Jeffrey R. Dugas, MD Birmingham, Al...Exclusively single -bundle Autograft PTG greater than 75%...
50
Jeffrey R. Dugas, MD Birmingham, Al Mark Clatworthy Tim Roberts Middlemore Hospital Auckland New Zealand
Transcript of Jeffrey R. Dugas, MD Birmingham, Al...Exclusively single -bundle Autograft PTG greater than 75%...

Jeffrey R. Dugas, MD Birmingham, Al
Mark Clatworthy Tim Roberts
Middlemore Hospital Auckland
New Zealand
No disclosures related to the subject matter of this presentation.

Significant changes in the way ACL surgery is performed Double Bundle Various Femoral Tunnel Drilling techniques Addition of various biologic “enhancements”

Basic science supports the fact that the ACL is comprised of two “bundles” of fibers which function in conert.
Idea of recreating two bundles certainly seems reasonable given the native anatomy
Clinically challenging technique to get two grafts at the native origin of the ACL

Clinical results have (to date) failed to show superiority or reliable equivalence to large scale clinical studies of single bundle ACL reconstruction.
Many early adopters of this technique have returned to single bundle ACL reconstruction.

Transtibial drilling was the most common technique until 5-10 years ago. Evidence that transtibial drilling led to
unacceptable position of the femoral tunnel Possible cause of early failure of ACL graft due
to vertical orientation. Medial Portal Drilling espoused as the solution
to more accurately recreate the normal anatomic origin of the ACL.
Miller et al and others 2010-2014 “It is borderline malpractice to drill through the
tibial tunnel.”


Exclusively single-bundle Autograft PTG greater than 75% Autogranft HS greater than 20% Allograft PTG less than 5%
Nearly all femoral tunnels drilled TT (>95%) ? Are we doing this wrong? If so, are we not seeing our own failures, or are we doing
something different which allows us to get lower on the wall Are we settling for a lesser graft position without knowing it?
Asked outgoing fellows how our technique is different from what they experienced in residency/experience
Bigger Notchplasty Use of a fixed angle tibial guide (45 degrees) Free-hand reaming of femoral tunnel
No drill guides for femoral tunnel placement
“you get pretty low” Compliment?

1. To determine if there was any benefit to notchplasty in placing the femoral tunnel transtibially
2. To determine the amount of fill of the native ACL origin using the two techniques before and after notchplasty.
3. To measure the tunnel length using the two techniques to better understand the risk of posterior cortical compromise
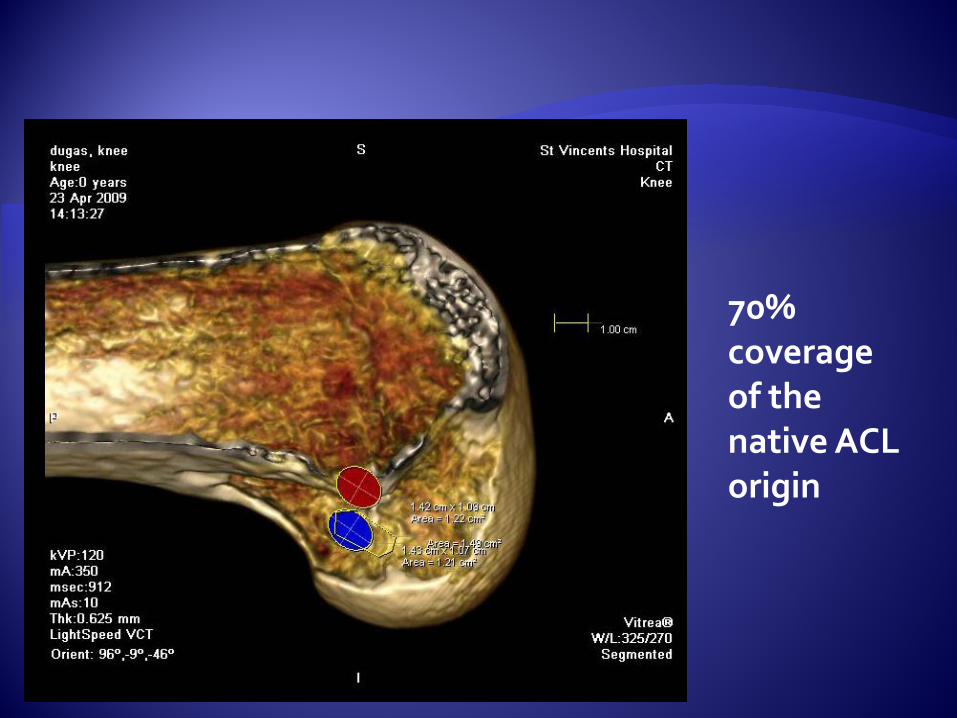
70% coverage of the native ACL origin
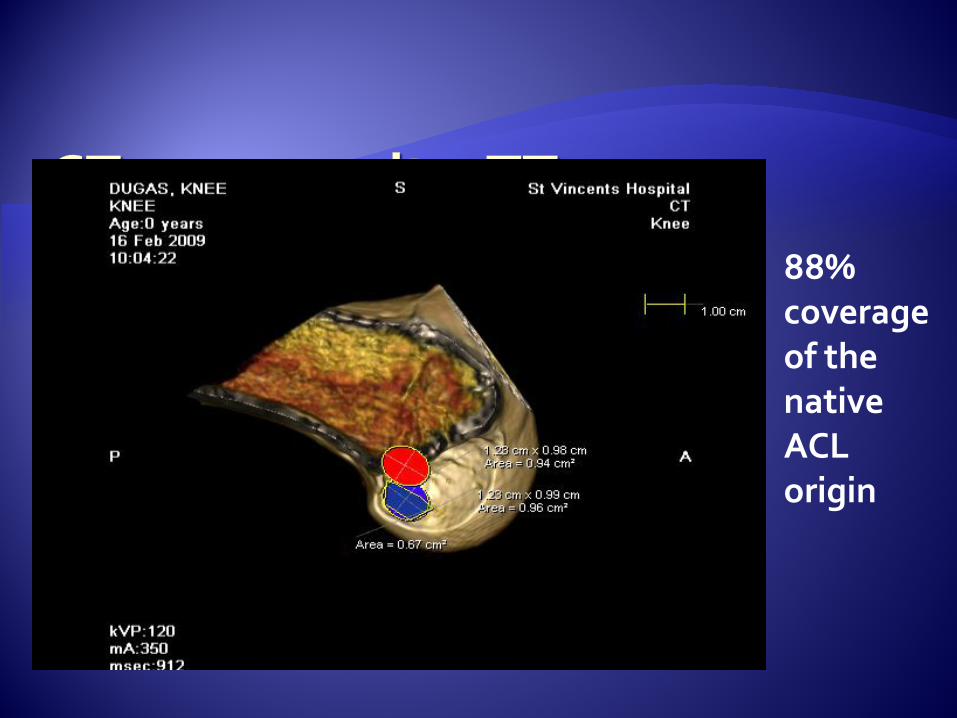
88% coverage of the native ACL origin

Post-notchplasty transtibial drilled femoral tunnels yielded 68.3% coverage of the native origin of the ACL.
Post-notchplasty MP drilled femoral tunnel yielded 67.6% coverage of the native origin of the ACL.
No Notchplasty yielded less than 30% coverage in the MP group and less than 10% coverage in the TT group

Single surgeon clinical experience with clinical follow-up

Prospective study - Private practice
August 2000 - May 2009 – Hamstring transtibial ACLR
Transtibial technique – . Medial tibial incision - oblique shallow tibial tunnel. High AM femoral position still within the footprint.
May 2009 – May 2013 – Hamstring Transportal ACLR
Transportal ACLR technique - 30% distal (forward) off the back wall and lower (posterior), More anterior tibial tunnel – centromedial
All patients had Endobutton/Retrobutton for femoral fixation and Intrafix/GraftBolt for tibial fixation
Failure - return to surgeon for revision, clinical failure with MRI and known revision by other surgeon - Will underestimate failure rate

TransTibial TransPortal

52 failures in 1016 TT ACLR followed for 6-15 years mean 8.9 years - 5.1% failure rate
31 failures in 464 TP ACLR followed for 2-6 years mean 4 years - 6.7% failure rate
13 failures in 419 TT ACLR followed for 2-6 years 3.1% failure rate TP technique 2.2 X higher failure rate
Hazard Ratio – more sophisticated evaluation that allows for variation in follow up The TP technique has a 2.4 X higher hazard ratio than the TT technique p=<0.001
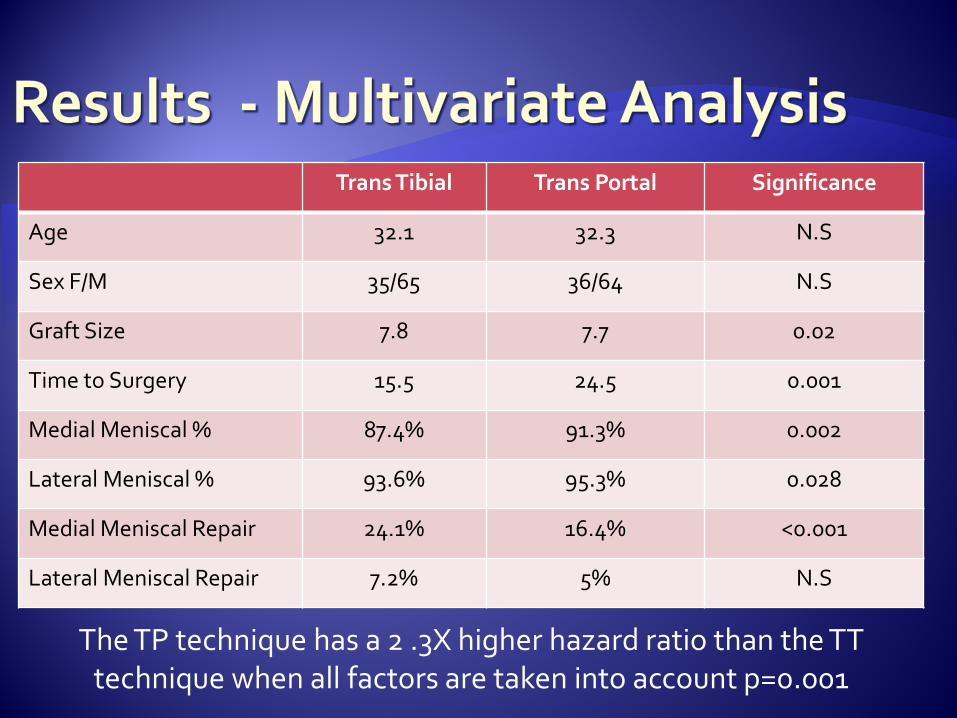
Trans Tibial Trans Portal Significance
Age 32.1 32.3 N.S
Sex F/M 35/65 36/64 N.S
Graft Size 7.8 7.7 0.02
Time to Surgery 15.5 24.5 0.001
Medial Meniscal % 87.4% 91.3% 0.002
Lateral Meniscal % 93.6% 95.3% 0.028
Medial Meniscal Repair 24.1% 16.4% <0.001
Lateral Meniscal Repair 7.2% 5% N.S
The TP technique has a 2 .3X higher hazard ratio than the TT technique when all factors are taken into account p=0.001
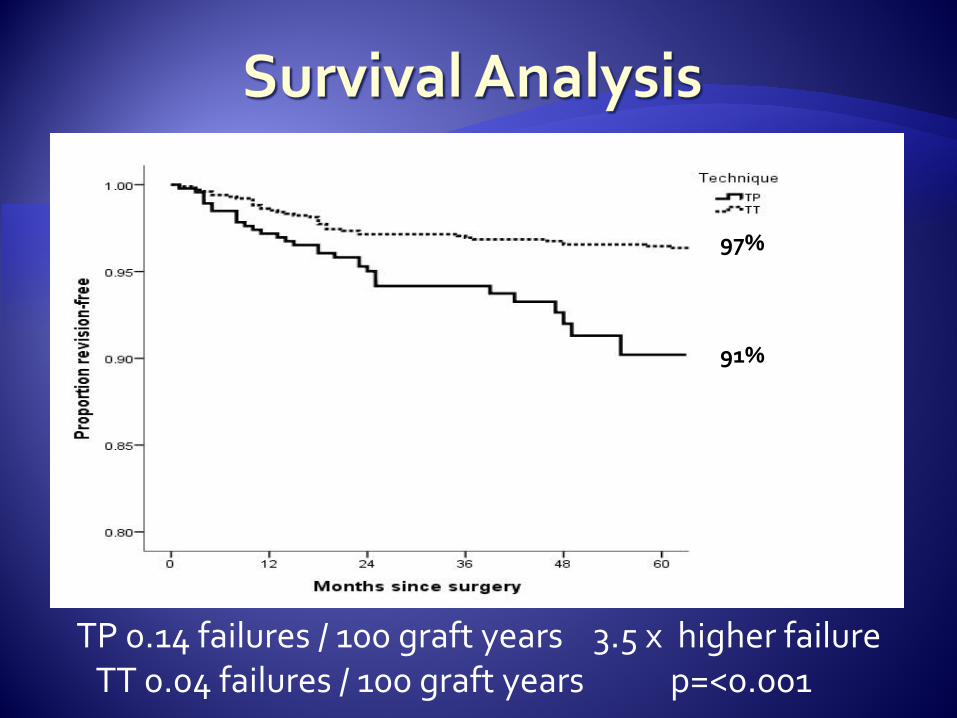
TP 0.14 failures / 100 graft years 3.5 x higher failure TT 0.04 failures / 100 graft years p=<0.001
97%
91%

61% of TP ACLR’s failed < 1 year post surgery
27% of TT ACLR’s failed < 1 year post surgery p=<0.0001
Mean time to failure within 6 years TP 12.2 months, TT 29.2 months p =0.02
Changed in May 2013 to AM femoral tunnel, continued with
transportal, maintained centromedial tibia. Increased BPB ACLR’s
Last two years TP AM femur - 178 hamstring patients 1 failure 0.5% ruptured within two years
BPB AM femoral footprint – 30 patients No failures
First 2 years TP central femoral footprint 238 patients. 9 graft failures – 3.8% ruptured within 2 years
First 2 years TT AM femoral footprint, posterior tibial tunnel 171 patients – 3 graft failures - 1.8% ruptured within 2 years
The TP technique has a 2.3 x higher hazard ratio for failure than the TT technique with a multi-variate analysis p=0.002
With a 6 year follow up TP ACLR has 2.2x higher failure rate than TT ACLR
The TP technique has a 3.5 X higher failure rate when utilising failures / 100 graft years
TP ACLR’s failure have a higher earlier failure rate - 61% vs 27% < 1 year post surgery p=0.001
Moving the femoral tunnel back to a high AM position has resulted in a 7.2X lower failure rate
Placement of the ACL graft in an more central footprint position results in a higher failure rate and an earlier failure than placement in a high AM position

Anatomy Re-evaluation – Direct vs Indirect Fibres
Histological Evaluation of Footprints Sectional Fibre ACL Biomechanical Analysis
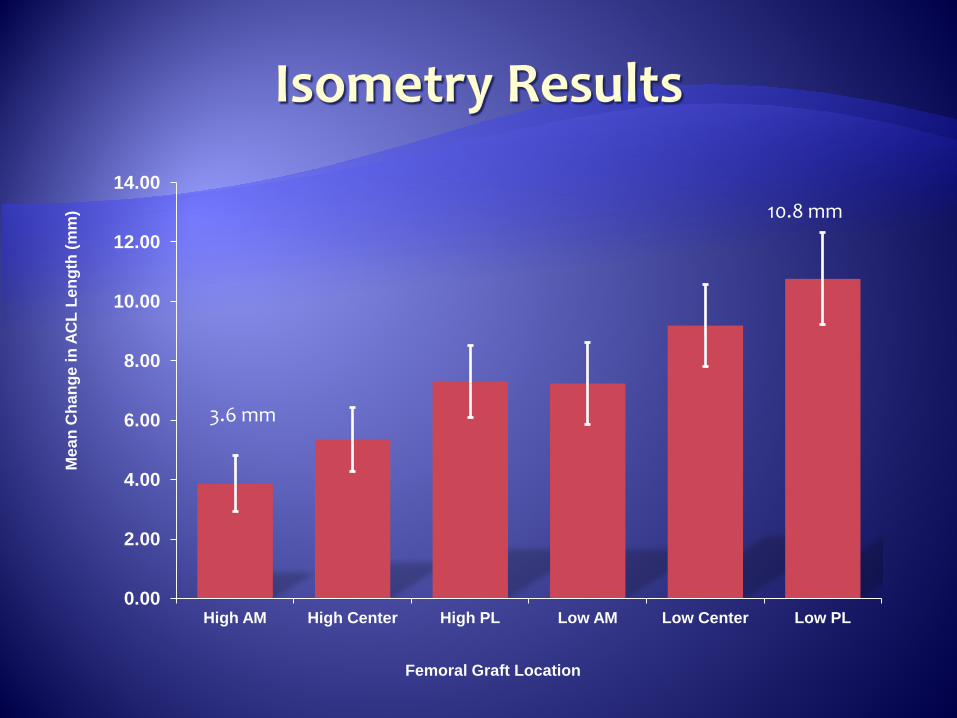
Isometricity Evaluation

Robert Smigielski Dissection of 111 fresh cadaveric knees Flat insertion; Not 2 bundles The ACL arises from the lateral intercondylar
ridge
Presenter
Presentation Notes
So we went ahead and revisited the anatomy. What became apparent from attending ACL-focused meeting, including the ACL study group, was that a number of groups had done so in the past year. One investigator deserves mention. Robert Smigielski, Orthopedic Surgeon in Warsaw, Poland.
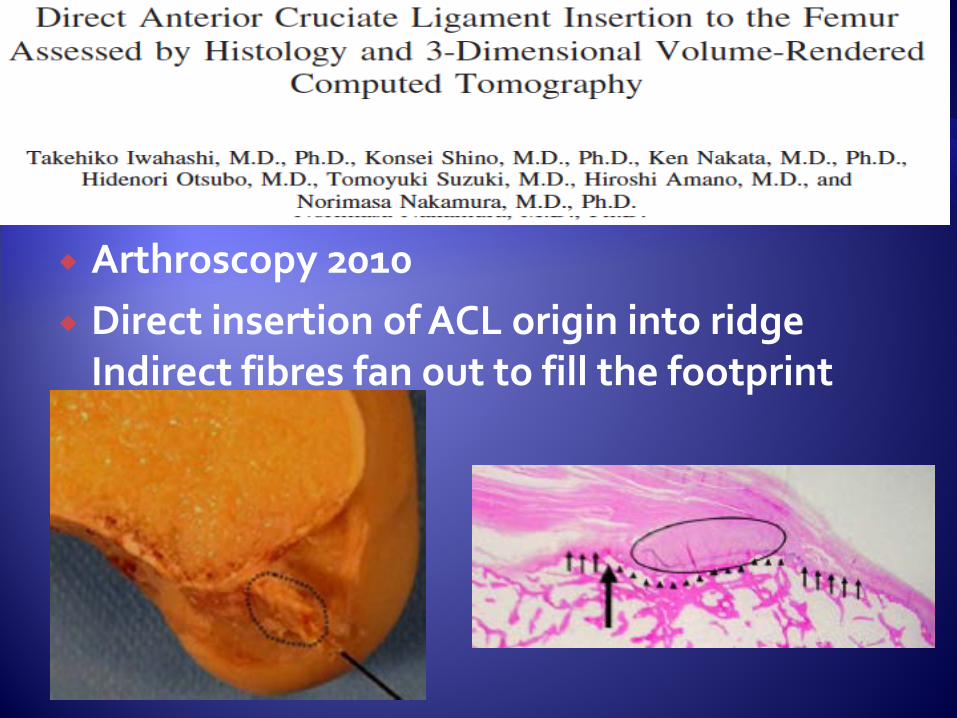
Arthroscopy 2010 Direct insertion of ACL origin into ridge
Indirect fibres fan out to fill the footprint
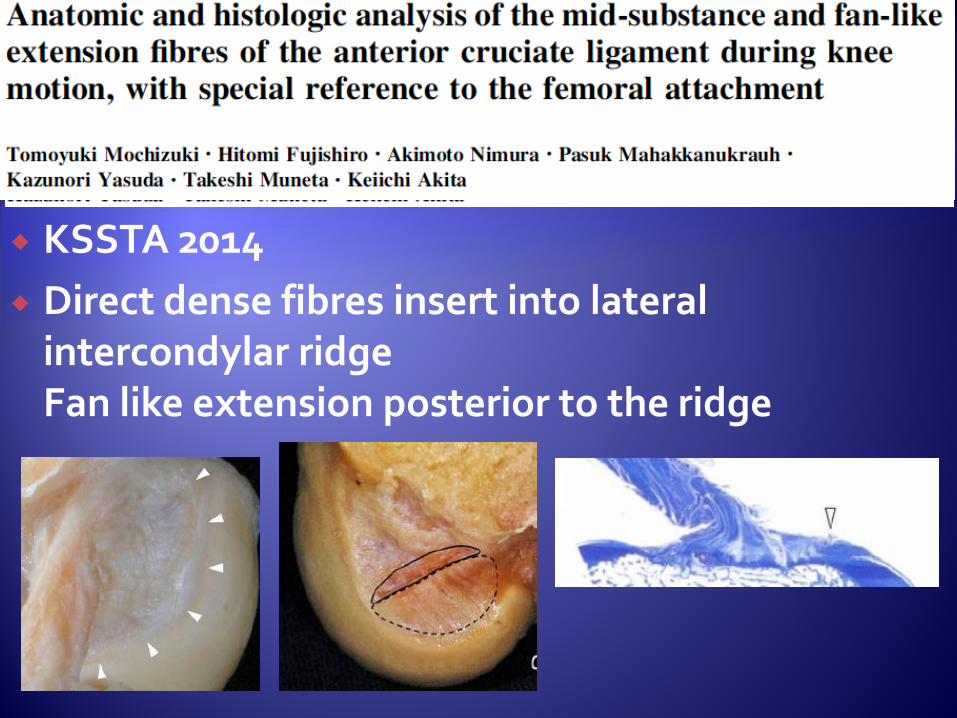
KSSTA 2014 Direct dense fibres insert into lateral
intercondylar ridge Fan like extension posterior to the ridge


Presenter
Presentation Notes
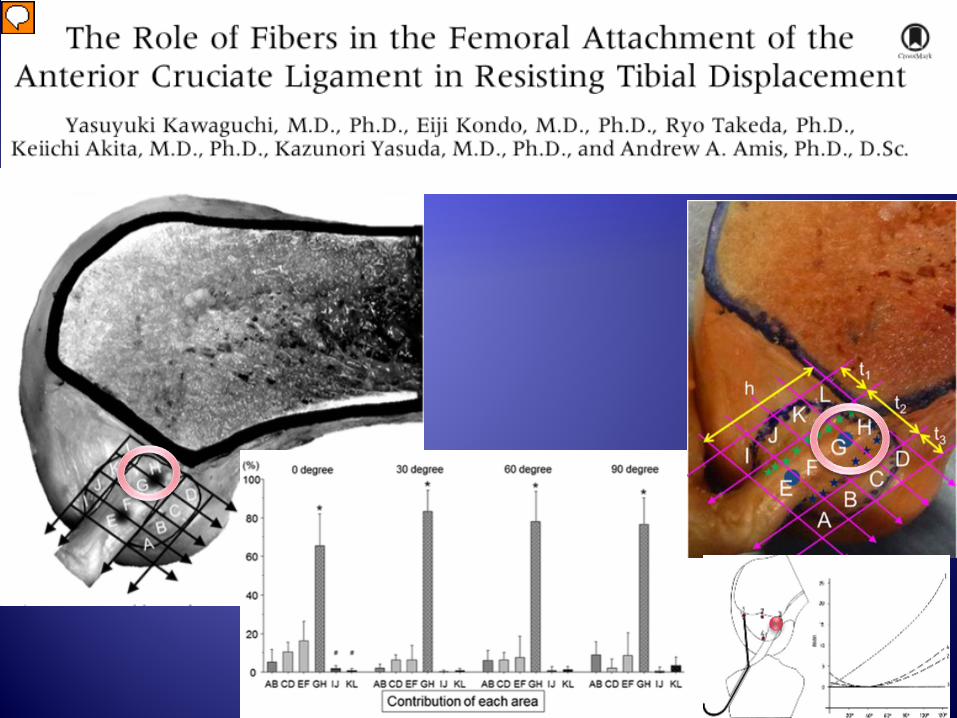
Central area resistd 80-90% of anterior force during anterior stress testing Proximal region (GH) resisted 70-80% of the anterior force during anterior stress testing

Lachman Anterior Draw

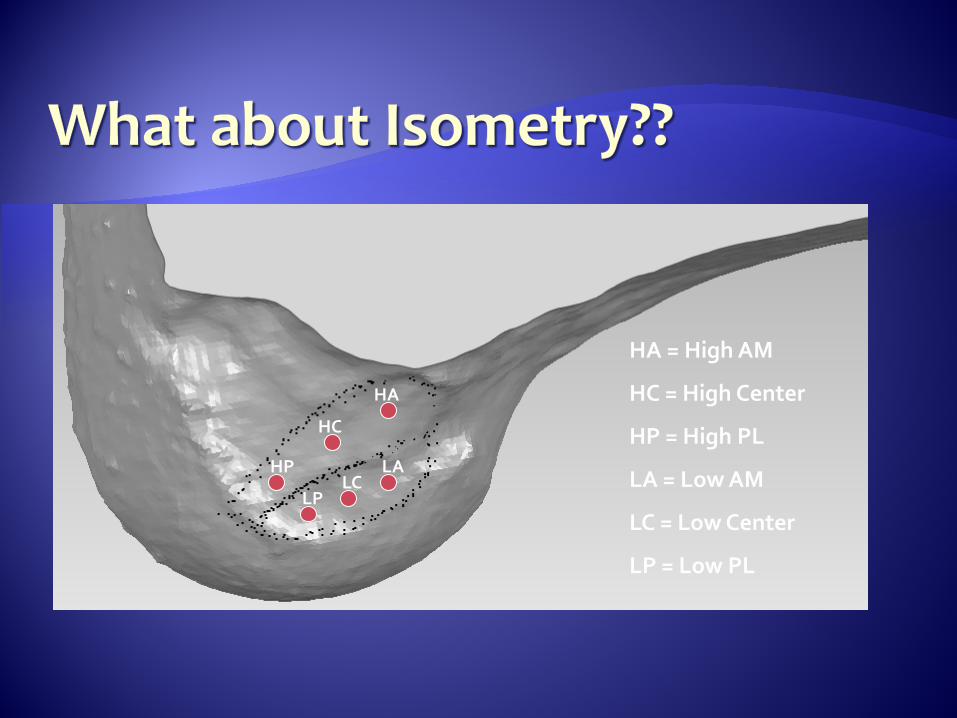
HA
HC
HP LA LC
LP
HA = High AM
HC = High Center
HP = High PL
LA = Low AM
LC = Low Center
LP = Low PL
0.00
2.00
4.00
6.00
8.00
10.00
12.00
14.00
High AM High Center High PL Low AM Low Center Low PL
Mea
n C
hang
e in
AC
L Le
ngth
(mm
)
Femoral Graft Location
3.6 mm
10.8 mm
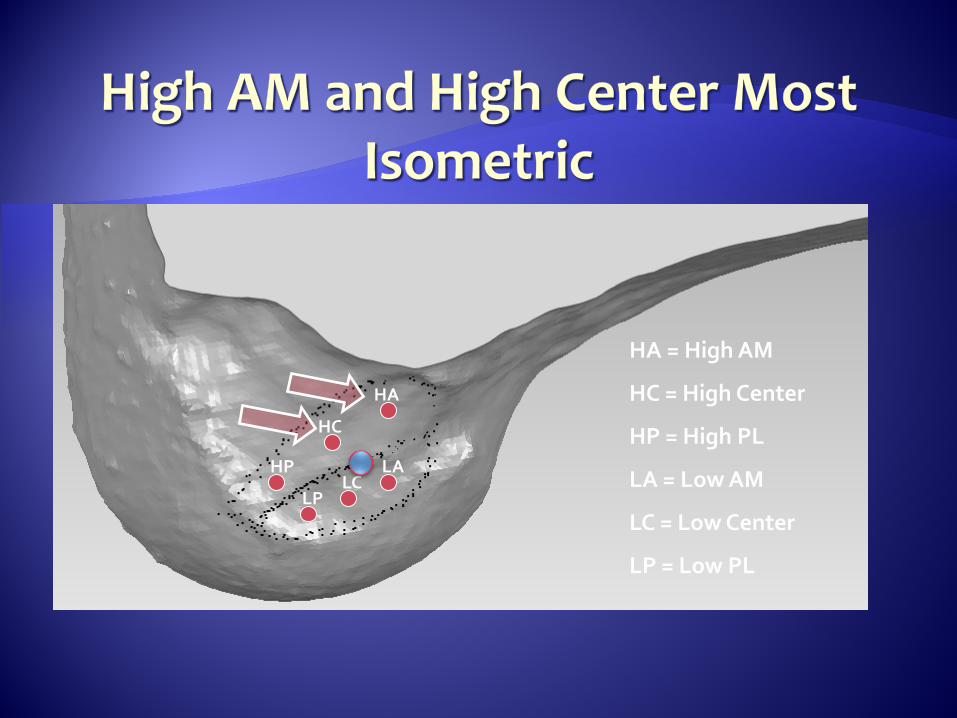
HA
HC
HP LA LC
LP
HA = High AM
HC = High Center
HP = High PL
LA = Low AM
LC = Low Center
LP = Low PL

More forward (distal) and lower (posterior) femoral graft placement does not replicate the direct insertion of the ACL which is the lateral intercondylar ridge This results in an anisometric graft with higher strain through the graft
This is the likely explanation for the increased failure rate of “Central Footprint ACLR”
80% of the functional ACL fibers arise from the AM bundle. The AM bundle is more isometric

Worse biomechanically to be lower on the wall (more posterior) than to be higher on the wall (more anterior).

“The biggest mistake I made in my entire career in sports medicine was to try to get lower on the wall drilling my femoral tunnels.” Dr. Russell Warren
Basic science studies that give us valuable information about native anatomy may not always lead us in the direction of clinical success. Time zero surgical appearance is not always
indicative of final clinical outcome
Must always strive first for clinical success

Regardless of how the femoral tunnel is drilled in ACL surgery, the key is to get the graft into the most normal position possible to allow for normal biomechanics when the graft is healed and mature.
Lower doesn’t mean better.