing
Kon Tum, 2012-2013
IR-3, CSD
14.3 PMTCT and NTP for HIV/AIDS plans
Kon Tum, 2012-2013
IR-3, CSD
14.4 Integrated management of acute malnutrition (IMAM)
Kon Tum, 2012-2013
IR-3, CSD
14.5 Household water treatment and storage (HWTS) to provide minimum service packages to women and children of ethnic minorities in hard to reach areas
Kon Tum, 2012-2013
IR-3, CSD
15 Support for data collection and co-ordination the implementation of MNCH-Nutrition package including PMTCT care, IMAM, and RWSS NTP3, and emergency responses
Kon Tum, 2012-2013
IR-3, CSD
16 Support promotion of breast feeding and IYCF practices among local health care network that includes strengthening hospital and health clinic based BFHI
Kon Tum, 2012-2013
IR-3, CSD
17 Conduct a cross-sectoral base-line evaluation on CSD, CP and SPG
Kon Tum, 2012-2013
IR-3, CSD
18 Support conduct of formative research and development/implementation of C4D integrated model to address behavioral and social change determinants on MNCH, Nutrition (focusing on IYCF/exclusive breastfeeding) and Hand washing with soap in targeted areas
Kon Tum, 2014-2014
IR-3, CSD
7.1 Review the latest MNCH-nutrition profile (including EPI), and status of implementation & coordination for implementation of the provincial MNCH-Nutrition Action for equity focus and action
Kon Tum, 2014-2014
IR-3, CSD
7.2 Develop a provincial analysis on equal access to immunization and maternal and child health interventions
Kon Tum, 2014-2014
IR-3, CSD
7.3 Conduct supervision of IMAM services at district, commune and village levels including consolidation and review of performance indicators and on the job training when required
Kon Tum, 2014-2014
IR-3, CSD
7.4 Support for interim purchasing of the RUFT/Hebi product until a sustainable national or provincial funding mechanism has been established
Kon Tum, 2014-2014
IR-3, CSD
7.5 Modelling of growth- watch for tracking of malnutrition using cell phone technology, and programme output monitoring applying Web based system
Kon Tum, 2014-2014
IR-3, CSD
7.6 Conduct training in IYCF for nutrition collaborators in Tu Mo Rong and Kon Ray dsitrict
Kon Tum, 2014-2014
IR-3, CSD
7.7 Support application of new National Quality Assessment Criteria for Hospitals to guide nationwide expansion, with focus on standards for Baby Friendly Hospital in selective districts
Kon Tum, 2014-2014
IR-3, CSD
7.8 Conduct integrated outreach services (pregnancy check-up, post natal visits, immunization, child growth monitoring, and C4D) in difficult communes
Kon Tum, 2014-2014
IR-3, CSD
7.9 Organize a provincial workshop on social health insurance to advocate for universal health coverage and provision of acid folic and essential medicine for pregnant women and children

188
Province Start and End Date
Intermediate Result
number and title
Activity #
Statement
Kon Tum, 2014-2014
IR-3, CSD
7.1 Organize workshop on equity in access to immunization and maternal and child healthcare interventions
Kon Tum, 2014-2014
IR-3, CSD
7.11 Conduct integrated monitoring and supervision on reproductive health/safe motherhood, skilled birth assistance, nutrition, IMAM, BFHI in provincial and district hospital and commune health centers
Kon Tum, 2014-2014
IR-3, CSD
7.12 Develop demand and supply chain assessment for introduction of social marketing and building public-private partnership for promotion of iron folic supplementation for anemia control among women
Kon Tum, 2014-2014
IR-3, CSD
7.13 Conduct training for provincial, district and commune health staff in data collection, analyses, and utilization for planning and monitoring programmes/interventions on reproduction health, safe motherhood, child health, immunization, nutrition and water and hygienic sanitation
Kon Tum, 2014-2014
IR-3, CSD
7.14 Conduct training in immunization for district and commune health staff in difficult communes for implementation of Decision 3029 by MOH
Kon Tum, 2014-2014
IR-3, CSD
7.15 Support for roll out of KMC in provincial and district hospitals
Kon Tum, 2014-2014
IR-3, CSD
7.16 Support a social audit on people's satisfaction to healthcare services (CRS) in collaboration with SPG and provincial DPI
Kon Tum, 2014-2014
IR-3, CSD
8.1 Support developing provincial behavioral change communication action plans on flagships areas(hand-washing & drinking water, diarrheal and pneumonia management; anemia prevention, IYCF, health insurance for children under 6
Kon Tum, 2014-2014
IR-3, CSD
8.2 Organize meetings with old people/village heads (gia lang) and religious leaders in commune with ethnic minorities to advocate on family planning, safe motherhood, child healthcare, nutrition and water and hygienic sanitation
Kon Tum, 2014-2014
IR-3, CSD
8.3 Conduct integrated BCC at community level on family planning, safe motherhood, child healthcare, immunization, nutrition, and water and hygienic sanitation, and HIV/AIDS incorporated in village meetings, household visits
Kon Tum, 2014-2014
IR-3, CSD
8.4 Conduct communication events in schools with participation of children to promote hand washing with soap to support GHWD in selected communes
Kon Tum, 2014-2014
IR-3, CSD
8.5 Maintain and scale up the community participation platforms of "clubs without malnourished children" integrated with maternal and child healthcare, immunization, nutrition, and water and hygienic sanitation in communes of Tu Mo Rong district
Kon Tum, 2014-2014
IR-3, CSD
9.1 Support updating NRWSS M&E system and conducting data analysis to understand inequity in sanitation and water safety
Kon Tum, 2014-2014
IR-3, CSD
9.2 Identify best practices on WASH in communes/villages for documentation and dissemination
Kon Tum, 2014-2014
IR-3, CSD
9.3 Support trial of ODF verification and certification
Kon Tum, 2014-2014
IR-3, CSD
9.4 Conduct study for application of CLTS model for EM people
Kon Tum, 2014-2014
IR-3, CSD
9.5 Organize meetings with relevant authorities for increased allocation of resources, engagement of private sector and increased loans from Social Policy Bank to promote drinking water safety, sanitation, and hand-washing as social norm
Kon Tum, 2014-2014
IR-3, CSD
9.6 Organize training and triggering on CLTS/SLTS/sanitation marketing/HWTS
Kon Tum, 2014-2014
IR-3, CSD
9.7 Develop trained masons/artisans and entrepreneurs to support low-cost sanitation promotion /marketing
Kon Tum, 2014-2014
IR-3, CSD
9.8 Organize forums to facilitate interaction among private entrepreneurs, community leaders, and line department officials- to help design latrine products for low-income communities and market existing latrine products
Kon Tum, 2014-2014
IR-3, CSD
9.9 Support regular monitoring, review meetings and cross-learning visits within and outside the province on WASH
Kon Tum, 2014-2014
IR-3, CSD
9.1 Support to organize WASH communication sessions through interpersonal communication (village meetings, household visits) in schools and on the occasion of GHWD.
Kon Tum, 2014-2014
IR-3, CSD
9.11 Promote sustainable schools WASH involving school and community
Kon Tum, 2014-2014
IR-3, CSD
9.12 Support to development of DRR/CCA planning in WASH (with technical and financial support from NCERWASS)
Kon Tum, 2015-2016
IR-4, CSD
16 Advocate, conduct supportive monitoring and supervision to ensure implementation and application of BFHI and nutrition related indicators (under new MOH quality assessment criteria); and 4 early essential newborn care interventions (active management of third stage of labor, delay cord clamping, immediate skin to skin contact, and early initiation of breastfeeding) in provincial and all district hospitals in the province.
Kon Tum, 2015-2016
IR-4, CSD
17 Advocate, conduct supportive monitoring and supervision to ensure implementation of KMC to support under-weight and premature newborns in the provincial and district hospitals.
Kon Tum, 2015-2016
IR-4, CSD
18 Conduct KMC training for provincial and district health staff.
Kon Tum, 2015-2016
IR-4, CSD
19 Conduct integrated outreach services (ANC, postnatal care, immunization, growth monitoring and communication) in difficult communes of Tu Mo Rong district.
Kon Tum, 2015-2016
IR-4, CSD
20 Capacity building on nutrition surveillance for local monitoring and planning (linked with national nutrition surveillance system).
Kon Tum, 2015-2016
IR-4, CSD
21 Support for integrated communication in project districts which included maintaining and scaling up the "no malnourished child club" in project communes districts.
Kon Tum, 2015-2016
IR-4, CSD
22 Procure HEBI for 03 districts implementing IMAM.
Kon Tum, 2015-2016
IR-4, CSD
23 Provide supportive supervision on IMAM implementation from provincial to district and commune levels.
Kon Tum, 2015-2016
IR-4, CSD
24 Conduct additional training on IMAM for healthcare workers (by provincial trainers).
Kon Tum, 2015-2016
IR-4, CSD
25 Support training activity on BFHI practices and nutrition related indicators to facilitate the hospital to achieve them at grade 3 or beyond (new MOH quality assessment criteria).
Kon Tum, 2015-2016
IR-4, CSD
26 Replicate CLTS to 4 communes in Dak Ha district and Support ODF verification and certification in Tu Mo Rang and Dak Ha districts:
Kon Tum, 2015-2016
IR-4, CSD
26.1 Organize CLTS/ODF planning meeting, including reviewing and classifying groups of villages/populations according to their latrine coverage
Kon Tum, 2015-2016
IR-4, CSD
26.2 Conduct CLTS/SLTS training and triggering, trainings on low cost latrine construction and sanitation marketing and develop ring molds for latrine construction for communes
Kon Tum, 2015-2016
IR-4, CSD
26.3 Organize forums for introduction of low cost latrine options and marketing of existing products
Kon Tum, 2015-2016
IR-4, CSD
26.4 Organize community mobilization on CLTS/ODF and regular monitoring, review meeting and study visits to best practices
Kon Tum, 2015-2016
IR-4, CSD
26.5 Verify and certify ODF villages
Kon Tum, 2015-2016
IR-4, CSD
27 Support development and implementation of post 2015 provincial WASH plans, focusing on scaling up sanitation and sustainability of WASH facilities in communities and at school.
Kon Tum, 2015-2016
IR-4, CSD
27.1 Develop provincial WASH sustainable plans 2016-2020 for water supply, sanitation in community and at school.
Kon Tum, 2015-2016
IR-4, CSD
27.2 Organize review meeting on O&M of community-managed water supply projects
Kon Tum, 2015-2016
IR-4, CSD
27.3 Capacity building training for 172 staff working on O&M of centralized water supply owned by communities in 86 communes (6 training courses) at district level
Kon Tum, 2015-2016
IR-4, CSD
27.4 Building a model of community-managed, simple and sustainable piped water supply system
Kon Tum, 2015-2016
IR-4, CSD
28 Maintain HWTS in 3 communes of Tu Mo Rong district and 3 communes of Dak Ha district.

189
Province Start and End Date
Intermediate Result
number and title
Activity #
Statement
Kon Tum, 2015-2016
IR-4, CSD
28.1 Support communication sessions in villages on HWTS
Kon Tum, 2015-2016
IR-4, CSD
28.2 Support for routine monitoring of HWTS and study visits to HWTS best practices
Kon Tum, 2015-2016
IR-4, CSD
28.3 Pilot a model on private sector involvement in HWTS, supporting promotion of the use of Cambodian ceramic pot filters
Kon Tum, 2015-2016
IR-4, CSD
29 Support updating NRWSS M&E system.
Kon Tum, 2015-2016
IR-4, CSD
30 Support implementation of provincial/ communal detailed WASH DRR/CCA plan
Lao Cai, 2012-2013
IR-3, CSD
13 Provide policy advice and technical support for development of:
Lao Cai, 2012-2013
IR-3, CSD
13.1 Provincial integrated action plan on nutrition & MNCH (focusing on most disadvantaged pregnant women and children)
Lao Cai, 2012-2013
IR-3, CSD
13.2 Provincial RWSS NTP3 2013-2014, focusing on equity, poor ethnic minority and venerable groups
Lao Cai, 2012-2013
IR-3, CSD
14 Support for promotion of:
Lao Cai, 2012-2013
IR-3, CSD
14.1 Integrated package of MNCH and Nutrition, including PMTCT VCT
Lao Cai, 2012-2013
IR-3, CSD
14.2 Skilled birth assistance
Lao Cai, 2012-2013
IR-3, CSD
14.3 CLTS and HWWS, sanitation marketing
Lao Cai, 2012-2013
IR-3, CSD
14.4 Breastfeeding and IYCF practice including strengthening BFHI standard and community based activities
Lao Cai, 2012-2013
IR-3, CSD
14.5 Integrated management of acute malnutrition (IMAM)
Lao Cai, 2012-2013
IR-3, CSD
15 Support for MNCH, Health insurance for children under 6, NRWSS data collection and M&E
Lao Cai, 2012-2013
IR-3, CSD
16 Support development of C4D integrated model and formative research to address behavioral and social change determinants to address MNCH, nutrition, sanitation and HWWS in selected areas
Lao Cai, 2014-2014
IR-3, CSD
7.1 Review of latest provincial MNCH-Nutrition profile (including EPI), and status of implementation & coordination for implementation of the provincial MNCH-Nutrition Action for equity focus and action.
Lao Cai, 2014-2014
IR-3, CSD
7.2 Support data collection, analysis and use of data for a more equity focuses planning (EPI, MNCH, Nutrition)
Lao Cai, 2014-2014
IR-3, CSD
7.2.1 Support EPI/MNCH data collection by local team
Lao Cai, 2014-2014
IR-3, CSD
7.2.2 Support data analysis
Lao Cai, 2014-2014
IR-3, CSD
7.2.3 Support the delivery of minimum MNCH, nutrition, to the most disadvantage locations
Lao Cai, 2014-2014
IR-3, CSD
7.3 Systematic training on emergent and high impact interventions:
Lao Cai, 2014-2014
IR-3, CSD
7.3.1 Management of EPI information
Lao Cai, 2014-2014
IR-3, CSD
7.3.2 Health information system and the use of data for equity planning (MNCH- nutrition-EPI)
Lao Cai, 2014-2014
IR-3, CSD
7.3.3 Training to introduce CLTS model in schools and communities, and on social marketing for hygiene and sanitation for new districts.
Lao Cai, 2014-2014
IR-3, CSD
7.3.4 Building hygienic latrines
Lao Cai, 2014-2014
IR-3, CSD
7.3.5 PMTCT
Lao Cai, 2014-2014
IR-3, CSD
7.4 Support integrated monitoring of the programme activities, and specific monitoring/supervision works in MNCH-nutrition: WASH; Safety EPI; Safe motherhood
Lao Cai, 2014-2014
IR-3, CSD
7.5 Support the Preventive Health Centre in improving data collection and analysis; application of Growth Watch using Cell phone technology to track child malnutrition and programme output monitoring, and applying a web based system in collaboration with NIN at national level
Lao Cai, 2014-2014
IR-3, CSD
7.6 Support maintaining IMAM in Bac Ha district including purchasing Hebe product, and supervisory monitoring at province, district, commune and village levels
Lao Cai, 2014-2014
IR-3, CSD
7.7 Support application of the MOH new assessment criteria for hospital practice with focus on the 10 steps BFHI to promote BF counseling
Lao Cai, 2014-2014
IR-3, CSD
7.8 Support quarterly CSD component; implementation review meetings, and a meeting for orientation of 2015 plan of the Health nutrition, and WASH components
Lao Cai, 2014-2014
IR-3, CSD
7.9 Model development in IYCF with focus on changing social practices in child feeding conducted in 2 selective communes
Lao Cai, 2014-2014
IR-3, CSD
8.1 Support developing provincial behavioral change communication action plans on hand-washing & drinking water, diarrheal and pneumonia management
Lao Cai, 2014-2014
IR-3, CSD
8.2 Support to organize Wash/Nutrition/MCH communication sessions through interpersonal communication (village meetings, household visits) counselling activities in schools
Lao Cai, 2014-2014
IR-3, CSD
8.3 Training on communication for the communication network
Lao Cai, 2014-2014
IR-3, CSD
8.3.1 Integration in communication
Lao Cai, 2014-2014
IR-3, CSD
8.3.2 Communication skills
Lao Cai, 2014-2014
IR-3, CSD
8.3.3 Monitoring of communication
Lao Cai, 2014-2014
IR-3, CSD
8.4 Conduct communication activities via local media to synchronize the key message during national campaigns on MNCH, nutrition, WASH key topics
Lao Cai, 2014-2014
IR-3, CSD
8.5 Support to conducting direct communication sessions at local cultural events (Market days) in the high land using video film and media equipment.
Lao Cai, 2014-2014
IR-3, CSD
8.6 Conduct festival communication on hand washing day in the 4 selective primary schools belonging to the 4 selective project communes.
Lao Cai, 2014-2014
IR-3, CSD
9.1 Support updating NRWSS M&E system and conducting data analysis to understand inequity in sanitation and water safety
Lao Cai, 2014-2014
IR-3, CSD
9.2 Identify best practices on WASH in communes/villages for documentation and dissemination
Lao Cai, 2014-2014
IR-3, CSD
9.3 Support trial of ODF verification and certification
Lao Cai, 2014-2014
IR-3, CSD
9.4 Organize training and triggering on CLTS/SLTS/sanitation marketing/HWTS

190
Province Start and End Date
Intermediate Result
number and title
Activity #
Statement
Lao Cai, 2014-2014
IR-3, CSD
9.5 Support the trained masons/artisans and entrepreneurs to roll-out low-cost sanitation promotion/marketing
Lao Cai, 2014-2014
IR-3, CSD
9.6 Organize forums to facilitate interaction among private entrepreneurs, community leaders, and line department officials- to help design latrine products for low-income communities and market existing products
Lao Cai, 2014-2014
IR-3, CSD
9.7 Support regular monitoring, review meetings and cross-learning visits within and outside the province on WASH
Lao Cai, 2014-2014
IR-3, CSD
9.8 Support to organize WASH communication sessions through interpersonal communication (village meetings, household visits) in schools and on the occasion of GHWD.
Lao Cai, 2014-2014
IR-3, CSD
9.9 Promote sustainable schools WASH involving school and community
Lao Cai, 2014-2014
IR-3, CSD
9.1 Support development of DRR/CCA planning in WASH (with technical and financial support from NCERWASS)
Lao Cai, 2015-2016
IR-4, CSD
13 Support application of BFHI and nutrition related indicators (under new MOH quality assessment criteria); key essential newborn care interventions (active management of the third stage of labor, delay cord clamping, immediate skin to skin contact, and early initiation of breastfeeding, KMC) in provincial and all district hospitals:
Lao Cai, 2015-2016
IR-4, CSD
13.1 Support training for capacity building of new practices
Lao Cai, 2015-2016
IR-4, CSD
13.2 Support integrated monitoring/supervision of new practices
Lao Cai, 2015-2016
IR-4, CSD
14 Conduct outreach services to provide health, nutrition services (including IMAM) to the hard to reach villages and communities in most disadvantaged districts
Lao Cai, 2015-2016
IR-4, CSD
15 Support IMAM services in 9 communes of Bac Ha, and 02 provincial/district hospitals:
Lao Cai, 2015-2016
IR-4, CSD
15.1 Purchasing of the HeBi products for IMAM
Lao Cai, 2015-2016
IR-4, CSD
15.2 Monitoring IMAM implementation in hospitals and in the communes
Lao Cai, 2015-2016
IR-4, CSD
16 Support implementation of the IYCF model in Bac Ha and Si Ma Cai:
Lao Cai, 2015-2016
IR-4, CSD
16.1 Support implementation and functioning of the two communal child feeding clubs in Bac Ha and Si Ma Cai district.
Lao Cai, 2015-2016
IR-4, CSD
16.2 Support communication and counselling activities implemented by the village support groups in Bac Ha and Simakai under the IYCF model.
Lao Cai, 2015-2016
IR-4, CSD
16.3 Support training for capacity building on IYCF for health worker in the two districts
Lao Cai, 2015-2016
IR-4, CSD
17 Support communication activities at community on local food, how gardening and use of family food supply for child feeding:
Lao Cai, 2015-2016
IR-4, CSD
17.1 Adaption for new IEC materials to promote local nutrient rich food available, and child feeding.
Lao Cai, 2015-2016
IR-4, CSD
17.2 Organize communication activity via local loud speakers. And the local cultural event (ethnic culture)
Lao Cai, 2015-2016
IR-4, CSD
18 Capacity building for provincial team in data analysis and use of data for local planning, including application of nutrition online reporting system.
Lao Cai, 2015-2016
IR-4, CSD
19 Support joint visit of the provincial team to the IYCF model developed in Bac Ha and Si Ma Cai.
Lao Cai, 2015-2016
IR-4, CSD
19.1 Monitoring/supervision of communication skills performed by local staff
Lao Cai, 2015-2016
IR-4, CSD
19.2 Monitoring performance of the communal child feeding clubs, and village support groups
Lao Cai, 2015-2016
IR-4, CSD
20 Support end-line evaluation of the IYCF model in two project communes after 2 years:
Lao Cai, 2015-2016
IR-4, CSD
20.1 Carry out a follow up survey
Lao Cai, 2015-2016
IR-4, CSD
20.2 The final implementation review of the model
Lao Cai, 2015-2016
IR-4, CSD
21 Conduct an implementation review meeting of the provincial plan of action for reduction stunting 2013-2016, and formulation of the action plan 2017-2020
Lao Cai, 2015-2016
IR-4, CSD
22 Support bi-annual review meeting of the CSD component conducted by DOH
Lao Cai, 2015-2016
IR-4, CSD
23 Maintain CLTS in 6 old communes and expand to 10 new communes and verify and certify 27 ODF villages in 4 district of Si Ma Cai, Bac Ha, Sa Pa and Muong Khuong
Lao Cai, 2015-2016
IR-4, CSD
23.1 Training and triggering of CLTS/SLTS, on low-cost latrine construction and sanitation marketing and ODF procedures
Lao Cai, 2015-2016
IR-4, CSD
23.2 Review meetings with leaders at district and commune levels
Lao Cai, 2015-2016
IR-4, CSD
23.3 Community mobilization such as village meeting, household visits.
Lao Cai, 2015-2016
IR-4, CSD
23.4 Organize forums with entrepreneurs, local leaders and related sectors on low-cost latrine options and promotion of sanitation products.
Lao Cai, 2015-2016
IR-4, CSD
23.5 Monitoring review meetings and study visits to best practices
Lao Cai, 2015-2016
IR-4, CSD
23.6 Verify and certify ODF villages
Lao Cai, 2015-2016
IR-4, CSD
24 Develop post 2015 provincial WASH plan, focusing scaling up of sanitation and sustainability of WASH facilities in communities and schools.
Lao Cai, 2015-2016
IR-4, CSD
25 Replicate HWTS to districts of Si Ma Cai and Sa Pa
Lao Cai, 2015-2016
IR-4, CSD
25.1 Training on HWTS
Lao Cai, 2015-2016
IR-4, CSD
25.2 Community mobilization activities (household visits, village meeting, radio, communication campaigns)
Lao Cai, 2015-2016
IR-4, CSD
25.3 Water quality testing
Lao Cai, 2015-2016
IR-4, CSD
25.4 Demonstrate low-cost locally appropriate HWTS options
Lao Cai, 2015-2016
IR-4, CSD
25.5 Monitoring of communication activities and HWTS guidance, and study visits to best practices
Lao Cai, 2015-2016
IR-4, CSD
26 Update NRWSS M&E system
Lao Cai, 2015-2016
IR-4, CSD
27 Support development and implementation of provincial/communal detailed WASH DRR/CCA plan

![For personal use only - ASX · LQ OLQH ZLWK WKH JURZWK LQ VL]H FKDQJHV LQ WKH QDWXUH DQG LQFUHDVH LQ FRPSOH[LW\ RI WKH &RPSDQ\µV EXVLQHVV 7KH %RDUG DLPV WR DFKLHYH DOO RI WKH %HVW](https://static.fdocuments.us/doc/165x107/6033be650997f55a9c1d9a47/for-personal-use-only-asx-lq-olqh-zlwk-wkh-jurzwk-lq-vlh-fkdqjhv-lq-wkh-qdwxuh.jpg)